
Abstract
Background and objectives
Previous studies suggest a link between tumor necrosis factor-alpha (TNF-alpha) levels and atrial fibrillation (AF). However, the nature of this relationship is disputed. To address this, we conducted a study to gather and assess evidence on the association between TNF-alpha and AF prediction.
Methodology
Studies were systematically searched and collected from four databases and different types of gray literature to cover all available evidence. After the screening, the selected articles’ quality and risk of bias assessment were evaluated. Meta-analysis calculated std. mean difference on the extracted data. Furthermore, heterogeneity, sensitivity, subgroups, and publication bias analyses were assessed.
Results
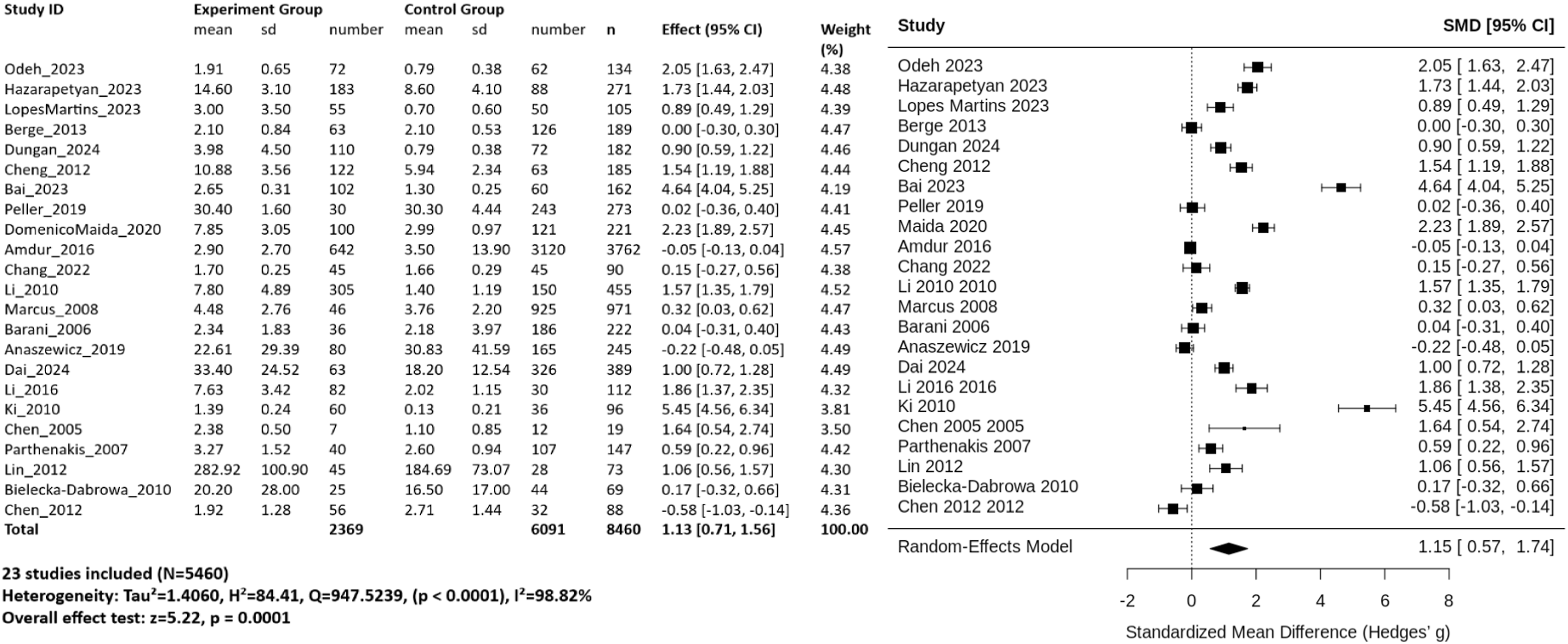
Twenty-three studies were included in this systematic review and meta-analysis, comprising a total of 2,369 patients with atrial fibrillation (AF) and 6,091 control participants. Pooled analysis using a random-effects model demonstrated a significant positive association between serum TNF-alpha levels and AF (standardized mean difference [SMD] = 1.15; 95% CI: 0.57–1.74; P = 0.0001). However, substantial between-study heterogeneity was observed (τ2= 1.4060; Cochran’s Q = 947.52; I2= 98.82%; P < 0.0001), indicating considerable variability in effect sizes across the included studies.
Conclusions
Elevated TNF-α levels are significantly associated with the presence of atrial fibrillation. Despite strong overall evidence, substantial heterogeneity and publication bias were observed among studies. These findings support a role for inflammation in AF and highlight the need for more standardized future research.
Introduction
Atrial fibrillation (AF) is a common sustained cardiac arrhythmia and a significant cause of morbidity and mortality, with recent estimates suggesting that at least 10.55 million Americans are affected.1,2 AF increases a person’s risk for stroke approximately five-fold when standard stroke risk factors are accounted for, and the condition causes about 1 in 7 strokes. 3 AF doubles the risk of mortality and increases risks of heart failure, myocardial infarction, chronic kidney disease and dementia, resulting in lower quality of life. Despite advances in therapeutic interventions including pharmacological management and catheter ablation, up to 45% of patients may experience AF recurrence within 12 months after radiofrequency catheter ablation, underscoring the persistent challenges in AF management.4-7
The fundamental mechanisms underlying AF remain incompletely understood, but atrial remodeling, including structural, electrical, contractile and autonomic remodeling, has been demonstrated to contribute to the AF substrate.8-10 Various inflammatory markers and mediators such as C-reactive protein, tumor necrosis factor-alpha, interleukin-2, interleukin-6, interleukin-8, and monocyte chemoattractant protein-1 have been linked with the presence or the outcome of AF.11,12 Functional analysis has revealed commonality in dysregulated cellular processes including extracellular matrix remodeling, cardiac conduction alterations, metabolic derangements, and innate immune system activity with Tumor necrosis factor-alpha (TNF-alpha) signaling pathways prominently implicated. This growing evidence suggests that inflammation plays a central role in both the initiation and perpetuation of AF.13-16
TNF-alpha is a pleiotropic proinflammatory cytokine that has emerged as a particularly important mediator in AF pathophysiology.17,18 Accumulating evidence shows that TNF-alpha plays exceedingly important roles in atrial remodeling. TNF-alpha is involved in the pathogenesis of atrial fibrosis and altered connexin-40 expression through the TGF-beta signaling pathway, activation of myofibroblasts and increased secretion of matrix metalloproteinases.19,20 In atrial tissue, TNF-alpha promotes structural remodeling through alterations in connexin-43 and metalloproteases while also reducing sarcoplasmic reticulum calcium content. 21 These molecular mechanisms provide biological plausibility for TNF-alpha’s involvement in creating an arrhythmogenic substrate conducive to AF development and maintenance. 22
Clinical studies examining TNF-alpha levels in AF patients have yielded important but sometimes inconsistent findings. 23 Research has revealed that TNF-alpha is elevated in the plasma and left atrial tissue and has positive correlation with left atrial diameter in patients of chronic AF. 24 Unadjusted analyses have shown that levels of inflammatory cytokines including TNF-alpha are significantly higher in AF patients compared to control patients, with patients having permanent and persistent AF showing higher serum levels than those with paroxysmal AF.25,26 However, the predictive value of TNF-alpha for AF recurrence after interventions remains unclear. Some studies found no significant correlation between TNF-alpha concentrations and the recurrence of arrhythmia after ablation, while radiofrequency catheter ablation has been associated with significant elevation in inflammatory mediators including TNF-alpha post-procedure, which may contribute to early AF recurrence and potentially impact long-term outcomes.27,28
These discrepancies in the literature may arise from differences in study design, patient populations, timing of biomarker measurement, AF subtypes studied, and analytical methodologies employed. Some investigations have focused on chronic or persistent AF while others examined paroxysmal forms. 29 The relationship between TNF-alpha various AF outcomes, including AF presence, disease progression, recurrence after cardioversion or ablation, and response to different therapeutic modalities, has not been systematically synthesized. Furthermore, whether baseline TNF-alpha levels or dynamic changes in TNF-alpha concentrations hold greater prognostic significance remains unresolved.30,31
To date, no comprehensive systematic review and meta-analysis has been conducted to synthesize the available evidence regarding the association between TNF-alpha levels and AF outcomes across diverse patient populations and clinical contexts. Such a synthesis is essential to clarify whether TNF-alpha serves as a clinically meaningful biomarker for risk stratification, prognostic assessment, or therapeutic decision-making in AF management. Animal model studies support this potential: TNF-alpha inhibition with etanercept reduced atrial fibrosis and AF inducibility in a canine model of heart failure, while TNF-alpha blockade attenuated atrial electrical remodeling in a rabbit model of sterile pericarditis, suggesting that TNF-alpha levels could guide therapeutic decision-making in AF management.32,33 Understanding these associations may also inform the potential utility of anti-inflammatory therapeutic strategies targeting TNF-α pathways in AF prevention and treatment. Potential anti-inflammatory therapeutic strategies targeting TNF-alpha pathways include TNF-alpha inhibitors such as etanercept and infliximab, which have shown protective effects against atrial remodeling in preclinical models. 34 Additionally, colchicine has demonstrated efficacy in reducing new-onset arrhythmias after transcatheter aortic valve replacement, though safety concerns warrant further investigation. 35 XPRO1595, a selective inhibitor of soluble TNF-alpha, has also prevented atrial fibrosis and AF susceptibility in animal studies. 36
Therefore, this systematic review and meta-analysis aim to comprehensively evaluate the existing literature examining the association between TNF-alpha levels and various AF outcomes. By quantitatively synthesizing the available evidence, we seek to provide clarity on the clinical utility of TNF-alpha as a biomarker in AF, identify sources of heterogeneity across studies, and highlight gaps in current knowledge that warrant further investigation.
Materials and Methods
Eligibility Criteria
This study was designed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 37
Furthermore, this review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420250652044 (Available: https://www.crd.york.ac.uk/PROSPERO2/view/CRD420250652044).
Eligible articles were defined as full-text human case-control or prospective cohort studies that measured TNF-alpha levels in blood using ELISA or validated methods, confirmed AF diagnosis by ECG, and reported sufficient data to calculate standardized mean differences between AF cases and non-AF controls. Detailed inclusion and exclusion criteria are provided in the following subsections.
Definition
Atrial Fibrillation
AF was the primary condition evaluated in this systematic review and meta-analysis. The diagnosis of AF was established using standard clinical criteria, which included sustained arrhythmias lasting more than 30 seconds in the absence of discernible P-waves. A 12-lead electrocardiogram (ECG) was utilized for diagnostic confirmation, specifically assessing irregular R-R intervals and the absence of P-waves. TNF-alpha levels were considered a key biomarker, reflecting potential pathophysiological links between TNF-alpha and AF. The inclusion of these criteria ensured an accurate identification of AF cases for analysis.3,5
Controls
Control participants were individuals without AF, as confirmed through comprehensive diagnostic assessments. These individuals exhibited normal 12-lead ECG results, with no signs of arrhythmia and consistent R-R intervals accompanied by identifiable P-waves.
Inclusion/Exclusion Criteria
Inclusion criteria encompassed: 1) Case-control and prospective cohort studies that investigated the relationship between TNF-alpha levels and AF incidence, 2) Human clinical study, 3) Studies reporting mean TNF-alpha levels with standard deviations or standard errors for both AF cases and control groups, or providing sufficient raw data to calculate these values.
TNF-alpha levels were assessed through blood-based testing using the enzyme-linked immunosorbent assay (ELISA). AF diagnosis was confirmed based on standardized ECG criteria, requiring irregular R-R intervals and an absence of P-waves in addition to sustained arrhythmic episodes lasting at least 30 seconds. 8
Sources and Search Strategy
Relevant studies published between 1990 and May 2025 were systematically retrieved from major electronic databases, including PubMed, ProQuest, Scopus, and Web of Science. The ProQuest database was also manually reviewed for relevant dissertations. The search strategy was formatted according to the PICO framework; Population: individuals with or at risk of atrial fibrillation; Exposure: TNF-alpha; Comparison: absence of AF or lower TNF-alpha; Outcome: atrial fibrillation. Additionally, systematic review protocols were searched in PROSPERO to identify related studies. To ensure comprehensive coverage, gray literature, such as conference abstracts and meeting proceedings from organizations like the American Heart Association and the European Society of Cardiology, was examined. Expert opinions were also solicited via email to identify any unpublished or ongoing research. Key cardiology journals, including The American Journal of Cardiology, European Heart Journal, and Circulation, were manually screened for relevant articles. Furthermore, reference lists of previous systematic reviews and primary research articles were reviewed to identify additional studies. No geographical restrictions were applied, and only full-text articles were included in the final selection. For database searching, the Medical Subject Headings (MeSH) database was used to identify relevant terms related to Atrial Fibrillation (AF) and Tumor necrosis factor (TNF-alpha). The primary search keywords included “TNF-alpha” and “atrial fibrillation.” A structured search strategy was developed using a combination of free-text terms, MeSH terms, and Boolean operators (AND/OR/NOT) to refine search accuracy. Additionally, the Number Needed to Read (NNR) was calculated as unique records after deduplication divided by included studies. After deduplication, 908 records were screened, and 23 studies were included, yielding an NNR of 39.5 (908 ÷ 23), meaning approximately 40 records were reviewed per eligible study. The complete search syntax applied in PubMed is provided in Supplementary File. 1. This syntax was adjusted accordingly for each database following its specific search guidelines.
All search results were exported into EndNote (Version X7; Thomson Reuters Corporation, Toronto, ON, Canada) to systematically identify and eliminate duplicate records. The initial screening phase involved reviewing titles and abstracts to determine potential relevance. Two independent reviewers (B.A. Y.Y) conducted a full-text evaluation of the selected studies and classified them into three categories: relevant, irrelevant, or uncertain, based on predefined eligibility criteria. Any disagreements between reviewers were referred to a third evaluator (A.F.) for resolution through discussion. If uncertainties persisted, the entire research team participated in the final decision-making process to ensure consistency and accuracy in study selection.
Quality and Risk of Bias Assessment
The methodological quality and risk of bias of the included studies were independently assessed by two reviewers (A.Z and A.Aj) using the Newcastle-Ottawa Scale (NOS) checklist. 38 Studies were categorized as poor, fair, or good based on scores ranging from 0 to 8 across selection, comparability, and outcome/exposure domains. Studies scoring ≥7 points were considered high quality, 5–6 points moderate quality, and <5 points low quality. Any discrepancies between reviewers were resolved through consensus, with the third reviewer (A.F.) providing arbitration when necessary.
Data Extraction
Two researchers (A.F. and A.T.) independently extracted data from each study according to a pre-defined protocol. The extracted data were grouped into three categories: 1) General Information: First author’s name, publication year, journal, country, and region; 2) The risk of bias assessment; 3) Study Characteristics: Study design, duration, sample size, inclusion/exclusion criteria, age distribution, gender, AF definition, Type of AF, TNF alpha, data sources, diagnostic methods, SMD and 95% confidence intervals (CIs), and ethical approval details. For missing or additional required information, corresponding authors of the respective studies were contacted via email.
Data Synthesis and Analysis
For quantitative data, if applicable, the SMD and 95% CIs were calculated using R statistics. Analyses were conducted using the meta and metafor packages in R, versions 6.5-0 and 4.4-0 respectively. The selection of statistical models, either the Fixed Effect Model (FEM) or the Random Effect Model (REM), was based on methodological similarities among the studies. A forest plot was generated to visualize the combined effect size. Heterogeneity analysis was conducted using Cochran’s Q test and the I2 statistic, with an I2 value exceeding 50% considered indicative of substantial heterogeneity. To further investigate potential sources of heterogeneity, meta-regression was performed using case mean age and the percentage of females as study-level moderators. If statistical pooling was not feasible, alternative methods such as subgroup analysis or meta-regression were employed to explore heterogeneity sources, followed by sensitivity analysis to ensure robustness. To assess potential publication bias, funnel plots, Begg’s and Egger’s tests were utilized. Additionally, the leave-one-out sensitivity analysis was used to evaluate the impact of individual studies on overall results. While meta-analysis remained the primary objective, it was conducted only when sufficient data were available for systematic review.
Results
Search Results
A comprehensive search of databases and gray literature identified 1,236 studies. After removing 328 duplicate entries, 908 studies remained for screening based on their titles and abstracts. Of these, 879 studies were excluded for not meeting the inclusion criteria, leaving 29 articles for full-text review. Ultimately, 23 studies were included in the systematic review, proceeding to meta-analysis. The inter-rater agreement between reviewers was substantial (Cohen's κ = 0.80). Figure 1.39-62 Five studies were excluded from the meta-analysis due to the absence of reported TNF-alpha levels in either the case or control groups. Among the included studies, four were classified as case-control, while seven followed a cohort design (Figure 2). Flowchart depicting the literature search, screening process, and selection of studies for systematic review and meta-analysis Forest plot of the association between serum TNF-alpha levels and AF, SMD with 95% confidence intervals (CI) are shown for each of the 23 included studies (black squares; size proportional to study weight). The vertical dashed grey line at SMD = 0 represents the line of no effect. The black diamond at the bottom shows the pooled SMD calculated using a random-effects model. Study labels indicate first author and year of publication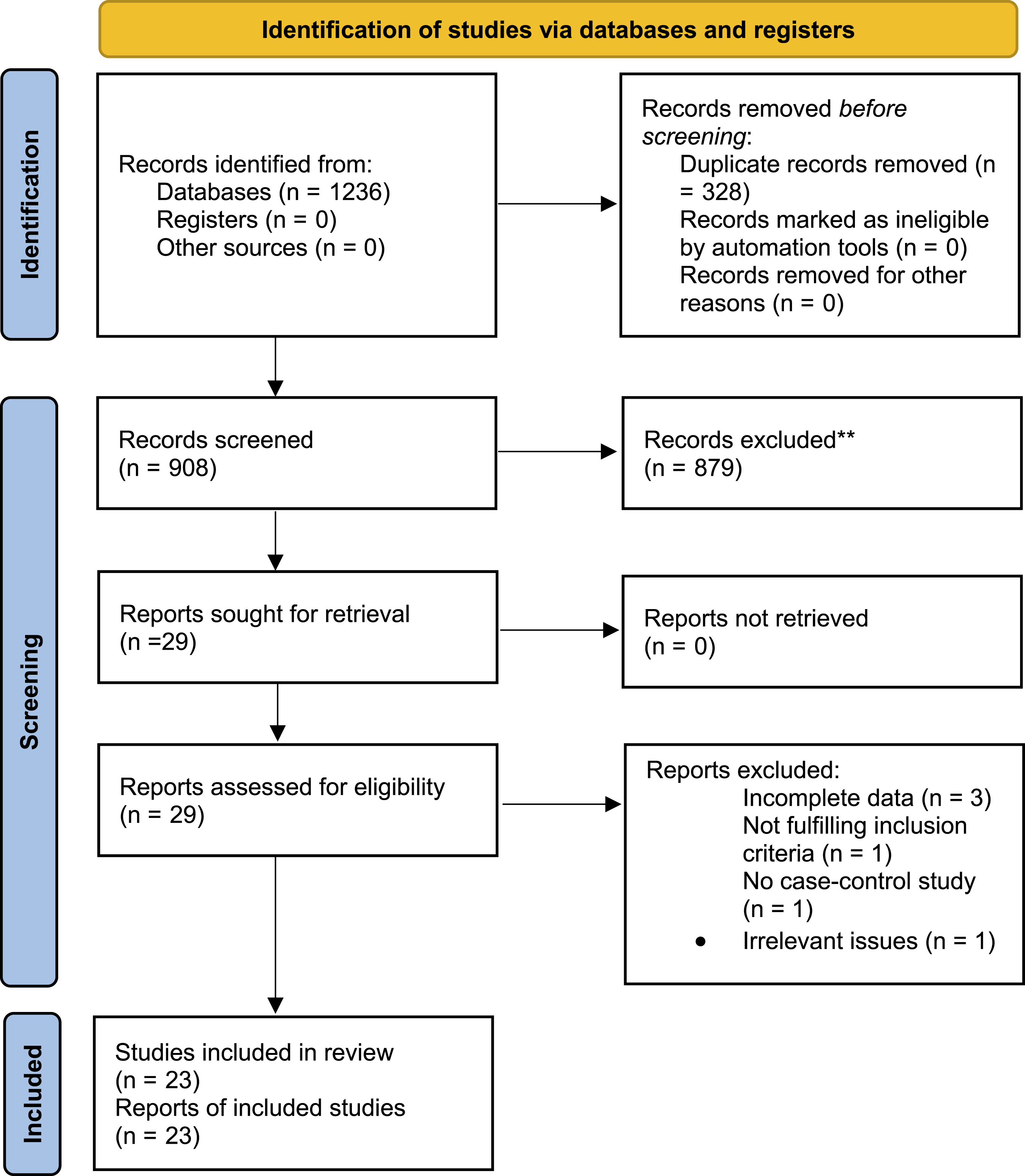
Characteristics of the Included Articles
Summary of Key Study Characteristics in the Meta-Analysis Exploring the Relationship Between TNF-Alpha Levels and AF
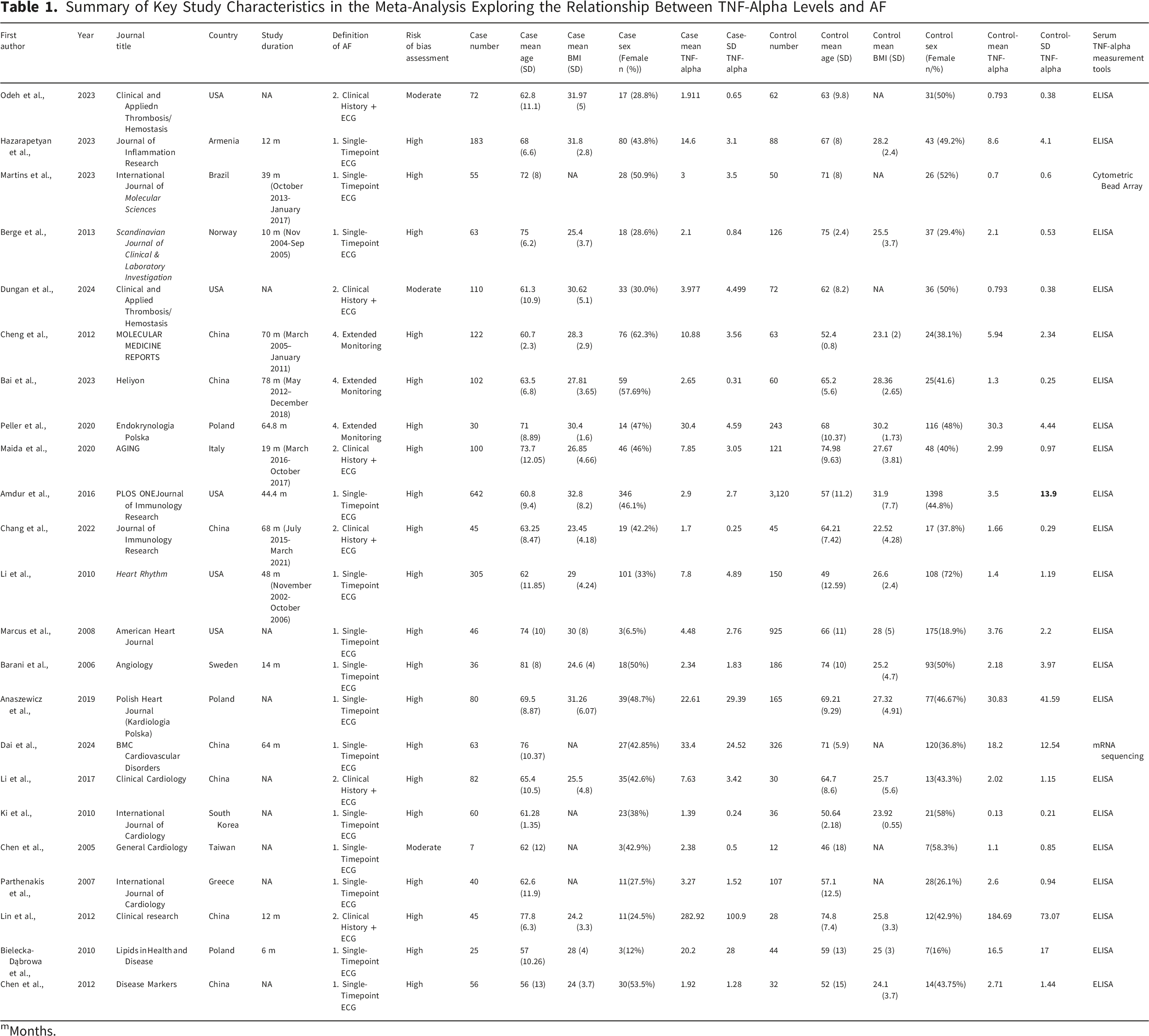
mMonths.
Association of TNF-Alpha Levels With AF Incidence
The drapery plot (Figure 3A) confirmed that the estimated effect size, expressed as SMD, remained below a value of 2.0 in most studies. Visual inspection of the funnel plot (Figure 3B) suggested asymmetry consistent with possible publication bias, which was further evaluated using a trim-and-fill analysis (Figure 3D). A trim-and-fill analysis was conducted to assess the potential impact of publication bias. As shown in Figure 3D, five potentially missing studies were imputed on the left side of the funnel plot. The original pooled SMD was 0.503 (95% CI: 0.446–0.560). After adjustment using the trim-and-fill method, the pooled SMD decreased to 0.336 (95% CI: 0.282–0.391), representing a relative reduction of 33.1%. Despite this attenuation, the association between TNF-α levels and atrial fibrillation remained statistically significant. (A) Drapery plot illustrating p-value functions for each included study. Each numbered curve represents an individual study. The bold red line indicates the pooled random-effects SMD across alpha levels. The horizontal dashed lines represent confidence intervals corresponding to common significance levels (α = 0.10, 0.05, 0.01, and 0.001). Across all prediction interval levels (90%, 95%, 99%, and 99.9%), the pooled random-effects estimate does not intersect the null effect line (SMD = 0), indicating a statistically significant overall association. (B) Funnel plot showing visual asymmetry, suggesting the presence of small-study effects consistent with publication bias. (C) Baujat plot depicting the contribution of individual studies to overall heterogeneity and influence on the pooled effect estimate, identifying Ki et al.
51
(study 18) as exerting the greatest influence. Each point represents a single study. (D) Trim-and-fill funnel plot. Filled blue circles represent observed studies; open red circles represent five imputed studies on the left side. The vertical dashed blue line indicates the original pooled SMD (0.503), and the vertical dashed red line shows the adjusted pooled estimate after trim-and-fill correction (0.336). The shaded triangular region represents the expected 95% confidence limits around the pooled effect
Statistical testing (Begg's test, Supplementary File 2.1) confirmed small-study effects (P = 0.0031). The Baujat plot (Figure 3C) showed that the study by Ki et al.
13
contributed more than other studies to the overall heterogeneity and influenced the pooled effect size. Despite this influence, the study was retained in the main analysis, as excluding a study solely based on heterogeneity contribution is not methodologically justified. Moreover, the leave-one-out sensitivity analysis (Figure 4) confirmed that removal of Ki et al. did not change the statistical significance of the overall association (pooled SMD decreased from 1.154 to 0.968, P < 0.001), demonstrating the robustness of our findings. Leave-one-out sensitivity analysis of the association between TNF-α levels and AF
Analysis of Subgroups
Heterogeneity across studies was evaluated using multiple subgroup analyses based on Year of publication, region, risk of bias assessment, study design, definition of AF, type of AF, and time of TNF-alpha measurement. For Year of Publication, studies published in ≥2020 showed a pooled SMD of 1.680 (95% CI = 0.987–2.372, I2= 96.7%), while those published before 2020 showed an SMD of 0.824 (95% CI = 0.375–1.272, I2= 97.0%). The test for subgroup differences was significant (Q-between = 4.14, P = 0.0419). For Region-based analysis, Europe showed a pooled SMD of 0.406 (95% CI = -0.247–1.059, I2= 96.0%), while Asia demonstrated the highest effect size with an SMD of 1.815 (95% CI = 0.989–2.641, I2= 97.2%). America had an SMD of 0.941 (95% CI = 0.211–1.670, I2= 98.2%). The test for subgroup differences was significant (Q-between = 6.88, P = 0.0321). Regarding Risk of Bias assessment, studies rated as “high” reported an SMD of 1.083 (95% CI = 0.630–1.535, I2= 97.9%), while studies rated as “moderate” showed a higher SMD of 1.510 (95% CI = 0.625–2.395, I2= 89.4%). The test for subgroup differences was not significant (Q-between = 0.71, P = 0.3991). For Study Design, prospective cohort studies yielded an SMD of 0.655 (95% CI = 0.042–1.268, I2= 97.9%), while case-control studies reported an SMD of 1.468 (95% CI = 0.846–2.091, I2= 97.3%). The test for subgroup differences was not significant (Q-between = 3.33, P = 0.0680). In terms of the Definition of AF, studies using single timepoint ECG showed an SMD of 0.825 (95% CI = 0.361–1.289, I2= 97.4%), those using clinical history + ECG had an SMD of 1.376 (95% CI = 0.714–2.039, I2= 94.0%), and studies with unspecified definitions of AF showed the highest SMD of 2.055 (95% CI = -0.155–4.265, I2= 98.8%). The test for subgroup differences was not significant (Q-between = 2.62, P = 0.2693). For Type of AF, non-permanent AF studies had an SMD of 1.989 (95% CI = 0.684–3.295, I2= 98.6%), permanent AF studies showed an SMD of 1.202 (95% CI = 0.461–1.942, I2= 96.8%), and studies where the type of AF was not identified reported an SMD of 0.509 (95% CI = 0.182–0.837, I2= 91.6%). The test for subgroup differences was significant (Q-between = 6.81, P = 0.0332). Finally, for Time of TNF-alpha Measurement, studies measuring TNF-alpha before AF diagnosis showed an SMD of 1.041 (95% CI = 0.434–1.649, I2= 96.6%), while studies measuring TNF-alpha at AF diagnosis had an SMD of 1.222 (95% CI = 0.597–1.848, I2= 98.2%). The test for subgroup differences was not significant (Q-between = 0.17, P = 0.6843). While subgroup analyses highlighted key differences, they did not fully explain the overall heterogeneity observed (I2= 97.7%). All subgroup forest plots are presented in Supplementary File. 2(2-8).
Different Subgroup Analyses by Stratifying the Data
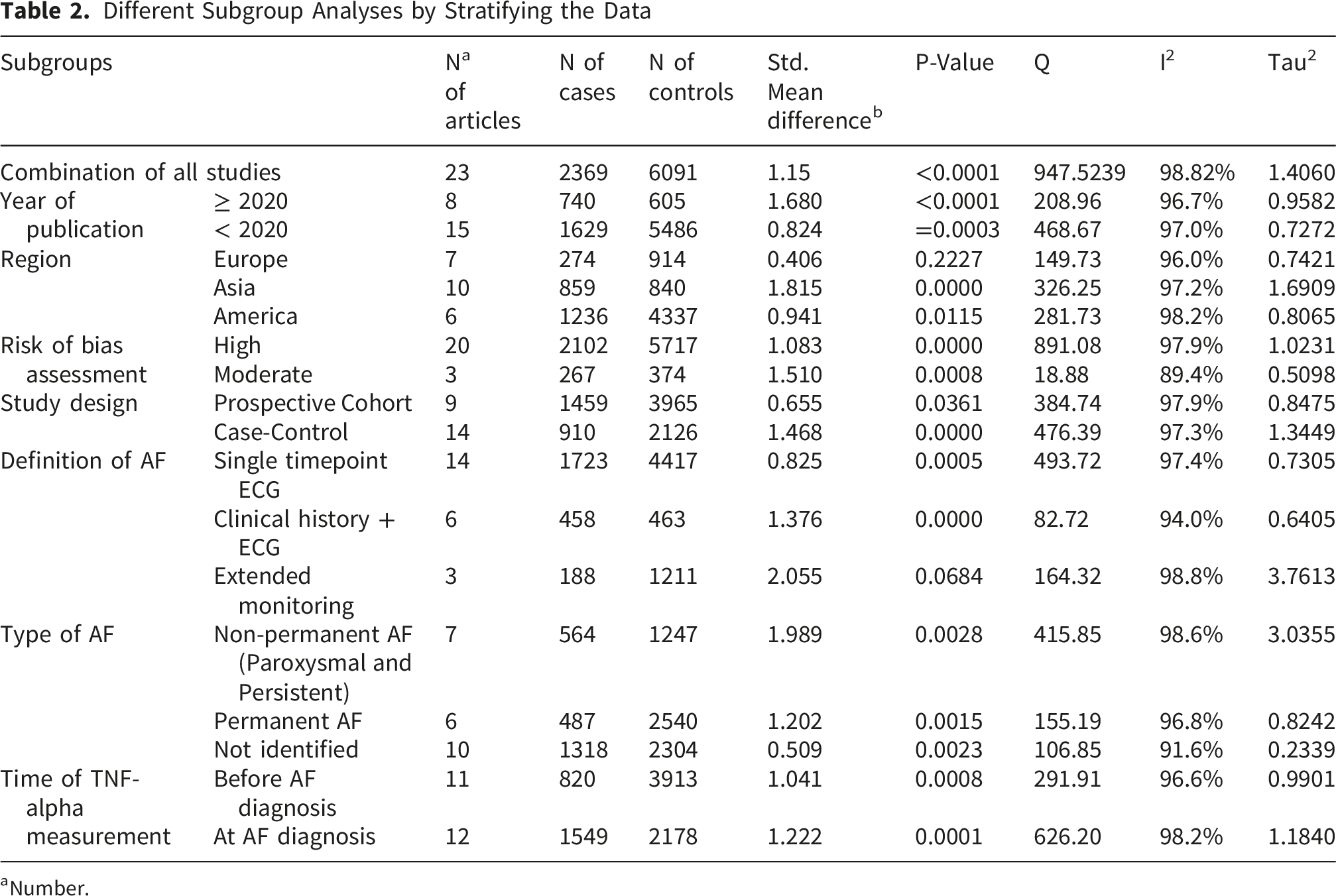
aNumber.
Leave-One-Out Sensitivity Analysis
Sequential exclusion of individual studies resulted in minimal variation in the pooled SMD, with effect estimates ranging from 0.97 to 1.23 (Figure 4). The largest reduction in the pooled effect size was observed following removal of Ki et al., yielding an SMD of 0.97 (Δ = −0.19 compared with the overall estimate), suggesting that this study modestly inflated the magnitude of the overall association despite its relatively small variance. In contrast, exclusion of Chen2 et al. produced the highest pooled SMD (1.23, Δ = +0.08), indicating a slight upward influence of this study on the summary effect.
Across all leave-one-out iterations, the direction and statistical significance of the association remained unchanged, with all pooled estimates remaining significant (P ≤ 0.0003) and no 95% confidence intervals crossing the null. Exclusion of individual studies resulted in only modest reductions in heterogeneity, with the largest decreases observed after removing Ki et al. (I2= 98.23%, τ2= 1.26) and Bai et al. (I2= 98.45%, τ2= 1.45); however, substantial heterogeneity persisted across all models (I2> 98%). Overall, the leave-one-out analysis confirms that the association between TNF-α levels and atrial fibrillation is robust and not driven by any single study, despite persistent between-study heterogeneity.
Meta-Regression Analysis
Meta-Regression Results – Coefficients (β), p-values, and 95% CIs for Covariates (Age, Sex, BMI) Predicting SMD Variation. Model Fit Statistics (Age/Sex model): Model type: Mixed-Effects Meta-Regression (REML); AIC = 81.6168; BIC = 85.5998; AICc = 84.2835; Residual Heterogeneity: τ2= 2.2131 (τ = 1.4876); Residual I2= 98.79%; Explained Heterogeneity: R2= 0.00%; Omnibus Moderators Test: QM2= 1.3276, p = 0.5149; Residual Heterogeneity Test: QE20= 985.1342, p < 0.0001. Model Fit Statistics (BMI Model): Substantial Residual Heterogeneity Remained (p < 0.0001)

Given the potential role of obesity in AF pathophysiology, a separate meta-regression analysis examined whether mean body mass index (BMI) moderated the association between TNF-alpha and AF. BMI data were available for 18 of the 23 included studies. As shown in Table 3, the meta-regression revealed a statistically significant negative association between mean BMI and SMD (β = −0.1065, SE = 0.0107, P < 0.0001). The intercept was 3.6364 (SE = 0.3223), indicating that at a theoretical BMI of 0, the predicted SMD would be 3.64. For each 1 kg/m2 increase in BMI, the effect size decreased by approximately 0.11 units. This suggests that as BMI increases, the magnitude of the difference in TNF-alpha levels between AF patients and controls tends to decrease substantially. Substantial residual heterogeneity remained (p < 0.0001), indicating that other unmeasured study-level factors contribute to the observed variability (Figure 5). Meta-regression analysis evaluating the relationship between mean BMI and the SMD of TNF-α levels between patients with atrial fibrillation and control groups. Each circle represents an individual study and is weighted according to its inverse variance. The solid red line represents the fitted meta-regression line and the shaded area indicates the 95% confidence interval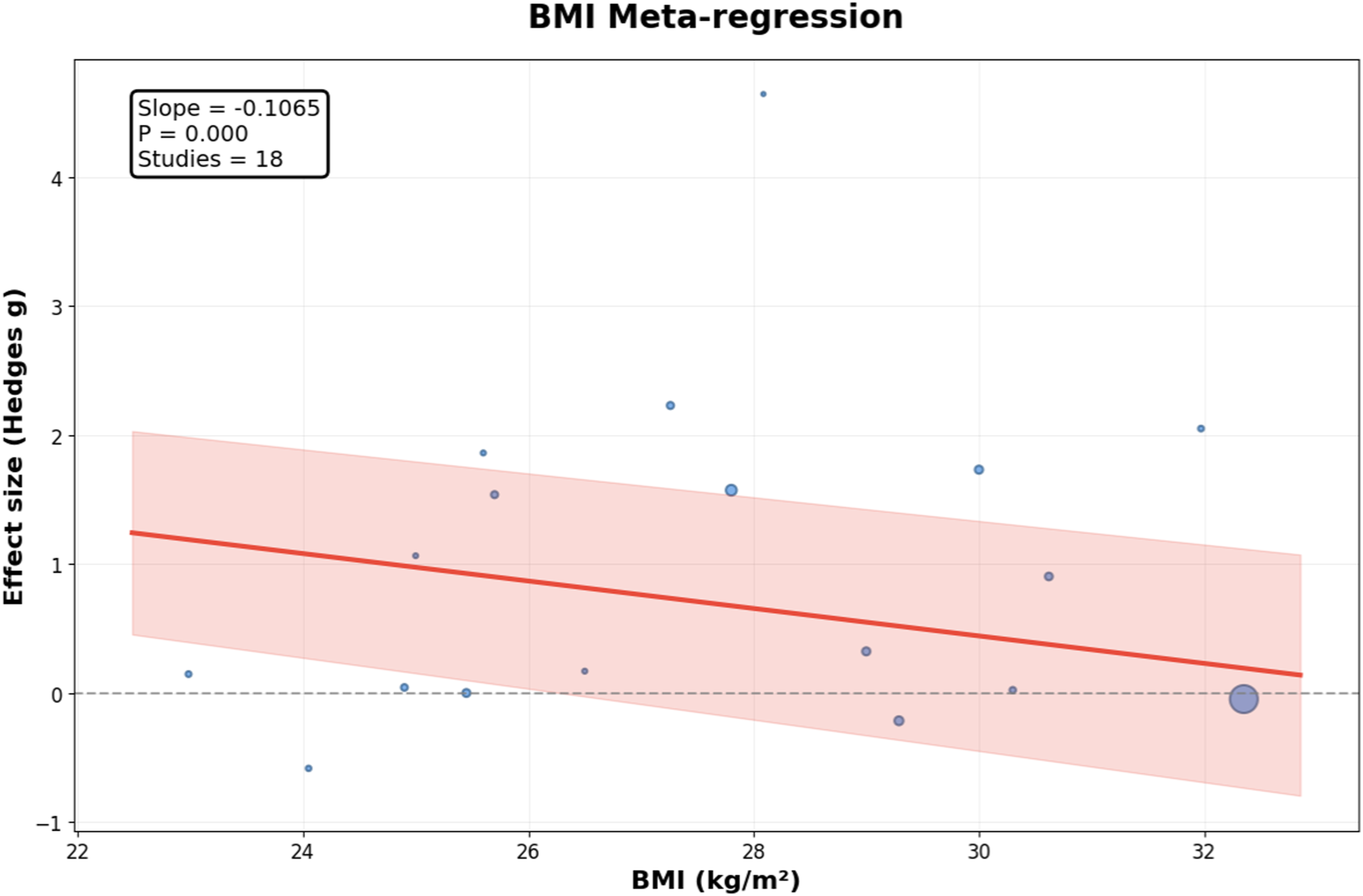
GRADE Certainty of Evidence Assessment
A GRADE evaluation was performed to assess the certainty of evidence regarding the association between serum TNF-α levels and atrial fibrillation (AF). Certainty was initially rated as low due to the observational design of all included studies. The evidence was further downgraded for the following reasons: risk of bias (−1), reflecting limitations related to cross-sectional and hospital-based sampling, lack of blinding, and insufficient adjustment for confounders; inconsistency (−2), given the substantial heterogeneity across studies (I2= 98.82%, τ2= 1.4060) and variability in populations and TNF-α measurement methods; and publication bias (−1), supported by trim-and-fill analysis identifying five potentially missing studies and reducing the pooled SMD from 0.503 to 0.336 (a 33.1% decrease). No downgrades were applied for indirectness or imprecision, as studies directly compared TNF-α levels between AF and control groups, and confidence intervals were narrow and excluded the null.
Overall, the certainty of evidence was rated as very low, indicating limited confidence in the observed association and a high likelihood that the true effect differs substantially. Consequently, the link between elevated TNF-α and AF should be interpreted cautiously. Future high-quality prospective studies with standardized biomarker assessment, comprehensive adjustment for confounders such as BMI and inflammatory comorbidities, and transparent reporting are needed to clarify the causal role of TNF-α in AF risk stratification and management.
Discussion
The present systematic review and meta-analysis demonstrate a significant positive association between elevated serum TNF-alpha levels and the presence of atrial fibrillation, with a pooled SMD of 1.15 (95% CI: 0.57–1.74; P = 0.0001). This finding, based on 23 studies encompassing 2,369 AF patients and 6,091 controls, provides robust evidence supporting the role of inflammation in AF pathophysiology. However, the substantial heterogeneity observed across studies (I2= 98.82%) and evidence of publication bias warrant careful interpretation of these results.
Our findings align with the broader body of evidence suggesting that inflammatory processes play a central role in AF initiation and maintenance. Li et al 55 reported significantly elevated levels of multiple inflammatory biomarkers including TNF-alpha in 305 AF patients compared to 150 controls, demonstrating a graded increase in TNF-alpha levels across paroxysmal, persistent, and permanent AF subtypes. This pattern is consistent with our subgroup analysis showing that permanent AF exhibited higher effect sizes compared to non-permanent AF (SMD = 1.202 vs 1.989, respectively). The progressive elevation of TNF-alpha with increasing AF persistence suggests that inflammation may contribute not only to AF onset but also to its progression and maintenance, supporting the concept of inflammation as both a cause and consequence of atrial remodeling.
The biological plausibility of TNF-alpha involvement in AF is well-established through multiple mechanistic pathways. TNF-alpha promotes atrial fibrosis through activation of the TGF-β signaling pathway, increases matrix metalloproteinase secretion, and alters connexin expression patterns critical for atrial electrical conduction. Odeh et al 39 demonstrated significant correlations between TNF-alpha and collagen remodeling biomarkers in AF patients, providing direct evidence of inflammation-mediated structural remodeling. Similarly, Hazarapetyan et al 40 reported moderate correlations between inflammatory markers and left atrial structural parameters, including left atrial diameter and stiffness, further supporting the mechanistic link between systemic inflammation and atrial substrate modification.
The regional variation observed in our subgroup analysis reveals important insights into the heterogeneity of this association. Asian populations demonstrated the highest effect size (SMD = 1.815), while European populations showed the lowest (SMD = 0.406), with American populations intermediate (SMD = 0.941). These differences may reflect genuine biological variation related to genetic factors, environmental exposures, or differences in AF phenotypes across populations. However, methodological factors including variations in TNF-alpha measurement techniques, patient selection criteria, and control group characteristics likely contribute substantially to this regional heterogeneity. Cheng et al 44 and Bai et al, 45 both conducted in Chinese populations, reported markedly elevated TNF-alpha levels in AF patients, whereas studies from European populations such as Berge et al 42 from Norway and Peller et al 46 from Poland showed more modest differences.
The temporal trend analysis revealing higher effect sizes in studies published after 2020 compared to earlier studies (SMD = 1.680 vs 0.824) raises important methodological considerations. This pattern could reflect improved measurement techniques, better patient phenotyping, or more rigorous control selection in recent studies. Alternatively, it may suggest publication bias, with more recent studies potentially more likely to report positive findings. The significant publication bias detected through Begg’s test and funnel plot asymmetry supports this concern and necessitates cautious interpretation of the overall effect size.
Several studies have examined TNF-alpha in the context of specific AF-related conditions and comorbidities. Marcus et al 51 demonstrated that among various inflammatory biomarkers including C-reactive protein, CD40 ligand, and monocyte chemoattractant protein-1, only IL-6 showed a significant association with AF in patients with coronary artery disease, suggesting that different inflammatory pathways may predominate in different clinical contexts. Parthenakis et al 58 found elevated TNF-alpha levels in AF patients with non-ischemic dilated cardiomyopathy, noting that AF represented a more advanced stage of heart failure syndrome. These findings highlight the complexity of inflammation in AF, where the arrhythmia coexists with and potentially contributes to multiple cardiovascular pathologies.
The question of whether elevated inflammatory markers reflect the AF itself or underlying cardiovascular disease remains incompletely resolved. Maida et al 47 specifically addressed this by comparing AF patients with and without structural heart disease, concluding that inflammatory markers were associated with AF per se rather than underlying cardiovascular conditions. However, Barani et al 52 found associations between TNF-alpha and critical limb ischemia with concurrent AF, suggesting that systemic vascular disease influences inflammatory status. Our meta-analysis cannot definitively resolve this causality question, but the consistent elevation of TNF-alpha across diverse patient populations and study designs supports a direct relationship between TNF-alpha and the arrhythmia substrate.
The relationship between TNF-alpha and specific AF types provides insights into disease progression. Our subgroup analysis indicated that studies defining AF through extended monitoring showed different effect sizes compared to single-timepoint ECG diagnosis, though this difference did not reach statistical significance. Studies examining TNF-alpha before versus at AF diagnosis showed similar effect sizes, suggesting that inflammatory activation may precede clinically apparent AF. Amdur et al 48 demonstrated that IL-6 predicted both prevalent and incident AF in chronic kidney disease patients, supporting the concept of inflammation as a risk factor rather than merely a consequence of AF.
Several studies have explored the potential modulation of inflammatory pathways in AF management. Bielecka-Dąbrowa et al 60 reported that atorvastatin treatment showed diminished efficacy in reducing inflammatory markers in AF patients compared to those in sinus rhythm, suggesting that established AF may create a persistent inflammatory milieu resistant to conventional anti-inflammatory interventions. Tian et al 62 found that heart rate control in AF patients with heart failure reduced inflammatory markers including TNF-alpha alongside improvements in cardiac function, indicating that rhythm management strategies may have anti-inflammatory benefits.
The substantial heterogeneity observed in our meta-analysis (I2= 98.82%) represents a significant limitation that persists despite extensive subgroup analyses. While we identified some sources of variation including geographic region, year of publication, and AF type, these factors did not fully explain the observed heterogeneity. Ki et al, 56 identified in the Baujat plot as contributing disproportionately to heterogeneity, examined VacA-positive Helicobacter pylori seropositivity alongside TNF-alpha in AF patients, representing a unique study design that may explain its outlier status. The leave-one-out sensitivity analysis demonstrated that no single study dramatically influenced the overall effect size, supporting the robustness of our findings despite heterogeneity.
Measurement methodology likely contributes to heterogeneity, as studies employed various TNF-alpha quantification methods, predominantly ELISA but with different commercial kits and protocols. Dai et al 54 utilized mRNA sequencing, a fundamentally different approach compared to protein quantification methods. Martins et al 41 employed Cytometric Bead Array, which may yield different absolute values than traditional ELISA. These technical variations, combined with differences in sample handling, storage conditions, and timing of blood collection relative to AF episodes, introduce measurement variability that compounds biological heterogeneity.
Patient selection criteria and control group definition represent another source of heterogeneity inadequately addressed by available data. Studies varied in their inclusion of lone AF versus AF with structural heart disease, acute versus chronic AF presentations, and anticoagulated versus non-anticoagulated patients. Control groups ranged from healthy volunteers to patients with cardiovascular risk factors but no AF, potentially influencing baseline inflammatory status. Dungan et al 43 examined patients before their first ablation procedure, representing a specific treatment-seeking population that may differ from community-based AF cohorts.
The timing of TNF-alpha measurement relative to AF diagnosis and clinical presentation introduces additional complexity. Some studies measured inflammatory markers during acute AF episodes, while others assessed patients in chronic AF or even before AF onset. Chang et al 49 specifically examined immune regulatory pathways including PD-1/PD-L1 signaling, demonstrating that T cell activation and inflammatory cytokine secretion vary dynamically in AF patients. This temporal variability in inflammatory activation may explain some inconsistency across studies and suggests that single timepoint measurements may inadequately capture the inflammatory status relevant to AF pathophysiology.
The clinical implications of elevated TNF-alpha in AF remain to be fully defined. While our findings demonstrate a clear association, the predictive value of TNF-alpha for AF development, progression, or response to treatment requires further investigation. Li et al 55 found that TNF-alpha correlated with left atrial and pulmonary vein sizes, suggesting potential utility in risk stratification for structural remodeling. However, Chen et al 44 reported that preoperative inflammatory markers including TNF-alpha did not predict success of maze procedure, indicating limitations in using these biomarkers for procedural outcome prediction.
Several studies have examined inflammatory markers in specific clinical contexts that may inform AF management strategies. Peller et al 46 investigated adipokines alongside inflammatory markers in type 2 diabetes patients, finding that resistin and adiponectin were elevated in AF patients but did not predict future AF development. This suggests that while inflammatory and metabolic derangements associate with prevalent AF, their predictive utility for incident disease may be limited. Anaszewicz et al 53 examined the complex interplay between obesity-related adipokines, irisin, and inflammatory markers, concluding that these factors exert weak effects on cardiac structure and AF risk, with substantial individual variation.
The potential for reverse causation deserves consideration. While inflammation may promote AF through structural and electrical remodeling, AF itself may trigger inflammatory responses through mechanical stress, thrombogenic activation, and hemodynamic alterations. Berge et al 42 examined stable, out-of-hospital AF patients and found persistently elevated IL-6 and PAI-1 activity independent of acute clinical events, supporting the concept of sustained inflammatory activation in established AF. However, distinguishing primary inflammatory triggers from secondary consequences of the arrhythmia remains methodologically challenging in cross-sectional and case-control designs.
Limitations of the current meta-analysis must be acknowledged. The predominance of case-control and cross-sectional studies limits causal inference. The inability to obtain individual patient data precluded more sophisticated analyses, such as adjusting for patient-level confounders, examining interactions between TNF-alpha and comorbidities, and performing time-to-event analyses for AF onset. The significant publication bias detected suggests that negative or null findings may be underrepresented in the literature, potentially inflating the observed effect size. The high degree of heterogeneity, despite extensive subgroup analyses, indicates unmeasured confounding or effect modification that cannot be addressed with available aggregate data. The high degree of heterogeneity indicates unmeasured confounding that aggregate data cannot address. Potential unmeasured factors include timing of blood sampling relative to AF episodes acute versus chronic, variations in ELISA kits and protocols, patient-level factors like medication use including statins and anticoagulants, comorbidities such as diabetes heart failure and obesity, genetic polymorphisms in TNF-alpha pathways, and control group definitions such as healthy volunteers versus patients with cardiovascular risk factors.
Future research directions should include prospective cohort studies with serial TNF-alpha measurements to clarify temporal relationships between inflammatory activation and AF onset. Mechanistic studies examining specific TNF-alpha signaling pathways in atrial tissue would help identify potential therapeutic targets. Randomized trials testing targeted anti-inflammatory interventions in AF prevention or management could establish whether TNF-alpha represents a modifiable risk factor. Studies incorporating genetic variants affecting TNF-alpha expression and signaling could illuminate causal relationships through Mendelian randomization approaches.
Conclusion
This systematic review and meta-analysis provide strong evidence for elevated TNF-alpha levels in AF patients compared to controls, supporting inflammation as a significant component of AF pathophysiology. The association appears consistent across diverse populations and study designs, though substantial heterogeneity and publication bias necessitate cautious interpretation. The progressive elevation of TNF-alpha with increasing AF persistence suggests involvement in disease progression as well as initiation. While TNF-alpha represents a promising biomarker reflecting inflammatory processes in AF, its clinical utility for risk prediction, prognostication, or treatment guidance remains to be established through prospective studies. Further research is needed to determine whether inflammatory pathways represent viable therapeutic targets for AF prevention or management, and to identify patient subgroups most likely to benefit from anti-inflammatory interventions.
Supplemental Material
Supplemental material - Association Between TNF-Alpha Levels and Atrial Fibrillation Outcomes: A Systematic Review and Meta-Analysis
Supplemental material for Association Between TNF-Alpha Levels and Atrial Fibrillation Outcomes: A Systematic Review and Meta-Analysis by Alireza Fatemi, Bahar Amirgholami, Yasmin Yazdooei, Aylin Taghipour, Amirali Zamani Ali Ajdarkosh in Clinical and Applied Thrombosis/Hemostasis.
Supplemental Material
Supplemental material - Association Between TNF-Alpha Levels and Atrial Fibrillation Outcomes: A Systematic Review and Meta-Analysis
Supplemental material for Association Between TNF-Alpha Levels and Atrial Fibrillation Outcomes: A Systematic Review and Meta-Analysis by Alireza Fatemi, Bahar Amirgholami, Yasmin Yazdooei, Aylin Taghipour, Amirali Zamani Ali Ajdarkosh in Clinical and Applied Thrombosis/Hemostasis.
Footnotes
Acknowledgments
Special thanks to all the fellow authors who contributed to this article.
Author Contributions
Conceptualization: A.F, B.A., Data curation: A.F, B.A, A.Z, A.Aj., Formal analysis: A.F., Investigation: B.A, A.F, Y.Y., Methodology: A.F, B.A, A.T., Project administration: A.F, A.Z., Software: A.F., Supervision: A.F., Validation: A.F, B.A., Visualization: A.F, A.T., Writing – original draft: A.F, B.A, Y.Y, A.T, A.Z, A,Aj., Writing – review & editing: A.F, B.A, Y.Y, A.T, A.Z, A,Aj.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Role of the Funder/Sponsor
The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Guarantor
Alireza Fatemi accepts full responsibility for the study, including the conduct of the research, having access to the data, and controlling the decision to publish.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.