
Abstract
Purpose
To evaluate the efficacy and safety of triple antithrombotic therapy (TT) versus dual antiplatelet therapy (DAPT) for prevention of left ventricular thrombus (LVT) following anterior myocardial infarction.
Methods
We conducted a systematic review and meta-analysis of randomized and observational studies comparing TT (DAPT plus anticoagulation) versus DAPT alone. The primary outcome was LVT formation. Secondary outcomes included all-cause mortality, stroke, systemic embolism, composite thromboembolism, bleeding, and net adverse clinical events (NACE). Pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using random-effects models. The protocol was registered in PROSPERO (CRD420261343867).
Results
Seven studies (2 randomized, 5 observational), including 2,273 patients (949 TT, 1,324 DAPT), were analyzed. TT was not associated with a reduction in LVT (OR 0.56, 95% CI 0.21–1.49; p=0.25; I2=59%). There was no significant difference in all-cause mortality (OR 0.75, 95% CI 0.27–2.06; p=0.58), ischemic cerebrovascular accidents (OR 1.17, 95% CI 0.20–6.79), systemic embolism (OR 0.69, 95% CI 0.27–1.75), or composite thromboembolism (OR 0.96, 95% CI 0.42–2.19). TT was associated with increased major bleeding (OR 2.82, 95% CI 1.40–5.68; p=0.004) and any bleeding (OR 2.58, 95% CI 1.73–3.85; p<0.001). There was no significant difference in NACE (OR 1.15, 95% CI 0.58–2.29).
Conclusion
In anterior myocardial infarction, available evidence did not demonstrate a statistically significant reduction in LVT or thromboembolic events with TT compared with DAPT, while bleeding risk was increased. Given moderate heterogeneity, limited randomized evidence, and potential imaging-related under-detection of LVT, these findings do not support routine prophylactic TT and favor individualized risk–benefit assessment.
Keywords
Introduction
Among ACS presentations, anterior ST-segment elevation myocardial infarction (STEMI), most commonly resulting from occlusion of the left anterior descending artery 1,2 is associated with extensive myocardial injury, greater infarct burden, and adverse left ventricular remodeling.3,4
Following a large anterior myocardial infarction, left ventricular thrombus (LVT) formation has historically been reported in up to 20%–25% of patients in the pre-reperfusion era; however, its incidence has declined substantially with the widespread use of primary percutaneous coronary intervention (PCI) and contemporary dual antiplatelet therapy (DAPT). 5 Nevertheless, LVT remains a clinically relevant complication, with contemporary studies reporting an incidence of 6% to 19% among high-risk patients, particularly those with large anterior infarctions. 6 Other risk factors include severely reduced left ventricular ejection fraction (<30%), left ventricular aneurysm formation, and delayed or unsuccessful reperfusion. 7
Early identification of LVT is essential in reducing systemic thromboembolic events. Transthoracic echocardiography is recommended as the first-line imaging modality due to its widespread availability and feasibility in routine clinical practice. 8 However, cardiac magnetic resonance imaging (CMR) has demonstrated superior sensitivity and specificity for the detection of LVT and is recommended when clinical suspicion persists despite inconclusive echocardiographic findings. 9
Strategies aimed at preventing thrombus formation in high-risk patients have attracted considerable clinical interest. However, the optimal prophylactic antithrombotic strategy remains uncertain. Contemporary American College of Cardiology/American Heart Association (ACC/AHA) guidelines suggest that prophylactic AC may be considered in selected high-risk patients, such as those with anterior ST-segment elevation myocardial infarction and significant apical wall motion abnormalities, when the anticipated benefits outweigh bleeding risk. 10 This recommendation carries a Class IIb indication with a low level of evidence, reflecting the limited availability of randomized data. Similarly, recent European Society of Cardiology (ESC) guidelines provide recommendations for the diagnosis and management of established LVT but do not specifically address strategies for its prevention. 11
Randomized clinical trials (RCTs) evaluating the addition of AC to DAPT for the prevention of LVT have yielded inconsistent results. In a randomized study by Zhang et al, the addition of low-dose rivaroxaban (2.5 mg twice daily) to standard DAPT was associated with a lower incidence of LVT without a significant increase in bleeding compared with DAPT alone. 12 In contrast, the more recent multicenter APERITIF trial did not demonstrate a significant reduction in LVT formation with intensified antithrombotic therapy and reported a numerically higher incidence of bleeding events. 13
Similar variability is reported in observational studies; accordingly, a comprehensive and updated synthesis of the available evidence was conducted to evaluate the efficacy and safety of triple antithrombotic therapy (DAPT plus AC) compared with DAPT alone in patients with ACS, with particular emphasis on the prevention of LVT and related clinical outcomes.
Methods
Data Sources
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 14 The study protocol was registered in PROSPERO before data extraction, ID: CRD420261343867. A comprehensive literature search was performed in the following electronic databases: PubMed, Web of Science, and Cochrane Central Register of Controlled Trials (CENTRAL) from inception until March 2026. The search strategy combined controlled vocabulary terms and free-text keywords related to acute coronary syndrome, ST-elevation myocardial infarction, left ventricular thrombus, AC, rivaroxaban, warfarin, dual antiplatelet therapy, and triple antithrombotic therapy. The detailed search terms based on the retrieved database are presented in Supplementary Table 1. Duplicates were removed using EndNote (Clarivate Analytics, PA, USA). The retrieved references were screened in two steps: the first step was to screen the titles/abstracts of all identified articles independently by all authors to assess relevance to this meta-analysis. The Rayyan website 15 was used in this process. The second step was to screen the full-text articles of the identified abstracts for final eligibility for meta-analysis. Any disagreement during the screening processes was resolved by discussion and consensus with a third author.
Study Selection and Outcomes
Studies were included if they met the following criteria: 1) Population of adult patients with acute coronary syndrome, particularly those with ST-segment elevation myocardial infarction. 2) Intervention: Triple antithrombotic therapy consisting of DAPT plus systemic AC. 3) Comparator: DAPT alone. 4) Reporting at least one of the predefined outcomes, including LVT formation, stroke, systemic embolism, major bleeding, or net adverse cardiovascular events (NACE). The outcome definitions are found in Supplementary Table 2. 5) Study design: Randomized controlled trials or observational comparative studies. Studies were excluded if they included no comparator group, did not report extractable outcome data, or were case reports, reviews, editorials, or conference abstracts without sufficient data. Pharmacokinetic studies, pharmacodynamic studies, and non-English studies were also excluded.
Data Extraction and Data Analysis
Data were extracted from the included studies on prespecified data extraction sheets. Extracted data included study characteristics, baseline patient characteristics, and outcome data. The primary outcome was the occurrence of LVT, while secondary outcomes included major bleeding, stroke, and systemic embolism. Two reviewers independently assessed the quality of the included studies using the modified Newcastle-Ottawa Scale (NOS) 16 for observational studies. The scale uses three main domains to assess study quality: selection criteria, comparability testing, and outcome assessment. The risk of bias in each study was classified as good, poor, or fair quality. In the event of disagreement, the reviewers discussed the issues to attain a consensus. Risk of bias for randomized controlled trials was assessed using the Cochrane Risk of Bias tool (RoB 2). 17
Statistical Analysis
Statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria) with the meta and metafor packages. Effect estimates were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Random-effects meta-analyses were conducted using the restricted maximum likelihood (REML) method to estimate between-study variance (τ2), and the Hartung–Knapp–Sidik–Jonkman adjustment was applied to account for uncertainty in variance estimation. Heterogeneity among the included studies was assessed using the I2 statistic and categorized as low, moderate, or high based on thresholds of 25%, 50%, and 75%, respectively. Sensitivity analysis included Leave-one-out sensitivity analyses which was conducted by sequentially excluding individual studies to assess their influence on pooled estimates and evaluate result robustness, as well as subgroup analyses to explore sources of heterogeneity. Publication bias was not formally assessed using funnel plots or Egger’s test because no pooled outcome included 10 or more studies, below which these methods are underpowered and may be misleading. For studies with zero events in one treatment arm, a continuity correction of 0.5 was applied to allow odds ratio estimation; studies with zero events in both arms for a given outcome were not included in the quantitative relative-effect estimate for that outcome because they do not contribute information to the odds ratio, but were retained in the qualitative outcome description when applicable. 18
Results
Study Selection
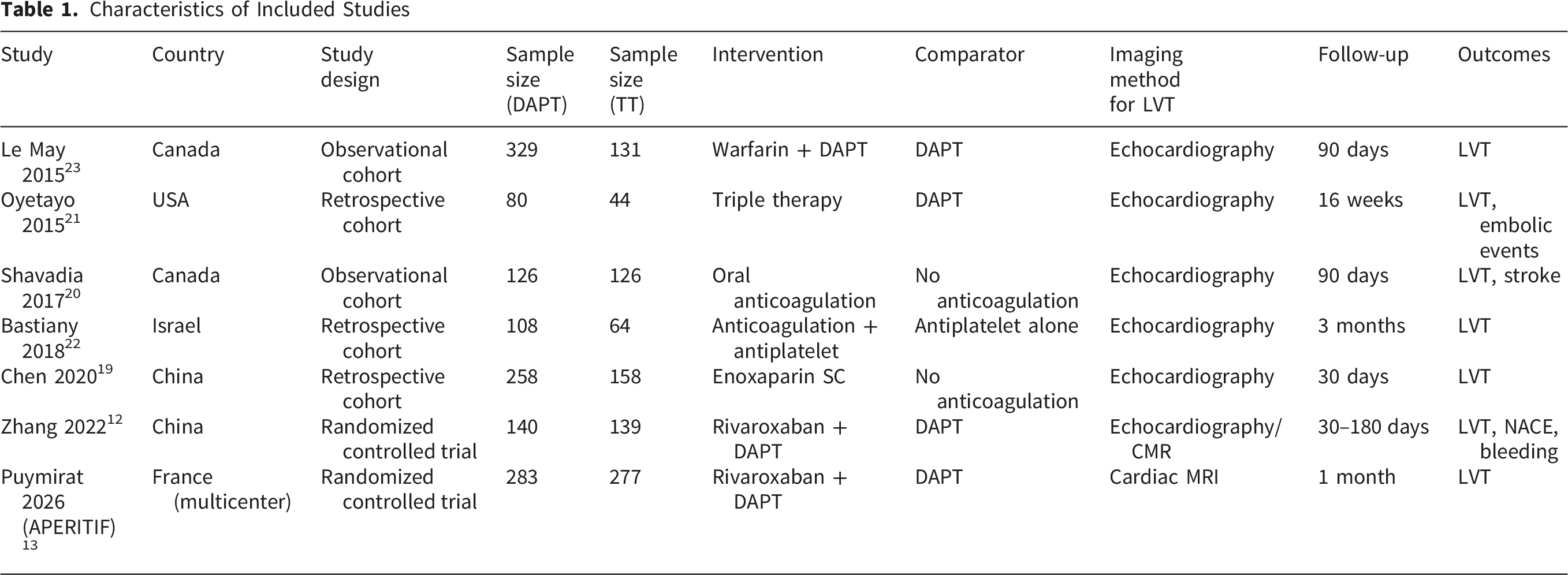
The initial database search identified 707 records from PubMed, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL). After removing 179 duplicate records, 528 studies remained for title and abstract screening. Of these, 502 records were excluded due to irrelevance to the study question. A total of 26 full-text articles were assessed for eligibility. Following full-text evaluation, 19 studies were excluded due to a lack of appropriate comparator groups, insufficient outcome data, or ineligible study design. Ultimately, 7 studies met the inclusion criteria 12,13,19-23 of which 2 were RCTs and 5 were observational studies and were included in the final analysis (Figure 1, Table 1). PRISMA flow diagram. Flow diagram of study identification, screening, eligibility assessment, and final inclusion in the meta-analysis Characteristics of Included Studies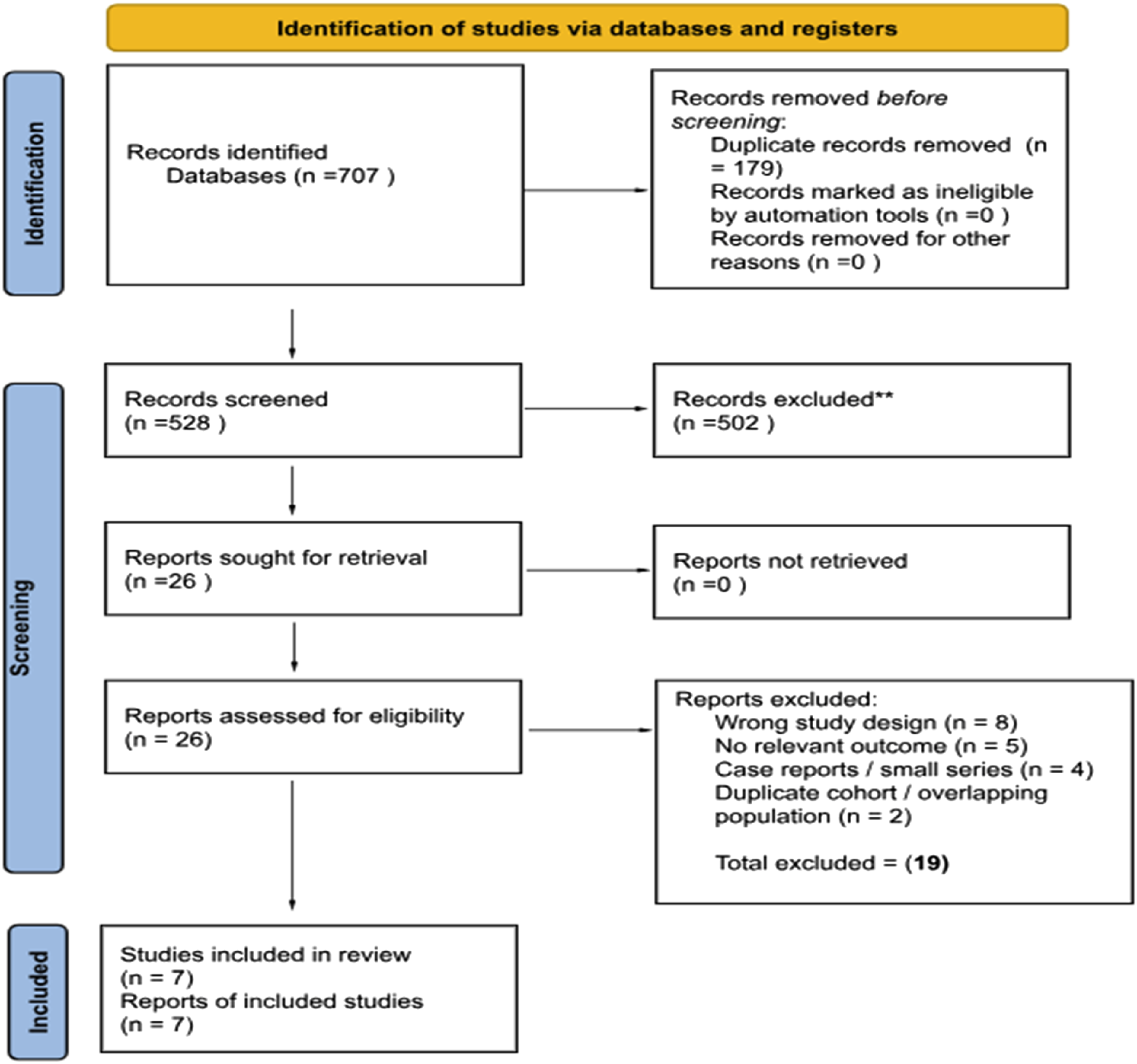
Quality Assessment
The Cochrane RoB 2 tool demonstrated low risk in the randomization process and selective reporting domains in both included trials. However, some concern was noted due to the open-label design, introducing potential deviations from intended interventions. In the APERITIF trial, minor concerns arose from missing outcome data, although this was limited and balanced between groups. In the Zhang trial, additional concern was related to outcome assessment, as LVT was primarily evaluated using echocardiography rather than cardiac magnetic resonance imaging. Overall, both trials were judged as having some concerns with no high-risk domains (Supplementary Figure 1). Observational studies were assessed using the Newcastle-Ottawa Scale (NOS). Methodological quality was moderate to high, with scores ranging from 8 to 9. Most studies achieved full scores in the selection and outcome domains, with minor limitations in comparability due to incomplete adjustment for confounders (Supplementary Figures 1 and 2).
Characteristics of Included Studies
Baseline Characteristics of the Included Patients

Outcomes
Six studies, including 2,017 patients; 821 on TT and 1,196 on DAPT, evaluated the incidence of LVT following acute coronary syndrome. The pooled analysis demonstrated no statistically significant difference in LVT formation between patients receiving TT and those receiving DAPT. The pooled effect estimate showed OR = 0.56 (95% CI 0.21–1.49), p = 0.25, I2 = 59.1%, indicating no statistically significant association between TT and lower LVT formation compared with DAPT alone. (Figure 2A). (A) Left ventricular thrombus (LVT). Forest plot comparing left ventricular thrombus (LVT) formation between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (B) Left ventricular thrombus (LVT) by anticoagulation strategy. Subgroup analysis of left ventricular thrombus (LVT) according to anticoagulation strategy in the triple antithrombotic therapy (TT) group (rivaroxaban vs warfarin/enoxaparin), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (C) Left ventricular thrombus (LVT) by study design. Subgroup analysis of left ventricular thrombus (LVT) according to study design (randomized controlled trials [RCTs] vs observational studies), reported as odds ratios (ORs) with 95% confidence intervals (CIs)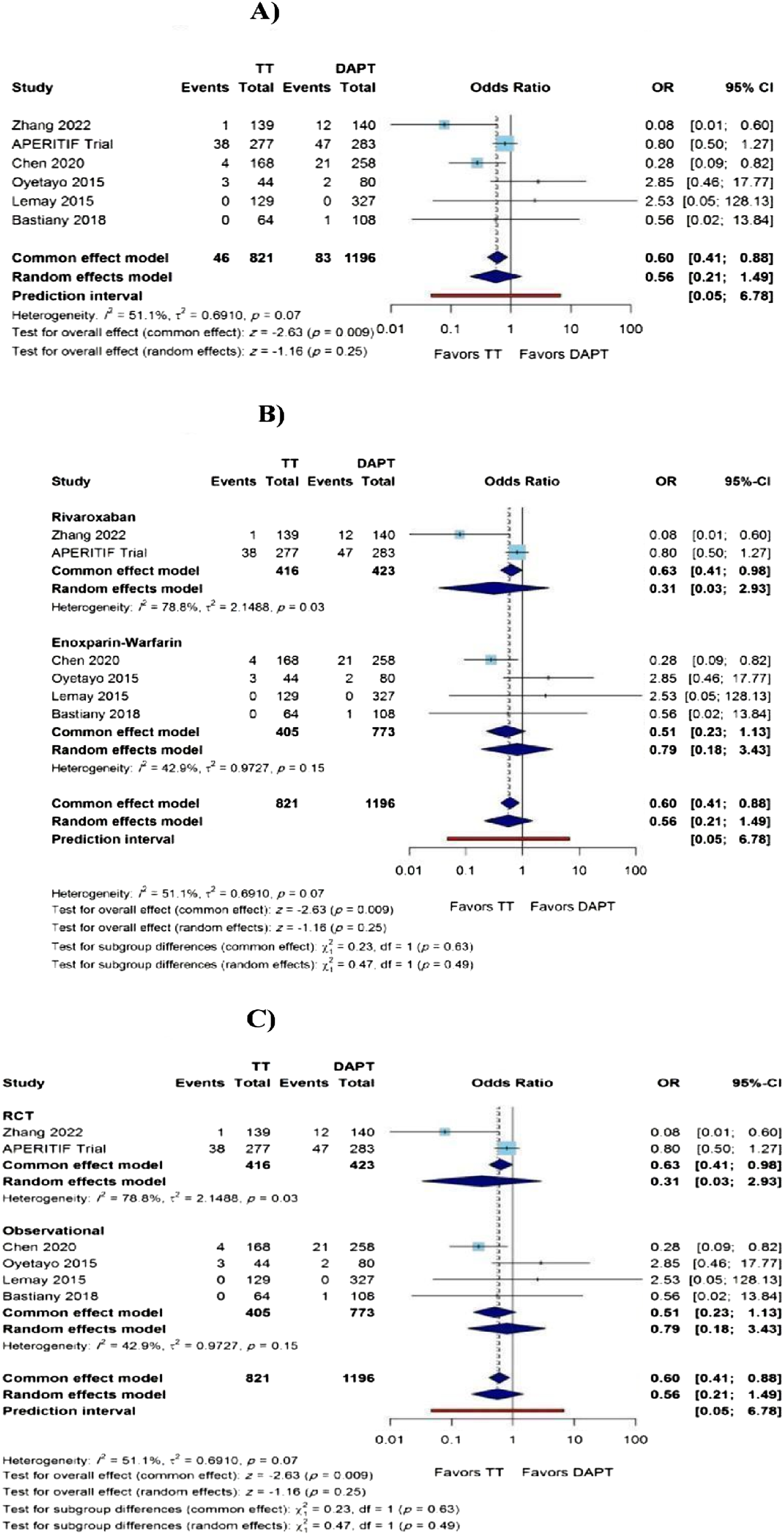
Prespecified exploratory subgroup analyses were conducted to evaluate potential sources of heterogeneity. A subgroup analysis of the AC type used in the TT group; rivaroxaban versus warfarin/enoxaparin did not demonstrate statistical significance for LVT (p = 0.25) (Figure 2B). Study design subgroup analysis (randomized trials versus observational studies) demonstrated no statistical significance (p = 0.25) (Figure 2C). Imaging modality subgroup analysis (cardiac magnetic resonance imaging versus echocardiography) reported a higher detection rate of LVT in studies that used cardiac magnetic resonance imaging compared with those that used echocardiography. However, the relative treatment effect between triple therapy and DAPT remained consistent across imaging modalities, with p for subgroup difference = 0.53. Overall, these subgroup analyses suggest that while diagnostic modality may influence LVT detection rates, the addition of AC to DAPT was not associated with a statistically significant reduction in thrombus formation across study designs or anticoagulation strategies used (Supplementary Figure 3). Finally, a leave-one-out sensitivity analysis was conducted for the primary outcome (LVT) to evaluate the robustness of the pooled estimates. Sequential removal of each study did not materially change the direction or significance of the pooled effect (Supplementary Figure 4).
There was no statistical difference in all-cause mortality across five studies including 1,977 patients, 841 TT, and 1,136 DAPT (OR 0.75, 95% CI 0.27-2.06; p = 0.58; I2 = 59%) (Figure 3A). Leave-one-out sensitivity analysis demonstrated overall stability of the pooled estimate. However, omission of the Le May et al study resulted in a more pronounced shift in the effect estimate (OR 0.44, 95% CI 0.21-0.92; p = 0.03) and complete resolution of heterogeneity (I2 = 0%), indicating that this study had a disproportionate influence on both heterogeneity and statistical significance of the pooled outcome (Supplementary Figure 5). Subgroup analyses according to anticoagulation type and study design showed no significant subgroup differences (p for interaction = 0.78) (Figures 3B and C). (A) All-cause mortality. Forest plot comparing all-cause mortality between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (B) All-cause mortality by anticoagulation strategy. Subgroup analysis of all-cause mortality according to anticoagulation strategy in the triple antithrombotic therapy (TT) group (rivaroxaban vs warfarin/enoxaparin), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (C) All-cause mortality by study design. Subgroup analysis of all-cause mortality according to study design (randomized controlled trials [RCTs] vs observational studies), reported as odds ratios (ORs) with 95% confidence intervals (CIs)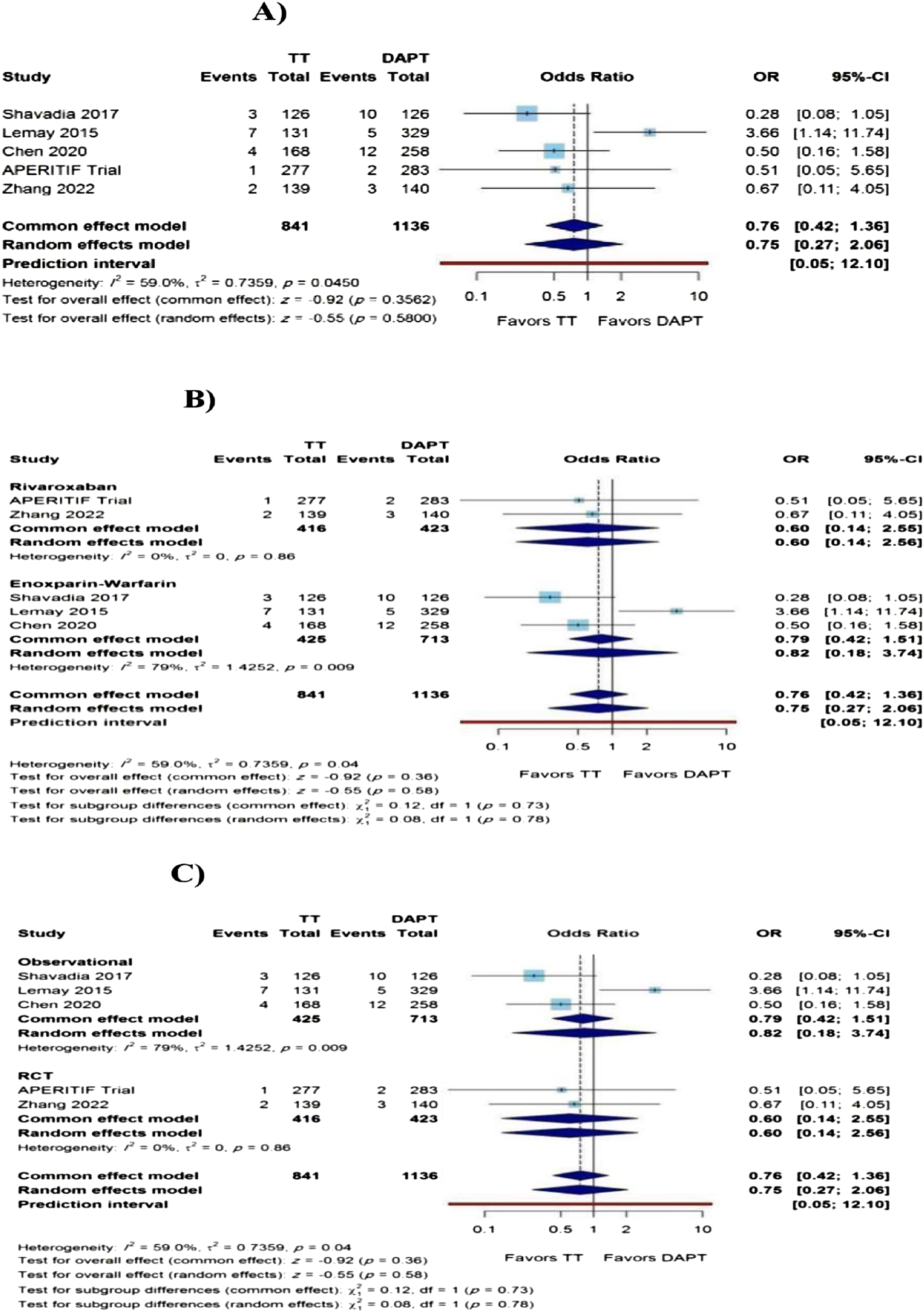
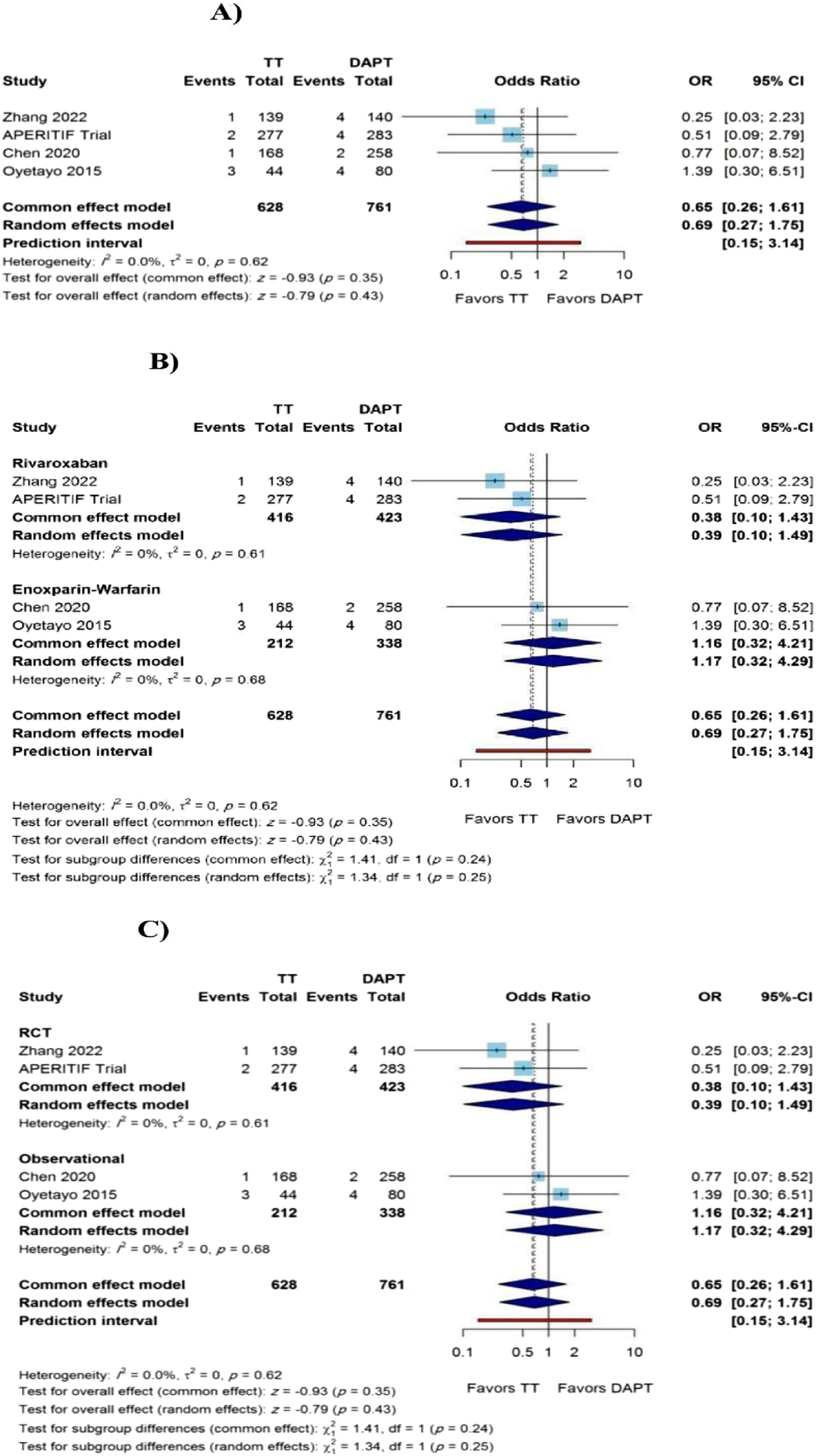
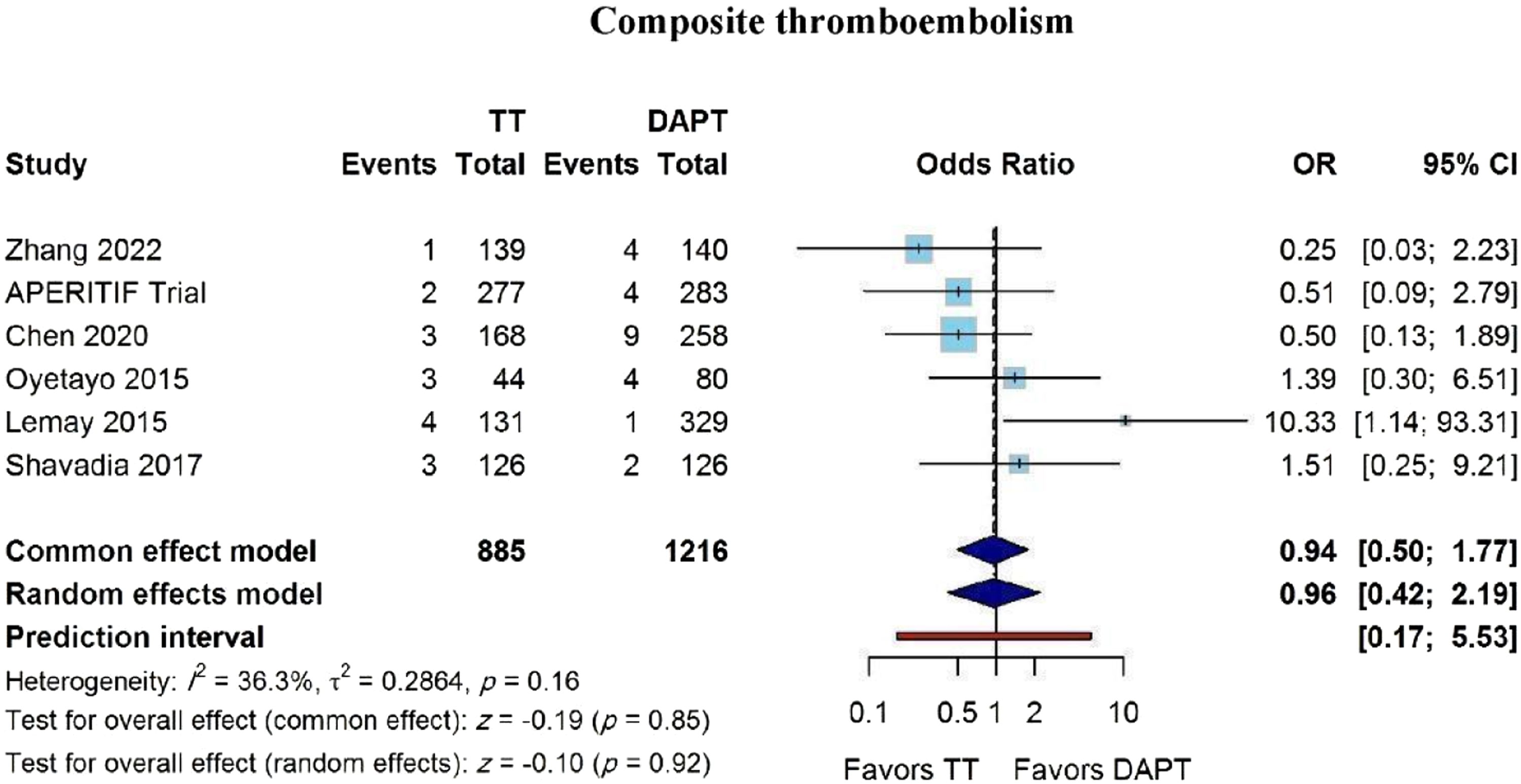
There was no statistical difference in ischemic cerebrovascular accidents across four studies, including 1,570 patients, 620 on TT and 950 on DAPT (OR 1.17, 95% CI 0.20-6.79; p = 0.86; I2 = 48.7%) (Figure 4). Leave-one-out sensitivity analysis demonstrated that the overall estimate remained stable after sequential exclusion of each study (Supplementary Figure 6). Subgroup analyses were not performed, as the APERITIF trial reported zero events in both arms, precluding statistical comparison between subgroups. There was also no statistical difference in systemic embolism across four studies, including 1,389 patients, 628 TT, and 761 DAPT (OR 0.69, 95% CI 0.27-1.75; p = 0.43; I2 = 0%) (Figure 5A). Sensitivity analysis using a leave-one-out approach demonstrated consistent results, with no single study materially influencing the pooled estimate (Supplementary Figure 7). Subgroup analyses stratified by anticoagulation strategy and study design demonstrated no significant difference between subgroups (p for interaction = 0.25) (Figures 5B and C). There was no statistical difference in composite thromboembolic events across six studies, including 2,101 patients, 885 TT and 1,216 DAPT (OR 0.96, 95% CI 0.42-2.19; p = 0.92; I2 = 36.3%) (Figure 6). Leave-one-out sensitivity analysis demonstrated consistent results, with no single study significantly altering the pooled estimate (Supplementary Figure 8). Subgroup analyses according to anticoagulation type and study design showed no significant subgroup differences (p for interaction = 0.14; I2 = 36.3%). Ischemic stroke. Forest plot comparing ischemic stroke between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs) (A) Systemic embolism. Forest plot comparing systemic embolism between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (B) Systemic embolism by anticoagulation strategy. Subgroup analysis of systemic embolism according to anticoagulation strategy in the triple antithrombotic therapy (TT) group (rivaroxaban vs warfarin/enoxaparin), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (C) Systemic embolism by study design. Subgroup analysis of systemic embolism according to study design (randomized controlled trials [RCTs] vs observational studies), reported as odds ratios (ORs) with 95% confidence intervals (CIs) Composite thromboembolism. Forest plot comparing composite thromboembolism between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs)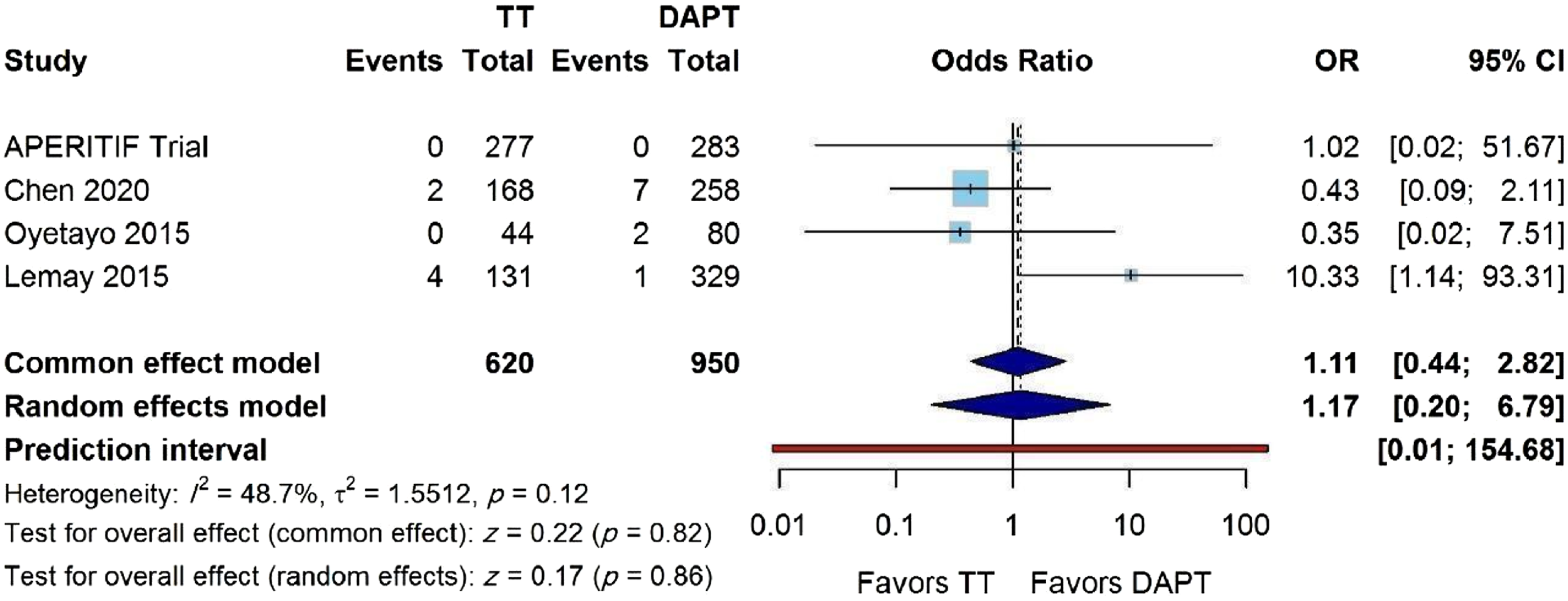
There was a statistically significant higher risk of major bleeding in the TT group across seven studies, including 2,273 patients, 949 TT and 1,324 DAPT (OR 2.82, 95% CI 1.40-5.68; p = 0.004; I2 = 0%) (Figure 7). Leave-one-out sensitivity analysis demonstrated generally consistent effect estimates across studies (OR range 2.03-3.85). Exclusion of the Le May et al study attenuated the association and rendered the result statistically non-significant (OR 2.03, 95% CI 0.84-4.87), suggesting some influence of this study on the overall precision of the estimate (Supplementary Figure 9). Subgroup analyses according to study design (RCT versus observational studies) and type of anticoagulation (rivaroxaban versus warfarin/enoxaparin) showed no significant subgroup interactions (p for subgroup difference = 0.75) (Supplementary Figure 9). Furthermore, TT was associated with significantly higher risk of any bleeding compared with DAPT (OR 2.58, 95% CI 1.73-3.85; p < 0.001; I2 = 0%). Leave-one-out sensitivity analysis demonstrated consistent results, with no single study significantly altering the pooled estimate. Subgroup analyses according to anticoagulation type and study design showed no significant subgroup differences (p for interaction = 0.58) (Supplementary Figure 10). Major bleeding. Forest plot comparing major bleeding between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs)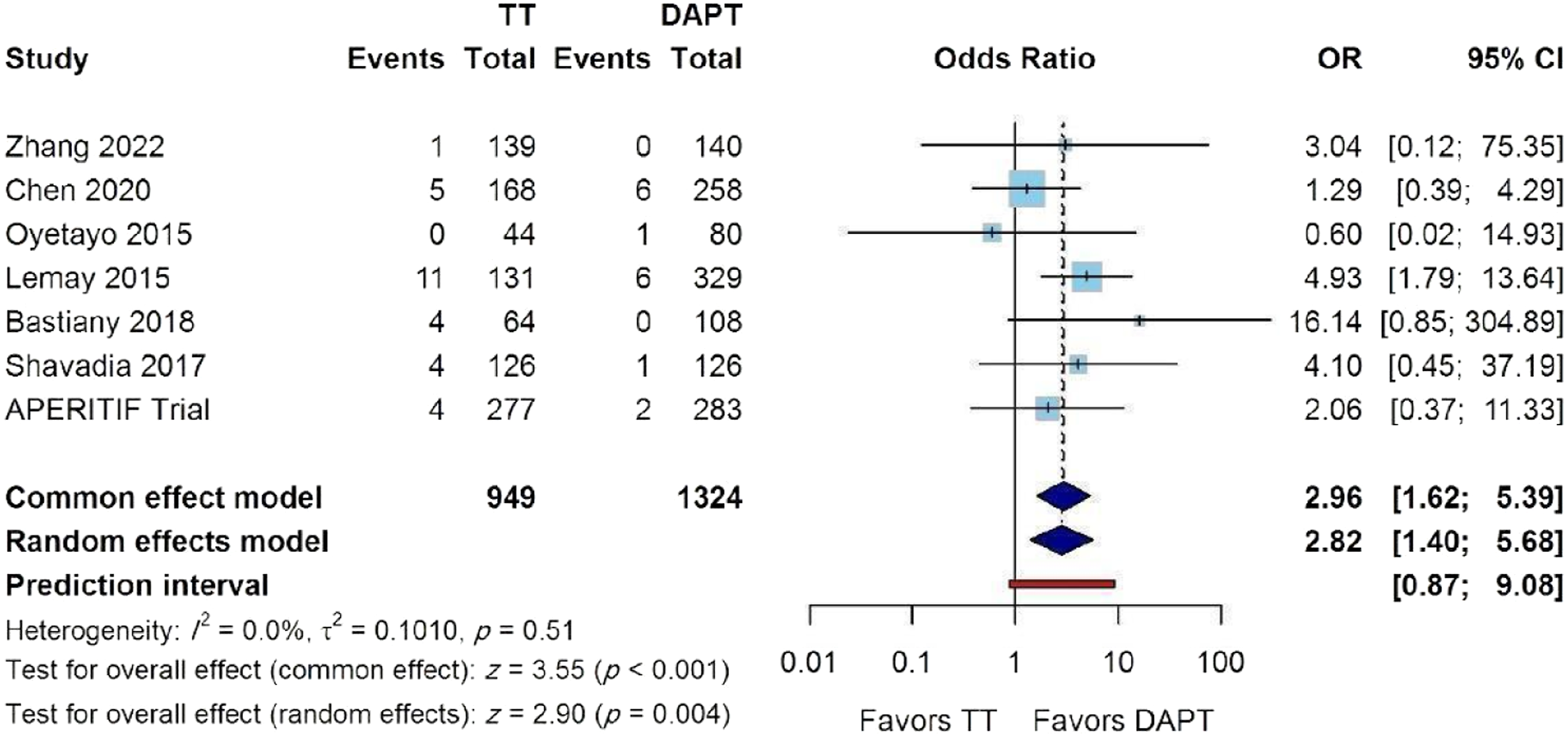
There was no statistical difference in net adverse clinical events across six studies, including 2,017 patients, 821 TT, and 1,196 DAPT (OR 1.15, 95% CI 0.58-2.29; p = 0.69; I2 = 73%) (Figure 8A). Leave-one-out sensitivity analysis demonstrated consistent results, with no single study significantly altering the pooled estimate (Supplementary Figure 11). Subgroup analyses according to anticoagulation type and study design showed no significant subgroup differences (p for interaction = 0.18) (Figures 8B and C). (A) Net adverse clinical events (NACE). Forest plot comparing net adverse clinical events (NACE) between triple antithrombotic therapy (TT) and dual antiplatelet therapy (DAPT), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (B) Net adverse clinical events (NACE) by anticoagulation strategy. Subgroup analysis of net adverse clinical events (NACE) according to anticoagulation strategy in the triple antithrombotic therapy (TT) group (rivaroxaban vs warfarin/enoxaparin), reported as odds ratios (ORs) with 95% confidence intervals (CIs). (C) Net adverse clinical events (NACE) by study design. Subgroup analysis of net adverse clinical events (NACE) according to study design (randomized controlled trials [RCTs] vs observational studies), reported as odds ratios (ORs) with 95% confidence intervals (CIs)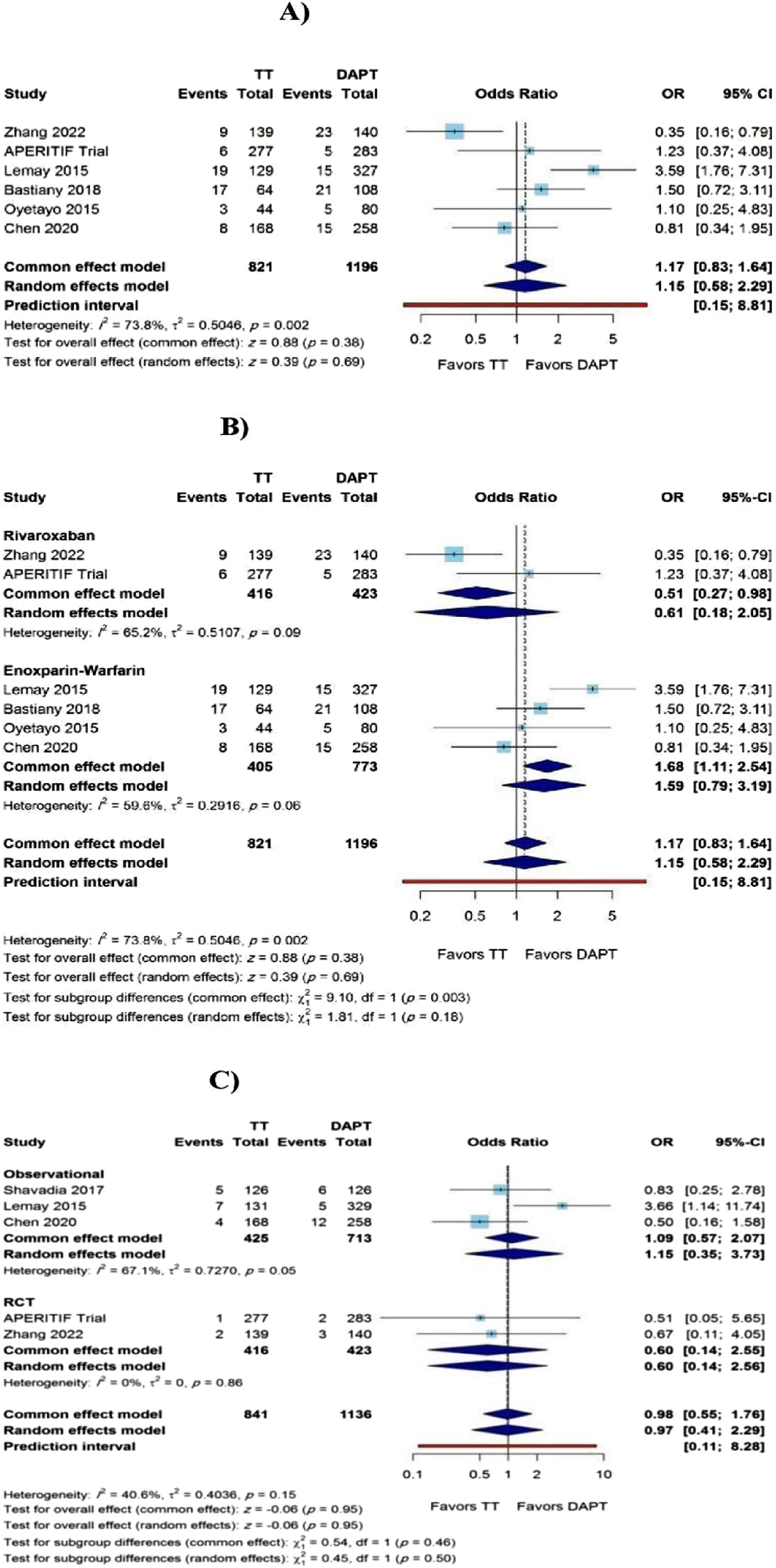
Discussion
This updated meta-analysis focused exclusively on prophylactic anticoagulation rather than treatment of established LVT. In the available evidence, TT was not associated with statistically significant reductions in LVT formation, mortality, ischemic cerebrovascular events, systemic embolism, composite thromboembolism, or NACE compared with DAPT alone. These findings should not be interpreted as definitive proof of no efficacy, particularly given moderate heterogeneity for the primary outcome and the predominance of observational data. However, TT was consistently associated with higher bleeding risk, including major bleeding and any bleeding, supporting a cautious and individualized approach to prophylactic anticoagulation after anterior myocardial infarction.
The 2025 American College of Cardiology (ACC)/American Heart Association (AHA) acute coronary syndrome (ACS) guidelines support AC for selected patients (eg, patients with ST-segment elevation myocardial infarction (STEMI) with anterior apical akinesis or dyskinesis) with a Class IIb recommendation and Level of Evidence C. Our findings support the cautious stance adopted by current guidelines and highlight the need for individualized risk–benefit assessment when considering triple antithrombotic therapy. Because five of the seven included studies were observational, and several lacked comprehensive adjustment for confounding, these findings should be considered hypothesis-generating rather than definitive evidence against prophylactic anticoagulation in all high-risk patients. Despite the strong theoretical rationale for AC in this setting, where ventricular akinesia, endothelial injury, and blood stasis following myocardial infarction create a prothrombotic milieu 24 we found no reduction in LVT with TT compared with DAPT. Moreover, our findings contradict the previous meta-analysis of 5 observational studies by Sacoransky et al 25 which reported a significant reduction in LVT for patients treated with TT compared with those receiving DAPT (OR 0.28, 95% CI 0.11 to 0.73, p < 0.01). Additional analyses further confirmed the robustness of the primary findings. Subgroup analyses according to type of AC (rivaroxaban versus warfarin/enoxaparin) and study design (randomized versus observational studies) demonstrated no significant subgroup interactions, suggesting that the absence of benefit of TT in LVT prevention was consistent across AC strategies and study methodologies. Moreover, leave-one-out sensitivity analysis demonstrated that sequential exclusion of individual studies did not materially change the pooled effect estimate, confirming the stability of the primary outcome.
An important source of clinical and methodological heterogeneity was the imaging modality used for LVT detection. Most included studies relied on transthoracic echocardiography, which is widely available and clinically practical but has lower sensitivity than CMR, particularly for small, mural, or apical thrombi. 26 As a result, echocardiography-based studies may have underestimated the absolute incidence of LVT and introduced outcome misclassification. In contrast, CMR provides higher diagnostic accuracy and may identify thrombi that would otherwise remain undetected. This issue is clinically relevant because differential or incomplete detection of LVT could attenuate observed treatment effects. Notably, the APERITIF trial used systematic CMR screening and still did not demonstrate a statistically significant reduction in LVT with intensified antithrombotic therapy, although the limited number of randomized studies prevents definitive conclusions.
The lack of a statistically significant reduction in thromboembolic outcomes, including stroke, systemic embolism, and composite thromboembolism, suggests that any potential benefit of TT may be smaller or more selective than anticipated, rather than uniformly applicable to all patients with anterior myocardial infarction. These findings suggest that thromboembolic risk following myocardial infarction is driven by multiple mechanisms and may not be adequately reduced by simply adding systemic AC to DAPT. Importantly, patients at highest risk for LVT, such as those with large anterior infarctions and reduced ejection fraction, also represent a population with inherently elevated ischemic risk.27,28
Our analysis extends prior evidence by evaluating ischemic cerebrovascular events as an independent endpoint, whereas earlier meta-analyses have largely focused on composite embolic outcomes, previous pooled analyses in anterior myocardial infarction populations suggested a numerical, but non-significant, reduction in embolic events with TT (OR ∼0.37), though these estimates were limited by low event rates and heterogeneous outcome definitions. Our findings align with more contemporary data and randomized evidence, including studies such as the APERITIF Trial, which have similarly failed to demonstrate a consistent reduction in clinically overt embolic events despite the theoretical benefits of AC. Taken together, the lack of efficacy across individual and composite thromboembolic endpoints, alongside consistent findings across sensitivity and subgroup analyses, supports current guideline recommendations that advocate for a selective, individualized approach to TT rather than routine use.
TT was associated with a significantly higher risk of major bleeding compared with DAPT alone, with no observed heterogeneity across studies. However, sensitivity analysis demonstrated generally consistent effect estimates across studies (OR range 2.03–3.85). The removal of the study by Le May et al attenuated the association and rendered the estimate non-significant. This may be explained by differences in treatment strategy, as the Le May study utilized approximately six months of warfarin, a longer duration than most included studies, which may have contributed to higher bleeding rates and a concomitant increase in mortality; additionally, patients receiving warfarin in this cohort had worse baseline ventricular function, suggesting potential confounding by indication. Importantly, subgroup analyses demonstrated consistent findings regardless of study design or AC strategy, suggesting that the increased bleeding risk appears to be related to the overall intensity of TT rather than a specific AC regimen. This observation is notable given that DOACs are generally considered safer and easier to use than vitamin K antagonists, with several studies demonstrating lower rates of intracranial hemorrhage and improved safety profiles in multiple cardiovascular settings. 29 This pattern is consistent with the prior trials including WOEST 30 PIONEER AF-PCI 31 RE-DUAL PCI 32 AUGUSTUS 33 and ENTRUST-AF PCI 34 which consistently demonstrated that TT significantly increases bleeding compared with strategies that minimize concurrent antiplatelet and AC exposure. Although DOAC-based regimens have been shown to reduce bleeding compared with VKA-based triple therapy, these studies also demonstrated that any form of TT remains associated with a higher bleeding risk than dual-pathway approaches.
This study has several limitations. First, only two randomized controlled trials were available, and most included studies were observational, introducing potential selection bias, confounding by indication, and residual confounding despite study-level quality assessment. Second, there was clinical and methodological heterogeneity across studies, including differences in anticoagulation regimens, antiplatelet strategies, treatment duration, patient risk profiles, and imaging protocols for LVT detection. Third, most studies relied primarily on transthoracic echocardiography, which has lower sensitivity than CMR and may have underestimated the true incidence of LVT, particularly small or mural thrombi. This measurement limitation could have biased absolute event rates and potentially attenuated observed treatment effects. Fourth, the relatively low number of events limited statistical power for clinically relevant outcomes such as LVT, systemic embolism, and ischemic cerebrovascular events. Finally, the lack of individual patient-level data precluded adjusted patient-level analyses and limited exploration of important treatment-effect modifiers.
Conclusion
In this systematic review and meta-analysis of patients with anterior myocardial infarction, the addition of prophylactic AC to DAPT was not associated with a statistically significant reduction in LVT formation, all-cause mortality, ischemic cerebrovascular events, systemic embolism, composite thromboembolism, or NACE, while bleeding risk was increased. These findings should be interpreted cautiously, given the limited number of randomized trials, predominance of observational evidence, moderate heterogeneity for LVT, and potential imaging-related under-detection of thrombus. Overall, the current evidence does not provide conclusive support for routine prophylactic TT after anterior myocardial infarction. Larger, adequately powered randomized trials using standardized imaging protocols, preferably including CMR, are needed to determine whether selected high-risk patients may derive net clinical benefit from prophylactic anticoagulation in addition to DAPT.
Supplemental Material
Supplemental Material - Triple Antithrombotic Therapy vs Dual Antiplatelet for Prevention of Left Ventricular Thrombus After Anterior Myocardial Infarction: An Updated Meta-Analysis
Supplemental Material for Triple Antithrombotic Therapy vs Dual Antiplatelet for Prevention of Left Ventricular Thrombus After Anterior Myocardial Infarction: An Updated Meta-Analysis by Mustafa Abomohsen, Ibrahim Elkhayat, Ahmed Elmorsy Mohamed, Abdul Hakim Almakadma, Zeyad Kholeif, Ahmed Farid Gadelmawla, Ameer Awashra, Muhammed A. Youssef, Osamah AlQassab, Mohamed Ghannam, Vikas Patel, Azad Mojahedi, Iyad Idries, Meena Farid, Moshe Gunsburg, and Hal L. Chadow in Clinical and Applied Thrombosis/Hemostasis.
Footnotes
Consent for Publication
All authors approved the final manuscript and the submission to this journal.
Author Contributions
M.A., I.E., and A.E.M. designed the study and wrote the main manuscript. M.A., I.E., A.E.M., A.H.A., Z.K., A.F.G., M.A.Y., O.A., M.G., V.P., A.M., I.I., and M.F. extracted the data and prepared the figures and tables. M.G. and H.L.C. reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are available in the manuscript and its Supplementary Material. Additional extracted data and analytic code are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.