
Abstract
Objectives
To systematically review and critically evaluate the risk prediction models for DVT in patients with sICH and provide references for clinical practice.
Methods
PubMed, Web of Science, The Cochrane Library, CINAHL, Embase, Scopus, CNKI, Wanfang Database, and China Science and VIP were searched from inception to July 15, 2025. Two researchers independently screened the literature, extracted data and assessed the risk of bias and applicability using the PROBAST checklist. The AUC values were pooled using a random-effects model. Sensitivity and subgroup analyses were conducted to explore potential sources of heterogeneity.
Results
A total of 9414 studies were initially identified, 19 risk prediction models were developed across the 15 included studies. The reported AUC across the 15 included studies ranged from 0.710 to 0.988. The pooled AUC for the 11 validated models was 0.82 (95% confidence interval: 0.78-0.85). Age, D-dimer levels, hematoma volume, and GCS score on admission emerged as the most frequently significant predictors of DVT in sICH patients.
Conclusions
Existing models show promising but not yet robust discriminative properties. Owing to the high risk of bias and substantial heterogeneity across studies, these models cannot be directly applied to routine clinical decision-making. Key variables including age, D-dimer level, hematoma volume and GCS score can support qualitative clinical risk stratification, and provide practical reference for formulating precise and individualized thromboprophylaxis strategies for sICH patients.
Keywords
Introduction
Spontaneous intracerebral hemorrhage (sICH) is one of the most disabling and deadly subtypes of stroke. 1 Recent epidemiological data reveal that sICH affects approximately 3.4 million individuals worldwide, with a two-year mortality rate as high as 49.5%, highlighting its significant public health burden.2,3 Patients with sICH are at significantly increased risk of venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), due to factors such as limb paralysis, impaired consciousness and prolonged bed rest. 4 The risk of VTE in sICH patients is 2-4 times higher than that in patients with ischemic stroke, 5 with a reported overall incidence ranging from 3% to 22.49% across multicenter cohorts.6-8 Furthermore, in-hospital VTE is independently associated with increased mortality and poor long-term prognosis in patients with sICH. 9
Accurate identification of DVT risk factors, early risk stratification and timely prevention are therefore essential to improve clinical outcomes in sICH patients. Currently, several well-established thrombosis risk assessment tools, including the Caprini Risk Assessment Model, Padua Scale and Autar Scale, are routinely used in clinical practice. 10 However, these models were largely developed based on general inpatient populations and fail to adequately incorporate disease-specific clinical features unique to sICH patients. Consequently, they demonstrate limited discriminative performance and poor adaptability in sICH populations, making it difficult to meet the needs of precise clinical risk stratification.
In recent years, several studies have developed and validated corresponding DVT prediction models specifically tailored for sICH patients.8,11 These models incorporate a concise set of predictors that capture disease-specific characteristics, such as hematoma volume and Glasgow Coma Scale (GCS) score. However, these models vary greatly in sample size, modeling approaches and study design. To date, no systematic review or meta-analysis has quantitatively pooled their predictive performance or comprehensively evaluated their methodological quality. The comparative superiority and clinical applicability of these models remain unclear, which has hindered their translation into routine clinical practice. Therefore, this study aims to systematically evaluate existing DVT risk prediction models for sICH patients, critically appraise their methodological quality and predictive performance, identify key predictive factors, and explore their potential for clinical implementation. The findings are expected to provide evidence-based support for DVT risk stratification, individualized intervention, and the future development of high-quality prediction models in this population.
Methods
This systematic review was conducted in accordance with the TRIPOD-SRMA (Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis: Systematic Review and Meta-Analysis) reporting guidelines, to ensure methodological rigor and reporting transparency. 12 Additional methodological details are available in the Supplementary File 1. The study protocol was registered on PROSPERO (registration number: CRD42024600505).
Search Strategy
Two investigators (Y.X. and L.W.) independently performed comprehensive literature searches in nine databases: PubMed, Web of Science, The Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, Scopus, China National Knowledge Infrastructure (CNKI), Wanfang Database, and China Science and Technology Journal Database (VIP). Supplementary searches of grey literature sources included the China Clinical Trials Registry, Chinese Cochrane Center, Open Grey, and GreyNet International. The search encompassed publications from database inception through July 15, 2025, with language restrictions to English and Chinese. We developed a systematic search strategy using a combination of Medical Subject Headings (MeSH) and free-text terms, encompassing keywords such as: “deep vein thrombosis”, “venous thrombosis”, “phlebothrombosis”, “VTE”, “DVT”, “spontaneous intracerebral hemorrhage”, “cerebral hemorrhage”, “ICH”, “intracranial bleeding”, “risk prediction model”, “risk factor”, “predictor”, “model” and “Nomogram”. The complete search strategies for all databases are available in Supplementary File 2. To ensure literature saturation, we manually examined reference lists of all included studies and relevant review articles. Any discrepancies in search results or study identification were resolved through consensus discussions with a third arbitrator (R.Z.).
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Study subject: adult patients with sICH. (2) Scope of research: research focused on the development or validation of a risk prediction model for DVT in patients with sICH. (3) Study design: a case-control, cohort or cross-sectional design. (4) Language: publications in the English or Chinese language.
Exclusion Criteria
(1) Patients with traumatic intracerebral hemorrhage, or extraparenchymal hemorrhage (e.g. subdural hematoma, subarachnoid hemorrhage). (2) Studies that only examined risk factors without developing a prediction model. (3) Models with less than two predictor variables. (4) Complete text not accessible. (5) Repetitive publications.
Literature Screening and Data Extraction
Two researchers (Y.X. and T.W.) independently conducted literature screening and cross-verification. All discrepancies were resolved through discussion with the corresponding author (R.Z.) until consensus was achieved. Initially, duplicate records were removed using NoteExpress software. Subsequently, titles and abstracts of the remaining articles were screened to exclude clearly irrelevant studies. Finally, a full-text review was further scrutinized to select eligible articles.
A standardized data extraction form was developed following the guidelines of the Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modeling Studies (CHARMS) checklist. 13 Corresponding authors were contacted to obtain missing data when necessary. The extracted information was categorized into two groups: (1) Basic information: author, publication year, country, study design, study subject, study site, main outcome, DVT incidence; (2) Model information: encompassed information related to the prediction model, including the processing method of missing value, variable screening method, modeling method, model performance (AUC value, sensitivity and specificity of the model), calibration method, final predictors, validation method and presentation form of prediction model. Two reviewers (L.W. and W.S.) independently performed the data extraction, which was subsequently verified by a third reviewer (Y.Y.) to ensure accuracy and consistency.
Assessment of Bias Risk in the Included Articles
Two reviewers (Y.X. and F.W.) independently assessed the methodological quality and applicability of the included studies using the Prediction Model Risk of Bias Assessment Tool (PROBAST) checklist. Any discrepancies in assessment were resolved through consensus or by consultation with a third reviewer (Y.Y.). PROBAST is a validated tool designed for the critical appraisal of studies that develop, validate or update prediction models. 14 It contains 20 signaling questions categorized into four domains: participants, predictors, outcome and analysis. Risk of bias was judged as “low”, “high” or “unclear” at both the domain and overall levels. A domain was considered to have a high risk of bias if at least one question within it was rated “no” or “probably no”. The overall risk of bias was rated as low only if all domains were judged to be at low risk. Applicability was assessed across three domains (participants, predictors and outcome) and rated using the same categories (“low”, “high” or “unclear”).
Data Synthesis and Statistical Analysis
All meta-analyses of model performance were performed using Stata 17.0, with the area under the curve (AUC) and its 95% confidence interval (95% CI) serving as the primary effect measure. It is important to note that the C statistic equivalent to the AUC, ranges from 0.5 to 1, with higher values indicating superior discriminatory performance. 15 Heterogeneity of studies was assessed by Cochran’s Q test and I2index. A fixed-effect model was applied when heterogeneity was negligible (P> 0.1 and I2< 50%), otherwise, a random-effects model was used. Statistical significance was set at P<0.05. To explore potential sources of heterogeneity, we conducted sensitivity analyses by sequentially excluding individual studies, as well as pre-specified subgroup analyses. Publication bias was assessed using Egger’s test, with P>0.05 indicating a low likelihood of publication bias.
Results
Study Selection
The initial search identified 9414 records from the databases, while no additional eligible studies were identified through grey literature sources. After removing 2344 duplicates, 7070 records underwent title and abstract screening, of which 100 articles were deemed potentially eligible for full-text review. During the subsequent evaluation, 85 studies were excluded with the following reasons: eight were literature type mismatches, 41 did not develop a predictive model or focused solely on risk factors, 26 involved an inconsistent study population, six had outcome indicators inconsistent with the review objectives, two were duplicate publications, and two lacked reported AUC values. Consequently, 15 studies comprising 19 prediction models were included in the final systematic review. The study selection process is illustrated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram (Figure 1), and a complete list of excluded studies with specific reasons is provided in Supplementary File 3. PRISMA flowchart of study search and selection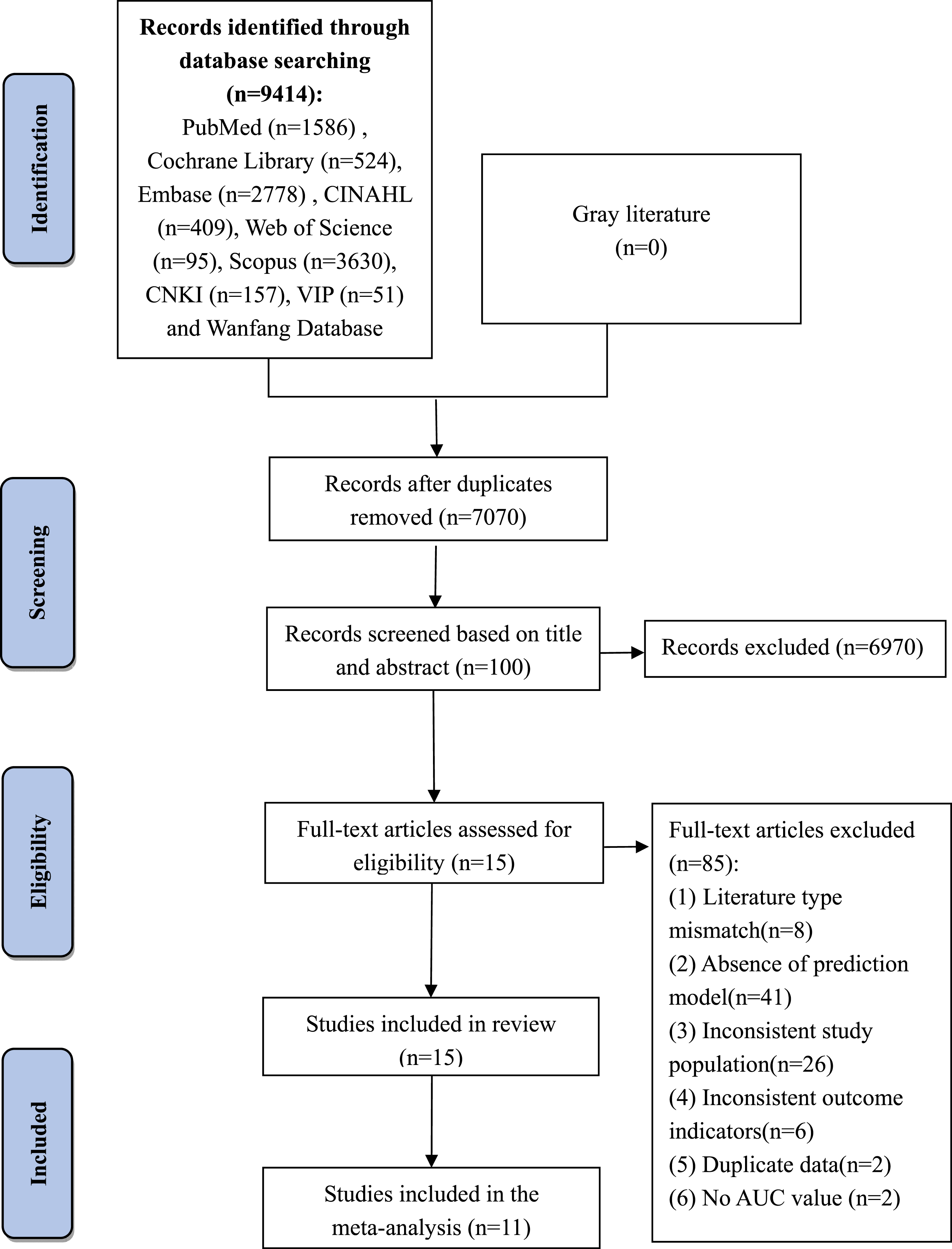
Study Characteristics
Basic Characteristics of the Included Studies (n= 15)
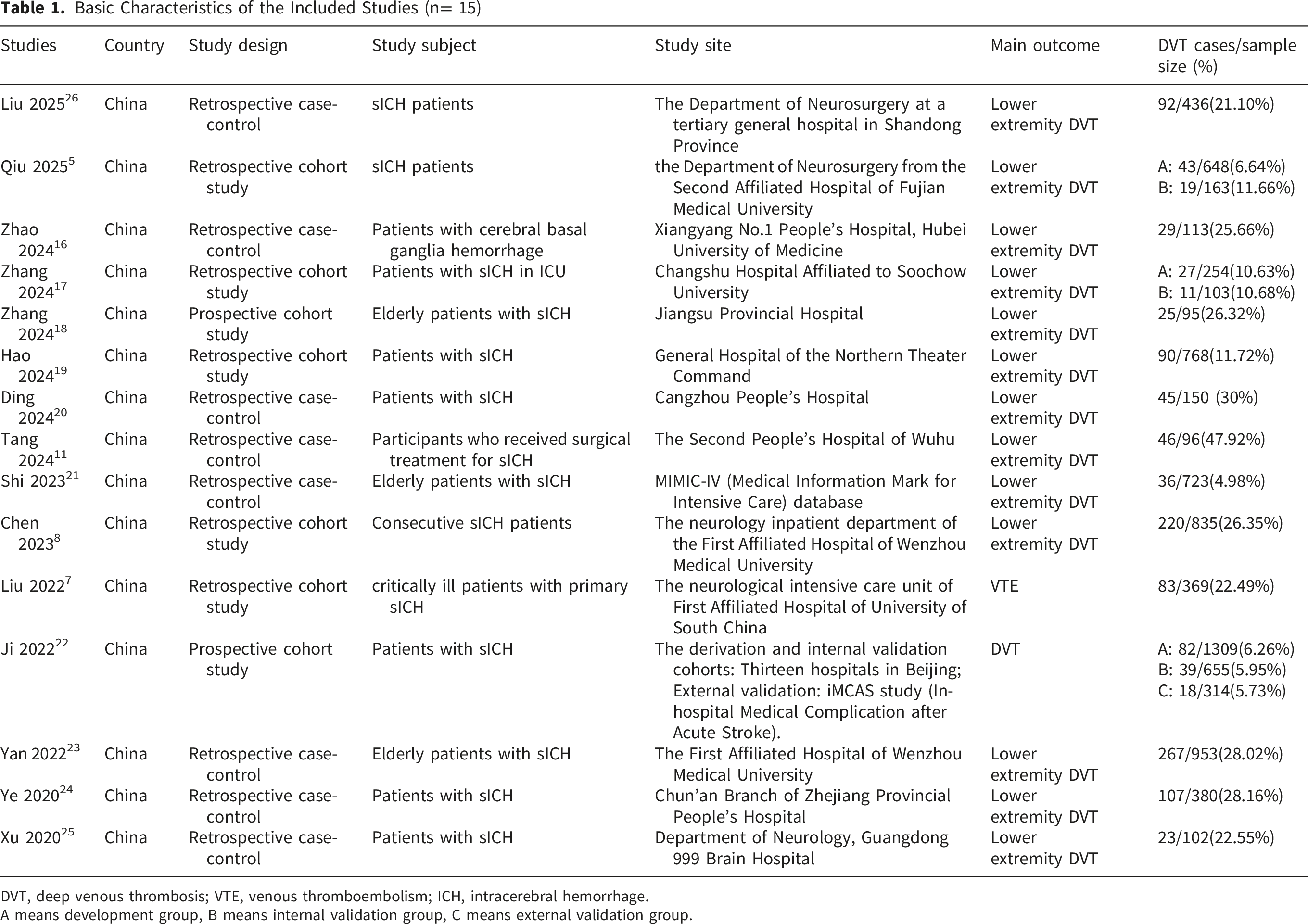
DVT, deep venous thrombosis; VTE, venous thromboembolism; ICH, intracerebral hemorrhage.
A means development group, B means internal validation group, C means external validation group.
Model Performance
A total of 19 risk prediction models for DVT in patients with sICH were developed across the 15 included studies. Regarding variable selection, four studies5,16,19,20 utilized the least absolute shrinkage and selection operator (LASSO) method, while the remaining studies primarily employed univariate and multivariate logistic regression. Two studies5,26 adopted machine learning algorithms such as the random forest (RF) and support vector machine (SVM) for model development, whereas the other 13 studies constructed prediction models using logistic regression. Age and D-dimer were the most frequently incorporated predictors, appearing in eight and five models, respectively. Hematoma volume was also commonly utilized, featured in five models. Other recurrent predictors included smoking history, GCS score on admission, and central venous catheterization (CVC), each of which was included in three distinct models.
Overview of the Information of the Included Prediction Models (n=15)
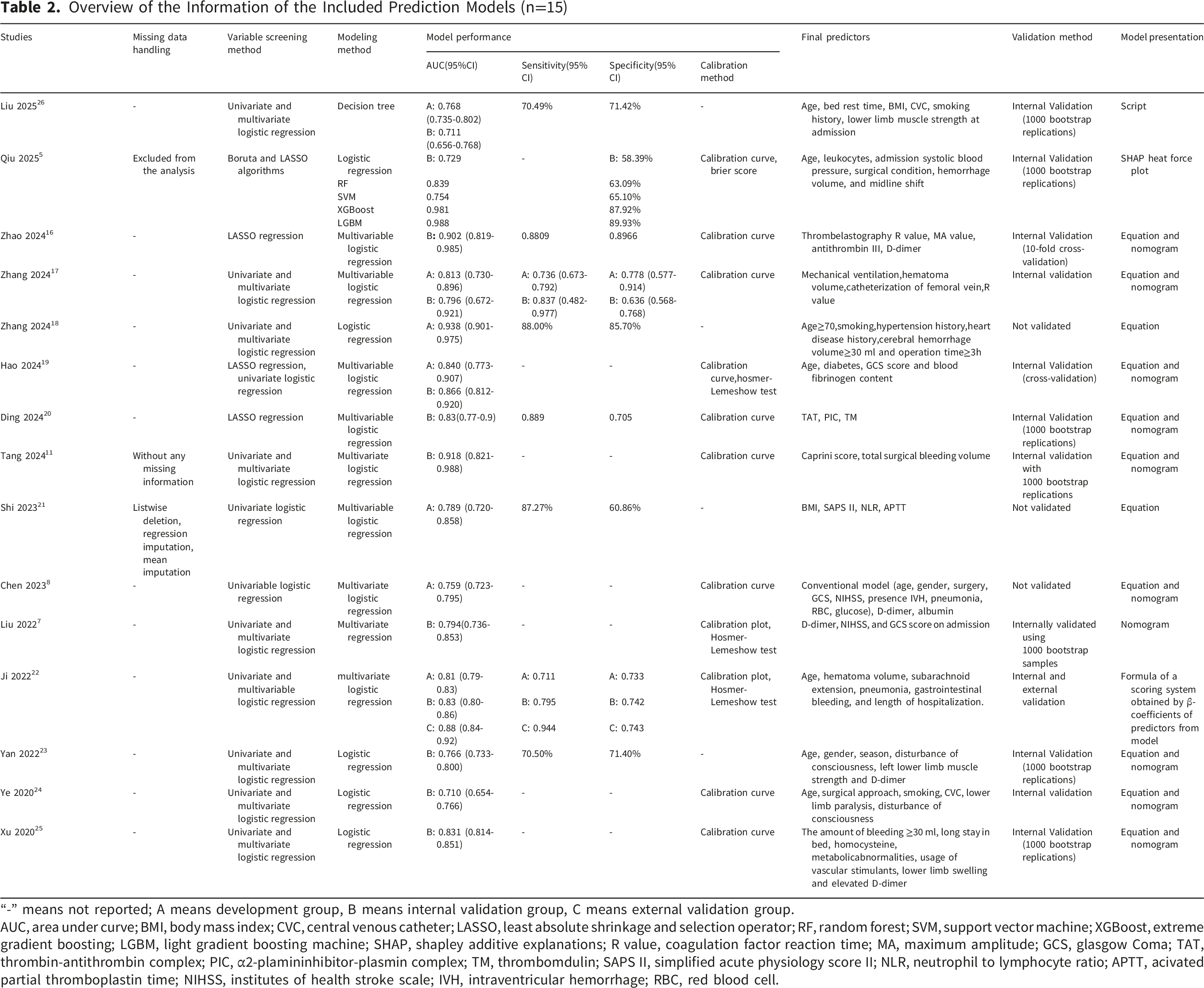
“-” means not reported; A means development group, B means internal validation group, C means external validation group.
AUC, area under curve; BMI, body mass index; CVC, central venous catheter; LASSO, least absolute shrinkage and selection operator; RF, random forest; SVM, support vector machine; XGBoost, extreme gradient boosting; LGBM, light gradient boosting machine; SHAP, shapley additive explanations; R value, coagulation factor reaction time; MA, maximum amplitude; GCS, glasgow Coma; TAT, thrombin-antithrombin complex; PIC, α2-plamininhibitor-plasmin complex; TM, thrombomdulin; SAPS II, simplified acute physiology score II; NLR, neutrophil to lymphocyte ratio; APTT, acivated partial thromboplastin time; NIHSS, institutes of health stroke scale; IVH, intraventricular hemorrhage; RBC, red blood cell.
Risk of Bias and Applicability Evaluation
PROBAST Results of the Included Studies (n=15)
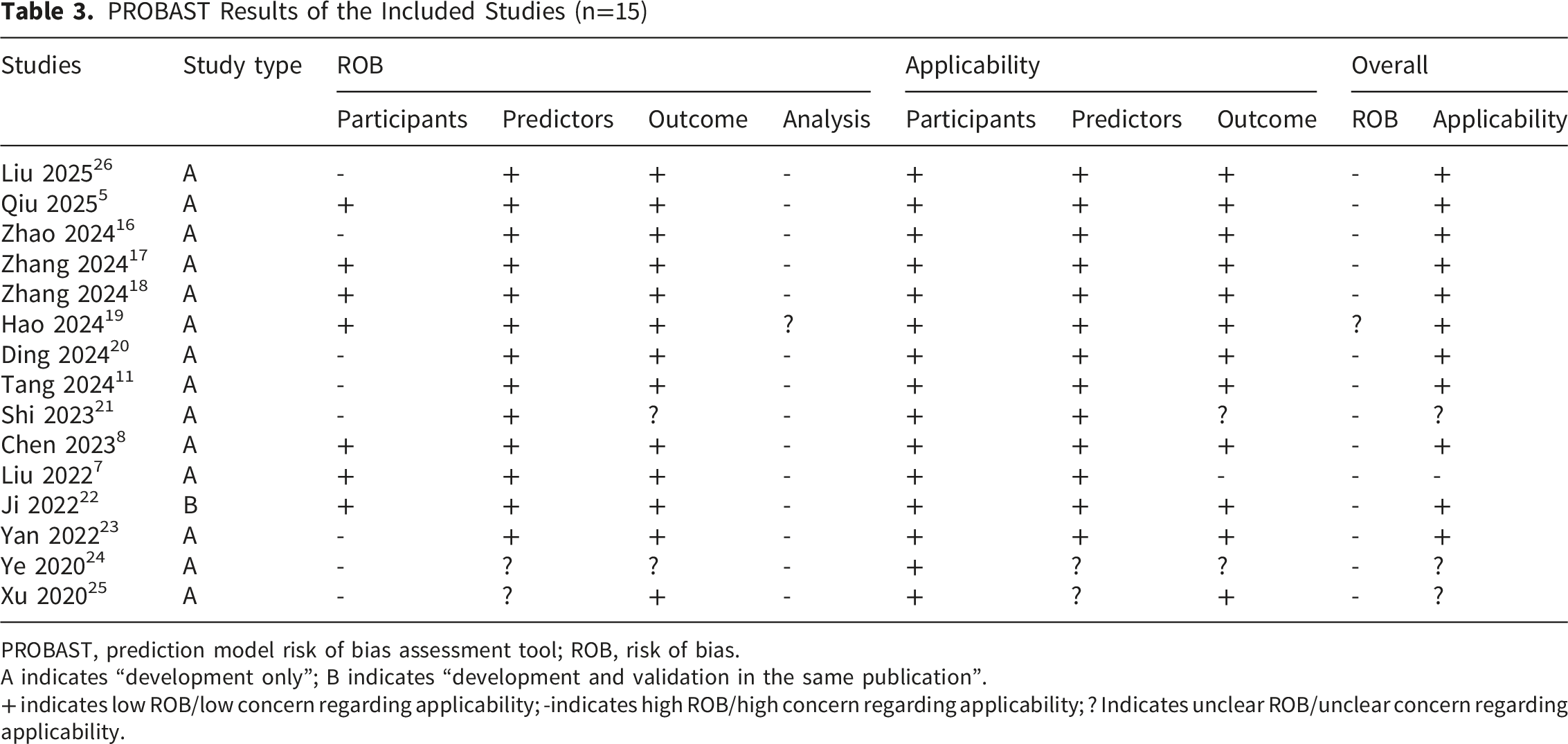
PROBAST, prediction model risk of bias assessment tool; ROB, risk of bias.
A indicates “development only”; B indicates “development and validation in the same publication”.
+ indicates low ROB/low concern regarding applicability; -indicates high ROB/high concern regarding applicability; ? Indicates unclear ROB/unclear concern regarding applicability.
In the analysis domain, 14 studies were rated as high risk of bias, with the remaining one 19 judged as unclear. Notably, 11 studies5,8,16-18,20-22,24-26 employed inadequate sample sizes that failed to meet the recommended threshold of 20 events per variable (EPV). In four studies,5,17,18,22 continuous variables such as age and intracerebral hemorrhage volume were converted into categorical variables without pre-defined cutoff criteria, introducing substantial bias. The handling of missing data remained largely unreported: only one study 11 explicitly stated the absence of missing data, while two others5,21 simply excluded incomplete cases, leaving the risk of bias unclear in the remaining studies. Additionally, 11 studies7,8,11,17,18,21-26 were considered high risk of bias due to variable selection based solely on univariate analysis. Regarding model performance assessment, four studies18,21,23,26 failed to assess model calibration, and three studies8,18,21 did not account for overfitting, underfitting, or optimism in their performance estimates.
Regarding applicability, 11 studies were rated as low risk, three studies21,24,25 were classified as unclear risk, and one study
7
was judged as high risk. In the participant domain, all studies provided sufficiently detailed participant characteristics. In the predictor domain, two studies24,25 demonstrated unclear risk of bias due to mismatches between predictor definitions, measurement methods, timing and the systematic review objectives. Regarding outcome domain, one study
7
was rated high risk because it combined DVT with PE as a composite outcome, while two others21,24 were deemed unclear due to insufficient reporting of outcome assessment methods. A summary of the overall risk of bias across all included studies is presented in Figure 2, with detailed results available in the Supplementary File 4. Risk of bias across all included studies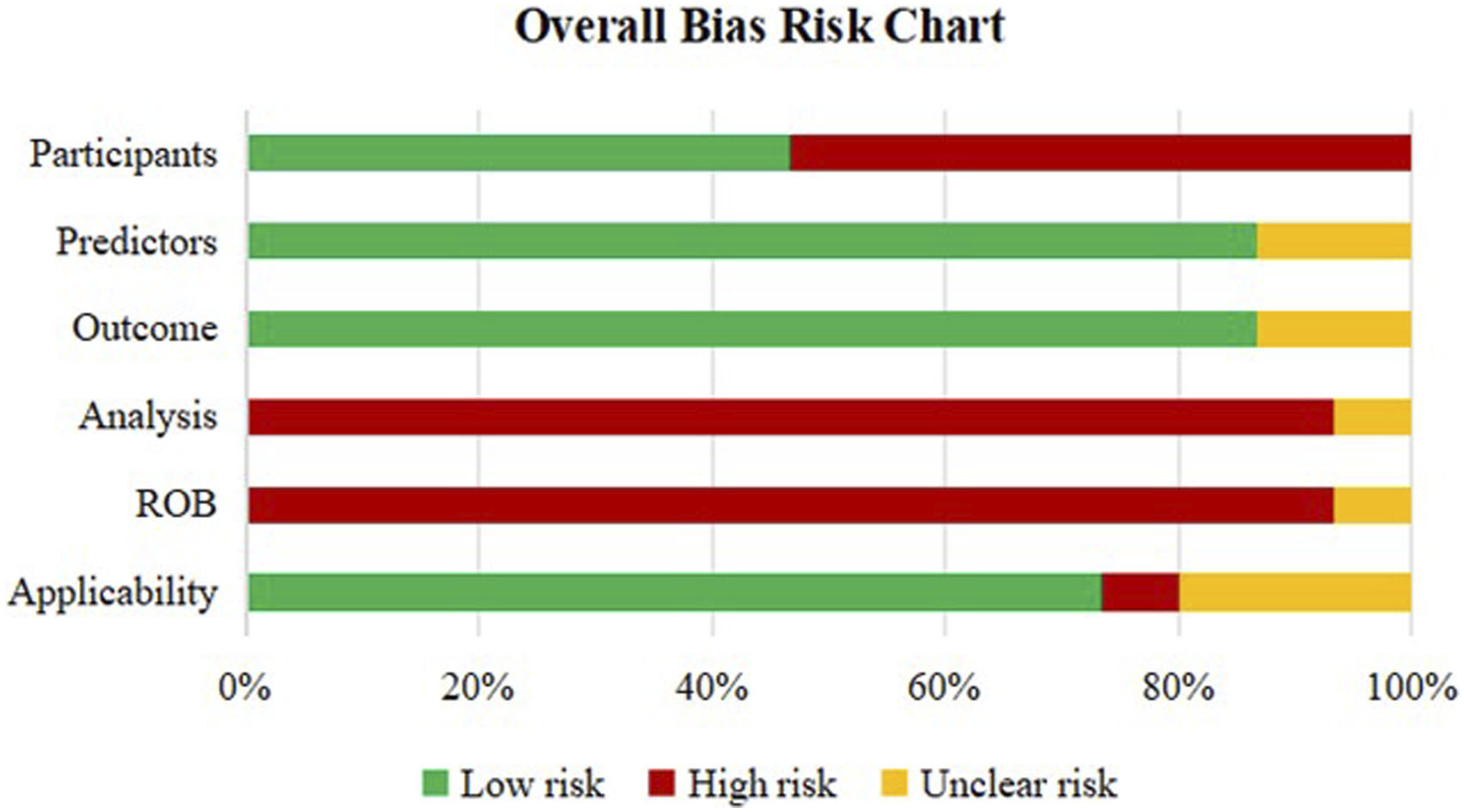
Meta-Analysis of Validation Models Included in the Review
Due to insufficient reporting on the development details of the models in the included studies, only 11 studies7,11,16,17,19,20,22-26 provided adequate data for meta-analysis. Among these, one study
22
conducted both internal and external validation of the model, and its externally validated AUC was included in the pooled analysis. A random-effects model was used to synthesize the AUC values. The overall pooled AUC was 0.82 (95% CI: 0.78-0.85) (Figure 3A), indicating promising discriminative performance. The I
2
value was 83.0% (p=0.000), suggesting significant heterogeneity among the studies. In the subgroup of 10 studies with DVT (excluding VTE) as the outcome, the pooled AUC was 0.82 (95% CI: 0.78-0.86) (Figure 3B), though with high heterogeneity (I
2
=84.5%, p=0.000). Similarly, among the 10 non-machine learning prediction models, the combined AUC was 0.83 (95% CI: 0.79-0.86) (Figure 3C), again suggesting promising performance, with considerable heterogeneity (I
2
=80.1%, p=0.000). Forest plot of the pooled AUC values of validation models: (A) all 11 validation models; (B) 10 validation models with DVT as the outcome; (C) 10 non-machine learning validation models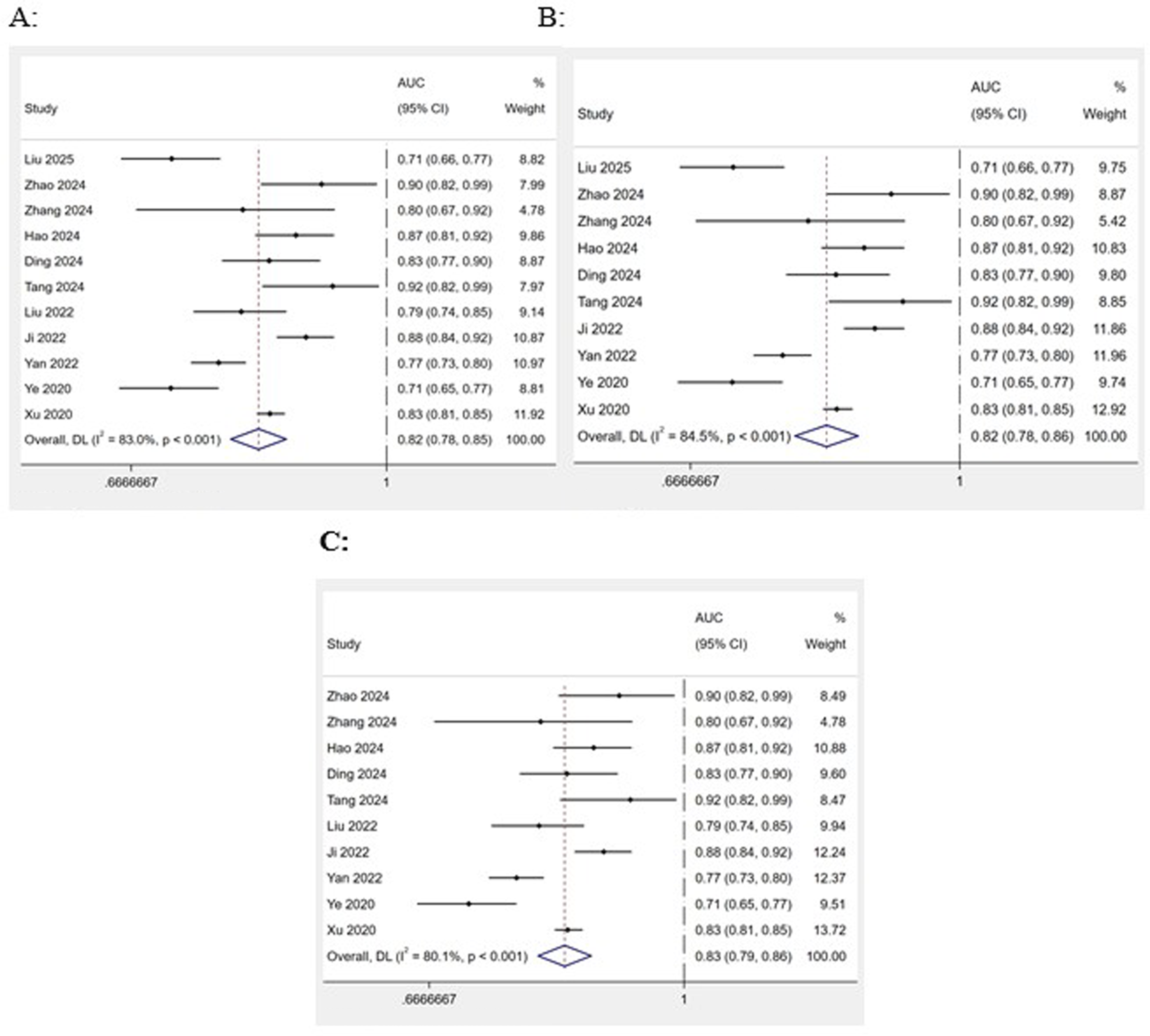
Subgroup Analysis
To explore potential sources of heterogeneity, we conducted a subgroup analysis stratified by ICU admission status (ICU vs. non-ICU patients). The findings revealed that the subgroup of Non-ICU patients exhibited a significant heterogeneity with p< 0.001 and I
2
=87.0%. The AUC value was 0.81(95% CI: 0.77-0.85), indicating a reasonable model performance. This heterogeneity may be attributable to variations in age, functional mobility, and comorbidity burden among sICH patients. By contrast, the ICU subgroup exhibited moderate, non-significant heterogeneity (I
2
=58.2%, p=0.092) and an AUC of 0.83 (95% CI: 0.76-0.91), indicating acceptable model performance in this population (Figure 4). The subgroup analysis of the pooled AUC values of validation models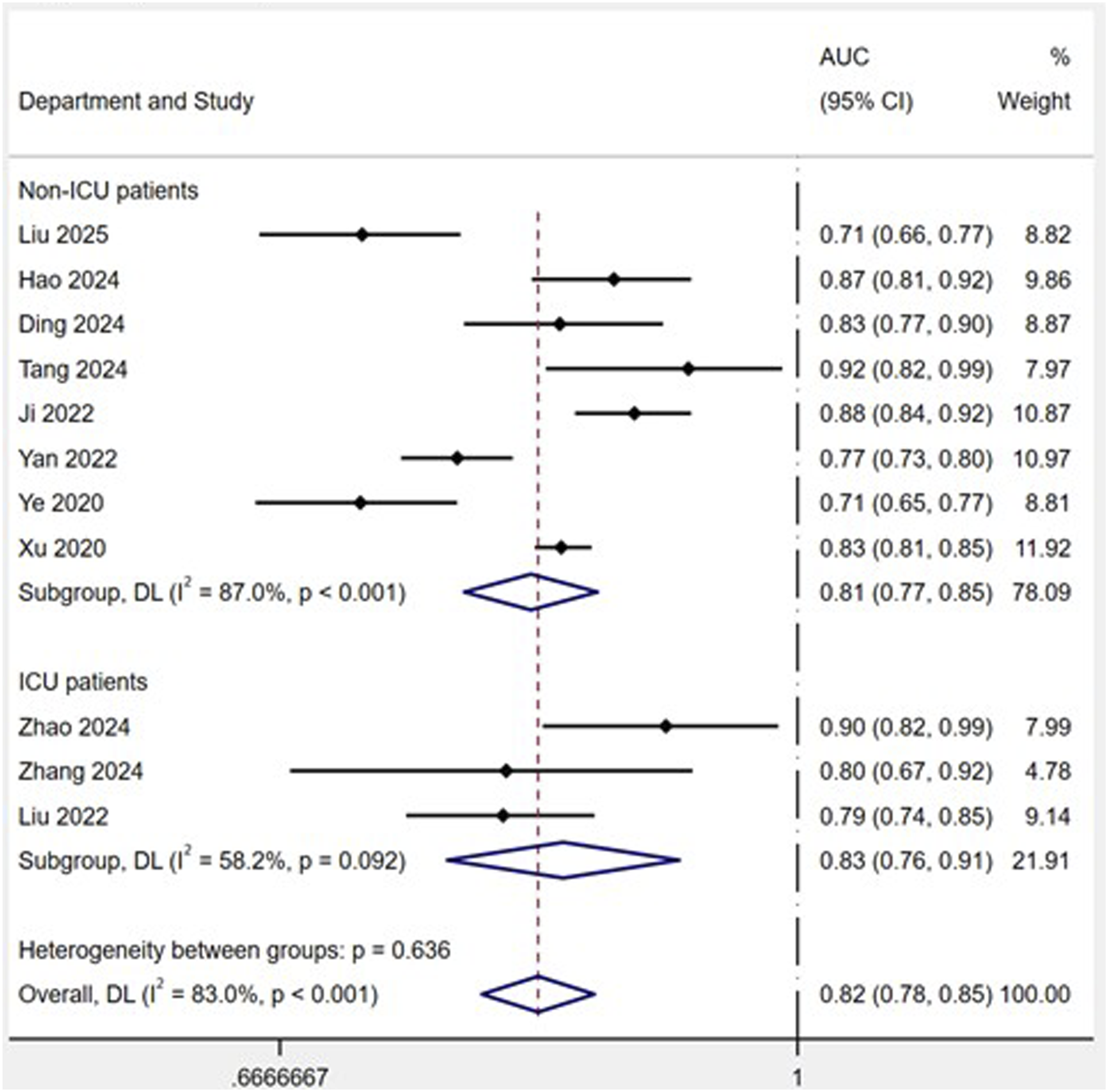
Sensitivity Analysis
After systematically removing individual studies, the pooled AUC remained stable, ranging from 0.81 to 0.83, indicating that no single study exerted undue influence on the overall results. Moreover, Egger’s test yielded a p-value of 0.678, indicating no significant publication bias.
Discussion
DVT is a common and severe complication in patients with sICH, which markedly increases long-term mortality and seriously impairs neurological rehabilitation and long-term functional prognosis. 27 Therefore, early and accurate identification of high-risk individuals for DVT and implementation of individualized risk stratification are of great clinical significance for standardizing thromboprophylaxis strategies and improving the overall prognosis of sICH patients. This systematic review identified 19 evaluated models for DVT in sICH patients. All models exhibited favorable predictive performance, with reported AUC values ranging from 0.710 to 0.988. The meta-analysis of 11 validated models yielded a pooled AUC of 0.82 (95% CI: 0.78-0.85), which statistically reflected the overall discriminative ability of existing models. However, most of the included studies were rated as having a high risk of bias, which may have overestimated the actual predictive performance of the models. Meanwhile, substantial heterogeneity was observed across studies, presumably attributed to discrepancies in patient populations, candidate predictor selection, and methodological design among individual studies. The coexistence of high bias risk and substantial heterogeneity markedly weakened the interpretability and reliability of the pooled AUC. In brief, although current models show promising discriminative potential, their predictive robustness remains insufficient, and the pooled AUC should not be overinterpreted for clinical application.
sICH patients admitted to the ICU are in critical condition, exposed to frequent invasive procedures and prolonged immobilization, leading to a remarkably higher DVT risk than those in general wards. Evidence indicates that DVT prediction models for critically ill sICH patients may differ significantly from those designed for non-ICU settings.7,18 To explore the potential sources of heterogeneity, we performed a subgroup analysis. The results revealed significant heterogeneity in DVT risk models between ICU and non-ICU populations, which may be closely associated with differences in physical mobility, early rehabilitation interventions, thromboprophylaxis regimens and clinical management pathways.22,24 These findings suggest that targeted DVT risk stratification tools tailored to different clinical scenarios are urgently needed for sICH patients.
PROBAST-based methodological evaluation demonstrated that the included studies generally suffered from a high overall risk of bias, with methodological flaws that increase overfitting risk and reduce model stability and predictive power. Future studies should adopt prospective large-sample designs, standardize predictor selection and missing data handling, and conduct comprehensive model evaluation covering discrimination, calibration, and decision-analytic measures of clinical usefulness. 28 Notably, all primary studies included in this review originated from a single country. The high homogeneity in population composition, healthcare systems and diagnostic and therapeutic strategies greatly limits the external generalizability of existing models. Therefore, multinational and multicenter collaborative studies are urgently needed, and rigorous temporal and geographical external validation should be performed to improve model generalizability and global applicability.
Four consistent core predictors including age, D-dimer level, hematoma volume and GCS score were identified in this study, which provides solid evidence for individualized thromboprophylaxis strategies among patients with sICH. Advanced age (>60 years) demonstrates significant correlation with in-hospital DVT development following sICH.18,29 Accordingly, strengthened basic prevention, standardized early mobilization and physical preventive measures are highly recommended for elderly patients. Accumulated studies have confirmed that elevated D-dimer level is correlated with DVT risk in sICH patients in a dose-response manner.30,31 Nevertheless, the increased D-dimer in the acute phase of sICH is mainly attributed to non-specific hyperfibrinolysis triggered by brain tissue injury, hematoma absorption and systemic inflammatory stress, leading to insufficient clinical specificity for DVT identification. Therefore, D-dimer is only suitable for combined risk evaluation and dynamic clinical monitoring, and cannot be used alone as a reliable indicator to predict DVT events. 32 Future studies are recommended to dynamically monitor its level changes or combine it with fibrin monomer, fibrinogen degradation products and other fibrinolysis-related biomarkers, so as to elevate the specificity and accuracy of DVT prediction.33,34 Patients with a hematoma volume >30 ml exhibit significantly increased susceptibility to DVT.17,22 However, hematoma volume is not a direct pathological driver of DVT. A larger hematoma usually corresponds to more severe neurological deficits and conscious disturbance, which results in prolonged bed rest and limited physical activity, thereby causing lower extremity venous stasis and indirectly increasing the incidence of DVT.35,36 For such high-risk patients, mechanical prophylaxis such as graduated compression stockings and intermittent pneumatic compression should be prioritized, together with standardized dynamic monitoring to identify occult DVT at an early stage. The GCS score, a standardized neurological assessment tool, 37 has similarly been validated as an independent DVT predictor in sICH patients.7,19 For patients with a low GCS score accompanied by severe disturbance of consciousness and limb dysfunction, clinical management should focus on passive limb exercise and bedside rehabilitation. In conclusion, these four indicators are readily available in routine clinical practice and can form a simple bedside risk assessment framework to guide timely individualized thromboprophylaxis. Nevertheless, most of these indicators are static baseline parameters collected at admission, and they mainly act as indirect correlational factors reflecting disease severity and physical activity status, with weak correlation with the direct pathological mechanism of DVT formation. To construct rigorous and high-quality prediction models, future studies should prioritize incorporating thrombotic predisposition factors including prior venous thromboembolism history, thrombophilia and malignancy history, as well as admission coagulation markers directly reflecting hypercoagulable status. Dynamic in-hospital parameter changes should also be included to optimize variable selection, so as to enhance model predictive accuracy, stability and clinical applicability.
From the perspective of clinical application and translational implementation, constrained by high bias risk, substantial heterogeneity and geographical limitation of original studies, existing predictive models lack sufficient overall robustness and are not recommended for routine clinical decision-making at present. Nevertheless, a few models with rigorous external validation and low risk of bias (e.g., the model developed by Ji et al 22 ) may serve as auxiliary reference tools for clinical risk assessment, helping healthcare professionals identify high-risk patients. Even so, it is not advisable to directly adopt model threshold values to guide anticoagulation or interventional decisions, comprehensive judgment based on individual patient conditions is still required. Machine learning algorithms show unique advantages in processing complex high-dimensional clinical data and mining potential risk associations, which can further improve model discrimination and stability. 38 In the future, besides optimizing study design and conducting large-sample prospective multinational multicenter external validation, machine learning algorithms can be applied to develop hierarchical predictive models with stronger generalizability, providing more reliable research tools for precise DVT prevention and management in sICH patients.
Limitations
This review has several limitations. Firstly, all included studies were conducted exclusively in China, which may restrict the external generalizability and wider clinical applicability of the existing prediction models. Secondly, the methodological quality of most studies was limited by their retrospective case-control designs. This heavy reliance on retrospective data increases susceptibility to recall and selection biases, potentially compromising the validity of the developed models. Thirdly, with the exception of Ji et al, 22 who incorporated external validation, all other studies relied solely on internal validation, significantly limiting the models’ generalizability to broader populations. Finally, this study only included prediction models with DVT or VTE as the endpoint and did not separately incorporate PE prediction models in patients with sICH. Further dedicated systematic reviews of PE prediction models in patients with sICH are warranted in the future.
Conclusion
Our analysis of 15 studies encompassing 19 models revealed that the pooled AUC of 11 validated models reached 0.82. Although existing models exhibit certain discriminative potential, their overall predictive performance remains insufficiently robust and cannot be directly applied to clinical decision-making due to the high risk of bias and substantial heterogeneity. Nevertheless, key variables such as age, D-dimer level, hematoma volume and GCS score can support qualitative clinical risk stratification, and provide practical reference for formulating precise and individualized thromboprophylaxis strategies for sICH patients. To advance the field, future research should strictly follow PROBAST and TRIPOD guidelines, adopt prospective multicenter large-sample designs, conduct rigorous external validation, incorporate more pathogenesis-related direct laboratory indicators and dynamic monitoring data, and properly combine machine learning approaches, so as to further improve model stability and external generalizability.
Supplemental Material
Supplemental Material - Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis
Supplemental Material for Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis by Yana Xing, Weixin Cai, Lin Wang, Tong Wang, Fei Wu, Weige Sun, Yuan Yuan and Ran Zhang in Clinical and Applied Thrombosis/Hemostasis.
Supplemental Material
Supplemental Material - Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis
Supplemental Material for Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis by Yana Xing, Weixin Cai, Lin Wang, Tong Wang, Fei Wu, Weige Sun, Yuan Yuan and Ran Zhang in Clinical and Applied Thrombosis/Hemostasis.
Supplemental Material
Supplemental Material - Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis
Supplemental Material for Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis by Yana Xing, Weixin Cai, Lin Wang, Tong Wang, Fei Wu, Weige Sun, Yuan Yuan and Ran Zhang in Clinical and Applied Thrombosis/Hemostasis.
Supplemental Material
Supplemental Material - Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis
Supplemental Material for Risk Prediction Models for Deep Vein Thrombosis in Patients with Spontaneous Intracerebral Hemorrhage: A Systematic Review and Meta-analysis by Yana Xing, Weixin Cai, Lin Wang, Tong Wang, Fei Wu, Weige Sun, Yuan Yuan and Ran Zhang in Clinical and Applied Thrombosis/Hemostasis.
Footnotes
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Funding Fund of Tiantan Hospital - Hospital Fund - Nursing special (2022-YQN-12).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trial Registration
The study protocol was registered on PROSPERO (registration number: CRD42024600505).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.