
Abstract
Background
Neutrophil extracellular trap (NET) formation has emerged as a key driver of thrombosis in myeloproliferative neoplasms (MPNs). Its role in congenital bleeding disorders, however, remains unexplored.
Objectives
To investigate circulating citrullinated histone H3 (cit-H3), a marker of NETosis, in thrombosis-prone MPNs and bleeding-prone severe hemophilia A.
Methods
In a cross-sectional study, plasma cit-H3 was quantified by ELISA in patients with JAK2-mutated polycythemia vera or essential thrombocythemia, patients with severe hemophilia A, and matched healthy controls. Clinical and laboratory data were analyzed for associations with cit-H3 levels.
Results
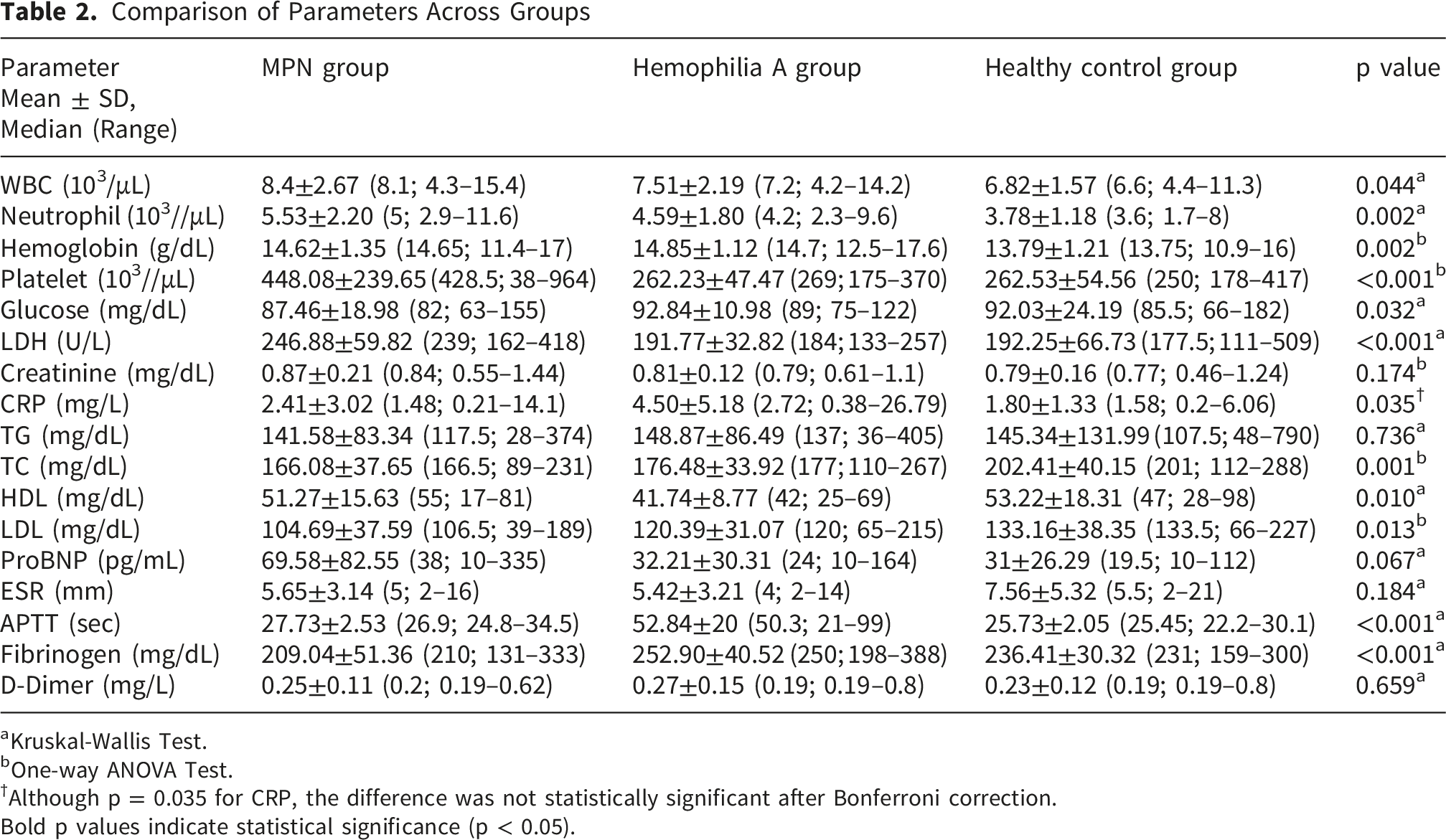
Eighty-nine participants were included: 26 with myeloproliferative neoplasms (MPNs), 31 with severe hemophilia A, and 32 healthy controls. Demographic characteristics were comparable across groups, though comorbidities were more frequent in MPNs. Laboratory analyses confirmed expected disease-specific differences, including elevated leukocyte, neutrophil, and platelet counts in MPNs and prolonged activated partial thromboplastin time in hemophilia A. Circulating citrullinated histone H3 (cit-H3) levels differed significantly among groups (p < 0.001), being lowest in controls, intermediate in MPNs, and highest in hemophilia A. Within disease groups, cit-H3 levels were unaffected by clinical variables such as MPN subtype, aspirin use, phlebotomy history, or factor replacement regimen.
Conclusions
Elevated circulating cit-H3 levels, suggestive of increased NETosis activity, were observed in both thrombosis-prone MPNs and bleeding-prone hemophilia A. These exploratory findings suggest a possible association between NET formation and thromboinflammatory processes across distinct hemostatic disorders.
Keywords
1. Introduction
Neutrophils play a central role in innate immunity and inflammation through mechanisms such as phagocytosis, oxidative burst, and the release of antimicrobial proteins. Beyond these classical functions, neutrophils are capable of releasing extracellular chromatin structures decorated with histones and granular enzymes, known as neutrophil extracellular traps (NETs).1,2 NET formation is a tightly regulated process involving reactive oxygen species generation, nuclear membrane disruption, and histone citrullination mediated by protein arginine deiminase 4, ultimately leading to chromatin decondensation and extracellular release.3-5
Accumulating evidence indicates that NET formation contributes to thromboinflammatory processes. Components of NETs, including histones, neutrophil elastase, and myeloperoxidase, promote platelet activation, enhance thrombin generation, and exert antifibrinolytic effects.6-8 In addition, NET associated histones and citrullination mediated modification of coagulation regulators impair the cleavage of von Willebrand factor, thereby facilitating thrombus formation.7,9 These observations underscore the close interaction between inflammation, innate immunity, and coagulation in the pathogenesis of venous thromboembolism.6,9,10
Myeloproliferative neoplasms are clonal hematologic disorders characterized by chronic inflammation and a markedly increased risk of arterial and venous thrombosis. Although classical clinical risk factors contribute to thrombotic events, the biological mechanisms underlying this prothrombotic state remain incompletely understood. Experimental and clinical studies have demonstrated enhanced NET formation by clonal myeloid cells in patients with myeloproliferative neoplasms, suggesting a mechanistic link between aberrant myelopoiesis and thromboinflammatory complications.11,12 However, data on circulating NET markers in patients who are not receiving cytoreductive therapy remain limited, and their clinical relevance is still being clarified.11,13
In contrast to myeloproliferative neoplasms, data regarding NET formation in congenital bleeding disorders are scarce. Hemophilia A is characterized by recurrent bleeding episodes and chronic joint inflammation, even in patients receiving replacement therapy. Experimental studies have shown that heme related molecules released during bleeding episodes can rapidly induce NET formation. 14 In line with this, recent clinical and experimental data suggest that NETs may contribute to synovial inflammation and joint damage in hemophilia, highlighting a potential role for neutrophil driven inflammatory pathways in disease related complications.15-17
Citrullinated histone H3 has been proposed as a relatively specific biomarker of NET formation and can be quantified in peripheral blood using ELISA based methods. 18 Measurement of circulating citrullinated histone H3 levels has also been associated with thrombotic risk in different clinical settings, supporting its potential utility as a circulating marker of NET activity. 19
This study was designed as an exploratory analysis to assess circulating citrullinated histone H3 (cit H3) as a marker of neutrophil extracellular trap (NET) formation across two clinically distinct conditions at opposite ends of the hemostatic spectrum—thrombosis-prone myeloproliferative neoplasms (MPNs) and bleeding-prone severe hemophilia A—compared with healthy controls. By examining these contrasting phenotypes, we aimed to explore the potential role of NETosis in hemostatic imbalance. A secondary objective was to evaluate associations between cit H3 levels and relevant clinical and laboratory parameters within each cohort.
2. Materials and Methods
2.1. Study Design and Participants
This study was designed as an observational cross sectional investigation and was conducted at the Hematology Outpatient Clinics of Istanbul University Cerrahpasa, Cerrahpasa Faculty of Medicine. Patients who attended the clinic between August 2023 and February 2024 were consecutively enrolled.
The study population was divided into three groups. Group 1 consisted of JAK2-positive polycythemia vera (PV, n=20) and essential thrombocythemia (ET, n=6) patients classified according to WHO diagnostic criteria, who were receiving no cytoreductive therapy other than acetylsalicylic acid and phlebotomy. None of the patients were receiving tyrosine kinase inhibitor or JAK inhibitor therapy at the time of enrollment. Group 2 included patients with severe hemophilia A, defined by a factor VIII activity level of one percent or lower. Group 3 comprised healthy volunteers who were selected to match the patient groups with respect to relevant demographic characteristics.
Patients with active infection, acute inflammatory conditions, recent surgery, or a history of malignancy other than myeloproliferative neoplasms were excluded from the study. All participants were evaluated during routine outpatient visits.
2.2. Data Collection Tools and Instruments
Venous blood samples were obtained from all participants during routine outpatient visits between 08:00 and 09:00 after an overnight fasting period. Blood samples were processed within the same hour and centrifuged at 3000 revolutions per minute for twenty minutes to separate plasma. The obtained citrated plasma samples were aliquoted into cryogenic tubes and stored at minus eighty degrees Celsius until laboratory analysis.
Demographic and clinical data including age, sex, body mass index, smoking status, comorbidities, history of thrombosis, and current treatments were collected retrospectively from electronic medical records. Laboratory parameters including complete blood count, activated partial thromboplastin time, fibrinogen, D dimer, and biochemical measurements were retrieved from patient files recorded at the time of study enrollment.
All laboratory analyses, except for citrullinated histone H3 measurement, were performed at the Hemostasis and Biochemistry Laboratories of Cerrahpasa Faculty of Medicine as part of routine clinical care.
2.3. ELISA Method
NET levels were determined in all patients and healthy volunteers using 4.5 ml sodium citrate blood samples and the Human Citrullinated Histone H3 ELISA test kit from Sunlong Biotech (SL3470Hu., Hangzhou, Zhejiang, China), which utilizes 96-well plates. The microplates in the kit were pre-coated with an antibody specific to citrullinated histone H3. Blood samples were processed using a standardized protocol for all participants. Plasma samples were separated by centrifugation immediately after collection and stored at −80°C until analysis. Reagents, samples, and standards were prepared according to the manufacturer’s protocol. Standards were diluted to a final volume of 50 µl. Each well received 50 µl of the standard or a mixture of 40 µl dilution buffer and 10 µl sample. The wells were sealed with a membrane cover and incubated at 37°C for 30 minutes.
After incubation, the plates were washed five times with 400 µl wash solution using an aspiration system. Except for the blank control well, 50 µl of Horseradish Peroxidase (HRP)-conjugated reagent specific for cit-H3 was added to each well. Subsequently, 50 µl of Chromogen Solution A and 50 µl of Chromogen Solution B were added to each well, and the plates were incubated in the dark at 37°C for 15 minutes. After the second incubation, the reaction was terminated by adding 50 µl of stop solution to each well.
The absorbance of each well was measured at 450 nm using a microplate reader. The optical density (OD) values were directly proportional to the concentration of cit-H3. The cit-H3 concentration in the samples was calculated in ng/ml by comparing the OD values to a standard curve. All measurements were performed according to the manufacturer’s instructions and under identical laboratory conditions.
2.4. Data Analysis
Descriptive statistics were presented as numbers and percentages for categorical variables and as mean, standard deviation, median, minimum, and maximum values for quantitative variables. The normality of the distribution of continuous variables was assessed using the Shapiro-Wilk test. For comparisons between two groups, the Independent Samples T-Test was used if the variables followed a normal distribution, and the Mann-Whitney U Test was applied otherwise. For comparisons among more than two groups, One-Way Anova was used for normally distributed variables, while the Kruskal-Wallis Test was employed for non-normally distributed variables. Pairwise comparisons for significant parameters were performed with Bonferroni corrections.
The relationship between quantitative variables was evaluated using Pearson correlation analysis for normally distributed variables and Spearman correlation analysis for non-normally distributed variables. All statistical analyses were performed using SPSS software (version 29.0.2.0, IBM Corp., Armonk, New York, USA), and a p-value of <0.05 was considered statistically significant.
3. Results
3.1. Participant Characteristics
A total of 89 participants were included in the study, comprising 26 patients with myeloproliferative neoplasms, 31 patients with severe hemophilia A, and 32 healthy controls (Figure 1). Baseline demographic and clinical characteristics of the study population are summarized in Table 1. Participant distribution flowchart Distribution of Participants by Descriptive Characteristics SD: Standard Deviation; BMI: Body Mass Index; DM: Diabetes Mellitus; MPN: Myeloproliferative Neoplasm.Data are presented as mean ± SD or n (%) as appropriate.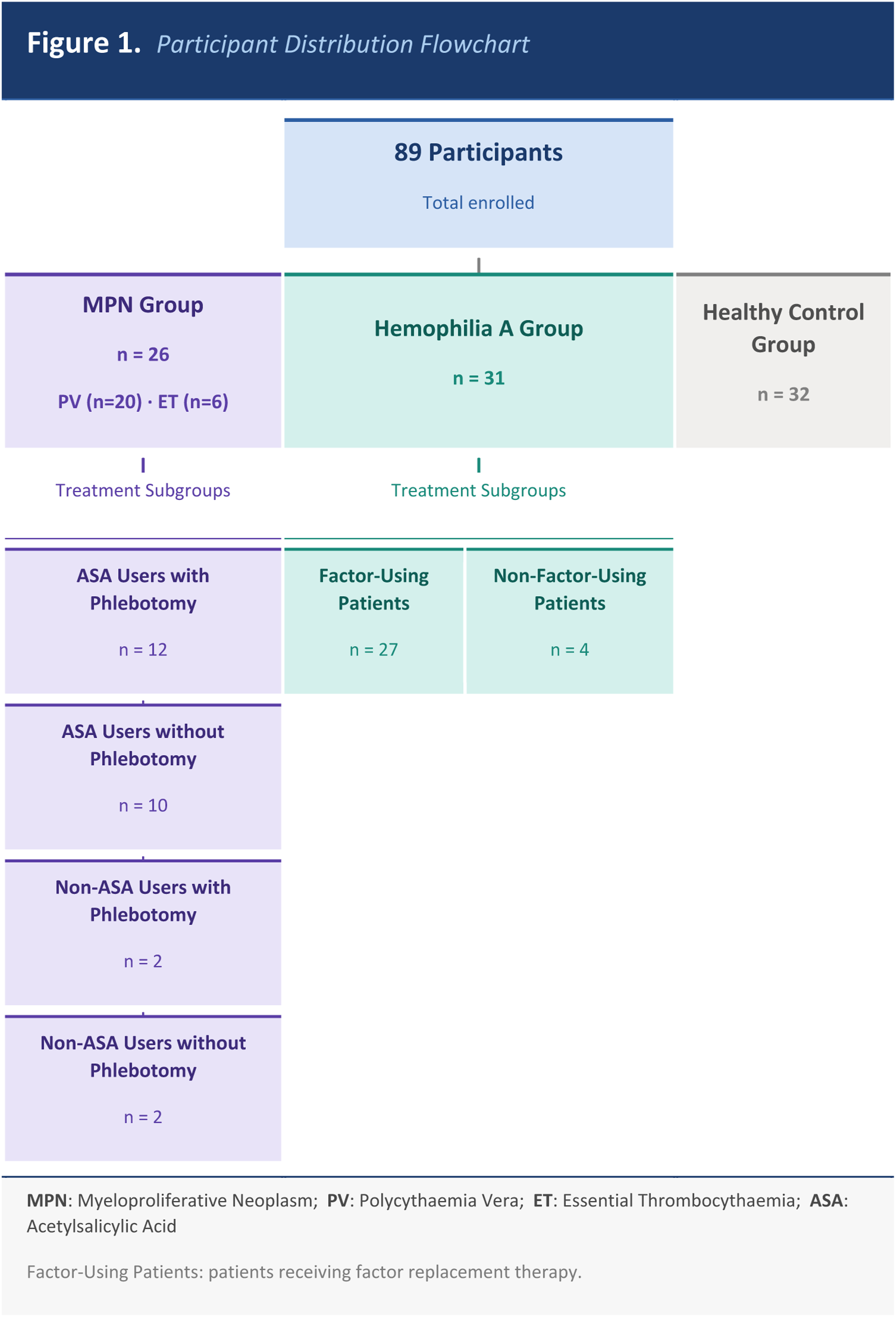
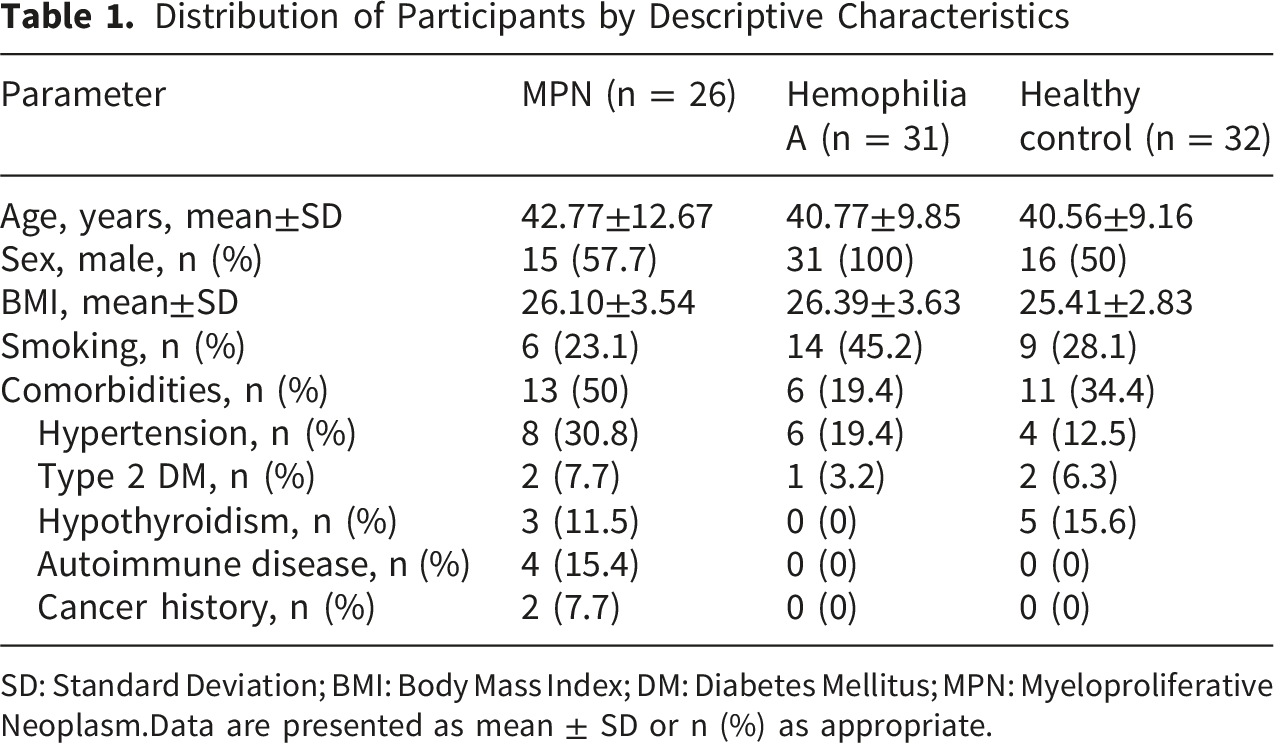
There were no significant differences among the three groups with respect to age or body mass index. As expected, all participants in the hemophilia A group were male, whereas sex distribution did not differ significantly between the myeloproliferative neoplasm group and healthy controls. Comorbid conditions were more frequently observed in patients with myeloproliferative neoplasms compared with the other study groups.
3.2. Laboratory Parameters Across Study Groups
Comparison of Parameters Across Groups
aKruskal-Wallis Test.
bOne-way ANOVA Test.
†Although p = 0.035 for CRP, the difference was not statistically significant after Bonferroni correction.
Bold p values indicate statistical significance (p < 0.05).
Activated partial thromboplastin time was markedly prolonged in patients with hemophilia A, whereas fibrinogen levels were lower in the myeloproliferative neoplasm group. Differences in inflammatory and lipid parameters among the study groups did not remain statistically significant after adjustment for multiple comparisons.
3.3. Circulating Citrullinated Histone H3 Levels
Circulating citrullinated histone H3 levels differed significantly among the three study groups (Figure 2). Levels were lowest in healthy controls, intermediate in patients with myeloproliferative neoplasms, and highest in patients with hemophilia A (p < 0.001). Comparison of Cit-H3 Levels Between Groups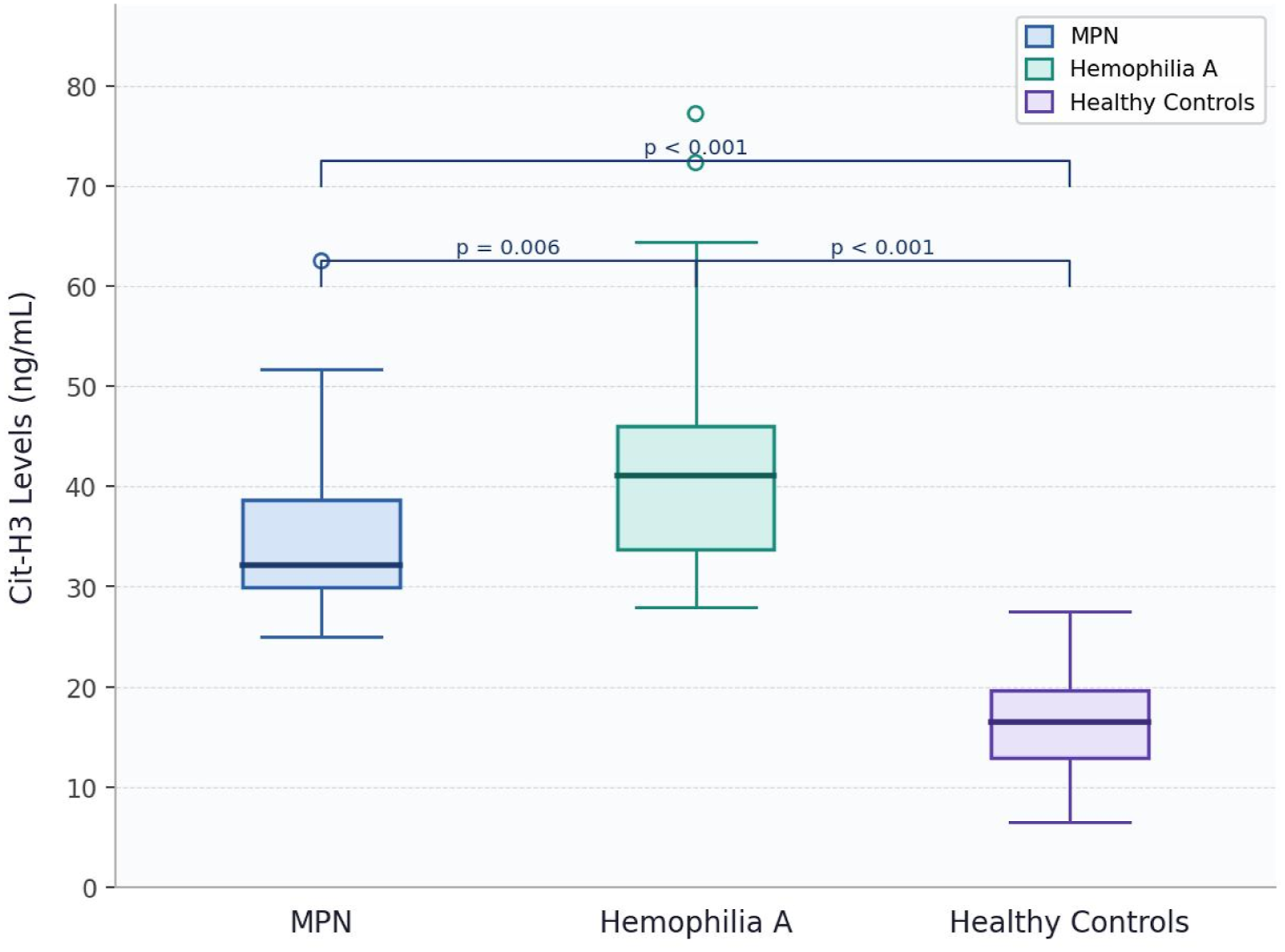
Within the myeloproliferative neoplasm group, citrullinated histone H3 levels did not differ significantly according to disease subtype, acetylsalicylic acid use, history of phlebotomy, or presence of hyperviscosity related symptoms. Similarly, no significant differences were observed in the hemophilia A group when patients were stratified according to the type of factor replacement therapy.
3.4. Correlation Analyses
When all participants were analyzed together, citrullinated histone H3 levels showed a weak positive correlation with neutrophil count and a weak negative correlation with total cholesterol levels. A moderate positive correlation was observed between citrullinated histone H3 levels and activated partial thromboplastin time (r = 0.52, p < 0.001) (Figure 3). Correlation of Cit - H3 levels with clinical variables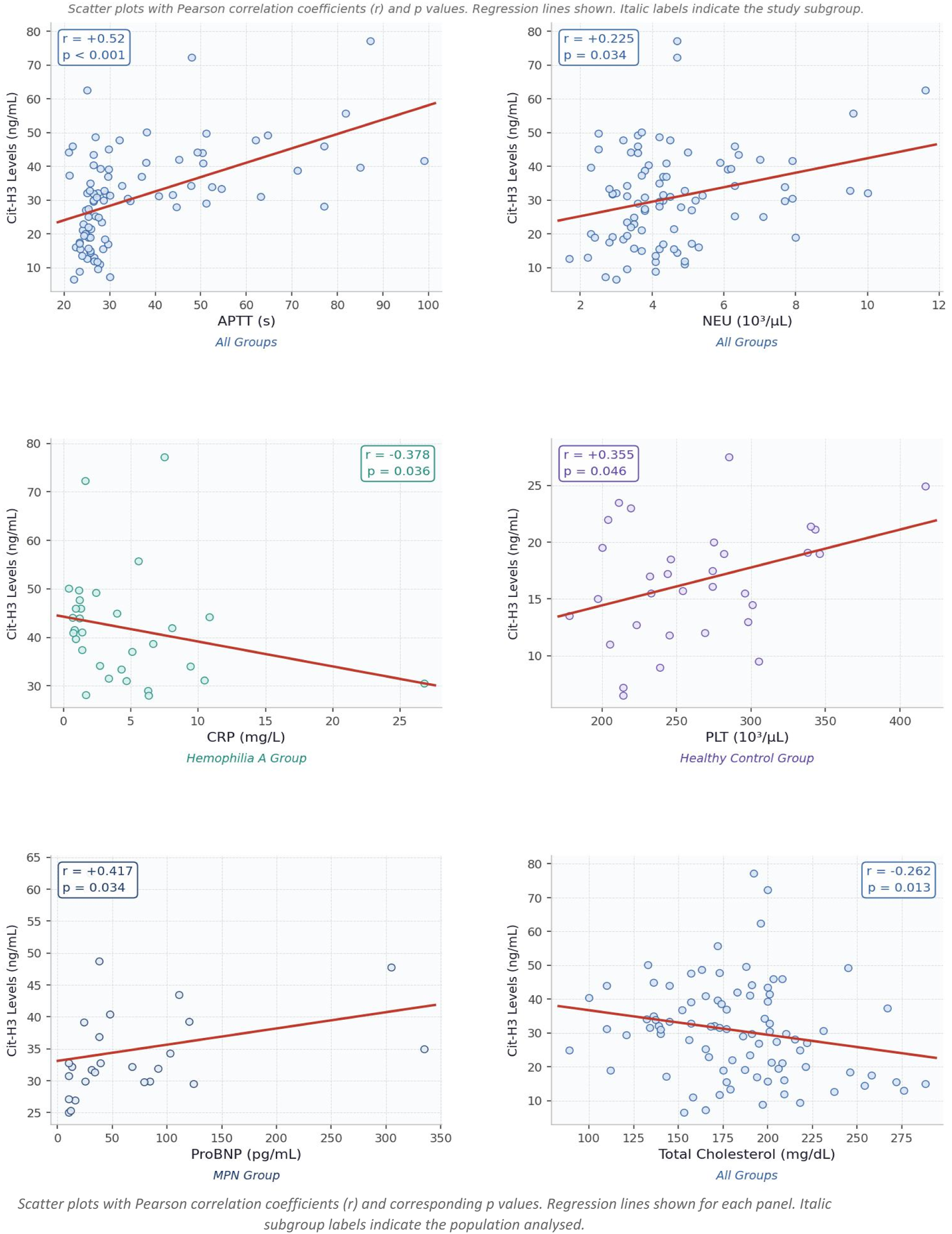
In subgroup analyses, citrullinated histone H3 levels demonstrated a weak negative correlation with C reactive protein levels in patients with hemophilia A. In patients with myeloproliferative neoplasms, a moderate positive correlation was observed between citrullinated histone H3 levels and pro brain natriuretic peptide levels. In healthy controls, a weak positive correlation was identified between citrullinated histone H3 levels and platelet count.
3.5. Additional Analyses
Citrullinated histone H3 levels were not significantly associated with age, body mass index, smoking status, or comorbidities when all participants were analyzed together. Although overall cit-H3 levels were higher in male participants than in female participants, sex based comparisons were limited to the myeloproliferative neoplasm and healthy control groups due to the sex distribution of the hemophilia A group.
Only one patient in the myeloproliferative neoplasm group had a history of thrombosis, which occurred in the portal vein twenty two months prior to study enrollment. The citrullinated histone H3 level in this patient was comparable to the median value of the myeloproliferative neoplasm group.
4. Discussion
NETosis, a form of neutrophil cell death, has been associated with various conditions, including autoimmune diseases, infections, cancer, vasculitis, thrombosis, atherosclerosis, and diabetes mellitus.1,2 In this study, citrullinated histone H3, a marker of NETosis, was measured in patients with MPN and hemophilia to investigate the relationship between NETosis and these disorders. Previous studies have demonstrated that cit-H3 levels are higher in MPN patients compared to healthy individuals, a finding that has also been observed in our study.12,13 However, in the study by Oyarzún et al, increased NETosis in unstimulated neutrophils was not detected in MPN patients. 11 This finding was attributed to the limited number of patients included in the study or the fact that the patients were undergoing cytoreductive therapy.
In our study, all MPN patients carried the JAK2 mutation. Consistent with this, a study by Schmidt et al reported that the JAK2 mutation is associated with increased NET levels. 11 Similarly, Massarenti et al identified a correlation between JAK2 allele burden and NET levels. 13 It has been reported in the literature that MPN patients with a history of thrombosis exhibit higher levels of NETosis.12,19 Nevertheless, in our study, the small number of patients with a history of thrombosis limited the ability to make a robust assessment of this subgroup. To clarify the role of NETosis in thrombosis development, well designed, long term prospective studies are needed.
Furthermore, the inhibitory effects of antiplatelet and anticoagulant drugs on NET formation complicate retrospective analyses of NETosis levels associated with thrombosis. In our study, no significant difference in cit-H3 levels was observed among the MPN subgroups. Nonetheless, Schmidt et al reported higher NETosis levels in patients with polycythemia vera compared to other myeloproliferative neoplasm subtypes. 12 However, Massarenti et al, in agreement with our findings, reported no significant difference in NETosis levels between patients with polycythemia vera and essential thrombocythemia. 13
No difference in cit-H3 levels was observed in MPN patients whether they were receiving phlebotomy or acetylsalicylic acid therapy. However, a study by Guy et al demonstrated that acetylsalicylic acid reduces plasma cit-H3 levels and decreases NETosis. 12 Studies examining the relationship between NETosis and blood counts or biochemical parameters have yielded varying results. For example, Oyarzún et al found that reactive oxygen species production and elevated leukocyte counts were associated with NETosis in MPN patients. 11 However, Schmidt et al reported no association between blood count parameters and NETosis in their study. 11
In hemophilia A patients, cit-H3 levels were found to be higher than in healthy individuals, suggesting a potential role for NETosis related to the complications observed in hemophilia, such as hemarthrosis.15-17 The literature indicates that heme related molecules play a significant role in the induction of NETosis and promote the rapid formation of NETs. 14 Czajkowska et al similarly demonstrated that plasma cit-H3 concentrations in hemophilia patients are higher than those in healthy individuals. 17
In our study, cit-H3 levels were higher in the hemophilia A group compared to both healthy individuals and the MPN group. Although this finding may appear biologically unexpected in a bleeding-prone disorder, several mechanisms may contribute to enhanced NETosis in hemophilia. Ongoing subclinical bleeding despite factor replacement therapy may promote NET formation through the release of proinflammatory molecules such as heme. 14 In addition, recurrent hemarthrosis, chronic arthropathy, and persistent inflammatory activation may also contribute to elevated circulating cit-H3 levels. Although exploratory, these findings may have potential clinical and translational implications, supporting the concept that NETosis-related inflammatory pathways may contribute to distinct hemostatic disorders. If validated in larger prospective studies, NETosis biomarkers such as cit-H3 may have potential utility in disease monitoring and risk stratification.18-20
One of the notable strengths of our study is the evaluation of NETosis and circulating cit-H3 levels across two hematologic conditions located at opposite ends of the hemostatic spectrum. In addition, the inclusion of relatively homogeneous patient populations, including JAK2-mutated MPN patients and patients with severe hemophilia A, may have reduced disease-related heterogeneity. The assessment of both overall patient groups and disease-specific subgroups also provided a broader exploratory overview of NETosis-related patterns.16,21
Nevertheless, several limitations should be acknowledged. First, this was a single-center study with a relatively small sample size, which may limit the generalizability of the findings. The relatively limited sample size, particularly in subgroup analyses, may also have reduced the statistical power to detect subtle differences across clinical strata. In addition, potential confounding factors, including sex imbalance between groups and differences in inflammatory burden and treatment regimens, could not be fully controlled because multivariable adjustment analyses were not performed. Detailed clinical data for the hemophilia cohort, including bleeding phenotype, history of hemarthrosis, inhibitor status, chronic arthropathy, and prophylactic treatment regimens, were not consistently available and therefore could not be incorporated into the analysis. These factors may have influenced circulating cit-H3 levels independently of disease-related NETosis activity. 17
Finally, although cit-H3 is considered a relatively specific marker of NETosis, additional complementary markers such as cell-free DNA or MPO–DNA complexes were not assessed, which may limit the robustness of NET quantification. ANC-normalized cit-H3 analyses were also not performed and may represent a useful approach for future studies to better distinguish increased per-cell NETosis activity from overall neutrophil burden. In addition, despite partial correction for multiple comparisons, the possibility of type I error cannot be completely excluded. Therefore, given the exploratory and hypothesis-generating nature of the study, these findings should be interpreted cautiously and validated in larger prospective mechanistic studies.21,22,23
5. Conclusion
Elevated circulating cit-H3 levels were observed in patients with JAK2-mutated myeloproliferative neoplasms not receiving cytoreductive therapy and in patients with severe hemophilia A, suggesting increased NETosis activity in these groups. These findings may support a possible association between NETosis and thromboinflammatory pathways across distinct hematologic disorders. However, given the cross-sectional design, the results should be considered exploratory and hypothesis-generating. Further prospective and mechanistic studies are needed to clarify the clinical implications and therapeutic relevance of these findings.
Footnotes
Ethical Considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Istanbul University Cerrahpasa Cerrahpasa Faculty of Medicine Clinical Research Ethics Committee (approval date July 24, 2023; approval number 83045809 604 01 01 739610). Written informed consent was obtained from all participants prior to enrollment.
Author Contributions
Conceptualization: M C A, S O, Study design: M C A, S O, Data collection and processing: S O, T E, A S, D O, M D O C, Z B, Analysis and interpretation: I M B, M C A, S O, A E E, Manuscript drafting: S O, M C A, All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.