
Abstract
Aim
To explore the causal effects of protein C and protein S on ischemic stroke (IS) risk.
Methods
Employing a two-sample bidirectional Mendelian randomization (MR) framework, we investigated the causal association between protein C, protein S and anti-thrombin with ischemic stroke and further performed the mediating analysis based on several risk factors for IS. Then, systematic review and meta-analysis of relevant literature was conducted to validate the association between protein C and ischemic stroke.
Results
Genetic data from a genome-wide association study involving 440,328 individuals, including 34,217 IS patients and 406,111 controls, revealed odds ratios for IS per standard deviation (SD) increases of 0.918 (95% CI: 0.884-0.954; P=1.027e-05) for protein C, 0.997 (95% CI: 0.986-1.035; P=1.027e-05) for protein S, and 0.990 (95% CI: 0.895-1.094; P=8.383e-01) for anti-thrombin (three anticoagulation factor). Mediation analysis indicated that body mass index (BMI) partially mediated this effect, with a mediated proportion of 5.88% (95% CI, 2.236% to 7.232%). In the meta-analysis of 2107 IS patients and 12209 healthy controls, we found that patients with decreased protein C had a significantly higher risk of IS compared with controls (risk ratio: 5.47; 95% CI 3.33, 9.00).
Conclusion
These findings suggest a potential relationship between protein C and ischemic stroke and BMI mediates this causal relationship, which might offer prevention strategies targeting protein C and ischemic stroke.
Introduction
Stroke is a prevalent neurological condition, with ischemic stroke (IS) accounting for approximately 70–80% of adult cases and its incidence rising annually. 1 Globally, stroke remains the second-leading cause of death, responsible for 6.2 million deaths (11.1% of total deaths) in 2015, and ranks third as a combined cause of death and disability (4.7%) in 2019. In individuals over 65, incidence reached 1,043/100,000 in men and 1,068/100,000 in women in 2019. 2 The Global Burden of Disease (GBD) 2023 highlighted 33,216,443 cases of ischemic stroke globally, resulting in 3,293,397 deaths in the same year.
Our previous research unveiled coagulation dysfunction as a risk factor in hematoma progression during brain insults. 3 However, the association between anticoagulation factors and ischemic stroke remains to be definitively elucidated. Notably, a lower protein C (PC) level has been linked to ischemic stroke, as opposed to ischemic heart disease. 4 Some studies have posited that reduced anticoagulant protein levels are linked to increased IS risk, as protein C aids in anticoagulation, thereby promoting thrombolus resolution and improving outcomes.5,6 However, data on the association between plasma PC, protein S (PS), antithrombin (AT), and IS onset have been inconclusive and controversial, particularly as increased activated protein C (APC) resistance is associated with recurrent spontaneous abortion. 7 Other observational studies and random-controlled trials (RCT)s have demonstrated no benefit or even increased mortality risk when relative protein C is increased via giving fresh frozen plasma. 8 A deficiency of protein C, and thus APC activity, leads to an inability to inactivate clotting factors and control thrombin production. 9
Mendelian randomization (MR) leverages genetic variants as instrumental variables to mimic the random allocation of alleles from parents to offspring, thereby circumventing confounding and reverse causality inherent to observational studies. 10 To explore the potential causal relationship between anticoagulant factors — particularly PC — and IS risk, we performed a two-sample bidirectional MR analysis, which distinguishes variants linked to the risk factor of interest from potential pleiotropic effects, ensuring robust causal inference. Given the importance of modifiable risk factors in IS prevention and management, we further conducted a two-step MR analysis to investigate mediating pathways from PC to IS through risk factor–related phenotypes. 11
Methods and Materials
Study Design and Data Sources
In accordance with prior research, we devised two-sample Mendelian randomization (MR) methods to assess the causal impact of protein C, protein S, and AT on ischemic stroke (IS) using genetic predictors of PC, PS, and AT levels as instrumental variables (IVs). Additionally, various clinical risk factors linked to IS incidence, including BMI, smoking, systolic blood pressure (SBP), diabetes mellitus (DM), and obesity, were incorporated. Single nucleotide polymorphisms (SNPs) serving as IVs for each trait were sourced from previously published genome-wide association studies (GWAS)12-14 and pruned to obtain independent genetic variants (linkage disequilibrium (LD) r^2 < 0.001; clumping distance of 1000 kb). An F-statistic exceeding ten was deemed sufficiently robust to predict the exposure of interest.15,16 We exclusively utilized datasets comprising individuals of European ancestry to mitigate selection bias and bolster analysis robustness.
Data for Exposure
SNPs associated with protein C and protein S at genome-wide significance (P <5 × 108) were obtained from a published GWAS paper included 10,708 participants of European ancestry. 17 As the same dataset lacked SNPs for antithrombin (AT), we turned to another dataset encompassing 3,301 participants of European ancestry. 18 Protein C levels were expressed as relative values (percentage of a reference normal pool) as reported in the source GWAS.
Data for Outcome
We relied on GWAS summary data on IS from two contributing studies encompassing 440,328 participants of European ancestry, comprising 7,537,579 SNPs. The coefficients for each SNP were transformed into the log odds ratio (OR) for IS. Additionally, we obtained GWAS summary data on cardioembolic IS from the Neale lab consortium, involving 211,763 participants of European ancestry.
Statistical Analysis
We employed the two-sample MR method to evaluate the causal effects of anticoagulant traits on outcomes, presenting results as ORs and 95% confidence intervals (CIs). Harmonization of SNP exposure and outcomes was conducted as previously described. 19 Five MR approaches (random-effect IVW, weighted median, MR-Egger, simple mode, and weighted mode) were employed to address potential heterogeneity and horizontal pleiotropy across causal estimates. 20 The weighted median was implemented to assess the robustness of the consistent estimation if more than 50% of the IVs were valid. 21 We performed MR-Egger analysis using weighted linear regression between SNP exposure and SNP outcome. We detected the presence of potentially horizontal pleiotropy by the intercept of the MR-Egger coefficient. 22 Additionally, we used the MR-PRESSO test to detect and calibrate potential pleiotropic outliers in summary-level MR analyses. 23 Heterogeneity statistics were performed using scatter plots and Cochran’s Q tests between causal estimates from multiple genetic variants. 24
MR-IVW Study
To explore causal estimates from MR studies, we ensured that genetic variants met three key assumptions. We excluded SNPs strongly associated with the outcome, harmonized SNP effects on exposure and outcome, and removed palindromic SNPs with intermediate allele frequencies and outlier pleiotropic SNPs via heterogeneity testing.
We then performed a two-sample bidirectional MR to assess the association of relative PC, PS and ATAT with IS risk. The multivariable MR-IVW method validated the causal associations between the PC and IS independent of other anticoagulant factors. We performed multivariable MR using the inverse-variance weighted approach to estimate the direct causal effects of PC, PS and AT on IS. We further performed the MR Steiger test to estimate the potential reverse causal impact of diet compositions on IS. A two-sided P < 0.05 was defined as a significant causal association. All statistical analyses were implemented using R software version 3.6.2 (‘TwoSampleMR’ 25 package version 0.5.2).
Potential Mediators
We incorporated genome-wide association study (GWAS) data sources focusing on potential mediators, specifically obesity-related phenotypes, while ensuring maximal sample sizes and avoiding sample overlap (Supplementary Table 1). The selected mediators encompassed diverse information, including: BMI from 461,460 individuals included in the Genetic Investigation of Anthropometric Traits (ukb-b-19953); smoking from 607,291 individuals included in the GSCAN (ieu-b-4877); obesity from 463,010 individuals included in MRC-ICU (ukb-b-15541), SBP in up to 757,601 individuals from the International Consortium of Blood Pressure Traits; and summary statistics for DM in up to 655,666 individuals (ebi-a-GCST006867).
Meta-Analysis
Two investigators (LS and CY) independently searched electronic databases, including PubMed, Web of Science and the Cochrane Library, for studies related to Protein C and ischemic stroke published from database inception to 01 March 2024. The keywords and subject terms used were (‘protein C’ OR ‘protein C deficiency’) AND (‘ischemic stroke’). The inclusion criteria were: (i) cohort, case–control or cross-sectional study design; (ii) cases were patients diagnosed with IS, and controls were healthy individuals, regardless of sex or ethnicity; and (iii) sufficient data on the association between PC and IS. The exclusion criteria were: (i) cellular and animal experiments; (ii) systematic reviews or meta-analyses; (iii) incomplete or insufficient data on the association between PC and IS; in addition, those with smaller sample sizes were excluded. References of eligible studies were manually checked to identify additional studies for inclusion.
Data Extraction and Quality Assessment
For eligible studies, the same two investigators extracted data from each article onto a standardized form. Disagreements were resolved by discussion. Information including first author, year of publication, ethnicity of the study population, sample size, assays used for measuring protein C, and effect size of the association between PC and IS were recorded. The quality of each included study was assessed using the modified Newcastle–Ottawa Scale, 26 with scores ranging from 0 to 9 points. Only studies with a quality score of 7–9 points were included here.
Results
Univariable Mendelian Randomization (MR) Analysis
Mendelian Randomization Results for the Relationship Between Protein C and Ischemic Stroke
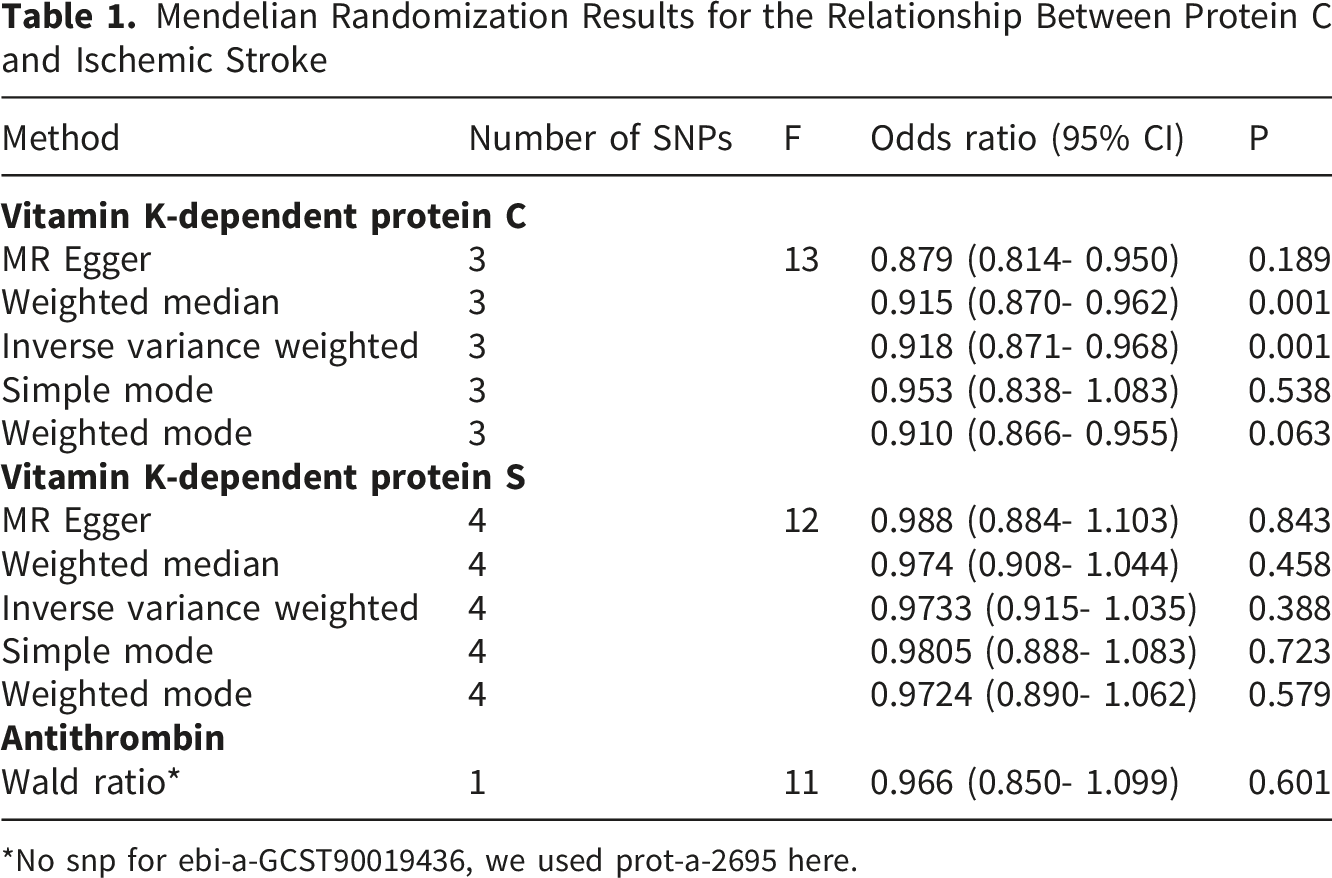
*No snp for ebi-a-GCST90019436, we used prot-a-2695 here.
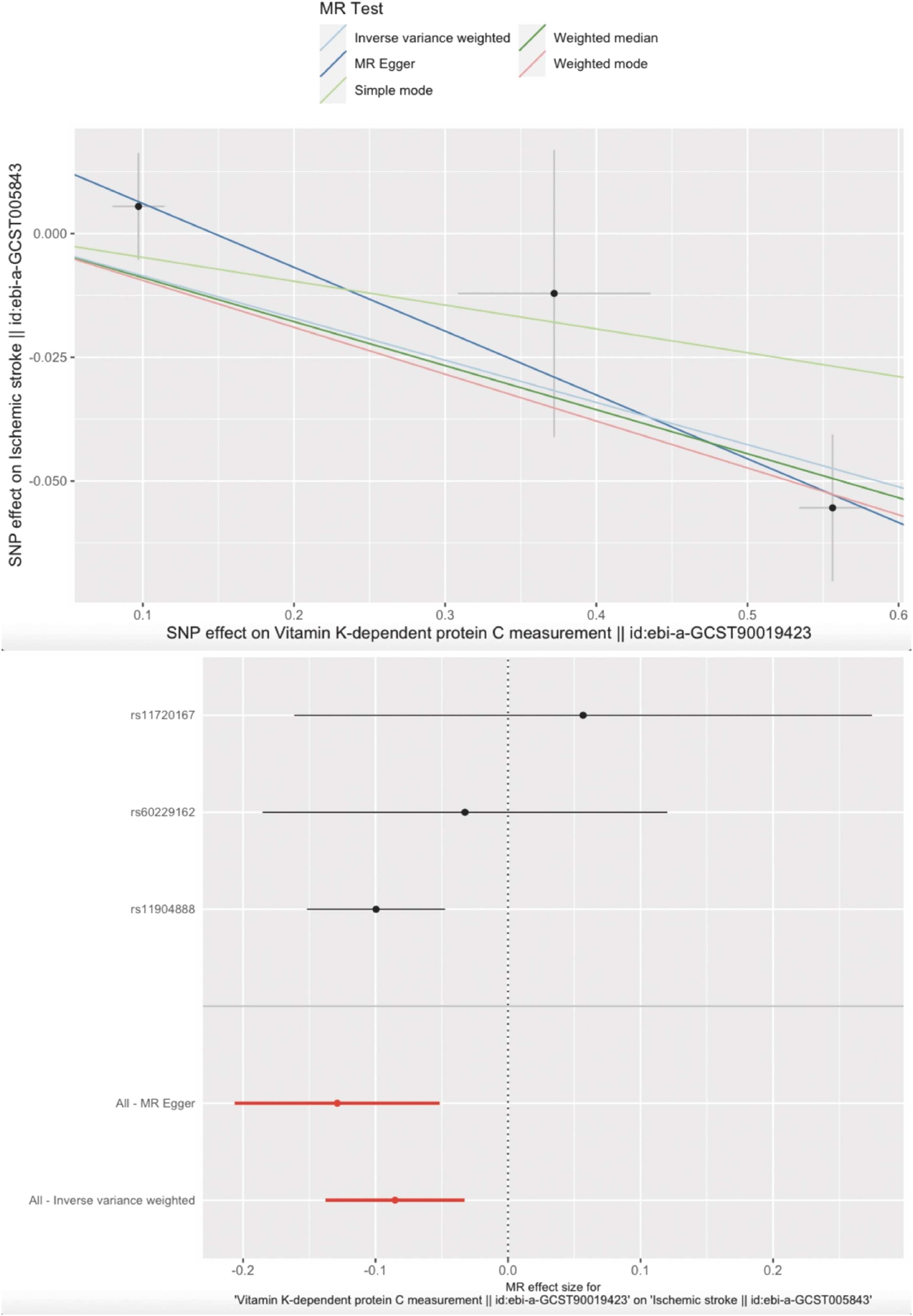
MR plots for the relationship of relative protein C with ischemic stroke. (A) Scatter plot of SNP effects on relative PC level versus IS, with the slope of each line corresponding to the estimated MR effect per method. The data are expressed as raw β values with 95% CIs. (B) Forest plot of individual and combined SNP MR-estimated effect sizes. The effect estimates represent the log odds for IS per one-s.d. increase in mean relative PC level, and the error bars represent 95% CIs
Multivariable Mendelian Randomization (MR) Analysis
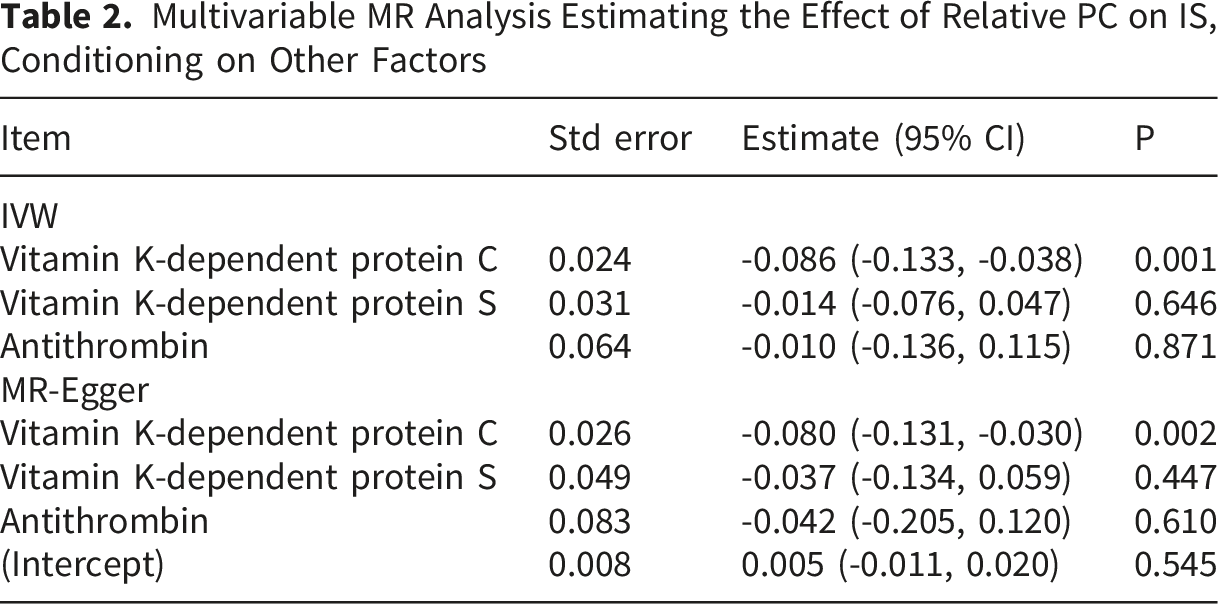
Multivariable MR Analysis Estimating the Effect of Relative PC on IS, Conditioning on Other Factors
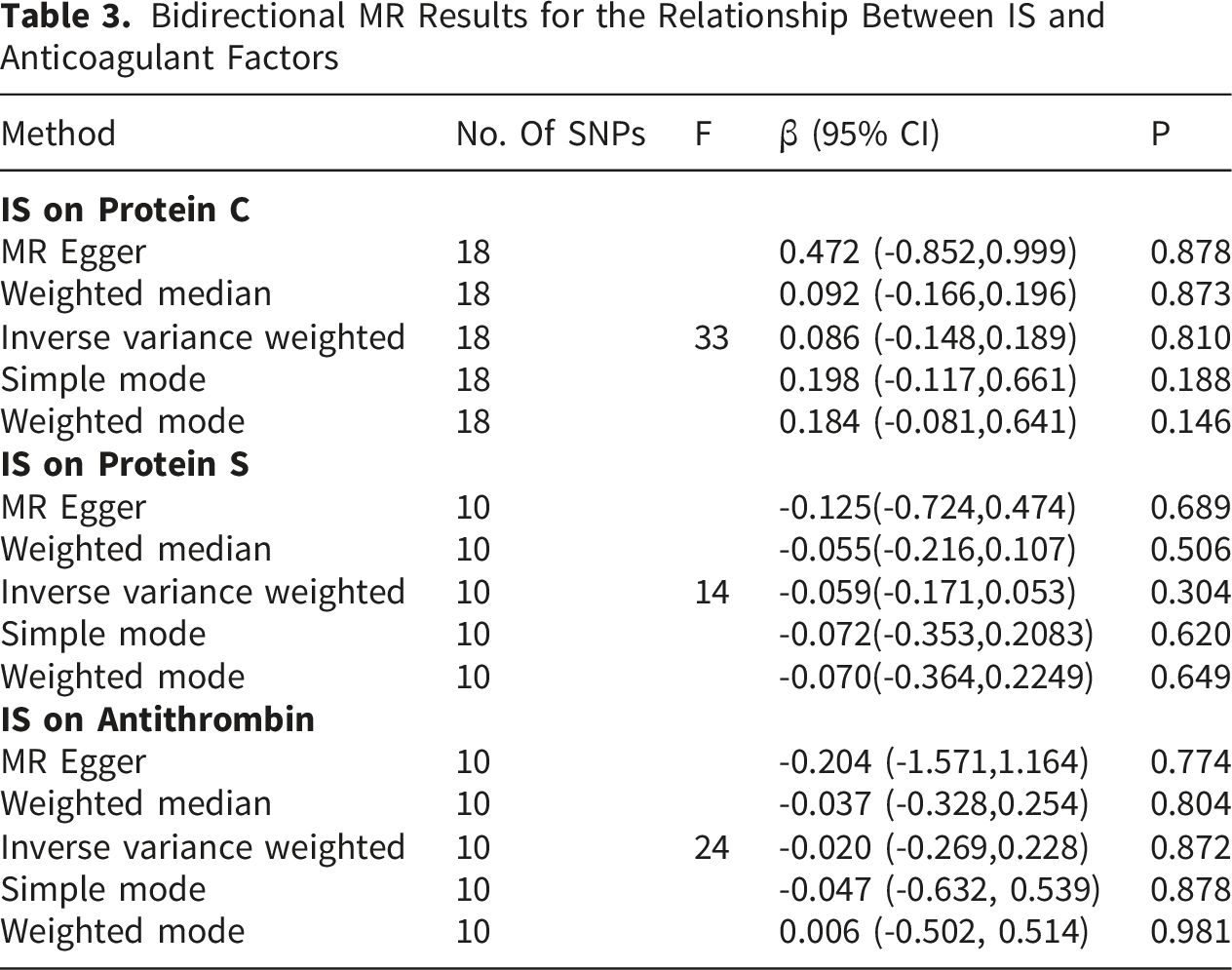
Effect of IS on Relative PC Level
Bidirectional MR Results for the Relationship Between IS and Anticoagulant Factors
Mediation Analysis
Given the critical role of risk factors in venous thrombosis prevention and management,
11
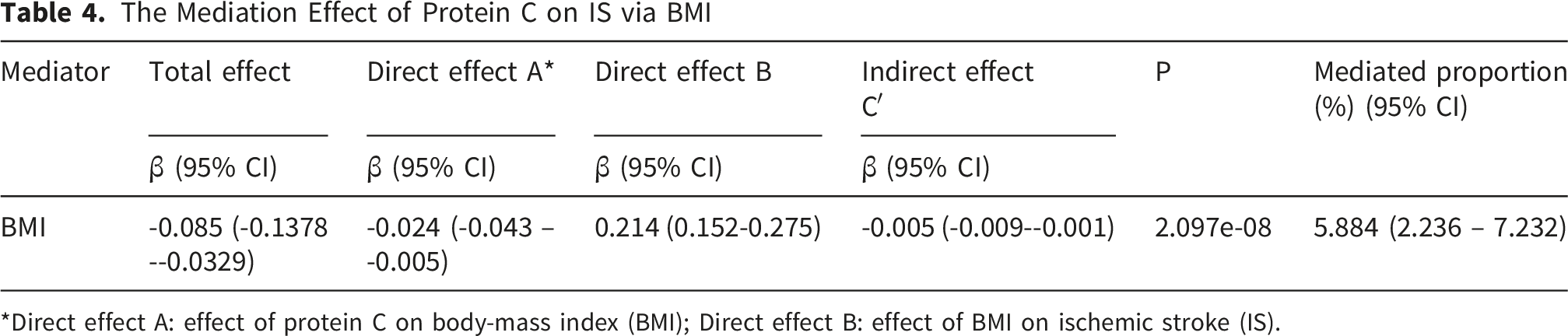
we conducted a two-step MR analysis to investigate the mediating pathway from relative PC to IS via five obesity-related phenotypes: BMI, smoking, systolic blood pressure (SBP), diabetes mellitus (DM), and obesity (Figure 2A). In the first step, among the five candidate mediators, only BMI showed a causal relationship with relative PC, whereby higher PC was associated with lower BMI (IVW β = −0.024; 95% CI: −0.043 to −0.005; P = 0.014) (Figure 2B; Supplementary Tables 2–4). In the second step, BMI demonstrated a significant causal effect on IS risk (IVW OR: 1.236; 95% CI: 1.164–1.313; P = 4.880×10-12), consistent across weighted median, weighted mode, and MR-Egger methods (Figure 2B; Supplementary Table 5). Multivariable MR confirmed this finding (IVW OR: 1.238; 95% CI: 1.164–1.317; P = 1.116×10-11), while other obesity-related measures showed no significant effects on IS (Supplementary Table 6). The estimated indirect effect of relative PC on IS mediated through BMI was −0.005 (95% CI: −0.009 to −0.001; P = 2.10×10-8), with BMI accounting for 5.88% (95% CI: 2.24%–7.23%) of the total effect (Table 4). Mediation analysis of the effect of relative protein C on ischemic stroke via potential mediators. (A) Two-step MR analysis framework. Step 1 estimated the causal effect of the exposure on the potential mediators, and step 2 assessed the causal effect of the mediators on IS risk. ‘Direct effect’ indicates the effect of relative PC level on IS risk after adjusting for the mediator. ‘Indirect effect’ indicates the effect of relative PC level on IS risk through the mediator. IVs, instrumental variables. (B) Summary MR estimates derived from the IVW, weighted median, weighted mode, and MR-Egger methods for the effect of relative PC level on BMI (left) and the effect of BMI on IS (right). The error bars represent 95% CIs. All statistical tests were two-sided. P < 0.05 was considered significant The Mediation Effect of Protein C on IS via BMI *Direct effect A: effect of protein C on body-mass index (BMI); Direct effect B: effect of BMI on ischemic stroke (IS).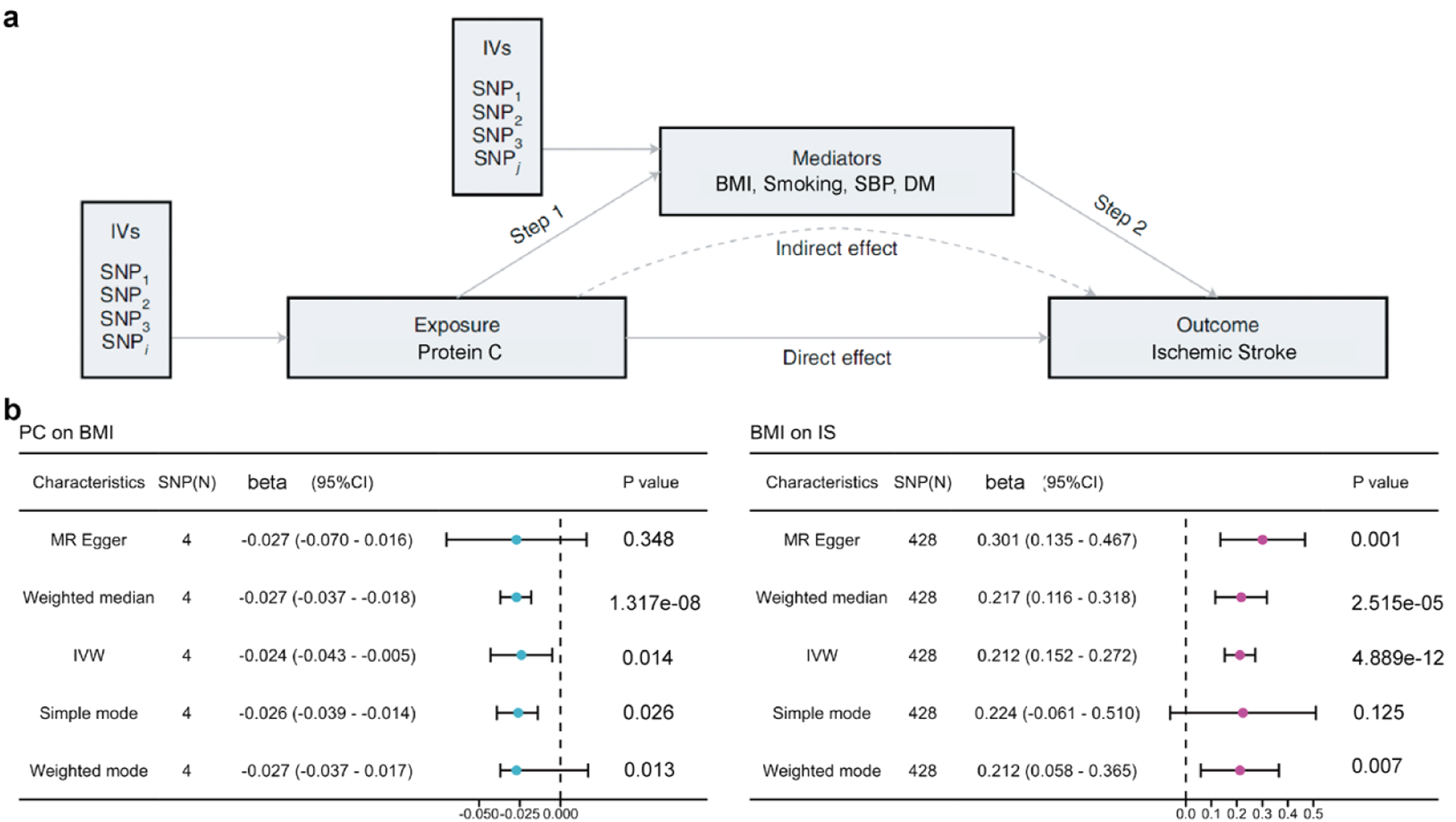
Patients With Reduced PC had a Higher Risk of IS Relative to Controls
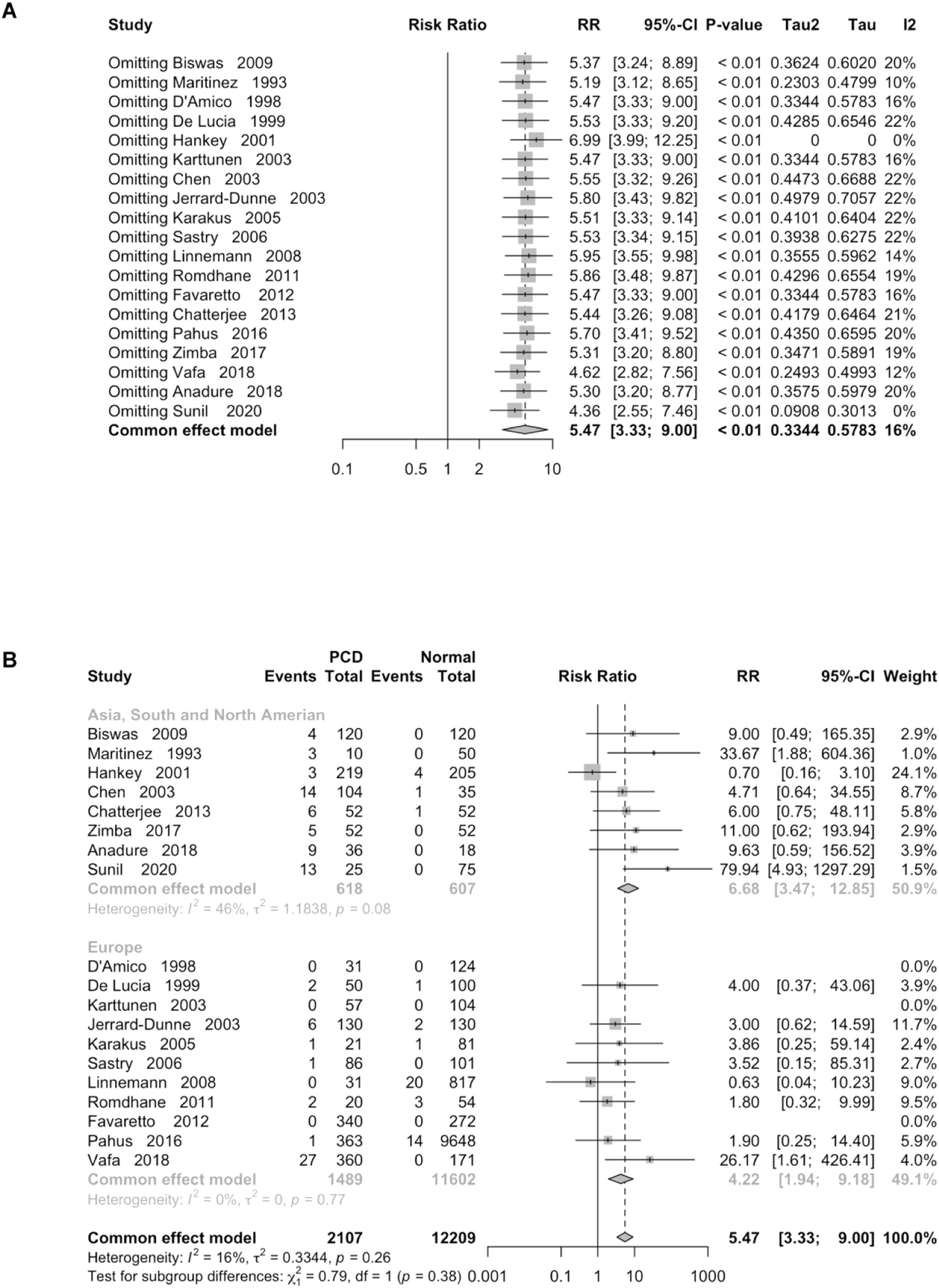
A total of nineteen studies (2107 IS cases and 12209 controls) were included in the meta-analysis. There were eleven case–control studies, two prospective cohort study, two retrospective cohort study, one nested case–control study, and one cross-sectional study. Detailed information for these included studies is listed in Supp Table 6 (named Meta1). The included studies demonstrated strong statistical consistency. There was no statistically significant heterogeneity observed between them(I2=16.0%, P=0.26). Therefore, we used the random-effects model to combine the effect sizes of the association between PC and IS. Figure 3A shows the forest plot of RR (95% CI) of the PC in IS patients relative to controls. The funnel plot was symmetrical (Figure 3B). Sensitivity analysis omitting one study at a time suggested none of these studies had a strong effect on the combined effect estimates (Figure 4A). Stratification analyses showed that the heterogeneity in Asia and America was higher than the Europe group (Figure 4B). Meta-analysis for protein C on ischemic stroke. (A) Forest plot of RR (95% CI) of the PC in IS patients relative to controls. (B) Funnel plot of RR of the PC in IS patients relative to controls Sensitivity analysis for the Meta-results. (A) Sensitivity analysis omitting one study at a time show the effect on the combined effect. (B) Stratification analyses showed that the heterogeneity in Asia, America and the Europe group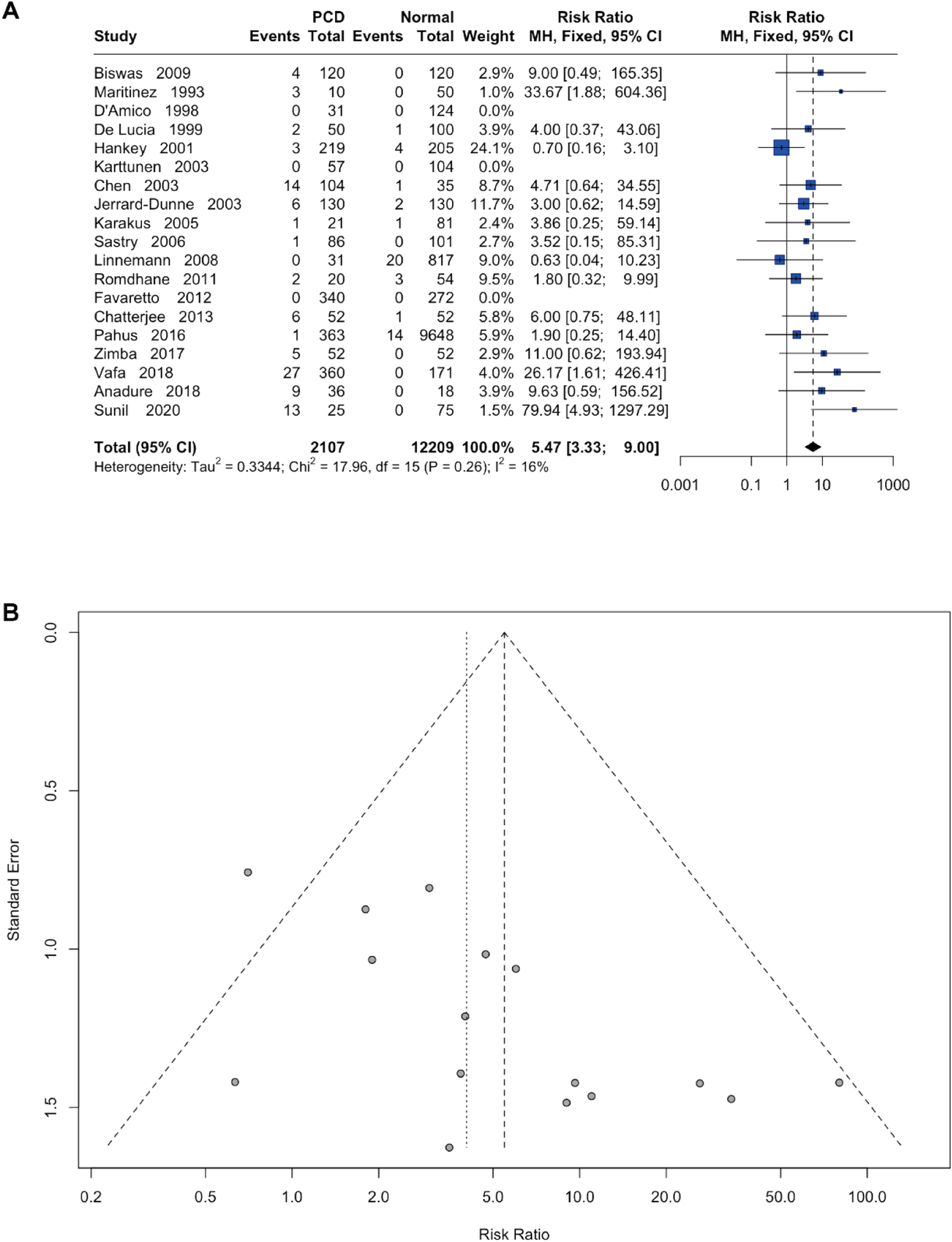
Discussions
This study represents the first application of MR to assess the causal relationships between protein C, protein S, and antithrombin and IS risk. Our MVMR analysis revealed a significant negative causal association between genetically predicted PC levels and IS risk, while no causal associations were identified for protein S or antithrombin. Mediation analysis further demonstrated that the effect of relative PC on IS risk is partially mediated through BMI, though the indirect effect was modest relative to the total effect.
When protein C is deficient or dysfunctional, the body’s capacity to regulate coagulation is compromised, substantially elevating thrombotic risk — particularly under high-risk conditions such as surgery, immobility, pregnancy, and inflammation. Hypercoagulable states associated with impaired PC activity, including protein S deficiency, antiphospholipid syndrome, and protein C deficiency, are well-recognized risk factors for IS and other thrombotic events. Notably, recombinant human activated protein C has shown promise in severe sepsis by improving hemodynamic parameters and reducing oxidative stress, thereby lowering mortality.27,28
In sensitivity analyses, our results were robust and consistent across various MR methods, indicating an unconfounded effect of plasma PC level on the risk of IS. Our findings contradict the results of a directly protective concept of protein C redundancy on cohorts, which provided that increased initial protein C was correlated with worse long-term survival after acute IS.29-31 However, these studies were complicated by limitations, such as small sample sizes and statistical errors. As for the application of recombinant protein C, continuous expression of activated protein C impairs host immune defense during severe Gram-negative sepsis. 32 While, overexpression of the endothelial Protein C Receptor has similar detrimental effect. 33 However, a recent study regarding the clinical trial of AB002, a protein C activator can rapidly dissolve the thrombus in baboons without obvious adverse effects. 34 The phase-2 clinical trial in end-Stage Renal Disease Patients on Chronic Hemodialysis is ongoing. 35
In the initial MR step, univariable analysis unveiled a potentially causal link between relative protein C levels and BMI, indicating that increased protein C levels correlate with decreased BMI. This finding aligns with prior research demonstrating a linear increase in APC resistance with rising BMI levels. This association was found in both men and women, but appeared to be slightly stronger in men (for men, β= - 0.0088, 95% CI -0.0133 to -0.0042; for women, β= -0.0036, 95% CI -0.0068 to -0.0004). They found coagulation factor VIII (FVIII) levels explained part of the relationship between BMI and decreased APC ratio. 9 However, the true relationship between protein C and body mass index (BMI) is complex and not fully understood.
The second MR step provided evidence that genetically determined higher BMI was associated with higher odds of ischemic stroke. Several MR studies have reported evidence for a causal risk factor of BMI on stroke or related thrombosis phenotypes,11,36 which is consistent with the second-step estimate of our mediation analysis. Claes and colleagues found the risk of adult stroke was higher when they had a higher BMI with hazard ratio at 1.21 (95% CI 1.14–1.28). 37 Furthermore, no significant causal relationships were reported for smoking, obesity, SBP and DM on IS risk, as we expected. It would be interesting to differentiate the different role of BMI and obesity, as we only found BMI had a mediating effect between protein C and ischemic stroke, rather than the obesity, which indicated that the BMI is more accurate compared to the vague definition for obesity. Lastly, we validated our results with meta-analysis and showed that those with decreased PC level has a higher risk for IS in both Europe, Asia and American races.
Several limitations warrant consideration. First, while horizontal pleiotropy cannot be entirely excluded, the use of MR-PRESSO and MR-Egger helped detect and mitigate potential biases, supporting the stability of our causal estimates. Second, canalization may have influenced the associations between genetically predicted PC, PS, and AT profiles and IS; however, our MR framework was designed to evaluate both heritable variations and the causal effects of environmental exposures. Third, all GWAS datasets were restricted to European-ancestry individuals to maximize statistical power and minimize population stratification, which limits generalizability to non-European populations where PC levels and genetic architecture may differ. Although our meta-data analysis included patients from diverse regions, replication in diverse-ancestry GWAS is warranted. Finally, while gene–environment interactions may confound environmentally modifiable causal estimates to some degree, the MR approach nonetheless provides a valuable framework for assessing such relationships and informing future randomized controlled trials.
Conclusions
Our MVMR and mediation analyses offer genetic evidence confirming a favorable causal link between PC levels and a decreased risk of ischemic stroke, with BMI partially mediating this effect. The potential significance of our findings in shaping stroke prevention strategies merits validation through well-designed randomized clinical trials with adequate power.
Supplemental Material
Supplemental Material - Association of Protein C, but Not Protein S or Antithrombin With Ischemic Stroke: Bidirectional Two-Sample Mendelian Randomization and Meta-Analysis
Supplemental material for Association of Protein C, but Not Protein S or Antithrombin With Ischemic Stroke: Bidirectional Two-Sample Mendelian Randomization and Meta-Analysis by Liang Shu, Bin He, Cong Yu, Jie Li, Liguo Zhang and Ping Zheng in Clinical and Applied Thrombosis/Hemostasis.
Footnotes
Ethical Considerations
The ethics is approved by the local hospital ethical committee, which is in accordance with the Declaration of Helsinki.
Consent for Publication
All authors agree to the submission.
Author Contributions
Shu Liang and Zheng Ping designed the study. Yu Cong, Li Jie and He Bin performed the Mendelian analysis. Zheng Ping and Shu Liang did the Meta analysis. All author contribute to the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the funding from Shanghai Jinshan District Science and Technology Innovation Fund Project, Shanghai, China (2021-3-54) and KYPT-WJ-2022-14. Externally Funded Project of Shanghai Ninth People’s Hospital (JYHX2021009)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All GWAS summary statistics analyzed in this study are publicly available for download by qualified researchers. The GWASs for relative PC, PS and AT can be obtained through the IEU data portal (https://www.thessgac.org/). The GWASs for ischemic stroke were provided by the IEU data portal (![]() ). All data generated in the current study can be obtained from the Supplementary Information. The data can be obtained from the corresponding author.
). All data generated in the current study can be obtained from the Supplementary Information. The data can be obtained from the corresponding author.
Code Availability
All the analyses used in this study were conducted using PLINK version 1.07 and R packages TwoSampleMR (version 0.5.2), MRPRESSO (version 1.0), RadialMR (version 0.4) and MendelianRandomization (version 0.5.1). The code to reproduce all results reported in the manuscript is available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.