
Abstract
The impact of an intensive care unit (ICU) admission on family caregivers of patients who have undergone hematopoietic stem cell transplantation (HSCT) has not been well described. Aims of this study were to determine the feasibility of conducting research with family caregivers of HSCT patients during an ICU admission and generate preliminary data about their experiences and engagement in care. Using a mixed-methods, repeated measures design, we collected data from family caregivers after 48 hr in the ICU (T1) and at 48 hr after transferring out of ICU (T2). Enrolling HSCT caregivers in research while in the ICU was feasible (10/13 consented; 9/10 completed data collection at T1); however, data collection at T2 was not possible for most caregivers. Caregiver distress levels were high, and engagement in care was moderate. The three themes that emerged from interviews (n = 5) highlighted that although HSCT family caregivers faced many challenges and received limited support during their ICU experience, they were able to access their own personal resources and demonstrated resilience.
Keywords
Background
In 2018, more than 22,000 patients received a hematopoietic stem cell transplantation (HSCT) in the United States (D’Souza & Fretham, 2019). HSCT is a potentially curative or life extending treatment for malignant and some nonmalignant diseases, but is also challenging in physical, emotional, and psychological ways for patients and their family caregivers (Bangerter et al., 2018; Kasberg et al., 2011; Tierney et al., 2014). Family caregiver involvement and well-being have been associated with less patient distress and improved survival after HSCT (Beattie et al., 2013; Song et al., 2021), and therefore, most transplant centers require a family caregiver to be available 24 hr a day, 7 days a week for the first 100 days following transplantation (Bangerter et al., 2018). However, these family caregivers are vulnerable to the adverse outcomes of chronic stress (Akgul & Ozdemir, 2014; Bevans et al., 2016; Poloméni et al., 2016). Unrelenting caregiving responsibilities coupled with treatment complications or transplant failure negatively impact family caregivers’ physical and psychological health (Beattie et al., 2013; Bevans et al., 2016). Family caregivers without support may struggle to effectively help patients manage their symptoms and provide complex day-to-day support for the patient, such as administering medications and helping the patient access weekly follow-up care with the transplant team and other specialists (Applebaum et al., 2023).
Unique Attributes of HSCT Caregiving
The prolonged trajectory of HSCT family caregiving is burdensome. Family caregiver engagement typically extends beyond the first 100 days post-transplantation and may span the duration of the patient’s life. Family caregivers struggle physically (fatigue and sleeping difficulties) and psychologically (distress, anxiety, and depressive symptoms) in their caregiving role (Bevans et al., 2011, 2016; Bevans & Sternberg, 2012; Fife et al., 2009; Mohammed et al., 2021; Waldman et al., 2021; Winterling et al., 2022). Family caregivers may even lose a sense of their own identity and meaning in their lives (Applebaum et al., 2015, 2016). In a longitudinal study of HSCT family caregivers, 70% of these caregivers needed support to process their feelings and this need was still present at 16 months post-transplantation (Kisch et al., 2021). HSCT family caregivers often feel invisible in patient-centric health care systems which increases their vulnerability (Applebaum, 2022). Insufficient family caregiver support could contribute to more emergency department (ED) visits for the HSCT patient, longer hospital days if complications are not addressed early, and even increased risk for mortality (Gertz et al., 2022; Sundaramurthi et al., 2017). The negative effects of inadequate family caregiver support also impact the family system as families are challenged to adjust and adapt along the HSCT journey.
The extreme risks and potential cascade of complications related to HSCT make this family caregiver burden unique. HSCT family caregivers must support their seriously ill family member through a long and arduous treatment process that may result in debilitating symptoms and possibly graft failure or rejection. No other cancer treatment impacts the immune system as severely as HSCT in which the cytotoxic conditioning regimen suppresses the immune system to promote engraftment (Bevans et al., 2016). HSCT patients have no immune defenses when they enter the intensive care unit (ICU) for a critical illness (Fornwalt et al., 2021). The immunologic consequences of HSCT render the patient vulnerable to life-threatening infections leading to septic shock and respiratory failure (Fornwalt et al., 2021; Saillard et al., 2016). Toxicities from the conditioning regimen for HSCT, engraftment syndrome, or cytokine release syndrome may cause acute kidney injury, respiratory failure, or neurological failure in the patient (Fornwalt et al., 2021; Saillard et al., 2016). Complications after HSCT may lead to critical illness, with ICU admissions rates for this population ranging from 9% to 57% (Saillard et al., 2016). Hospital mortality for allogeneic HSCT recipients requiring an ICU admission ranges from 50% to 80% (Saillard et al., 2016) which is higher than the overall mortality rate of 10% to 29% for ICU patients (Society of Critical Care Medicine, 2021). An ICU admission is known to be a highly distressing experience for families (Aghaie et al., 2021; de Beer & Brysiewicz, 2017; Rodriguez-Almagro et al., 2019; Wong et al., 2019). However, HSCT family caregivers may enter the ICU experience already depleted from high levels of distress experienced prior to and during the transplantation process, especially if they had been providing care for many months or even years. While patients with serious chronic diseases also require extensive family caregiving and may experience an acute health crisis warranting an ICU admission, their prognosis and disease trajectory may be more definitive than for patients undergoing HSCT (Jika et al., 2021; Walavalkar et al., 2022). Notably, HSCT, particularly allogeneic HSCT, is one of the most intense and burdensome cancer treatments (Bevans et al., 2016) with prognostic uncertainty (El-Jawahri et al., 2020).
Importance of Studying the HSCT Caregiver ICU Experience
To our knowledge, the impact of an ICU admission on HSCT family caregivers and their engagement in care has not been studied. Closing this research gap is important as this family caregiver population may have different needs than other family caregivers in the ICU. Most ICU family experience studies elicit information from family members of heterogeneous patient populations. Studying the ICU experiences of family caregivers of a homogeneous patient population sheds light on how a patient’s disease process impacts the caregiving experience and family caregivers’ ability to be engaged in care during the ICU experience. We chose to study family members of patients with hematologic malignancies as this disease process involves considerable prognostic uncertainty (El-Jawahri et al., 2020) and HSCT is a particularly burdensome treatment. Although an ICU stay is a time of uncertainty for all families, the families of patients who have undergone HSCT come to the ICU already experiencing high levels of uncertainty related to this life-altering and high-risk treatment. Critical illness can heighten this sense of uncertainty, undermining the hope and optimism inherent in the transplant process.
Psychosocial support for family caregivers during the inpatient HSCT process is limited (Wang et al., 2021), despite the acuity of medical issues and heightened possibility of patient death (Uceda-Torres et al., 2016). HSCT already represents uncertainty regarding the success of the treatment. The addition of a life-threatening complication to a burdensome and lengthy treatment is likely to have devastating effects on family caregivers and family systems. To begin to explore the impact of an ICU admission following HSCT on families, we focused this study on the family caregiver who is intimately involved in the day-to-day care of the patient. The purpose of this study was to determine the feasibility of conducting research with HSCT family caregivers during an ICU admission to (a) determine whether conducting mixed-methods repeated measures research with family caregivers at this time point is feasible (enrollment and completion of data collection), and (b) generate preliminary data about family caregiver experiences by measuring distress, family protective factors, family engagement, and family well-being, and by summarizing themes from one-on-one interviews. We hypothesized that we could recruit HSCT family caregivers in the ICU and obtain qualitative and quantitative data regarding their ICU experiences. The data obtained from this study will guide our future research with this understudied and highly burdened caregiving population.
Method
The Resiliency Model of Family Stress, Adjustment, and Adaptation guided the conceptualization of the HSCT family experience and selection of variables in this study (M. A. McCubbin & McCubbin, 1996). This seminal family systems theory, rooted in stress and coping, is a family strength-based model and posits that families bring resources (family cohesiveness, problem-solving skills, family coping) that in turn, can help the family adapt to adverse circumstances (M. A. McCubbin & McCubbin, 1993). This well-tested model has been applied in prior ICU family research (Leske & Brasel, 2010; Leske et al., 2017; McAndrew et al., 2019) and with family caregivers of patients undergoing chemotherapy (Carey et al., 1991).
An additional concept included in this study is the quality of family care (family engagement and experience of family care in the ICU), an important factor that may affect the family experience in the ICU (Mitchell et al., 2009, 2016). Figure 1 depicts the conceptual framework developed for this study and includes specific measures of key variables. Within this framework, the stresses and strains on a family caregiver related to their family members’ HSCT are compounded when there are treatment complications leading to an ICU admission. The family’s appraisal of this compounding stress is influenced by protective factors (problem-solving communication, family coping, and family resources). In addition, the quality of family care (family engagement and experience of family care in the ICU) may also impact their appraisal of these stressors. Family adjustment to the illness experience may influence their psychosocial outcomes (anxiety, depression, distress, and well-being).
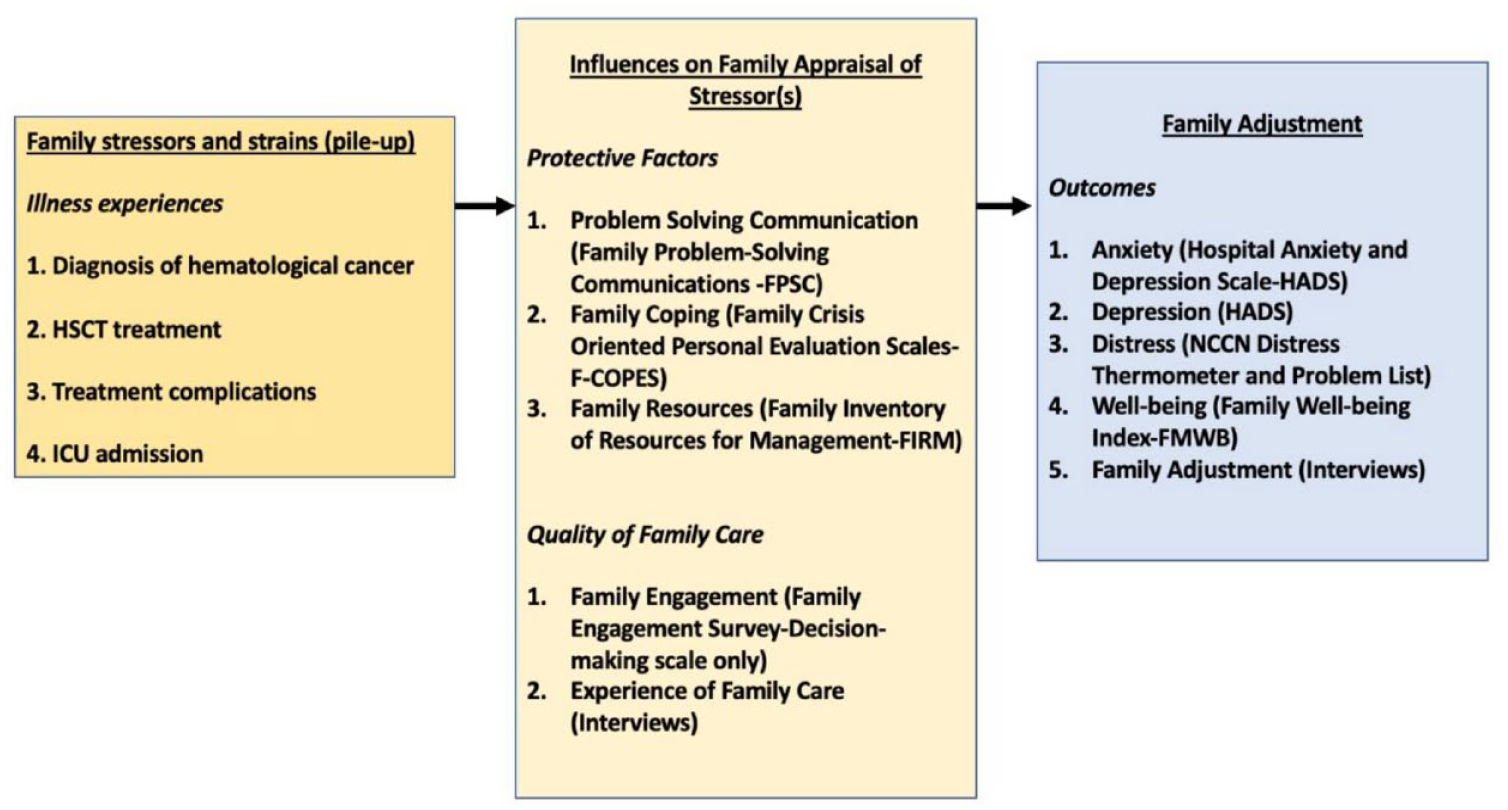
Conceptual Model of the HSCT Family Experience.
Design
We used a convergent mixed-methods design in this descriptive study (quan + QUAL) (Creswell & Clark, 2018). Qualitative and quantitative data were collected from family caregivers of HSCT patients. We collected data at two time points: 48 hr after the patient’s ICU admission (in-depth interview and assessments of family protective factors, family engagement, family well-being, distress, anxiety, and depression symptoms) and 48 hr after the patient was transferred out of the ICU.
Ethics
The Institutional Review Board of the study site granted ethics approval to conduct this study (PRO00032242). All family caregivers engaged in an informed consent process prior to completing study activities. The study team was granted a waiver of the Health Insurance Portability and Accountability Act (HIPAA) of 1996 authorization requirements (45 CFR 164) and a waiver of the informed consent requirements (45 CFR 46.116) for patient medical record review. Family caregivers were made aware that they could stop their participation at any time and that their participation in the study would not impact the care of their critically ill family member in any way. Participants were provided the number for a crisis hotline should they require further support after participation. Informed consent and data collection were completed by the study PI who is an experienced ICU nurse researcher and clinician.
Setting
The study was conducted at a large academic medical center situated within an urban community in the Midwest United States. This hospital has a robust Blood and Marrow Transplant Program that performs autologous and allogeneic transplants (300 transplants in 2021) and is accredited by the Foundation for Accreditation of Cellular Therapy (FACT). Inpatient HSCT patients are cared for on a 32-bed unit and if they require critical care they are transferred to the Medical Intensive Care Unit (MICU), a closed 26-bed ICU.
Sample
We used a convenience sampling strategy in this study. We define family caregiver as a family member or friend identified by the patient who (a) has a significant relationship with the patient, and (b) provides unpaid assistance to them (AARP & National Alliance for Caregiving, 2020; Applebaum, 2022; Family Caregiver Alliance, 2006; Wright & Leahey, 2012). The family caregiver may live with or separately from the patient (Family Caregiver Alliance, 2006). In the context of HSCT, during the first 100 days following transplantation the family caregiver must live with the patient to provide ongoing care and support in the day-to-day care of this patient. We included family caregivers of patients who had undergone HSCT (allogeneic or autologous) and subsequently admitted to the ICU who were as follows: (a) 18 years or older; (b) identified themselves as a family member (bound by social, biological, or legal relationships including nonmarried and same-sex partners) who provides social or emotional support to the patient and/or the person who has signed a caregiving agreement (unique document for HSCT population completed before HSCT) for HSCT treatment; and (c) could read, write, and understand the English language. Family caregivers were excluded from participation if (a) the patient was moribund and life-sustaining treatments were discontinued due to imminent death, and (b) English was not the preferred language for communication (translators and translation of study tools were beyond study resources).
Instruments and Data Collection
Our selection of instruments was based on our conceptual model and prior research with this population of family caregivers, as well as ICU family research. See Table 1 for a list of instruments and their description. The following domains were assessed: family protective factors (problem-solving, resources, and coping), distress, clinically significant anxiety and depression symptoms, family engagement in decision-making, and family well-being (mental, social, and physical aspects of family health). All instruments were reliable and valid with the exception of the researcher-developed acceptability measure, family caregiver characteristics data collection form, and the Family Engagement in Decision-Making Scale, for which published psychometric data are pending (Heyland, 2018). All instruments are self-report, and total scores were used in analysis. Problem-solving was measured with the Family Problem-Solving Communications (FPSC) instrument (M. A. McCubbin et al., 1988/1996). Family coping was measured with the Family Crisis-Oriented Personal Scale (F-COPES; H. I. McCubbin, Olson, & Larson, 1981/1996), and family resources were measured with the Family Inventory of Resources for Management (FIRM)—Family Strengths II scale (H. I. McCubbin, Comeau, & Harkins, 1981/1996). Family engagement was measured with the Family Engagement Survey decision-making scale (Heyland, 2018). Anxiety and depression were measured with the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983). Distress was assessed with the National Comprehensive Cancer Network (NCCN) Distress Thermometer (DT; and this instrument has been tested with caregivers and correlated with other measures of distress (Bevans et al., 2011). Family well-being was measured with the Family Well-being Index (FMWB; H. I. McCubbin & Patterson, 1983/1996). The family protective factors and family well-being instruments have been used in prior ICU family research with reliability of these instruments ranging from .70 to .84 (Leske, 2000; Leske & Brasel, 2010; Leske et al., 2017; Leske & Jiricka, 1998; McAndrew et al., 2019). The HADS instrument has also been used in ICU studies and studies with cancer caregivers, with reliability ranging from .77 to .85 (Applebaum et al., 2018; Mykletun et al., 2001; Zigmond & Snaith, 1983).
Theoretical Concepts, Variables, Instruments, and Description.
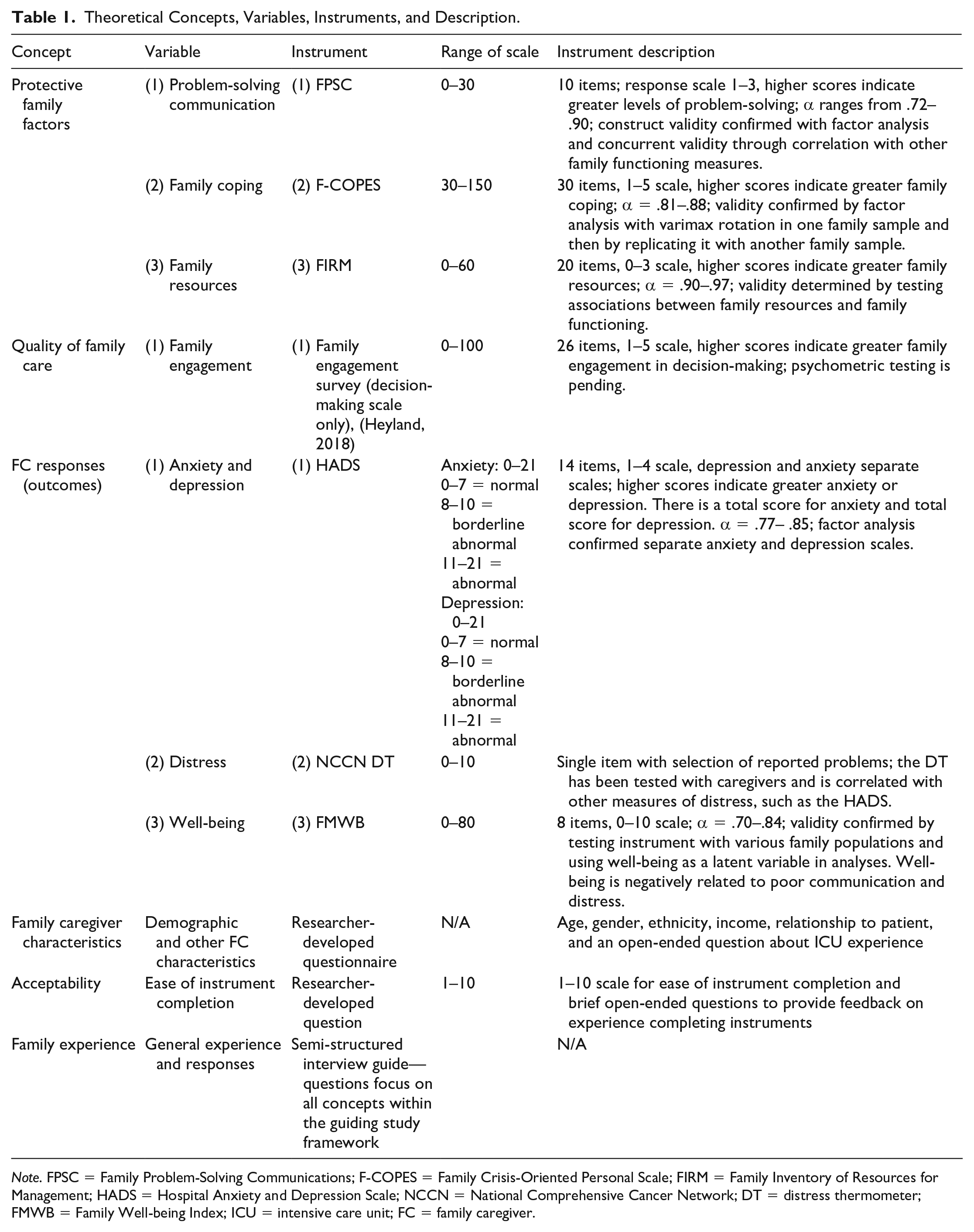
Note. FPSC = Family Problem-Solving Communications; F-COPES = Family Crisis-Oriented Personal Scale; FIRM = Family Inventory of Resources for Management; HADS = Hospital Anxiety and Depression Scale; NCCN = National Comprehensive Cancer Network; DT = distress thermometer; FMWB = Family Well-being Index; ICU = intensive care unit; FC = family caregiver.
We collected family caregiver characteristics including age, race, income, and length of time caregiving. We measured acceptability of completing this battery of instruments with a researcher-developed survey that asked family caregivers to rate ease of completion on a scale of 1 (difficult to complete) to 10 (easy to complete). Family caregivers provided open-ended comments regarding completion of study instruments as well.
Family caregivers were interviewed about their ICU experience using an interview guide. The opening question was “Can you describe your experiences in the ICU?” with follow-up probes focused on the study variables of the family protective factors, stressors and strains on the family system, quality of family care in the ICU and the family caregiver’s perception of their family’s adjustment and adaptation. We determined the length of time to complete instruments before launching our study with a subgroup of volunteers (family and friends of the research team) who reported a range of 20 to 30 min to complete the instruments. We found that most family caregivers in our study completed the instruments in 30 to 40 min. Quantity of instruments and number of items is similar to prior ICU studies with family members as participants (Hetland, McAndrew, Kupzyk, Krutsinger, Pozehl, et al., 2022; Hetland, McAndrew, Kupzyk, Krutsinger, Turnbull, et al., 2022; Leske, 2000, 2003; Leske et al., 2017).
We collected the following HSCT patient data from the electronic medical record (EMR): (a) demographic: age, gender, and ethnicity; (b) clinical: date of hospital admission; hospital unit admitted to and length of stay; ICU admitted to or transferred to and length of stay; diagnosis; type of HSCT; code status; a calculated Sequential Organ Failure Assessment Score (SOFA) using ClinCalc (https://clincalc.com/IcuMortality/SOFA.aspx), an instrument to determine risk of mortality (scores greater than 12 associated with a 95.2% risk of mortality), within first 24 hr of ICU admission (ClinCalc LLC, 2022; Ferreira, 2001; Vincent et al., 1998); number and type of life-sustaining treatments; presence of an advance directive; and final patient disposition at the end of their hospitalization (discharge from the hospital or death during the hospitalization). We entered all data into Research Electronic Data Capture (REDCap) and exported it into SAS 9.4 for analysis.
Feasibility
We documented all screened patients, enrolled family caregivers, and family caregivers who declined participation, including their reason for declining if offered. The feasibility benchmark for study enrollment was a 50% consent rate. The 50% consent rate was based on our prior work with families in the ICU with enrollment rates of 71% or higher (Leske et al., 2017; McAndrew et al., 2019) and studies conducted with the HSCT family caregiver populations with consent rates of 60% or higher (Bangerter et al., 2018; Bevans et al., 2014; Kim et al., 2019). Given the stress of the ICU admission on this family caregiver population and the high risk for patient mortality, we used a more conservative benchmark of a 50% consent rate.
There is a paucity of data about HSCT patients in the ICU; therefore, to fully inform our recruitment benchmark and ensure we would have enough family caregivers to complete the study, we analyzed deidentified data from July 10, 2017 to July 9, 2018, using Slicer Dicer. This data exploration program enabled us to estimate the number of HSCT patients admitted or transferred to the ICU who may have a caregiver. Although there were 244 patients who underwent HSCT only, 35 patients were admitted directly to the ICU or transferred from an oncology floor to the ICU. In our study, the patient had to be in the ICU 48 hr or longer to qualify and some of the patients in our historical sample were in the ICU for less than 24 hr; therefore, 35 was a high estimate of available HSCT family caregivers. Given the high mortality rate for patients requiring an ICU admission post-HSCT, we estimated approximately two to three eligible family caregivers each month. Our goal was to obtain a sample size of 10 family caregivers within 1 year. We documented the number of family caregivers who completed the instruments at each time point and measured their perception of feasibility and acceptability of the instruments on a 1 to 10 scale and with open-ended questions. The feasibility benchmark for completion was a 75% completion rate at T1 and a 50% completion rate at T2. The acceptability benchmark was a mean of 7 or higher out of 10 for ease of instrument completion.
Procedures
Screening, Recruitment, and Data Collection
We screened for HSCT patient admissions to the MICU using EMRs and collected data from September 3, 2019 to March 24, 2021. Due to the COVID-19 pandemic, the study was halted from March 19, 2020 through June 5, 2020. When we resumed the study in June 2020, we completed all study processes remotely due to visitor restrictions in the hospital. Data were initially collected at two time points: T1 (5–7 days of admission to the ICU) and T2 (48 hr after transferring out of the ICU). Our review of the screening data within the first 5 months of the study revealed 18 patients who were in the ICU for fewer than 72 hr. We wanted to ensure as many HSCT caregivers as possible could share their perspectives about the ICU experience. Therefore, early in the study, we moved T1 data collection from 5 days to 48 hr after ICU admission to increase the number of eligible family caregivers. It has been our experience in our prior ICU research studies (McAndrew et al., 2020) and in other studies (Bailey et al., 2010) that 24 hr is an adequate amount of time for family caregivers to provide meaningful feedback about their ICU experience. Another change we made to procedures early in the study was moving the interview from T2 to T1 after we observed that four patients died before their family caregivers could complete the T2 interview. This was a necessary change because qualitative data were prioritized in this mixed methods study.
After determining that a family caregiver was eligible, the PI spoke with bedside health care professionals (nurse and provider) to ensure that it was an appropriate time to approach the family caregiver about participation in the study. Family caregivers who were interested engaged in an informed consent process. The PI consented HSCT family caregivers, collected all data from participants, and conducted one-on-one interviews. The PI is a nurse scientist, an advanced practice nurse, and has prior professional experience in ICU nursing and family nursing. At the time of the study, the PI was not working in clinical practice, ensuring that HSCT family caregivers had no relationship with the PI prior to engaging in research activities. When data collection was in person, family caregivers completed the study instruments independently. Following COVID-19 restrictions, research instruments were completed with the researcher via phone. For both in-person and virtual data collection, the one-on-one interview followed the completion of study instruments. In appreciation of their contributions to the research study, all family caregivers who consented to participate received a US$50 Amazon gift card following the first point of data collection.
Analysis
Frequencies and percentages were used to summarize recruitment, retention, patient, and family caregiver characteristics. Descriptive statistics (mean, standard deviation, and range) were used to summarize numerical data for the age of the family caregiver and their years of caregiving. Given the small sample size, median and interquartile range, as well as overall range, were used to summarize family caregiver responses to study instruments. Feasibility of enrollment was determined from the percentage of approached family caregivers consenting to participate in the study. Feasibility of data collection was determined by the number of participants completing one or more instruments at each point of data collection. Acceptability was determined from the overall mean for the question about the ease of instrument completion and from participants’ written comments about what it was like to complete study instruments (content analysis).
Interviews were transcribed verbatim. Field notes were reviewed by the PI. An inductive approach to content analysis was used to determine themes in the interview data (Erlingsson & Brysiewicz, 2017; Hsieh & Shannon, 2005). The PI listened to the interviews with transcripts in hand to get a sense of the data and then created codes during line-by-line analysis of each interview. These codes were then collapsed into themes and subthemes. Themes and subthemes were explored to provide insight into the family characteristics and outcome variables.
To achieve trustworthiness, the following strategies were employed to ensure credibility, dependability, and transferability (Lincoln & Guba, 1985). To address credibility, we interviewed family caregivers of different backgrounds and genders and caregiving experiences. During the course of the interviews, the PI kept a reflexive journal about her interview processes, her experiences, and interpretations (Lincoln & Guba, 1985). The PI engaged in regular peer debriefings with research team members trained in qualitative research, and as a team, they discussed the ongoing analytic process and emerging findings (Graneheim & Lundman, 2004). The data were analyzed to determine whether there was a “negative case” in which one family caregiver’s experience was drastically different from those of the others (Lincoln & Guba, 1985). To meet the requirements of dependability, we provided an audit trail of all analytic processes and decisions. To address transferability, we provided a description of the research setting, we detailed the selection process and characteristics of the HSCT family caregivers who participated in the study, and we provided a rich description of our findings with participant quotes. To ensure confirmability, the results were audited by a member of the research team with qualitative research expertise.
Results
We screened 85 patients for the study, and 13 of their family caregivers were eligible and approached for participation (see Figure 2). The main reasons for ineligibility were that the patient did not meet the required ICU length of stay or the patient had not yet undergone HSCT.
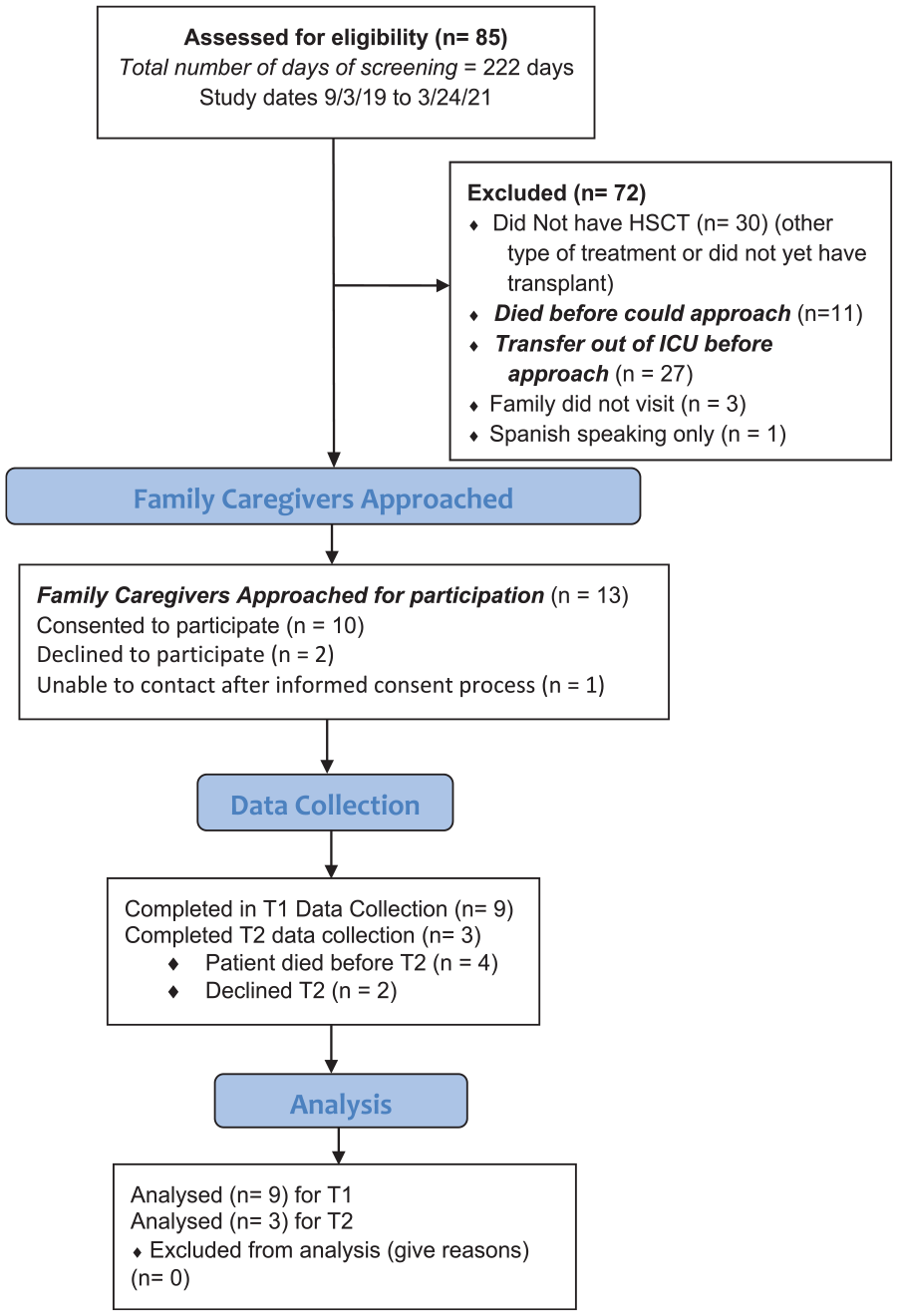
Flow Diagram for Study Enrollment.
Patient Characteristics
Patient characteristics (n = 9) are listed in Table 2. Eight of the nine patients received an allogeneic HSCT. The average SOFA suggests a 15% to 20% risk of death upon ICU admission (ClinCalc LLC, 2022). Five patients received two or more life-sustaining treatments, including mechanical ventilation, continuous renal replacement therapy, vasopressors, inotropes, and intra-aortic balloon pump. Four patients received only mechanical ventilation. Six patients died in the ICU or during their hospital stay.
Patient Characteristics.
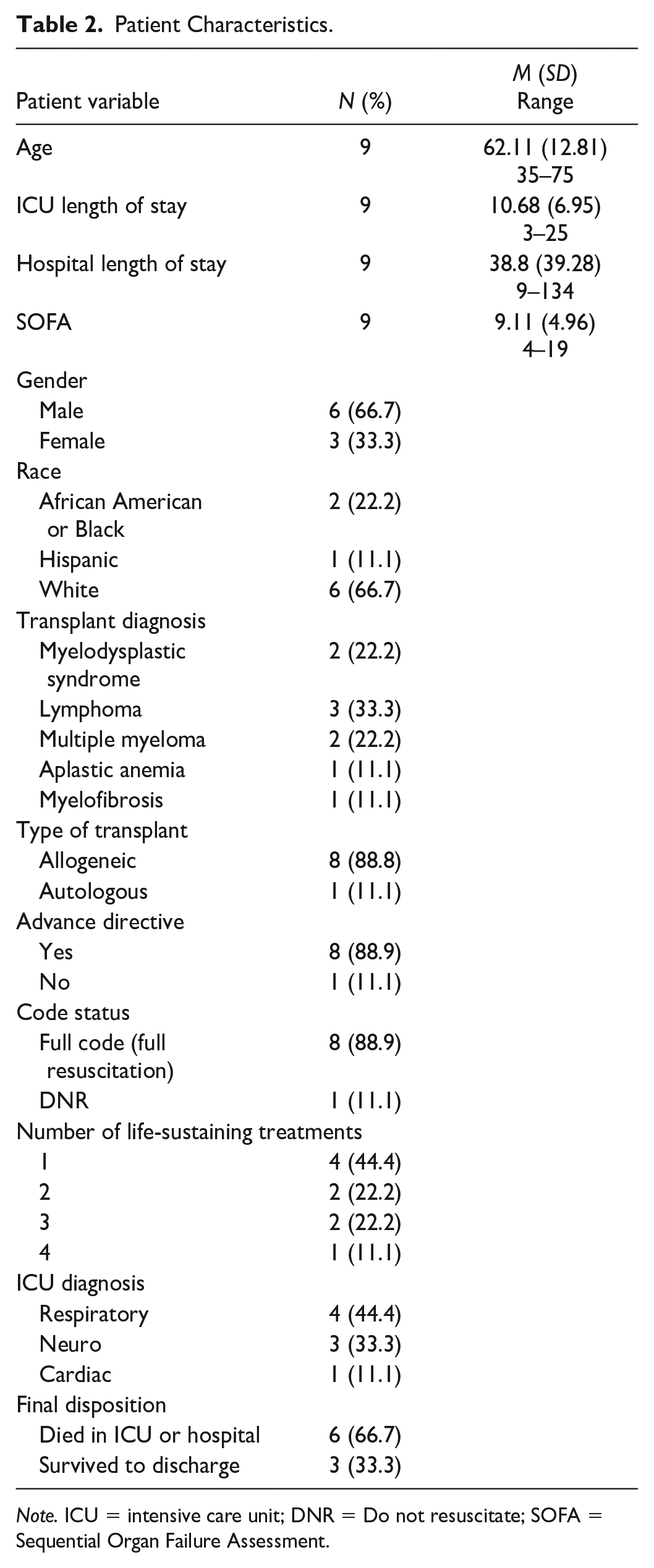
Note. ICU = intensive care unit; DNR = Do not resuscitate; SOFA = Sequential Organ Failure Assessment.
Family Caregiver Characteristics
Family caregiver characteristics (n = 9) are listed in Table 3. The majority of family caregivers were female and had some college or a college degree. Most family caregivers were spouses/partners and had not experienced a previous ICU stay with the patient. Five family caregivers participated in individual interviews. Interview participants included two Black/African American women, two White women, and one White man. All were providing care to patients who had received an allogeneic transplant that occurred between 1 month and 2 years prior to the ICU admission. Of these five caregivers, two were employed and three were retired. ICU length of stay ranged from 3 to 25 days (Mdn = 9), and hospital length of stay ranged from 23 to 135 days (Mdn = 23).
Family Caregiver Characteristics.

Note. ICU = intensive care unit.
One caregiver did not report age.
Feasibility of Enrollment
Of the 13 caregivers who were approached to participate, 10 enrolled in the study for a 77% enrollment rate, exceeding our benchmark of 50% and consistent with consent rates in other ICU studies (Leske et al., 2017; McAndrew et al., 2019). We were unable to recruit the 10 caregivers within the 1-year timeframe due to challenges posed by the COVID-19 pandemic. Reasons for nonparticipation included feeling too overwhelmed or lack of interest in research. Although 10 caregivers consented, one was not reachable at T1 for data collection.
Feasibility and Acceptability of Quantitative and Qualitative Data Collection
Initially, T1 data collection occurred 5 to 7 days after ICU admission. Six of 10 family caregivers completed data collection in this timeframe with no missing data, and two completed T2 data collection, which included the interview. After shifting the interview to T1, three additional family caregivers completed the interview and two completed T1 data collection without missing data. One of these three family caregivers completed T2 data collection (T2 completion of 33%). For four family caregivers, T2 data collection was not possible because of patient death; two other family caregivers were too overwhelmed by the patient’s situation to complete T2 data collection.
Family caregivers (n = 8) generally found the study instruments easy to complete (M = 7.25, SD = 2.60) with a range of responses from 3 (more difficult to complete) to 10 (very easy to complete). One family caregiver shared, “This was easy to comprehend and very applicable, and I appreciated the questions.” In contrast, one family caregiver shared “Good questions, but too long.” Regarding the Family Engagement Decision-Making Instrument, one caregiver noted that the contemplation questions did not make sense to them and another wrote that the item on this tool about making a decision on quality versus quantity of life included too many choices.
Family Caregiver Outcomes
Family caregivers had middle range scores for family coping, family resources, engagement in patient care, and well-being (Table 4). Their problem-solving scores were at the higher end of the range for the problem-solving instrument. Based on cutoffs defined by the HADS, family caregiver anxiety and depression symptom levels were clinically significant, with distress level scores were well above 4 (Zwahlen et al., 2008). Distress for these family caregivers was identified as being associated with both physical and psychosocial problems. The most common concerns reported included worry, sadness, work or school challenges, fears, eating difficulty, sleep difficulty, fatigue, depression, problems with treatment decisions, and family health worries.
Mean Caregiver Scores on Study Instruments.
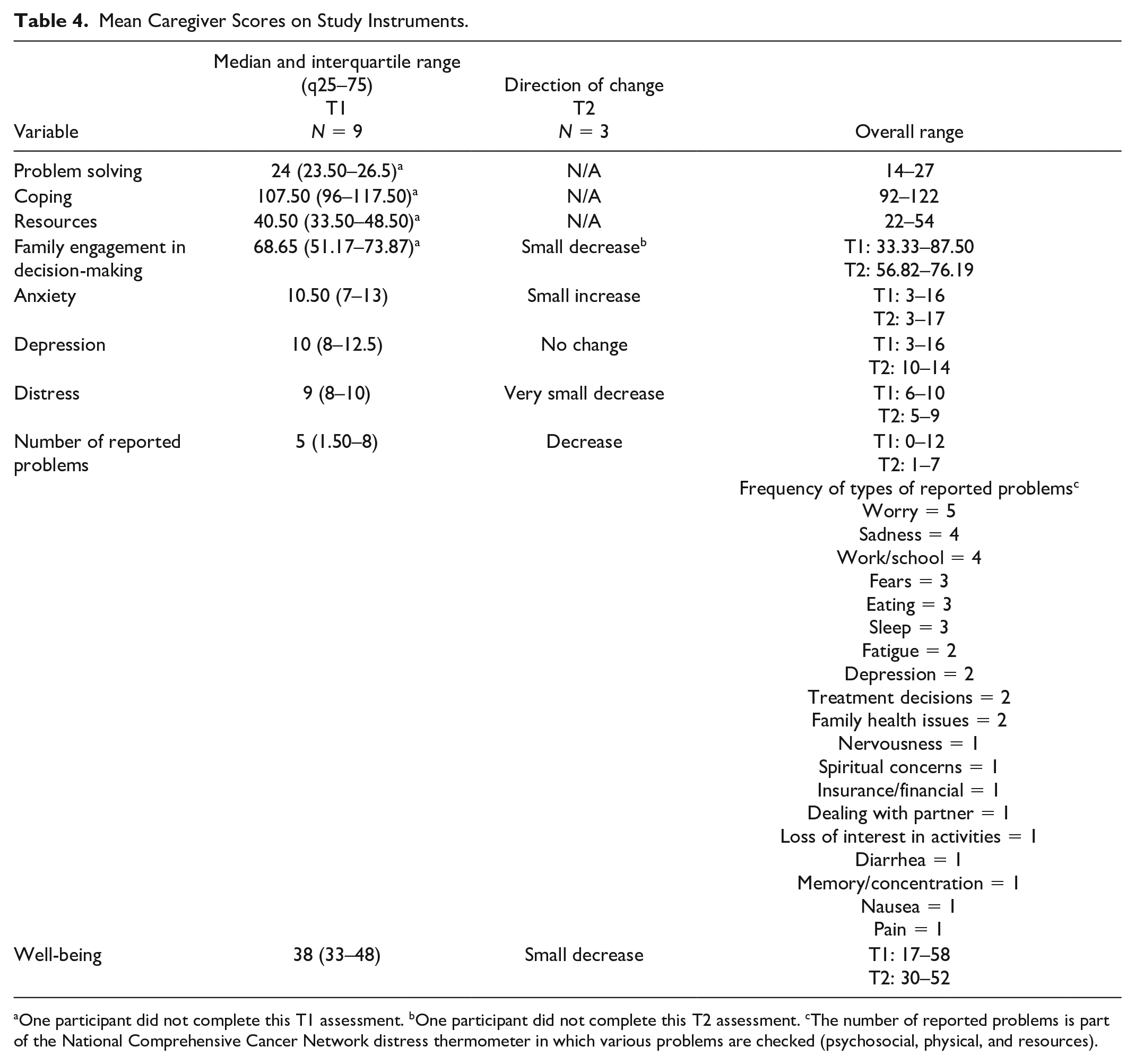
One participant did not complete this T1 assessment. bOne participant did not complete this T2 assessment. cThe number of reported problems is part of the National Comprehensive Cancer Network distress thermometer in which various problems are checked (psychosocial, physical, and resources).
Individual Family Caregiver Interviews
Two of the interviews were conducted in a conference room in the hospital, and three were conducted via phone. Three themes and 13 subthemes emerged from these interviews (Table 5) and are described in the following section, with subthemes in italics.
Summary of Qualitative Themes and Subthemes.
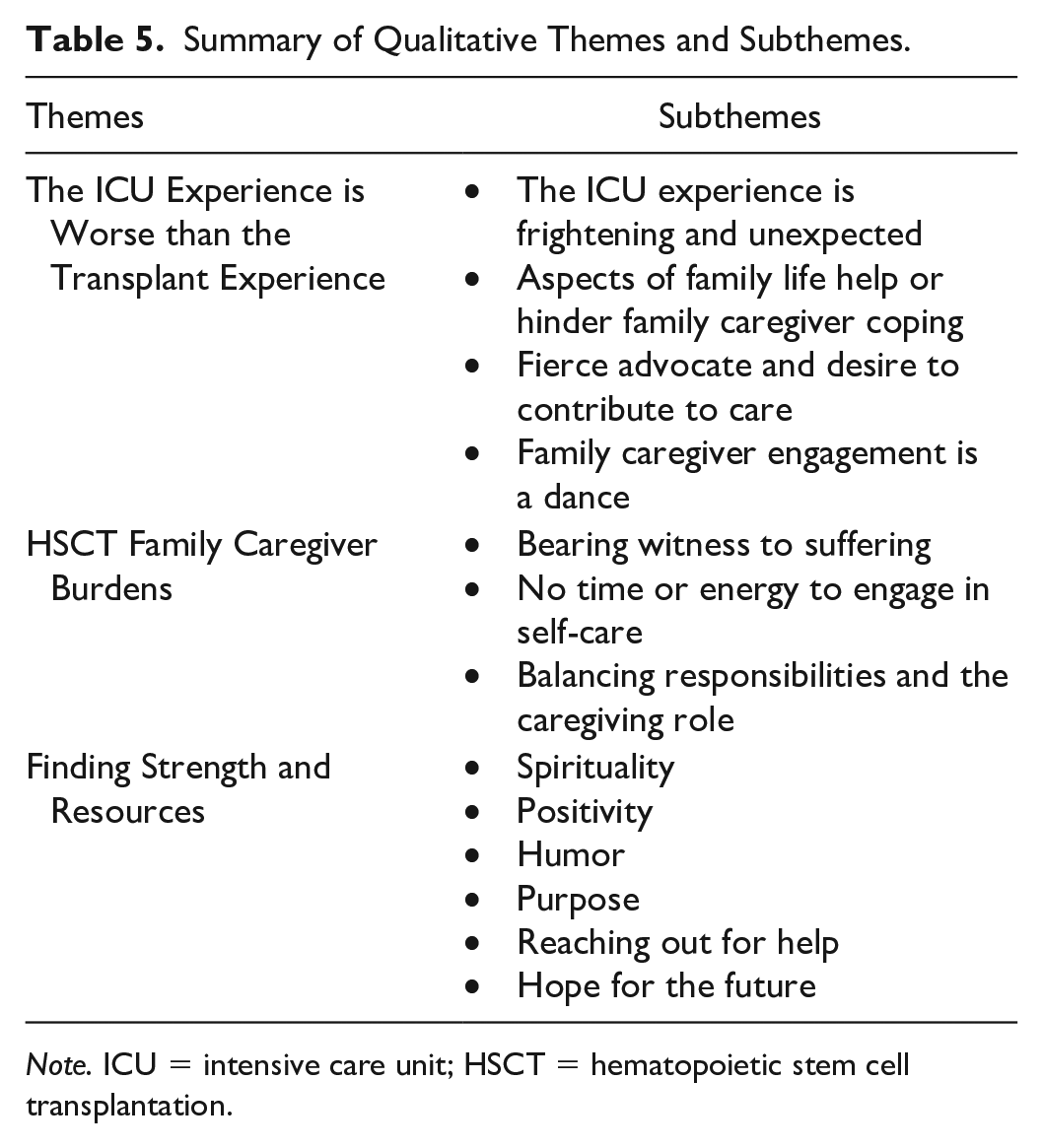
Note. ICU = intensive care unit; HSCT = hematopoietic stem cell transplantation.
Theme 1: The ICU Experience Is Worse Than the Transplant Experience
Caregivers compared their ICU experience to their transplant experience.
As scary as (the transplant) was in some ways, it was a sense of unending optimism. This (ICU experience) is really the most stressful time in my life . . . because this is something I don’t understand. I haven’t done reading in advance on it. (Participant 7)
During the transplant experience, family caregivers are given materials and instruction and have ongoing interaction with their hematologist. As one family caregiver put it, the HSCT team was “Filling me in, like keeping me in the loop about everything” (Participant 8). However, in the ICU, family caregivers felt disconnected from the familiar transplant world and did not feel the same level of engagement with the ICU team as they did with the transplant team.The ICU Experience is Frightening and Unexpected. Family caregivers reflected that the ICU experience is frightening and unexpected. One participant remarked, “Very upsetting and very scary. You know he’s already in there for transplant and now you’re rolling him into ICU” (Participant 9). Family caregivers expressed that their family member’s sudden admission to the ICU was extremely troubling because it was not part of their vision for the transplant experience. A family caregiver explained their frustration with the fact that “things are not going the way I would’ve expected . . .” (Participant 7). Family caregivers discussed their bewilderment in seeing their family member hooked up to lines, tubes, and monitors. A family caregiver shared, “It was just kind of hard for the family to adjust to seeing him that way” (Participant 1). Interviewees described their distress with living with uncertainty in the ICU where there were “no answers and no timeline” (Participant 2) for their loved one’s recovery and felt like they were “jumping around from one fire to the next . . .” (Participant 7).
Aspects of Family Life Help or Hinder Family Caregiver Coping
Prior family illness experiences impacted the family caregiver’s coping in the ICU. A family caregiver (Participant 1) explained that the transplant experience prompted discussion with her husband about his wishes for care, and in turn, this allowed them to provide guidance to the family regarding ICU decision-making. Another reflected on a time when her husband became her caregiver (Participant 7) which inspired her to reciprocate. A family caregiver explained that multiple family caregiving roles made her experience supporting her husband in the ICU more challenging.
A family’s developmental phase of life influenced the level of support that family system was able to offer the HSCT patient and the family caregiver. Family caregivers who had adult children with young families remarked how hard it was for them to balance parenting, working, and supporting the family through the illness experience. A family caregiver explained, “(It) is hard on young families . . . they obviously can’t be available because the three of them and their spouses are working” (Participant 7). Family cohesion and family dynamics generally had a positive impact on the ICU and illness experience. “We do talk things over a lot and the kids talk to each other, you know, so they become a united front” (Participant 7). The family also acknowledged benefits from the ICU experience: “I think we became closer as a family” (Participant 1). Family spiritual traditions and beliefs helped the entire family through a time of ongoing uncertainty and promoted their resilience as a family. “Part of this process for everybody has just been connecting, praying together . . . making sure that everybody is just staying positive” (Participant 8). A family caregiver explained how her family worked hard to care for each other. “Our daughter . . . she’s always there for emotional support” (Participant 7).
Other family changes and stressors contributed to family strain. One family caregiver described moving, as well as changing jobs, during the course of the patient’s treatment and hospitalizations. Family caregivers interviewed during the COVID-19 pandemic described its negative impact on their ability to be present at the bedside with their family member. A caregiver expressed, “It is hard to . . . not be there” (Participant 7). A caregiver anguished over the fact that the pandemic “separated us in a way that we’ve never been separated before” (Participant 7). Family caregivers also explained the importance of promoting family communication through Caring Bridge, text groups, emails, and phone calls to help others in the family understand what was happening at the hospital.
Fierce Advocate and Desire to Contribute to Care
Family caregivers considered patient advocacy their primary role. However, at times, advocacy was challenging in the acute care environment. Family caregivers expressed the difficulty of knowing when and how to advocate for the patient and what questions to ask in the ICU. A family caregiver expressed her strong desire to advocate for her husband, but “The truth is I don’t even know who to advocate to” (Participant 7). Another family caregiver (Participant 2) acknowledged the challenge of advocating for comfort in the plan of care when in “cancer culture” the emphasis is on continued treatment and intervention. Family caregivers wanted to be present as much as possible with the patient and make every moment count. “I go and sit with my husband, even though he’s not alert” (Participant 9). Family caregivers were determined to be involved in some way in the care of their family member. “You just want to figure out what you can do to help” (Participant 8). Some family caregivers were able to provide basic care to the patient, such as shaving and washing. As one family caregiver pointed out, “I do think that it’s important for families to be involved in the care because a person’s illness is a family affair” (Participant 7).
Family Caregiver Engagement Is a Dance
The health care team and the HSCT family caregiver had to learn the “dance” of interpersonal communication to bridge a chasm of medical information in a time of crisis. As one family caregiver stated, “the availability (of the ICU team) and the communication really matters” (Participant 7). Family caregivers felt supported when health care professionals acknowledged the family caregiver and provided clear and understandable explanations. For example, “She (advanced practice provider) came in and was very ‘into’ our family . . . and how we were (doing)” (Participant 1). Family caregivers appreciated ICU health professionals who were friendly and made an effort to connect. It was helpful for family caregivers to be in an ICU at the hospital where the transplant took place because the transplant provider would be consulted on the HSCT patient’s care. Family caregivers felt a deep connection with transplant providers and their presence in the ICU offered caregivers some comfort while they were in an unfamiliar place.
Certain ICU and health care delivery factors impaired caregivers’ ability to navigate the ICU experience for their loved one. Family caregivers expressed frustration with the rules of the ICU and feared not following rules could limit their access to their family member. “It started as a challenge when you always had to pick up that phone to get in” (Participant 1). Many participants observed there were multiple leaders in the ICU compared with one leader in transplant. A family caregiver shared, “I don’t have a sense (in the ICU) that there is a single voice anywhere” (Participant 7). Lack of collaboration among specialties and conflicting information was distressing for caregivers, especially “when the experts don’t agree” (Participant 2). The complexity of care for HSCT patients required the involvement of multiple specialists who did not understand their family member’s full story. A family caregiver shared, “. . . There was the radiology oncology people, the transplant team, the infectious disease team . . . not everybody knew everything that had gone on” (Participant 8). Family caregivers shared their distress regarding inadequate communication. “The doctors didn’t seem to know what was the cause. There were differing opinions. Communication with the family about that was frustrating, because I didn’t feel like it was handled real well, real collaboratively” (Participant 2). Another felt “a little discombobulated” when left out of communication with the ICU team (Participant 7).
Family caregivers felt they were left on their own to make sense of a complex trajectory of ICU care and had to find resources to cope. They noted that, other than overcrowded waiting rooms, they did not have a comfortable place to go when they were asked to step out of the ICU for procedures and other patient care. Family caregivers described working hard to understand the plan of care and looking up certain drugs, procedures, and tests on their own phones or tablets. A family caregiver (Participant 2) suggested that an introduction to the ICU would be helpful.
Theme 2: HSCT Family Caregiver Burdens
Family caregivers faced many challenges prior to and during the course of their family member’s hospitalization. A major source of family caregiver distress was bearing witness to suffering.
Bearing Witness to Suffering
A family caregiver explained, “To be so, so hurt in watching him in pain” was difficult (Participant 9). Another family caregiver questioned the appropriateness of painful treatments given the ambiguity of whether or not his wife would survive, “We want the tubes removed, but it doesn’t make good medical sense to do that . . . Those are just things that families have to bear” (Participant 2). HSCT family caregivers described emotional struggles balancing the emotional needs of their family member with their own. When a family caregiver contemplated why the transplant did not yield more than 1 year of remission for his wife he shared a feeling of regret, “She went through a lot . . . And we had 1 year and we are grateful for that year . . . but maybe we would’ve done more (together) if we would’ve only known it was going to be a year?” (Interview 2). Now in the ICU with a guarded prognosis, this family caregiver questioned every prior and current decision.
No Time or Energy to Engage in Self-Care
As one family caregiver explained, “When I’m stressed my self-care goes to the very bottom of the list” (Participant 8). Family caregivers described exhaustion and not being able to do the activities that had brought them joy in the past, “I’ve kind of gotten away from some of my favorite things to do” (Participant 1).
Balancing Responsibilities and the Caregiving Role
Caregivers described their struggles balancing responsibilities and the caregiving role. “It’s like the two things in my life are work and cancer . . . All of a sudden I gotta get on top of this stuff (at work), and I couldn’t concentrate” (Participant 2). Another caregiver shared that she struggled and felt unprepared to assume her new caregiving role when her husband returned home post-transplant. “He was so weak that we were concerned about even just him getting up” (Participant 8).
Theme 3: Finding Strength and Resources
Family caregivers in this study found strength in many different aspects of their life.Spirituality. An important source of strength for most caregivers was spirituality, with participants describing putting faith in God and practicing prayer. One caregiver shared, “I ask God every day to continue to strengthen me so I can help him (the patient) in whatever capacity I need and have to” (Participant 9). Family caregivers spoke of support from members of their religious and work communities. “I’ve been fortunate . . . (my boss) just said ‘You take whatever time you need’” (Participant 2).
Positivity
Positivity was a coping strategy used by family caregivers during the transplant process and ICU experience. One family caregiver example was “Making sure that everybody is staying positive and not taking everything that doctors say at face value” (Participant 8). For another caregiver, positivity was critical to her own mental health: “It just helps (me) overcome being thrown into depression” (Participant 9).
Humor
Humor was another way that caregivers and their families coped with the difficulty of serious illness. “We use a lot of teasing and joking with each other” (Participant 2).
Purpose
Finding purpose helped caregivers draw strength from their caregiving experience. A family caregiver discussed wanting to give back to other families who were going through the transplant experience such as, “Doing something, volunteering, dealing with new patients and families (undergoing HSCT)” (Participant 7). Another explained that service helps you, “Take the focus off yourself . . . so if you’re feeling sorry for yourself . . . try to help someone else” (Participant 2).
Reaching Out for Help
Family caregivers recognized the value of reaching out for help and did so through mental health support from their Employee Assistance Program or primary care physician, as well as through their family, friends, and communities. Family and friends sustained these caregivers during difficult times. One described supportive interactions with her family: “We just talk to each other all the time. The kids are always checking in with me” (Participant 7). Another caregiver explained, “So having that extra layer of comfort and support . . . Everyone is kind of wrapping me up in love” (Participant 8). One caregiver explained how she delegated to family members the task of communicating health updates to others because she did not have the capacity.
Hope for the future
Almost every family caregiver discussed hope for the future. A caregiver explained, “It’s really going to be a new life once he recovers fully from the transplant” (Participant 8). Another caregiver shared that without transplantation, her husband would not have been able to meet his grandchildren. For these family caregivers, transplant is a chance to continue living life and the ICU experience is a bump in the road. However, for one family caregiver, the ICU experience was a reminder that time with his wife may be shorter than he hoped.
Discussion
Although it may be difficult for family caregivers to participate in research while the patient is in the ICU, our current study demonstrates that HSCT family caregivers are willing to participate in research. In our study, 77% of the approached caregivers agreed to participate in the research and completed survey-based data and individual interviews. However, repeating data collection was not feasible based on our benchmark (33% completion of T2 data).
Family Caregiver Symptoms: Distress, Anxiety, and Depression
While others have explored the distress of family caregivers longitudinally, to our knowledge we are the first to specifically measure HSCT family caregiver distress in the ICU context. Family caregivers in our ICU study reported higher levels of distress, anxiety, and depression than what has been reported at pretransplant levels, a time of great distress for HSCT family caregivers (Bevans et al., 2011; Posluszny et al., 2019; Waldman et al., 2021). This finding is likely attributed to the crisis-related stress that an ICU admission adds to the constant uncertainty that is the nature of the HSCT and recovery process.
In comparison with other family caregiver populations in the ICU, family caregivers in our study had anxiety and depression levels that were similar to the levels of family members of ICU patients who were at high risk of dying (McAdam et al., 2012). Notably, many of the enrolled patients in our study were not at high risk of dying according to their SOFA score calculated at 24 hr postadmission. Another distinctive difference of HSCT family caregivers in the ICU was that their well-being scores in our study were lower than those of a sample of family members of patients who suffered a motor vehicle accident or coronary artery bypass grafting surgery (Leske, 2003); family members of patients who experienced traumatic injury (Leske et al., 2017); and family members of patients from surgical, medical, transplant, and cardiovascular ICUs (McAndrew et al., 2019). These comparisons highlight that HSCT family caregivers need support and resources to cope with the ICU experience as they transition back to navigating the patient’s ongoing and complex HSCT care regimen.
Family Caregiver Burden Specific to HSCT
Our qualitative data confirm and further elucidate the high levels of distress, anxiety, and depression discovered in the quantitative data, and the caregiver’s stories and experiences shared suggest that the ICU experience exacerbates cumulative caregiver burden. It is well accepted that HSCT family caregivers experience burden and strain as part of their ongoing caregiving role, and this burden can impair their ability to support the patient and sustain their own psychosocial and physical well-being (Applebaum et al., 2016). Family caregivers described the difficulty of bearing witness to the suffering of their family member. They shared emotional concerns, challenges to self-care, and difficulty balancing caregiving with other responsibilities. In a recent correlational study of allogeneic HSCT caregivers, 45% of the respondents reported having to reduce their hours to accommodate treatment demands, and reduced caregiver employment was associated with higher anxiety and depression scores (Natvig et al., 2022). Addressing caregiver role concerns while the patient is hospitalized may help caregivers strategize and put resources in place for more intensive caregiving responsibilities after discharge.
The burdens experienced by family caregivers of patients with end-stage diseases, such as renal failure or heart failure, share some similarities with that of HSCT caregivers: uncertainty, financial strain, competing responsibilities, exhaustion, and unending care responsibilities (Kitko et al., 2020; Lahoz et al., 2021; LeSeure & Chongkham-Ang, 2015; Oyegbile & Brysiewicz, 2017a, 2017b; Walavalkar et al., 2022). In the cancer caregiving literature, there are recognized benefits of caregiving, such as deeper relationships (LeSeure & Chongkham-Ang, 2015). Similarly, finding benefits in caregiving is also recognized in other caregiving literature. For example, family caregivers of renal failure patients described balancing caregiving burden with the opportunity for enhancing relationships with the patient (Oyegbile & Brysiewicz, 2017b).
There are important differences in the experience of HSCT family caregivers that make their caregiving trajectory unique. For example, the burden for family caregivers of heart failure patients increases as the patient steadily deteriorates and requires higher levels of supportive care (Lahoz et al., 2021). In contrast, the burden for HSCT family caregivers remains high throughout the recovery process (Akgul & Ozdemir, 2014; Bevans et al., 2016). For HSCT family caregivers, the hope for cancer remission is tempered by the fear of transplant failure or complications. As described in one study, the HSCT caregiving experience is like “riding a roller coaster in the dark” (Wilson et al., 2009). Hope for end-stage disease family caregivers may look different than for HSCT family caregivers, as those caregivers must confront negotiation of deterioration and the impending dying process (Walavalkar et al., 2022). Due to the patient’s lack of an immune system, family caregivers and patients must engage in social isolation for extended periods during the HSCT process, increasing psychological burden and vulnerability (El-Jawahri et al., 2020). Furthermore, cancer caregiving culture which focuses on “fighting” the disease may contribute to limited discussions about prognosis and survival, increasing a sense of helplessness for HSCT caregivers, as noted by one participant in our study. Importantly, cancer caregivers report the impetus to stay positive and search for hope (LeSeure & Chongkham-Ang, 2015). In chronic, life-limiting diseases such as organ failure family caregivers may have more time to adjust to the prognosis and increasing caregiving demands and plan for impending death. There are several nuances in the cancer caregiving experience that differentiate it from other caregiving contexts. One is that the cancer diagnosis is often sudden, so the caregiver must cope with the shocking news and are immediately thrust into a new role that may lead to feelings of helplessness and inadequacy (LeSeure & Chongkham-Ang, 2015). Another is that due to the prognostic uncertainty that occurs in many hematologic cancers, transitions to end of life are abrupt and difficult (El-Jawahri et al., 2020).
Family Caregiver Protective Factors
Despite their vulnerabilities, the HSCT family caregivers in our study also reported moderate levels of protective family factors suggesting they bring important family strengths to the ICU experience. Family coping and problem-solving levels in our study are similar to those conducted with family members of patients with trauma and cardiovascular diseases (Leske, 2003; Leske & Brasel, 2010). HSCT family caregivers reported greater levels of resources compared with other ICU family populations (Leske & Brasel, 2010). These HSCT family caregivers likely developed an infrastructure of resources during the transplant process. In individual interviews, caregivers in our study discussed how their prior experiences with illness brought them closer together as a family and contributed to new understandings and perspectives about supporting each other and the patient (family cohesion). They expressed that supporting each other as a family during the uncertainty of transplant promoted resilience that helped them cope with the ICU experience. Interview data also suggested that caregivers used coping mechanisms in the ICU that they had strengthened during the transplant process, such as spirituality, positivity, humor, finding purpose, and leaning into hope for the future. Our findings are similar to those of a qualitative study that examined spouses’ experiences with HSCT (Langer et al., 2020). While spouses experienced anxiety/worry, fear, uncertainty, and feeling overwhelmed, they also expressed optimism, gratitude, hope, and pride.
Family Caregiver Bereavement Experience
Approximately 15% of HSCT patients will require an ICU admission for an HSCT- related complication, and mortality is approximately 50% for these patients (Fornwalt et al., 2021). Notably, four of nine of the patients in our study died during the data collection period, a barrier to further data collection from these patients’ family caregivers. Two additional patients died after data collection but during the hospitalization. The close relationship between HSCT patients and their caregivers may contribute to a unique bereavement experience (Thompson et al., 2021). A sudden end to this dyadic relationship may lead to a more complicated grief experience (Buck et al., 2022; Thompson et al., 2021). Despite the tremendous strain of HSCT caregiving, support for HSCT family caregivers remains focused on addressing their informational needs rather than addressing their complex psychosocial and spiritual needs (Wang et al., 2021). Palliative care aims to relieve physical, psychological, social, and spiritual suffering to improve quality of life for patients and their families (World Health Organization, 2022). There is evidence that integrating palliative care throughout the HSCT journey may improve patient and family outcomes (El-Jawahri et al., 2017, 2020). During the ICU experience, palliative interventions could provide enhanced support to HSCT family caregivers as they navigate the prognostic challenges of critical illness after transplant. However, the literature suggests that palliative care is rarely offered to HSCT patients and caregivers for several reasons: Transplant is viewed as a curative treatment, the erroneous view that palliative care is only for transitions to end-of-life, lack of clarity about when palliative care should be involved, and standard palliative care triggers may not be relevant to the unique trajectory of hematologic malignancies (El-Jawahri et al., 2020; Uceda-Torres et al., 2016). Palliative and hospice care for HSCT patients and families, including bereavement support, is underexplored in the literature and remains an important research gap to fill. Improving access to palliative and hospice care in the inpatient and community setting is an important opportunity to address the unmet needs of this population.
Family Caregiver Engagement in ICU Care
HSCT family caregiver engagement in care is critical to transplantation success. However, family caregivers in our study reported obstacles to being present with the patient due to visitation restrictions, ongoing procedures, and tests, as well as an environment with little to no privacy. The ability to be in close proximity to the patient is a well-documented family need in the ICU literature (Al-Mutair et al., 2013; Brysiewicz & Chipps, 2017; Leske, 1986; Molter, 1979; Scott et al., 2019; Wetzig & Mitchell, 2017). Hospital policies and practices may prevent family caregivers from being fully engaged in the ICU (Naef et al., 2021), and this is particularly of concern for HSCT caregivers who have been playing an instrumental role in the care of patient. Family engagement in the ICU is an emerging priority for research, practice, and policy (Davidson & Strathdee, 2019). Family inclusion and involvement in decision-making and direct care of the patient may decrease the risk of some adverse outcomes for family caregivers after the ICU experience (Goldfarb et al., 2017; Haines et al., 2015; Zante et al., 2020). Although family caregivers in our study reported moderate levels of engagement in ICU decision-making, they also described many challenges to being fully engaged in care. The paucity of reliable and valid measures of family caregiver engagement hinders improvement efforts. We used a new tool to measure engagement (Heyland, 2018), and we do not have published comparative literature for this measure. Our findings suggest there is opportunity in the ICU to increase engagement for HSCT family caregivers, as these caregivers are already highly involved as designated caregivers during the transplant process. It is important that these family caregivers are fully engaged in the ICU setting given their expertise in the care of the patient, their understanding of the patient’s needs and wishes, their ongoing relationship with the transplant team, and their continuing caregiving role upon discharge.
A critical component of engagement is the quality of communication between health care professionals and patients and their family members (Davidson et al., 2017). Our qualitative data suggest opportunities for improvement in communication between the ICU team and family caregivers. In the ICU literature, communication remains a challenging aspect of patient care, particularly during prognostic uncertainty (Anderson et al., 2020; Peoples et al., 2020). Communication is frequently rated lower than other dimensions of ICU family care (Carlson et al., 2015). The most distressing communication issue for the family caregivers in our study was the disconnection between specialists and the ICU team that led to conflicting information relayed to the family. While it is recommended that oncology specialists work collaboratively with ICU teams (Azoulay et al., 2015), this may not be well translated into practice. Collaboration among specialties is necessary to provide consistent and clear communication to family caregivers who are often making decisions regarding patient care. Given the close relationship that family caregivers develop with the transplant team, and their experience working primarily with one team during the transplant experience, involving members of the transplant team in ICU care for this population may have high yield for both the patient and the family.
There is opportunity to build on prior HSCT family caregiver research with new studies that focus on the family system. Our study was guided by a family systems theoretical framework and sought to elicit the broader family experience through the eyes of the caregiver. Caregivers expressed being strengthened and challenged by their family system. For example, some caregivers had other family members requiring their support which stretched their caregiving capacity, while for other caregivers, the family had abundant resources to support both the caregiver and the patient. To advance family nursing science, future research could explore both the HSCT and ICU experience with a family systems lens. This approach could uncover additional opportunities for intervention development and begin to develop the evidence base for expanding the HSCT model of care to include the family system. This is important, as caregivers may need the support of their family to fully support the patient.
Directions for Future Research With HSCT Family Caregivers
Our data suggest a need for screening family caregivers for distress during and after an ICU stay and developing tailored interventions to address the adverse psychological symptoms that can be heightened for HSCT family caregivers in the ICU. An ICU admission may impact long-term outcomes for HSCT family caregivers and significantly increase their risk for anxiety, depression, and post-traumatic stress (Grant et al., 2020; Stayt & Venes, 2019). Although not specifically tested during an ICU stay, BMT-CARE, a six-session psychosocial intervention that uses cognitive-behavioral strategies to promote caregiving coping skills showed improvements in HSCT family caregiver reports of quality of life and symptoms of anxiety and depression compared with standard of care (Jacobs et al., 2020). These findings suggest psychosocial interventions hold promise to support family caregivers through a health crisis in the ICU. For example, a small pilot of a cognitive-behavioral acceptance-based intervention, EMPOWER (Enhancing and Mobilizing the POtential for Wellness and Resilience), was found to be helpful to ICU family members and decreased symptoms of anxiety, peritraumatic distress, experiential avoidance, and improvements in prolonged grief (Lichtenthal et al., 2022). Continued study of BMT-CARE and EMPOWER is warranted, particularly with HSCT family caregivers who may be supporting their hospitalized loved one through treatment complications or treatment failure. Furthermore, family-focused interventions after ICU discharge may help caregivers and family members address the long-lasting impact of both critical illness and the transplant experience.
Future studies with the HSCT family caregiver population in the ICU setting will need to account for the likelihood of caregiver bereavement. This study has highlighted the need to address gaps in care for HSCT caregivers, particularly access palliative interventions during an acute crisis, such as an ICU admission. The relatively small number of HSCT patients and their higher-than-average mortality rate poses recruitment challenges for conducting research with this vulnerable patient and caregiver population. Multisite study designs will be needed to ensure representativeness and adequate sample sizes.
Limitations
Based on 2017 to 2018 data, we estimated 35 potential HSCT patients transferring into the ICU. We found in our study that spanned a 16-month period that 38 HSCT patients transferred to the ICU. Our inclusion criteria specified that the patient must be in the ICU for 48 hr before a caregiver was approached for participation. A number of HSCT patients in our study transferred out in less than 48 hr or died before we were able to approach their family caregiver, leaving only 13 caregivers eligible for participation in our study. In addition, our study was conducted during the height of the COVID-19 pandemic, and this historical effect required pauses to data collection and modifications to our data collection plan (all remote data collection). Furthermore, the COVID-19 pandemic may have affected participants’ responses on the psychosocial domains measured in this study. Our accrual of HSCT caregivers was slow because HSCT patients and their family caregivers who met the study criteria were only sporadically available, making this population more challenging to study when they are in the ICU. Nonetheless, we overcame these challenges and successfully recruited and collected data from nine caregivers. We heard commonalities across our five interviews, although more interviews would have further confirmed data saturation. Although we obtained meaningful data about family caregiver outcomes, we did not have a large enough sample for comparisons based on caregiver and/or patient characteristics. Finally, from the perspective of transferability of these findings, HSCT is largely performed in high-income countries; thus, these insights may not be as relevant in low- to middle-income countries in which transplant may not be a treatment option (Rivera Franco & Leon Rodriguez, 2018; Ruiz-Argüelles et al., 2022).
Conclusion
In our study, we learned valuable information about how and when to approach HSCT caregivers and determined it was feasible to recruit HSCT family caregivers in the ICU. Multisite studies will be needed to reach a larger group of HSCT caregivers during the ICU experience. Mixed-methods data from this study provide a rich description of what HSCT caregivers endure during the ICU experience and highlight important opportunities for health care teams to provide increased support and intervention. Family caregivers reported communication challenges, as well as limited support for their well-being while in the ICU, but they also demonstrated resilience and strength. Understanding HSCT family caregiver experiences and responses is necessary to develop novel interventions to support them during an ICU event and augment family well-being. Our study demonstrates the value of studying a caregiving population based on the trajectory and treatment of the patient’s disease. Hematologic cancers have a unique disease trajectory, and HSCT is a highly specialized and complex treatment. Therefore, it is a priority for future studies to develop and test interventions specifically designed to support HSCT family caregivers. Providing meaningful opportunities for HSCT caregivers to engage as a true partner in care will build their capacity to fully support the patient and improve their own well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by an internal grant from the University of Wisconsin-Milwaukee—Research And Creative Activities Support Award (AAG6469).