
Abstract
Objective:
Paediatric cancer impacts both children and their families, transforming relationships and parenting styles. Within this context, hospitalisation at home (HaH) is increasingly offered in paediatric oncology, transferring care to the home setting and reconfiguring parenting styles. However, the literature on how parents redefine their roles and strategies at home remains limited. The aim of this study is to describe how parents of children with cancer redefine parenting in HaH by identifying the roles and strategies they use.
Methods:
A qualitative study using semi-structured individual interviews was conducted. The interviews were recorded, transcribed and analysed using Reflexive Thematic Analysis.
Results:
Twenty-seven parents were interviewed (18 mothers and 9 fathers). Analysis highlighted four themes: (a) adapting to a new care dynamic; (b) sharing parenting with health care teams; (c) taking on multiple parental roles (emotional parent, caregiver, mediator, child’s guide, parent for siblings and leader/coordinator); and (d) developing parenting strategies (mutual support between spouses, anticipation and control strategies, selective distancing and negotiating personal distress).
Conclusion:
HaH transforms parenting into a demanding experience that requires constant adjustments. Parenting manifests itself as an ongoing process, not just based on creativity and adaptability, but also marked by a silent vulnerability that highlights the need to fully recognise and support parents.
Introduction
According to the French National Cancer Institute, approximately 1,700 new cases of cancer are diagnosed in children under the age of 15 annually in France (Institut National du Cancer [INCa], 2024). Although therapeutic advances have significantly improved survival rates, paediatric cancer has major psychosocial impacts on the children affected by the illness (Lewandowska et al., 2021; McCaffrey, 2006; Tao et al., 2022). Cancer is also a deeply affecting experience for the entire family (Patterson et al., 2004), which is obliged to reorganise its daily life and relationships (Rolland, 2005).
Hospitalisation at home (HaH), which is increasingly offered to children with cancer, allows them to remain in a familiar environment while ensuring continuity of specialised care (Hansson et al., 2012). The HaH system denotes a model of care where medical treatment is provided in the patient’s home under conditions of equivalent safety and quality, and has proven to be both feasible and effective (Carter et al., 2014; Levine et al., 2021; McCann et al., 2012).
Although HaH has been increasingly promoted in several countries, its development remains highly heterogeneous, particularly in paediatric oncology. Models of HaH vary considerably across health systems in terms of eligibility criteria, resources, professional involvement, and the extent to which children with cancer are included (Fraser et al., 2020). While home-based care has been described in adult oncology, evidence focusing specifically on paediatric home hospitalisation for children with cancer remains limited and uneven across countries. In paediatric oncology and complex paediatric care, HaH has been described as feasible and acceptable in specific contexts, particularly when supported by specialised teams and adequate resources (Kassam et al., 2014; McCann et al., 2012).
This model also reduces prolonged hospital stays, which are often experienced as physically, psychologically and organisationally challenging (de Flon et al., 2021; Hansson et al., 2012). In many countries, HaH is typically the preferred option of children and parents since it provides the comfort of a familiar environment and the reassuring presence of family and friends (Carter et al., 2014; Kassam et al., 2014; McCann et al., 2012). In France, although paediatric home hospitalisation remains limited, its development has increased significantly, with an average annual growth of 8% between 2016 and 2020, now accounting for 4.7% of total HaH admissions (Baussant-Crenn et al., 2023).
A systematic review by Noyes et al. concluded that there is no universal preference for homecare. The authors noted that the choices are heterogeneous and evolving, and may depend on factors such as the quality of communication with professionals, confidence in hospital staff, the availability of care, the option of a home environment and the child’s wishes when they can express an opinion (Noyes et al., 2022). While HaH provides benefits in terms of quality of life, family proximity and reduced hospital time (Verberne et al., 2019), it also introduces a new complexity: the home becomes a hybrid space, both a place of living and a place of care. This requires parents to reorganise themselves materially, relationally and emotionally (de Flon et al., 2021; Kirakosyan & Bacqué, 2025). In addition, HaH disrupts everyday routines and redefines the role of parents (Kars et al., 2015).
The concept of parenting – defined as all the activities, care and skills exercised by adults who look after their children (Arendell, 1997) – is particularly appropriate. Many studies recognise the importance of the family, and parents in particular, in the daily care of children with cancer (Alsem et al., 2014; Smith et al., 2015).
Qualitative studies in paediatric oncology emphasise that the parental experience is based on a fragile balance between family continuity and the integration of medical care (Aasen et al., 2019; Kars et al., 2015). Yet, in the context of HaH, parental involvement can become even more intense. Several studies have shown that parenting in cases of chronic illness or disability embraces multiple roles: caregiver, mediator, protector and emotional resource (Kirakosyan et al., 2025; Lowes et al., 2005; Salomé et al., 2024). This research also highlights the cost of this intense parenting, characterised by exhaustion and the constant mobilisation of resources to manage the situation (Woodgate et al., 2015). During HaH, in addition to ordinary care and family responsibilities, parents must cope with expanded roles and constantly adapt to medical requirements (Coad et al., 2015; Hobson & Noyes, 2011). They also need to provide some of the often complex medical care on a daily basis. HaH can reconfigure parenting since it concentrates the demands of care and the needs of the child with cancer, their siblings and the broader family within the same space and time.
Research on parenting in paediatric oncology, however, does not take into account how parents actively redefine their roles and employ strategies in a medicalised home environment. The aim of this study, therefore, is to explore how parents of children with cancer receiving homecare redefine parenting. More specifically, this article seeks to analyse the parental roles and strategies deployed in this context, highlighting the adjustments, tensions and resources that shape the parenting experience.
Method
This research forms part of a larger PEP-HAD study – Parenting and Paediatrics in Hospital at Home (Parentalité et Pédiatrie en Hospitalisation à Domicile) – that aims to describe parenting and parent-child relationships when a child has cancer and is hospitalised at home.
Study Design
This study was shaped by an interpretive descriptive design, which focuses on exploring and understanding “participants’ subjective experiences and sense-making” (Braun & Clarke, 2013). Interpretive description is aligned to a constructivist paradigm, which assumes that a persons’ reality is actively constructed based on their experiences and thoughts (Hunt, 2009). These insights can be used to describe how parents experience and give meaning to parenting in the context of HaH, suggesting that parenting is understood as constructed within a socio-cultural context, influenced by complex lived experience, multiple roles and responsibilities, fluid dynamics and home setting that has become hybrid: that is, a domestic space and a place of medical care. So, participants perspectives are contextually bound and ultimately subjective, and knowledge is co-constructed between participants and researchers (Guba & Lincoln, 1994). Within this interpretive descriptive design, reflexive thematic analysis was employed as the analytic method, in line with the constructivist epistemological framework of the study.
Participants and Procedure
Participants were recruited between June 2024 and March 2025 in two organisations: Fondation Santé Service (Levallois-Perret, Paris) and Hôpital à Domicile des Vignes & des Rivières (Libourne), both of which provide hospitalisation, medical care and psychosocial support to patients at home. The inclusion criteria were as follows: (a) participants had to be a parent of a child aged between 5 and 12 years. This age range was defined in the initial study design in order to focus on school-aged children, for whom parenting roles, family organisation, and daily care practices present specific characteristics in the context of home hospitalisation. Including children under 5 years old or adolescents would have involved substantially different developmental, relational, and caregiving dynamics, which were beyond the scope of the present study. (b) Children had to be diagnosed with cancer (oncological or haematological) and receive home hospitalisation in the months following diagnosis and the end of the initial treatment. We excluded parents whose child was in palliative care or who had recently died in order to avoid biases linked to acute psychological distress that was not yet stabilised.
For the recruitment process, the HaH teams – nurses, paediatricians and psychologists – first identified individuals at the time of recruitment. They approached all the parents of children with cancer who met our criteria (n = 41) during regular home visits. Among the 41 parents approached, 27 were mothers and 14 were fathers. They (third and fourth authors) presented the study orally to all the parents and gave them a written information sheet. Some parents (9 mothers and 5 fathers) refused to take part, but did not explain their reasons. Parents who expressed an interest in taking part gave their consent by signing the consent form and providing a telephone number where the researcher (initials will be given later) could contact them.
Since the researcher had no prior relationship with the parents, the first telephone call served to build trust between the researcher and the participant. It also aimed to introduce the researcher, present the study, answer any questions, and schedule an appointment at a time that suited the participant based on their preferences: in-person, by phone or via video conference. All parents who agreed to take part opted for a telephone interview, explaining that they did not want to be away from home and did not want to receive visitors. The second call was used to conduct the research interview.
Data Collection
The interviews started with the parents providing background information (such as age, family composition, cancer diagnosis, and how long their child had been hospitalised at home) in order to contextualise their experiences. In accordance with French legislation (Loi Informatique et Liberté, CNIL, 1978), it is strictly prohibited to collect and record directly or indirectly information indicating the ethnic origins and religious affiliations of individuals, and such information is not provided.
A semi-structured research interview was conducted by the researcher (first author) on a one-to-one basis. A single interview guide was developed to provide a common framework for all participants, inviting interviewees to describe their experience (see Box 1). The guide was based on the existing literature and prior clinical observations. Rephrasing and prompts were used during the interviews, where necessary, to elicit further information and clarify responses.
Interview Framework.
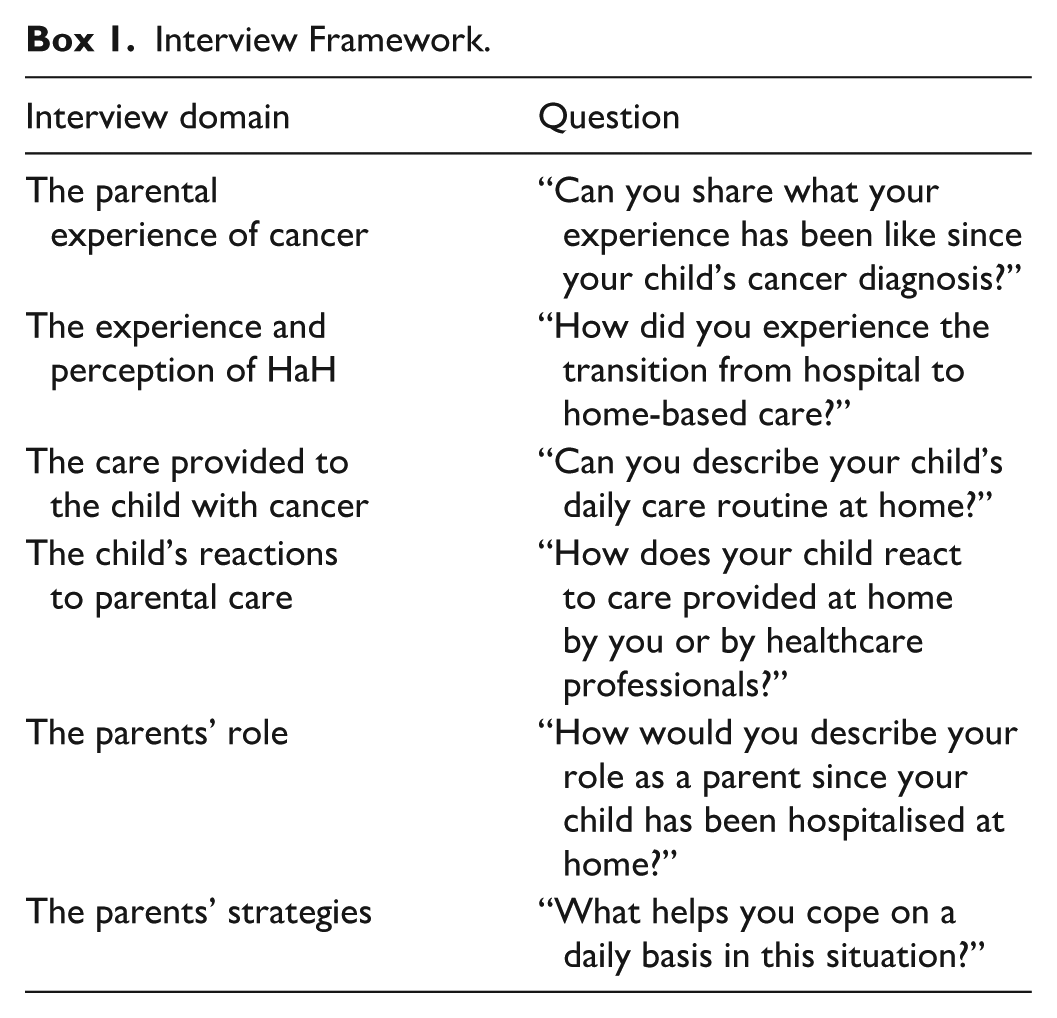
Each interview was recorded with the consent of the participant and transcribed in full by the researcher. Each participant’s file was coded to ensure confidentiality, and all first names were changed to ensure anonymity. The interviews lasted between 30 and 90 min, with a mean duration of approximately 59 min. Field notes were made after the interviews. Data collection was guided by the principle of information power, whereby the adequacy of the sample was assessed based on the relevance, richness, and diversity of the parental experiences in relation to the study aim (Malterud et al., 2016). Interviews were conducted until sufficient variation and depth were achieved to allow an in-depth interpretive analysis of parenting in the context of hospitalisation at home.
Ethical Considerations
The study received approval from the Research Ethics Committee of the University of Strasbourg under the number Unistra/CER/2024-27. It was included in the register of data processing activities under reference number 5580, certifying its compliance.
Data Analysis
The data were analysed using Braun and Clarke’s six-phase reflexive thematic analysis process (Braun et al., 2019). This method was used to identify and interpret patterns of meaning within the data, in coherence with the epistemological assumptions of interpretive description.
First, the first author sought to develop familiarisation and immersion with the data after transcription. The transcripts were read and re-read by the first author to look for common patterns, and notes were completed on initial responses. Second, after reading the transcripts, the codes were generated manually in the margins. The third phase involved codes being reviewed and analysed by the first author using an Excel file to develop initial themes across the data. The construction of themes extends the active process of the previous phases. The fourth phase involved the development and review of themes by all authors. At this stage, we have developed thematic mapping to facilitate this process. During the fifth phase, the themes were reviewed and revised by all authors to ensure their internal and external consistency. We developed a clear sense of how each theme related to the others. We then assigned names to each theme. Finally, themes were converted into a report by all authors. In line with reflexive thematic analysis, themes are analytical constructs derived from the researcher’s creative work at the intersection of data, analytical process, and subjectivity.
The quality of a reflexive thematic analysis is based on the researcher’s thoughtful and reflexive engagement with their data and the analytical process (Braun & Clarke, 2019).
Thus, the reflexive thematic analysis aims to acknowledge the researcher’s active role in interpreting data. As an insider researcher, the first author kept a reflexive journal to record personal observations (Braun & Clarke, 2021). In addition, the first author was supervised by one experienced qualitative researcher (the last author). The use of reflexive thematic analysis involves constantly reflecting on and challenging the researcher’s assumptions about the data (Braun & Clarke, 2024). The research team met regularly to discuss enhancing understanding, interpretation and researcher reflexivity (Braun & Clarke, 2021; Nowell et al., 2017).
The description of the analysis process guarantees the quality of the research (Nowell et al., 2017). We deliberately selected a sample with varied ages and genders, including parents of children with different types of cancer (Guba & Lincoln, 1994). We also recognise that the researchers’ prior clinical experience in paediatric oncology influences and enriches the entire research process, which underscores the “researcher as instrument” viewpoint (Braun & Clarke, 2021). This study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong et al., 2007) to ensure quality and rigour.
Results
Presentation of Participants
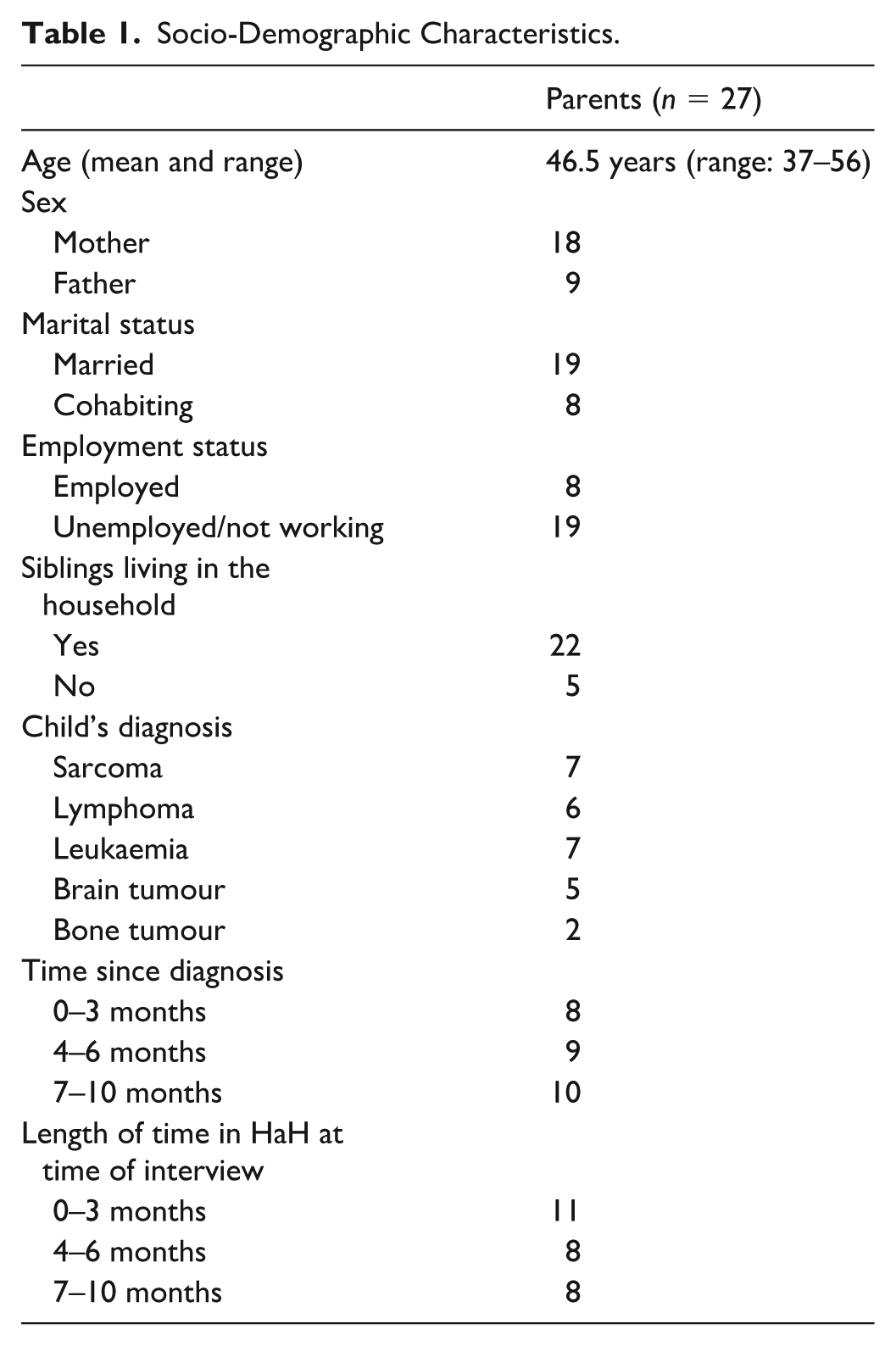
Twenty-seven participants (9 men and 18 women) were interviewed. In nine families, both parents wanted to participate. All other interviews were individual. Participants’ average age was 46.5 years (range = 37–56 years). The parents had a child with cancer hospitalised at home. The socio-demographic characteristics and type of illness of our sample are shown in Table 1.
Socio-Demographic Characteristics.
Reflexive Thematic Analysis
HaH required a reorganisation: it allowed the child with cancer to return to the family environment while accommodating cancer and care. This was not a simple transition, but a situation that required parents to actively renegotiate parenting by redefining their roles in order to maintain a certain degree of “normality” and to cope with the illness and medical equipment in the home. The analysis identified four central main themes that together structure parents’ experiences of parenting in the context of HaH that include (a) adapting to a new care dynamic; (b) sharing parenting with healthcare teams; (c) taking on multiple parental roles; and (d) developing parenting strategies. These themes were developed through an iterative analytic process that sought to clarify the hierarchical relationships between themes and subthemes, rather than to present them as isolated or equivalent categories. Each theme captures a distinct aspect of the parenting experience, while the subthemes specify how these experiences are enacted and negotiated in everyday family life. The themes are presented in a logical sequence that reflects how parents first encounter and adapt to home-based care, then position themselves in relation to healthcare teams, before taking on multiple parental roles and developing strategies to sustain parenting over time. This organisation aims to provide a coherent analytic narrative that reflects the progressive and interconnected nature of parenting in hospitalisation at home.
Table 2 shows how each theme was developed from organising subthemes within the data. These four themes reflect different analytical levels of parenting in HaH: the first two describe the contextual and relational conditions of parenting, while the latter two focus on how parenting is enacted through roles and sustained over time through strategies. More specifically, the first two themes refer to the contextual framework of parenting in HaH, shaped by the medicalisation of the home and by ongoing interactions with health care professionals, which together constitute the conditions within which parenting is reorganised. Parental roles refer to the functions parents assume and embody in everyday life, while strategies describe the ways parents regulate, sustain, and adapt these roles over time in order to cope with the cumulative demands of HaH.
Themes and Subthemes.
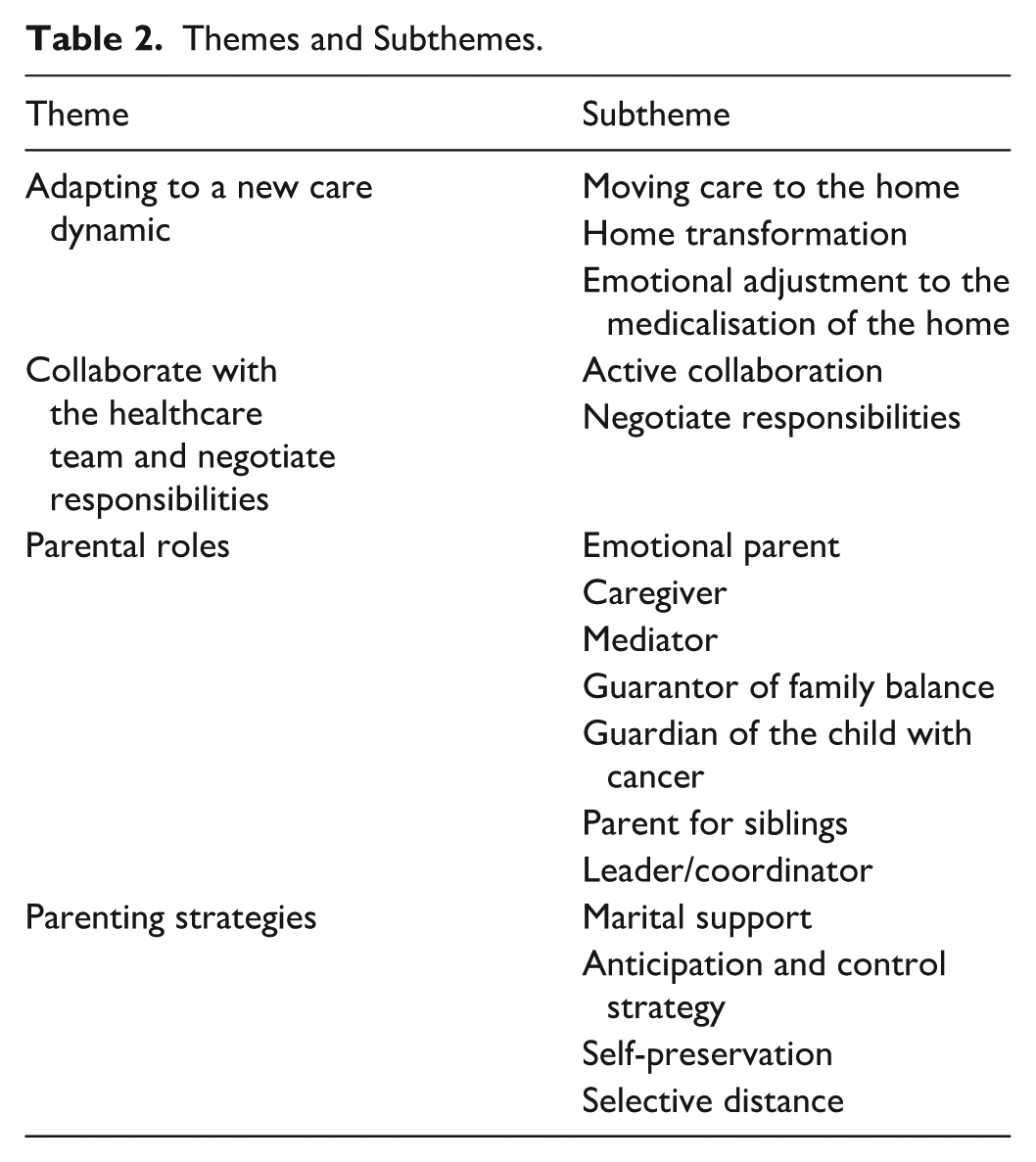
Figure 1 presents the structural organisation of parenting in the context of HaH as a dynamic and processual configuration. It illustrates how the contextual conditions of HaH – namely the medicalisation of the home and shared parenting with health care teams – constitute the framework within which multiple parental roles are enacted and sustained over time through the deployment of specific parenting strategies.
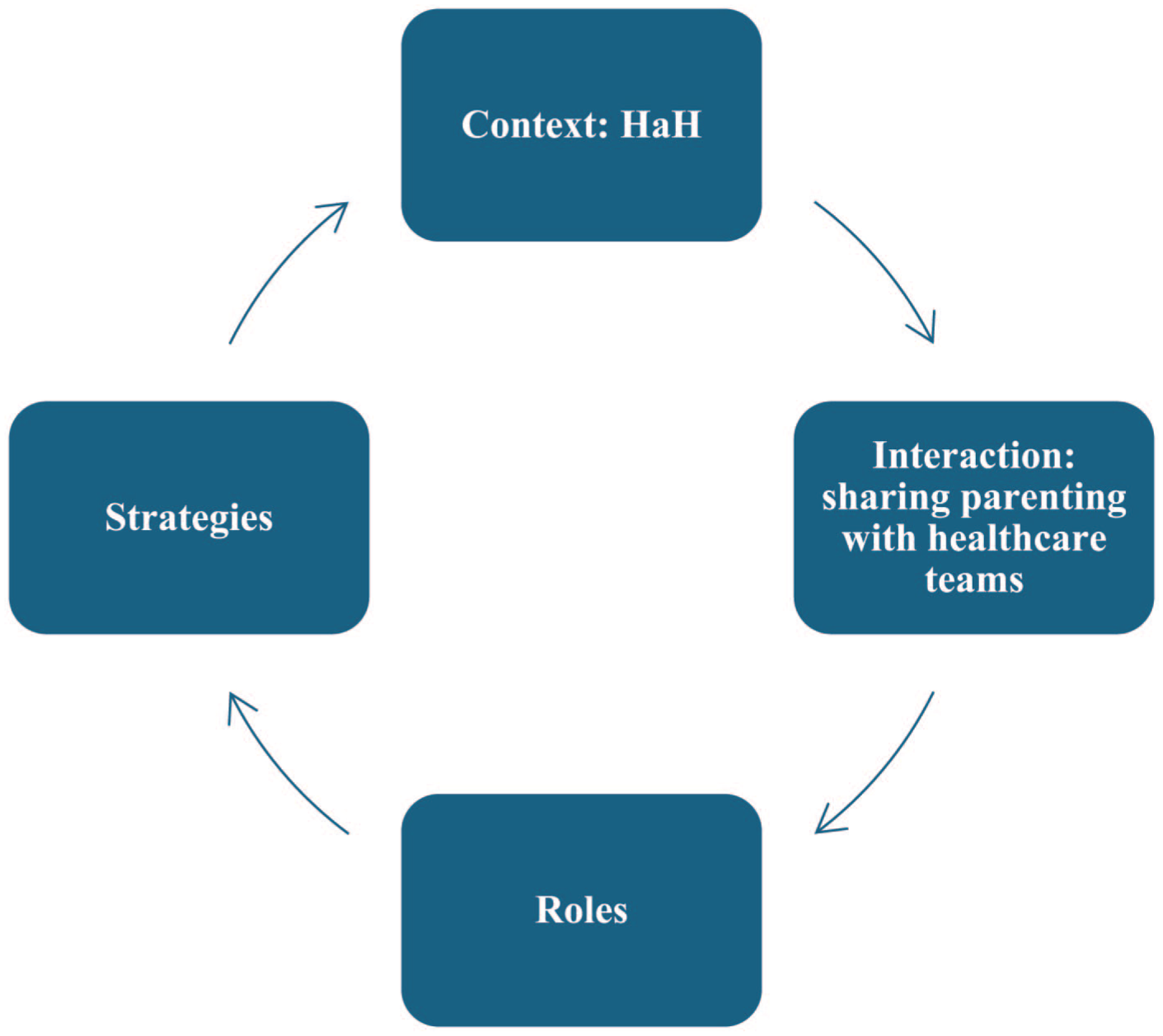
Parenting in HaH as a dynamic and processual configuration.
Adapting to a New Care Dynamic
What changes in daily life are the equipment and medicines that arrive at home. All these small changes add up and reveal the reality of the situation, and we have to adapt to all of that (mother, 38 years old).
We have to organise the room, for example, to make space and maintain hygiene. I have to dust every day (mother, 43).
As this mother explained, adapting to the new care dynamic required a reconfiguration of the living space, which the parents had to transform to accommodate the demands of care, while trying to preserve their family character. This process of adjustment, which is often invisible, led parents to question themselves: We had to rearrange everything in the house. The bedroom became almost like a hospital room, with IVs and equipment. But we tried to keep her things, her toys, so that she would still feel like it was her room (mother, 36).
There is some apprehension when you see these machines in your home, transforming your daily life and your living space. But you quickly get used to it, I would say, you get accustomed to it (father, 39).
This reorganisation forced parents to rapidly adjust to a daily routine punctuated by medical care, team interventions and technical protocols. The home thus became a hybrid space, both a place of everyday life and a place of care. This adjustment to home-based care was a gradual process, with parents eventually integrating the presence of care into their daily lives to the point where it became a new form of normality.
Collaborate With the Health Care Team
When the teams arrive, I let them get on with it and wait patiently for them to give my daughter the necessary treatment. I just stand there and watch (mother, 40).
This experience showed that collaborating with health care professionals sometimes required parents to accept taking a back seat during treatment, while remaining attentive and available for their child. Some parents managed to negotiate a balanced position during HaH: being there for their child without hindering the technical procedures.
I’m there at the beginning to provide a maternal and reassuring presence, and when I see that she’s comfortable with the nurse, I leave the room, but I don’t go very far, so that if they need me, I’m there (mother, 54).
This account underscored how important it was for this mother to be present at the beginning to reassure her child by providing emotional support, before gradually withdrawing when trust had been established between the child and the health care professional. The parent remained available but took a step back. Withdrawal does not mean giving up the parental role or relinquishing one’s place, but it does require subtle negotiation that recognises the competence of professionals while retaining parental responsibility by adjusting one’s presence and involvement. This cohabitation of roles required parents to be highly flexible in the way they exercised their authority, autonomy and availability in order to remain present without feeling dispossessed of their parenting.
Parental Roles
Returning home required parents to take on several roles, including maintaining emotional support for their child while simultaneously performing technical, relational and organisational tasks. These roles were not mutually exclusive: they coexisted and complemented each other, demanding constant adjustments as parents switched between roles depending on the situation and specific requirements.
We try to do normal things, watch a film, play cards, even if sometimes we have to stop for treatment. It’s important that he remains a child above all else, and as his mother, I have to give him that impression (mother, 39).
By protecting the child’s identity as a child, this mother was able to preserve her own identity as a parent. Love and reassurance were not secondary to care: they were the framework for it and structured parenting. Even when children had cancer, they remained children and needed their parents.
At first, changing the dressing was very difficult. I was afraid of doing it wrong, afraid of hurting him. But then, with the nurses’ explanations and after doing it several times, it became more natural. Now, it’s a moment when I can show him that I’m there for him, even in these small acts (father, 45).
This situation required parents to accept the idea that technical and medical care were now part of their role, just like feeding and protecting their child. Gradually, these medical procedures, initially perceived as alien, became part of their day-to-day routine and helped redefine their identity as parents.
When the team arrives, we give them an update. We tell them whether he’s eaten and slept or if he’s in pain anywhere. It’s important for them to know how he is really doing (mother, 38).
This mother, like most of the other parents, explained the importance of relaying all relevant information to the team. This communication role was essential to ensuring continuity and adaptation of homecare. The role of mediator demanded that parents be highly vigilant and observant while being constantly involved in order to ensure continuity of care in the absence of the teams. This function strengthened parents’ sense of responsibility and made their position more complex. They evolved into their child’s spokesperson.
I try to do everything I can to keep the house running as it did before . . . to keep things going, to keep it clean, so we can all have dinner together. That’s my way of maintaining normality (mother, 48).
This role as “guardian of normality” and family balance helped protect family life, supporting its cohesion and cushioning the intrusion of the illness and medical care.
I wake up during the night to check if my child is sleeping, if he’s okay, if he’s breathing normally. I did a lot during his illness when we were in hospital, and I’m still doing a lot now. I think we develop a kind of anxiety about looking after our child, who needs us even more. That’s it, we’re scared. I wake up at night to check on my child (mother, 51).
In common with other parents, this mother explained that she remained vigilant (waking up at night, checking her child’s breathing and regularly monitoring his condition), which kept her on high alert. This hypervigilance was based on repeated micro-decisions (getting up, checking and reassessing) aimed at detecting any worrying signs or health problems. The resulting anxiety was costly: sleep deprivation and constant tension. But the anxiety was also functional: it mobilised control and constant presence, which reassured the parents. The role of guardian was thus carefully balanced between the need to protect the child by remaining alert and the psychological and physical strain imposed by this constant vigilance.
We mustn’t forget that I also have another son, who is also a child and needs us. So, now that my daughter is at home, we can also spend time with my son and feel less guilty (father, 55).
Parents coped by dividing their attention and giving time to each child. Some parents set aside specific moments for siblings, while others try to include them in the medical routine in a reassuring manner. Yet all emphasised the burden of this dual requirement: supporting the sick child without making the others feel left out. This role, often overshadowed by medical emergencies, was nevertheless an essential pillar of family balance.
I’m the one who writes everything down: treatment times, when the nurses are due to visit, hospital appointments . . . I make sure everything runs smoothly and on time. And then there’s my son’s and daughter’s schoolwork to think about, helping them with their homework. Sometimes I feel like I’m the control tower of the house (mother, 47).
Taking on this “control tower” role not only helped bring consistency to a family life disrupted by illness but also prevented day-to-day life from falling into disarray. The role of coordinator ensured continuity and coordination between care, domestic life and everyone’s needs. But it also highlighted the organisational and mental burden that adds to the emotional and technical demands.
In the context of HaH, parenting referred to a mosaic of evolving and fragmented roles that were continuously adjusted over time, with parents evolving into true “orchestral conductors.” This plurality of roles, often invisible to professionals or those around them, demonstrated the complexity of parenthood, which also has its limits. It required parents to manage their own vulnerability by developing appropriate strategies.
Parenting Strategies
In contrast to parental roles, which refer to what parents do and what they represent, parenting strategies describe how they managed to persevere, adjust and cope over time. These strategies were developed across several areas, enabling parents to balance the emotional, organisational and medical burdens.
He knows when I can’t take it anymore, he takes over without me even saying anything. We’ve become complementary in what we do, we help each other, we support each other and we try to move forward (mother, 39).
Some parents spoke of “teamwork,” where each partner took on what the other was temporarily unable to do. This complementarity strengthened the sense of parental competence and helped preserve the couple’s cohesion.
I write everything down: medication, appointments, visiting hours. I set alarms on my mobile phone so I don’t forget anything. It reassures me; it makes me feel like I’m in control (father, 46).
This strategy reflected a need to control an uncertain environment. It helped reduce anxiety by organising daily life around a stable framework, and it helped parents feel empowered rather than overwhelmed.
When she’s asleep, I take five minutes to relax and drink a cup of coffee in silence. It may not seem like much, but without it, I wouldn’t be able to cope (mother, 41).
This strategy reflected the need to set aside time for recovery, however minimal, in order to maintain a presence for the child. It highlighted the fragile balance between giving everything and sustaining effort over time, revealing the importance of micro-resources in parenting in HaH.
When we had HaH, everyone wanted to come over, but we couldn’t. I had to say no to some people, otherwise my daughter would have been exhausted, and so would I (mother, 42). I try to put certain medical information out of my mind and not think about it. Otherwise, our minds become cluttered and we have no mental space left (father, 59).
This distancing was not an emotional withdrawal, but a way for parents to protect themselves from relational and emotional overload. By filtering what entered the home – words, presences or outside emotions – the parents built a kind of buffer zone that allowed them to maintain a certain amount of control and prevent the illness from spilling over into every aspect of family life.
I cry when he’s asleep. In front of him, you have to be there, strong (mother, 37). I can’t break down, because if I break down, things won’t work out. You have to hold on for him, for the others. Even when you can’t take it anymore (father, 47).
Although this internalised vulnerability sometimes manifested itself, it was often contained and controlled, as if acknowledging distress might threaten the parent’s own stability and the already-fragile stability of the family. In order to continue parenting, parents had to negotiate their distress. As a result, the home – which had become a place of care rather than a place for living – rarely allowed parents to have any space of their own. The absence of boundaries between the private and the medical made it more difficult to withdraw and take a step back.
Discussion
The aim of this study has been to explore how parents of children with cancer receiving homecare redefine parenting. The analysis has highlighted four central themes: (a) adapting to a new care dynamic; (b) sharing parenting with health care teams; (c) taking on multiple parental roles (emotional parent, caregiver, mediator, guarantor of family balance, guardian of the child with cancer, parent for siblings, and leader/coordinator); and (d) developing parenting strategies (marital support, anticipation and control strategy, self-preservation, selective distancing and negotiating personal distress). A central contribution of this study is to highlight the specific features of parenting within a formal hospitalisation at home (HaH) model, beyond home-based care in a more general sense. In HaH, the home becomes an institutionally organised site of care, structured by clinical protocols, scheduled professional interventions, and safety requirements, which parents must integrate into everyday family life. This hybridisation of the domestic space creates distinctive expectations for parents, who are required not only to provide care but also to coordinate with HaH teams, negotiate their presence during medical procedures, and ensure continuity between hospital-level care and family routines. By documenting these dynamics, our findings extend existing literature on parental caregiving in paediatric oncology by showing how HaH produces a specific configuration of parenting shaped by the continuous co-presence of institutional care within the home.
Our findings confirm that HaH is not limited to a simple transfer of care from hospital to home. It involves a profound transformation of the domestic space, which becomes a hybrid place where family intimacy and medical constraints overlap. Parents must rearrange this space, integrate medical equipment and devise new routines while seeking to preserve the familiar character of the home. This medicalisation of the private sphere has been described in other contexts, such as chronic paediatric illness (Knapp et al., 2010) or adult oncology (Auret et al., 2015), where care and support involve a profound reorganisation of daily life. However, our findings suggest that HaH forces parents to navigate simultaneously between family continuity and medical requirements, confirming the observations of the home as a “buffer zone” between normality and medical hospitality (Verberne et al., 2019). Our research also highlights that this adaptation is not merely logistical; it constitutes a genuine emotional endeavour, requiring individuals to come to terms with the daily visibility of the illness and medical equipment, which is described as an affective integration of the illness into the heart of family life (Kars et al., 2015). This dual nature of the space (both intimate and medicalised) not only transforms the physical environment but also creates a unique setting that distinguishes HaH from other forms of care, transforming the way parents parent.
Our study also shows that HaH is defined by cohabitation with health care teams and the relationship with health care professionals. Within the formal HaH model, collaboration with the health care team emerges as a central component of parenting, structured through active collaboration during care delivery and ongoing negotiation of responsibilities between parents and professionals within the home. This position is consistent with the findings of previous research on the co-construction of parental presence in care (Angelhoff et al., 2015; Kirakosyan et al., 2025), yet it underscores one specific feature: the repeated intrusion of carers into the home forces parents to constantly adjust their position so as not to feel deprived of their parental authority. Within the formal HaH model, collaboration with the health care team emerges as a central component of parenting, structured through active collaboration during care delivery and ongoing negotiation of responsibilities between parents and professionals within the home. This phenomenon is also observed in other contexts, such as among fathers of children with complex needs (Hobson & Noyes, 2011). However, HaH makes it particularly visible, as the boundary between the personal and the medical overlaps. Furthermore, the balance depends not only on mutual trust and recognition but also on the parents’ ability to adjust their presence and authority. This collaborative work does not imply a loss of parental responsibility but rather requires parents to continuously adjust their involvement, presence, and authority in response to professional interventions, highlighting collaboration as a situated and dynamic process specific to HaH.
These findings should also be interpreted in light of the specific characteristics of the French health care system and the organisation of hospitalisation at home. In France, HaH is embedded within a publicly regulated health care system, where care is predominantly financed by national health insurance and delivered through specialised, physician-led teams. This institutional framework shapes parents’ experiences by formalising expectations regarding safety, availability, and coordination of care within the home, while simultaneously reinforcing parents’ responsibility for day-to-day organisation and vigilance. In addition, cultural understandings of parenting in the French context, which strongly value parental presence, protection, and involvement in children’s care, may further intensify parents’ engagement in HaH. The combination of institutional regulation and culturally grounded expectations of parental responsibility provides a specific context within which parenting is reconfigured, and should be considered when interpreting the transferability of these findings to other health care systems or cultural settings.
One of the major contributions of this research is that it demonstrates the breadth and diversity of parental roles in an HaH context. This plurality has already been described in the literature on disability (Geuze et al., 2023) and paediatric diabetes (Nieuwesteeg et al., 2017), where parenting unfolds through technical, educational and emotional functions. Our study adds two major contributions. First, it highlights the role of the parent as the guarantor of family balance, aiming to maintain reference points and normality in the face of disorganisation. Second, our research identifies the role of pilot/coordinator, which centralises organisational and logistical responsibilities, making parents the true “control tower” of domestic and medical life. While the literature has already emphasised the concept of “extended parenthood” (Aasen et al., 2019) and the “dual identity” of parents who have become quasi-professionals, we go a stage further by showing that this identity is multiple, fragmented and constantly readjusted. Our findings confirm and extend the concept of “intensive parenting” (Woodgate et al., 2015), which is characterised by exhaustion, constant resource mobilisation, considerable cognitive and emotional strain and the permanent coexistence of family life and caregiving. The originality of HaH lies in the fact that these roles must coexist in the same space and at the same time, without the possibility of compartmentalisation. As a result, the burden of care increases greatly as responsibilities extend beyond the usual boundaries (Page et al., 2020). Our findings invite a wider understanding of parental roles in home hospitalisation, emphasising their orchestral nature: parents become true “conductors” of family and medical life.
Finally, the parenting strategies observed demonstrate creativity in terms of “holding out” over time. Mutual support between spouses (Li et al., 2018) and organisational anticipation (Hobson & Noyes, 2011) appear to be major resources. But our study also shows the importance of more discreet strategies: self-preservation through micro-spaces of respite; selective distancing by filtering out emotional and relational intrusions; and silent negotiation of distress, that is, privately managing one’s own vulnerability, which is essential in order not to undermine family stability. These results confirm the importance of intimate and invisible adjustments, which are often absent from more technical descriptions of parenting in a medical context. They highlight that HaH parenting is not only an organisational feat or a combination of roles, but also active daily work to regulate emotions, protect the child and safeguard the family. Recognising this specificity is essential in order to adapt support practices and assist these parents, who are the “conductors” of a family life transformed by illness.
Implications and Potential Future Research
The results of this study have several implications for clinical practice and research. Clinically, they highlight the importance of education, preparation, and sustained professional support for families who assume intensive care responsibilities in hospitalisation at home. Beyond recognising the complexity of parenting in this context, the findings emphasise the central role of nurses and other HaH professionals in preparing parents for home-based care. This preparation extends beyond technical training to include anticipatory guidance regarding organisational demands, emotional challenges, and the coordination required to manage multiple parental roles within the home. Professionals are also uniquely positioned to provide ongoing support, help parents adjust their involvement over time, and identify early signs of vulnerability, overload, or exhaustion – such as sleep disruption or anxious hypervigilance – allowing timely adaptation of support. Structured educational interventions, regular opportunities for dialogue, and explicit recognition of parents’ organisational and emotional labour may help sustain parenting capacities while preserving family balance in HaH.
Beyond clinical implications, these findings open avenues for future research. Longitudinal studies would enable examination of how parental roles and strategies evolve over time and across different phases of illness, including curative and palliative trajectories. Comparative research across care contexts (oncology, chronic illness, disability, and technological dependence) could further clarify which aspects of parenting experiences are specific to formal HaH arrangements and which reflect broader processes of caregiving at home. Finally, integrating mixed methods approaches – combining qualitative analyses with quantitative measures of parental burden, sleep, anxiety, and quality of life – would deepen understanding of how parents regulate and sustain their caregiving roles over time.
Limitations of the Study
This research has several limitations. First, the most vulnerable or least available families were probably underrepresented, which may introduce selection bias. The experiences of these families could reveal other facets of HaH parenting. Our sample consisted of French parents, and we were unable to survey other cultural contexts that might reveal cross-cultural differences. Second, the study was conducted in a specific context: HaH in paediatric oncology in France. The results cannot be directly generalised to other chronic conditions or other cultural or organisational contexts where home hospitalisation arrangements, resource availability or relationships with carers may differ. Furthermore, the research does not take into account the perspectives of all family members. It focuses on parents, yet the experiences of the sick children themselves and their siblings should also be studied in order to complement and add nuance to our understanding of parental dynamics.
Conclusion
Home hospitalisation transforms parenting into a demanding experience, where parents must integrate medical care into their private space and simultaneously preserve family continuity despite illness. Four themes structure this experience, which functions as an ongoing process: adapting to a new care dynamic; sharing parenting with health care teams; assuming multiple roles; and devising strategies for coping over time. Parents are no longer seen merely as carers, but as actors involved in the organisational, medical, emotional and symbolic aspects of parenting in HaH. They devote all their energy to maintaining family life in spite of the intrusion of homecare. Home health care condenses and intensifies parenting in the same space and time, revealing parental creativity, adaptability and vulnerability.
Footnotes
Acknowledgements
We would like to thank the Fondation Santé Service for funding our research. We thank the participating families and the teams from Fondation Santé Service and HAD des Vignes & des Rivières for their valuable contributions.
Ethical Considerations
The study received approval from the Research Ethics Committee of the University of Strasbourg under the number Unistra/CER/2024-27. It has been included in the register of processing activities with the reference number 5580, confirming its compliance.
Author Contributions
VK: conceptualisation, data curation, formal analysis, investigation, project administration, visualisation, writing (original draft). MP: conceptualisation, visualisation, writing (review and editing). CM: conceptualisation, visualisation, writing (review and editing). AM: conceptualisation, visualisation, writing (review and editing). BP: conceptualisation, visualisation, writing (review and editing). IC: conceptualisation, visualisation, writing (review and editing). Marie-Frédérique Bacqué: conceptualisation, formal analysis, visualisation, supervision, writing (review and editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Fondation Santé Service. No Grant Number is available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not available. Please contact the corresponding author.