
Abstract
The aim of this study was to investigate current nursing practice related to end-of-life discussions with incurable lung cancer patients and their family caregivers from the perspectives of patients, family caregivers, and nurses in an oncology outpatient clinic. This phenomenological hermeneutic study included nine patients, eight family caregivers, and 11 nurses. Data were collected using participant observation, informal and semi-structured individual or joint interviews with patients and family caregivers, and focus group interviews with nurses. A Ricoeur-inspired approach was used to analyze the data. Three themes were identified: (a) content of end-of-life discussions, (b) timing of end-of-life discussions, and (c) challenges in end-of-life discussions. End-of-life discussions were seldom initiated; when they were, it was often too late. Discussions addressed treatment, place of care, practical/economic concerns, and existential matters. The physical environment at the outpatient clinic, lack of continuity, and nurses’ instrumental task workloads and time pressure posed challenges to initiating end-of-life discussions.
Lung cancer is the primary cause of cancer-related mortality worldwide (Ferlay et al., 2015). In Denmark, 7% of all deaths are related to lung cancer (Danckert et al., 2019). In light of the 1-year relative survival rate of 44% for men and 53% for women, many patients are offered palliative chemotherapy (Danckert et al., 2019; Lee et al., 2015). Due to the limited life span of many patients with lung cancer, initiating end-of-life discussions with patients and family caregivers early in the treatment course may be important preparation for later care (Walczak et al., 2016).
The goal of end-of-life discussions is to engage patients and their families at an early stage of the disease to discuss topics such as treatment, prognosis, expectations, thoughts, and wishes for end-of-life and care planning (Bergenholtz et al., 2019, 2020). End-of-life discussions are beneficial, often allowing patients to die in their preferred locations, and some patients even live longer and improve their quality of life (Brinkman-Stoppelenburg et al., 2014; Hansen et al., 2020; Janssen et al., 2012). Rylander and colleagues (2019) investigated end-of-life discussions in an oncology ward in Sweden and concluded that they often only included physician- and treatment-focused topics. However, the authors did not investigate such discussions in oncology outpatient clinics. In addition, a systematic review concluded that most families want to talk about end-of-life issues, but readiness and being comfortable and willing to talk about end-of-life issues were main facilitators of end-of-life discussions among family members or with health care professionals (Zwakman et al., 2018).
Nurses talk with and interact with families on a daily basis and are among the health care professionals who spend the most time with patients and family caregivers (Butler et al., 2018). Due to their central role in active treatment, nurses have the opportunity to facilitate timely end-of-life discussions (Rylander et al., 2019). Nurse-described barriers to facilitating discussions with patients with incurable cancer and their families include lack of nurse experience and education, a focus on medical issues, and nurse discomfort with initiating this type of discussion (Broom et al., 2016; de Angst et al., 2019; McLennon, Lasiter, et al., 2013; McLennon, Uhrich, et al., 2013; Mohammed et al., 2020; Pettersson et al., 2018).
In Denmark, the Danish Health Authority recommends that end-of-life discussions take place during the course of treatment in the community, at the hospital, and/or at the general practitioner’s office. Despite this recommendation and documented benefits, no structured approach to end-of-life discussions exists to date in Denmark, which very likely contributes to delays in initiating these discussions (Skorstengaard et al., 2017). Bergenholtz and colleagues investigated the nursing practice of end-of-life discussions with a mixed population in a medical department in Denmark, concluding that these discussions are often initiated too late or not at all (Bergenholtz et al., 2015, 2016, 2019). Thus, existing knowledge is limited about current nursing practice for end-of-life discussions with patients with incurable cancer in outpatient oncology settings in Denmark and internationally. To our knowledge, no studies have investigated end-of-life discussions in an outpatient oncology setting from the perspective of patients, family caregivers, and nurses. These three perspectives could together contribute significantly to existing knowledge and give insight into and clarify what is needed to improve current practice from all perspectives.
The aim of this study was to investigate current nursing practice related to end-of-life discussions with incurable lung cancer patients and their family caregivers from the perspectives of patients, family caregivers, and nurses in an oncology outpatient clinic.
Method
The phenomenological hermeneutic approach used in this study was inspired by the formative work of Paul Ricoeur and guided the collection of data and analysis (Simony et al., 2018). To structure the article, we used the Standards for Reporting Qualitative Research (SRQR; O’Brien et al., 2014).
Concepts
Several concepts related to end-of-life discussions are documented in the literature: end-of-life conversations, end-of-life communication, shared decision making, and advance care planning (Bergenholtz et al., 2020; Brighton & Bristowe, 2016; Elwyn et al., 2010; Mullick et al., 2013).
End-of-life discussions
End-of-life discussions in this study refers to a broad concept of discussions between nurses, patients, and family caregivers that may include treatment decisions, prognosis, preferences, and wishes for daily life.
Family caregivers
Family caregivers are defined by the patient and include blood-related relatives, close friends, or both (Holstein & Gubrium, 1999).
Palliative care
This study uses the World Health Organization definition of palliative care: an approach that improves the quality of life of patients (adults and children) and their families who are facing problems associated with life-threatening illness. It prevents and relieves suffering through the early identification, correct assessment, and treatment of pain and other problems, whether physical, psychosocial, or spiritual (World Health Organization, 2020).
In Denmark, palliative care is organized into specialized palliative care provided by a multidisciplinary team educated in palliative care in hospices, palliative teams, and palliative departments, and general palliative care provided by any health care professional who is not a member of a specialist team as a part of standard clinical practice in hospitals, homecare, nursing homes, and at general practitioners’ offices (Danish Health Authority, 2017).
Participants and Setting
Patients were included if they had been diagnosed with non-small-cell lung cancer, small-cell lung, or mesothelioma and were receiving second-line palliative chemotherapy. Family caregivers were included if they were older than 18 years. Nurses were included if they provided the patient’s chemotherapy. Purposeful sampling targeted a diverse set of participants who had experience with end-of-life discussions. The sample consisted of 28 participants: nine patients, eight family caregivers, and 11 oncology nurses. The characteristics of patients and family caregivers and of nurses are, respectively, presented in Tables 1 and 2. All participants were recruited from an outpatient oncology clinic providing general palliative care at an academic teaching hospital in Denmark.
Characteristics of Patients and Family Caregivers.
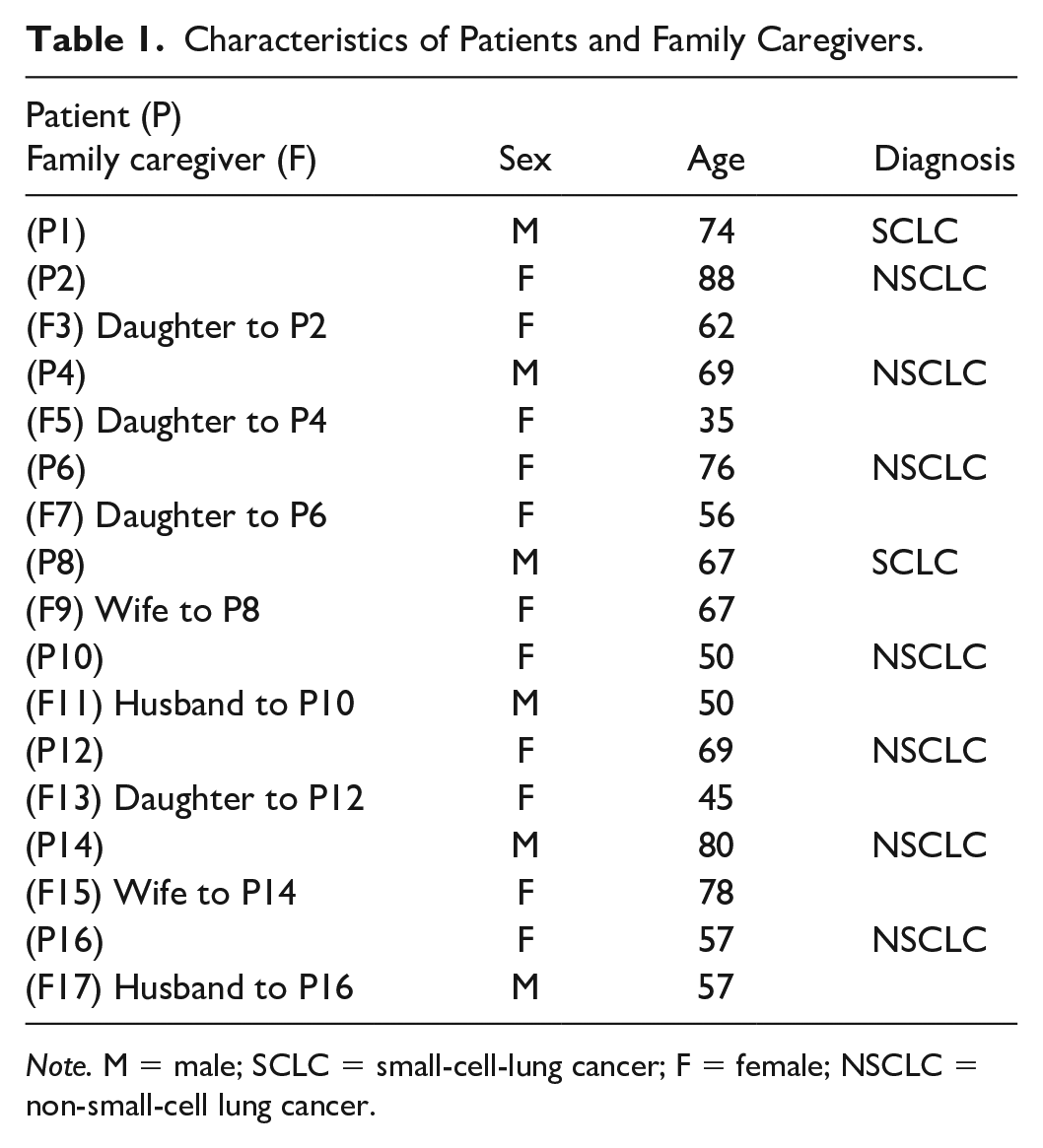
Note. M = male; SCLC = small-cell-lung cancer; F = female; NSCLC = non-small-cell lung cancer.
Characteristics of Nurses.
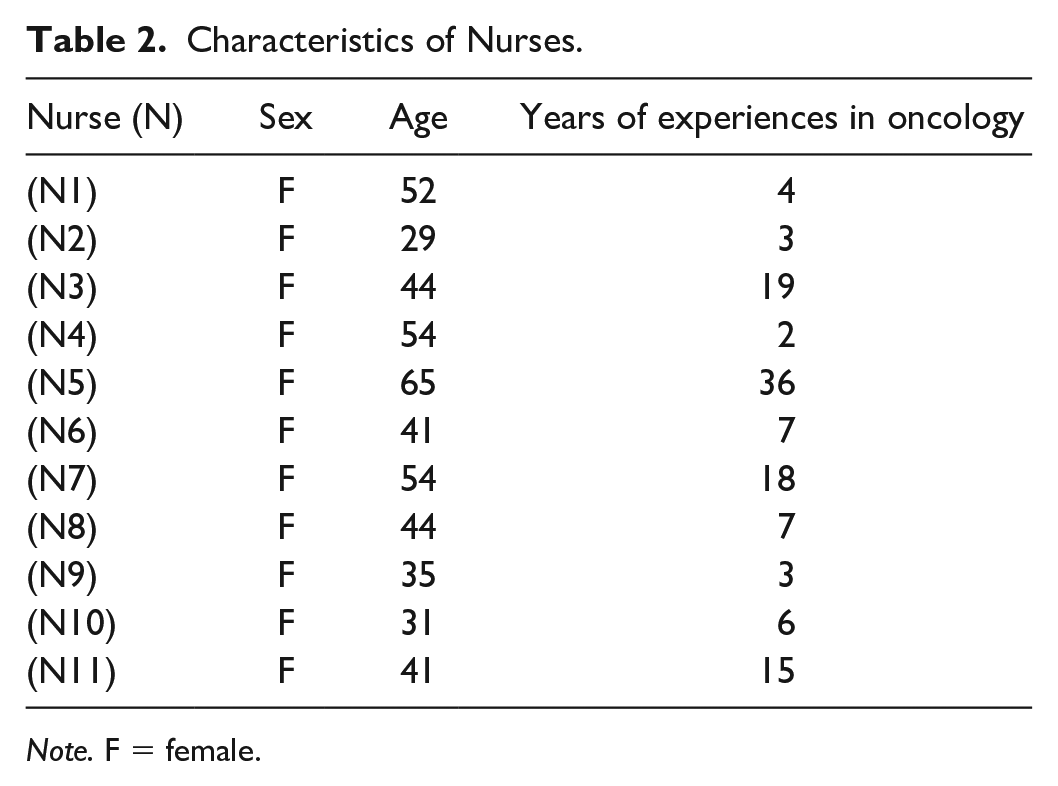
Note. F = female.
Data Collection
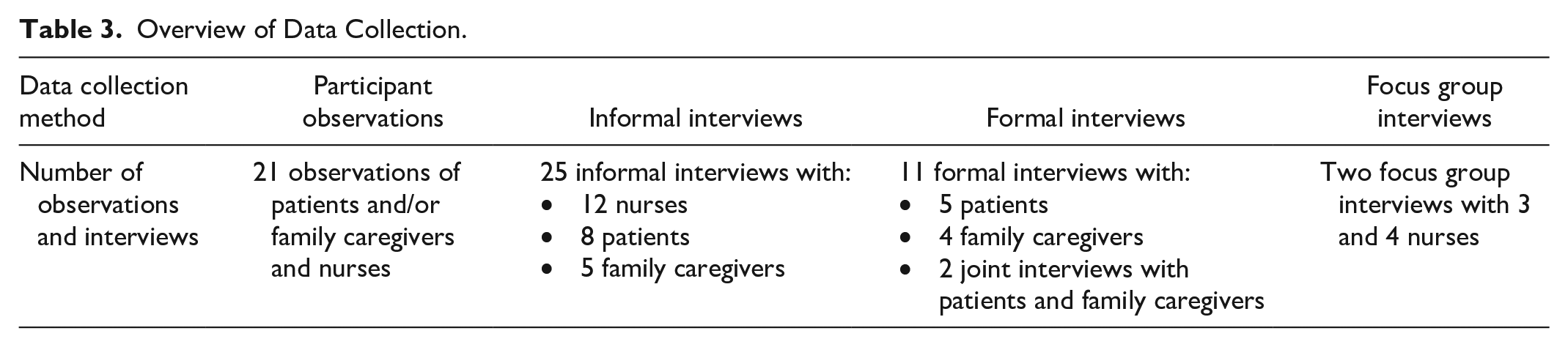
Data were collected through participant observations and informal interviews with patients, family caregivers, and nurses inspired by Kristiansen and Krogstrup (2015) and Spradley (2016); semi-structured individual or joint interviews with patient and family caregivers; and semi-structured focus group interviews with nurses inspired by Kvale and Brinkman (2009). The methods were chosen to ensure obtaining detailed knowledge about current practice (Table 3). The first author (T.I.) collected all data between August 2019 and June 2020.
Overview of Data Collection.
Participant observations and informal interviews
Participant observations included all situations where patients, family caregivers, and nurses interacted, for example, patients receiving chemotherapy; conversations between patients, family caregivers, and nurses; and medical conversations with physicians. The first author observed patients and their family caregivers up to 4 times during the course of treatment: (a) when initiating the first series of palliative chemotherapy, (b) when receiving the second series of palliative chemotherapy, (c) at follow-up consultations with the oncologist and nurse, and (d) when receiving the third series of palliative chemotherapy. Sample questions guiding observations included the following: Who was present? What did they talk about? What did they do? (Spradley, 2016). Observations lasted from 30 min to 2 hr. A total of 21 participant observations were undertaken with a collective duration of 21 hr. A total of 25 short informal interviews lasting 2 to 15 min were also conducted during participant observations. Handwritten field notes developed during observations consisted of short notes of what was said and done.
Formal interviews
Semi-structured individual or joint interviews were conducted with patients and family caregivers. Interview participants decided the place, time, and type (individual or joint) of the interview. The semi-structured interview guide consisted of questions about decisions during the cancer trajectory, daily life with cancer and palliative chemotherapy, and experiences with end-of-life discussions at the outpatient clinic and at home within families. One family lacked resources to attend interviews, and one family attended only interviews and no participant observations due to COVID-19. A total of 11 formal interviews were completed: five with patients, four with family caregivers, and two joint interviews. Interviews were audio recorded and transcribed within 24 hr by T.I.
Focus group interviews
Two focus group interviews lasting 90 min each were conducted with nurses during their regularly scheduled shifts. T.I. facilitated group interviews and K.B.D. acted as co-moderator by monitoring the time and asking any follow-up questions. An interview guide addressed the study aim and consisted of questions about nurses’ experiences with end-of-life discussions, challenges to and facilitators of end-of-life discussions, and timing and content of end-of-life discussions (Kvale & Brinkman, 2009).
Ethical Considerations
The study was approved by the Danish Data Protection Agency (Journal No. 18/60988). The study did not require approval by the Regional Committees on Health Research Ethics for Southern Denmark (Journal No. S-20172000-90). Data were stored safely in SharePoint. Participants received verbal and written information about the study and were informed that they could withdraw at any time without consequence. Names were anonymized. All patients were receiving palliative chemotherapy, some after a relapse following initial surgical treatment and some from the time of diagnosis, and first author continuously reflected on how to approach vulnerable patients and family caregivers. A challenging situation occurred during simultaneous observations and interviews. Many patients were sad and cried, especially during the interviews, and the interviewer had to balance whether to continue with the interview or to stop. Patients and family caregivers were always given a telephone number after the interviews, and told they should call directly if they had questions or thoughts afterward, but no one did. Because patients often received chemotherapy in the same room as other patients, in-depth and more sensitive questions related to participant observations, that is, questions about end of life, were postponed to semi-structured interviews.
Data Analysis
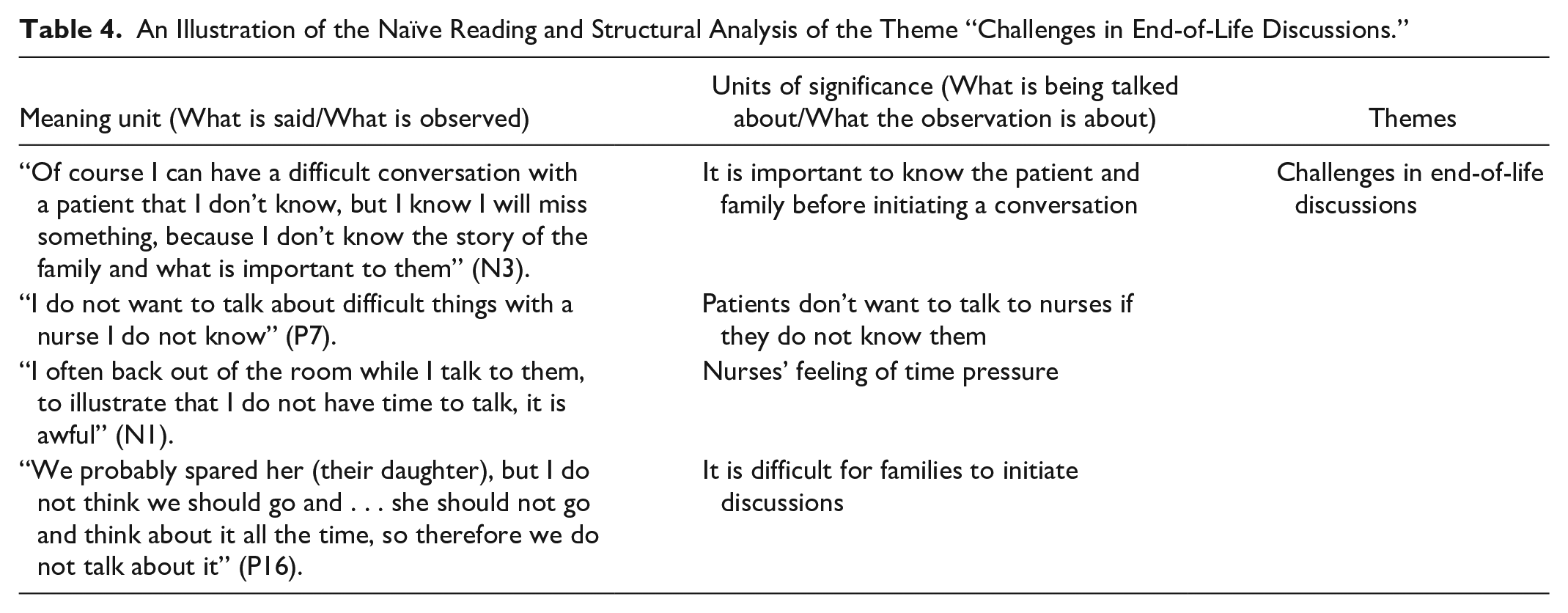
A method inspired by Paul Ricoeur for analyzing participant observations and interviews was used to analyze the data (Simony et al., 2018). It consisted of three related phases: naïve reading, structural analysis, and critical interpretation and discussion. Naïve reading involved transcribing the text and reading it through several times to obtain a first understanding of the text and participants’ experiences. The purpose of the structural analysis was to validate the first interpreted whole and understand the meaning of the text from what was said/observed to what was being talked about/what the observation was about and afterwards find patterns. Based on their similarities and differences, meaning units were then merged to create themes (Table 4). The final phase, critical interpretation and discussion, led to a comprehensive understanding. The findings were discussed from the perspectives of Family Systems Nursing theory, theory of organizational culture, and existing literature.
An Illustration of the Naïve Reading and Structural Analysis of the Theme “Challenges in End-of-Life Discussions.”
Results
Three themes synthesizing the perspectives of patients, family caregivers, and nurses emerged from the analysis: (a) content of end-of-life discussions, (b) timing of end-of-life discussions, and (c) challenges in end-of-life discussions.
Content of End-of-Life Discussions
The most common topics addressed in end-of-life discussions were treatment, location of care, practical and economic concerns, and existential matters.
End-of-life discussions often were treatment focused, initiated by the oncologist during medical conversations at which nurses were also present, but seldom engaged: “So, how long will it prolong life if I continue the treatment?” the patient asked. The oncologist says that she can’t tell exactly. The oncologist asks what the patient thinks about the treatment. The patients says she wants to continue. The conversations ends. The nurse doesn’t take any part in the conversation, she looks into the computer and writes in the medical record. (Observation, P2, N1)
Patients and family caregivers experienced end-of-life discussions as rarely being initiated. One patient said, “They (the nurses) really know a lot about side effects, so of course we talk a lot about that” (Interview, P6). Even though patients and family caregivers experienced discussions with the nurses as being primarily focused on treatment, they had many thoughts about the end of life, as in the case of a 50-year-old woman: The other day on the way home from the hospital, I told my husband that I wanted to be cremated and where I wanted the urn to be buried. That was really good, because he actually did not have any clue about it. (Interview, P10)
Similarly, some family caregivers had end-of-life concerns and wishes, but they rarely initiated family discussions. As a husband described, We soon need to talk about hospice referral; I cannot handle it at home anymore . . . We have not talked about what will happen when she gets more ill. I have thought about it many times, but does she feel I am selfish if I want to talk about it? Because I mean, this care is difficult. She cannot put on her sweater now, but if I have to change underwear and clothes. I cannot. It won’t work. (Interview, F17)
Nurses noted that they seldom initiated end-of-life discussions with patients and family caregivers. As one said, So I actually don’t think we talk much with the families, but of course you can have a talk with them whether they want to end their life on hospice or at home, but it is only if you sense they want to talk about it. (Interview, N9)
Nurses only initiated end-of-life discussions if they sensed that patients were ready. Even though nurses seldom had end-of-life discussions with patients and family caregivers, two described discussing practical and economic concerns, such as the sale of a home, because they believed it was important for families to clarify those topics. One nurse said, “I believe it is important to the families, at least early in the process, to talk about what should happen to the house” (Focus group interview, N5). Almost all patients described considerations about selling their home or moving into a smaller apartment. A 74-year-old man living alone said, “Soon I will consider selling the house and moving closer to the city in a smaller apartment, it will get easier to do grocery shopping and my family also lives in the city” (Interview, P1). Family caregivers also described the importance of talking and making decisions about house sales. One daughter said, “I really think it is important to talk about selling the house, at least before my mother gets more ill. It is important to plan while she is still capable of making her own decisions” (Interview, F7). Only one family had talked through the entire course of palliative treatment: “Everything from the last will, to funeral, to house sale is completely in order. It gives us all peace of mind” (Interview, P7). The family of another patient described discussing and clarifying their practical and economic concerns as a “huge relief.”
Some nurses described talking with patients about existential matters, but none had done so with any of the participating families. One nurse said, “I have experienced that they are afraid of dying, and they ask me how the dying process takes place” (Focus group interview, N6). The nurses who discussed existential matters were those with the most experience in oncology nursing.
Timing of End-of-Life Discussions
Most patients and family caregivers wanted to talk about the future at different times throughout treatment, and the timing depended on the topic. In interviews, most patients expressed thoughts about practical and economic concerns early in treatment. As one said, “I have thought about selling my house, but I have not thought about what should happen in the future, I believe my health is too good to talk about topics like that” (Interview, P1). Most patients believed their health was too good to talk about future care in the palliative care trajectory. Conversely, early in treatment, family caregivers wanted to plan the future and end-of-life care: “I really think it would be a relief to get things in order before my mother become more ill” (Interview, F5). However, both patients and family caregivers reported that they had not talked to any nurses about their considerations. One patient said, “We haven’t talked to the nurses about it. It is only me and my husband” (Informal interview, P16). The nurses also described end-of-life discussions as initiated too late, often during medical consultations when no more treatment options were available. One nurse described, I remember once we talked to a patient about her wishes for end-of-life. It was at the end of a medical conversation. She looked at me and said: “So this is the end?” And then we had a talk about where she wanted to spend the rest of her life. (Focus group interview, N2)
Nurses agreed that discussions about end-of-life matters with patients and family caregivers were important. Ideally, they wanted discussions to be offered continually during the course of palliative treatment, but they also recognized that families might not be ready. As one nurse said, Often, I don’t think they are ready. Perhaps we could early in the process say to the patient: It may not be that you are ready now, but we actually have the opportunity to offer you a talk about future plans. (Focus group interview, N11)
Only a single patient stated that he was not at all ready for such a discussion: “I take one day at a time. There is no reason to think about such things now” (Informal interview, P8).
Challenges in End-of-Life Discussions
Most family members wanted to talk about the end of life but found it challenging to initiate discussions. A family caregiver said, “If we start to talk about it now while she is treated with chemotherapy, I feel like it is the same as giving up. It is a dilemma” (Interview, F17). Furthermore, family members did not want to hurt each other by initiating discussions. A woman with a 19-year-old daughter living at home said, “I do not think she should go and think about it all the time, so therefore we do not talk about it” (Interview, P16). Even families that had already discussed and clarified end-of-life matters like house sales and funerals reported that the joint interview made them reflect on things they had not discussed within the family, such as what was important to them in the present moment and how they wanted to spend their remaining time together.
Another finding was that the treatment rooms could pose a challenge for nurses to initiate discussions: The chemotherapy room is approximately 40 square meters, the walls are white, and there are two very small windows and four chemo chairs—each placed in a corner. Three patients are receiving chemotherapy. The chemo chairs and the patients are all facing each other. It is quiet while two of the patients are sitting alone as their nurses just left the room. The nurse (N8) who is giving the patient (P14) chemotherapy asks him about side effects, toilet habits, vomiting, etc. There is really an awkward atmosphere. It feels like the other patients are in a conversation they do not want to be part of. The other two patients frantically try to come up with something to do while the conversation takes place. A female patient pulls up her bag and grabs her iPad while the conversation takes place. A male patient turns his head in a hurry and looks into the wall. The only sound in the room is the nurse talking. The nurse (N8) asks if the patient (P14) has further questions. The patient (P14) answers: “We have lots of questions, but not now, it’s all a bit confusing.” (Observation, P14, N8)
Observations revealed that the treatment rooms were not suitable for end-of-life discussions. Nevertheless, families did not talk much about the physical environment; a single family caregiver said, “It is really difficult to be in the same treatment room as other patients, to see their condition and hear their conversations” (Interview, F5). Nurses found the physical environment challenging for initiating conversations. One said, “I do not start a conversation that can turn out emotional, if there are many patients in the same room” (Informal interview, N4).
Families also experienced lack of continuity as a challenge to opening up. One patient said, “I do not want to talk about difficult things with a nurse I do not know” (Interview, P7). Almost all family caregivers said that continuity was “really important” for discussions about end-of-life matters but also because it helped them feel calm. The husband of a patient said, “It would mean everything if it was the same physician or nurse every time, it is an advantage. For example the palliative care team never forgets things we have talked about. You can count on them” (Interview, F17). All nurses also discussed the importance of knowing families. Nurses could initiate discussions with patients and families they didn’t know well, but it was difficult. One nurse said, “Of course I can have a difficult conversation with a patient that I don’t know, but I know I will miss something, because I don’t know the story of the family and what is important to them” (Focus group interview, N3). Nurses emphasized the importance of not missing any areas during end-of-life discussions that could be significant for families.
Nurses also found it challenging to choose between instrumental work tasks and discussions about end-of-life matters. One said, I get upset as a nurse and often think that I might really be able initiate a conversation but I simply do not dare because I want to be a proper person. I do not want to start such a terrible conversation and after half an hour the drop counter starts beeping, and then I need to end the conversation. I cannot do it. (Focus group interview, N10)
Observations also revealed that nurses had many tasks: The nurse is about to hand some chemotherapy tablets to the patient, but it seems very hectic. She has just left the treatment room where two other patients with their families receives chemotherapy. Now she talks to a colleague because she needs some help to replace the chemotherapy with NaCl while she hands out the tablets to a third patient. In a hurry, she leaves the conversation with the other nurse and almost runs down the hall and turns straight into the waiting area and calls in the patient. (Observation, P1, N1)
Nurses felt frustrated because they wanted to initiate end-of-life discussions and conduct them well without being interrupted. Families also described the nurses as “always busy” and nurses often felt pressured for time. As one said, “I often back out of the room while I talk to them to illustrate that I do not have time to talk, it is awful” (Focus group interview, N1). Another nurse talked about the outpatient clinic as solely focused on production: Another week at the little chemo factory is now over. This is written in the weekly letter. It is exactly what it is. A chemo factory. It is just production. Five treatments per hour, boom, boom, boom. They are all palliative, they will all die . . . it sucks. (Focus group interview, N2)
Many tasks and time pressure meant that nurses often did not initiate discussions and had to refer families to patient associations. One nurse said, “I get so embarrassed. We just push them away, you can go there and you can go here. We should take some of those things on us” (Focus group interview, N8). Nurses described referral to other patient associations such as the Danish Cancer Society as leading to a risk that families did not get needed help because they had to take the initiative to contact the organization.
Discussion and Critical Interpretation
End-of-life discussions addressed treatment, location of care, practical and economic concerns, and existential matters. They were rarely initiated in practice, and patients and family caregivers had different wishes for the timing of end-of-life discussions. Family caregivers found it challenging to initiate discussions with other family members. Nurses also found it challenging to initiate discussions due to the physical environment, time pressure, and lack of continuity. These findings will be discussed within a framework of Family Systems Nursing (Bell, 2009; Friedman et al., 2003; Wright & Bell, 2009) and a theory of organizational cultures (Schein, 2016).
Family caregivers are often the main support for patients with cancer and, due to an increasing focus on home-based care, bear primary responsibility for providing care for patients (Ferrell & Wittenberg, 2017). At the outpatient clinic, patients are released immediately after receiving chemotherapy into the care of family members (Andersen et al., 2019).
In a Family Systems Nursing theoretical framework, a life-threatening disease affects the entire family and family members affect each other (Bell, 2009; Friedman et al., 2003; Wright & Bell, 2009). Family members experience the stress inherent in serious illness differently; if the family as a unit cannot effectively cope with the stress, all family members become exhausted (Friedman et al., 2003). Physical and mental strain can result if the family unit does not receive needed support (Lyons et al., 2016; Rha et al., 2015; Romito et al., 2013). If the focus is solely on the patient, it is easy to neglect the rest of the family, in terms of relationships, roles, and problems that may follow (Bell, 2009; Friedman et al., 2003; Wright & Bell, 2009). The importance is clear of focusing on both patients and family caregivers and improving clinical nursing practice related to end-of-life discussions and family involvement. In Denmark, the Danish Health Authority (2017) recommends that all patients and family caregivers be offered conversations about end-of-life matters during the palliative trajectory. As noted in the background section of this article, no structured approach exists in Denmark for involving families in cancer care and end-of-life discussions (Skorstengaard et al., 2017). The findings of this study also revealed that patients and family caregivers are not systematically invited to attend end-of-life discussions. Family caregivers described a particular need to be included in end-of-life discussions earlier in the course of treatment and asked that nurses initiate and facilitate these discussions. Likewise, nurses revealed during the interviews that conversations could be time-consuming and that they needed a structure and a room for these kinds of sensitive discussions. Wright and Leahey (1999, 2013) also state that lack of time is a main reason for not involving families in family nursing conversations. However, family involvement may not always have to be time-consuming, and Wright and Leahey (1999) argue that a 15-min or less conversation may be sufficient.
Another challenge may be constraining beliefs within the families (Wright & Bell, 2009; Wright & Leahey, 2013). A systematic review of nurses’ involvement in end-of-life discussions nurses found it challenging to involve families in end-of-life discussions, because the family could have other wishes for treatment than the patient (Ikander et al., 2021). Wright and Bell introduced the Illness Beliefs Model for advanced clinical practice with families (Bell & Wright, 2015; Wright & Bell, 2009). The model focuses on various beliefs held by patients, families, and health care professionals. For example, health care professionals’ beliefs about caring for families can be constraining or facilitating (Wright & Bell, 2009). For improving family involvement in clinical practice, nurses may find it helpful to adopt the belief that “illness is a family affair” (Wright & Bell, 2009, p. ix), and thereby routinely involve the entire family in the care that is provided (Coyne et al., 2020; Dieperink et al., 2018; Wright & Bell, 2009). A way of working within a frame of Family Systems Nursing theory in clinical practice is described by Wright and Leahey, who introduced the brief 15-Minute Family Interview, as a way to embrace families in busy nursing practice (Wright & Leahey, 1999, 2013). The Illness Beliefs Model can be a useful tool to guide therapeutic conversations with families. By acknowledging and discussing different views of illness beginning with an individual perspective and moving to a relational perspective where the beliefs of all family members are explored and illness suffering is acknowledged and addressed would broaden the range of possibilities for family nursing interventions (Wright & Bell, 2009). This approach could be a way of working in future outpatient oncology clinics and palliative care (Mehta et al., 2009), and family interviews may be integrated with end-of-life discussions, as they embrace some of the same important questions (Glajchen & Goehring, 2017).
However, our findings revealed that several organizational and culturally conditioned issues posed a challenge to involving both patients and family caregivers in end-of-life discussions. Nurses did not initiate discussions with patients and family caregivers, the treatment room was unsuitable for end-of-life discussions, and nurses’ workloads and feelings of time pressure hindered practice development related to end-of-life issues. According to Schein (2016), if a practice needs improvement, it is important to analyze the organization within which it takes place. Thus, it is important to analyze organizational culture related to how nurses approach and involve family caregivers in end-of-life discussions in the outpatient clinic. Culture can be expressed through routines, habits, and values through which nurses navigate without necessarily being aware of them (Schein, 2016).
Artifacts, espoused values, and basic assumptions define a culture (Schein, 2016). Artifacts are apparent in the physical and social environment in the outpatient clinic. How do the nurses talk to and about families? How do they talk to each other? How do they approach families? How is the work with end-of-life discussion shared between the physician and the nurse? An example may be the use of language in the outpatient clinic between nurses, as described in the findings: “I often back off, to illustrate that I don’t have time . . .” and “. . . the little chemo factory.” The nurses seldom talked to the families about end-of-life matters, primarily talking to them about treatment and side effects. This finding is similar to those of recent studies in Denmark (Bergenholtz et al., 2015) and elsewhere (Broom et al., 2015; Mohammed et al., 2020; Rylander et al., 2019; Valente, 2011), in which conversations primarily had a medical focus and end-of-life discussions were initiated too late. In a newly published integrative review about nurses’ involvement in end-of-life discussions, we found that nurses’ task in end-of-life discussions was organized around specially a supportive role and an advocating role (Ikander et al., 2021). Furthermore, similar to nurses in an integrative systematic review by Bergenholtz et al. (2019), the nurses in this study also experienced that end-of-life discussions were treatment-oriented and it was unclear who should initiate the discussions (Ikander et al., 2021). However, because the patients in our study were diagnosed with an incurable lung cancer and undergoing palliative chemotherapy, we expected that nurses would have the recommended end-of-life discussions with patients and their family caregivers (Danish Health Authority, 2017). Although this was not the case, the findings also add new knowledge about end-of-life discussions in terms of both an outpatient oncology setting and content.
Espoused values are the organizational values and beliefs about how work should be done (Schein, 2016). They can be evidenced in strategies or guidelines the organization attempts to follow. In other words, espoused values are inherent in how the organization and nurses want their work to be done. Nurses wanted to initiate end-of-life discussions with the patients and families and explicitly stated the importance of doing so; they viewed it as a fundamental act of nursing. No clear division of responsibility existed between nurses and physicians for end-of-life discussions, nor was there evidence of a clear plan for development of competences in end-of-life discussions. However, nurses with the most oncology experience had learned to initiate into end-of-life discussions.
Basic assumptions are the core of the organization and difficult to change. They are manifested in routines of nurses and other organizational actors, and can be explicitly or tacitly expressed as “the way we usually do things” (Schein, 2016). Basic assumptions are communicated to new members of the organization, such as new nurses at the outpatient clinic. An example is implicit rules in the outpatient clinic; for instance, nurses described giving chemotherapy as their main task and end-of-life discussions as an option only if available time remained. Another hypothetical example could be an assumption among nurses that families are not ready to engage in end-of-life discussions because they do not ask for questions. However, patients may not want to express their needs due to the time pressure nurses experience (Chan et al., 2018). In summary, there is a discrepancy between the espoused values and basic assumptions about involving patients and family caregivers in end-of-life discussions, representing an organizational issue that requires attention (Schein, 2016).
Strengths and Limitations
Our findings provide new knowledge about end-of-life discussions in an outpatient oncology setting. We followed families up to 4 times during palliative chemotherapy and validated participant observations during interviews, which is a strength as the combination of data collection methods increases validity and credibility of findings (Noble & Heale, 2019). We included patients, family caregivers, and nurses, and were able to compare their varying perspectives on their involvement in end-of-life discussions. In this study, we only focused on the nurses’ role in end-of-life discussions; this may be a limitation because palliative care is defined as an inter-professional approach. However, we do believe it is important to highlight the nurses’ role in the interprofessional team. The approach of the analysis was phenomenological/hermeneutical, and one can argue that the themes came out to be overall themes, instead of in more in-depth knowledge of lived experiences and meanings attached. We could although have worked deeper into the data, but it would be on behalf of the amount of data and the three perspectives represented. We, although, believe the approach to data analysis was suitable, as it is an approach target to include data from participant observations and interviews (Simony et al., 2018). Limitations also include challenges inherent in recruiting a vulnerable population of patients and family caregivers. However, only three patients receiving late-line treatment chose not to participate due to their declining conditions. Similarly, the fluctuating situations of patients and families made it difficult to retain them in the study. Because the topics patients wanted to discuss varied with their position along the palliative treatment trajectory, it may have been valuable to follow patients and families over a longer period of time, perhaps until chemotherapy was discontinued. Finally, a strength is the transparent description of data collection, analysis, reporting of findings, and a discussion with existing studies, and we thereby believe the findings of the study have the potential to be transferred to other similar settings.
Conclusion and Implications for Family Nursing Practice
Our findings emphasize that end-of-life discussions between patients, family caregivers, and nurses were seldom initiated and, when they were, it was often too late. Treatment decisions, location of care, practical and economic concerns, and existential matters were primary discussion topics. At home, patients and family caregivers found it difficult to initiate and carry out end-of-life discussions on their own. In the outpatient oncology clinic, the physical environment, lack of continuity among nurses, and nurses’ instrumental task workloads posed significant challenges to initiating end-of-life discussions.
This knowledge is especially valuable for nurses and other health care professionals providing general palliative care in hospital settings. The study findings confirm previous reports, identifying a need to improve clinical nursing practice related to end-of-life discussions with patients with incurable thoracic cancer and their family caregivers in Denmark and elsewhere so that it aligns with espoused values about and recommendations for care near the end of life. For example, at a structural level, a clear need exists to set aside time for and invite patients and family caregivers to participate in structured end-of-life discussions during the palliative care trajectory, during which beliefs and values about the end of life can be explored and end-of-life care can be discussed and planned. The International Family Nursing Association’s (IFNA) Position Statement on Generalist Competencies for Family Nursing Practice (2015) and the IFNA Position Statement on Advanced Practice Competencies (2017) may be useful to guide these important conversations. End-of-life discussions can be carried out by nurses in collaboration with oncologists and should be offered several times during the course of palliative trajectory. Nurses should proactively invite patients and family caregivers to end-of-life discussions, ensuring that they take place in a timely way. End-of-life discussions must be individualized, with patients and family caregivers determining the content. Finally, although this study has mainly focused on the nurses’ role, we believe palliative care is an inter-professional approach and that future research should focus on the collaboration between all providers of end-of-life discussions at the general palliative care level.
Footnotes
Acknowledgements
We thank all the patients, family caregivers, and nurses for their valuable contributions and Jennifer Green for proofreading the manuscript.
Author Contributions
T.I., K.B.D., O.H., and M.R. contributed to study design and revising the manuscript critically and given the final approval. T.I. contributed to data collection and data analysis. T.I., K.B.D., and M.R. contributed to interpreting the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Danish Cancer Society (Grant Number R156-A9971-10226982), the Region of Southern Denmark (17/33611), Aage Theodor Larsen Fund of Cancer Research, Academy of Geriatric Cancer Research (Age Care; ![]() ), and the Department of Oncology, Odense University Hospital, Denmark.
), and the Department of Oncology, Odense University Hospital, Denmark.