
Abstract
To assess the moderating effect of family resilience on the relationship between adverse family living conditions and anxiety and depression among adolescents with special health care needs (ASHCN). We conducted a secondary analysis of data of 13,097 ASHCN (aged 10–17 years old) from the combined 2022 and 2023 National Survey of Children’s Health (NSCH), representing a total population of 8,069,879 ASHCN. Measures included demographics, parent-proxy-reported diagnosed anxiety and depression, functional difficulties, family structure, family resilience, and family living conditions. The data were analyzed using survey-weighted descriptive statistics and logistic regression models combined with marginal effects analysis. Family resilience mitigated the negative influence of a maximum of two cumulative adverse family living conditions on the likelihood of having parent-proxy-reported diagnosed depression among ASHCN. When looking at the effects of each separate family living condition, family resilience moderated the effect of household dysfunction and adverse childhood experiences on the likelihood of having parent-proxy-reported diagnosed depression. The study found no moderating effects of family resilience on the relationship between living conditions and the likelihood of having parent-proxy-reported diagnosed anxiety. Consideration of family resilience and living conditions among ASHCN intervenes to reduce the incidence of negative health outcomes like anxiety or depression among these vulnerable youth.
Keywords
Introduction
Over 8 million adolescents aged from 10 to 17 years in the United States have a chronic physical, developmental, behavioral, or emotional condition—or medical complexity—that requires health care services beyond what is typically needed (Child and Adolescent Health Measurement Initiative [CAHMI], 2019; McPherson et al., 1998). These adolescents represent a subset of children and youth with special health care needs (CYSHCN), a population that continues to grow by approximately 130,000 each year (Allshouse et al., 2018; Wisk & Sharma, 2025). Physical and psychological challenges associated with their conditions elevate the risk of mental and behavioral health issues, including depression and anxiety (Barker et al., 2019; Leyenaar et al., 2024). Most importantly, adolescents with special health care needs (ASHCN) are undergoing a critical developmental transition that increases their vulnerability to impaired mental health (Balocchini et al., 2013). Depression and anxiety are the most common mental health issues among ASCHN. According to a recent report, up to 62% of children and adolescents (age 5–17) were more likely to have a mental health disorder (Suryavanshi & Yang, 2016). Depression and anxiety can further compromise their physical and psychological well-being by decreasing life satisfaction and increasing perceived illness burden, which ultimately decreases quality of life (Kovács et al., 2025). Prior research has also linked depression and anxiety with poor treatment adherence, worsening disease conditions, and school absenteeism (Cobham et al., 2020). Over time, these mental health challenges may have cascading effects into adulthood, increasing the risk of cardiovascular disease, arthritis, and diabetes through biological mechanisms such as reduced heart rate variability, autonomic nervous system dysregulation, and elevated inflammatory responses (Morales-Muñoz et al., 2023). In severe cases, children with critical illness and pre-existing mental health conditions have been shown to have higher odds of death within one year after receiving critical care (Krawiec et al., 2024).
Among the diverse factors that might impact psychological and mental illness among ASHCN, the focus of this study is the impacts of social disadvantages imposed by adverse family living conditions, which is defined as nine family-level adversities, including caregiver unemployment, low educational attainment, food insecurity, poorly built environment, housing instability, household dysfunction adverse childhood experiences (ACEs), racism, poverty, and poor access to health care (Yang et al., 2023). Adverse family living conditions are conceptually aligned with the more widely known term social determinants of health (SDOH), defined as the non-medical factors that influence health outcomes (Centers for Disease Control and Prevention, 2024). In this paper, however, we use the term adverse family living conditions to emphasize how these broader conditions are experienced within the family context. Evidence shows that the adverse family living conditions are strongly associated with mental health and contribute to both the onset and progression of mental illnesses (Compton & Shim, 2015). These conditions capture broader social and structural disadvantages within families and are among the most important contributors to mental health outcomes, second only to genetic factors and access to health care services (Hood et al., 2016). Studies have shown that the impact of adverse family living conditions on child’s overall health appears to function in two ways: cumulatively across multiple conditions (Bauman et al., 2006), and individually through specific family circumstances, such as caregiver unemployment, limited education, food insecurity, poorly built environments, housing instability, household dysfunction, adverse childhood experiences (ACEs), racism, poverty, and poor access to health care, are associated with an increased risk of anxiety and depression among adolescents (Yang et al., 2023).
Previous research indicates that family resilience may mitigate the negative impact of adverse family living conditions, and SDOH, on mental health. Family resilience refers to a family’s ability to withstand and recover from crises by engaging in relational processes that promote adaptation as a functional unit (Walsh, 1996). It is cited as one of the most influential factors in children’s mental health outcomes (Brajša-Žganec et al., 2024; Ho et al., 2022). A resilient family is one in which members can successfully navigate adversity, maintain or restore effective functioning, and achieve positive growth even in challenging circumstances (Sabah et al., 2025; Walsh, 2021). Family resilience has been shown to promote better health outcomes for children with various special health care needs through coping and adaptation processes (Omoladun-Tijani & Vish, 2023). A recent scoping review highlighted that interventions empowering families show promise in building resilience and improving health outcomes in CYSHCN (Mardhiyah et al., 2022). This finding is supported by a meta-synthesis by Huang et al. (2022), which found that enhanced family resilience fosters growth, such as increased empathy, better understanding, and willingness to support others. Most importantly, enhanced family resilience was associated with better adjustment and potentially more favorable health outcomes for ASHCN (Cheng et al., 2024; Suwanwong & Raksat, 2025).
Despite the growing body of literature on the impact of SDOH and family living conditions on the mental health of children and adolescents, little is known about the role of family resilience in mitigating the effects of adverse family living conditions on anxiety and depression among ASHCN. Therefore, the aim of this study was to examine the effects of cumulative and individual adverse family living conditions on the likelihood of having parent-proxy-reported diagnosed anxiety and/or depression among ASHCN, with a particular focus on the moderating role of family resilience.
Methods
Data Source
We conducted a secondary analysis of combined data from the 2022 and 2023 National Survey of Children’s Health (NSCH), a publicly available, de-identified, nationally representative survey collected annually in the United States (CAHMI, 2019). Parents and primary caregivers of children and youth provided proxy reports for one randomly selected adolescent residing in their household. The selection of the analytical sample for this study included two steps. On the first step, children and youth with special health care needs (CYSHCN) were identified using the NSCH screener. It assessed whether adolescent met one or more of the following criteria: (a) need and use of prescription medication; (b) above-routine use of medical, mental health, or educational services; (c) presence of functional limitations; (d) need and use of specialized therapies; and (e) need and use of treatment or counseling for an emotional, behavioral, or developmental condition. These criteria were considered in addition to endorsement of a related physical, mental, behavioral, or other health condition expected to last at least 12 months (Black et al., 2024). On the second step, we selected adolescents of age from 10 to 17 years among the ASHCN, resulting in a final analytic sample of 13,097 adolescents, representing 8,069,879 of ASHCN in the U.S. This age group (10–17 years) was deliberately selected because this range captures early (10–14 years) and middle (15–17 years) adolescence (National Research Council and Institute of Medicine, 1999). This restriction also aligns with the NSCH survey structure, which uses different age-specific questionnaires across developmental stages. This research was determined exempt by the Institutional Review Board of the University of Tennessee, Knoxville.
Measures
Several measures were assessed, including demographic characteristics, family structure, residence, mental health outcomes, family resilience, adverse family living conditions, and functional difficulties, used to identify eligible ASHCN. Demographic characteristics such as age, sex, race and ethnicity, family structure, and residence were included as covariates. The mental health outcomes were parent-proxy-reported of diagnoses of depression and/or anxiety. Family resilience was examined as a moderator, and adverse family living conditions served as the primary predictor.
Functional difficulties were measured as the number of difficulties experienced from a list of 10 options, then these were grouped into four: no difficulties, one difficulty, two difficulties, and three or more difficulties (Black et al., 2024). Caregivers reported these difficulties in response to two questions: whether, during the past 12 months, the adolescents had frequent or chronic difficulty with breathing or other respiratory problems; eating or swallowing; digesting food (including stomach or intestinal problems, constipation, or diarrhea); or repeated or chronic physical pain (including headaches or other back or body pain). The second question asked whether the adolescent had serious difficulty concentrating, remembering, or making decisions; serious difficulty walking or climbing stairs; difficulty dressing or bathing; difficulty doing errands alone (such as visiting a doctor’s office or shopping); deafness or hearing problems; or blindness or vision problems even when wearing glasses.
Family structure was a covariate in this study to improve the precision of the effect of the variables of interest. Family structure was categorized into five groups: two parents currently married, two parents not currently married, single mother, single father, and other marital status. Family resilience was measured using the NSCH Family Resilience Index, which assesses the extent to which family members “talk together,” “work together,” “know they have strengths to draw on,” and “stay hopeful” when facing problems over the past 12 months. Families were considered resilient if respondents answered “most of the time” or “all of the time” for all 4 items; otherwise, they were classified as having poor resilience (CAHMI, 2019).
Residence was included as a covariate and categorized as metropolitan or non-metropolitan based on clarification provided in the NSCH dataset. Metropolitan residence indicates that the child lived in a country within a metropolitan statistical area, whereas non-metropolitan residence indicates that the child lived in a country outside a metropolitan statistical area (CAHMI, 2019).
Adverse family living conditions, a predictor in this study, included caregiver unemployment, low educational attainment, food insecurity, poorly built environment, housing instability, household dysfunction, adverse childhood experiences (ACEs), racism, poverty, and poor access to health care (Yang et al., 2023). Each condition was dummy-coded, with 1 indicating its presence and 0 indicating its absence. The composite adversity score was calculated as the sum of all conditions. The use of a cumulative adversity score was consistent with prior NSCH-based studies that used cumulative ACE/adversity measures (Bethell et al., 2014, 2017). Prior researchers have suggested that this approach demonstrates strong internal validity and has discriminative and predictive utility for mental health conditions.
Analytic Approach
Descriptive statistics were reported for each variable. Frequencies were unweighted, whereas percentages, mean values, and their standard errors were calculated using survey weights. Applying survey weights ensured that study estimates were representative of the general population of U.S. adolescents aged from 10 to 17 years. All statistical analyses were conducted using Stata (StataCorp, 2025).
Due to the large positive skew in the adversity score for family living conditions, this variable was transformed using the winsorization technique (Boudt et al., 2020); values above the 90th percentile were replaced with the value at the 90th percentile. As a result, the maximum value was reduced from 9 to 4.
The moderation effect of family resilience on the association between adverse family living conditions and the likelihood of having parent-proxy-reported diagnoses of depression and/or anxiety among ASHCN was estimated using two sets of models. In the first set, two survey-weighted logistic regression models were developed to estimate the effects of the cumulative adversity score and its interaction with family resilience on the odds of having parent-proxy-reported diagnosis of anxiety (Model 1) and depression (Model 2). In the second set, two survey-weighted logistic regression models examined the effects of each of the nine family living conditions and their interactions with family resilience on the likelihood of having a parent-proxy-reported diagnosis of anxiety (Model 3) and depression (Model 4).
Model fit was assessed using pseudo-R², and collinearity was evaluated using the mean Variance Inflation Factor (VIF). Statistically significant interactions were further examined using marginal effects analysis, which estimated the probabilities of having parent-proxy-reported diagnoses of anxiety and/or depression in families with high versus low resilience (Busenbark et al., 2022). For Models 1 and 2, due to the large number of categories (5 categories of cumulative adversity by 2 levels of family resilience), statistical significance of differences between probabilities was determined through visual inspection of 95% confidence intervals in bar plots, with non-overlapping confidence intervals indicating statistical significance. For Models 3 and 4, statistical significance was reported using pairwise comparisons of margins (Busenbark et al., 2022).
Results
Sample Demographics
Sample demographics and health characteristics are presented in Table 1. Among the 13,097 ASHCN, 49% were female, and the mean age was 14 years (SE = 0.04; range: 14–17). Racially and ethnically, 52% were non-Hispanic White, 14% were non-Hispanic Black, 23% were Hispanic, and 11% were of other ethnicities. Based on parent proxy reports, 45% of the adolescents were diagnosed with anxiety, 27% with depression. In addition, 64% of ASHCN had at least one functional difficulty. The most common family structure was living with two parents (58%), followed by being raised by a single mother (25%). The remaining adolescents lived in families with two parents, not currently married (i.e., cohabitating parents; 6%), single father (4%), or other relationship (6%). Among families, 21% reported no resilience. The most common adverse living conditions were poverty (55%), followed by a poorly built environment (48%), household dysfunction ACEs (27%), and housing insecurity (24%). Families reported between 0 and 4 adverse living conditions, with the mean cumulative adversity score of 2 (SE = 0.02). In terms of residence, 13% of adolescents resided in non-metropolitan areas.
Characteristics of the Sample (N= 13,097; Weighted Population Size = 8,069,879 of ASHCN).
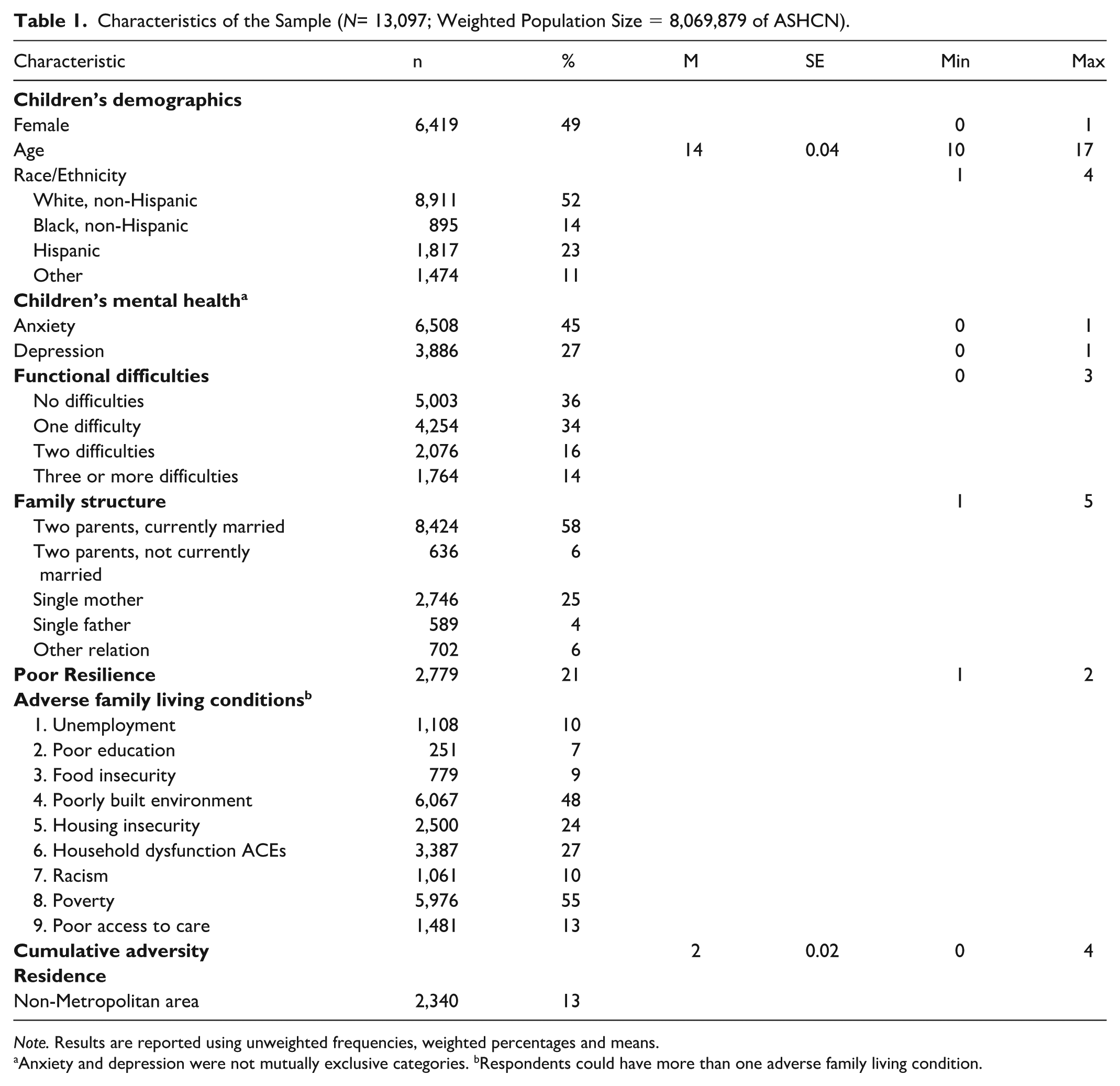
Note. Results are reported using unweighted frequencies, weighted percentages and means.
Anxiety and depression were not mutually exclusive categories. bRespondents could have more than one adverse family living condition.
Results of the regression analysis predicting the likelihood of a parent-proxy-reported diagnosis of anxiety among ASHCN are presented in Model 1 of Table 2. Compared to males, females were more likely to have parent-proxy-reported diagnosed anxiety (OR = 1.7, SE = 0.01, p < .001). Non-Hispanic Black, Hispanic, and adolescents of other ethnicities were less likely to have parent-proxy-reported diagnosed anxiety compared to non-Hispanic White adolescents (OR = 0.3, 0.6, and 0.6, respectively; SE = 0.1; p < .001). Adolescents with a parent-proxy-reported diagnosis of depression were more likely to report anxiety compared with those without depression (OR = 9.5, SE = 1.2, p < .001). An increase in the number of functional difficulties was associated with a higher odds of parent-proxy-reported diagnosis of anxiety, ranging from OR = 1.3 (SE = 0.1, p < .001) for adolescents with one difficulty to OR = 2.4 (SE = 2.8, p < .001) for those with three or more difficulties. Compared to adolescents living with two currently married parents, those living with two parents who were not currently married were less likely to report parent-proxy-reported diagnosed anxiety (OR = 0.6, SE = 0.1, p = .023). The interaction between cumulative adversity and poor family resilience on the likelihood of parent-proxy reported diagnosis of anxiety was not statistically significant (OR = 1.1, SE = 0.1, p = .526).
Regression Models Predicting Anxiety and Depression for the Cumulative Adversity Score (N= 13,097; Weighted Population Size = 8,069,879 of ASHCN).
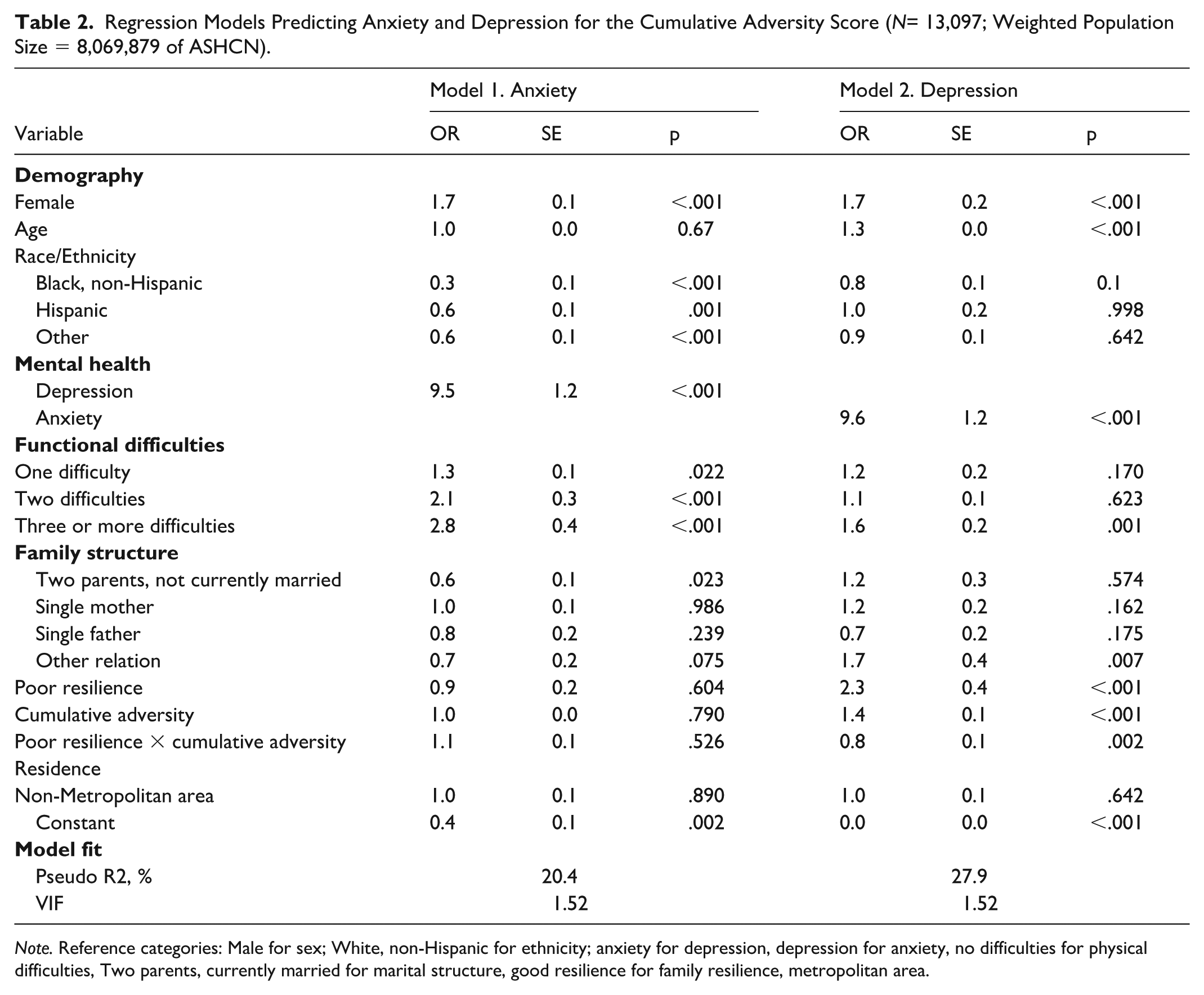
Note. Reference categories: Male for sex; White, non-Hispanic for ethnicity; anxiety for depression, depression for anxiety, no difficulties for physical difficulties, Two parents, currently married for marital structure, good resilience for family resilience, metropolitan area.
Results of the regression analysis predicting parent-proxy-reported diagnosis of depression in ASHCN are presented in Model 2 of Table 2. Compared to males, females were more likely to report parent-proxy-reported depression diagnosis (OR = 1.7, SE = 0.02, p < .001). Each 1-year increase in age was associated with a 30% increase in the odds of having parent-proxy-reported diagnosed depression (OR = 1.3, SE = 0, p < .001). Compared to those without anxiety, adolescents with anxiety were more likely to report parent-proxy-reported diagnosed depression (OR = 9.6, SE = 1.2, p < .001). Adolescents living in families with poor resilience were more likely to report parent-proxy-reported diagnosis of depression than their peers in families with good resilience (OR = 2.3, SE = 0.4, p < .001). Every additional adverse family living condition was associated with 40% increase in the odds of having a parent-proxy-reported diagnosis of depression (OR = 1.4, SE = 0.1, p < .001). The interaction between poor family resilience and cumulative adversity score was also statistically significant (OR = 0.8, SE = 0.1, p = .002).
The marginal effects of the interaction between poor family resilience and cumulative adversity in predicting parent-proxy-reported diagnosis of depression in ASHCN are presented in Figure 1. As the cumulative adversity increased from 0 to 2 conditions, adolescents in families with good resilience were consistently less likely to report parent-proxy-reported diagnosis of depression than those in families with poor resilience. Adolescents residing in families with no adverse living conditions and good resilience were two times less likely to report parent-proxy-reported diagnosed depression than similar children from families with poor resilience (Pr = .20, SE = 0.03 vs. Pr = .10, SE = 0.01; p < .001). Adolescents residing in families with one adverse living condition of any kind and good resilience were almost 2 times less likely to report parent-proxy-reported diagnosed depression than similar adolescents from families with poor resilience (Pr = .22, SE = 0.02 vs. Pr = .13, SE = 0.01; p < .001). Adolescents residing in families with two adverse living conditions and good family resilience were 1.3 times less likely to report parent-proxy-reported diagnosis of depression than similar adolescents from families with poor resilience (Pr = .24, SE = 0.02 vs. Pr = .18, SE = 0.01; p < .001). Families with three or more adverse living conditions, whether resilient or not, did not differentiate in probability of a parent-proxy-reported diagnosis of depression among ASHCN (as can be seen in Figure 1, the 95% confidence interval bars of estimates of probability of depression overlap after the cumulative score of 3).
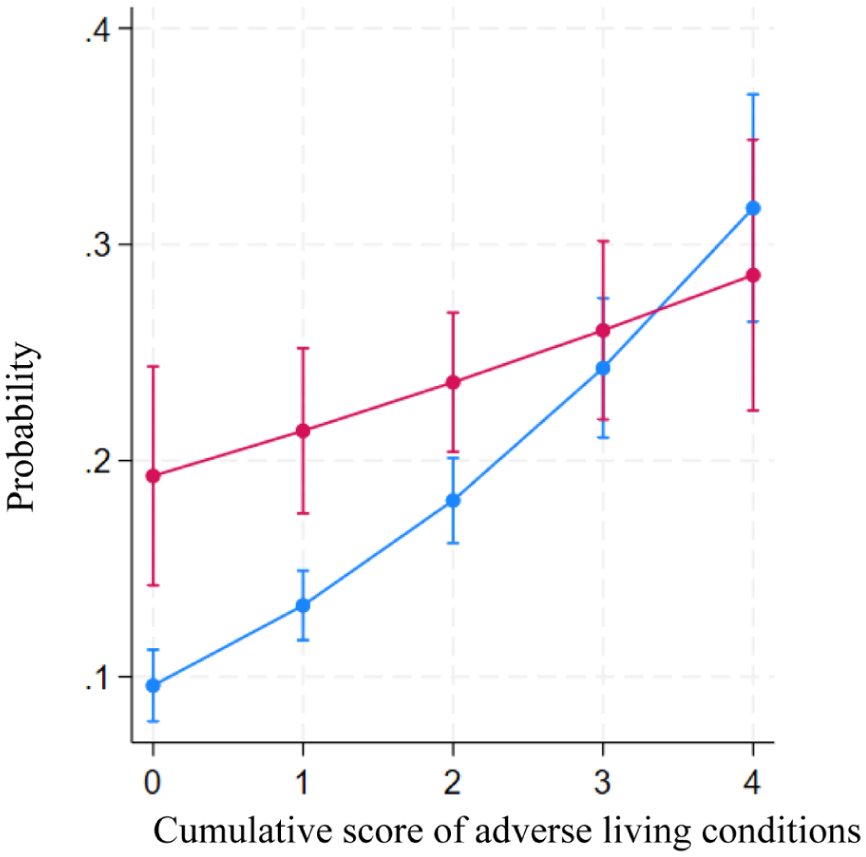
Marginal effects of interaction between cumulative adversity and family resilience in predicting depression.
Logistic regression model with interaction effects between poor family resilience and individual family living conditions on a parent-proxy-reported diagnosis of anxiety in ASHCN is presented in Model 3 of Table 3. Three adverse family living conditions had statistically significant effects on parent-proxy-reported diagnosed anxiety: poor education (OR = 0.28, SE = 0.09, p < .001), racism (OR = 1.47, SE = 0.26, p = .027), and poor access to care (OR = 1.66, SE = 0.31, p = .007). The interaction effects between poor family resilience and individual family adversities were not statistically significant.
Regression Models Predicting Anxiety and Depression for the Adverse Family Living Conditions (N= 13,097; Weighted Population Size = 8,069,879 of ASHCN).
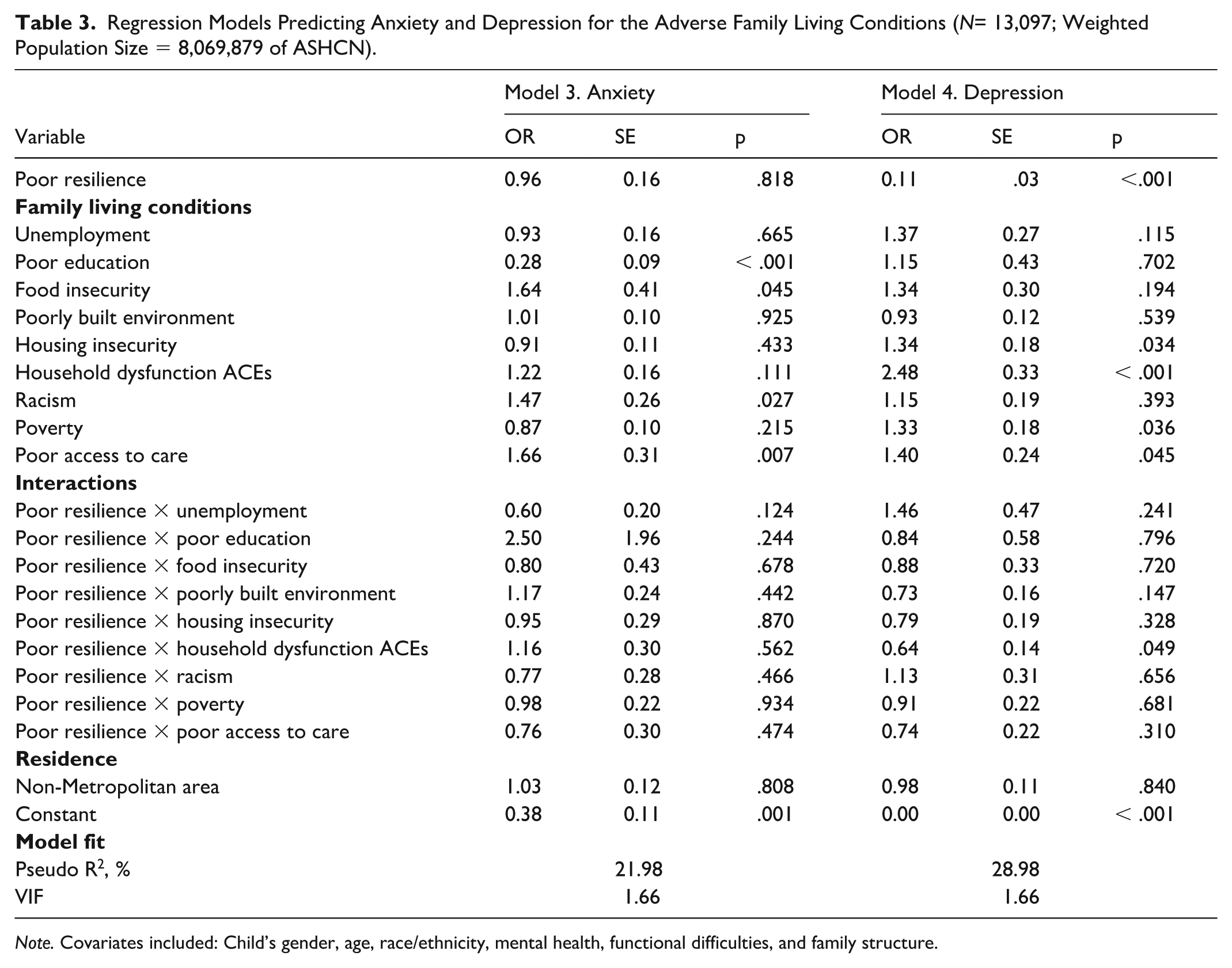
Note. Covariates included: Child’s gender, age, race/ethnicity, mental health, functional difficulties, and family structure.
Logistic regression model with interaction effects between poor family resilience and individual family living conditions on a parent-proxy-reported diagnosis of depression in ASHCN is presented in Model 4 of Table 3. Four family living conditions had statistically significant effects on parent-proxy-reported diagnosed depression: housing insecurity (OR = 1.34, SE = 0.18, p = .034), household dysfunction ACEs (OR = 2.48, SE = 0.33, p < .001), poverty (OR = 1.33, SE = 0.18, p = .036), and poor access to care (OR = 1.40, SE = 0.24, p = .045). The interaction between poor family resilience and household dysfunction ACEs had a statistically significant effect on a parent-proxy-reported diagnosis of depression (OR = 0.64, SE = 0.14, p = .049).
The marginal effects of the interaction between poor family resilience and household dysfunction ACEs on parent-proxy-reported diagnosed depression are presented in Figure 2. Adolescents in families without household dysfunction ACEs and with good family resilience were 1.3 times less likely to have a parent-proxy-reported diagnosis of depression than those in families with poor resilience (Pr = 0.22, SE = 0.01, p <.001 vs. Pr = 0.29, SE = 0.02, p <.001, respectively), with differences between these probabilities being statistically significant (difference in means = .06, SE = 0.018, p < 0.001).
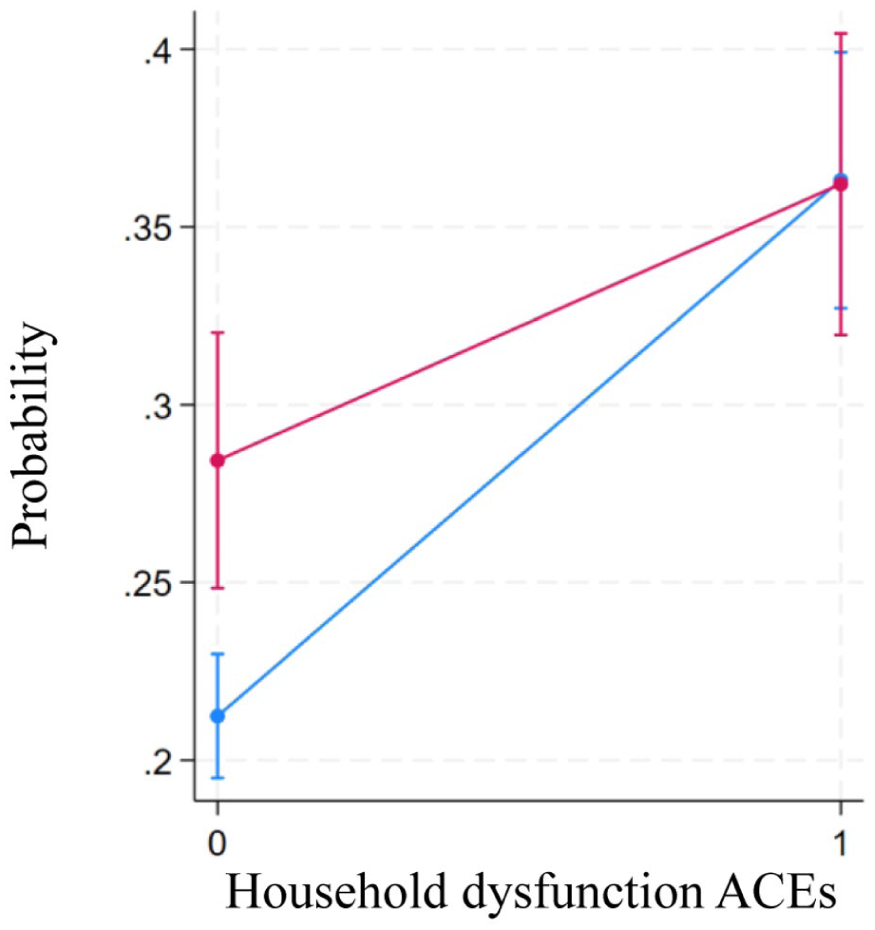
Marginal effects of interactions between household dysfunction, ACEs, and family resilience in predicting depression.
Families with household dysfunction ACEs, whether resilient or not, did not differentiate in probabilities of having a ASHCN with parent-proxy-reported diagnosed depression (Pr = 0.35, SE = 0.02, p <.001 vs. Pr = 0.36, SE = 0.02, p <.001, respectively), with differences between these probabilities being not statistically significant (difference in probabilities = 0.01, SE = 0.03, p = .785).
Discussion
This study aimed to examine the association between adverse family living conditions and parent-proxy-reported diagnoses of anxiety and/or depression among ASHCN, with particular attention to whether family resilience moderated these associations. The adverse family living conditions included: caregiver unemployment, low caregiver education, food insecurity, poorly built neighborhood environment, housing insecurity, household dysfunction, ACEs, experienced racism, poverty, and poor access to health care. Their effects on parent-proxy-reported diagnoses of anxiety and depression were analyzed both cumulatively (as a total score of all nine conditions) and individually for each condition. Strong associations were observed between adverse family living conditions and both parent-proxy-reported diagnoses of anxiety and depression. Our findings revealed strong associations between adverse family living conditions and both conditions. However, family resilience moderated these relationships only for parent-proxy-reported diagnosed depression, not for anxiety.
The present study found that, among the nine adverse family living conditions examined, poverty and a poorly built neighborhood environment were the most prevalent, each affecting approximately one in two ASHCN. These findings align closely with those of Yang et al. (2023), who reported similar patterns in a general population sample of U.S. adolescents. Interestingly, compared to caregivers in the general population of adolescents, caregivers of ASHCN were less likely to have poor education (12.6% vs. 7%), as parents with better education and socioeconomic status may be at an advantage for identifying children or adolescents as having elevated service needs (Black et al., 2024). However, compared to the general population of adolescents (Yang et al., 2023), families of ASHCN were more likely to experience housing insecurity (13.7% vs. 24% in our study), food insecurity (4.9% vs. 9%), and household dysfunction ACEs (19.4% vs. 27%), while less likely to have poor access to health care (38.2% and 13%). These findings indicate that parents and primary caregivers of children with special health care needs continue suffering from burdens of providing care, stemming from large out-of-pocket costs, necessity for the family member to stop working, cut back on work to care for their child, require additional income for medical expenses, or facing the need to relocate to be closer to the treatment center and family support (see Fluchel et al., 2014; Kuo et al., 2011). Future research is needed to examine the impact of a broader set of ecological living conditions, such as water and air quality—which were not examined in this study—on the mental health of ASHCN.
This study also found a statistically significant association between cumulative adversity and a parent-proxy-reported diagnosis of depression. Each additional adverse living condition was associated with a 40% increase in the odds of depression among ASHCN. Although this finding aligns with previous research demonstrating the gradient effects of cumulative social disadvantage on children’s physical and mental health (Keilow et al., 2020; Moore et al., 2025), it is the first to provide a specific estimate of this effect. It is exacerbated by the fact that families living in disadvantaged communities rarely experience a single hardship; rather, they commonly face multiple, interconnected challenges—such as poverty, housing and food insecurity, racism, and unemployment—which together contribute to chronic stress and limited access to resources (see Peverill et al., 2021). While this study offers a general estimate of the effect, future research should examine how it varies geographically, particularly across regions with differing welfare policies and histories of poverty. It may be hypothesized that the impact of adverse family living conditions on the mental health of ASHCN is more pronounced in some Southern communities with persistent poverty, socioeconomic disadvantages, and limited access to health care.
This study also found that family resilience moderated the association between cumulative adversity and the likelihood of a parent-proxy-reported diagnosis of depression. Specifically, among families with strong resilience and no more than two adverse family living conditions, ASHCN were up to twice less likely to develop a parent-proxy-reported diagnosis of depression compared to similar families with low resilience. Family resilience is characterized by hope, positive communication, and collaborative decision-making aimed at building a better future (Walsh, 1996). These qualities may provide a protective effect against common symptoms of depression—such as hopelessness, guilt, loss of optimism, social withdrawal, and diminished interest in daily activities—by fostering emotional support and coping strategies (Brajša-Žganec et al., 2024; Li et al., 2026). Another explanation is that resilient families often engage in “benefit finding,” a process of identifying positive changes or advantages that emerge from adversity (Lechner, 2021). This cognitive adaptation involves positive reinterpretation and meaning-making, which can buffer stress and promote psychological well-being (Tennen & Affleck, 2002). However, when families faced more than two adverse conditions, resilience alone was insufficient to counteract the cumulative negative impact. Interestingly, the average number of adverse family living conditions in this study was two, which suggests that family resilience may be able to buffer the impact of only up to a certain threshold of adversity on depression among ASHCN. This finding highlights the continued importance of maintaining health policies and community-based programs that directly reduce adverse family living conditions (Kirkbride et al., 2024). Emerging changes in federal programs- such as proposed adjustments to Medicaid, housing assistance, and welfare support-may reduce the resources available to families facing multiple adversities. Continued monitoring of these policy shifts is essential, given their potential implications for the family health and well-being of ASHCN.
When examining the individual effects of adverse living conditions, this study found that among the other living conditions, poor access to health care was the only factor consistently associated with parent-proxy-reported diagnoses of anxiety and depression. This finding is not surprising and well-documented elsewhere (see Black et al., 2024). Interestingly, two factors—parental unemployment and poorly built neighborhood environments—were not associated with parent-proxy-reported diagnoses of anxiety or depression among ASHCN, contradicting existing literature (see Butler et al., 2012). This discrepancy may stem from the fact that unemployment status in this study was measured as current status, at the time of the survey; as a result, it may not have become a serious issue that may impact adolescents’ mental health and well-being. The lack of impact of poorly built neighborhood environments may suggest that the impact of poor neighborhood quality may be less pronounced for ASHCN, as their health limitations often reduce exposure to the neighborhood environment. This study also found that other conditions showed complementary effects on anxiety and depression, reflecting differences in the nature of living conditions and the mechanisms of development of anxiety or depression. The anxiety was associated with food insecurity and racism—stressors that tend to occur episodically and create feelings of uncertainty and threat (Paulus & Stein, 2006). For instance, families relying on welfare support may have adequate food early in the month but face shortages later. Racism, often experienced through discrete events, can trigger acute anxiety responses (Williams et al., 2018). In contrast, the most significant contributors to depression were household dysfunction, ACEs, housing insecurity, and poverty. These conditions are persistent and chronic, fostering long-term feelings of hopelessness and entrapment, which are the defining characteristics of depression (Brajša-Žganec et al., 2024). Despite these findings, more research is needed to understand how parents’ low educational attainment may affect anxiety in ASHCN.
Interestingly, among all measured conditions, family resilience moderated the effect only of household dysfunction ACE. Household dysfunction ACE—such as parental conflict, substance abuse, or inconsistent caregiving—is an internal, relational stressor that directly affects family dynamics. Family resilience, which includes positive communication, collaborative problem-solving, and emotional support, is specifically designed to counteract these relational disruptions (Brajša-Žganec et al., 2024; Li et al., 2026). When families practice resilience strategies, they can maintain stability and emotional security despite internal challenges, reducing the psychological impact on children. In contrast, other adverse conditions—like poverty, housing insecurity, or racism—are external, structural stressors beyond the family’s immediate control. While resilience helps families cope emotionally, it cannot fully offset the material deprivation or systemic discrimination that drives chronic stress. Therefore, resilience shows its strongest moderating effect where families have agency to adapt and reorganize internally, as in household dysfunction.
Strength and Limitations
Overall, this study has several strengths. First, we utilized a comprehensive list of nine conditions, which were conceptually justified using the comprehensive framework of Social Determinants of Mental Health (Compton & Shim, 2015). This approach allowed us to consider the comprehensive cumulative effect of not only economic but also social, environmental, and behavioral risks. A cumulative scoring approach of the adverse family living condition into a single index score can be highly predictive of negative impacts on a child’s mental condition; however, this approach might fail to differentiate the more harmful exposures from the less dangerous ones (Bossert et al., 2024; Xiao et al., 2023). Another strength is the use of nationally representative data, enhancing the generalizability of the study findings and presenting both the sum of adverse family living conditions and a dimensional approach. Most importantly, this study examined family resilience as a moderator, which provides insights for developing targeted interventions. Although the contribution of family living conditions to health outcomes is well established and recognized as the most modifiable set of targets of interventions (Kirkbride et al., 2024), addressing those factors through clinical interventions can be challenging (Astorino et al., 2024). Therefore, it is necessary to identify the moderators that can buffer the effects of adverse family living conditions on mental health outcomes, particularly depression and anxiety among ASHCN.
Limitations of this study that warrant further discussion should not be overlooked. First, the family resilience index comprises four items and may not represent the total capacity of the family unit’s resilience. Although this measure has been commonly used in the literature, alluding to its conceptual validity. Regarding mental health symptoms, the presence of depression or anxiety was identified using parent-proxy responses to the NSCH, meaning misdiagnosed or undiagnosed psychiatric symptoms could impact results. Due to recall bias or social desirability bias, caregiver-reported data may not accurately determine the prevalence of depression, anxiety, or family resilience. At the same time, it is a recognized methodological limitation of large population surveys. Furthermore, the lack of diagnostic codes or detailed descriptions of mental health conditions means it is not possible to distinguish depressive or anxious symptoms that are reactionary or appropriate to significant environmental stressors from sustained psychiatric illnesses, such as major depressive disorder or generalized anxiety disorder.
Clinical Implications
This study showed that family resilience plays an important role in preventing the occurrence of depression and anxiety among ASHCN, emphasizing the critical role of family in managing mental health well-being. Based on our findings, health care providers should regularly assess the level of family resilience among families of ASHCN at clinical visits, particularly among those who are at elevated risk for the development of depression and anxiety. Furthermore, family resilience interventions should be considered as part of clinical practice. In general, family resilience interventions aim to enhance families’ coping and recovery in the face of adversity by strengthening their existing strengths and resources (Walsh, 2012). Several programs have demonstrated success among families of children with chronic illnesses and those exposed to trauma, such as military families. For instance, the Integrated Family and Systemic Treatment (I-FAST) Program (Lee et al., 2009) has been shown to reduce the negative impact of chronic illness on children’s behavioral problems and to improve overall family functioning and developmental capacity. The FOCUS Family Resilience Program (Saltzman, 2016) emphasizes open and effective communication to counteract family misattributions and estrangement, helping members develop a shared understanding of their experiences and enhance resilience and adjustment after trauma. Similarly, the Australian Child Illness and Resilience Program (CHiRP; Hamall et al., 2014) successfully strengthened family and social support. Collectively, these interventions have proven both practical and adaptable across various settings, including community and clinical environments, requiring relatively minimal resources to implement. Health care providers should proactively adopt family resilience programs to help prevent depression and anxiety among individuals at elevated risk and promote long-term psychological well-being.
Research Implications
Improving mental health among ASHCN is crucial. Although this study observed the influence of adverse family living conditions on parent-proxy-reported diagnoses of depression and anxiety among ASHCN, the findings of this study related to the limited buffering role of family resilience in the incidence of depression or anxiety raise a variety of intriguing questions for future study. For instance, while we observed a significant negative impact of cumulative adverse living conditions on a parent-proxy-reported diagnosis of depression, this association was not evident for anxiety. Moreover, several specific indicators showed no measurable effects. Future studies employing longitudinal designs are warranted to move beyond descriptive analyses and enable stronger cause-and-effect assessments, thereby clarifying the underlying mechanisms linking adverse family living conditions to the incidence of depression and anxiety among ASHCN.
In addition, the buffering role of family resilience observed in this study underscores the importance of examining broader contextual factors, including community, local, and state-level policies. Research in this area should incorporate the influence of social drivers of health across multiple levels (i.e., individual, family, community, health care system, and government/policy) to comprehensively identify factors shaping mental health outcomes and family living conditions (Kirkbride et al., 2024). Specifically, researchers can explore how family resilience interacts with broader structural and community factors, such as access to resources, neighborhood safety, and policy supports, to better understand what conditions family resilience effectively protects against poor mental health outcomes. Future national surveys of children’s health should also integrate community-engaged input from ASHCN to ensure that key survey items reflect their lived experiences. Such efforts will help build the evidence base needed to inform the design and pilot testing of interventions that can enhance mental health care for this population.
Conclusion
This study identified the buffering role of family resilience in reducing the development of depression or anxiety among ASHCN. Given the importance of family resilience, assessing its level among families of ASHCN and implementing interventions to strengthen it are warranted. Furthermore, future longitudinal studies incorporating a wider range of variables at multiple socioecological levels are needed to better understand effective strategies to mitigate the impact of poor living conditions on mental health outcomes among ASHCN.
Footnotes
Acknowledgements
This study is based on secondary analysis of existing data. The authors thank the organizations and individuals involved in collecting and providing access to these data. We also thank Dr. Jeremy Mills at the University of Tennessee, Knoxville, for his valuable expertise in adolescent mental health.
Ethical Considerations
This study was a secondary analysis of publicly available, de-identified national data and was exempt from IRB review.
Consent to Participate
Informed consent was not required for this secondary analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The data underlying this article are available in the Child and Adolescent Health Measurement Initiative’s Data Resource Center for Child and Adolescent Health (National Survey of Children’s Health, NSCH), at https://www.childhealthdata.org. The datasets were derived from sources in the public domain: the National Survey of Children’s Health (NSCH) public-use data files provided by the U.S. Census Bureau and the Health Resources and Services Administration’s Maternal and Child Health Bureau (https://www.census.gov/programs-surveys/nsch.html; ![]() .
.