
Abstract
This study addresses the national clinical trial recruitment crisis by chronicling the development of a campaign to move people toward enrollment in an online clinical research registry. The public typically encounters clinical trial information in controversies or study-specific recruitment ads, which limits full understanding. Ten focus groups were conducted with healthy and impaired persons to identify perceived benefits and barriers to participation. Altruism and self-efficacy emerged as key motivators. Three theoretically informed campaigns were developed and tested. Resulting materials have been shared with members of a National Institutes of Health–funded national consortium to improve the way biomedical research is conducted across the country.
Introduction
In summer 2011, Francis S. Collins, the director of the National Institutes of Health (NIH), summarized the precarious state of clinical research in the United States: “Despite great progress, many difficulties remain—difficulties that can delay or even thwart efforts to move scientific discoveries from the lab to the medical clinic.” Collins went on to identify low levels of clinical trial participation by both healthy and impaired Americans as one of the most significant challenges facing the enterprise.
Clinical trials are considered the gold standard for assessing the effectiveness of a new drug, medical device, diagnostic product, or treatment procedure on humans (NIH, 2007). Funding for clinical research comes from federal government organizations such as the NIH and the Department of Veterans Affairs or from private industry such as pharmaceutical and biotech companies, medical institutions, and foundations. Because trials are designed to minimize bias and increase precision to interpret research findings, they require very large sample sizes—often from numerous clinical sites across multiple countries. Without an adequate supply of research participants, clinical research is compromised.
Clinical trial recruitment is in a state of crisis. Fifty percent of clinical research sites enroll one or no patients in their studies (Pierre, 2006). According to Beasley (2006), clinical trials last 30% to 42% longer than expected because of recruitment delays that result in an average of 4.6 months lost per trial, or an annual cumulative loss of 26 years, on average, for each company. Due in large part to research participant shortages, the average cost of clinical trials has risen to nearly 60% of total development costs, as compared to just over 30% in the 1980s (Center for Information and Study on Clinical Research Participation [CISCRP], 2012).
Two important factors influence low participation rates, particularly among healthy volunteers: (a) a lack of overall knowledge about the clinical research enterprise and (b) mistrust of clinical research. According to the CISCRP (2012), 94% of the public recognize that participation in clinical research is very important to advance medical science, yet 74% say they have no “real” knowledge of the clinical research process, and 98% do not know where or how to identify appropriate clinical studies (CenterWatch, 2008). At present, study-based recruitment messages comprise the majority of communication about clinical research, and there is limited educational information about the why or how of participation. Outside of specific trial recruitment initiatives, the public’s only other exposure to clinical research often comes from sensational television dramas or controversies well publicized in the news (Getz, 2008). In sum, there is a need for general education about the clinical research process, including the risks, benefits, and rights of participants.
This study reports on the development of an evidence-based social marketing campaign to increase awareness of, and inclination to participate in, clinical research in North Carolina. The study was funded by the North Carolina Institute for Clinical and Translational Research. Although recruitment into clinical trials is struggling nationally, North Carolina faces unique challenges because more than 50% of residents live in rural areas with limited access to clinical research networks and infrastructure (Carpenter et al., 2012; Feldmann et al., 2008). This article focuses on the formative research, development, and pretesting of a branded website, an online registry, and promotional materials. Research findings and campaign materials have been shared with members of an NIH-funded national consortium to improve the way biomedical research is conducted across the country.
Background
The Knowledge Challenge
In 1947, David Rapaport pondered the future of research in clinical psychology and psychiatry and noted the importance of informing the public about the “why” of clinical research. More than 60 years later, a review of the literature reveals limited public education efforts that are not study specific but rather address the broader benefits of clinical research.
Consumer behavior and health communication research suggests that people progress through stages as they approach deciding whether or not to undertake a certain behavior. Furthermore, people respond to different motivators and require different types of communication at each stage of the process (e.g., Armstrong & Kotler, 2013; Prochaska, Redding, & Evers, 2008). With regard to clinical research, communication must move the general public from awareness to education to interest to participation. Such efforts are crucial to the long-term success of clinical research, which currently “faces a crisis” amid low awareness, limited understanding, and mistrust (Getz, 2008).
Engaging the general public is important for two reasons. First, clinical research depends on the involvement of healthy participants, as well as patients currently experiencing the health condition under study. As a result, healthy participants must be engaged and motivated to actively seek out opportunities to participate in clinical trials for conditions from which they personally may not suffer. Yet research suggests that the public may want to avoid discussions about diseases, such as cancer, unless they relate to someone about whom they care (Collyar, 2000). Second, patients with the condition under study are also needed for the success of clinical research. Yet they are often approached to enroll in a study when they are already under stress due to illness. This may not be the ideal time for education about the benefits, risks, and process of clinical research, especially because at present, much of that information is provided in a long, highly technical informed consent document. Thus, engagement with information about clinical research prior to invitations to participate in studies may increase interest in participation for healthy people and impaired patients alike. Comis, Miller, Aldige, Krebs, and Stoval (2003) note that the ability to recruit for future trials will depend, in part, on understanding and responding to adults’ attitudes toward participation in clinical trials as a whole.
Because most communication about clinical research is study based (e.g., Chan, Guttormson, Tracy, & Bremmer, 2009; Villarruel, Jemmott, Jemmott, & Eakin, 2006), the typical adult first encounters information about an individual study independent of context about clinical research in general. The absence of this education component may limit the effectiveness of recruitment efforts. Simmons (2008) points out that the first critical step in building public trust related to clinical research is providing public education that addresses the broader benefits of clinical research. Simmons suggests that an understanding of the benefits of clinical research needs to be embraced by all stakeholders in clinical research and health care.
Mistrust of the Clinical Research Enterprise
A second barrier to clinical research enrollment lies in the cloud of suspicion that surrounds clinical research. Trust in clinical research has eroded steadily in the past decade due to well-publicized controversies, including media coverage of volunteer reactions that resulted in harm or death, court cases of data falsification and failure to disclose safety information, public challenges of pharmaceutical and biotechnology companies for submitting fraudulent safety data or manipulating study results, and physician conflicts of interest (Getz, 2008). Mistrust is even higher among minority groups such as Blacks and Hispanics (M. Brown & Moyer, 2010; Langford, Resnicow, & An, 2010).
Mass communication research has established that the amount and content of news coverage affects participation in clinical trials. For example, Pentz et al. (2002) found that positive media coverage about the launch of a Phase 1 clinical trial for Endostain motivated respondents to contact their physician about participating in the trial. Len-Rios and Qiu (2007), however, found that negative stories about clinical trials received more prominent coverage than did positive stories and that greater exposure to such negative news stories about clinical trials resulted in lower intentions to participate. Positive stories were defined as those having “a favorable outcome or desired condition” (e.g., a drug or medicine received Food and Drug Administration approval or a treatment proven effective; p. 31). Conversely, negative stories featured negative outcomes or unfavorable conditions (e.g., problems with clinical trials, side effects, and patient complaints). Getz (2008) concludes that an abundance of negative media coverage about the clinical research enterprise needs to be mitigated by more counterinformation about the benefits of clinical research to both the individual and society.
National Education Efforts
A few national organizations have recognized and responded to the lack of public education information. The notion is that education may have a priming effect, helping create a favorable predisposition toward participation in clinical studies before the enrollment “ask” occurs. In 2004, the NIH launched a Public Trust initiative to ensure the public’s access to, and understanding of, the operations and outcomes of biomedical research and the role that the public plays in participating in and funding such research (Kaeser & Maddox, 2008). One aspect of this initiative was the Partners in Research program to engage scientists, community leaders, advocacy groups, and the public in partnerships to increase understanding of research among community members (U.S. Department of Health and Human Services, 2007).
The CISCRP spearheaded the development of a 2008 national pro bono media campaign. Titled Medical Heroes, the campaign underscored the contributions of ordinary people to finding cures for disease and advancing medical science. The CISCRP saw a 30% improvement in monthly clinical trial subject enrollment when it ran its Medical Heroes campaign concurrent with study-specific ads in select markets (Getz, 2008).
At the same time, a more geographically targeted ad campaign may be more effective than a national campaign sponsored by a national organization, particularly if the sponsoring organization is a trusted resource. Targeting involves developing messages with a specific population segment in mind (Noar, Benac, & Harris, 2007). Many health communication campaigns take a targeted approach, which divides the market into unique segments and then aligns messaging more saliently with targeted segments (Grunig, 1989). The more relevant a message is to the target audience, the more effective the campaign (Kreuter & Wray, 2003). Geography has been established as a key segmentation variable over the years (Armstrong & Kotler, 2013). Therefore, a geographically targeted, branded campaign that provides positive counterinformation about the benefits of clinical research may be more likely to resonate with the target audience before they, or someone they care about, face a personal medical crisis. Ad placement funding may also be easier to secure and sustain with a geographically targeted effort.
Systematic Message Development
A number of researchers have advocated for a systematic, theory-based approach to conducting formative research with the target audience (Lindsey et al., 2009; Maddock, Silbanuz, & Reger-Nash, 2008; Noar, 2006; Salem, Bernstein, Sullivan, & Lande, 2008). Two stages of research comprise systematic message development and design: formative (preproduction) research and concept/message testing (production) research. Formative research explores the target audience’s understanding of the issue, associated attitudes and beliefs, and what factors are likely to motivate or deter behavior change (Lindsey et al., 2009; Maddock et al., 2008; Noar, 2006). By comparison, concept testing and message testing assess the target audience’s reactions to specific message materials. This can include cognitive and affective reactions to the materials and measures of audience appropriateness, such as comprehension, attention, readability, relevance, and appeal (K. M. Brown, Lindenberger, & Bryant, 2008; Center for Substance Abuse Prevention, 1994; National Cancer Institute, Office of Cancer Communications, 2002). Formative research, concept testing, and message testing were undertaken for this project.
Campaign development incorporated a number of aspects from several theoretical frameworks and focused most specifically on the health belief model and social cognitive theory. The health belief model posits that people first conduct an appraisal of the benefits and barriers for participating in a certain behavior before taking action (Rimer, 2008). According to social cognitive theory (as well as other theoretical frameworks, e.g., health belief model, theory of planned behavior), efficacy is an important component in the process of encouraging action. Self-efficacy refers to one’s belief that he or she can exert control over a specific health behavior (Bandura, 2004). Social cognitive theory posits that individuals can learn from the modeling of others, including those in the media, and that watching characters receive rewards or avoid punishments may spur people to act in similar ways (Bandura, 2004).
An additional theoretical framework that applies to such work is the transtheoretical model. The transtheoretical model posits that people progress through a series of stages of change before participating in a behavior (Prochaska et al., 2008). These stages include precontemplation, when a person is unaware or has no intention to take action in the near future; contemplation, when a person intends to take action in the next 6 months; preparation, when a person intends to take actions soon and has taken steps toward taking action; action, when a person has changed behavior; maintenance, when a person has changed behavior and the change has been sustained for more than 6 months; and termination, when the person has no temptation to relapse (Prochaska et al., 2008). For a person to get to the action phase, he or she must first pass through the earlier phases of precontemplation and contemplation.
Formative Research
The campaign development process began with formative research to understand North Carolinians’ knowledge and perceptions of clinical research, including perceived benefits and barriers. Five research questions were posed:
Research Question 1: Where do North Carolinians encounter information about “clinical research” and “clinical trials”?
Research Question 2: What do North Carolinians know about “clinical research” and “clinical trials?”
Research Question 3: What types of people do North Carolinians believe participate in clinical research at the University?
Research Question 4: What do North Carolinians perceive to be the benefits of participation in clinical research at the University?
Research Question 5: What do North Carolinians perceive to be barriers to participation in clinical research at the University?
Method
To answer the research questions, the authors conducted 10 focus groups (n = 55) across North Carolina during August and September 2011. Each focus group lasted 1 hour and consisted of four to six participants. Focus groups have been used previously to examine perceptions of clinical research (Joshi & Kulkarni, 2012; Nodora, Nuno, O’Day, Yrun, & Garcia, 2010).
Participants
Because research findings were intended to identify common denominator factors to be used in the creation of a university health care–branded campaign template that could be further tailored for specific populations and health conditions, recruitment of participants was inclusive in nature in terms of geography (rural and metro), ethnicity, and prior involvement in clinical research (see Table 1 for a demographic profile). Three focus groups each were conducted in metropolitan areas and rural areas in meeting rooms in public libraries. Three additional focus groups were conducted to ensure that special populations were represented: graduate and undergraduate students at University, African Americans, and English-speaking Latinos. Focus group participants included people with prior or no experience with clinical trials. Participants received a $25 gift card as compensation for their time (Latinos each received $50 gift cards due to recruitment challenges in prior studies related to a lack of trust in the medical field).
Demographic Characteristics of Focus Group Participants.
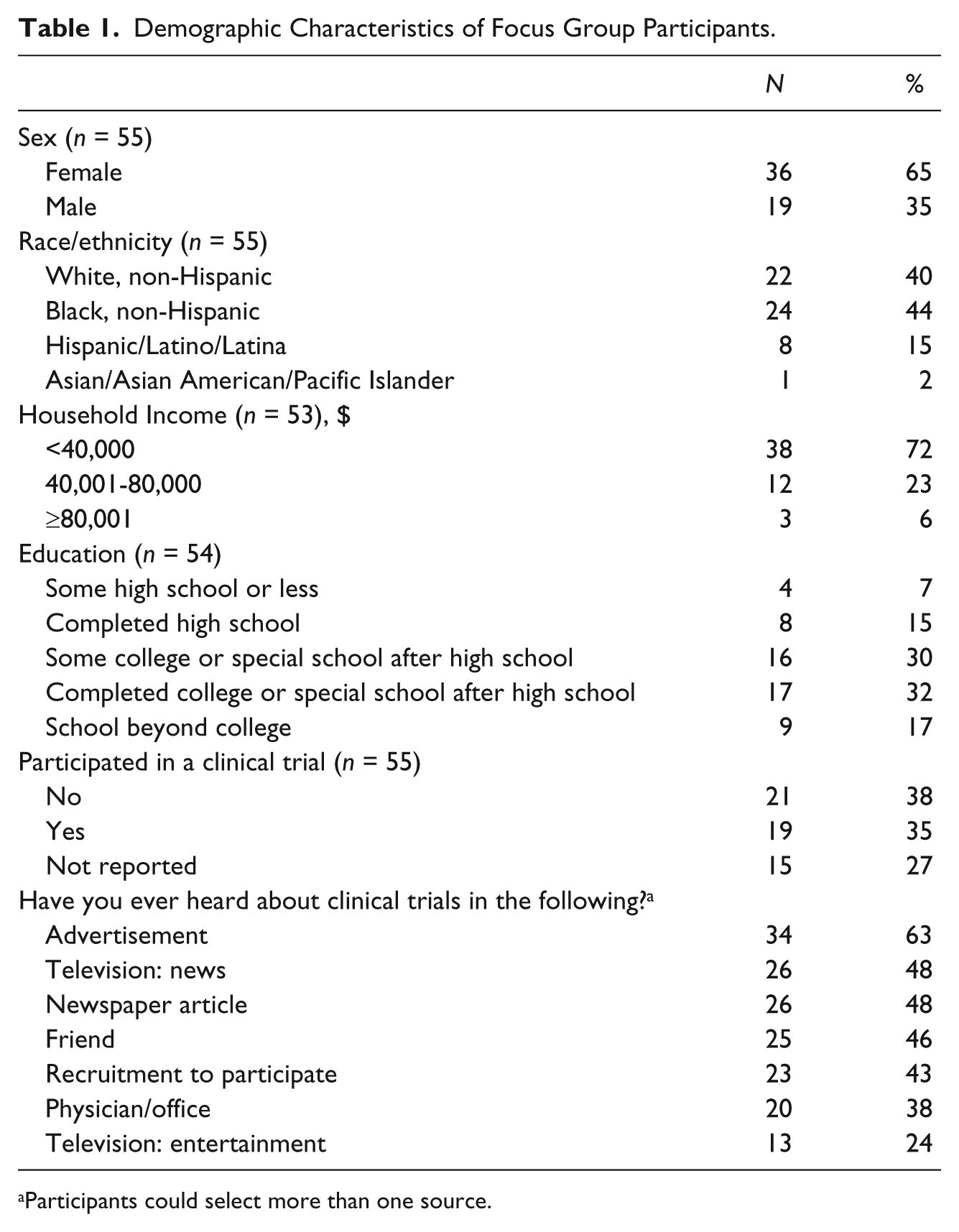
Participants could select more than one source.
Focus Group Format and Protocol
A semistructured focus group guide was developed, following the parameters outlined by Kvale and Brinkman (2009), to uncover specific information and provide opportunities for relevant information to emerge. A pilot study was conducted to test the effectiveness of the guide (Lindlof & Taylor, 2011). Minor adjustments were made to question wording and order based on the pilot study findings.
Analysis
All 10 focus groups were digitally recorded and professionally transcribed. Information about gender and location of participants was retained for analysis. The transcripts were analyzed using the constant comparative method, also known as grounded theory, which allows the researcher to identify trends or discover relationships from the ideas presented (Charmaz, 2007; Corbin & Strauss, 2008). Working independently, the authors reviewed and organized the focus group transcripts into sets of emerging themes and met to discuss their findings. Discrepancies resulted in the formation of new themes or categories.
Findings
Awareness and Information Sources
Consistent with the literature, participants largely encountered information about clinical research from clinical trial recruitment ads and news stories about drug or treatment introductions and controversies. Participants also identified peer referrals and direct-to-consumer advertisements for prescription drugs or legal services as information sources. One participant noted,
The YAZ pill ad pops in my head. They did a clinical study and how well it performed in a certain percentage of people versus another percentage of people. And when they talk about clinical trials, they talk about the side effects. So it always makes me think about the downside of testing medication. (Female, Rocky Mount)
Some participants associated clinical trials with legal services advertisements for victims of faulty medical devices or drugs. Information from these sources likely tied in to news stories about clinical trial controversies, underscoring negative associations.
Yeah, and it’s pretty common to see lawyers on TV say, “Have you been a part of this trial? If so, you can be compensated.” I think there’s a lot of, I guess, distrust of science, and I think [these ads] definitely feed into it. (Male, Raleigh)
Despite awareness of the term, focus group participants with no prior involvement in clinical trials had limited understanding of what clinical research entails. They knew clinical studies occurred but were not sure of where, why, or how to participate, underscoring the need for general education.
I think we know that clinical trials are supposed to be conducted, but everything else is just kind of . . . you don’t know what it really is, how it works, how to do it, why it’s important or anything like that. (Female, Durham) I actually tried to find something [on it in general]. I have not been able to. Why is it so difficult? (Female, Rocky Mount)
Regardless of prior involvement in clinical studies, participants tended to associate clinical research with highly invasive studies for breakthrough pharmaceutical products. Rarely did participants discuss less invasive studies that often include healthy participants, studies that may serve as an entry-level threshold for participation in clinical research. In sum, one African American participant from Durham eloquently noted the potential link between education, understanding, and interest and successful recruiting efforts.
Sometimes you have to educate people before you can get them to be interested in participating, unless they’re just going for the money. Because most of them really don’t know what [clinical research] is. I think most people think some kind of study is going on all the time. But they don’t really know the basis of the big picture. I think if people are more educated and more aware of what [clinical research] was doing, a lot more people would do it.
Perceptions of Participants, Benefits, and Barriers
Participants identified two basic motivational categories: personal benefit and altruism. As an example, one participant said, “They’re doing it because they know that down the line, it will help somebody else or even themselves and then, of course, there are the people who do it for the money.”
Regardless of prior study participation status, virtually all participants viewed personal benefit motives as most common. Personal benefit motivators included financial compensation, complimentary treatment, or participation in a clinical research study after having exhausted all other treatment options. Interestingly, the valence ascribed to these personal benefit motivators varied based on prior experience participating in a clinical trial. Most participants with prior involvement in clinical studies viewed clinical research as empowering and unabashedly shared their strategies for identifying clinical trial opportunities to supplement (or provide) income. One male participant from Durham said, “I think healthy people like me participate as long as the financial incentive outweighs the risks.” Another male from Raleigh noted, “I only recommend money. Money is what talks. So what’s wrong with money as a motivator?”
However, for participants who had not been involved in clinical studies, clinical research participants were viewed as victims—unfortunate persons stricken by health or economic hardship that forced them into participation. Consequently, this perceived motivation schema may stigmatize participation for those who have never participated in a study.
I was thinking more about the free medication . . . like if you had cancer and needed chemo treatments but couldn’t afford them, you might find a trial that could provide them as long as you were going to be a participant. (Female, Wilmington) If you’re sick or this is your only option, you really want it to work, so you would risk it. Healthy people like me? No. (Female, Durham)
Altruistic motivators were mentioned less frequently and included a desire to help others or to advance scientific knowledge—being a part of the next big discovery.
I do believe that some people participate so they can help general “others.” A lot of the times when I participate, that’s my reasoning, because I feel like I’m already past the half century mark. I don’t know how much on the other side I’m going to be here, but if you can do something to help somebody, yeah. (Female, Kinston) Personally, to be part of when something is [discovered or verified] . . . when something is progressive. (Male, Wilmington)
Several participants noted that people might be motivated by altruism only for certain types of conditions or studies. One participant said, “I’m sure if there was a research study on a condition that your friend or family member had, you would probably join.” Another said,
It’s either you know someone who’s sick, and you want to help find a cure so no one else had to go through what they go through. Or you see a heartfelt story. I watched a story about a little boy who needed bone marrow. It was talking about how people need to donate bone marrow, and it really motivated me to think, “Hmm, maybe I need to research it some more so I can figure out if I can help.” (Female, Rocky Mount)
Other participants also mentioned the importance of seeing whom you could help through clinical research:
Like a personal appeal that really pulls at the heartstrings maybe. I don’t know if that [looking at the bigger picture benefits of research] would work for me necessarily, but I might not know someone with a certain condition, but if they show someone, like on a TV commercial with a certain condition, I’m like “I can help them.” (Female, Carrboro)
At the same time, participants mentioned knowing people who would never consider participating in any type of study except as a last resort of treatment. A female from Durham said, “But some healthy people are just, ‘I don’t care how much you pay me or who it helps. I’m not going.’ My husband is like that . . . he will not do a study.” Follow-up probes with participants revealed that this attitude is primarily linked to overall mistrust of the clinical research enterprise, especially fear of being a guinea pig or not getting treatment at all.
Focus group participants identified a number of barriers consistent with the literature, including fear, mistrust, stigma, and low self-efficacy. Fear and mistrust were tied to a number of things, including fear of the unknown, side effects, and assignment to a control group that would preclude treatment. For example,
If it’s a drug study, what’s going to happen to me? What will the side effects be? Or if I give my data and there’s a family illness down the road and they want to do a gene study. Well do I want to know if I carry that gene? That’s the fear I think people feel and say, “I’m not going to participate.” (Female, Wilmington) There’s one group that may get the actual medicine and then there’s another group that gets the placebo. My concern would be if I’m sick and I have cancer, and I want to be a part of this study because I’m hoping I’m the one getting this medicine, the drawback could be that I’m not getting any medicine, and I can’t take anything else, so my cancer could progress more. (Male, Rocky Mount)
Participants also indicated that volunteering for clinical research may be stigmatizing. This could relate to clinical trial participation in general (i.e., a victim who needs money or free treatment) or be associated with specific topics, such as volunteering to be a healthy participant in HIV research. For example,
You’re saying you’re doing this. Everyone’s like, “Why are you doing that?” A, are you sick? B, are you broke? It’s just kind of like, that’s kind of a weird thing to let people do. (Female, Wilmington) You’re associated with the research. Even though it’s confidential, your family or someone may know and they may say, “She’s helping a research study for people with HIV or AIDS,” and then everyone says, “She must got AIDS.” (Female, Rocky Mount)
Participants also cited a lack of transparency about clinical trials. People felt that information about clinical trials was often confusing in nature, unclear about what participation entails or how to get involved, and that results were often not communicated after the study concluded. An African American male from Kinston said, “You never know what happens, and I think that’s unfair to ask people to participate and then not give them an update.”
Finally, there was an overwhelming sense of personal inadequacy—particularly at the individual level. A Latino male from Raleigh said, “Yeah, . . . that’s probably what they are thinking to themselves. ‘Oh, maybe I can help out, but wait a minute, I’m just one person. What can I do?’” In the words of another participant,
There have been times when I’ve been curious about what was available. I went to clinicaltrials.gov and everything was so very specific. A specific location, a specific illness, and even if I wanted to participate . . . from what it looked like, there was nothing for a person of my description. So even if you wanted to participate, the chances that you can, it seemed nil. (Female, Wilmington)
In sum, three key actionable insights emerged from the formative research. First, broadening the base of participants will require targeting new segments with a case for why the benefits of participation outweigh the costs of participation. Based on the research, North Carolinians can be segmented into four groups: (a) patients experiencing the medical condition who typically are recruited by medical personnel; (b) active seekers of clinical trials, often motivated by financial or other free treatment incentives; (c) nonparticipants with a propensity for altruism; and (d) nonparticipants who have decided never to participate. At present, the majority of clinical trial participants fall into the first two categories. Patients experiencing a medical condition under study are likely to be in the contemplation or preparation stages and in consult with health care providers about clinical research options. Active seekers of clinical trials are likely to be in the maintenance stage, and current recruitment efforts in the form of study-specific ads should continue to reflect the benefits sought by this segment—financial or other types of incentives.
This research suggests another segment for whom clinical trials are not salient currently but who might be motivated to participate with a different exchange message that emphasizes altruism (wanting to benefit scientific knowledge, society, friends, or family) or efficacy (the belief that they can actually do what is required to make a difference). This segment is likely in the precontemplation stage and would benefit from an awareness campaign with an online information hub to assist them as they move from the precontemplation to the contemplation and preparation stages.
Second, counterinformation is needed to offset the largely negative valence of clinical trials encountered in the media. At present, there is a paucity of information that contextualizes clinical research beyond what people encounter in the media. The bigger picture of “reason why” and “how to” participate is not on their radar. The clinical research mission, contribution, and process need to become more available, relevant, and transparent. An online content hub might be an ideal place to showcase proof points for this message and to demystify the clinical trial process; a media campaign could drive traffic to this site, which would then connect seamlessly to a new online clinical trial registry system that includes postregistration and postparticipation updates. The knowledge acquired through this counterinformation is expected to help foster more positive—and accurate—perceptions.
Finally, two fundamental positioning points should be incorporated into the campaign to help address misperceptions: (a) changing the public’s perception of clinical trial participants from victims for whom participation is a last resort (economically or medically) to include healthy people helping save lives and (b) putting a human face on study outcomes through a narrative approach, as participants noted the resonance of a human story over pure factual information about the clinical research enterprise.
Concept Development and Testing
Findings from the formative research guided the development of three distinct campaign concepts, each intended to drive traffic to a university health care–branded website offering contextual information about clinical research and the opportunity to sign up for a new online clinical research registry. The primary target audience for campaign concepts was people with a propensity for altruism who had no prior clinical trial participation experience. The secondary target audience consisted of patients experiencing a medical condition or active seekers of clinical trials who might benefit from additional motivation to participate in clinical research.
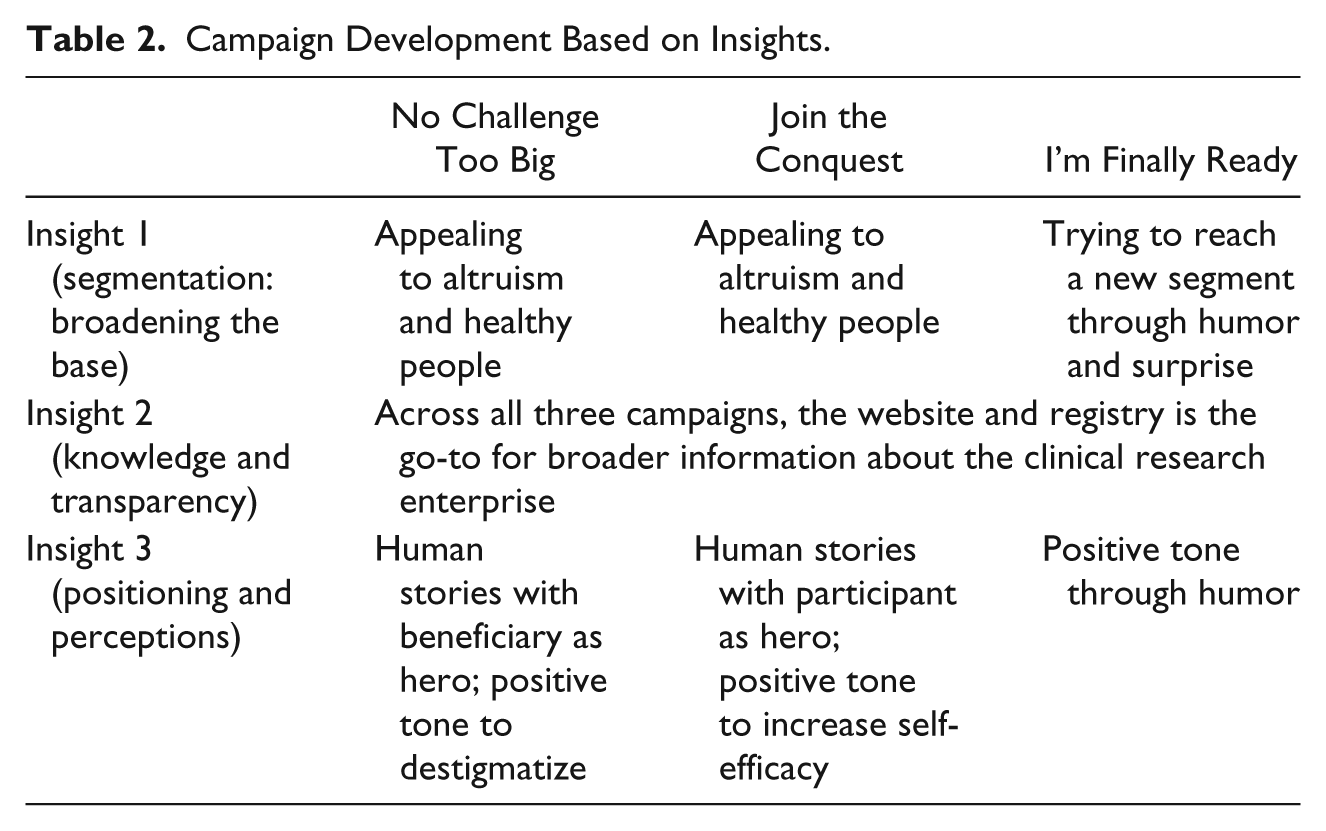
The “No Challenge Too Big” concept was designed to elicit altruistic motives and reduce stigma by featuring the beneficiaries of clinical research in a positive light (see Figure 1). The “Join the Conquest” concept was designed to convey the ease with which healthy people who want to help can begin to participate in clinical research. The materials featured a person signing up for the online registry and a promise of receiving “regular updates for studies that fit your lifestyle” (see Figure 2). The “I’m Finally Ready” concept used humor to capture the attention of people who might not attend to explicit clinical research messages by grabbing attention through well-known vernacular phrases (e.g., when pigs fly; when hell freezes over) and whimsical graphics (see Figure 3). All three concepts were designed to be optimistic in tone, avoiding stigmatization of participants or research beneficiary. See Table 2 for an overview of how each campaign concept aligns with the three key insights that emerged from the formative research.
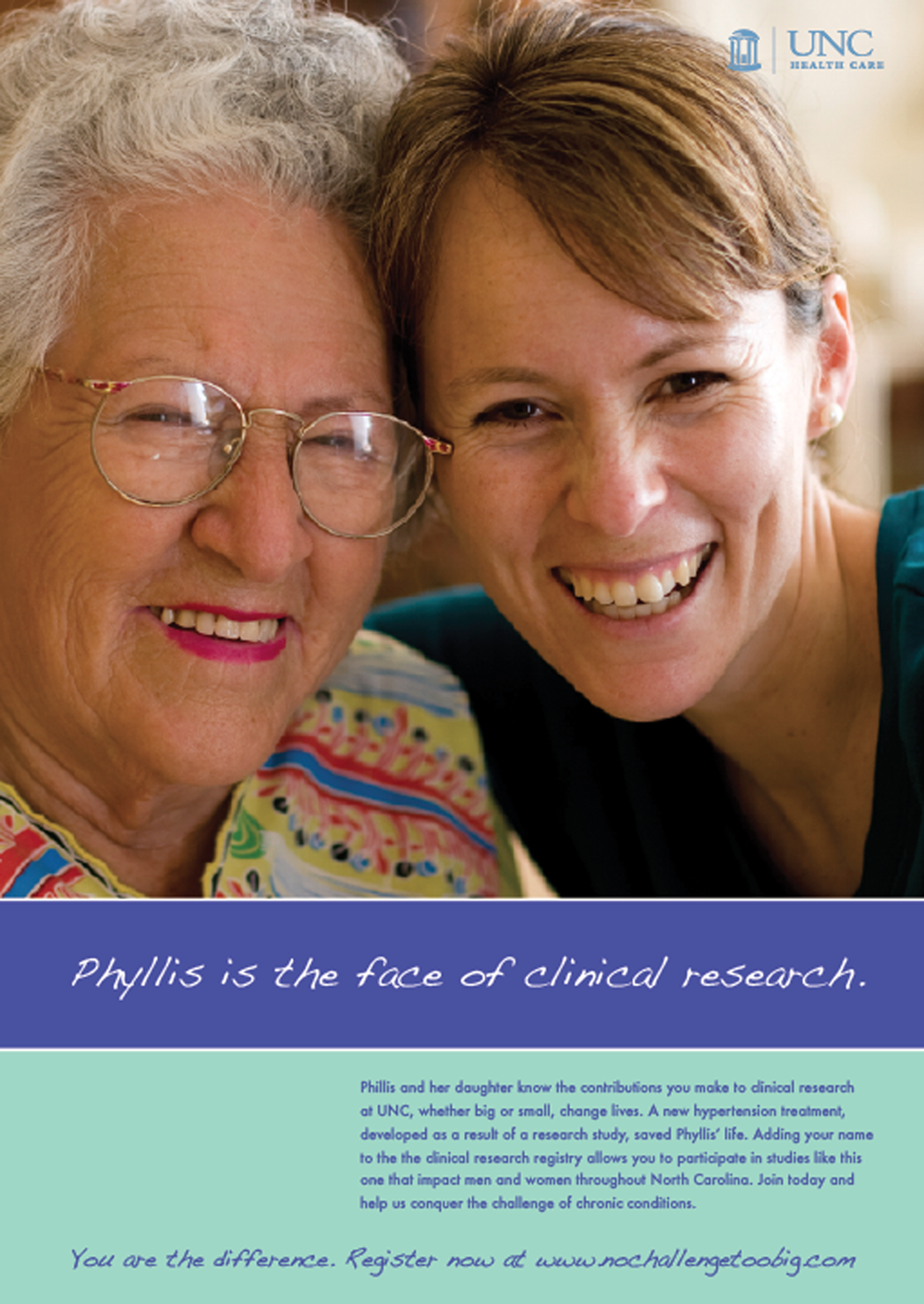
No Challenge Too Big. ©iStockphoto.com
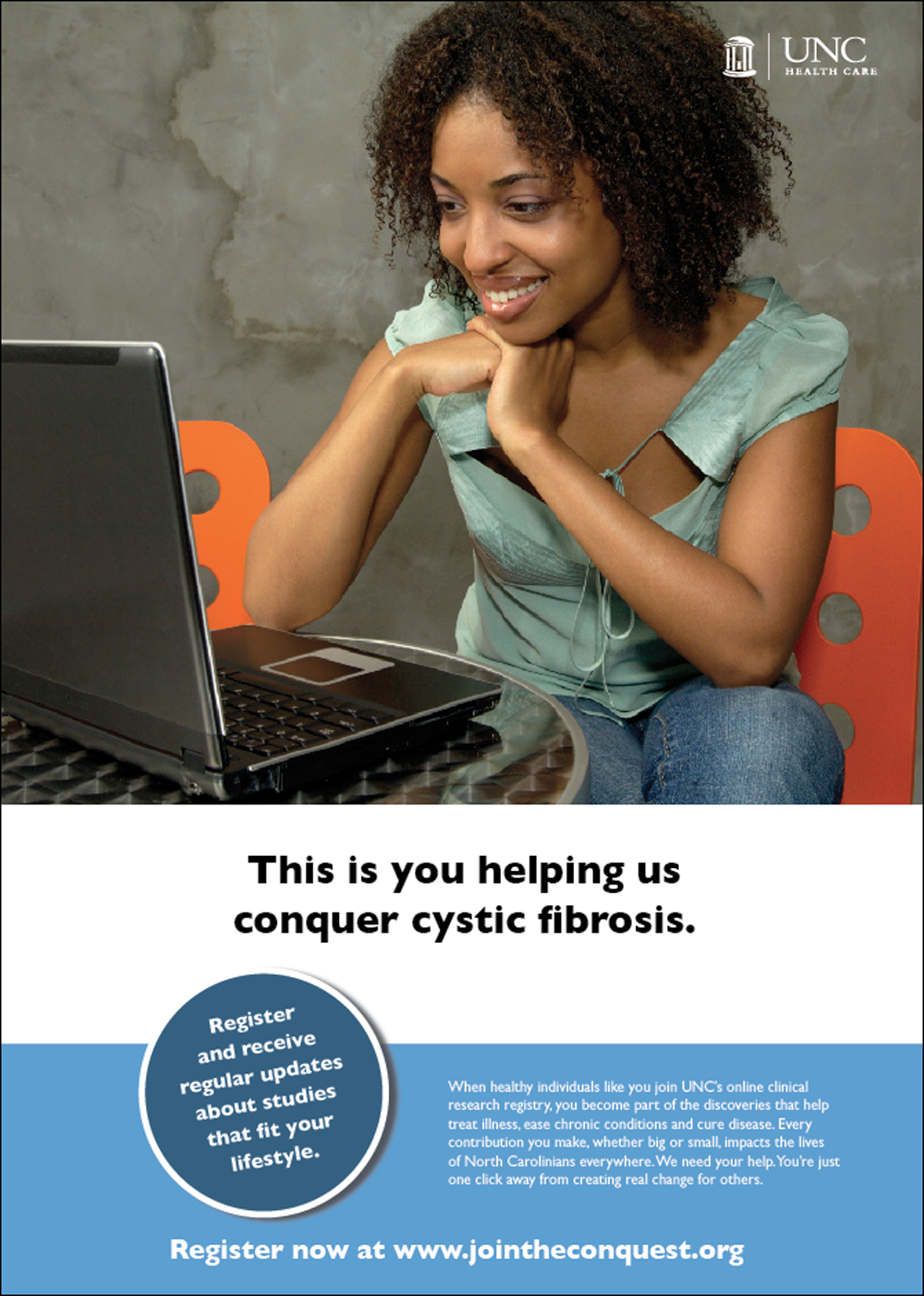
Join the Conquest. ©iStockphoto.com

I’m Finally Ready. ©iStockphoto.com
Campaign Development Based on Insights.
Multiple print ads and a website landing page were developed for each concept and tested with members of the target audience. All concepts used stock photography, which imposed some limitations on the age and ethnicity of models.
Method
A multimethod approach was used to test the three concepts. Focus groups were conducted to capture rich, reflective responses; intercept interviews were conducted with additional participants to elicit responses within a context more akin to how messages actually are encountered and processed outside of a group dynamic. Messages were assessed for comprehension, relevancy, and liking (K. M. Brown et al., 2008).
Focus Groups
Four focus groups (n = 18) were conducted by the authors with adults in rural and metropolitan markets in North Carolina and ranged in size from four to five participants. To ensure that messages resonated with the target audience of clinical study prospects without alienating existing participants, two focus groups were conducted with people without prior clinical study experience, one with prior clinical study participants, and one with a mix of both prior and nonparticipants. Participants received a $50 gift card in exchange for their time. Participants were shown all three concepts, and presentation order was rotated. Focus groups were digitally recorded and professionally transcribed.
Intercepts
Intercept interviews (n = 28) were conducted with members of the target audience—adults without prior clinical research experience who were not opposed to considering clinical research participation in the future. Interviews were conducted in both metropolitan and rural areas in public places (e.g., farmers’ markets, main street shopping districts, bus stops, and public libraries). Participants were approached by a member of the research team and asked if they would be willing to review campaign materials and provide comments. Participants received a $25 gift card for their time. Presentation order was rotated. One researcher conducted the interviews while another took notes on a laptop computer. Responses reached saturation.
Analysis
Working independently, the authors reviewed and organized the focus group transcripts and intercept notes into sets of emerging themes and met to discuss their findings. Discrepancies resulted in the formation of new themes or categories.
Findings
Participants in the focus groups and intercepts were evenly divided in their preference for “Join the Conquest” and “No Challenge Too Big” concepts. The “I’m Finally Ready” concept was dismissed because it lacked the credible tone believed to be necessary for medical research and because it fostered the unintended, negative impression of clinical research as disheartening (e.g., if it’s that difficult to recruit people, there must be some valid reason why). Participants found that the “I’m Finally Ready” concept caught their attention but not in a positive manner.
Participants appreciated the direct, literal, and actionable nature of “Join the Conquest” (e.g., I know what you want me to do and I’m able to do it). At the same time, participants were confused by the term healthy people (e.g., am I healthy if I don’t have the malady being featured or if I have no medical issues) and the phrase “register and you’ll receive regular updates that fit your lifestyle” (e.g., am I signing up for an RSS feed about scientific discoveries related to a particular disease?). Many participants did not relate to the young models featured in the ads due to their age and the emphasis on computer work, showing that these ads were not seen as relevant or attention catching by the target audience. Furthermore, some participants believed the overall message to be potentially misleading (e.g., all you need to do to help is sign up for the registry—is it really that simple?). In other words, people thought they knew what you wanted them to do, but there was confusion as to what happens next (after you register). So there was a sense of efficacy but confusion about the process.
Other participants preferred “No Challenge Too Big” because of the motivational stories of people who are cured or are experiencing an improved quality of life. Participants also appreciated the diversity of the models portrayed in the ads and felt the pictures drew their attention and saw the people presented as relevant to them. At the same time, participants misinterpreted the word contribution to mean a financial donation and were unclear about what to do next to help. In other words, there was motivation but not efficacy.
Concept Refinement and Final Message Testing for “Join the Conquest”
The “Join the Conquest” concept was modified to include elements of the “No Challenge Too Big” campaign (see Figure 4). Although the revised concept continued to focus on how an individual could help, the clinical research beneficiary became the visual hero in the ad, and the text provided a brief synopsis of their story. Unclear language was revised.

Final creative. ©iStockphoto.com
Eighteen intercept interviews were conducted to test the final ads, using the same criteria as in the earlier intercepts. Participants included nine females and nine males, six of whom were Caucasian, six African American, four Latino/Latina, and two Asian American. Responses indicated significant improvement in the areas of concern identified during concept testing.
Message comprehension was very strong: “You’re trying to get people to sign up so they can be part of research studies to help people”; “By signing up for a registry, you can learn how to participate in clinical research that helps people.”
Participants now understood what to do and what would happen next—that signing up for the registry was a first step and not a commitment to participate in a study: “It tells me I can learn about this stuff first before committing to anything.” Participants also responded positively to the website landing page and appreciated the information that would be provided about types of studies, the research process, and more stories about how research has helped people. “I like that I can go to a site to learn more about what the registry is and more about types of studies.” Participants also had a clearer understanding of what the registry service would provide: “If you join, you’ll get information about relevant studies.” “I would assume you are able to input demographic information and preferences and it will give me studies that meet my demographics and preferences.”
Discussion
Increasing the pool of clinical research participants in North Carolina will require broadening the knowledge base and changing the attitudes of the general public, moving them from awareness to education/knowledge to interest to participation. According to the theory of planned behavior, people must have positive behavioral beliefs, normative beliefs, and control beliefs about a behavior to lead an intention to participate, which then leads to participating in a specific behavior (Ajzen, 1991). This campaign is designed to help move people from precontemplation to contemplation to preparation by raising awareness of the benefits of clinical research and providing information about how clinical research works and how to get involved. The campaign targets behavioral beliefs with the success stories; it targets norms by indicating that people similar to the viewer participate in clinical research; and it targets control beliefs by showcasing how easy it is to get involved. The campaign (the website, registry, and promotional materials) showcases the stories of people who have been helped through clinical research and includes information on what “people like you” have done to help others. This aims to increase self-efficacy, which is an important component of health behavior change (Strecher, DeVellis, Becker, & Rosenstock, 1986).
“Join the Conquest” is a university healthcare system–branded, reason-why campaign designed to elicit altruism and provide a simple, clear path to a website where people can expand their knowledge of clinical research processes and outcomes, identify with real people who have benefitted from participation, and sign up for a registry that will automatically notify them about opportunities to participate in studies for which they have designated interest. Additionally, branding elements from the campaign will be featured in all study recruitment advertisements within the university health care system, providing a link between contextual information about clinical research and the promotion of specific study opportunities and also helping increase relevance for participants. The benefits of the campaign may extend beyond North Carolina. The research and resulting materials have been shared with other recipients of the NIH Clinical and Translational Science Awards, who comprise a national consortium of 60 medical research institutions working to improve the way biomedical research is conducted across the country.
As with any study, there are limitations. Qualitative studies have an inherent limitation as their results may not be representative or generalizable. Participants in the focus groups may have differed from other North Carolinians or the U.S. population in general. For example, our sample for the focus groups was fairly well educated, with 49% having completed college or school beyond college compared to 38% of North Carolinians aged 25 to 64 years (Lumina Foundation, 2012). A second issue is related to the broad, inclusive nature of the campaign. Although the campaign is more geographically targeted than prior national campaigns, its umbrella approach does not take into consideration the nuances that may be associated with specific ethnic populations or health issues. Finally, although a central tenet of this campaign is to better inform the public about how the clinical research enterprise works and what benefits it provides in order to address barriers associated with mistrust, we recognize that education alone will not be enough to overcome all barriers to clinical trial participation. Future research should further examine what barriers may exist for individuals once motivated to participate, particularly in relation to specific disease states and populations.
Future research will address some of the limitations. Going forward, additional formative research will need to occur for the campaign to be tailored to effectively resonate with specific population, particularly underserved populations with higher levels of mistrust and populations experiencing specific health issues that are a priority for clinical trial recruitment in North Carolina (e.g., What are the disease conditions that are most prevalent? Who are the target audiences from which the clinical samples need to be drawn? How can we best reach out to these individuals?). Next steps also include developing a channel strategy to promote the website; designing website content, registry creation, and pilot testing; and developing an evaluation plan to monitor and the impact of the campaign and registry on clinical trial participation.
Conclusion
Although a few national campaigns have attempted to bolster support for clinical research (e.g., Medical Heroes; Getz, 2008), most promotion of clinical research continues to come from study-specific trial recruitment ads or information presented by a health care professional to a patient at the time of recruitment. As a result, these calls for participation continue to fall on people typically unaware of the overall purpose, benefits, and processes of clinical research and often predisposed to distrust the enterprise.
This locally branded campaign will reach out to North Carolina residents and provide information to help address some of the barriers that limit study participation. These findings confirm some of the suggested barriers and benefits that emerged from prior research but also extend them, particularly for North Carolinians. For example, participants indicated that they had heard about clinical research and knew it was happening, but they had trouble defining clinical research and what it entailed. This suggests that a campaign that increases awareness about clinical research and whose features include a robust online content hub where people can learn about clinical research, experience the stories of those who have both participated and benefited from clinical research, and decide whether to take immediate action to enroll in an online participant registry with just one click may provide one important step toward increasing participation in clinical research by the people of North Carolina.
This research was an essential first step in campaign development and included audience segmentation and message testing. Amid unprecedented budget cuts and an increasingly fragmented media environment, evidence-based campaign development is vital to addressing the participant recruitment challenge within a targeted geographic area.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the National Center for Research Resources, Grant UL1RR025747, and is now at the National Center for Advancing Translational Sciences, Grant UL1TR000083. The authors received funding for participant research incentives for formative research and message testing as well as creative services (McMahon).