
Abstract
Objective
The aim of this study was to assess the effectiveness of an integrated, evidence-based nursing protocol combining traditional Chinese and Western medicine for the management of upper limb circulatory complications in patients undergoing transradial access (TRA) coronary intervention.
Methods
A non-randomized, sequential (before–after) comparative study was conducted in 346 patients undergoing transradial artery coronary intervention at a tertiary hospital. Patients treated between March and April 2024 received routine perioperative nursing care (control group, n = 195), whereas patients treated between October and November 2024 received an evidence-based integrated nursing protocol combining traditional Chinese medicine and Western nursing approaches (observation group, n = 151). The integrated protocol included a standardized “six-step finger exercise,” digital and early health education, optimized postoperative monitoring, and acupoint massage interventions. Upper limb swelling and pain were assessed 2 hours postoperatively using palm circumference measurements and the Numerical Rating Scale. Outcomes were compared between the two groups using chi-squared tests.
Results
Baseline characteristics were comparable between groups. The observation group demonstrated a lower incidence of upper limb swelling (21% reduction), fewer cases of moderate-to-severe swelling (13.9% reduction), and a lower incidence of pain (15.3% reduction) compared with the control group (all p < 0.05).
Conclusion
The integrated nursing protocol was associated with reductions in postoperative upper limb swelling and pain in patients undergoing TRA coronary intervention, indicating potential value in improving the management of circulatory complications.
Keywords
Introduction
Percutaneous coronary angiography (CAG) is regarded as the gold standard for diagnosing coronary artery disease (CAD), whereas percutaneous coronary intervention (PCI) is a primary therapeutic modality for patients with CAD. 1 Transradial access (TRA) has become the preferred vascular access route for PCI due to its advantages, including simplified hemostasis, a lower incidence of vascular complications, earlier patient mobilization, and accelerated recovery. 2
Mechanical compression, typically achieved using devices such as spiral compression hemostats, is widely used to achieve hemostasis at the radial artery puncture site following TRA coronary intervention. However, this approach has been frequently associated with upper limb circulatory complications, including numbness, swelling, ecchymosis, and pain. These complications pose significant challenges in the perioperative management of patients undergoing TRA coronary intervention.3,4
Traditional Chinese medicine (TCM), through both pharmacological and non-pharmacological interventions, has demonstrated effectiveness in improving circulation.5,6 In this study, an evidence-based integrated perioperative nursing protocol, combining traditional Chinese and Western medicine, was implemented in patients who received mechanical compression for radial artery hemostasis during TRA coronary intervention. The protocol was associated with significant improvements in compression-related upper limb circulatory symptoms. The findings are presented as follows.
1. Participants and Methods
1.1. Participants
Individuals who underwent coronary intervention in the cardiology department of a tertiary hospital were enrolled in this study. The control group comprised 195 patients treated between March 1 and April 30, 2024. The observation group included 151 patients who underwent coronary intervention between October 15 and November 15, 2024.
Inclusion criteria: ① Coronary intervention via the radial artery approach was performed. ② Full consciousness and the ability to respond accurately to verbal questions were maintained. ③ Informed consent was provided, and participation in the study was voluntary.
Exclusion criteria: ① Pre-existing swelling, numbness, ecchymosis, or other circulatory complications were present. ② A diagnosis of depression, anxiety disorders, or other psychiatric conditions was documented.
1.2. Research Methods
1.2.1. Interventional Methods
Control group: Participants in the control group were provided with routine perioperative nursing care for TRA coronary intervention in accordance with departmental protocols. The intervention included: ① A spiral compression hemostat was applied to the radial artery puncture site immediately following the procedure. Compression force was adjusted to achieve hemostasis while avoiding excessive pressure. The device was gradually loosened at 2, 4, and 6 hours postoperatively by releasing one loop at each time point. Complete pressure release was achieved after the third adjustment. In cases of marked swelling, ecchymosis, or bleeding during compression, the pressure was reduced accordingly. If bleeding was observed at the puncture site during loosening, pressure was reapplied until hemostasis was achieved, and the loosening schedule was adjusted as required. The hemostat was removed the following morning, and the puncture site was disinfected. ② Postoperatively, verbal instructions on performing upper limb and finger exercises during radial artery compression were provided by nursing staff to promote circulation. ③ Routine postoperative monitoring was conducted, including assessment of puncture-site bleeding, hematoma formation, hand swelling, pain, skin temperature, skin color, numbness, and distal circulation, and coordination with physicians was undertaken for the management of any complications.
Observation group: Participants in the observation group were provided with an evidence-based, integrated perioperative nursing protocol combining TCM and Western medicine approaches. All interventions were implemented by trained members of the research nursing team according to standardized procedures. This protocol was developed based on the PIPOST framework and informed by a review of relevant literature and current evidence-based guidelines. In addition to receiving the same mechanical compression hemostasis procedure as the control group, the observation group was provided with the following components of the integrated protocol (Figure 1):7-10 (1) Core intervention Flowchart of the integrated perioperative nursing protocol, illustrating the six-step finger exercise, acupoint stimulation, health education, postoperative monitoring schedule, and adjunctive TCM interventions
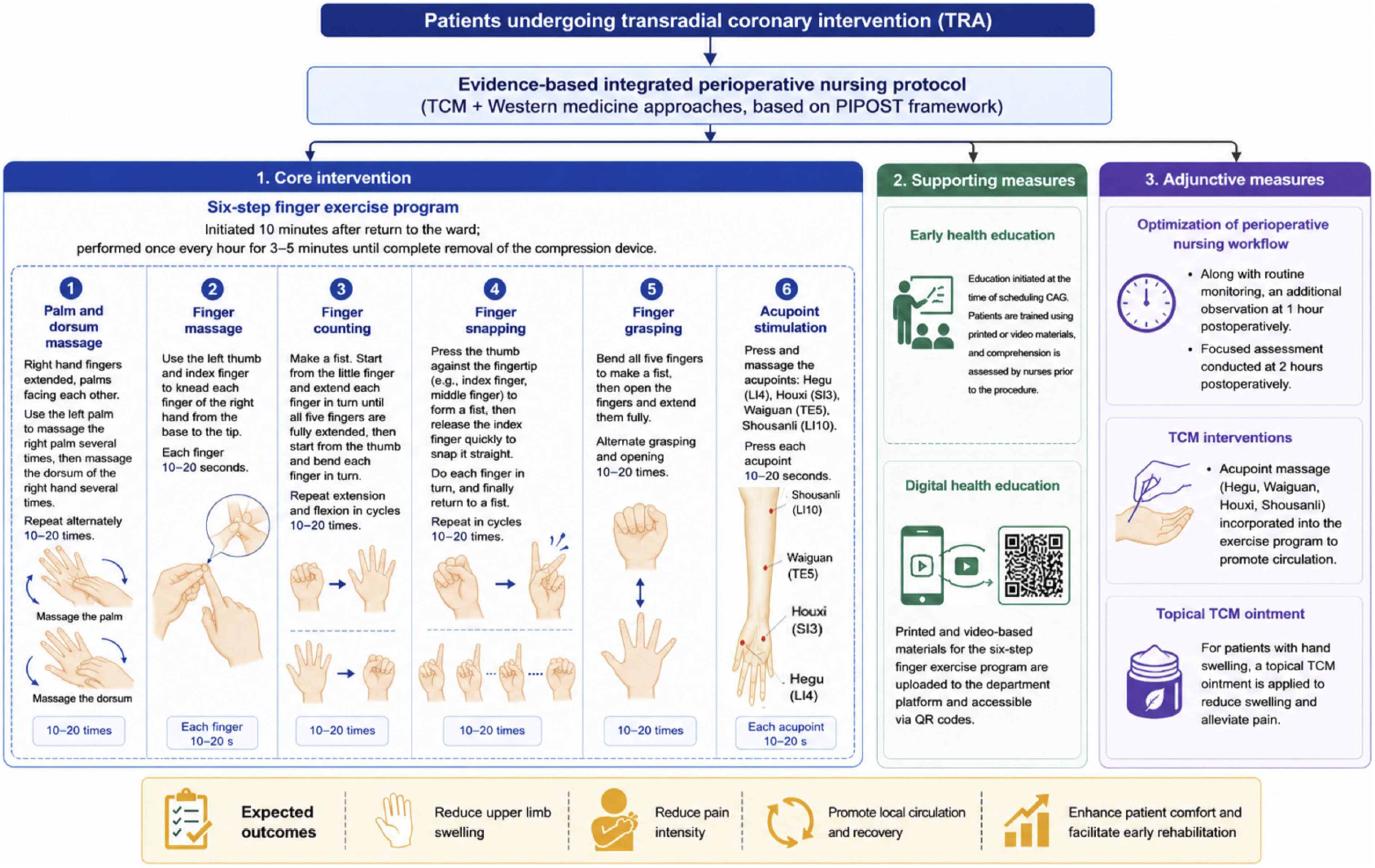
The primary component consisted of the “six-step finger exercise,” a standardized upper limb activity designed to promote local circulation. The six steps included palm massage, dorsum hand massage, finger massage, finger counting movements, finger snapping movements, and finger grasping exercises combined with acupoint stimulation. The exercise was initiated 10 minutes after return to the ward and was performed once every hour for 3–5 minutes until complete removal of the compression device. (2) Supporting measures
To improve adherence and standardization, the following measures were implemented: ① Digital health education: Printed and video-based instructional materials for the “six-step finger exercise” were developed. The instructional videos demonstrated the standardized exercise procedures, movement frequency, precautions, and acupoint locations. The videos were uploaded to the department’s health education platform and made accessible via QR codes to facilitate patient access; ② Early health education: Education was initiated at the time of scheduling CAG. Patients were trained using printed or video materials, and comprehension was assessed by nurses prior to the procedure. Patients were educated regarding the purpose, timing, frequency, and standardized procedures of the exercise protocol before intervention implementation. (3) Adjunctive measures ① Optimization of perioperative nursing workflow: Along with the routine monitoring, an additional observation time point at 1 hour postoperatively was incorporated, with focused assessment conducted at 2 hours after the procedure to evaluate puncture-site bleeding, hematoma formation, hand swelling, pain, skin temperature, skin color, and distal circulation status for early identification of complications. ② Integration of TCM interventions: Acupoint massage (e.g., Hegu [LI4], Waiguan [TE5], Houxi [SI3], Shousanli [LI10]) was incorporated into the exercise protocol to promote circulation. For patients presenting with postoperative hand swelling or pain, a physician-prescribed topical TCM ointment with blood-activating and swelling-relieving effects was externally applied around the affected area. The ointment was prepared from pulverized Chinese herbal medicine and formulated into a paste for topical application. The intervention was administered by trained members of the research nursing team according to standardized nursing procedures to promote local circulation, reduce swelling, and alleviate pain.
1.2.2. Evaluation Indicators
(1) Swelling severity of the upper limb: Swelling was assessed at two hours postoperatively using a flexible measuring tape.
11
Participants were instructed to hold their fingers together, and the circumference of the palm was measured at the level of the second phalanx of the thumb.
12
The degree of swelling was determined by calculating the difference between postoperative and preoperative measurements. Swelling severity was classified as follows: a swelling value < 0.5 cm indicated no swelling; 0.5 ≤ swelling value < 1.4 cm indicated mild swelling; 1.4 ≤ swelling value < 3.0 cm indicated moderate swelling; and a swelling value ≥ 3.0 cm indicated severe swelling. (2) Pain intensity in the affected limb: Pain intensity in the affected upper limb was assessed at two hours postoperatively using the Numerical Rating Scale. Scores were interpreted as follows: 0 points indicated no pain; 1–3 points indicated mild pain; 4–6 points indicated moderate pain; and 7–10 points indicated severe pain.
1.2.3. Statistical Analysis
All data were independently computed by two researchers and analyzed using SPSS software, version 29.0. Categorical variables were expressed as frequencies and percentages. The chi-squared (χ2) test was used for intergroup comparisons and for the assessment of changes in group composition. A value of p < 0.05 was considered statistically significant. The analysis focused on between-group comparisons using univariate statistical methods, and no multivariate analysis was performed.
1.2.4. Ethical Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethics Committee of China–Japan Friendship Hospital (Approval No.: No.2024-KY-031). Written informed consent was obtained from all participants prior to inclusion in the study.
1.2.5. Consent for Publication
Not applicable.
2. Results
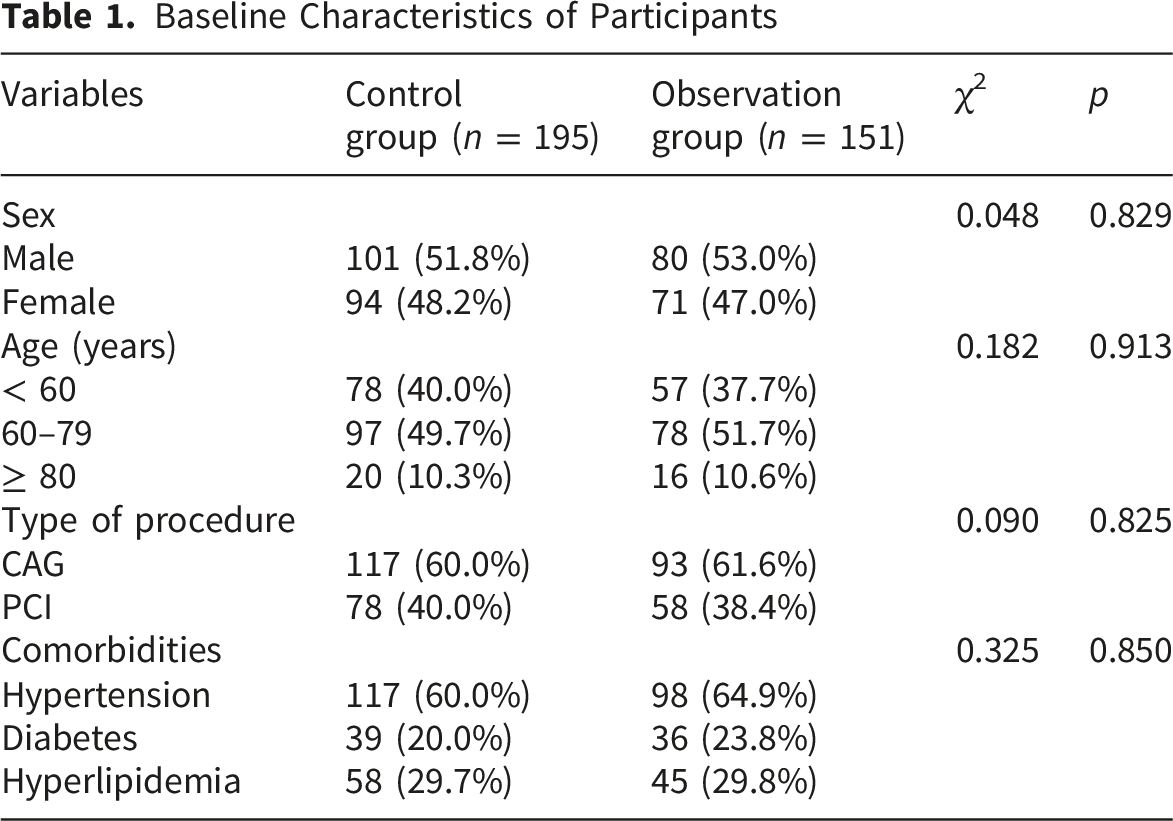
2.1. Comparison of General Characteristics Between Groups
Baseline Characteristics of Participants
2.2. Comparison of Upper Limb Swelling Between Groups
Comparison of Upper Limb Swelling Between Groups
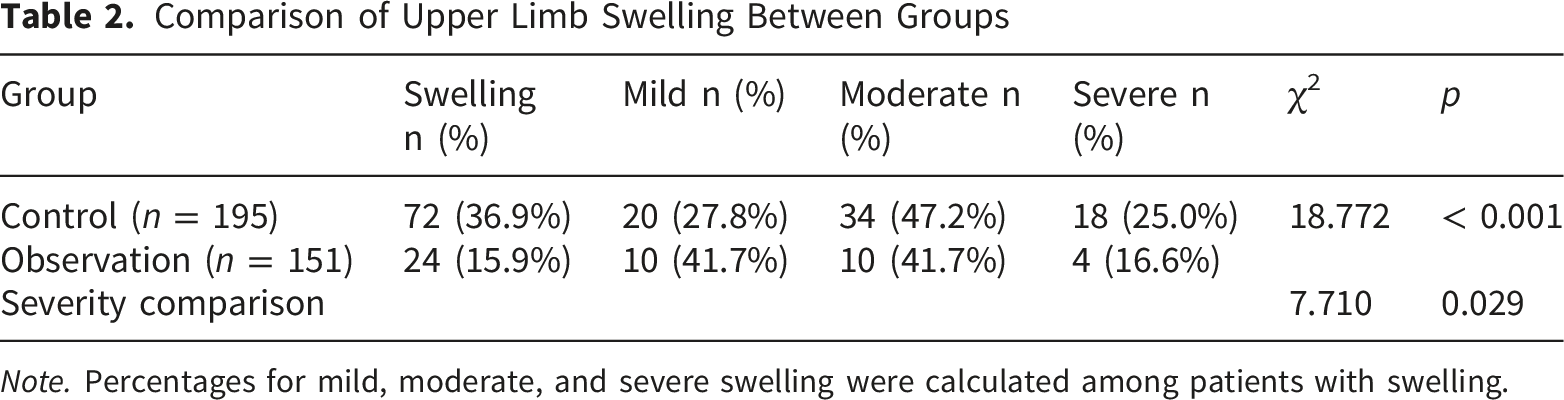
Note. Percentages for mild, moderate, and severe swelling were calculated among patients with swelling.
2.3. Comparison of Upper Limb Pain Intensity Between Groups
Comparison of Upper Limb Pain Intensity Between the Two Groups
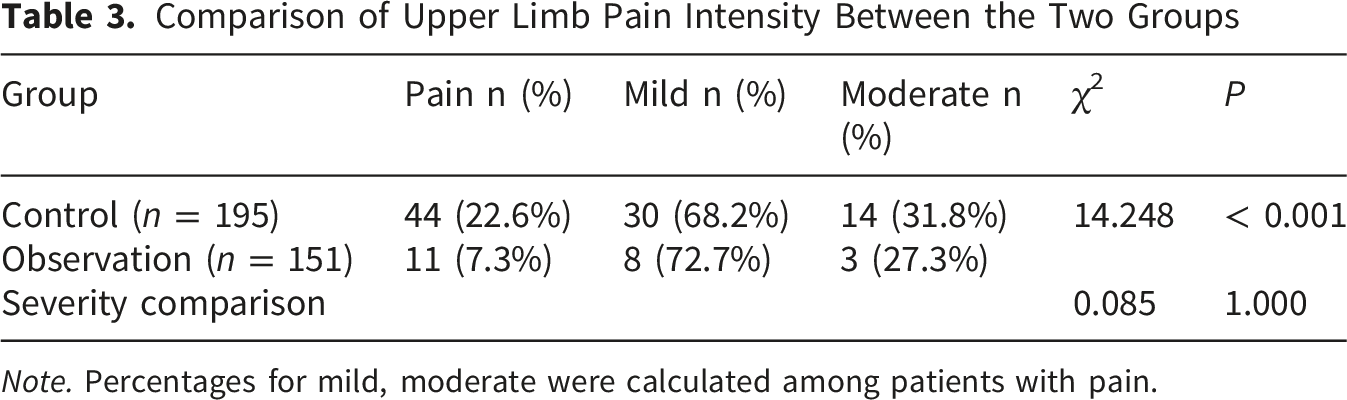
Note. Percentages for mild, moderate were calculated among patients with pain.
3. Discussion
3.1. Impact of Radial Artery Compression Hemostasis on Circulatory Complications
The findings of this study indicated that the incidence rates of upper limb swelling and pain in the control group were 36.9% and 22.6%, respectively. Although these rates decreased to 15.9% and 7.3% in the observation group, circulatory complications associated with radial artery compression hemostasis following coronary intervention remained clinically relevant. The use of mechanical pressure on the wrist area may partially obstruct venous return from the distal limb, resulting in local accumulation of blood and interstitial fluid, which manifests as edema. Compression of the median and radial nerves by mechanical pressure and localized edema may lead to pain and numbness in the affected limb. As the radial artery predominantly supplies blood to the index finger and thumb, sustained compression may impair perfusion to these digits, contributing to numbness and pain in the fingers.13,14
Although these complications are generally less severe than other TRA-associated vascular events, such as radial artery perforation, occlusion, spasm, pseudoaneurysm, or hematoma, they may still significantly affect patient comfort. In more severe cases, these complications may be associated with psychological conditions such as anxiety and fear, which may adversely affect postoperative recovery. 15 Therefore, targeted interventions during the hemostasis period are required to enhance distal circulation and reduce the severity and incidence of swelling and pain.
3.2. Efficacy of an Integrated TCM and Western Medicine Nursing Protocol
The findings of this study indicated a significant reduction in both the incidence and severity of swelling, including moderate-to-severe cases, in the observation group. These results were consistent with those reported by Liu et al. 16 The protocol included structured finger exercises, comprising palm massage, finger flexion, and stretching movements. These activities were designed to facilitate venous and lymphatic return from the distal upper limb, thereby reducing edema and alleviating nerve compression. These exercises enhanced blood circulation and increased blood supply to the muscles and joints of the hand.17,18
Acupoint massage was incorporated into the exercise regimen, targeting specific sites including Hegu (LI 4), Waiguan (TE 5), Houxi (SI 3), and Shousanli (LI 10). These acupoints facilitate the movement of blood and qi, activate meridians and collaterals, relieve muscle spasm, and reduce pain in the affected limb. 19 The topical application of TCM ointments, recognized for their symptom-relieving and analgesic properties, was used. These preparations promote symptom relief through transdermal absorption and localized action. 20 Collectively, the intervention demonstrated the clinical value of integrating TCM and Western medicine approaches in the perioperative nursing care of patients undergoing TRA coronary intervention.
3.3. Advantages of a Standardized Perioperative Nursing Protocol
The implementation of a standardized perioperative nursing protocol in this study emphasized early health education and structured postoperative monitoring intervals. Insufficient functional exercise of the affected limb may increase the risk of complications such as hematoma or thrombosis, whereas excessive movement may disrupt hemostasis and impair puncture site healing. The protocol provided structured guidance through educational materials, including both video and printed formats, enabling patients to perform appropriate upper limb exercises consistently.
Postoperative monitoring was initiated within the first hour after the procedure, enabling timely adjustment of hemostatic device pressure to prevent excessive compression. For patients presenting with early signs of circulatory complications, prompt diagnosis and intervention, including the use of TCM ointments, contributed to symptom alleviation.
This evidence-based protocol leveraged the complementary strengths of TCM and Western medicine nursing practices. The integration of acupoint massage and topical TCM ointments with structured health education and systematic observation was associated with improved peripheral circulation during the compression phase, promotion of correct implementation of upper limb exercises, and facilitation of early detection and management of circulatory complications.
3.4. Limitations
Several limitations were identified in this study. First, as a single-center study with a non-randomized, time-sequential (before–after) design, potential temporal bias and residual confounding could not be fully excluded, which may have influenced the internal validity of the findings. Although baseline characteristics were comparable between groups, unmeasured factors may still have been present. Second, only univariate analyses were performed, and no multivariate adjustment was conducted; therefore, the independent effect of the intervention could not be fully determined, and the findings should be interpreted with appropriate caution. In addition, because the present study adopted a multimodal integrated perioperative nursing protocol combining multiple components, including finger exercise, acupoint massage, TCM ointment application, health education, and enhanced monitoring, the independent contribution of each individual component could not be separately evaluated. Third, a formal a priori sample size (power) calculation was not performed, which may have affected the statistical robustness and generalizability of the results. Future studies with more rigorous designs, including randomized controlled trials, larger and more diverse populations, component-specific intervention analyses, and multivariate analyses, are warranted to further validate these findings and confirm their reliability.
4. Conclusion
This study demonstrated that a standardized, integrated perioperative nursing protocol combining TCM and Western medicine approaches was associated with a lower incidence and severity of upper limb swelling and pain related to radial artery compression hemostasis following TRA coronary intervention.
The implementation of this evidence-based protocol may have facilitated early identification and intervention for circulatory complications, improved the quality and consistency of nursing care, and promoted improved postoperative comfort and recovery in patients undergoing TRA procedures. These findings underscore the value of integrating traditional and modern nursing practices to optimize perioperative outcomes.
Footnotes
Ethical Considerations
This study was conducted with approval from the Ethics Committee of China-Japan Friendship Hospital (No.2024-KY-031). This study was conducted in accordance with the declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all participants.
Author Contributions
Conception and design of the research: Qiao Wang, Hongyue Ge. Acquisition of data: Xiaoyun Wang, Qianqian Guo, Yanyan Nan, Yan Jin, Sibo Liu. Analysis and interpretation of the data: Qianqian Guo, Yanyan Nan, Yan Jin, Sibo Liu. Statistical analysis: Qiao Wang, Xiaoyun Wang. Obtaining financing: Peng Yang. Writing of the manuscript: Qiao Wang, Hongyue Ge. Critical revision of the manuscript for intellectual content: Peng Yang. All authors read and approved the final draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Key Research and Development Program of China (No.2023YFC3503702).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.