
Abstract
Objective
The D-dimer to fibrinogen ratio (DFR) has been suggested as a biomarker reflecting disease severity in multiple conditions. This study investigated the relationship between DFR and 3-month outcomes in acute ischemic stroke (AIS) patients undergoing intravenous thrombolysis.
Methods
Consecutive AIS patients treated with intravenous thrombolysis were enrolled. Clinical and laboratory data were collected, and functional outcomes were assessed at 3 months using the modified Rankin Scale (mRS), with scores of 3–6 defined as unfavorable. Receiver operating characteristic (ROC) analysis identified the optimal DFR cutoff, and multivariable logistic regression determined predictors of unfavorable outcomes.
Results
Among 184 patients included, 66 (35.9%) experienced unfavorable outcomes. Compared with patients with favorable outcomes, those with unfavorable outcomes had higher fasting blood glucose, D-dimer, fibrinogen, DFR, and baseline NIHSS scores (P < 0.05), and lower high-density lipoprotein (HDL) levels (P < 0.05). The optimal DFR cutoff for predicting 3-month outcomes was 0.146. Three multivariable logistic regression models were constructed because of the potential collinearity among D-dimer, fibrinogen, and DFR. After adjustment for confounding factors, DFR remained independently associated with unfavorable outcomes (OR = 3.827, 95% CI: 1.289–11.365, P = 0.016).
Conclusion
In summary, our findings suggest that DFR is associated with outcomes in AIS patients receiving intravenous thrombolysis.
Introduction
Acute ischemic stroke (AIS) is caused by thrombotic occlusion of cerebral vessels, leading to cerebral ischemia, hypoxia, and subsequent tissue necrosis. It remains a primary cause of both mortality and disability worldwide.1-3 Intravenous thrombolysis is a key therapeutic strategy for restoring cerebral perfusion in the early stage of stroke and improving neurological outcomes. Although significant advances have been made in the treatment of AIS in recent years, a substantial proportion of patients still experience unfavorable functional outcomes. Stroke-related speech and motor impairments often persist lifelong, imposing considerable economic and social burdens on patients, families, and society.4,5 Therefore, identifying reliable biomarkers that can rapidly predict clinical outcomes is of great clinical importance for achieving individualized and precise management of AIS.
The dynamic balance between coagulation and fibrinolysis is critical in the initiation, progression, and outcomes of various diseases.6-8 Fibrinogen is not only a key substrate for thrombus formation but also an acute-phase reactant, and elevated levels of this marker are linked to poor outcomes of stroke. 9 D-dimer, a fibrin-specific degradation product, reflects activation of the fibrinolytic system and overall thrombus load, and higher levels have been reported to predict early poor outcomes in AIS patients. 10 The D-dimer to fibrinogen ratio (DFR), as a composite biomarker, may more comprehensively reflect the net effect between coagulation activation and secondary fibrinolytic responses than a single indicator. Studies have reported that elevated DFR levels are significantly associated with the diagnosis, disease severity, and unfavorable outcomes of AIS.11,12 Moreover, the prognostic value of DFR has also been validated in other arterial thrombotic diseases.13-17 Elevated DFR levels independently predict cardiovascular events following percutaneous coronary intervention. 18 These findings suggest that DFR, as a marker of systemic hypercoagulability and prothrombotic status, may have prognostic value beyond a single disease entity.
However, despite growing evidence supporting the prognostic value of DFR in AIS, data specifically evaluating its role in patients undergoing intravenous thrombolysis remain limited. Given that intravenous thrombolysis profoundly influences coagulation and fibrinolytic pathways, the prognostic significance of DFR in this specific population may differ from that observed in unselected AIS cohorts. Therefore, the present study aimed to investigate the association between baseline DFR levels and 3-month functional outcomes in AIS patients treated with intravenous thrombolysis, with the goal of providing a simple and practical tool for early risk stratification and clinical decision-making.
Methods
Study Population
This study consecutively enrolled patients with AIS who received intravenous thrombolysis at the Affiliated Fuyang People’s Hospital of Anhui Medical University between April 2024 and November 2025. AIS was diagnosed based on clinical presentation and confirmed by magnetic resonance imaging (MRI). Intravenous thrombolysis was performed in eligible patients according to established guideline-based protocols. Inclusion criteria were patients diagnosed with AIS. Exclusion criteria were: (1) contraindications to intravenous thrombolysis; (2) coexisting hematologic or immunologic disorders; (3) cognitive impairment or psychiatric disorders; (4) malignancy or infectious diseases; (5) receipt of bridging endovascular therapy; (6) prestroke disability defined as a modified Rankin Scale (mRS) score >2. (7) incomplete clinical data.
Clinical Data Collection
Baseline clinical characteristics, including age, sex, diabetes mellitus, hypertension, atrial fibrillation, coronary artery disease, and history of stroke, were recorded for all patients. Door-to-needle time (DNT) was collected. Blood samples for coagulation parameters were collected on admission before thrombolysis to prevent the influence of thrombolytic therapy. Fasting biochemical indicators were obtained the following morning. Despite the different collection times, all measurements represent early hospitalization status and were included as baseline prognostic variables. Plasma D-dimer and fibrinogen (FIB) levels were measured using an automated coagulation analyzer following the manufacturer’s protocol. DFR was calculated as the ratio of D-dimer to fibrinogen. 19
Stroke Severity and Outcome Assessment
Stroke severity at admission was evaluated using the National Institutes of Health Stroke Scale (NIHSS). Functional outcome, measured by the modified Rankin Scale (mRS), was defined as the primary endpoint. All enrolled patients were followed up at 3-month by neurologists blinded to the patients’ grouping and imaging data. Outcomes were categorized based on mRS scores: 0–2 indicated favorable outcomes, whereas mRS ≥3 indicated unfavorable outcomes (severe disability or death). 20
Statistical Analysis
Descriptive statistics summarized baseline data as frequencies, means±SD/medians, or median (M) and interquartile range (IQR). The 3-month functional outcome was defined as the dependent variable. DFR was analyzed as both a continuous and categorical variable. In the primary analysis, DFR was treated as a continuous variable and included in correlation analyses and multivariable logistic regression models to evaluate its association with clinical outcomes. For descriptive and clinical interpretability purposes, patients were additionally stratified into low and high DFR groups. The optimal cutoff value of 0.146 was determined using receiver operating characteristic (ROC) curve analysis based on the Youden index. Variables with P < 0.1 in univariate analysis were included in a multivariable binary logistic regression model. Because DFR is derived from D-dimer and fibrinogen, separate multivariable logistic regression models were constructed to avoid potential multicollinearity. Statistical significance was set at P < 0.05. The predictive performance of DFR for unfavorable outcomes was evaluated using receiver operating characteristic (ROC) curve analysis. All statistical analyses were performed using SPSS version 22.0.
Results
Clinical and Demographic Data
Clinical and Laboratory Indicators Between Favorable and Unfavorable Outcomes

Abbreviations: SBP, systolic blood pressure; DBP, Diastolic blood pressure; FBG, fasting blood glucose; TG, triglycerides; TC, total cholesterol; HDL, High-density lipoprotein; LDL, Low-density lipoprotein; DFR, D-dimer/fibrinogen ratio; NIHSS, National Institutes of Health Stroke Scale.
Comparison of Clinical and Laboratory Parameters Between Outcome Groups
Patients with unfavorable outcomes exhibited significantly higher fasting blood glucose, D-dimer, fibrinogen, DFR, and baseline NIHSS scores, whereas high-density lipoprotein (HDL) levels were significantly lower compared with those with favorable outcomes (P < 0.05). As illustrated in Figure 1, DFR levels were significantly elevated in the unfavorable outcome group (P < 0.001). No other variables differed between the two groups (P > 0.05). DFR levels were significantly higher in the unfavorable outcome group compared with the favorable outcome group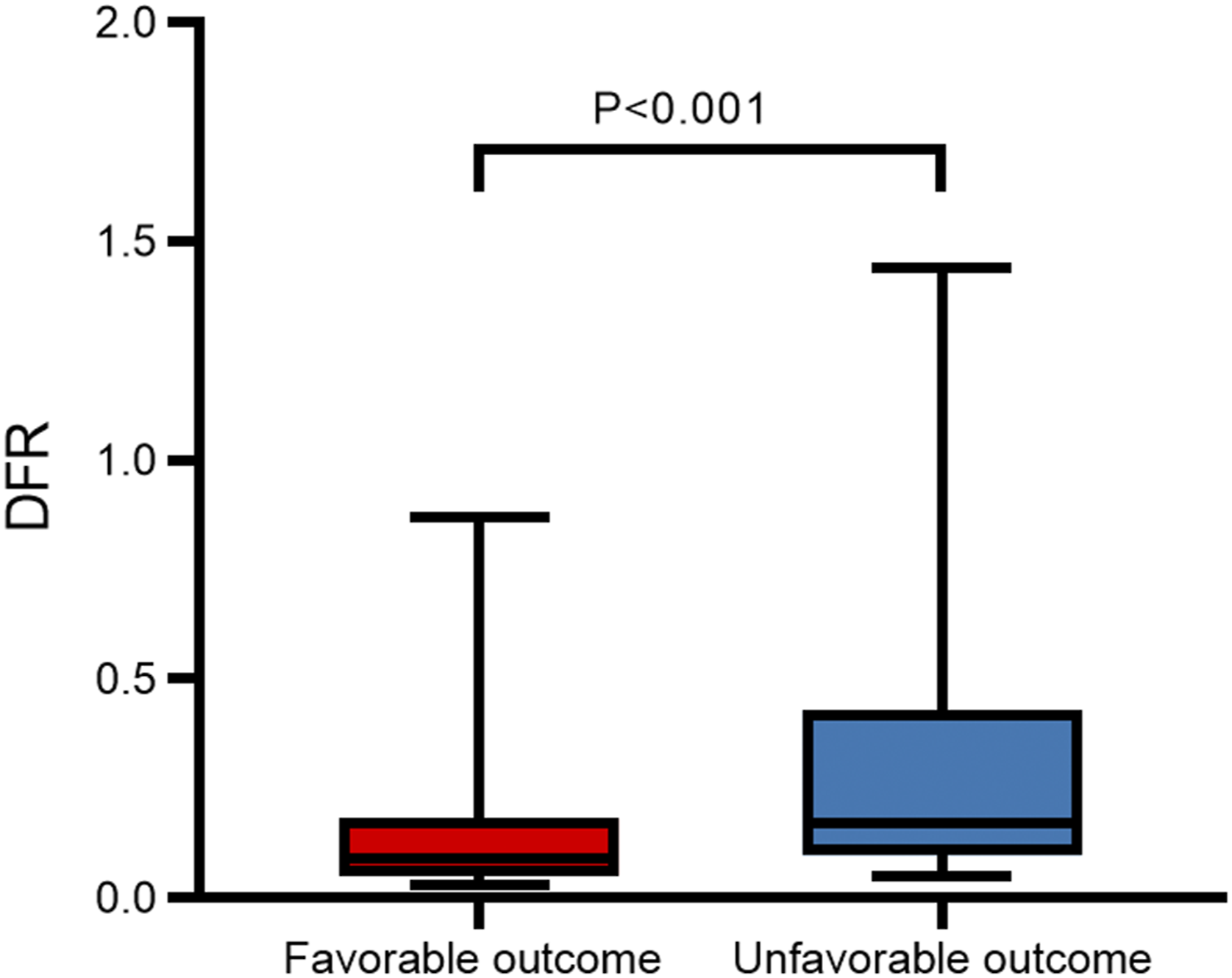
Association Between DFR and 3-Month Clinical Outcomes
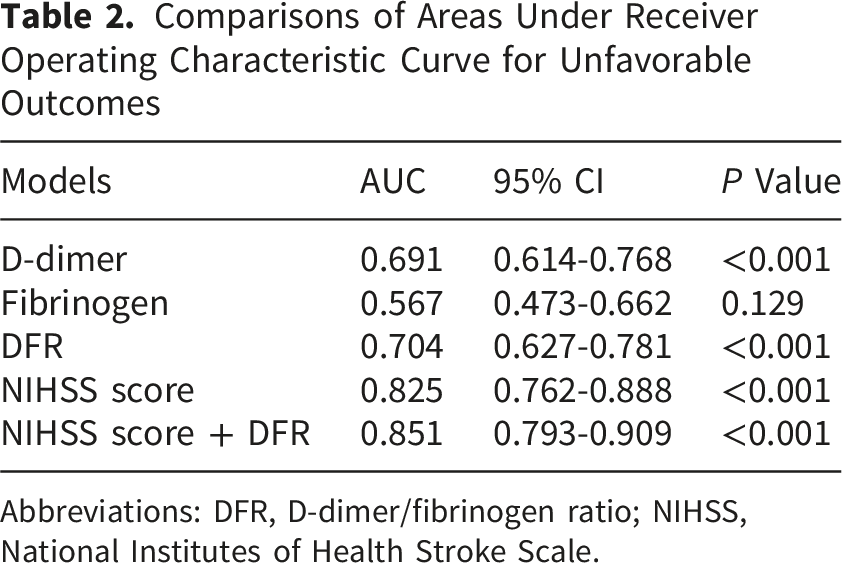
To evaluate the incremental predictive value of DFR, additional receiver operating characteristic (ROC) curve analyses were performed. DFR demonstrated a higher discriminative ability than D-dimer and fibrinogen alone, with an area under the curve (AUC) of 0.704 (95% CI: 0.627–0.781), compared with 0.691 (95% CI: 0.614–0.768) for D-dimer and 0.567 (95% CI: 0.473–0.662) for fibrinogen.
These findings indicate that DFR provides better risk discrimination than its individual components, likely reflecting a more balanced representation of coagulation and fibrinolysis. This composite index may better capture the underlying pathophysiological state associated with stroke severity and post-thrombolysis outcomes than single biomarkers.
In addition, the addition of DFR to the NIHSS score improved predictive performance (AUC increased from 0.825 to 0.851), indicating incremental value beyond established clinical severity assessment (Figure 2, Table 2). Receiver operating characteristic (ROC) curve analyses for predicting unfavorable outcomes after intravenous thrombolysis. (A) ROC curves of DFR, D-dimer, and fibrinogen for outcome prediction. (B) ROC curves of NIHSS score and NIHSS + DFR model Comparisons of Areas Under Receiver Operating Characteristic Curve for Unfavorable Outcomes Abbreviations: DFR, D-dimer/fibrinogen ratio; NIHSS, National Institutes of Health Stroke Scale.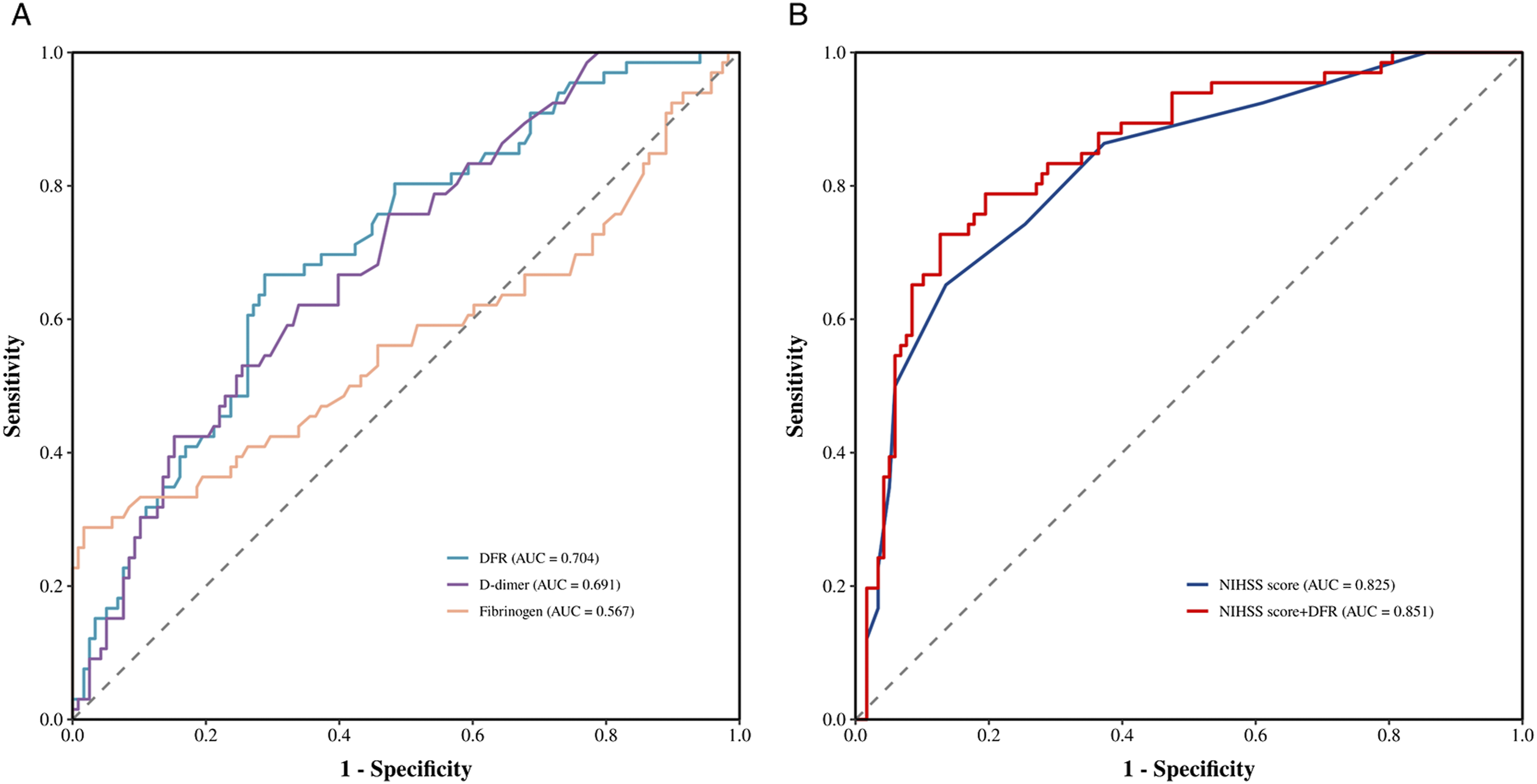
Comparison of Clinical Characteristics by DFR Stratification
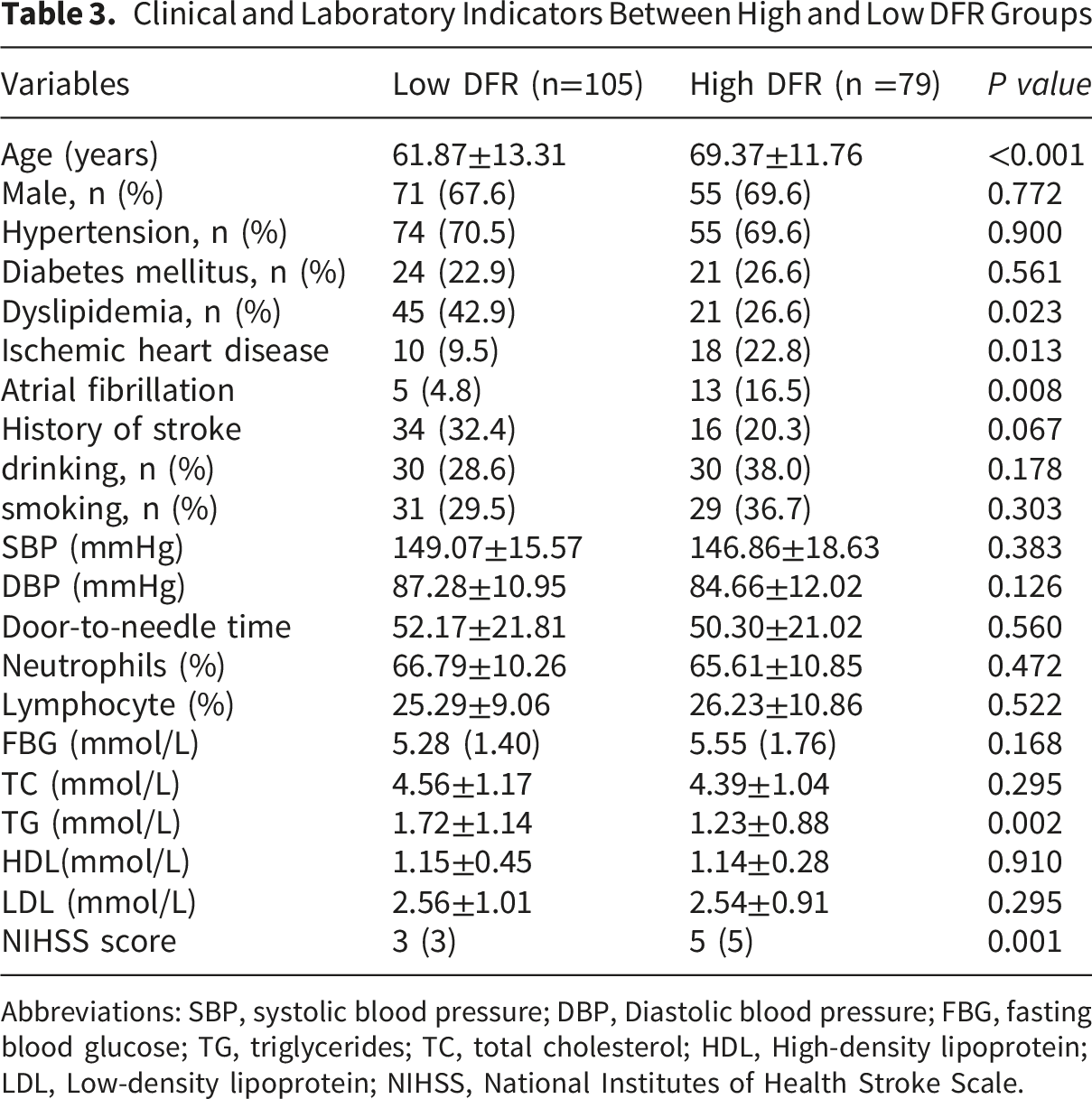
Clinical and Laboratory Indicators Between High and Low DFR Groups
Abbreviations: SBP, systolic blood pressure; DBP, Diastolic blood pressure; FBG, fasting blood glucose; TG, triglycerides; TC, total cholesterol; HDL, High-density lipoprotein; LDL, Low-density lipoprotein; NIHSS, National Institutes of Health Stroke Scale.
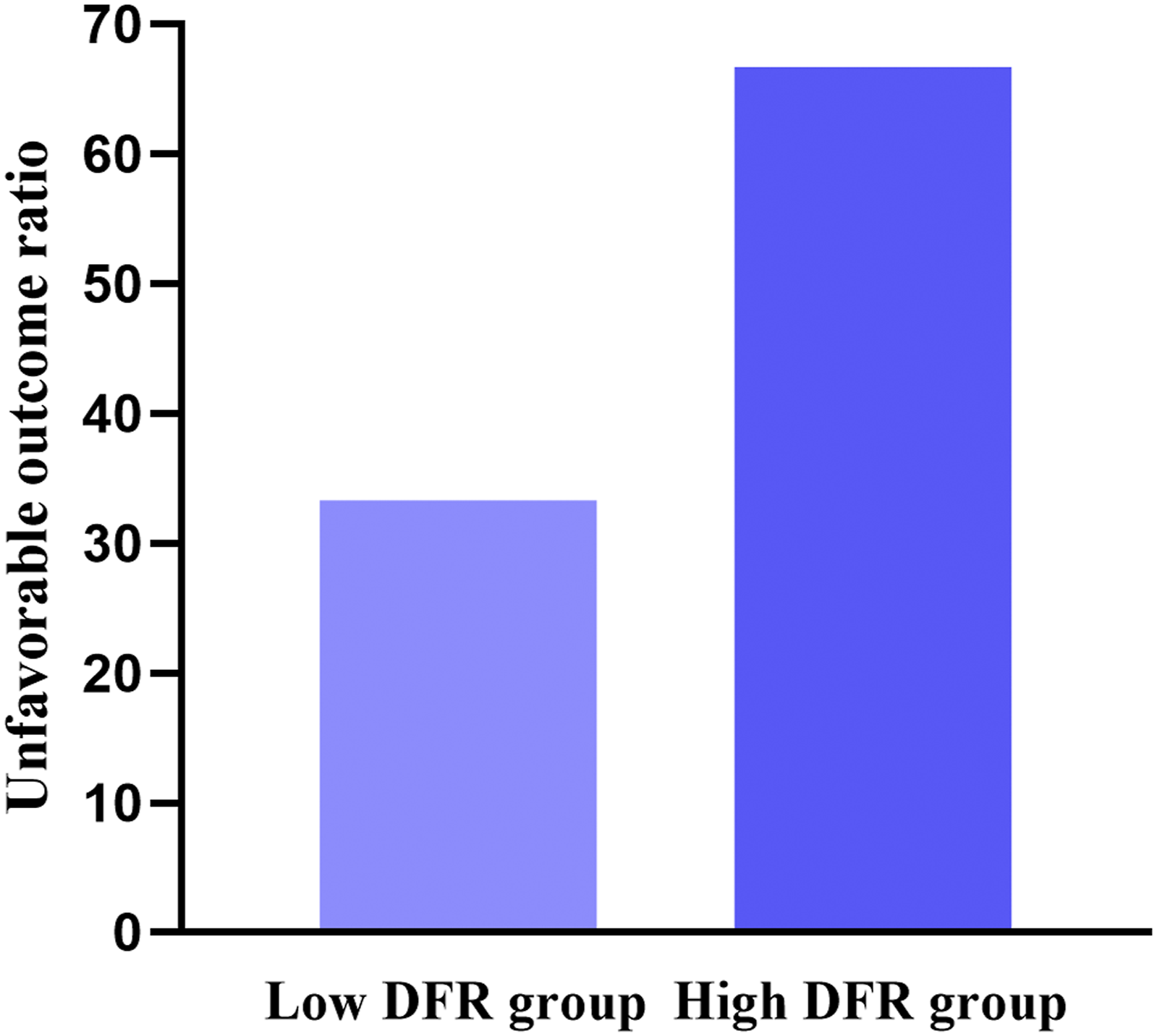
Percentage of patients with unfavorable outcomes stratified by DFR
Association Between DFR and Unfavorable Outcomes
Multivariate Logistic Regression Models of Associated Factors for Unfavorable Outcomes
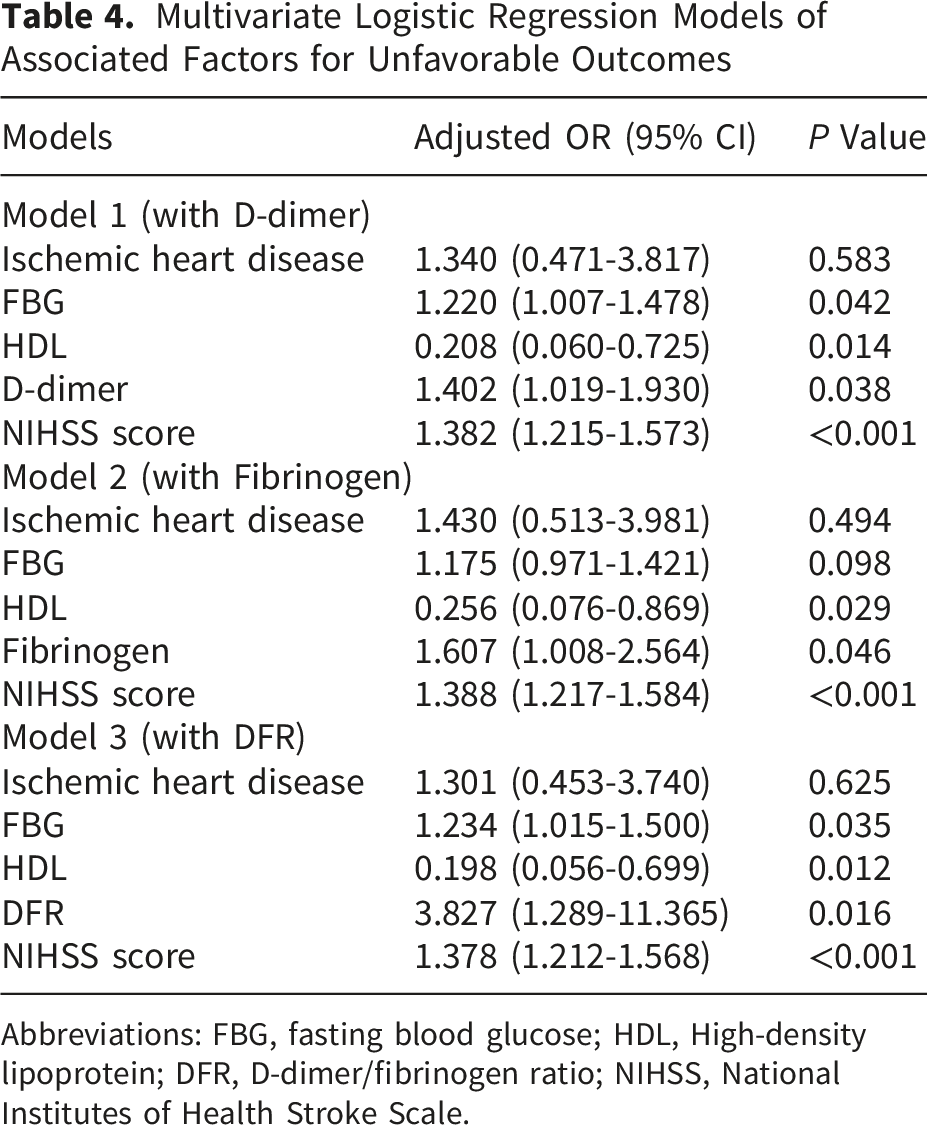
Abbreviations: FBG, fasting blood glucose; HDL, High-density lipoprotein; DFR, D-dimer/fibrinogen ratio; NIHSS, National Institutes of Health Stroke Scale.
Discussion
This study evaluated the relationship between DFR and unfavorable outcomes in AIS patients receiving intravenous thrombolysis. The results indicated that elevated DFR levels were significantly associated with poor functional outcomes after intravenous thrombolysis in AIS patients. DFR may serve as a simple and readily available biomarker to assist in outcome assessment in this population.
Increasing evidence suggests that inflammatory and coagulation-related pathways play a central role in the pathophysiology of acute ischemic stroke, contributing to thrombus formation, endothelial injury, and subsequent neurological deterioration.7,21 Growing evidence indicates that dysregulation of coagulation and fibrinolysis is central to the pathophysiology of acute ischemic stroke. Circulating hemostatic biomarkers, including tissue factor–related components and factor VIIa–antithrombin complexes, have been shown to reflect systemic activation of coagulation pathways and to be associated with stroke severity and treatment-related changes. 22 In parallel, traditional markers such as fibrinogen and D-dimer capture complementary aspects of thrombin generation, fibrin formation, and fibrinolytic activity.
Fibrinogen is closely related to thrombosis, platelet aggregation, blood viscosity, atherosclerosis formation, and inflammatory response. 23 During coagulation, fibrinogen is converted to fibrin by thrombin and forms a cross-linked fibrin network that participates in platelet aggregation, serving as a key component for maintaining normal hemostasis and stabilizing blood clots. 24 Fibrinogen also contributes to inflammatory and oxidative stress responses and may induce cerebral vasospasm, leading to endothelial injury and atherosclerosis. 25 Additionally, fibrinogen can destabilize the fibrous cap and increase adhesion molecule expression, resulting in endothelial dysfunction and thrombosis, which may promote plaque rupture and exacerbate AIS severity, ultimately leading to poorer clinical outcomes.26,27 Consistently, our findings also suggest that fibrinogen is associated with 3-month unfavorable outcomes in AIS patients with intravenous thrombolysis.
D-dimer is a soluble fibrin degradation product generated through polymerization and cross-linking of fibrinogen under the action of thrombin and activated coagulation factors, followed by plasmin-mediated degradation, containing two covalently linked D domains. 28 D-dimer levels may increase under certain physiological and pathological conditions, including acute infection, tissue injury, shock, hypercoagulable states, and acute myocardial infarction.29,30 Increased D-dimer concentrations may reflect active cerebral vessel thrombosis. Moreover, D-dimer can activate inflammatory processes by promoting the release of pro-inflammatory cytokines, which play a critical role in atherosclerosis, endothelial dysfunction, acute-phase reactions, and hypercoagulable states. 31 All of these factors may contribute to adverse outcomes in AIS patients. D-dimer levels are significantly elevated in AIS patients with unfavorable outcomes.32,33 Consistently, our study found that elevated D-dimer levels were associated with unfavorable outcomes following intravenous thrombolysis in AIS patients.
Elevated DFR reflects an imbalanced coagulation-fibrinolysis state. An increased DFR may indicate secondary hyperfibrinolysis in the context of widespread thrombosis or coexistence of systemic hypercoagulability and hyperfibrinolysis. The studies have indicated that this novel marker is correlated with acute cerebral venous thrombosis, postpartum pulmonary embolism, and lower extremity deep vein thrombosis, showing strong clinical utility.13,15,34 DFR has also been linked to adverse outcomes in intracerebral hemorrhage patients, and to clinical outcomes after percutaneous coronary intervention,17,18 collectively indicating that DFR serves as a marker of activity and severity in systemic atherosclerotic thrombotic diseases. Moreover, in young stroke patients, the correlation between DFR and carotid plaque suggests that this marker may reflect vulnerable plaque burden, which could partially explain its prognostic role in AIS. 35
High DFR levels were associated with unfavorable outcomes of AIS, potentially because this coagulation-fibrinolysis imbalance reflects extensive endothelial injury, increased thrombotic burden, or impaired collateral circulation. 12 By integrating the pathophysiological characteristics of fibrinogen and D-dimer, DFR provides comprehensive information about AIS patients and can effectively predict prognosis. This is consistent with our findings and highlights its significance in outcome assessment.
It should be noted that patients in the high-DFR group were older and had a higher prevalence of comorbidities and more severe stroke at baseline, suggesting that DFR may partly reflect an overall high-risk clinical profile rather than an isolated biological factor. Previous studies have shown that advanced age is associated with poorer clinical outcomes and higher mortality rates. 36 Although multivariable analyses were adjusted for potential confounders, including demographic characteristics, vascular risk factors, and baseline NIHSS, residual confounding cannot be fully excluded in this retrospective study. Therefore, the association between DFR and outcomes should be interpreted as a statistical association rather than evidence of causality. Further prospective studies are needed to validate these findings.
This study is the first to explore the relationship between DFR and outcomes in AIS patients undergoing intravenous thrombolysis. Nevertheless, several limitations warrant consideration. First, the relatively small sample size and limited number of outcome events may affect the robustness and stability of the multivariable analysis, leading to relatively wide confidence intervals. Therefore, the present findings should be considered exploratory and require validation in larger, prospective, multicenter studies. Second, only baseline D-dimer and fibrinogen measurements were available, and temporal changes in DFR were not assessed. Third, several treatment-related variables were not fully available and could not be included. Residual confounding cannot be excluded. Prospective studies are needed for validation. Finally, this study evaluated only short-term outcomes at 3 months post-treatment, and long-term prognostic value was not assessed; extended follow-up is needed to examine the predictive performance of DFR for long-term outcomes.
Conclusion
Our study indicates that elevated DFR is independently associated with unfavorable outcomes in AIS patients after intravenous thrombolysis. As a readily calculable hematological marker, DFR may have potential value as a biomarker to assist in risk stratification and prognostic assessment in this population. However, further studies are needed to validate its clinical utility.
Footnotes
Acknowledgements
The authors thank the study participants.
Ethical Considerations
The study was approved by the Research Ethics Committee of the Affiliated Fuyang People’s Hospital of Anhui Medical University ([2022]180).
Consent to Participate
Written informed consent was obtained from the patients or their legal proxies.
Author Contributions
XZ was involved in the design of the study, data collection and manuscript writing. YF participated in data collection and statistical analysis. JL participated in the interpretation of the data and manuscript revision. All authors read and approved the protocol.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Fuyang City Key Research and Development Plan for Clinical Medical Research Translation Special Project (Grant No. FYZDYF2023LCYX011) and the Fuyang Health and Health Commission Project (FYZC2024-029).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during the current study are available from the corresponding author on reasonable request.