
Abstract
Background
D-dimer have been frequently used to assess the preliminary risk of muscular calf vein thrombosis (MCVT) after knee arthroplasty. However, D-dimer is usually higher than the clinical reference range in clinical settings, the relationship between D-dimer and postoperative MCVT remains to be explored.
Objective
To investigate the association between postoperative MCVT and D-dimer after knee arthroplasty.
Methods
A retrospective case-control study was conducted on patients who received knee arthroplasty in the Department of Orthopaedics from September 1, 2022, to December 31, 2022.We collected basic demographic information, disease history, surgical and anesthesia information, blood examination results on admission and the first day of postoperative, and postoperative MCVT from patients. A multivariate logistic regression model was adopted to evaluate the association between D-dimer and postoperative MCVT, and the restricted cubic spline was used to analyze the dose-response relationship between D-dimer and postoperative MCVT.
Results
Postoperative MCVT was diagnosed in 103 out of 401 patients, with a prevalence of 25.69%. The median of preoperative and postoperative D-dimer was 0.47 ug/mL and 3.80 ug/mL in patients with postoperative MCVT, compared with 0.42 ug/mL and 2.42 ug/mL in patients without postoperative MCVT. After adjustment for the covariates, postoperative D-dimer was statistically significantly associated with an increased risk of postoperative MCVT. Restricted cubic spline regression showed a nonlinear dose-response relationship between postoperative D-dimer and postoperative MCVT and an increased risk of postoperative MCVT overall with higher D-dimer levels when D-dimer was over 2.62 ug/mL. There was no interaction between D-dimer and postoperative MCVT for the subgroups of age, sex, lacunar cerebral infarction, nerve block anesthesia, and surgery duration in the subgroup analyses.
Conclusions
With the high incidence of postoperative MCVT in patients with knee arthroplasty and the positive dose-response relationship between postoperative D-dimer and the risk of postoperative MCVT, risk stratification strategies should be developed for postoperative D-dimer to reduce the incidence of postoperative MCVT in patients with knee arthroplasty.
Introduction
Knee arthroplasty (KA) is an effective and common surgical treatment for knee osteoarthritis, mainly including total knee arthroplasty and partial knee replacement, 1 which alleviates pain but also causes early complications, such as myocardial infarction, stroke, infection, and venous thrombosis. 2 Deep vein thrombosis (DVT) has been the most common complication after arthroplasty, 3 caused by reduced blood flow in the postoperative period due to inactivity, ischemic tissue damage, and blood vessel damage. 4 The incidence of isolated distal DVT in patients who underwent arthroplasty ranged from 0 and 27.2%, 5 with the highest incidence reported at 52%. 6 muscular calf vein thrombosis (MCVT), which occurs at the gastrocnemius and soleus muscles, accounts for 63.0% of isolated distal DVT cases. 7 MCVT can leads to various adverse outcomes, including susceptibility to pulmonary embolism 8 and all-cause mortality at 30 days of admission. 9
As MCVT is usually asymptomatic, early assessment and anticoagulation treatment after surgery is particularly important. The American College of Chest Physicians clinical practice guideline recommend that patients receive 10–14 days of continuous anticoagulation after knee arthroplasty. 10 Orthopedic surgeons typically choose between aspirin or anticoagulants based on the risk to patients. However, additional anticoagulation treatment can elevate the risk of bleeding. 11 Therefore, it is crucial to establish an effective anticoagulation strategy that involves dynamically assessing the patient's risk of postoperative MCVT. Currently, there are no guidelines for the assessment or diagnosis of postoperative MCVT. Instead, the risk of DVT is usually assessed by D-dimer in combination with a clinical score.12,13 The estimated sensitivity of D-dimer for DVT was 96.1%, and the false negative rate was less than 5%, indicating a reliable relationship between D-dimer and DVT. 14 Nevertheless, in the case of orthopaedic surgical injuries, old age, and various other factors, the sensitivity and specificity of D-dimer may be reduced. 15 It has been indicated that the mean postoperative D-dimer in patients without DVT after arthroplasty is 2.09 ug/mL, 16 whereas in contemporary clinical practice, 0.5 ug/mL is still used as a reference for assisting with DVT diagnosis. Therefore, it is necessary to adjust the threshold of D-dimer in the prevention of MCVT to improve the accuracy of the preliminary assessment in patients after knee arthroplasty.
Existing studies usually combined D-dimer and other covariates in multiple regression analysis or developed nomograms 17 to explore the risk associated with postoperative MCVT. 18 However, it is not feasible to determine the association between D-dimer and postoperative MCVT. The Restricted cubic spline plots have been extensively used as methods to explore the relationship between quantitative variables and outcomes. 19 Therefore, this study aimed to investigate the dose-response relationship between postoperative D-dimer levels and postoperative MCVT in patients who received knee arthroplasty.
Materials and Methods
Participants and Study Design
All hospitalized patients 18 years of age and older who received a knee arthroplasty during the study period (September 1, 2022, to December 31, 2022) and without lower extremity MCVT detected by preoperative venous ultrasound were included in the study. In addition, patients who had not undergone preoperative and postoperative lower limb venous Doppler ultrasound examinations or had incomplete clinical data were also excluded. A total of 436 patients underwent knee arthroplasty in the orthopedic unit in the First Affiliated Hospital of the University of Science and Technology of China during the period 9.1-12.31.2022, of which 401 patients were selected to match the inclusion criteria (Figure 1). A retrospective case-control study with a division of the included patients into two groups based on the occurrence of complications of postoperative MCVT was designed.
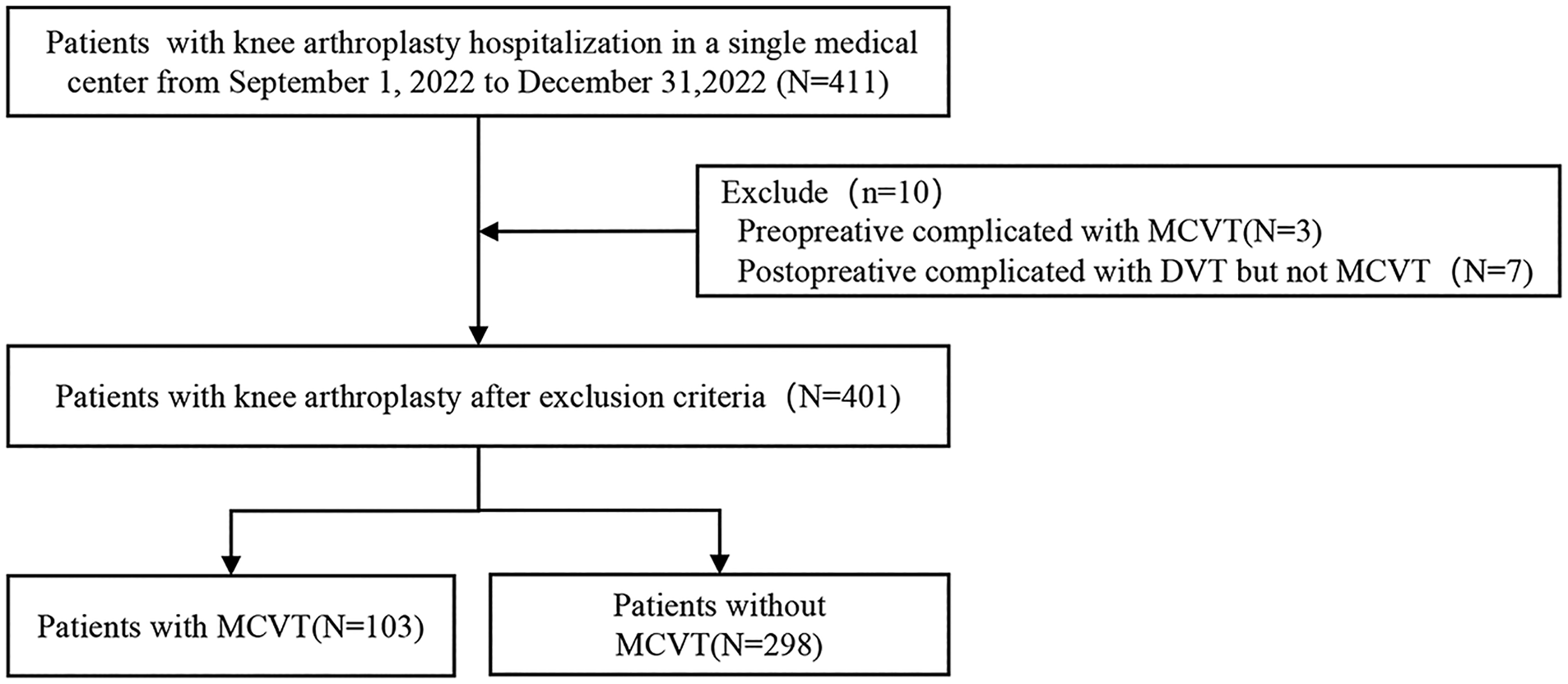
Flowchart for the selection of research population.
Data Collection
A structured clinical information collection form was designed by reviewing the literature and consulting with clinical experts, and two researchers collected patient information in the clinical record system through the collection form. Dependent variables included general demographic information about the patient, the history of disease, information about surgical and anesthetic history, and blood examination results on admission and the first day of postoperative, and postoperative MCVT from patients. General demographic information included sex, age, and BMI. The disease history included the presence of hypertension, diabetes, stroke, and lacunar infarction. Surgery and anesthesia information included surgical approach, limb on which the surgery was operated, surgery duration, intraoperative bleeding, general anesthesia approach, whether or not the anesthesia was combined with nerve block anesthesia, and the duration of tourniquet use during surgery. The first preoperative blood examination included prothrombin time (PT), activated partial thromboplastin time (APTT), international normalized ratio (INR), fibrinogen (FIB), white blood cell count, ultrasensitive CRP, platelet count, and serum albumin. The postoperative (first postoperative day) blood examination included D-dimer, white blood cell count, and ultrasensitive CRP. Plasma D-dimer was determined by enzyme-linked immunosorbent assay (ELISA). The assay is based on the specific antibody–antigen interaction between D-dimer and its corresponding antibody, with signal generation via an enzyme-catalyzed reaction, allowing sensitive and specific quantification of plasma D-dimer concentrations.
Dependent variable:Patients were diagnosed with postoperative MCVT by lower-extremity venous Doppler ultrasound examinations. In this study, all patients underwent preoperative ultrasonography to exclude the presence of pre-existing thrombosis. A routine ultrasonographic examination was performed on the second postoperative day with the aim of early detection of potential MCVT and ensuring timely intervention. All ultrasound examinations were conducted by experienced and qualified sonographers. These personnel held relevant medical imaging certifications and had received rigorous professional training. All examinations were performed independently by sonographers in the ultrasound department, who were blinded to the patients’ clinical information and the study hypotheses. The ultrasound reports were subsequently uploaded independently to the electronic medical record system.
Statistical Analysis
Continuous variables were reported as median with interquartile range (IQR) or mean with standard deviation (SD) and compared using the Wilcoxon rank sum test or Student t-test, respectively. Categorical variables were reported as counts with percentages (%) and compared with Fisher's exact test or Pearson's chi-squared, respectively. Variables with a low proportion of missing values, a complete case analysis (CCA) approach was applied, whereby only patients with complete data for the relevant variables were included in the corresponding analyses. Importantly, there were no missing data for the main exposure variable or the primary outcome. Univariate and multivariate binary logistic regression were utilized to investigate the independent and adjusted relationship between postoperative MCVT and D-dimer in accordance with the STROBE statement. 20 Model 1 was a crude model without any adjustment, while Model 2 adjusted for gender and age. Model 3 was built on Model 2 with further adjustments for variables that were statistically significant at the baseline of lacunar cerebral infarction, nerve block anesthesia, and surgery duration. A restricted cubic spline with three knots was conducted to further assess the dose relationship between D-dimer and MCVT. Subgroup analyses were adopted to compare the relationship between D-dimer and MCVT in different age groups, gender groups, lacunar cerebral infarction groups, nerve block anesthesia groups, and surgery duration groups by using a fully adjusted model (Model 3). Interactions were computed using the likelihood ratio test. Statistical analyses were conducted using SPSS 24.0 and R4.3.2, where the ‘RMS’ package was used for restricted cubic spline and the ‘jstable’ package was used for subgroup interaction analyses. P < 0.05 was considered statistically significant.
Ethical Approval and Consent to Participate
The First Affiliated Hospital of the University of Science and Technology of China approved this study (Ethical Approval Number:2023ky123). The study used de-identified electronic medical records for retrospective analysis of data, and and patient exemption from informed consent
Results
Baseline Characteristics
Postoperative MCVT was found in 103 patients, and the incidence of postoperative MCVT was 25.69%. The median preoperative and postoperative D-dimer were 0.47 (0.35, 0.88) µg/ml and 3.80 (2.04, 6.14) µg/ml in patients with postoperative MCVT, compared to 0.42 (0.25, 0.71) µg/ml and 2.42 (1.38, 4.31) µg/ml in patients without postoperative MCVT (Table 1). Statistically significant differences were found in age, gender, lacunar cerebral infarction, nerve block anesthesia, surgery duration, preoperative CRP, and preoperative and postoperative D-dimer among the two groups of patients (P < 0.05).
Baseline Characteristics of the MCVT and no MCVT Groups.
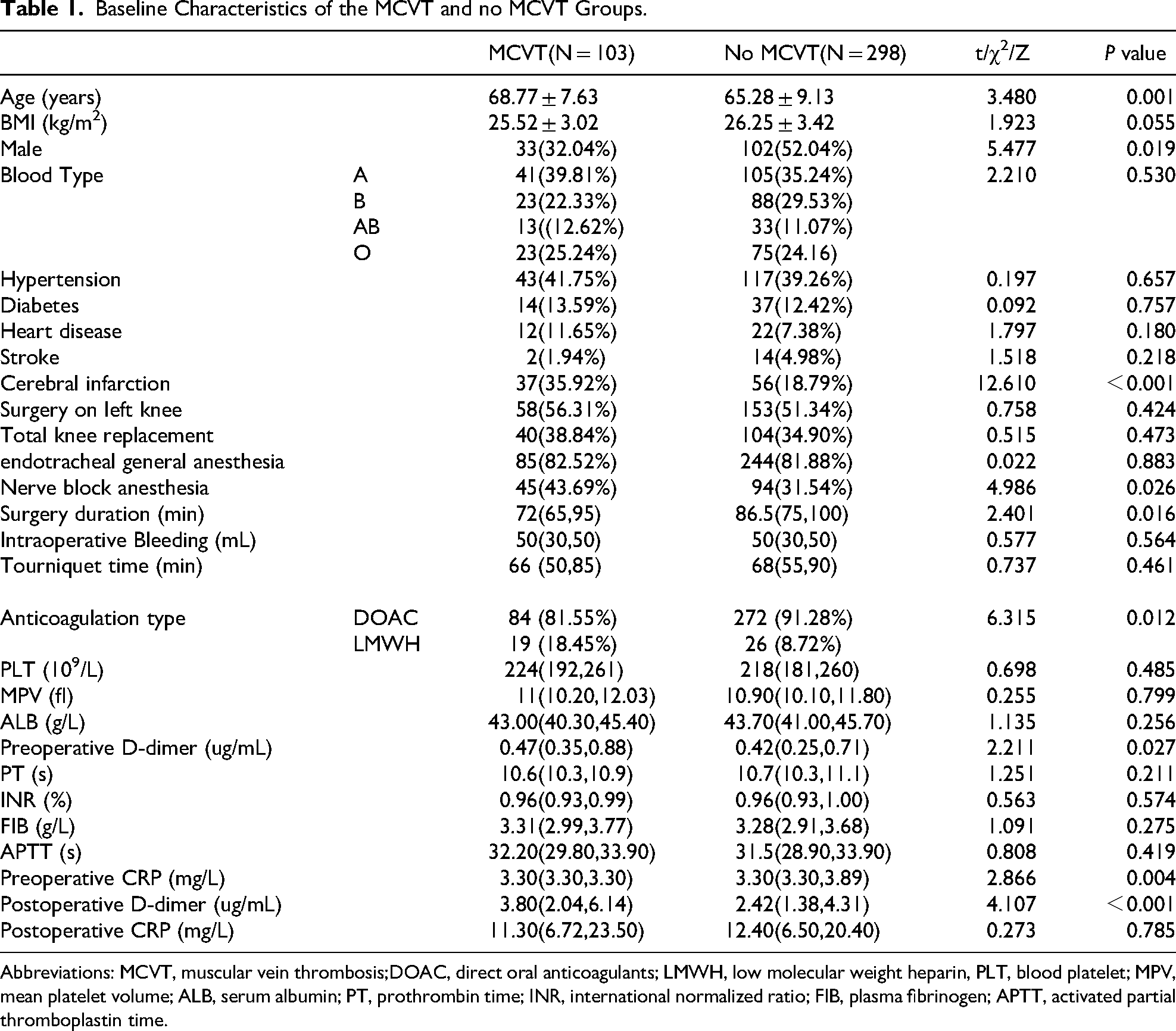
Abbreviations: MCVT, muscular vein thrombosis;DOAC, direct oral anticoagulants; LMWH, low molecular weight heparin, PLT, blood platelet; MPV, mean platelet volume; ALB, serum albumin; PT, prothrombin time; INR, international normalized ratio; FIB, plasma fibrinogen; APTT, activated partial thromboplastin time.
Univariate and Multivariate Binary Logistic Regression Analysis of D-Dimer and MCVT
In order to investigate the relationship between D-dimer and postoperative MCVT, a multivariate logistic regression analysis was performed with preoperative and postoperative D-dimer as the only independent variables, respectively (Table 2). The results showed that postoperative D-dimer was a risk factor for postoperative MCVT, with an OR (95% CI) of 1.11 (1.05-1.18), whereas preoperative D-dimer was not, with an OR (95% CI) of 1.11 (0.91-1.35). After adjustment for confounders of age and sex, anticoagulation type, the strength of the association between postoperative D-imer and postoperative MCVT remained statistically significant, with an OR (95% CI) of 1.12 (1.05-1.19). In addition, in a fully adjusted model, there was a significant positive correlation between postoperative D-dimer and postoperative MCVT, with an OR (95% CI) of 1.15 (1.07-1.22).
Univariate and Multivariate Binary Logistic Regression Analysis of D-Dimer and MCVT.
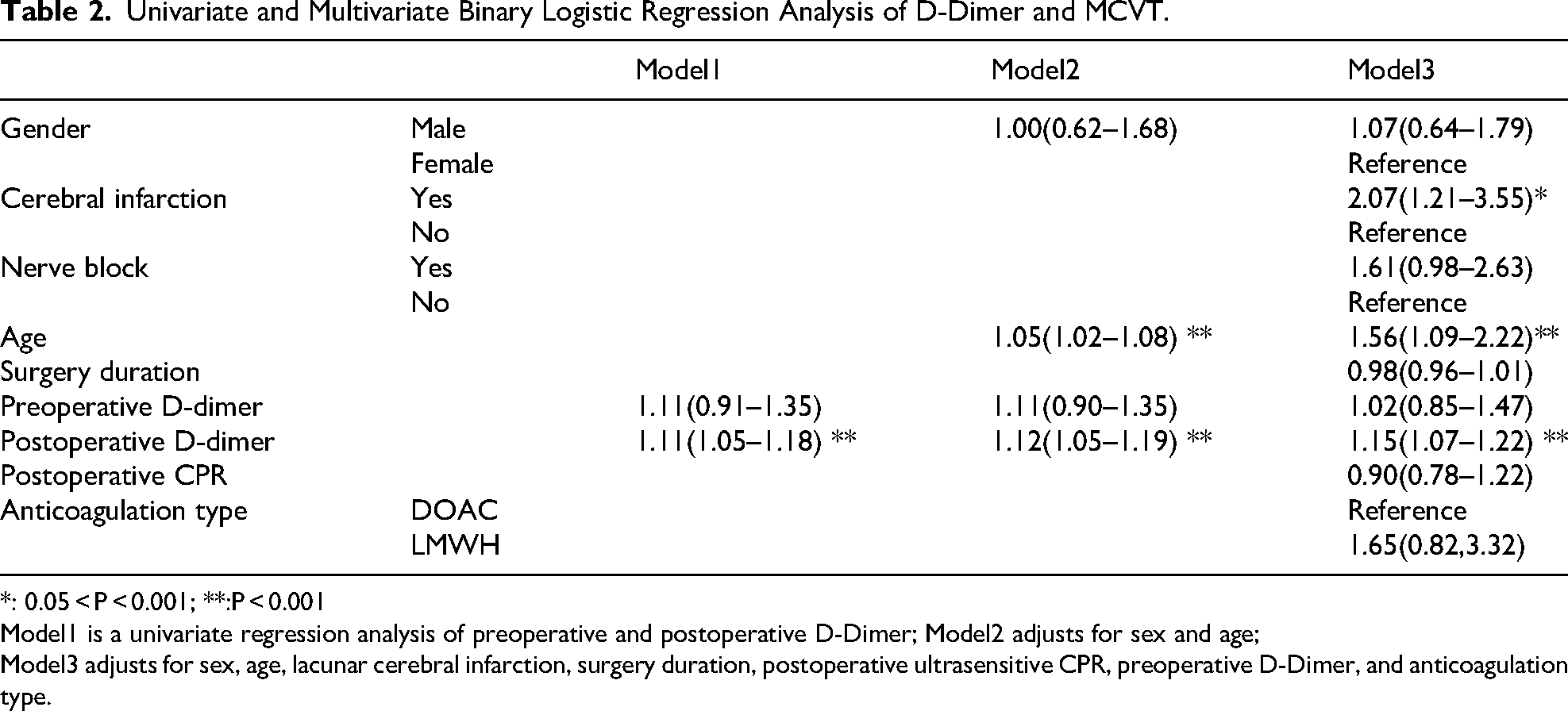
*: 0.05 < P < 0.001; **:P < 0.001
Model1 is a univariate regression analysis of preoperative and postoperative D-Dimer; Model2 adjusts for sex and age;
Model3 adjusts for sex, age, lacunar cerebral infarction, surgery duration, postoperative ultrasensitive CPR, preoperative D-Dimer, and anticoagulation type.
RCS Analysis Based on Logistic Regression
The knot of RCS was selected based on the smallest AIC value (AIC = 426.93). The RCS plot demonstrated a positive non-linear dose-response relationship between postoperative D-dimer and the risk of postoperative MCVT (χ2d−dimer = 18.09, PD−dimer <0.001; χ2non−linear = 6.54, and P non−linear = 0.011). The estimated OR was 1.001 (95% CI = 1.000–1.002) when D-dimer was at 2.62 ug/mL, and although the growth rate of the risk of postoperative MCVT slowed down after a D-dimer greater than 5 ug/mL, the overall risk increased with higher postoperative D-dimer (Figure 2).
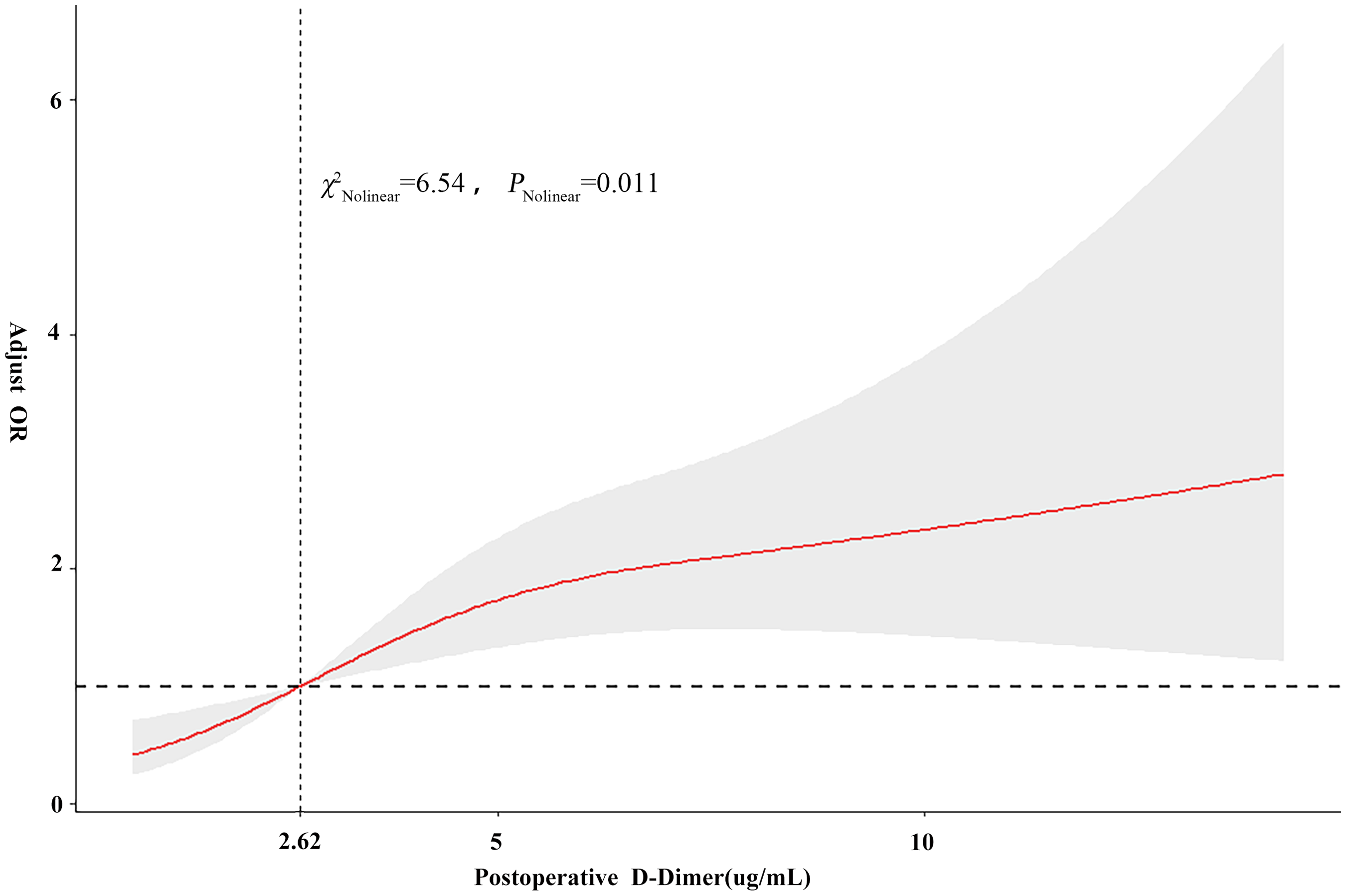
Restricted cubic spline curve for the association between the postoperative D-dimer and the risk of postoperative MCVT.
To investigate whether the association between postoperative D-dimer and postoperative MCVT differed between populations, subgroup analyses based on age, gender, presence of lacunar cerebral infarction, nerve block anesthesia, and surgery duration were further investigated (Figure 3). The negative association between postoperative D-dimer and postoperative MCVT was maintained in the subgroups of age, sex, lacunar cerebral infarction, and surgery duration (P < 0.05). Nevertheless, the results showed that the relationship between postoperative D-dimer and postoperative MCVT was not statistically significantly different in all subgroups (interaction P < 0.05).

Subgroup analysis of the association between the postoperative D-dimer and the risk of postoperative MCVT.
Discussion
In this study, we retrospectively reviewed 401 hospitalized patients who received knee arthroplasty from September to December 2022, including 101 with postoperative MCVT, and analyzed the association between D-dimer and postoperative MCVT. The results showed a positive association between postoperative D-dimer and the postoperative MCVT after adjusting for age, sex, and other confounders. Restricted cubic spline plots showed a nonlinear dose-response relationship between postoperative D-dimer and postoperative MCVT.
Lower extremity DVT has been the most common complication in patients who underwent knee arthroplasty, with MCVT accounting for the majority of these events. The incidence of postoperative MCVT in this study was 25.69% (103/401), which confirms this finding. Due to numerous branches, small venous valves, and slow blood flow, 21 the calf intermuscular veins were more susceptible to venous thrombosis and were likely to spread to the popliteal vein or even higher compared to other veins of the lower extremities. The incidence of MCVT after knee arthroplasty in our study was slightly higher than the 16.89% in Huang's 22 study and was similar to that in other patients with periprosthetic knee fractures (20.5%–26.3%). 23 All patients in this study received ultrasound examinations of both lower extremities, which increased the reported rate of postoperative MCVT. Additionally, the higher incidence observed in this study is attributed to the more intensive screening protocol, which was based on time rather than symptom-based screening.
The guidelines recommend the utilization of clinical risk scores in combination with D-dimer as a preliminary screen method for DVT, and a normal range of D-dimer can reliably exclude clinically symptomatic VTE when the clinical probability of venous thrombosis is low. Conversely, when the predicted probability 24 was considered low, higher D-dimer levels suggested a more likely thrombotic risk. Although the clinical score of the Caprini is the most commonly used clinical assessment tool for DVT in orthopaedics, it is debated for its postoperative applicability due to the high baseline score of patients with knee replacements. 16 It has been shown that D-dimer as an independent indicator 25 reduces the proportion of required lower limb ultrasound from 81.8% to 72.2%, which indicates a reliable relationship between D-dimer and DVT.
D-dimer is a fibrin degradation product reaching a very high level during active fibrinolysis, which occurs in the case of intravascular fibrin deposition or extravascular fibrin deposition. On the first day after surgery, postoperative D-dimer peaks at approximately nine multiples of preoperative D-dimer in patients who underwent total joint replacement surgery and then declines rapidly on the third day after surgery. 26 Jiang 27 indicated that on the first postoperative day, the AUC for D-dimer was 0.889, showing higher diagnostic value for predicting DVT compared to postoperative days 3 and 7. Therefore, it is more valuable to monitor peak D-dimer levels on the first day after surgery compared to follow-up. This study supports other studies that found that the risk of MCVT was twice as high when D-dimer levels were reported at 2.62 ug/mL measured on the first postoperative day. Yang 28 retrospectively analyzed 150 patients with lower limb fractures who underwent incisional reduction and internal fixation and recommended screening with postoperative D-dimer at a threshold of 3 ug/mL, with an AUC of 0.924, a slightly lower sensitivity of 88.37%, and a significantly higher specificity of 96.96%. In contrast, some studies have been more conservative in setting cut-off values, and in a study in which postoperative MCVT accounted for 90.5% of patients, 29 the optimal cut-off for postoperative D-dimer was set at 1.0 ug/mL, twice the standard upper limit of 0.5 ug/mL, which was associated with a 3.50-fold increase in the risk of postoperative MCVT. Zhuang 30 analyzed 651 patients who received hip replacements and found that the optimal cut-off value for postoperative D-dimer was set at 1.44 ug/mL, which increased the risk of DVT by about 1.04-fold, with a sensitivity of 73.7%, a specificity of 64.6%, and an AUC of 0.732 for the diagnosis of new-onset DVT. The optimal cut-off value of D-dimer in the prediction of venous thrombosis in the setting of orthopaedics varied from study to study due to differences in study populations, timing of postoperative D-dimer measurements, and types of distal lower extremity DVT, but all suggest that postoperative D-dimer has a predictive value in DVT and that its optimal cut-off value needs to be continually explored.
There was no interaction between the subgroups regarding the impact of postoperative D-dimer on postoperative MCVT. However, there were different risks of DVT in other studies within the same postoperative D-dimer range for ages and genders. As the performance of postoperative D-dimer in screening the risk of venous thrombosis decreases with age, age-adjusted postoperative D-dimer thresholds have been reported in patients with knee or hip replacement. 31 As the performance of D-dimer in screening the risk of venous thrombosis decreases with age, adopting age-adjusted D-dimer thresholds for an age multiplied by 10 criteria instead of 500 in patients over 50 years old 32 can increase the diagnostic specificity from 47% to 61%, 33 which suggests that this strategy is safe and cost-effective. Fewer studies have adjusted DD for gender. Haase C 34 classified the reference ranges of normal D-dimer in men and women of different ages by stratifying the 1352 general population according to gender and age. Reagh 35 showed that the 95% sensitivity D-dimer cut-off value was 0.33 mg/L for women and 0.32 ug/mL for men, but there was no statistically significant difference between gender and thrombotic after control for the D-dimer. Gender differences in thrombosis and immune responses have been extensively studied. However, given that the results of this analysis approached statistical significance, we recommend further validation of this gender difference in future studies, particularly in larger sample sizes or multicenter research settings.
Limitations
There remain unavoidable limitations to this study. First, this study retrospectively explored perioperative MCVT, whereas long-term postoperative D-dimer trends may be more advantageous for identifying typical MCVT in patients with short hospital stays due to the enhanced recovery after surgery. In addition, the proposed D-dimer cutoff was not evaluated using conventional diagnostic performance measures, such as receiver operating characteristic (ROC) curve analysis or area under the curve (AUC) values. As a result, the cutoff value of 2.62 μg/mL for risk stratification should be considered exploratory and interpreted with caution. Further prospective studies are needed to assess the predictive value of D-dimer levels in early risk stratification of MCVT in clinical practice.
Conclusion
D-dimer has been extensively researched as an important independent factor influencing postoperative MCVT, along with other variables. The strength of the association with the risk of DVT was estimated in a conventional logistic model that ignored the continuous trend of the variation in postoperative D-dimer and DVT. This study shows that there is a non-linear positive relationship between postoperative D-dimer levels and postoperative MCVT. Postoperative D-dimer thresholds and risk stratification can be developed based on the correspondence between postoperative D-dimer and postoperative MCVT in cubic spline plots.
Footnotes
Author Contributions
Honghui Zhang: investigation, methodology, formal analysis, writing – original draft, writing – review & editing. Mengmeng Liu: investigation, writing – review & editing. Qi Qin: formal analysis, writing – review & editing. Aiqin Chu: resources, project administration, writing – review & editing. Lingyun Tian: conceptualization, project administration, investigation, data curation, writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (grant number 72304261), China Postdoctoral Science Foundation (grant number 2025M782290), the Research Funds of the Centre for Leading Medicine and Advanced Technologies of IHM (grant number 2025IHM01220), the 2025 Postgraduate Research Innovation Program of Bengbu Medical University (grant number Byycx25052) and Scientific Research Program of Colleges and Universities in Anhui Province (Natural Science Category) [grant number 2022AH051259].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.