
Abstract
Type 1 diabetes mellitus (T1DM) is typically diagnosed in pediatric patients. Transitioning from supported management in childhood to self-management in adolescence is an important step. Parental psychosocial influence is a possible factor in adolescents’ disease control. This review summarized the effects of parental involvement on glycemic control in adolescents with T1DM by focusing on hemoglobin A1c (HgbAIc). A scoping review per the Guidance for Systematic Scoping Reviews was conducted with the following inclusion criteria: (a) studies in English, (b) focused on adolescents with T1DM, (c) outcomes included HgbAIc, and (d) focused on parental influence of children with T1DM. Of 476 articles, 14 were included. The study outcomes were classified based on direct or indirect influence. “Parental support for adherence” and “parental conflict” significantly affected HgbAIc control. This study provides current evidence on parental influence on glycemic control in adolescents.
Type 1 diabetes mellitus (T1DM) is a disease that tends to develop in children and adolescents and is one of childhood’s most common chronic diseases (Chiang et al., 2020). Moreover, its occurrence is gradually increasing (Ruiz-Aranda et al., 2018), with a global incidence of 15 per 100,000 people (Mobasseri et al., 2020). In Japan, 500-600 pediatric patients are registered yearly for T1DM (Information Center for Specific Chronic Diseases, Japan, 2022). T1DM requires strict lifelong care and blood glucose control to maintain well-being. Patients are typically diagnosed with T1DM in childhood; thus, their parents must provide day-to-day care. This includes serving healthy foods, administering insulin injections, and controlling hyperglycemia and hypoglycemia (Centers for Disease Control and Prevention, 2022). Parental support is indispensable for patients with T1DM during childhood.
Adolescence, defined by the World Health Organization as ages 10-19 years, is a period of rapid and often asynchronous development in the physical, psychosocial, cognitive, and emotional realms (Sanders, 2013). Generally, adolescents are in a developmental period of transition from being children cared for by their parents to young adults capable of self-care, independent judgment, and self-directed problem-solving (Carroll et al., 2011). Children transforming into adolescents and preparing for emerging adulthood encounter psychosocial changes, and independence from parents is one challenge. For chronic diseases diagnosed in childhood, such as T1DM, although parents have several years of experience in managing their child’s disease and have developed a parental instinct, many parents remain unsure of how to instill this knowledge and intuition in the adolescent, and they fear this wealth of knowledge may be lost (Kayle et al., 2016). Thus, parents are concerned and conflicted about whether to protect or foster independence in their adolescent child. Therefore, transitioning of adolescents to self-management is a common challenge for children with chronic diseases and their parents (Kayle et al., 2016; Knopf et al., 2008; Lerch & Thrane, 2019; Sawicki et al., 2015). Notably, children with T1DM encounter challenges in the self-handling of daily care and overseeing blood glucose control (Babler & Strickland, 2015), and adolescence is a period associated with poor glycemic control (Ibfelt et al., 2022). Adolescent patients’ psychological and psychosocial functioning plays a vital role in disease control (Khadilkar & Oza, 2022; Tuohy et al., 2019). King et al. (2014) reported that associations between both maternal acceptance and diabetes monitoring and subsequent adolescent adherence were mediated by the adolescents’ self-efficacy. As King et al. (2014) suggested, parental involvement might affect the adolescents’ psychosocial function and glucose control. Parental psychosocial support during this transition may be considered one of the most significant factors. A systematic review comprising 40 studies concluded that family conflict, critical parenting, support, involvement, and relationship quality are associated with psychological health outcomes in youth with T1DM (Trojanowski et al., 2021).
Furthermore, single-parent families are reported to display worse adherence to self-monitoring of blood glucose (Lv et al., 2021). Lv et al. reported that adolescents with two parents have more resources that may contribute to better diabetes management, including self-monitoring of blood glucose, and they conclude that the adolescents gain support from both parents in terms of motivation for self-care. Thus, parental support for motivation remains important during adolescence to transition toward independence, suggesting that the psychosocial influence of parents is important during adolescence. In other words, parents, including their attitudes, communication, or familial relationships with the adolescents, can be the facilitative or inhibitory psychosocial factor for disease control.
Previous studies support an indirect association between parental involvement and their influence on T1DM self-control in adolescents, which is mediated by the adolescents’ psychosocial status. However, there is no clear consensus on the effects of parental involvement; thus, we were unable to use this information on parental influence as a predictor of family nursing intervention for families of children with T1DM. Presenting the predictors of family nursing interventions would assist in improving self-care for children with T1DM, a common challenge worldwide. The specific aim of this scoping review was to summarize and determine the effects of parental involvement on glycemic control in adolescents with T1DM. Additional objectives were to provide suggestions for clinically useful family nursing interventions. We intended to focus on hemoglobin A1c (HgbAIc) as an assessment measure, which is considered a better objective index than short-term indices (i.e., the frequency of blood glucose monitoring) for psychosocial function.
To date, no such review or synthesis on this topic has been identified in the Cochrane Database of Systematic Reviews and Joanna Briggs Institute Evidence Synthesis.
Methods
A scoping review (Munn et al., 2018) was deemed the most suitable approach for analyzing the reliability of evidence for the parental psychosocial influence on HgbAIc. It generally includes diverse sources of evidence and can be used to identify the types of available evidence in a field (O'Grady et al., 2022). Therefore, scoping reviews are useful when the literature has not been comprehensively reviewed or is not amenable to a more detailed systematic review of the evidence owing to complex or heterogeneous studies. This review was conducted according to the “Guidance for Systematic Scoping Review” (Peters et al., 2020). According to this guideline, we developed an a priori protocol.
Research Question
The study objective focused on the parental psychosocial influence on self-controlled blood glucose levels in adolescents with T1DM with HgbAIc as the outcome. This question was guided by the following research questions: (a) What were the facilitative/inhibitory psychosocial influences of parents of adolescents with T1DM? (b) What was the reliability of the studies comprising evidence of parental influences assessed in relation to HgbAIc control?
Inclusion Criteria
The inclusion criteria for the selected studies were as follows: (a) published in English, (b) primary focus on adolescents with T1DM, (c) the study outcomes included HgbAIc, and (d) the studies focused on parental influence on their children with T1DM. All study designs were considered eligible. The exclusion criteria for the studies were as follows: (a) not published in English, (b) conducted on animals, and (c) conducted more than 20 years ago.
Search Strategy
The first electronic search was conducted from June 10, 2020, to June 25, 2020, with the guidance of a librarian of the Medical Literature Analysis and Retrieval System Online (MEDLINE) and the Cumulated Index to Nursing and Allied Health Literature (CINAHL) databases. As the MEDLINE database was available in PubMed, the PubMed online database was used. The search focused on studies published in the previous two decades (2000–2020). Initially, a limited search of these online databases was performed to identify relevant articles on this topic. In the identification search, 190 articles from CINAHL and 286 articles from PubMed were included. The index terms and search history are shown in Table 1.
The Search History.
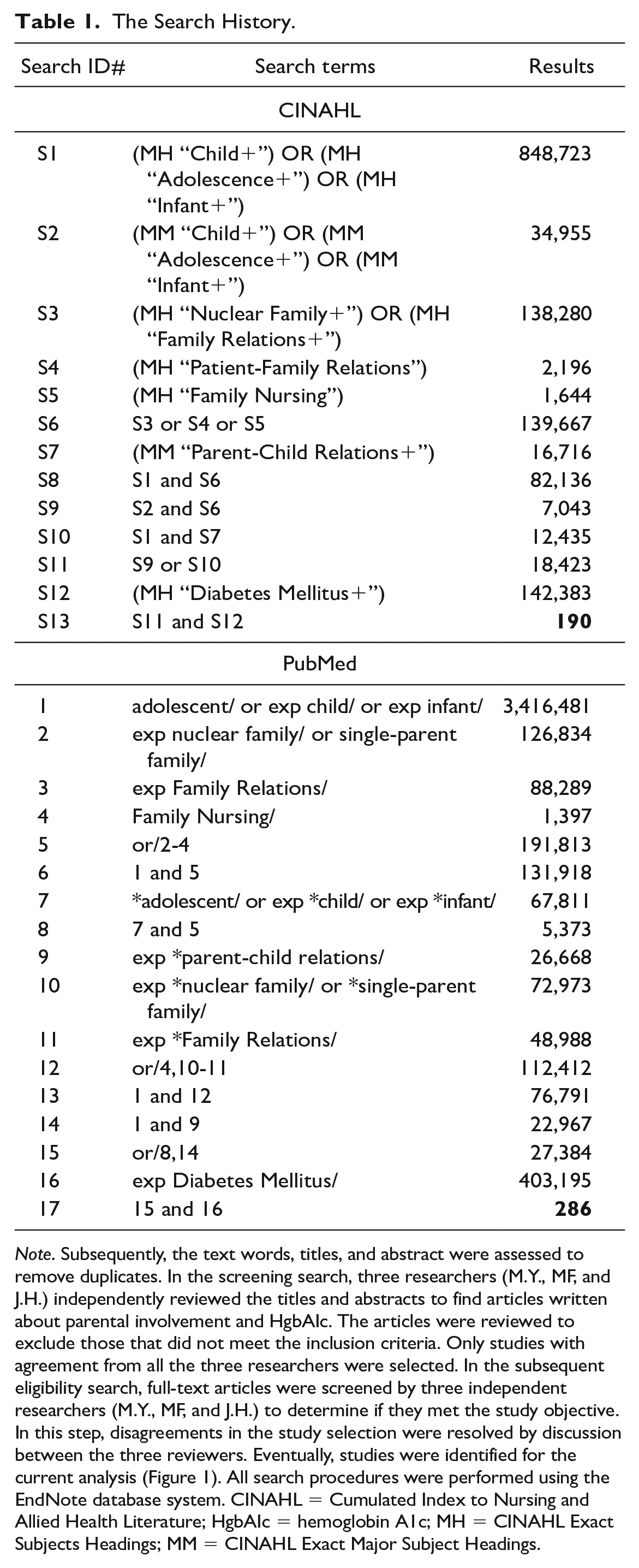
Note. Subsequently, the text words, titles, and abstract were assessed to remove duplicates. In the screening search, three researchers (M.Y., MF, and J.H.) independently reviewed the titles and abstracts to find articles written about parental involvement and HgbAIc. The articles were reviewed to exclude those that did not meet the inclusion criteria. Only studies with agreement from all the three researchers were selected. In the subsequent eligibility search, full-text articles were screened by three independent researchers (M.Y., MF, and J.H.) to determine if they met the study objective. In this step, disagreements in the study selection were resolved by discussion between the three reviewers. Eventually, studies were identified for the current analysis (Figure 1). All search procedures were performed using the EndNote database system. CINAHL = Cumulated Index to Nursing and Allied Health Literature; HgbAIc = hemoglobin A1c; MH = CINAHL Exact Subjects Headings; MM = CINAHL Exact Major Subject Headings.
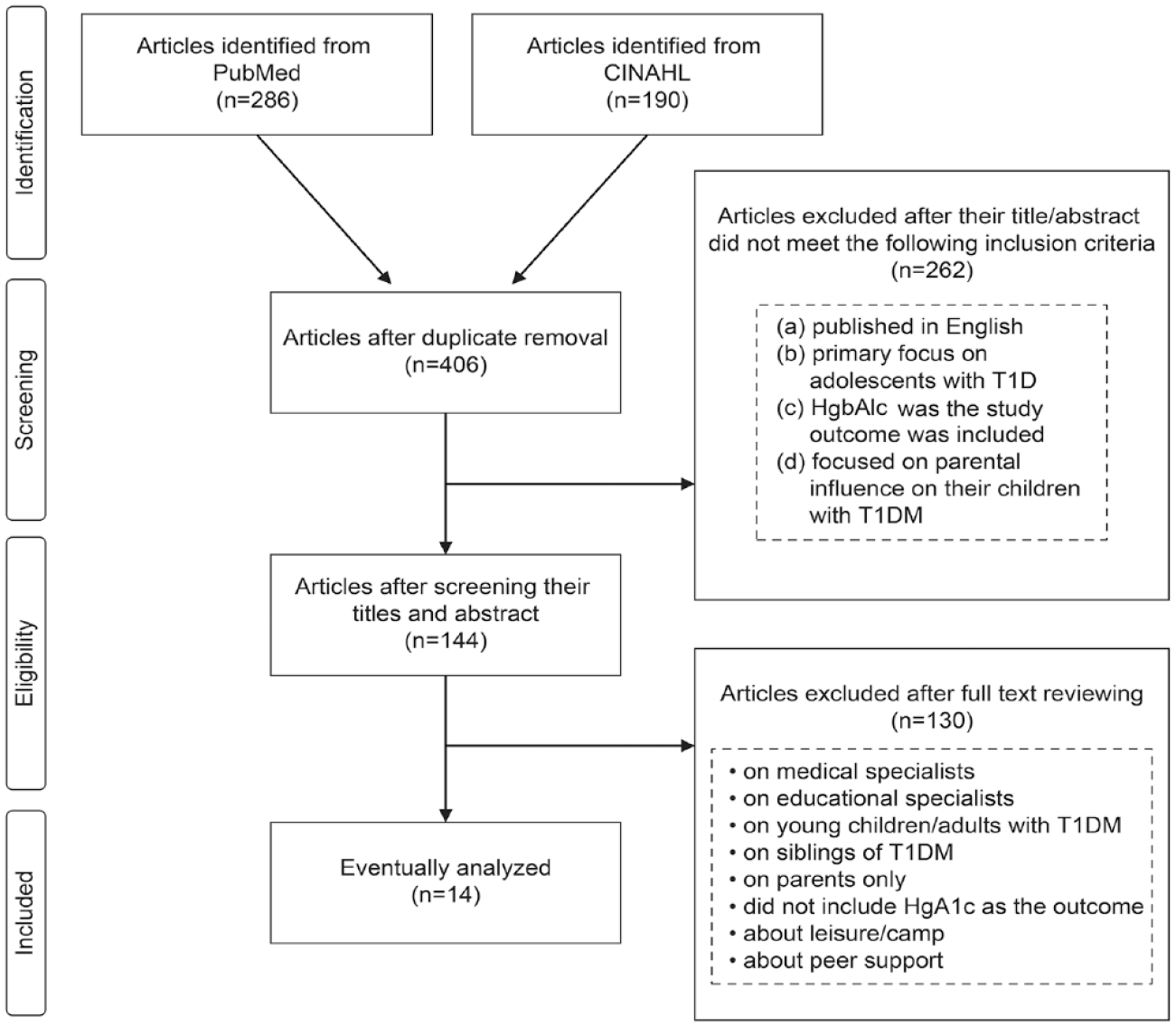
Flow Diagram Summarizing the Database Search.
Data Collection and Synthesis
The three reviewers discussed their key findings and found a high level of consistency in the data extracted from the studies. However, if a study did not contain significant results, the nonsignificant results were reported when all the three researchers agreed that the findings were important for the focus of this review. Finally, MY created a data list and extracted the following from the selected articles: authors, title, country, design, sample size, participants’ age, demographics, measurement tools (containing HgbAIc), and key findings. After data extraction, the results were collated and summarized to include the study characteristics based on the research question. The key findings were outlined in the reported results and then synthesized based on the viewpoint of the effect of parental influence and HgbAIc outcome.
Study Design Appraisal
The “Guidance for Systematic Scoping Review” (Peters et al., 2020) states that a formal assessment of the methodological quality of the included studies is generally not performed. However, there are now discussions about scoping reviews regarding the usefulness of additional assessments of the quality and methodological rigor of the included studies (Levac et al., 2010). Thus, we used the Quality Assessment Tool for Studies with Diverse Designs (QATSDD) to appraise the study design quality (Kwan et al., 2020) (Table 2) and ensure that the data are rigorous. QATSDD is a 16-item quality assessment tool that can be applied to various study designs (Sirriyeh et al., 2012).
Quality Assessment of the Included Studies Based on the QATSDD Tool.
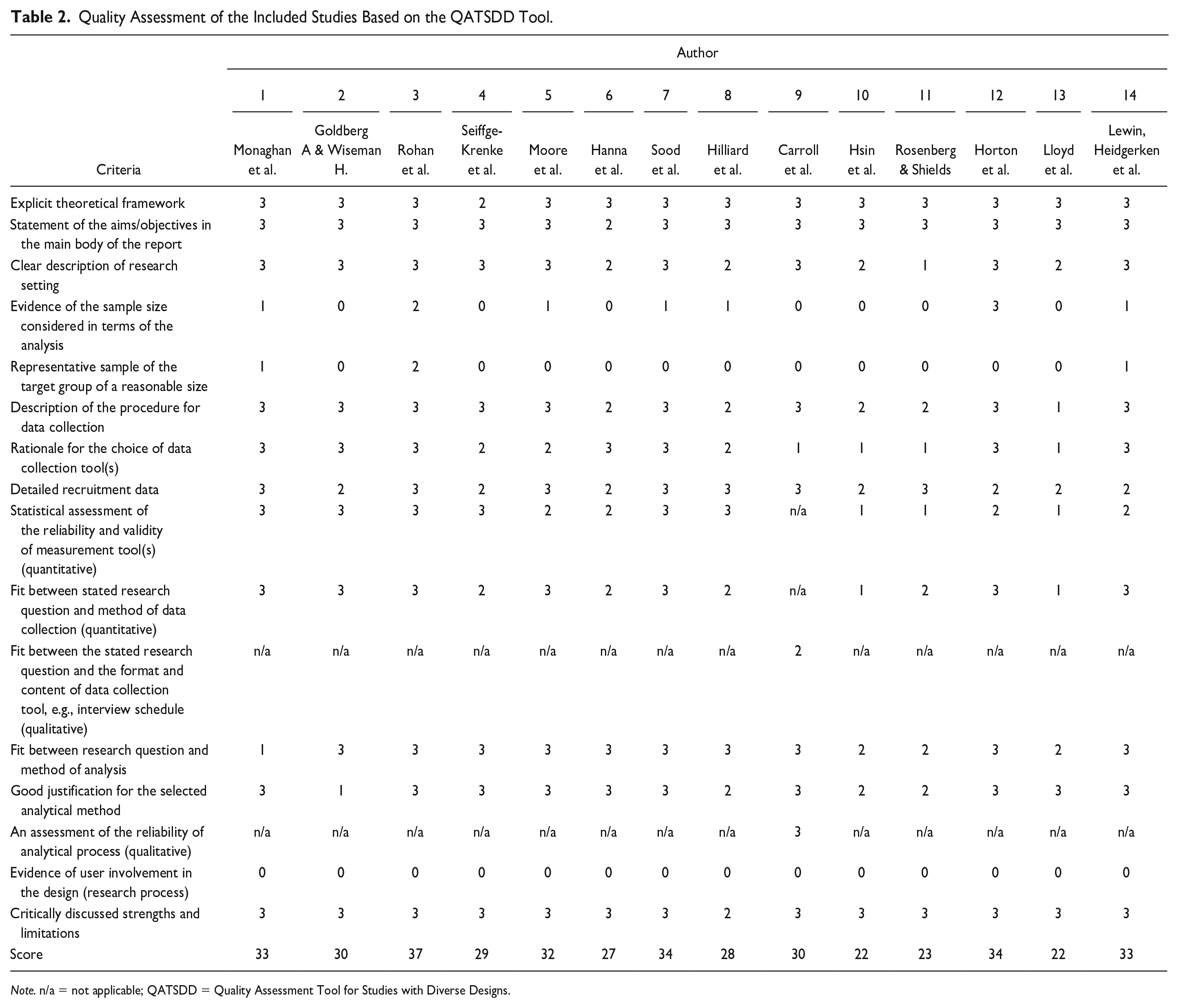
Note. n/a = not applicable; QATSDD = Quality Assessment Tool for Studies with Diverse Designs.
Results
Figure 1 depicts the number of studies identified at each search stage. A total of 476 articles were identified in the initial search, including 286 and 190 articles from PubMed and CINAHL, respectively. We removed 70 duplicate articles and screened the titles and abstracts for the remaining 406 articles. Moreover, we assessed the titles and abstracts of the selected studies. Subsequently, the full text of the remaining 144 articles were independently reviewed by three authors to determine if they met the inclusion criteria and objectives. In this step, we excluded the studies conducted on medical specialists, educational specialists, young children/adults with T1DM, their siblings, parents only, not using HgbAIc as the outcome, and about leisure/camp or peer support. Eventually, this scoping review included 14 articles (see Table 3).
Summary of the Included Studies.
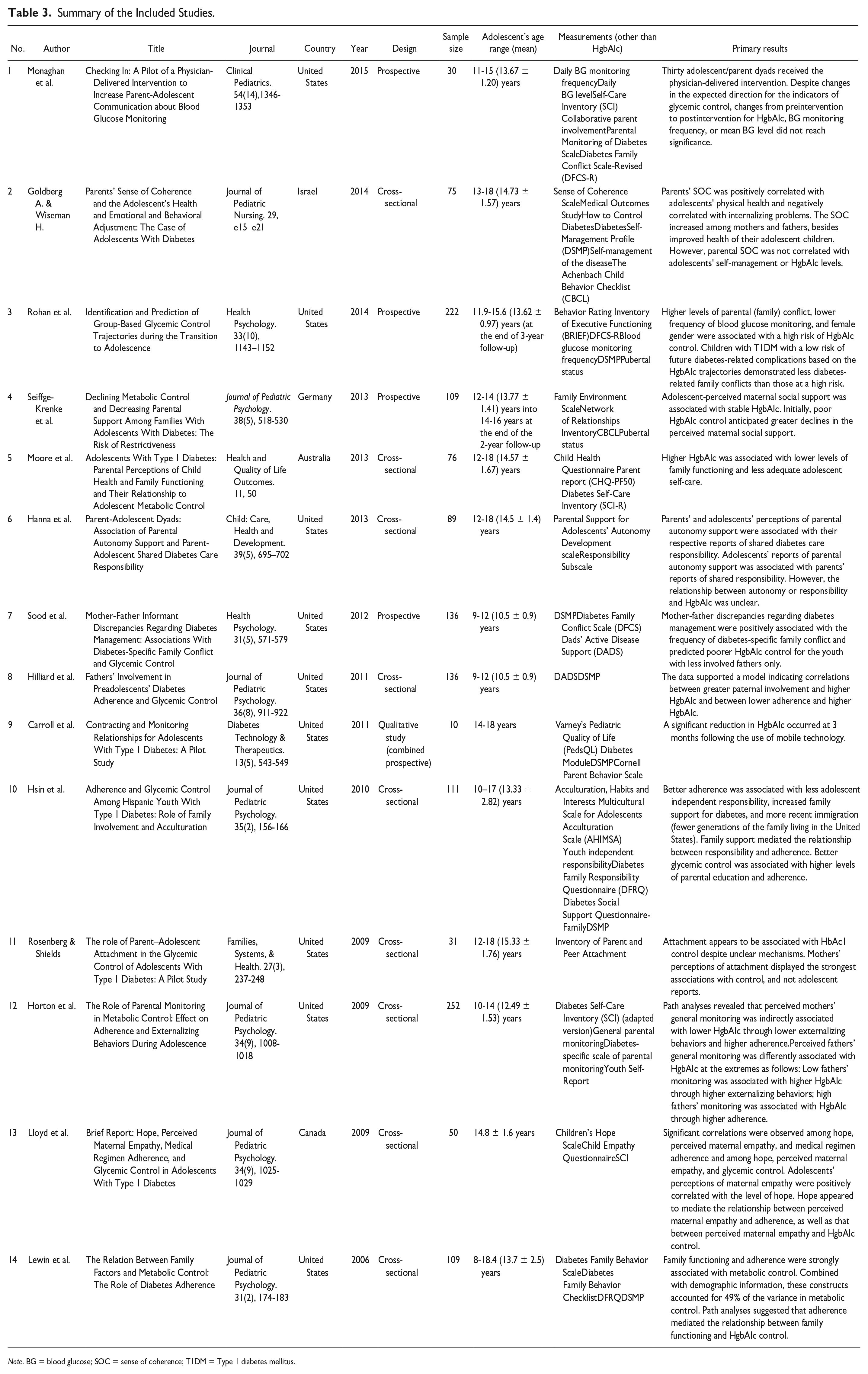
Note. BG = blood glucose; SOC = sense of coherence; T1DM = Type 1 diabetes mellitus.
Study Characteristics
The selected studies were published between 2006 and 2015. Ten studies were conducted in the United States. The remaining studies were from Australia, Israel, Germany, and Canada. There were nine and four cross-sectional and longitudinal studies, respectively. Only one study comprised a qualitative analysis (combined statistical prospective study).
Study Participants
The sample sizes varied from 10 to 252, and 1,436 adolescents with T1DM (mean age: 13.08 years) participated in these studies (see Table 3 for each study’s sample size). All studies except one were based on a dyad of children with T1DM and either of their parents. Only one study comprised children with T1DM as the participants (article no. 13) and investigated the relationship between adolescents’ perception of maternal empathy and glycemic control.
The Measurement of Parental Influence
Table 3 summarizes the included articles. All articles used HgbAIc as the primary outcome. Parental psychosocial influences were directly or indirectly assessed using different scales. Family conflict was one of the psychosocial environments. Therefore, the Diabetes Family Conflict Scale and its module-type scale (Hood et al., 2007) were used in three studies (articles 1, 3, and 7). Six studies used the Diabetes Self-Management Profile (Harris et al., 2000) (articles 2, 3, 7, 8, 10, and 14), whereas four studies used the Self-Care Inventory for specific diabetes self-care (La Greca, 2004; La Greca et al., 1995; Lewin et al., 2009) (articles 1, 5, 12, and 13) to measure the adherence to self-care or management behaviors in adolescents affected by parental psychosocial influences. Two studies focused on the fathers’ involvement in diabetes management and used the Dads' Active Disease Support Scale (Wysocki & Gravin, 2004) (articles 7 and 8). The Diabetes Family Responsibility Questionnaire (Anderson et al., 1990) was used in two studies (articles 10 and 14) to assess the number of independent diabetes management tasks for which the adolescents were responsible. Other measurements or scales were used in each study sequentially for the following aspects: parent-adolescent collaboration (article 1), network (article 4), attachment (article 11), behavior (articles 4, 9, 14), and empathy (article 13); the parents’ sense of coherence (article 2); the adolescents’ sense of control (article 2), self-management (article 2), autonomy (article 6), independence (article 10), and hope (article 13); and the adolescent’s quality of life (article 9). This scoping review analyzed these scales or their subconcepts (as required). The family function was a comprehensive concept for assessing families; this study focused on parental influences without siblings or the total function of familial members. Thus, we decided not to include family function among the influencing factors. Instead, we analyzed the subconcepts of family function as required. Figure 2 depicts an evidence map of the 14 articles, with evidence of the importance of study outcomes and quality appraisal.
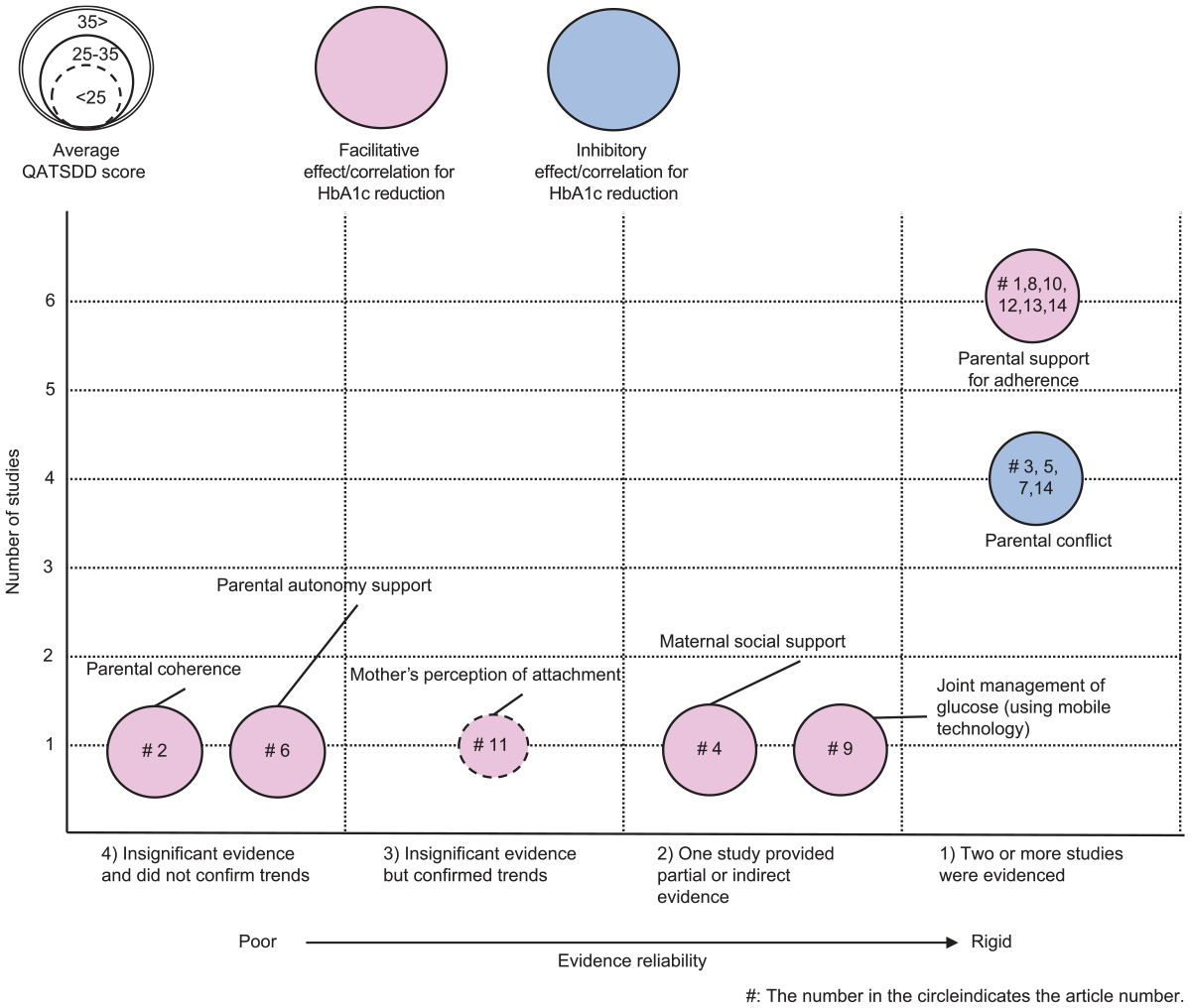
Evidence Map of Studies on the Effect on Glycated Hemoglobin (HgbAIc).
Evidence of Study Outcomes
The study outcomes were classified according to the effects of direct or indirect parental influence and were divided into four evidence levels: (a) Two or more studies provided evidence for a facilitative/inhibitory significant relation or correlation for the reduction of HgbAIc; (b) one study provided evidence for a facilitative/inhibitory significant relation or correlation for the reduction of HgbAIc/partial or indirect evidence for a facilitative significant relation or correlation for the reduction of HgbAIc; (c) insignificant evidence but confirmed trends; and (d) insignificant evidence and unconfirmed trends. Figure 2 depicts the inhibitory significant relation or correlation for the reduction of HgbAIc. Each study was grouped in relation to its outcome as the subitems of parental psychosocial influence, and the level of evidence was determined for each study group. Each group is described with the theme of subitems and detailed information in the following sections.
Parental Support for Adherence
Promoting adolescent adherence linked to parental influence significantly affected HgbAIc. Article 1 hypothesized that an intervention program to improve adherence might improve HgbAIc control. The results did not report significant changes in preintervention and postintervention adolescent adherence. However, it demonstrated trends in improved HgbAIc (Monaghan et al., 2015). Article 8 showed a significant relationship between lower adolescent adherence and higher HgbAIc. Parental involvement was associated with poorer HgbAIc. Despite no direct association between adolescent adherence and parental involvement, the authors confirmed the trend (Hilliard et al., 2011). Article 10 demonstrated better adherence related to greater family support and better HgbAIc control associated with improved adherence (Hsin et al., 2010). Article 12 hypothesized the path model that parental glucose monitoring influences adolescent adherence, which in turn influences HgbAIc. It revealed that parental glucose monitoring was indirectly associated with lower HgbAIc through higher adherence (Horton et al., 2009). Article 13 confirmed significant correlations of adolescent-perceived maternal empathy with adolescent adherence and HgbAIc. Despite no confirmation of the direct relationship between HgbAIc and adolescent adherence, these related factors were influenced by mediators, such as adolescent-perceived hope (Lloyd et al., 2009). Article 14 was an integrated analysis of family function with adherence and HgbAIc. Moreover, an analysis of both standardized regression weights and structure coefficients suggested that adherence was strongly related to HgbAIc despite its multicollinearity with family functioning (Lewin et al., 2006). In other words, parental involvement was substantially correlated with adolescent adherence, which was related to HgbAIc.
Parental Conflict
Parental conflict was significantly related to the HgbAIc of adolescents with T1DM, as confirmed by the evidential influencing factors. Article 3 concluded that children with T1DM at low risk of future diabetes-related complications based on the HgbAIc trajectories demonstrated lower diabetes-related parental conflict than those at high risk (Rohan et al., 2014). Article 5 concluded that higher HgbAIc (poorer metabolic control) was associated with lower levels of the specific items from the Child Health Questionnaire Parent report that target parental conflict. Therefore, it was associated with family functioning (Moore et al., 2013). Article 14 focused on parental conflict as a part of family function; HgbAIc was associated with parental conflict (Lewin et al., 2006). Article 7 studied the relationship among parental conflict, mother-father discrepancies, and HgbAIc. Mother-father discrepancies were positively associated with family conflict. These discrepancies regarding diabetes management predicted poorer HgbAIc control for youth with less-involved fathers; nonetheless, family conflict and HgbAIc were not irrelevant in this study (Sood et al., 2012). Thus, articles 3, 5, 7, and 14 provided evidence for the relationship between poor HgbAIc control and high familial conflict. Article 1 used the Diabetes Family Conflict Scale-Revised (DFCS-R). However, the DFCS-R score was not assessed in relation to HgbAIc levels. Instead, it was used to compare the preintervention and postintervention findings, and the results reported that family conflict improved after the intervention (Monaghan et al., 2015). The mentioned studies did not confirm a causal relationship between HgbAIc and family conflict; however, they demonstrated the importance of reducing family conflict for the psychosocial stability of adolescents with T1DM, which may be indirectly associated with HgbAIc control.
Parental Coherence
Article 2 was the only study focusing on the parents’ sense of coherence, which was not correlated with the adolescents’ self-management or HgbAIc (Goldberg & Wiseman, 2014).
Maternal Social Support
Article 4 focused on parental social support and HgbAIc control in adolescents. It confirmed statistically significant associations between adolescents’ maternal social support and HgbAIc control (Seiffge-Krenke et al., 2013). However, no other studies supported this outcome.
Parental Autonomy Support
Article 6 studied the importance of parental autonomy support. However, it could not demonstrate the relationship between parental autonomy support and HgbAIc in adolescents (Hanna et al., 2013).
The Joint Management of Glucose
Article 9 aimed to develop a mobile technology system to manage negotiable points of conflict within the parent-child relationship regarding self-monitoring. It predominantly adopted a qualitative approach to interview data. It conducted a supplementary statistical analysis and demonstrated a significant reduction in HgbAIc because of the joint management of glucose monitoring with technology intervention and adolescent-parent relationships (Carroll et al., 2011).
Mothers’ Perception of Attachment
Article 11 focused on mothers’ perception of attachment. Despite unclear mechanisms, mothers’ perceptions of adolescents’ attachment were significantly correlated with HgbAIc (Rosenberg & Shields, 2009).
Quality Appraisal
A quality assessment was performed using the QATSDD (see Table 2). The included studies scored between 22 and 37 (mean 29.6).
Discussion
This novel review included articles that focused on parental influences as psychosocial factors of HgbAIc control in adolescents with T1DM.
Previous clinical data have repeatedly demonstrated that patients have difficulty reaching and maintaining glucose control during adolescence (Amiel et al., 1986; Dabadghao et al., 2001; Eilander et al., 2015). The Diabetes Control and Complications Trial demonstrated that better glycemic control during adolescence lowers the risk of developing complications later in life (White et al., 2001). This scoping review comprised studies performed across several countries. The issue of T1DM and glucose control during adolescence and into adulthood is an important study area to improve health care.
Interestingly, this review highlighted two evidential parental influences. First, parental support for adherence exerted a facilitative effect on HgbAIc control, whereas parental conflict exerted an inhibitory effect on HgbAIc reduction.
Adherence commonly describes a patient who appropriately follows medical advice based on positive patient-medical specialist relationships. The development of children into young adults through adolescence necessitates medical specialists and parents to understand the changing needs of youth with T1DM to improve the quality and efficacy of pediatric diabetes care. This study’s findings were consistent with those of most recent studies. In a random sampling study (Temmen et al., 2022), the high-parental-collaborative involvement group demonstrated the best adherence, glycemic control, and psychosocial well-being compared with the low-parental-collaborative group. Hsin et al. (2010) mentioned that better adherence was associated with lower adolescent independence and greater parental support. To summarize these findings, parental involvement in diabetes care is important in adolescence, but the optimal form of involvement may need to be adjusted to be consistent with the child’s level of development. Nurses must guide the parents to watch their children carefully and provide the necessary support. Parents should continually act as primary advisers to adolescents to maintain good patient-medical relationships and follow their medical instructions.
As T1DM requires frequent medical follow-up and ongoing intensive self-care (Garvey et al., 2014), it is clear that the psychosocial context may influence their self-care. Our study supports the previous studies’ (Drotar et al., 2013; Miller-Johnson et al., 1994) conclusion that parental conflicts exert a negative impact on an adolescent’s recuperation. Family conflict affects glucose control by interfering with the quality of diabetes management through increased stress levels in the child and parents. However, our study could not distinguish the conflict between or within the adolescent, mother, or father. The latest study (Campbell et al., 2022) revealed that adolescents with greater conflict with their mothers and fathers (average of 14 days) had higher blood glucose levels. Additional studies are needed to further understand their conflicts. In addition, as some studies (Matsumoto et al., 2022; Saßmann et al., 2022) reported, more research is needed to understand the parents’ burden and stress management.
New technology makes it possible to support adolescents to be capable of self-care and self-directed problem-solving. A pilot study used a cellphone-based glucose monitoring system and shared the health care information with parents. A recent study on diabetic adults reported an app-based monitoring system (Johnston, 2022). More technology applications are needed for T1DM adolescents.
Parental coherence is an important factor for parenting T1DM children, as it may disable children (Farhadi et al., 2022). However, as the evidence is not sufficient to make conclusions, further research is needed.
Additional parental influence was reported in the present study: Maternal social support, attachment, and autonomy support were also important for adolescent-parent relationships. These themes possibly relate to the parents’ psychosocial status; thus, more studies focusing on T1DM adolescents are needed in the future.
Our findings have important implications for both clinical and future research. Parental psychosocial factors may facilitate or inhibit glucose control in adolescents. However, we did not comprehensively clarify other or unknown parental psychosocial influences. This warrants future research to determine the influencing factors for better glycemic control with adolescents experiencing the developmental issues of transition to adulthood.
Our scoping review showed that only one study conducted a qualitative analysis (combined statistical prospective study). Further qualitative or mixed studies are needed to explore the experiences of adolescents and their parents, which may negatively influence HgbAIc levels.
Study Limitations
Numerous studies were based on adolescence and parental objective or self-report questionnaires to provide the leading sources that examined the psychosocial parental effects. However, as parental psychosocial influences on T1DM adolescence are complex and diverse, it cannot be said that these target studies have determined all parental influences. Therefore, one limitation was that our review could not provide all evidence of parental influence. However, it can suggest interventions to clinical specialists for adolescents with T1DM experiencing difficulties in glycemic control. Furthermore, it demonstrated that parents might exert either facilitative or inhibitory effects on adolescents with T1DM. Therefore, specialists should support both adolescents and their parents. Ultimately, further studies on alternative parental influences that have not been adequately studied (such as parental attachment or autonomy support) are warranted.
Conclusion
This scoping review included studies conducted in the last 20 years about the psychosocial influence of parents on HgbAIc control in adolescents with T1DM. This review presented new evidence and concluded that “parental support for adherence” and “family (parental) conflict” were the facilitative and inhibitory influences, respectively, and the study assessed their effect on HgbAIc in adolescents. As parental psychosocial influences on adolescents with T1DM are complex and diverse, our review cannot provide all evidence of parental influence. Further studies must focus on alternative parental influences that have not been adequately studied.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from the JSPS KAKENHI (grant number J222004155) is gratefully acknowledged.