
Abstract
Background
Hospital-associated venous thromboembolism (HA-VTE) is the leading preventable cause of death among patients undergoing gynecological surgery. Standard risk assessment methodologies, such as the Caprini score, which is a commonly utilized tool for risk assessment, do not sufficiently account for the unique vulnerabilities inherent to this specialty. To address these deficiencies, we aimed to develop a preliminary machine learning framework for predicting venous thromboembolism (VTE) in gynecological contexts.
Methods
In this retrospective case-control investigation, we identified 75 patients who were consecutively diagnosed with postoperative VTE after undergoing gynecological surgery at Ningbo NO.2 Hospital between March 2020 and February 2025. Controls were chosen using a matching protocol at a ratio of 1:3, resulting in the random selection of 225 patients free from VTE within the same surgical cohort during the same period. An Extremely Randomized Trees (Extratrees) machine learning classifier was constructed, incorporating 22 clinically relevant predictors identified by univariate analyses. We utilized the new model to compare it against the Caprini score.
Results
The model was trained and validated with a class-stratified 70:30 split and exhibited remarkable discriminative ability, achieving an area under the curve (AUC) of 0.907 [95% confidence interval (CI): 0.833–0.972], significantly exceeding the performance of the Caprini score (AUC 0.731, 95% CI: 0.660–0.803). The model showed consistent discrimination across validation groups, yielding an accuracy of 0.833.
Conclusion
This preliminary machine learning framework, tailored specifically for gynecology, provides enhanced risk stratification for VTE.
Keywords
Strengths and Limitations of This Study
1. Current risk assessment models, such as the 2. An
Introduction
Venous thromboembolism (VTE) is recognized as a prevalent cardiovascular condition globally. Each year, the global incidence of VTE is approximately 0.5 to 1 case per 1,000 individuals. 1 Notably, more than 50% of VTE instances occur as a direct result of medical procedures, leading the World Health Organization (WHO) to identify hospital-associated VTE (HA-VTE) as the foremost preventable cause of death within healthcare settings. 2 Specific factors, such as surgical trauma, extended periods of immobilization, cancer treatments, and pre-existing medical conditions, collectively stimulate coagulation pathways in patients receiving hospital care. 3 This combination not only prolongs the period of hospitalization but also increases healthcare expenses and results in preventable deaths, making HA-VTE a critical concern both clinically and economically. 4
In this context, patients undergoing gynecological surgery encounter a set of uniquely compounded risks. Biological sex-specific factors, including hormonal fluctuations 5 or the use of contraceptives, 6 interact with the natural tendency for blood clotting associated with gynecological cancer. 7 These aspects are compounded by procedural risks. For example, extended periods in the lithotomy position can exert pressure on the popliteal veins. 8 Existing prevention strategies are fundamentally misaligned with these particular issues. Commonly used risk assessment tools (for instance, Caprini scores 9 ), which have predominantly been validated within general surgical or orthopedic demographics, do not sufficiently account for gynecological considerations, such as specific histological subtypes of cancer, hormonal influences or the features of minimally invasive surgical techniques. 10 This misalignment leads to a significant clinical dilemma in that the rates of pharmacological prophylaxis are inadequate for gynecological procedures, especially those that are benign, thus placing high-risk patients in a vulnerable position for preventable VTE while exposing low-risk patients to unnecessary bleeding complications arising from anti-coagulation treatments.
To address these systemic deficiencies, we developed a preliminary machine learning framework known as Extremely Randomized Trees (Extratrees) that was specifically designed for predicting VTE in gynecological settings. As a powerful ensemble technique characterized by its dual randomization approach, Extratrees provided an extra layer of randomness by selecting split thresholds entirely at random for each candidate feature; this approach differed significantly from standard random forest analyses, which determine optimal split thresholds at the nodes of the trees. 11 This algorithm exceeded the linear limitations typically associated with conventional scoring through three key transformative features. 12 First, the recursive random partitioning framework of Extratrees handled high-dimensional heterogeneous datasets by combining multimodal indicators, such as preoperative characteristics (e.g., tumor biomarkers), intraoperative factors (e.g., duration of surgery and volume of blood loss), and evolving postoperative patterns (e.g., trends in D-dimer), to identify nonlinear interactions for features that standard models may omit. Second, by randomly selecting both features and split thresholds during the construction of trees, Extratrees naturally reduced the risk of overfitting and improved generalizability, even with a limited number of gynecological samples. This ensures ongoing vigilance from preoperative assessment to critical postoperative stages. In contrast, traditional tools focus on macroscopic phenomena and lack a sufficient understanding of specific time windows, such as the 24-hour postoperative time point. This methodological advancement signifies a substantial shift towards personalized prevention of VTE in gynecological surgical practice.
Methods
Study Design and Patient Recruitment
This research involved adult female individuals who were undergoing gynecological surgeries at Ningbo NO.2 Hospital between March 2020 and February 2025. Each participant underwent imaging examinations prior to surgery to eliminate any pre-existing VTE. Those identified with postoperative VTE via imaging results were categorized into the case group. A control group was established by randomly selecting non-VTE subjects at a ratio of 1:3 to the cases, utilizing the sampling tool within the Analysis ToolPak of Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA), with the criterion that they did not show evidence of postoperative VTE in their imaging results. Patients with additional high-risk factors for VTE in other systems, such as new fractures or pneumonia, should be excluded from the study. Additionally, our research did not involve any participants under the age of 18.
Data Collection
Data relating to preoperative baseline characteristics, routine laboratory tests conducted within 1 week prior to surgery, intraoperative documentation and postoperative laboratory results obtained within 24 hours following surgery were retrieved from the hospital’s electronic medical record system. During the 5-year research period, the analytical methods for all laboratory assays were maintained consistently; the Department of Laboratory Medicine carried out rigorous quality control testing on reagents, using both intra- and inter-batch testing, thus ensuring that all results adhered to set standards.
Ethics Statement
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Approval for the study protocol was granted by the Ethics Committee at Ningbo NO.2 Hospital (Ethics number: PJ-NBEY-KY-2025-056-01). This research featured the retrospective examination of medical records and stored samples and ensured that there were no detrimental consequences to patient interests or privacy. All clinical data were completely anonymized, and the Ethics Committee waived the need for informed consent. Patients or the public WERE NOT involved in the design, or conduct, or reporting, or dissemination plans of our research.
Statistical Analysis
Data management was performed using Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA, USA) with dual-entry verification. Statistical analyses were carried out with SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and the SPSSPRO online platform (Version 1.0.11; Beijing QingSi Data Technology Co., Ltd.). All graphical representations were created using GraphPad Prism version 10.1.2 (GraphPad Software, San Diego, CA, USA).
For continuous variables, normality was assessed using Shapiro-Wilk tests; normally distributed data are presented as the mean ± standard deviation (SD), while non-normally distributed data are expressed as the median (interquartile range; P25–P75). Group comparisons were executed with independent t-tests after confirming homogeneous variance via Levene’s test for parametric data, whereas non-parametric variables were analyzed by Mann-Whitney U tests. Categorical variables are presented as the frequencies (percentages) and were analyzed by χ2 or Fisher’s exact tests, with two-sided p-values < 0.05 deemed statistically significant.
An Extratrees classifier model was developed with SPSSPRO, utilizing features that exhibited inter-group differences in univariate analyses. Preprocessing steps: continuous variables were used as-is (tree-based models do not require scaling); missing values (none); categorical variables were one-hot encoded. The modeling procedure entailed training on 70% of randomly selected data, assessing feature importance based on Gini impurity reduction 13 and evaluating performance on the remaining 30% test dataset, and kept all other parameters at their default settings. Model assessment included four main metrics: accuracy (the ratio of correctly classified instances, where higher values signified better performance), recall (the rate of true positive identification, with greater sensitivity being preferred), precision (the positive predictive value, for which higher precision indicated fewer false positives) and F1-score (the harmonic mean of precision and recall, providing insights into the balance between these metrics).
Results
Baseline Characteristics of Cases and Controls
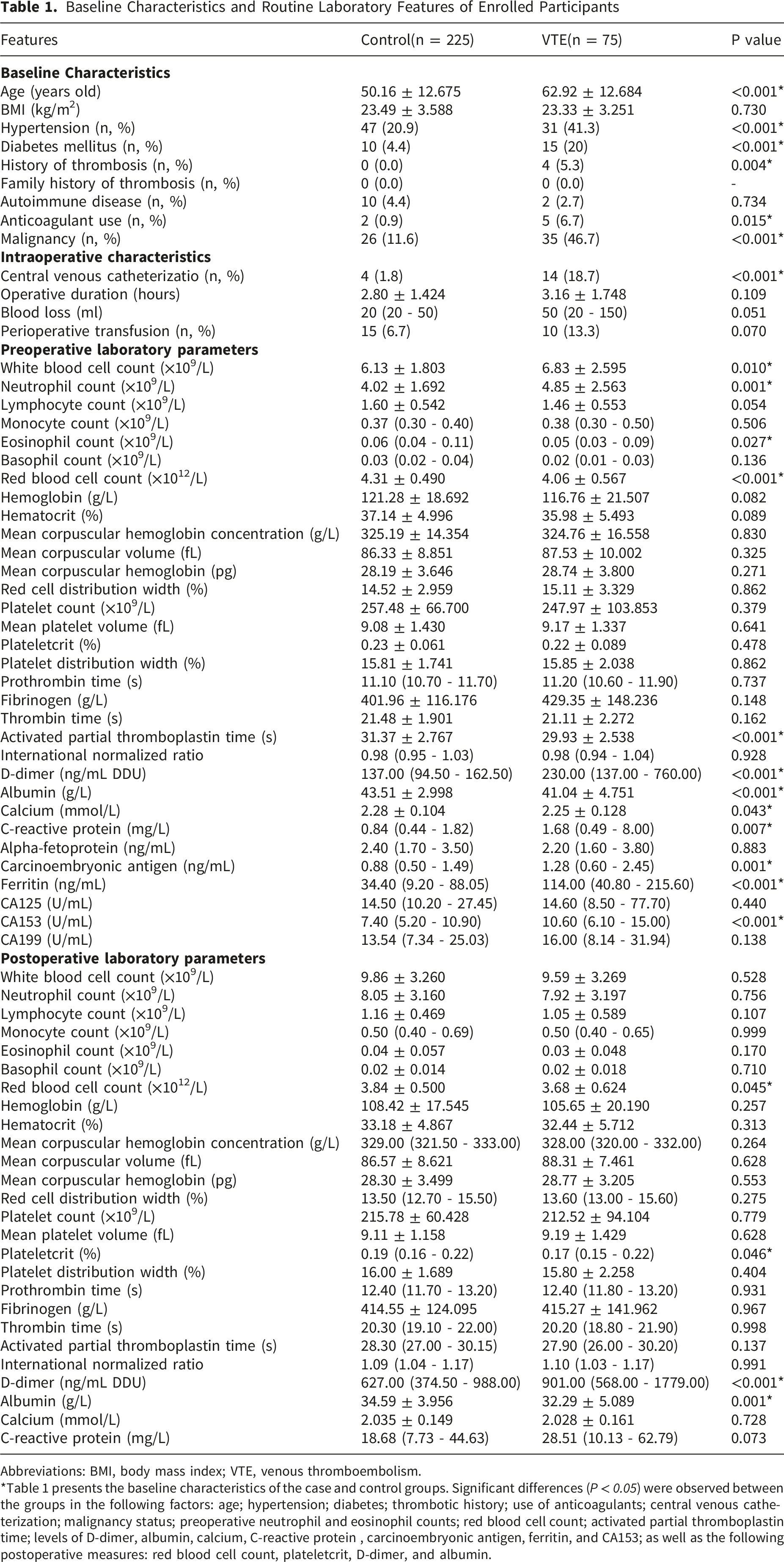
A group consisting of 75 cases and 225 corresponding controls participated in the study (refer to Figure 1 for a flowchart describing participant recruitment). We identified significant differences between the groups (P<0.05) with regards to several factors: age, the presence of hypertension, the occurrence of diabetes, thrombotic history, the use of anticoagulants, central venous catheterization, malignancy status, preoperative counts of neutrophils and eosinophils, red blood cell count, activated partial thromboplastin time (APTT); the levels of D-dimer, albumin, calcium, C-reactive protein (CRP), carcinoembryonic antigen (CEA), ferritin, and CA153; in addition to postoperative metrics (red blood cell count, plateletcrit, D-dimer, and albumin) (as detailed in Table 1). Flow of case data collection. Abbreviations: VTE, venous thromboembolism Baseline Characteristics and Routine Laboratory Features of Enrolled Participants Abbreviations: BMI, body mass index; VTE, venous thromboembolism. *Table 1 presents the baseline characteristics of the case and control groups. Significant differences (P < 0.05) were observed between the groups in the following factors: age; hypertension; diabetes; thrombotic history; use of anticoagulants; central venous catheterization; malignancy status; preoperative neutrophil and eosinophil counts; red blood cell count; activated partial thromboplastin time; levels of D-dimer, albumin, calcium, C-reactive protein , carcinoembryonic antigen, ferritin, and CA153; as well as the following postoperative measures: red blood cell count, plateletcrit, D-dimer, and albumin.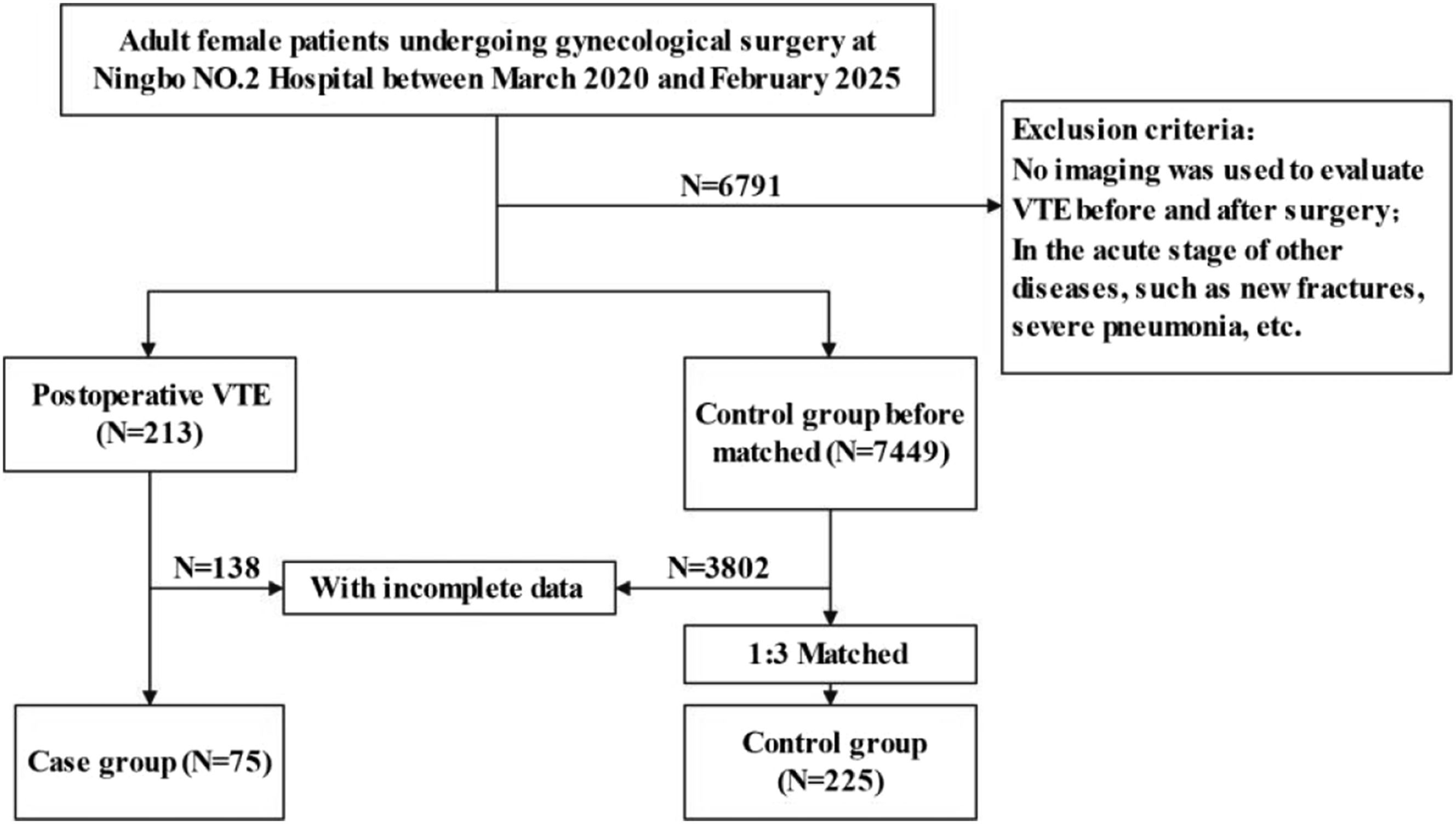
Caprini Score Classification Performance
The most recent version of the Caprini risk assessment models was published in 2013.
14
There was a significant difference in Caprini risk scores between the case group and the controls (5.13 ± 1.73 compared to 3.45 ± 1.27; P<0.05). When applying the defined high-risk threshold (Caprini score ≥ 5), receiver operating characteristic (ROC) analysis revealed an area under the ROC curve (AUC) of 0.731 for the prediction of VTE, with a 95% confidence interval (CI) ranging from 0.660 to 0.803 (see Figure 2). Receiver Operating Characteristic (ROC) Curves Comparing Extratrees Model and Caprini Score for Predicting Postoperative venous thromboembolism in Gynecological Surgery. Abbreviations: AUC, area under the ROC curve
Extratrees Prediction Modeling and Machine Learning Classification Performance
Parameter Values of the Extratrees Classifier Prediction Model
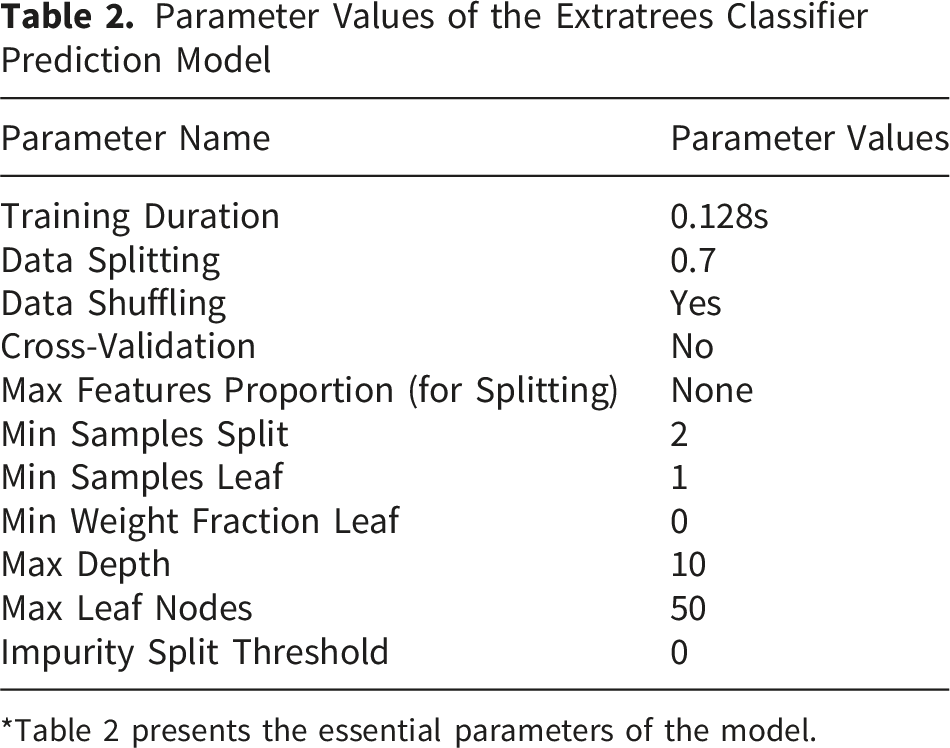
*Table 2 presents the essential parameters of the model.
An analysis of feature importance ranked the following variables in order of their contribution: age, the presence of malignancy, preoperative D-dimer levels, preoperative APTT, plateletcrit at the postoperative stage, postoperative D-dimer levels, preoperative albumin levels, CEA prior to surgery, red blood cell count preoperatively, eosinophil count prior to surgery, red blood cell count post-surgery, albumin levels post-surgery, neutrophil count prior to surgery, preoperative calcium levels, diabetes status, ferritin levels prior to surgery, preoperative CA153, preoperative CRP, the use of central venous catheters, hypertension, previous occurrences of thrombosis, and the use of anticoagulants (Figure 3). Feature Importance Ranking in the Extratrees Classifier Prediction Model. Abbreviations: APTT, activated partial thromboplastin time; CEA, carcinoembryonic antigen; CRP, C-reactive protein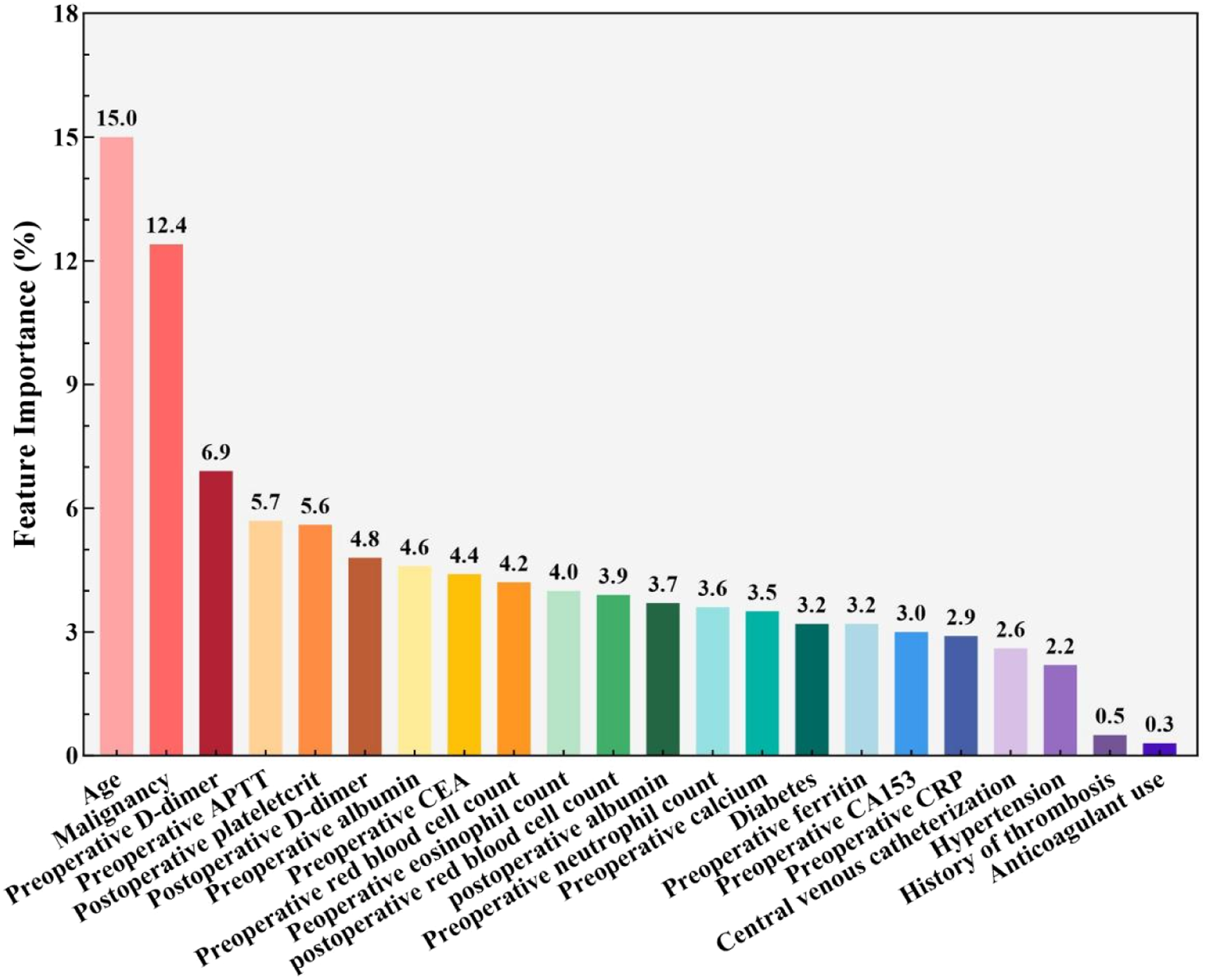
Discussion
This exploratory study presents a machine learning framework for assessing the risk of VTE in patients undergoing gynecological surgery. Our preliminary Extratrees model utilized 22 clinically relevant predictors, which were identified by extensive univariate analyses, and achieved an AUC of 0.907, exceeding the Caprini score (with an AUC ranging from 0.660 to 0.803 in similar populations) by more than 15%.
This significant improvement was attributed to our Extratrees model, with the distinctive ability to integrate multi-dimensional data specific to gynecology, such as patient demographics (age 15 ), existing health conditions (previous thrombosis, 16 hypertension, 17 diabetes 18 ), procedural factors (the use of central venous catheters 16 ), cancer status, 19 and importantly, evolving laboratory indicators covering preoperative inflammatory markers (such as leukocytosis and neutrophilia, 20 CRP 21 ) as well as perioperative coagulation variations (including preoperative APTT, 22 both pre- and postoperative D-dimer levels, 23 and changes in postoperative plateletcrit 24 ). Notably, the model incorporated biomarkers that have been largely ignored in the assessment of surgical risk, such as preoperative eosinopenia 25 ; this biomarker was indicative of a corticosteroid stress response that was linked to reduced fibrinolysis. Another biomarker that has been overlooked is hypocalcemia, which enhances platelet aggregation via exposure to calcium-dependent phosphatidylserine. 26 By elucidating these specific interactions, our preliminary algorithm addressed the significant shortcomings of current assessment scores.
The biological relevance of these predictors confirmed their clinical applicability. Preoperative hypoalbuminemia significantly increases the risk of VTE via several mechanisms: the reduced production of natural anticoagulants (such as antithrombin III and protein C), enhanced plasma viscosity and the endothelial dysfunction resulting from oxidative stress. 27 The association between hypoalbuminemia and VTE likely involves various factors. First, albumin exerts anticoagulant characteristics by binding to arachidonic acid, which in turn restricts its conversion into pro-aggregatory agents (including endoperoxides and thromboxane A2) and reduces both platelet activation and aggregation. 28 Second, the concentration of albumin can stimulate inducible nitric oxide synthase in macrophages in a dose-dependent manner, leading to increased synthesis of the powerful platelet inhibitor, nitric oxide. 29 Third, hypoalbuminemia can indicate the presence of underlying comorbidities (such as nephrotic syndrome, chronic kidney disease, and malignancy) that can independently increase the risk of VTE. 30 Finally, as a negative acute-phase reactant, hypoalbuminemia may serve as a marker of systemic inflammation, a recognized pathophysiological contributor to thrombosis. 31
Profiles of cancer antigens (such as elevated CA153
32
or CEA
33
with suppressed ferritin
34
) are known to indicate the biological characteristics of mucin-secreting adenocarcinoma, in which tissue factors derived from tumors directly activate Factor Xa. Mucins interact with P-selectin to facilitate the formation of platelet microthrombi. Increased levels of preoperative D-dimer are known to be associated with a greater risk of VTE following surgery for gynecological cancer.
35
The prediction of postoperative D-dimer levels is not reliable. Our current investigation revealed an AUC ranging from 0.585 to 0.697 (as shown in Figure 4); previous research also indicated that postoperative D-dimer levels are ineffective for the prediction of VTE, serving better as a rule-out test.
36
Following surgery, the fact that D-dimer did not decrease by more than 50% within 72 hours, which has been recognized as the most significant predictor, reflected ongoing fibrinolytic imbalance, typically appearing 48 hours before symptomatic events.
23
These mechanisms explained why conventional models do not perform well in populations of patients with gynecological cancer. Caprini’s straightforward point system failed to account for the combined risk presented by concurrent neutrophilia and anemia, which increased thrombotic risk by enhancing the formation of neutrophil extracellular traps and the expression of adhesion molecules on erythrocytes.
37
Receiver Operating Characteristic (ROC) Curves of Postoperative D-dimer for Predicting Postoperative venous thromboembolism in Gynecological Surgery. Abbreviations: AUC, area under the ROC curve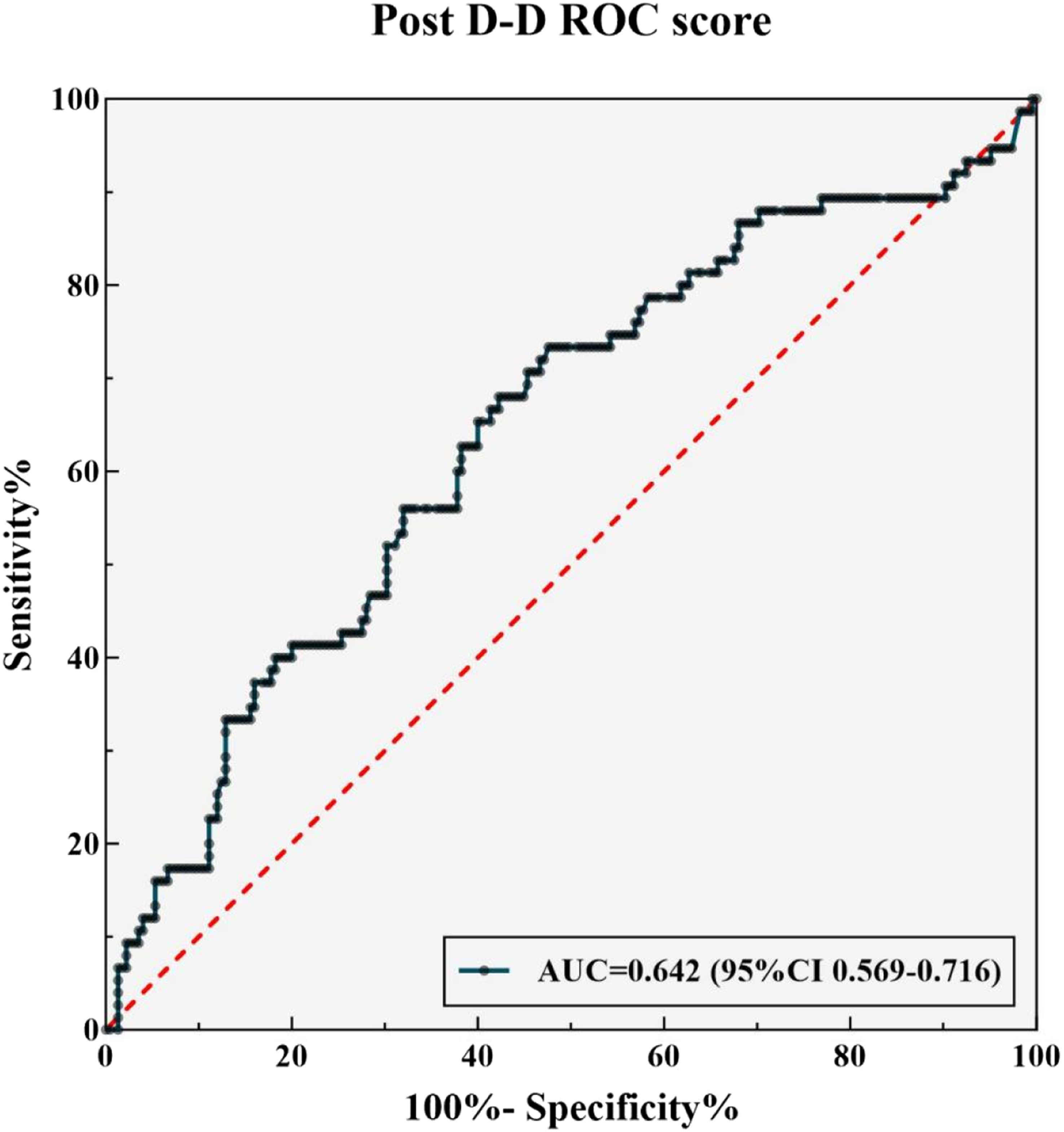
From a methodological standpoint, the dual randomization framework employed in the Extratrees model proved crucial for navigating the intricate nature of gynecological perioperative data. Our new model may transform in-hospital VTE prediction by effectively capturing hyper-acute biological cascades that may be overlooked by typical risk assessment tools. By randomly selecting the features for splitting and their corresponding thresholds during the construction of trees, our algorithm successfully reduced the risk of overfitting, even with a high number of predictor variables (n=22), while preserving strong discriminative capabilities across internal validation samples (AUC range: 0.833–0.972). The quantification of variable importance highlighted a clinically significant hierarchy, predominantly influenced by age (15.0%) and malignancy status (12.4%), which collectively represented more than a quarter of the overall predictive strength. In addition, hematological and biochemical markers made notable contributions; preoperative D-dimer (6.9%) and activated partial thromboplastin time (APTT, 5.7%) worked in conjunction with postoperative plateletcrit (5.6%) and preoperative albumin (4.6%), serving as key indicators of coagulation. Importantly, the computational design of our model was the best in interpreting nonlinear relationships among cellular factors such as preoperative eosinophil counts (4.0%) and evolving erythrocyte changes (preoperative 4.2%, postoperative 3.9%). This adaptability may allow for the incorporation of changing postoperative biomarkers, contrasting with traditional models that typically depend solely on static preoperative data. The recursive partitioning approach, which managed biological changes from pre-to postoperative phases within a cohesive framework (validated by non-linear interaction principles 38 ), signified a major step forward in precision risk evaluation, as it translated the complexities of perioperative pathophysiology into practical clinical predictions.
Several limitations should be acknowledged. The relatively small sample size (300 patients, 75 events) and 22 predictors raise a risk of overfitting. External validation in larger, independent cohorts is required before clinical application. Additionally, the model relies on high-quality laboratory data, limiting implementation in resource-constrained settings; its “black-box” nature without SHAP visualization may hinder clinical trust; the predominantly East Asian sample limits generalizability to other ethnic groups; temporal validation is needed as surgical techniques evolve; and psychosocial factors (e.g., depression-related inactivity) and health literacy were not considered. Future work should integrate point-of-care tools, explainable AI, and social determinants alongside external validation.
Conclusion
In this exploratory study, we developed and internally evaluated an ExtraTrees classifier model that incorporates gynecology-specific multi-dimensional data to predict postoperative VTE. This preliminary model demonstrated better discriminative ability than the Caprini risk score (AUC 0.907 vs. 0.731). The integration of biomarkers suggests potential for dynamic risk assessment, but this finding is hypothesis-generating. Further prospective and external validation studies are needed before considering any clinical application. This machine learning approach may, after rigorous validation, eventually contribute to personalized VTE prophylaxis in gynecological surgery, but current results should be interpreted as exploratory.
Declaration
Footnotes
Ethical Considerations
No animal studies are presented in this manuscript. Approval for the study protocol was granted by the Ethics Committee at Ningbo NO.2 Hospital (Ethics number: PJ-NBEY-KY-2025-056-01)
Consent to Participate
The consent to participate was waived by the Institutional Review Board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the Declaration of Helsinki.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Yingsha Yao, Huizhen Lin, Chuhan Wang, Danli Ma and Yanhong Fu. The first draft of the manuscript was written by Yingsha Yao, Huizhen Lin and Ting Wang. All authors read and approved the final manuscript. Ruan Jiang and Huimin Yu contributed to the study as supervision and critical revision of the manuscript for important intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author. Requests to access these datasets should be directed to Ruoan Jiang,