
Abstract
ObjectivesTo explore independent risk factors for preoperative venous thromboembolism (VTE) and to evaluate the predictive value of D-dimer levels and their interactions with key clinical variables.
MethodsIn total, 1,004 elderly patients with hip fractures (≥60 years) admitted between December 2012 and February 2023 were retrospectively analyzed. Routine preoperative lower-extremity venous ultrasonography was performed to screen for deep vein thrombosis (DVT), and computed tomography pulmonary angiography was conducted when pulmonary embolism (PE) was clinically suspected. Multivariable logistic regression identified independent risk factors and interaction analyses assessed modifiers of the D-dimer–VTE association. Model performance was evaluated by ROC curves and AUC.
ResultsThe incidence of preoperative VTE was 21.4% (215/1,004, 95% CI: 19.0%–24.1%), comprising 21.2% (213/1,004, 95% CI: 18.8%–23.9%) for DVT and 0.9% (9/1,004, 95% CI: 0.5%–1.7%) for PE, with seven patients having both DVT and PE. Multivariable logistic regression identified the following independent predictors: cardiovascular disease (OR = 2.787, 95% CI: 1.985–3.950, p < 0.001), injury-to-admission time of >1 day (OR = 2.471, 95% CI: 1.483–4.085, p < 0.001), history of VTE (OR = 3.676, 95% CI: 1.285–10.964, p = 0.016), shortened activated partial thromboplastin time (APTT) (OR = 0.941, 95% CI: 0.909–0.972, p < 0.001), and lower hemoglobin (OR = 0.983, 95% CI: 0.975–0.991, p < 0.001). D-dimer alone had poor discrimination for VTE (AUC = 0.533). Interaction analysis showed that sex (p for interaction = 0.018), injury-to-admission time (p for interaction = 0.002), and bedridden time (p for interaction < 0.001) significantly modified the association between D-dimer and preoperative VTE risk. The baseline multivariable model yielded an AUC of 0.728 for predicting VTE, which improved to 0.742 after including D-dimer interaction terms (ΔAUC = 0.013, 95% CI: 0.000–0.027, p < 0.05).
ConclusionsCardiovascular disease, injury-to-admission time of >1 day, a history of DVT or PE, shortened APTT, and lower hemoglobin were identified as independent risk factors for preoperative VTE in elderly patients with hip fractures. Although D-dimer alone demonstrated limited discriminatory ability, incorporating its interactions with sex, injury-to-admission time, and bedridden time improved predictive performance.
Introduction
Hip fractures are common and serious injuries in the elderly population, and their incidence increases markedly with age, particularly among women. 1 Elderly patients with hip fractures are prone to various perioperative complications, including cognitive impairment, cardiopulmonary dysfunction, venous thromboembolism (VTE), gastrointestinal bleeding, urinary tract infection, anemia, and malnutrition.2,3 Among these, VTE is one of the most frequent and life-threatening complications, consisting primarily of deep vein thrombosis (DVT) and pulmonary embolism (PE).4,5 Shin et al reported a preoperative VTE prevalence of 11.1% among patients with hip fractures whose surgery was delayed. 6 In another study, the preoperative prevalence of VTE was 12.6% among patients with hip fractures and elevated D-dimer levels. 7 The development of VTE not only complicates perioperative management but can also lead to fatal PE due to thrombus detachment. 8 Therefore, early identification of preoperative VTE in elderly patients with hip fractures is crucial for timely intervention and for reducing perioperative mortality and complications. 9
Identifying risk factors for VTE is of critical importance. However, existing studies on the occurrence of preoperative VTE in patients with hip fracture are limited, and effective screening and early detection remain major clinical challenges. 10 Venous stasis, endothelial injury, and hypercoagulability—collectively known as Virchow’s triad—provide the classical framework for understanding VTE pathogenesis, 11 whereby clinical conditions that trigger one or more of these mechanisms may promote its development. 12 Prolonged preoperative waiting time has been widely recognized as a major risk factor for preoperative VTE.13,14 In addition, factors such as female sex, advanced age, subtrochanteric fracture type, coronary heart disease, hepatic or renal dysfunction, pulmonary disease, low hemoglobin level, and elevated fibrinogen have been reported as contributors to preoperative DVT in patients with hip fracture. 15 Nevertheless, the role of D-dimer—an important biomarker reflecting both thrombotic and fibrinolytic activity—remains insufficiently characterized in the preoperative phase of hip fracture.
D-dimer, a soluble fibrin degradation product, exhibits elevated concentrations in the presence of active thrombosis and is therefore closely associated with VTE development. 16 Because of its high sensitivity, D-dimer has been widely used as a screening tool for the initial detection and exclusion of VTE. 17 It has also been shown to predict postoperative VTE events in various surgical populations, including orthopedic procedures.18-21 Our previous studies have confirmed the clinical value of D-dimer in predicting preoperative DVT among patients with knee osteoarthritis.22,23 However, patients with hip fractures often experience substantial tissue injury, systemic inflammation, and surgical trauma—conditions that can elevate D-dimer levels even in the absence of VTE, thereby markedly reducing its specificity. 24 Furthermore, D-dimer concentrations can be influenced by a range of factors, including sex, age, malignancy, infection, trauma, hepatic or renal dysfunction, and anticoagulant therapy. 25 Our previous research further showed that the injury-to-admission time also affects D-dimer levels. 26 As a result, the predictive performance of D-dimer for preoperative VTE in patients with hip fracture remains uncertain and warrants further investigation.
This study aimed to identify independent risk factors for preoperative VTE in elderly patients with hip fractures and to evaluate the predictive performance of D-dimer, including its interactions with key clinical variables, thereby providing evidence to support preoperative VTE risk assessment and individualized preventive strategies in this population.
Methods
Study Population
In total, 1,664 consecutive elderly patients (≥60 years) with hip fractures admitted to the Department of Orthopedics at Peking Union Medical College Hospital from December 2012 to February 2023 were retrospectively reviewed. The inclusion criteria were an age of ≥60 years; an admission diagnosis of hip fracture, including femoral neck or intertrochanteric fractures; planned surgical treatment with a hospital stay exceeding 48 hours; injury-to-admission interval of ≤30 days; and receipt of anticoagulant prophylaxis during hospitalization. The exclusion criteria were a second hip fracture, periprosthetic femoral or periprosthetic hip fractures, subtrochanteric fractures, absence of preoperative lower-extremity venous ultrasonography, and incomplete clinical records or laboratory data. This study complied with the Declaration of Helsinki (1964) and received approval from the Ethics Committee of Peking Union Medical College Hospital (approval No. K3624). Informed consent was waived because the study was retrospective and the data were anonymized. Figure 1 illustrates the patient selection process, resulting in a final cohort of 1,004 patients included in the analysis. Flow chart of study inclusion and exclusion criteria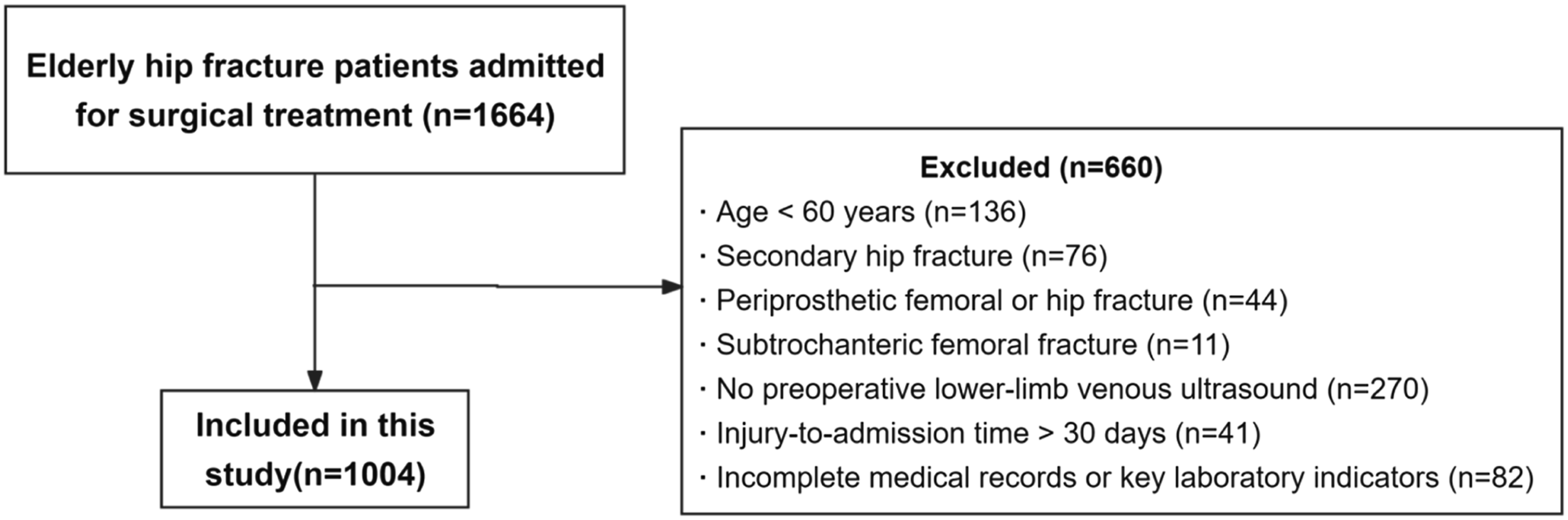
Data Collection
Clinical data were retrieved from the hospital information system. Demographic variables included age, sex, body mass index (BMI), side of injury, fracture type, smoking and drinking status, activities of daily living (ADL) score, length of hospital stay, injury-to-admission interval, and bedridden time (defined as the duration of preoperative bed rest). Comorbidities included hypertension, diabetes mellitus, dyslipidemia, a history of DVT or PE, cardiovascular disease, respiratory disease, endocrine or metabolic disorders, gastrointestinal disease, neurological disease, musculoskeletal disease, hematologic disease, renal or urinary disease, and oncologic disease. These comorbidities were identified according to predefined International Classification of Diseases, 11th Revision (ICD-11) terms extracted from all recorded diagnoses in the hospital information system, including both current and prior documented diagnoses (Table 1S, Supplemental Appendix). Oncologic disease was therefore defined as any recorded diagnosis of cancer rather than active malignancy. Pre-admission medication data included the use of antiplatelet agents, lipid-lowering agents, and anticoagulant therapy.
Laboratory parameters measured preoperatively included D-dimer, fibrinogen, international normalized ratio, activated partial thromboplastin time (APTT), platelet count, white blood cell count, neutrophil count, and hemoglobin level. These tests were routinely performed as part of the institutional perioperative assessment, generally within the first 3 days after admission. For each laboratory parameter, the earliest available preoperative value was used for analysis according to the following priority: day 1 values were selected first, followed by day 2 values when day 1 values were unavailable; the earliest available value from day 3 or later was used only when no results were available from the first 2 days. This approach was applied to improve the consistency of laboratory data comparisons across patients. According to institutional practice, thromboprophylaxis was initiated as early as possible after admission unless contraindicated.
VTE Diagnosis
For elderly patients with hip fractures, routine preoperative venous ultrasonography of the lower extremities was performed within 3 days of hospital admission to detect the presence of DVT. The examination identified three types of thrombosis: proximal DVT, mainly involving the popliteal and femoral veins (i.e., the popliteal vein, common femoral vein, and superficial femoral vein); distal DVT, involving the deep veins of the calf (i.e., the posterior tibial vein, peroneal vein, and intramuscular veins of the calf); and mixed DVT, involving both proximal and distal segments.
Regardless of the preoperative DVT status, if a patient presented with acute clinical symptoms—such as tachycardia or decreased oxygen saturation—PE was suspected, and computed tomography pulmonary angiography was promptly performed to confirm or exclude symptomatic PE.
Statistical Analysis
The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Variables with a normal distribution were presented as mean ± standard deviation (SD) and compared using the Student’s t-test, whereas non-normally distributed variables were expressed as median (interquartile range) and analyzed with the Mann–Whitney U test. Categorical variables were summarized as frequencies and percentages, and compared using the chi-square test or Fisher’s exact test, as appropriate. Incidence was expressed as a percentage, and 95% confidence intervals (CIs) were calculated using the Wilson score method.
Receiver operating characteristic (ROC) curves were generated to evaluate the diagnostic performance of D-dimer for preoperative VTE, and the area under the curve (AUC) was calculated to quantify its discriminative ability. Based on the optimal cutoff value, patients were categorized into low and high D-dimer groups. To mitigate baseline imbalances between these groups, propensity score matching (PSM) was performed. Propensity scores were derived from a logistic regression model, in which high D-dimer status was specified as the dependent variable and all clinical variables were entered as covariates. One-to-one nearest-neighbor matching was implemented using a caliper width equivalent to 0.2 SD of the logit of the propensity score, without replacement. Covariate balance before and after matching was quantified using standardized mean differences (SMDs), with SMD < 0.1 denoting acceptable balance. An SMD plot was generated to visualize covariate balance.
After identifying potential confounders through the PSM procedure, interaction effects between D-dimer and other clinical risk factors were examined in the overall cohort. Variables that showed the greatest baseline differences between the high and low D-dimer groups in the PSM analysis, along with commonly reported VTE risk factors (e.g., sex, injury-to-admission time >1 day, bedridden time >72 hours, anticoagulation, antiplatelet therapy, and lipid-lowering therapy 27 ), were included in the interaction analysis. A multivariable logistic regression model was fitted with preoperative VTE as the dependent variable, incorporating separate interaction terms between D-dimer and each selected variable to test for statistical significance (p for interaction).
To evaluate the combined effects of D-dimer and other variables on the risk of preoperative VTE, multivariable logistic regression models were developed using the enter method, in which all independent variables were entered simultaneously. Model A included variables with p < 0.05 in the univariate analysis—cardiovascular disease, hematologic disease, injury-to-admission time, bedridden time, history of DVT/PE, fibrinogen, APTT, and hemoglobin. Model B was based on Model A, with D-dimer additionally included. Model C was based on Model B, with variables showing significant interactions with D-dimer (i.e., sex, bedridden time, and injury-to-admission time) further incorporated.
The incremental predictive performance of Models B and C relative to Model A was then assessed. The DeLong test was used to compare differences in the AUC between models, while the integrated discrimination improvement (IDI) and continuous net reclassification improvement (NRI) were calculated to quantify improvements in discrimination and reclassification.
All statistical analyses were performed using R software (version 4.4.2). A two-sided p value of <0.05 was considered statistically significant.
Results
Baseline Characteristics
Comparison of Demographic and Clinical Characteristics Between Patients With and Without Preoperative VTE in Elderly Patients With Hip Fractures (N = 1,004)
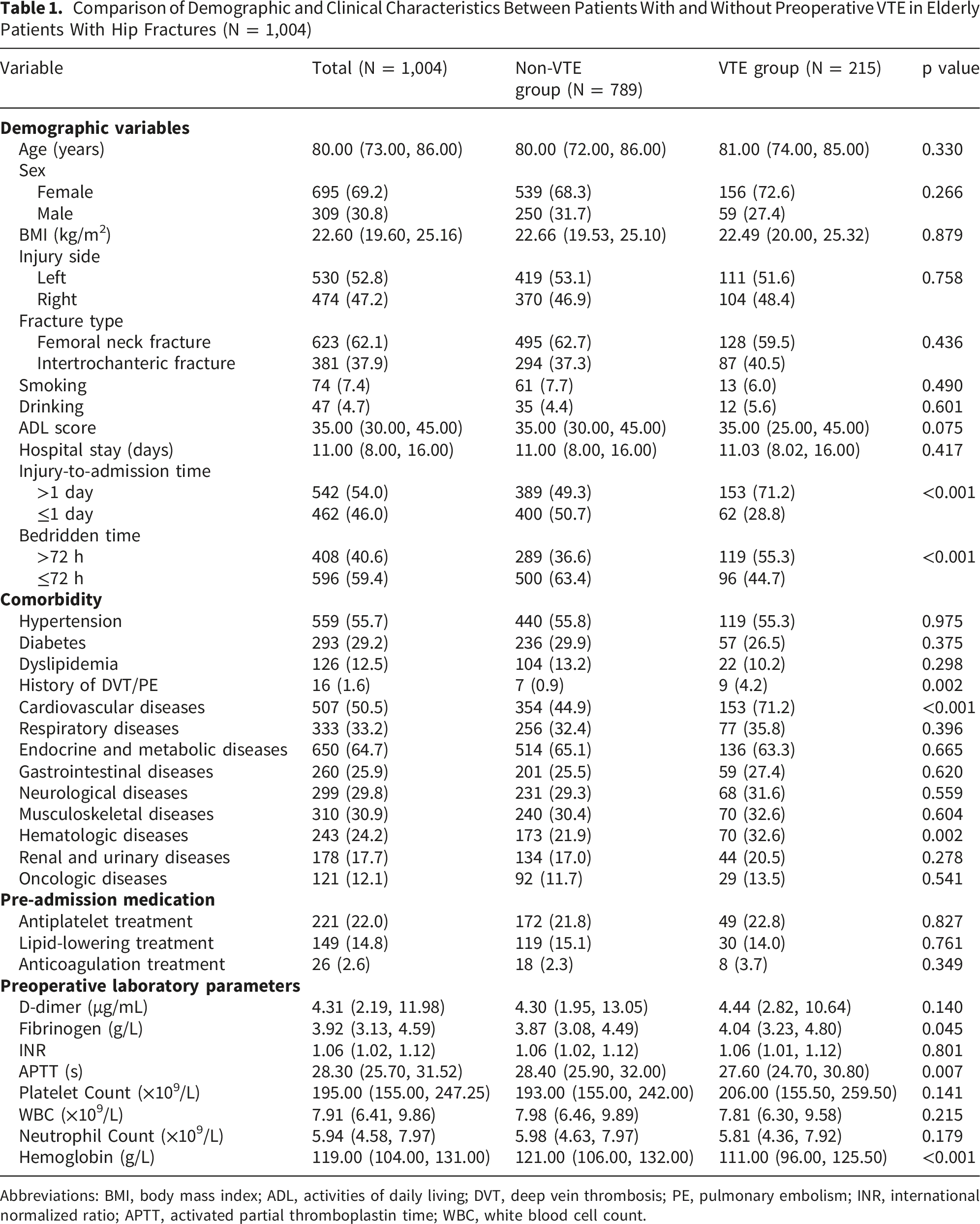
Abbreviations: BMI, body mass index; ADL, activities of daily living; DVT, deep vein thrombosis; PE, pulmonary embolism; INR, international normalized ratio; APTT, activated partial thromboplastin time; WBC, white blood cell count.
Univariate Analysis of Risk Factors Associated With Preoperative VTE
Univariate analysis revealed that compared with the non-VTE group, patients in the VTE group were more likely to have cardiovascular disease (71.2% vs. 44.9%; p < 0.001) and hematologic disease (32.6% vs. 21.9%; p = 0.002). They also had a longer injury-to-admission interval (>1 day: 71.2% vs. 49.3%; p < 0.001) and a longer bedridden time (>72 h: 55.3% vs. 36.6%; p < 0.001). In addition, patients with VTE had a higher prevalence of prior DVT/PE (4.2% vs. 0.9%; p = 0.002), higher preoperative fibrinogen levels (4.04 [3.23–4.80] vs. 3.87 [3.08–4.49] g/L; p = 0.045), lower preoperative APTT (27.60 [24.70–30.80] vs. 28.40 [25.90–32.00] s; p = 0.007), and lower preoperative hemoglobin levels (111.00 [96.00–125.50] vs. 121.00 [106.00–132.00] g/L; p < 0.001) (Table 1).
Analysis of D-Dimer Levels and PSM Results
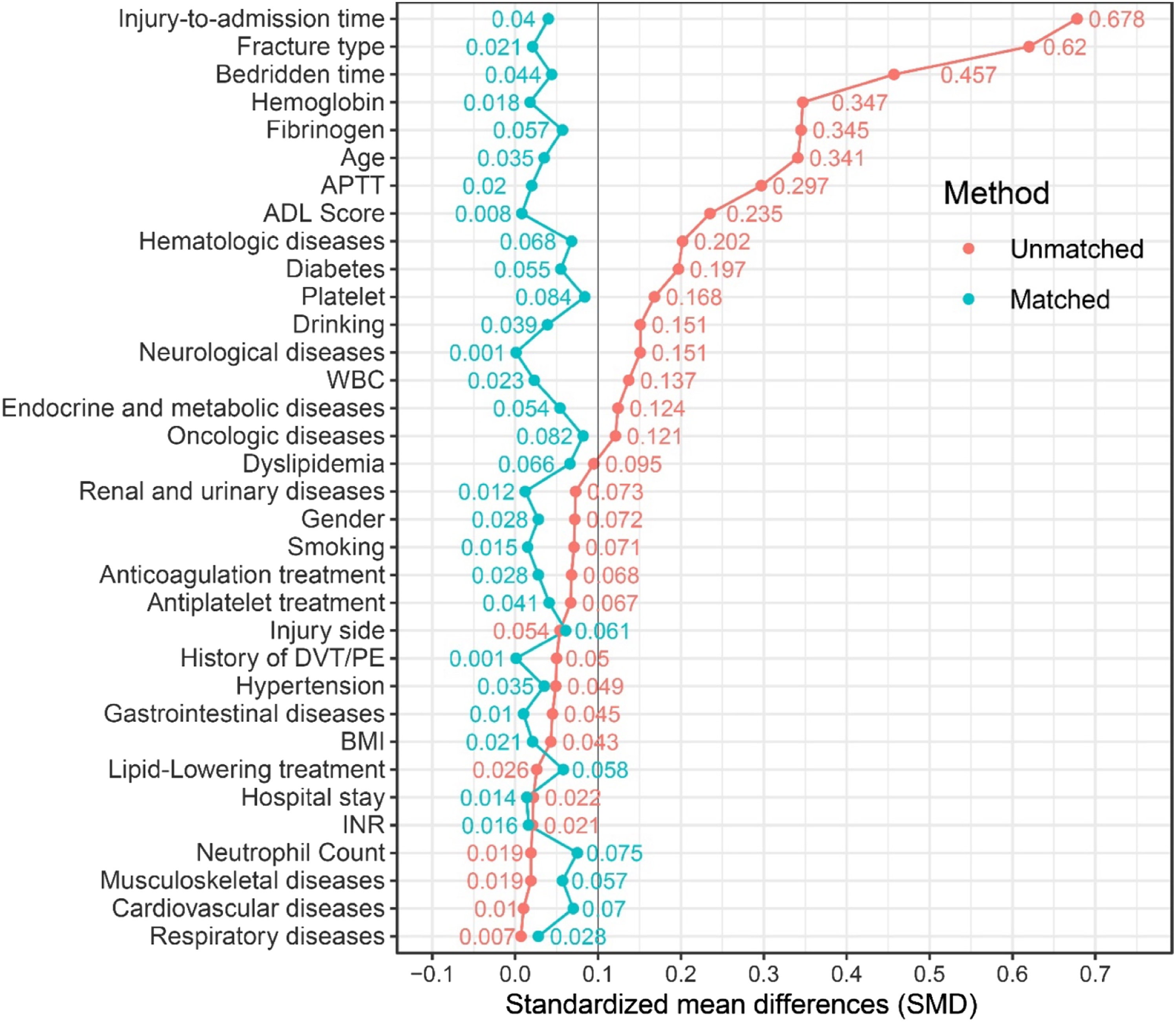
D-dimer levels did not differ significantly between the VTE and non-VTE groups (4.44 [2.82–10.64] vs. 4.30 [1.95–13.05] μg/mL; p = 0.140) (Table 1). ROC curve analysis of D-dimer for predicting VTE yielded an AUC of 0.533 (95% CI: 0.493–0.572), with an optimal cutoff value of 2.275 (Figure 2). Based on this cutoff value, patients were classified into “high D-dimer” and “low D-dimer” groups for PSM analysis. After PSM, most covariates achieved an SMD of <0.1, indicating good covariate balance. Before matching, injury-to-admission time, fracture type, and bedridden time exhibited the highest SMD values, reflecting the most pronounced baseline differences between the two groups (Figure 3). ROC curve of D-dimer for predicting preoperative VTE in elderly patients with hip fractures Covariate balance before and after propensity score matching assessed using standardized mean differences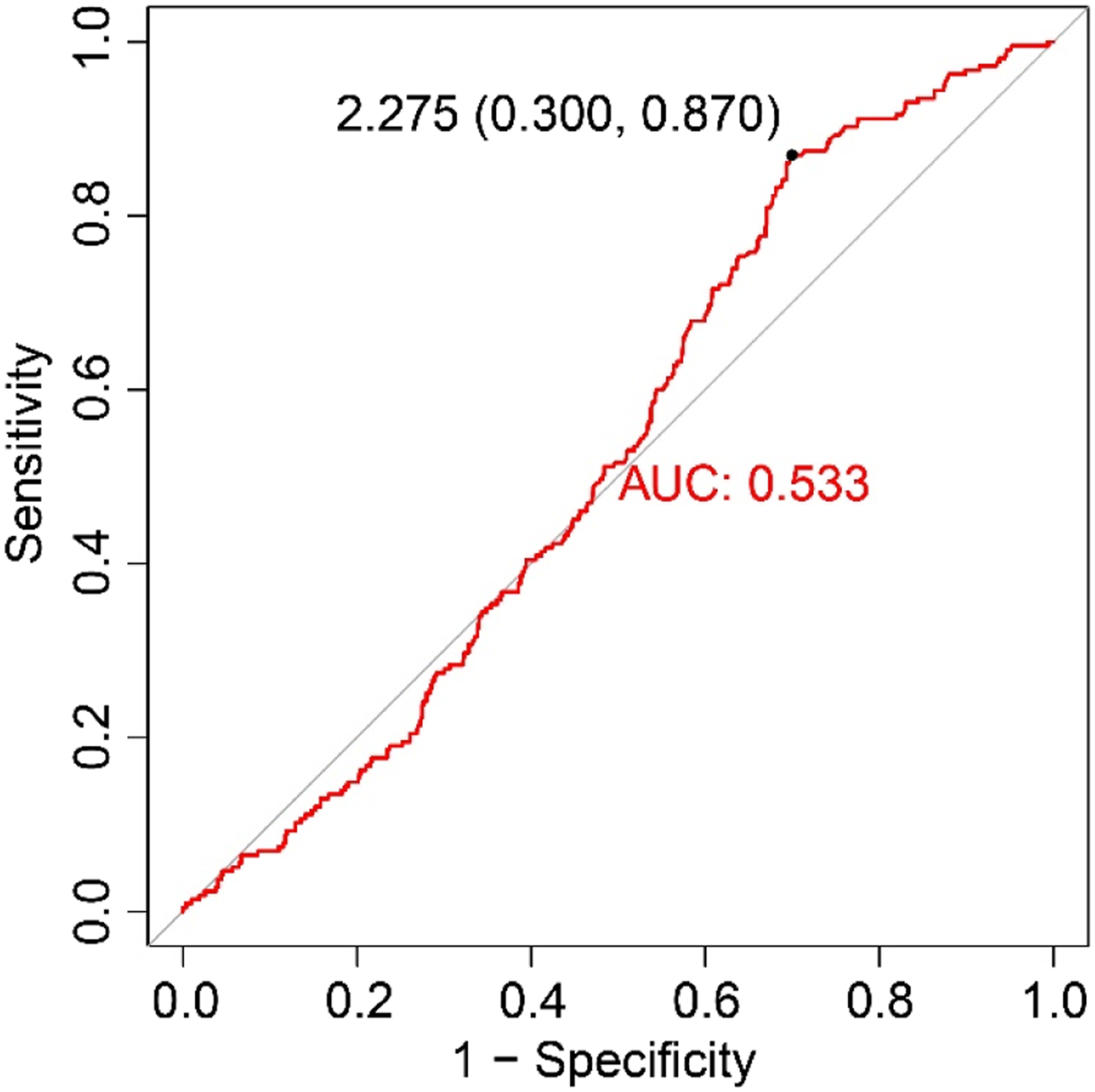
Interaction Analysis of D-Dimer Levels and Preoperative VTE Risk
Interaction Effects Between D-Dimer and Clinical Variables on Preoperative VTE Risk in Elderly Patients With Hip Fractures
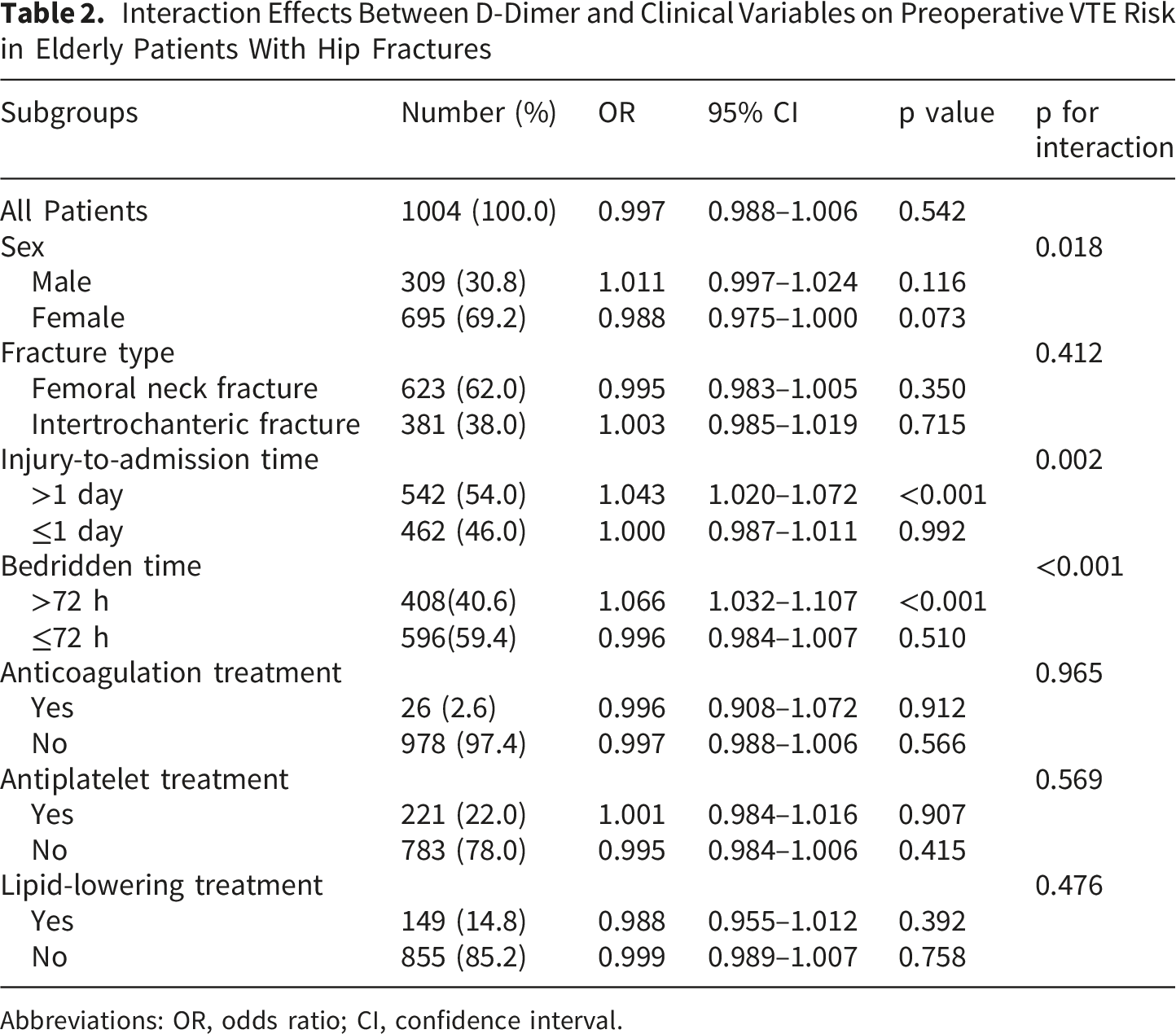
Abbreviations: OR, odds ratio; CI, confidence interval.
Multivariate Logistic Regression Analysis of Risk Factors for Preoperative VTE
Multivariate Logistic Regression of Risk Factors for Preoperative VTE in Elderly Patients With Hip Fractures
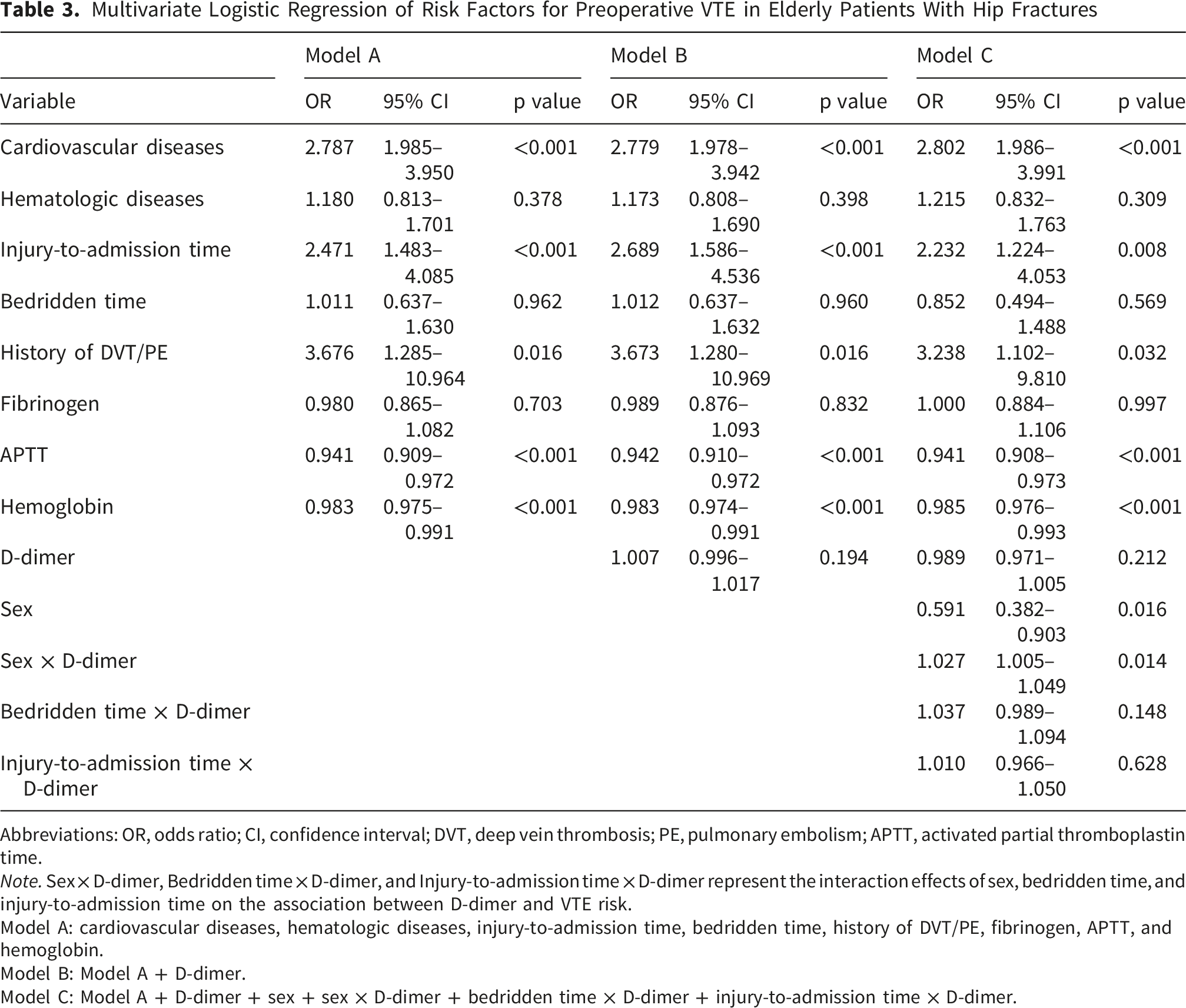
Abbreviations: OR, odds ratio; CI, confidence interval; DVT, deep vein thrombosis; PE, pulmonary embolism; APTT, activated partial thromboplastin time.
Note. Sex × D-dimer, Bedridden time × D-dimer, and Injury-to-admission time × D-dimer represent the interaction effects of sex, bedridden time, and injury-to-admission time on the association between D-dimer and VTE risk.
Model A: cardiovascular diseases, hematologic diseases, injury-to-admission time, bedridden time, history of DVT/PE, fibrinogen, APTT, and hemoglobin.
Model B: Model A + D-dimer.
Model C: Model A + D-dimer + sex + sex × D-dimer + bedridden time × D-dimer + injury-to-admission time × D-dimer.
Comparison of Predictive Performance Among Models A, B, and C
The ROC curves comparing the predictive performance of Models A, B, and C for preoperative VTE in elderly patients with hip fractures are shown in Figure 4. The AUCs for Models A, B, and C were 0.728 (95% CI: 0.690–0.766), 0.729 (95% CI: 0.691–0.767), and 0.742 (95% CI: 0.704–0.779), respectively. ROC curves of Models A, B, and C for preoperative VTE prediction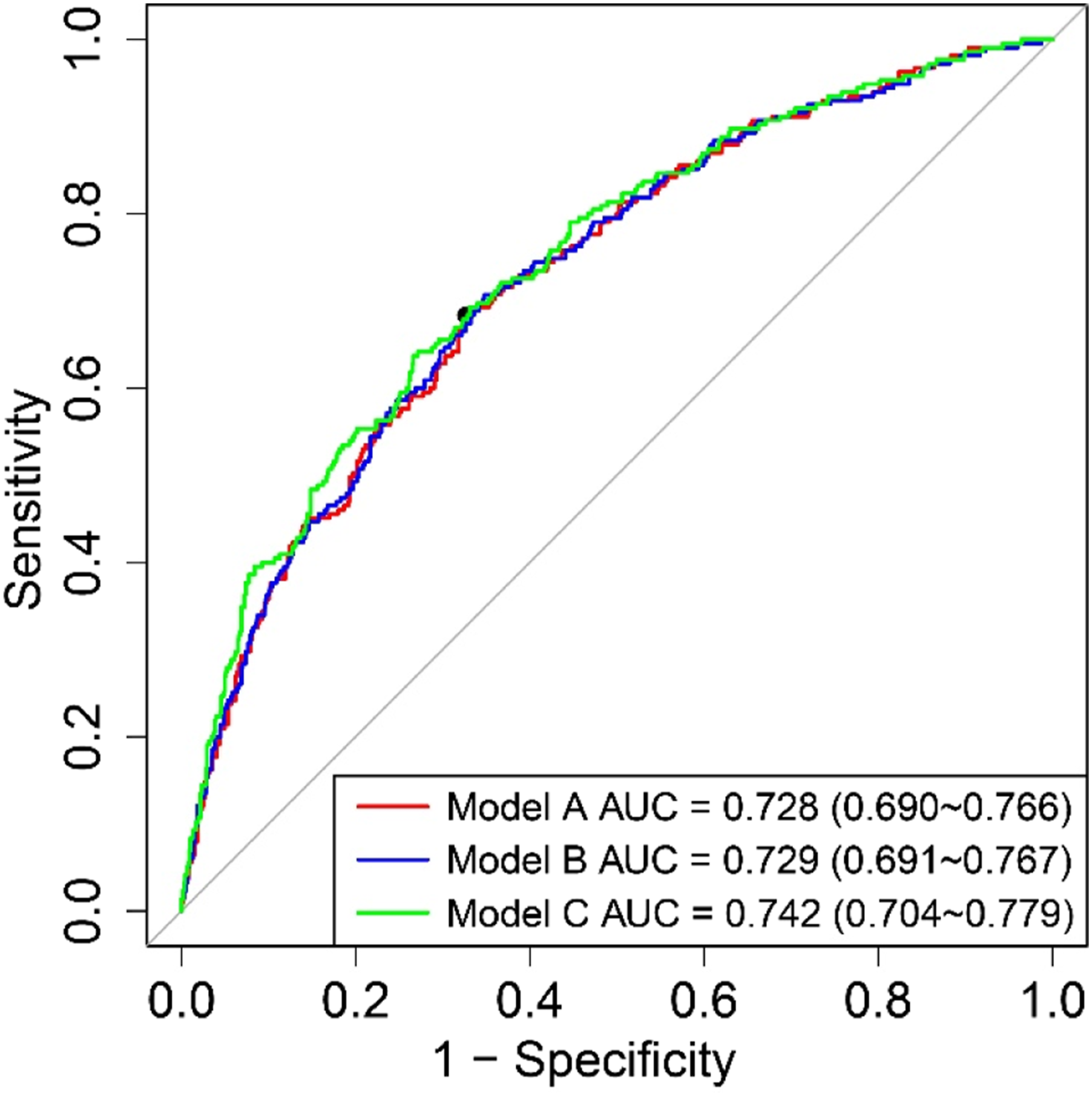
Comparison of Predictive Performance Among Models A, B, and C for Preoperative VTE
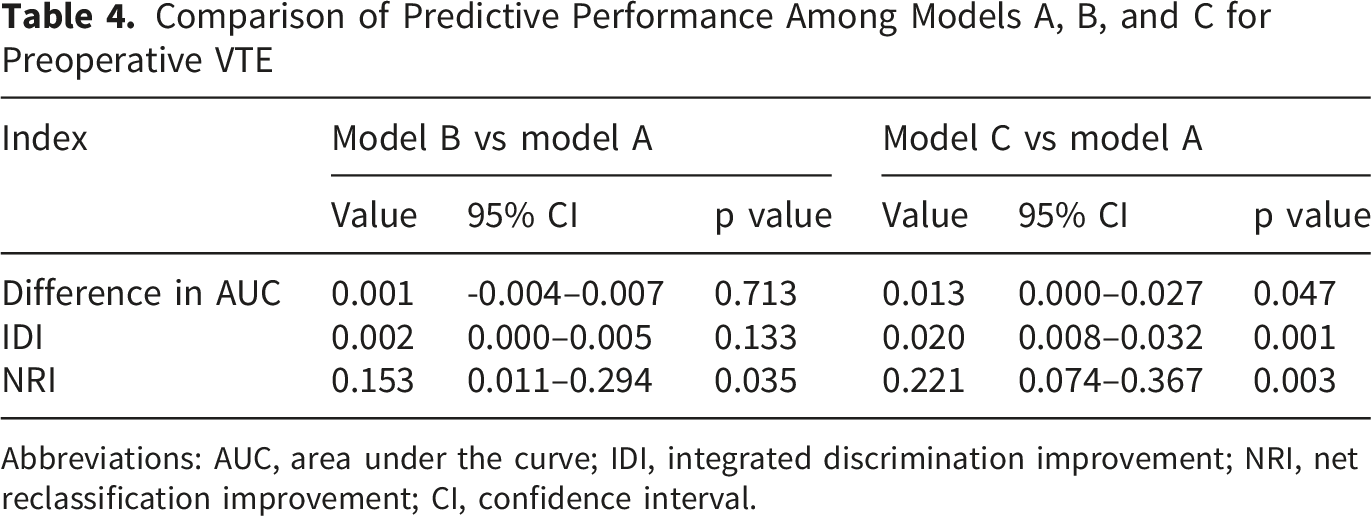
Abbreviations: AUC, area under the curve; IDI, integrated discrimination improvement; NRI, net reclassification improvement; CI, confidence interval.
Discussion
Elderly patients with hip fractures often experience reduced mobility and multiple age-related comorbidities, both of which substantially increase the risk of developing preoperative VTE. 10 Because preoperative VTE can lead to severe adverse outcomes, its early identification in this vulnerable population is particularly important. In this study, cardiovascular disease, injury-to-admission time greater than 1 day, a history of DVT or PE, shortened APTT, and decreased hemoglobin levels were identified as independent risk factors for preoperative VTE in elderly patients with hip fractures. However, D-dimer alone demonstrated limited predictive value, likely because of the influence of various confounding factors. To further clarify this relationship, PSM and interaction analyses were performed, revealing significant interactions between D-dimer levels and several clinical factors, including injury-to-admission time, bedridden time, and sex. Incorporating these interaction terms into the multivariate logistic regression model modestly improved its predictive performance compared with the inclusion of D-dimer alone.
This study identified cardiovascular disease, an injury-to-admission time greater than 1 day, and a history of DVT or PE as independent risk factors for preoperative VTE in patients with hip fractures. Among these, three factors were particularly prominent. First, cardiovascular disease encompasses a broad spectrum of disorders affecting cardiac and vascular structure and function. A common pathophysiological feature among these conditions is hemodynamic disturbance, which corresponds to venous stasis—one component of Virchow’s triad. 11 Moreover, both atherosclerosis and myocardial ischemia can activate platelets and coagulation factors, thereby inducing a hypercoagulable state. 28 Chronic arteriosclerosis and inflammatory endothelial injury further impair the release of endogenous anticoagulants, including nitric oxide and prostacyclin, promoting thrombogenesis. 29 Previous studies have likewise demonstrated that coronary artery disease and peripheral vascular disease are associated with an increased risk of developing preoperative DVT.15,30
Second, delayed admission after fracture markedly increases the risk of developing preoperative VTE. This may be partly explained by the progressive inflammatory response following fracture, during which inflammatory cytokines activate the coagulation cascade and promote a hypercoagulable state. 31 In addition, prolonged bed rest reduces venous return, leading to venous stasis, while delayed hospital admission postpones the initiation of pharmacologic or mechanical prophylaxis, further compounding thrombotic risk. Consistent with our findings, previous studies have reported that a surgical delay exceeding 48 hours significantly increases postoperative VTE risk 32 and that an injury-to-admission time of ≥21 hours independently predicts preoperative DVT in elderly patients with hip fractures. 33
Finally, a history of DVT or PE was also identified as a significant risk factor for preoperative VTE. Prior thrombotic events often leave residual thrombi or fibrotic changes within the venous system, leading to venous stenosis and valvular incompetence, which in turn cause hemodynamic abnormalities and increase the risk of thrombus propagation.34,35 In addition, such patients frequently have inherited or acquired hypercoagulable states; even after clinical resolution, their coagulation system may remain hyperactivated, substantially heightening the risk of recurrence.36,37 Consistent with our findings, earlier studies have shown that a history of VTE is an independent predictor of new-onset VTE following hip surgery.11,38 Taken together, these results highlight the importance of early identification and targeted thromboprophylaxis in patients with hip fracture and concurrent cardiovascular disease, delayed admission, or a history of VTE.
In addition to the aforementioned clinical characteristics, this study identified two laboratory indicators significantly associated with an increased risk of VTE—shortened APTT and decreased hemoglobin levels. APTT serves as a key marker reflecting the activity of the intrinsic coagulation pathway. A shortened APTT typically indicates enhanced coagulation factor activity or the presence of circulating procoagulant substances, suggesting a hypercoagulable and imbalanced state. 39 Previous studies have demonstrated that a shortened APTT is independently associated with subsequent VTE events, 40 underscoring its potential value in preoperative VTE risk assessment among patients with hip fractures. Similarly, decreased hemoglobin levels reflect reduced oxygen-carrying capacity, rendering tissues more susceptible to hypoxia. Hypoxia stimulates monocytes, macrophages, and vascular smooth muscle cells to express tissue factor, thereby activating the coagulation cascade. It also upregulates plasminogen activator inhibitor-1 expression and suppresses fibrinolysis, contributing to a hypercoagulable state. 41 Furthermore, hypoxia-inducible factor-2α activates the vascular endothelial growth factor signaling pathway, promoting megakaryocyte differentiation and platelet production, which further increase thrombotic risk. 42 In addition, decreased hemoglobin may reflect underlying pathological conditions associated with VTE, such as malnutrition, chronic inflammation, chemotherapy, or endothelial dysfunction. 43 Consistent with our findings, previous orthopedic trauma studies have shown that preoperative anemia significantly increases the risk of perioperative DVT in patients with hip fracture. 44 Therefore, these two routinely measured laboratory parameters have independent predictive value for preoperative VTE, and incorporating them into preoperative risk assessment systems may facilitate early identification of high-risk patients.
This study further identified three clinical factors that significantly interacted with D-dimer— sex, injury-to-admission time, and bedridden time. Among the interaction terms examined, the sex × D-dimer interaction was statistically significant, suggesting that sex may modify the association between D-dimer levels and preoperative VTE risk. However, in sex-stratified analyses, the association between D-dimer and preoperative VTE did not reach statistical significance in either male or female patients; therefore, this finding should be interpreted cautiously. Previous studies have reported sex-related differences in D-dimer levels, VTE risk profiles, and the clinical interpretation of D-dimer testing, including proposed sex-specific D-dimer cutoff values.45,46 However, the biological basis underlying the sex × D-dimer interaction observed in our study remains unclear. Further studies are needed to validate this finding and clarify its potential clinical implications. The other two interacting factors—injury-to-admission time and bedridden time—also markedly amplified the predictive effect of D-dimer on VTE risk. As discussed earlier, delayed admission and prolonged immobility are closely linked to increased thrombotic potential, which may explain the stronger association between elevated D-dimer levels and VTE observed under these conditions. In such patients, D-dimer levels are less likely to be confounded by chronic comorbidities or nonspecific factors common in the elderly 47 and may therefore more accurately reflect the ongoing thrombotic process. In clinical practice, several studies have proposed adjusting D-dimer thresholds based on specific clinical contexts—such as age, sex, and renal function—to improve diagnostic accuracy in defined patient populations.47-49 Focusing on elderly patients with hip fractures, the present study further confirmed the predictive value of D-dimer for preoperative VTE risk and provided additional evidence supporting the refinement of risk-adjustment strategies in this population.
Building upon these findings regarding D-dimer interactions, we further evaluated the predictive performance of multiple logistic regression models. Among the models tested, Model C demonstrated the highest predictive performance for preoperative VTE in patients with hip fractures (AUC = 0.742). However, although the increase in AUC from 0.728 to 0.742 was statistically significant, its magnitude was modest and should not be interpreted as definitive evidence of clinically meaningful improvement. This modest gain may reflect the incorporation of D-dimer together with the clinical variables that exhibited significant interactions with it, suggesting that the predictive value of D-dimer may vary across different clinical contexts. By contrast, adding D-dimer alone (Model B) produced no meaningful improvement in model performance, underscoring that a single biomarker has limited predictive utility in complex clinical settings and should be interpreted in conjunction with relevant clinical characteristics. Unlike previous studies that included D-dimer directly as an independent predictor,50-52 our findings suggest that D-dimer-related interaction effects may contribute additional information for risk assessment. Nevertheless, given the limited incremental gain in AUC and the additional complexity introduced by interaction terms, the interaction-based model should be regarded as exploratory rather than ready for routine clinical implementation. Its clinical utility should be confirmed in independent cohorts before being used to guide clinical decision-making.
Several limitations of this study should be acknowledged. First, the single-center retrospective design and relatively limited sample size may have introduced selection bias. As a tertiary referral center, our institution manages a relatively high proportion of elderly patients with complex comorbidities, which may have contributed to the relatively high prevalence of preoperative VTE observed in this study and may limit the generalizability of our findings. Moreover, because most VTE events consisted of DVT, particularly distal DVT, whereas proximal DVT and symptomatic PE were relatively uncommon, the overall VTE incidence should be interpreted in the context of thrombus location and clinical significance. Second, the predictive models were developed and evaluated in the same cohort and lacked both internal and external validation. Consequently, their performance may be optimistic, particularly for the more complex interaction-based model, which is more susceptible to overfitting. The applicability of these models to other patient populations and clinical settings therefore requires further validation. Third, the timing of blood sampling for D-dimer and other coagulation or hematological tests was not standardized. Because D-dimer levels may change dynamically after trauma, variation in sampling time may have influenced the measured concentrations. In addition, patients routinely received anticoagulant therapy as early as possible after admission, and some blood samples may have been obtained after post-admission anticoagulation had been initiated. Although our interaction analysis showed no significant interaction between pre-admission anticoagulant therapy and the association between D-dimer and preoperative VTE, the potential influence of post-admission anticoagulation timing on D-dimer levels was not specifically evaluated. Future studies with standardized sampling time points and detailed documentation of anticoagulation timing are needed to further clarify this issue. Finally, oncologic disease was identified from recorded ICD-11 diagnosis codes and included both current and prior documented diagnoses; therefore, active malignancy could not be distinguished from a history of cancer. This may have introduced exposure misclassification and residual confounding when evaluating the association between oncologic disease and preoperative VTE.
Despite these limitations, this study provides additional insight into the interpretation of D-dimer in elderly patients with hip fractures by highlighting the potential influence of clinical context and interaction effects on its predictive performance for preoperative VTE. Rather than considering D-dimer as an isolated biomarker, our findings suggest that its predictive utility may vary across different patient subgroups and clinical conditions. Future large-scale multicenter prospective studies incorporating dynamic D-dimer assessment may help further refine individualized preoperative VTE risk stratification in elderly patients with hip fractures.
Conclusions
Cardiovascular disease, an injury-to-admission time exceeding 1 day, a prior history of DVT or PE, shortened APTT, and reduced hemoglobin levels were identified as independent risk factors for preoperative VTE in elderly patients with hip fractures. Although the predictive value of D-dimer alone was limited, incorporating D-dimer and its significant interactions with sex, injury-to-admission time, and bedridden time modestly improved model discrimination. These findings underscore the potential value of integrating D-dimer with key clinical variables to enhance early risk assessment and guide prophylactic strategies in this high-risk population. In practical terms, the combined model could be incorporated into routine admission assessment to automatically flag patients at high risk for VTE. This would enable timely Doppler ultrasonography, individualized prophylaxis, or expedited surgical planning, thereby supporting more proactive perioperative management and potentially improving outcomes.
Supplemental Material
Supplemental material - Preoperative Venous Thromboembolism in Elderly Patients With Hip Fractures: Independent Risk Factors and Interactions Between D-Dimer and Clinical Variables
Supplemental material for Preoperative Venous Thromboembolism in Elderly Patients With Hip Fractures: Independent Risk Factors and Interactions Between D-Dimer and Clinical Variables by Chengyi Zhong, Weinan Liu, Yaping Chen, Baozhong Zhang, Jia Zhang, Peng Gao, Yan Zhang, Bingdu Tong, Xiaopeng Huo and Yi-Feng Guo by Clinical and Applied Thrombosis/Hemostasis.
Footnotes
Ethical Considerations
The study was approved by the Institutional Review Board of the Peking Union Medical College Hospital (K3624).
Consent to Participate
The ethics committee waived the requirement for informed consent because this study was retrospective and the data are anonymous.
Author Contributions
Yi-Feng Guo is the lead contact. Yi-Feng Guo: Conceptualization, Methodology, Formal analysis, Funding acquisition, Writing—original draft, Writing—review & editing, Project administration. Chengyi Zhong: Methodology, Data curation, Formal analysis, Writing—original draft, Writing—review & editing. Weinan Liu, Yaping Chen: Data curation, Formal analysis, Writing—original draft. Baozhong Zhang, Jia Zhang, Peng Gao: Investigation, Resources. Yan Zhang: Visualization, Supervision. Bingdu Tong, Xiaopeng Huo: Writing—review & editing, Project administration. All authors read and approved the final manuscript to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (72204268), the National High Level Hospital Clinical Research Funding (2025-PUMCH-A-062), the Fundamental Research Funds for the Central Universities, Peking Union Medical College (3332022002), and the Nursing Research Fund of Peking Union Medical College Hospital (XHHLKY202502).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Because of ethical and privacy restrictions regarding patient data, the datasets from this study are not available publicly. If needed, you can request the data from the corresponding author with a reasonable inquiry.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.