
Abstract
Background and Purpose
Current AHA and ACC guidelines warrant studies comparing direct oral anticoagulant (DOAC) and warfarin for post-myocardial infarction (MI) left ventricular thrombus (LVT). DOAC is increasingly considered due to its minimal monitoring requirement. However, DOAC efficacy in LVT resolution remains uncertain. We aim to evaluate the efficacy and safety of DOAC versus warfarin in post-MI LVT.
Methods
We searched Medline/PubMed, Scopus, Web of Science, and Cochrane. Library databases from inception up to August 2025. The primary outcome was LVT resolution. Secondary outcomes included all-cause death, stroke, and major bleeding rates.
Results
Four RCTs encompassing 396 patients (240 DOAC, 156 warfarin) were included. LVT resolution occurred in 90.0% of DOAC patients versus 86.5% in warfarin patients, with no significant difference (RR 0.99, 95% CI 0.94-1.06, p=0.84). Subgroup analysis revealed comparable outcomes for both rivaroxaban and apixaban versus warfarin. Stroke rates were higher in DOAC compared to warfarin but not statically significant between groups (2.5% vs 1.2%, RR 1.37, 95% CI 0.15-12.95). Similarly, all-cause mortality (3.3% vs 1.9%) and major bleeding (1.6% vs 1.9%) showed no significant differences.
Conclusion
DOACs demonstrate comparable efficacy and safety to warfarin for post-MI LVT management, with similar rates of thrombus resolution and complications. However, TSA indicates that current evidence is underpowered, and further large-scale randomized trials are required to confirm these findings.

Keywords
1. Introduction
Several studies showed an overall LVT incidence is about 2.7–6% in unselected patients, increases to roughly 10–13% in anterior STEMI with cardiac magnetic resonance (CMR) imaging showing LVT rates as high as one in five in those with anterior STEMI and reduced ejection fraction.1-4 LVT is associated with greater embolic risks in the first weeks, before reverse remodeling and thrombus organization occur. 5 If left untreated, LVT is linked to a four-fold higher risk of stroke or systemic embolism and a two-fold increase in long-term mortality. 6 Warranting the need for prompt initiation of anticoagulation and follow-up imaging during the first months to reassess the thrombus.
Management of LVT remains variable in practice, reflecting the balance between preventing embolism and minimizing bleeding risk, particularly in patients requiring dual antiplatelet therapy after PCI. 2 Warfarin is the standard first-line treatment and remains FDA-approved for this indication. When maintained within the therapeutic INR range, it effectively reduces thromboembolic events. However, its use is limited by the need for frequent INR monitoring, delayed onset of action, and numerous drug and food interactions. 7
Given these limitations, attention has increasingly turned toward direct oral anticoagulants (DOACs), particularly factor Xa inhibitors. These agents offer predictable anticoagulation, avoid the burden of routine monitoring, and carry fewer drug–food interactions, factors that have fueled their growing off-label use in LVT. 4 Importantly, several randomized controlled trials show that DOACs such as apixaban and rivaroxaban are non-inferior to warfarin for thrombus resolution, while maintaining comparable safety profiles.8-11
Current guidelines, including the 2025 American Heart Association (AHA) and 2023 European Society of Cardiology (ESC) statements, recognize DOACs as a reasonable alternative to Vitamin K Antagonists (VKAs) for LVT. However, they also emphasize that strong evidence specifically from randomized trials remains limited. This meta-analysis of RCTs aims to provide the necessary evidentiary support for these clinical recommendations.5,12 To fill this gap, we performed a meta-analysis of RCTs comparing DOACs and warfarin in post-MI LVT, evaluating thrombus resolution, embolic events, mortality, and bleeding to provide clearer guidance for clinical practice.
2. Methods
Our study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines and the Cochrane Handbook of Systematic Reviews and Meta-analysis of Interventions guidelines. It was registered with PROSPERO CRD420251180201.
2.1. Eligibility Criteria and Outcome
We included randomized controlled trial design (RCTs) addressing adult patients with LVT following MI treated in two different antithrombotic regimen arms with DOAC as the intervention group and warfarin as the control group. We excluded animal studies, conference abstracts, editorials, and case reports.
The selection process resulted in the exclusion of two randomized trials due to population heterogeneity. The No-LVT trial was excluded as 21.5% of its cohort had non-ischemic cardiomyopathy. 13 Similarly, the pilot study by Isa et al was excluded because it enrolled a mixed population of heart failure patients (including non-ischemic dilated cardiomyopathy) rather than focusing strictly on post-MI LVT. 14 To ensure the reliability of our findings for the post-MI population, only RCTs restricted to this clinical setting were included.
2.2. Literature Search and Screening
We conducted an electronic search on Scopus, PubMed, Web of Science, and Cochrane Central from conception to Aug 8th, 2025, using the following search strategy: (DOAC OR rivaroxaban OR apixaban) AND (warfarin) AND (LVT OR “left ventricular thrombus”) AND (Myocardial infarction). Supplemental Table 1 shows the full Boolean operators search strategy for each database.
Fifty-nine duplicates were removed using EndNote version 21.2 (Clarivate, Philadelphia, PA, USA). The results were then exported to Rayyan, 15 and the screening was carried out independently by two authors. The first was a title and abstract screening, followed by a full-text screening of the relevant studies. Any disagreements were settled through discussion and by consulting a senior author. Finally, all included studies were retrieved manually for additional studies.
2.3. Data Extraction
Two authors independently extracted the summary and baseline characteristics from the eligible studies trial registration and center, number (%), dosage and route of heparin bridging with INR target, dual antiplatelet therapy (DAPT) regimen dosage and route, duration of follow-up (months), country, target population with LVT, inclusion and exclusion criteria, and conclusion. While the baseline variable was patients’ age in years, gender, current smokers, left ventricular ejection fraction, comorbidities such as hypertension, diabetes mellitus, prior ischemic heart disease, and previous coronary revascularization, and thrombus size in length and width. Outcomes were obtained using an intention-to-treat approach. The primary outcome was LVT resolution, which has a detailed definition from each study as provided in Supplemental Table 2. The secondary outcomes were major adverse cardiovascular events (MACE), all-cause death, stroke, and major bleeding. The primary outcomes and secondary outcomes were assessed at the end of follow-up.
2.4. Risk of Bias and Certainty of Evidence
Two authors conducted an independent quality assessment of the included studies using the Cochrane Risk of Bias 2 (ROB2) tool. 16 Using five domains, studies are classified as low risk, some concerns, or high risk of bias: 1) bias due to the randomization process, 2 deviation from intended intervention, 3 missing outcome data, 4 measurement of outcomes, 5 selection of the reported result, and “overall risk of bias” judgment. Any discrepancies between authors were resolved through discussion with the senior author.
We assessed the certainty of evidence for each critical outcome using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach (-), evaluating five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Because all included studies were RCTs, the certainty of evidence initially started as high and was downgraded by one or two levels when we identified serious or very serious limitations in any domain. Summary of Findings tables and the rationale for each judgment were prepared using the online GRADEpro GDT software.
2.5. Statistical Analysis
Categorical variables are expressed as the number of events and the total number of participants in each group and pooled as risk ratio (RR) or odds ratio (OR) for rare events, and with their respective 95% confidence intervals (CIs) using the Restricted maximum likelihood (REML) random-effects model. The results were considered significant if the P-value was less than 0.05. The chi-square test (Cochran’s Q test) was used to evaluate statistical heterogeneity among the included studies. Results were considered significantly diverse if the p-value was < 0.1 or I2 > 50%. Additionally, for our primary outcome, we conducted a subgroup analysis based on the type of DOAC used. We conducted a sensitivity analysis using the leave-one-out method to test the stability of the effect size and its direction by removing one study at a time.
Finally, as the cumulative pooling of trials and the limited data increase the risk of type 1 and 2 errors, we performed a trial sequential analysis (TSA) to assess whether the evidence generated from the analysis was reliable and conclusive.
The confidence level is conclusive and sufficient, indicating no other studies are needed, when the z-line of the TSA curve crosses both the conventional and sequence-monitoring boundaries. On the other hand, if the z-line does not cross any boundary on the curve, the evidence is inconclusive, and further trials are still required. In this meta-analysis, we used an alpha error of 0.05, a beta error of 80% power, and a risk reduction of 10% as recommended. 17 For all statistical analyses, we used R version 4.4.0 and R Studio version 2024.04.1 (Build 748, RStudio, Inc.).
3. Results
3.1. Characteristics of Included Studies and Population
We included 4 RCTs,9,18-20 in which DOAC was compared to warfarin. The selection process of the studies was demonstrated in detail in the PRISMA (Figure 1). Prisma flow diagram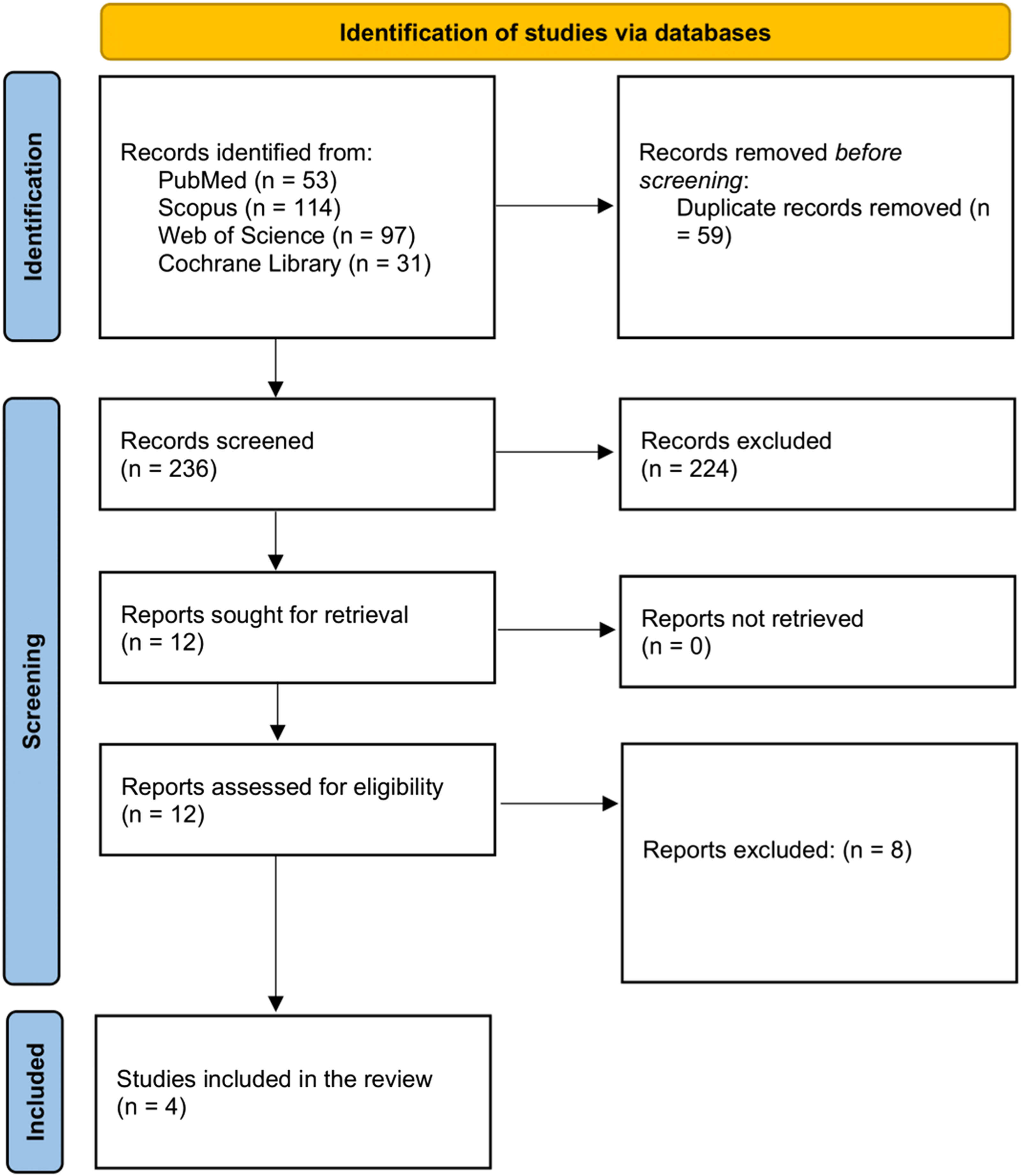
All studies enrolled 396 patients: 240 who used DOAC and 140 who used warfarin, with a mean age of 54.5±10.2 years. The mean of follow-up was 3.7 months. Regarding the DOAC used, REWARF-STEMI(21) and RIVAWAR(20) trials used rivaroxaban (15mg and 20mg, respectively), while Youssef et al. 9 and Alcalai et al 20 used apixaban (5mg and 2.5mg, respectively).
Baseline Characteristics of Included Randomized Controlled Trials
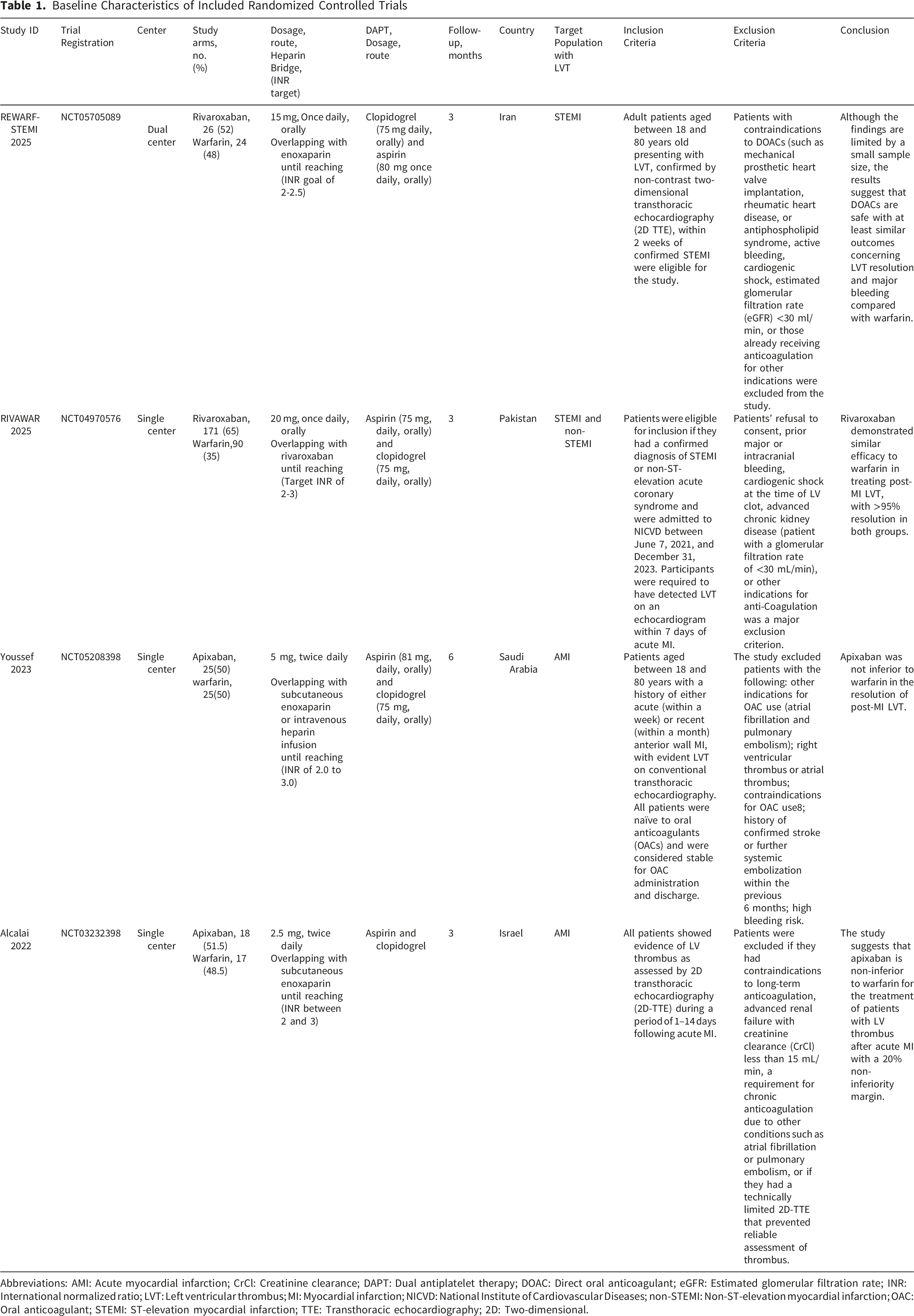
Abbreviations: AMI: Acute myocardial infarction; CrCl: Creatinine clearance; DAPT: Dual antiplatelet therapy; DOAC: Direct oral anticoagulant; eGFR: Estimated glomerular filtration rate; INR: International normalized ratio; LVT: Left ventricular thrombus; MI: Myocardial infarction; NICVD: National Institute of Cardiovascular Diseases; non-STEMI: Non-ST-elevation myocardial infarction; OAC: Oral anticoagulant; STEMI: ST-elevation myocardial infarction; TTE: Transthoracic echocardiography; 2D: Two-dimensional.
Regarding bridging therapy, all four trials required initial heparinization for the warfarin group. REWARF-STEMI 19 and Alcalai et al 20 utilized enoxaparin until an INR of 2.0-2.5 or 2.0-3.0 was reached, respectively. Youssef et al. 9 allowed for either subcutaneous enoxaparin or intravenous heparin infusion until reaching an INR of 2.0-3.0. In RIVAWAR, 18 bridging was continued until the target INR of 2.0-3.0 was achieved. These variations in background therapy were considered when evaluating the comparable safety outcomes observed between the DOAC and warfarin groups.
Summary of Included Randomized Controlled Trials
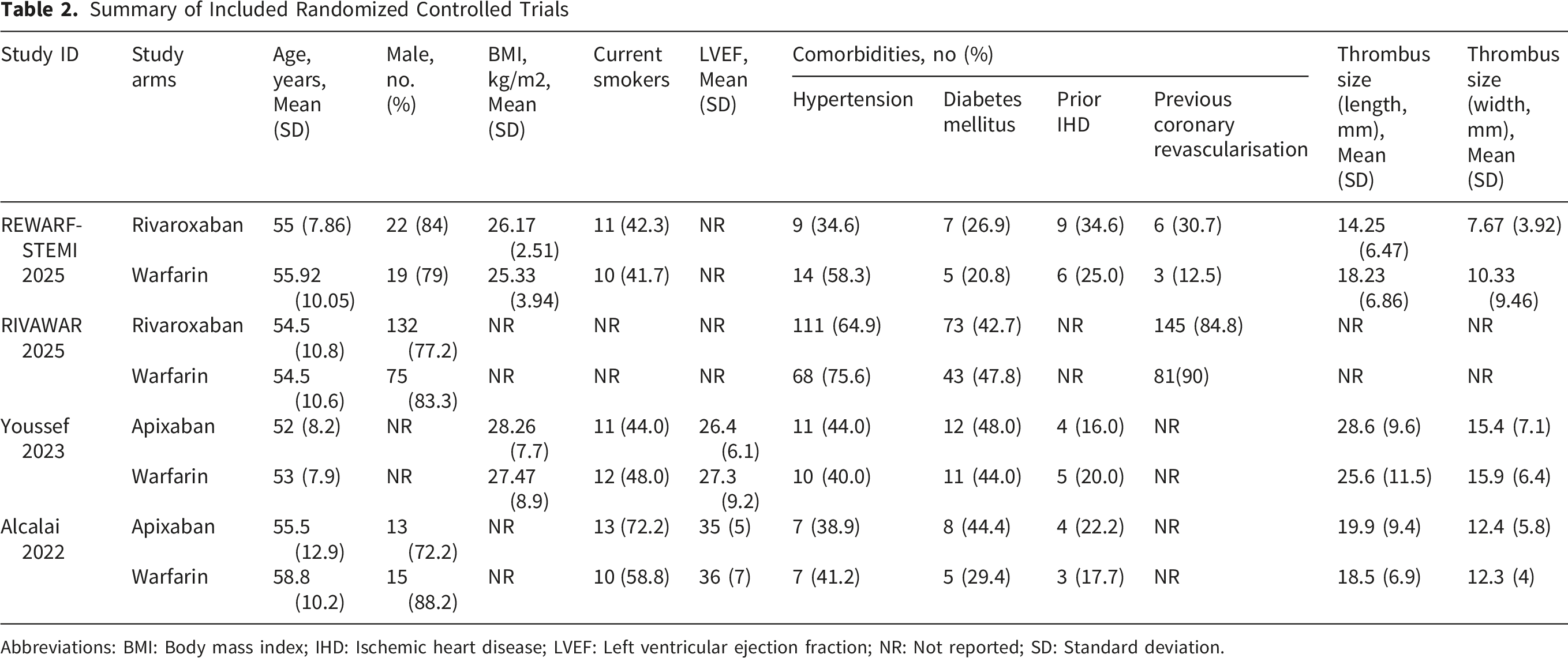
Abbreviations: BMI: Body mass index; IHD: Ischemic heart disease; LVEF: Left ventricular ejection fraction; NR: Not reported; SD: Standard deviation.
3.2. Risk of Bias Assessment
All studies demonstrated a low risk of bias based on the Cochrane Risk of Bias 2 (RoB 2). Figure S1 shows a summary and graph of the risk of bias in our studies.
3.3. Primary Outcome
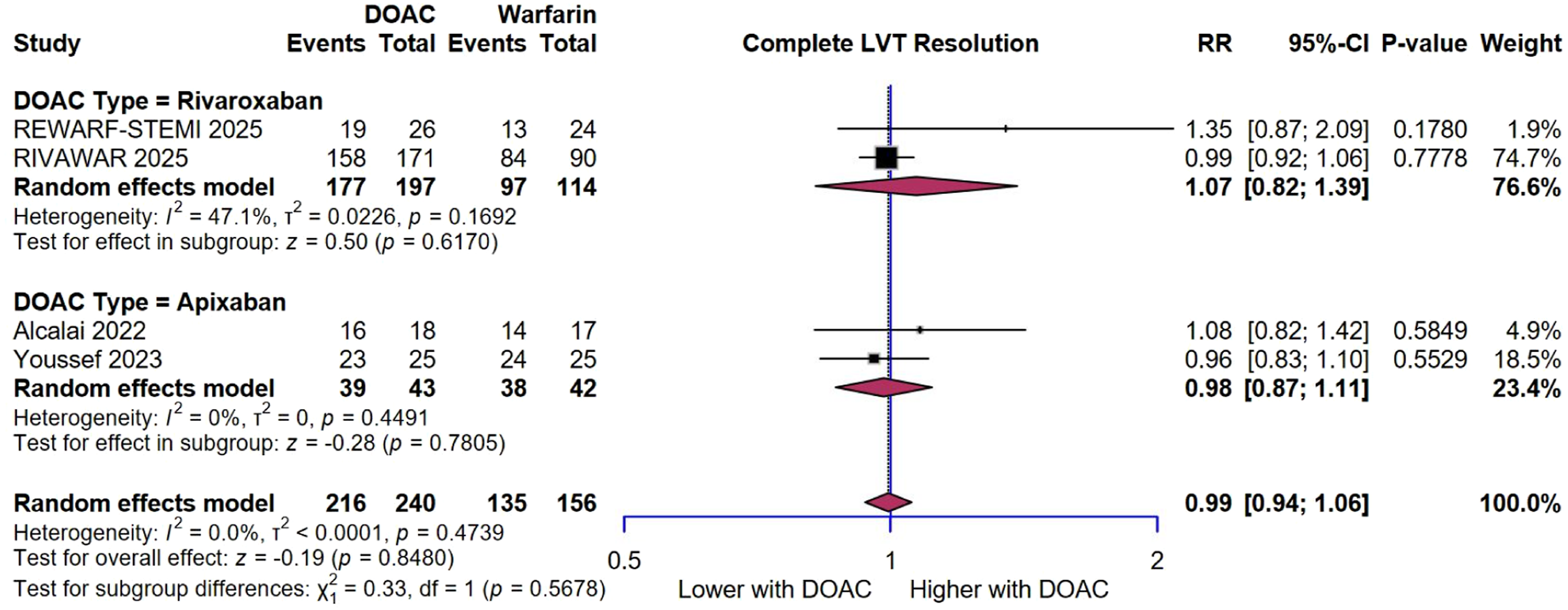
The LVT resolution rate was 90% (216 of 240) in the DOAC group, compared to 86.5% (135 of 156) in the warfarin group. The pooled estimate showed no significant difference between the DOAC group and the warfarin group regarding LVT resolution (RR = 0.99, 95% CI [0.94 – 1.06], p = 0.84; I2 = 0%, p = 0.47) (Figure 2). We performed leave-one-out sensitivity analysis, and no single study has a disproportional effect on the overall result (Figure S2). Additionally, when stratifying studies according to the DOAC used, both rivaroxaban and apixaban showed no comparable LVT resolution rates between the DOAC and warfarin groups (RR = 1.07, 95% CI [0.82 – 1.39], p = 0.61; I2 = 47.1%, p = 0.16) and (RR = 0.98, 95% CI [0.87 – 1.11], p = 0.78; I2 = 0%, p = 0.44), respectively (Figure 3). Forest plot for left ventricular thrombus resolution Subgroup analysis of left ventricular thrombus resolution by DOAC type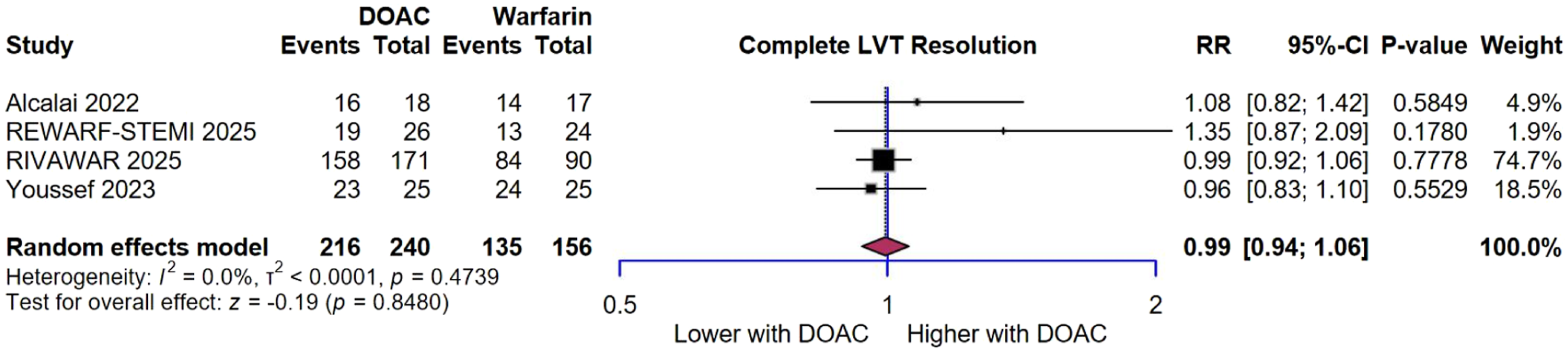
We conducted a TSA analysis evaluating the effect of DOAC and warfarin on LVT resolution, as demonstrated in Figure 4; the cumulative Z-curve did not cross the conventional boundary or the trial sequential monitoring boundary for benefit, suggesting that it did not favor DOAC over warfarin. However, as the required information size was not reached, the analysis remains underpowered to definitively confirm the absence of a treatment effect. Trial sequential analysis for left ventricular thrombus resolution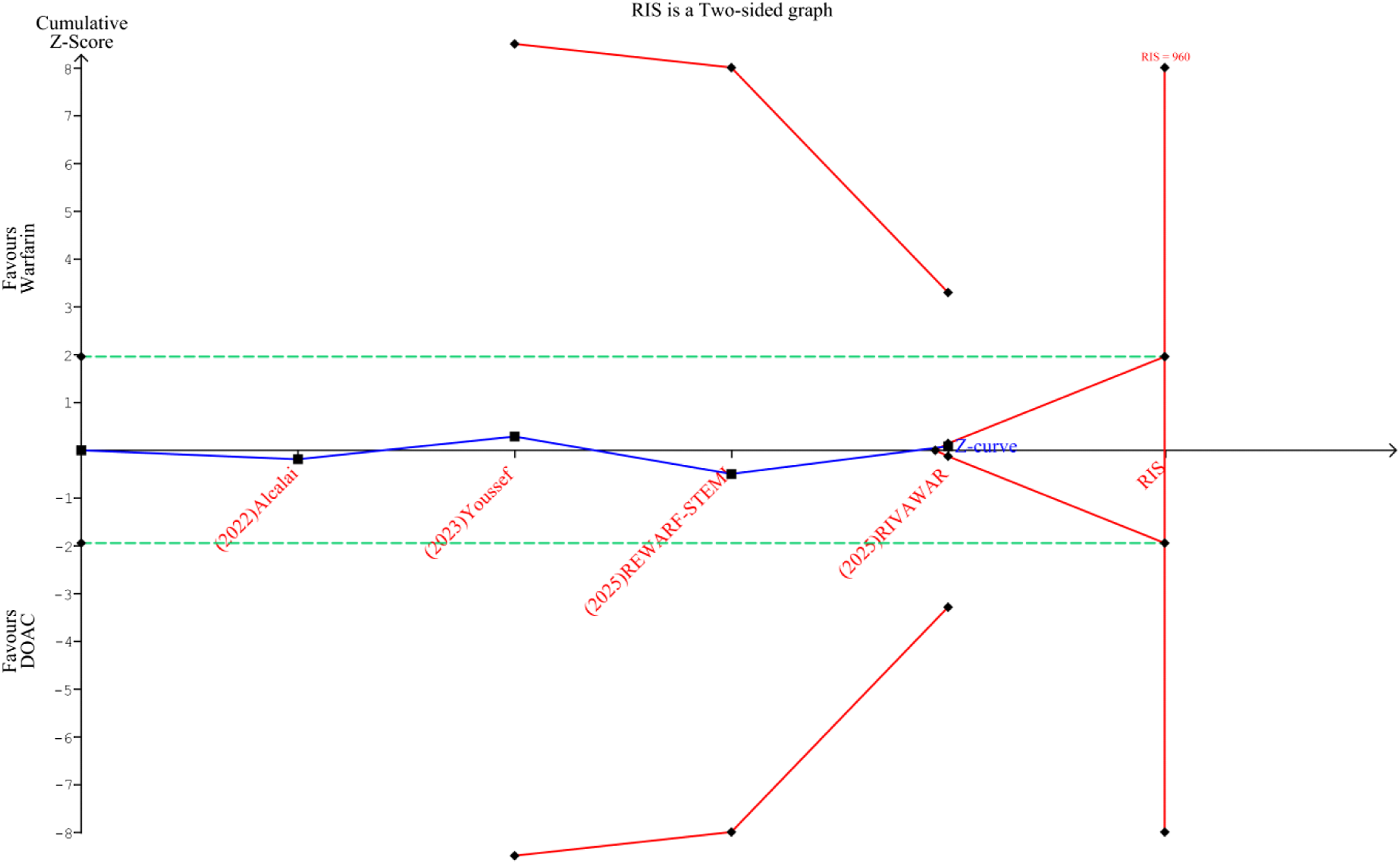
3.4. Secondary Outcomes
Four RCTs reported stroke rates, encompassing 396 patients. The event rate was 2.5%
(6 of 240) in the DOAC group, compared to 1.2% (2 of 156) in the warfarin group. The pooled estimate showed no significant difference between the DOAC group and the warfarin group regarding stroke (OR = 1.37, 95% CI [0.15 – 12.95], p = 0.783; I2 = 30.4%, p = 0.23) (Figure 5A). Similarly, all-cause death rate was 3.3% (8 of 240) in the DOAC group, compared to 1.9% (3 of 156) in the warfarin group, with no significant difference between the two groups (OR = 1.39, 95% CI [0.42 – 4.64], p = 0.58; I2 = 0%, p = 0.75) (Figure 5B). Forest plots for secondary outcomes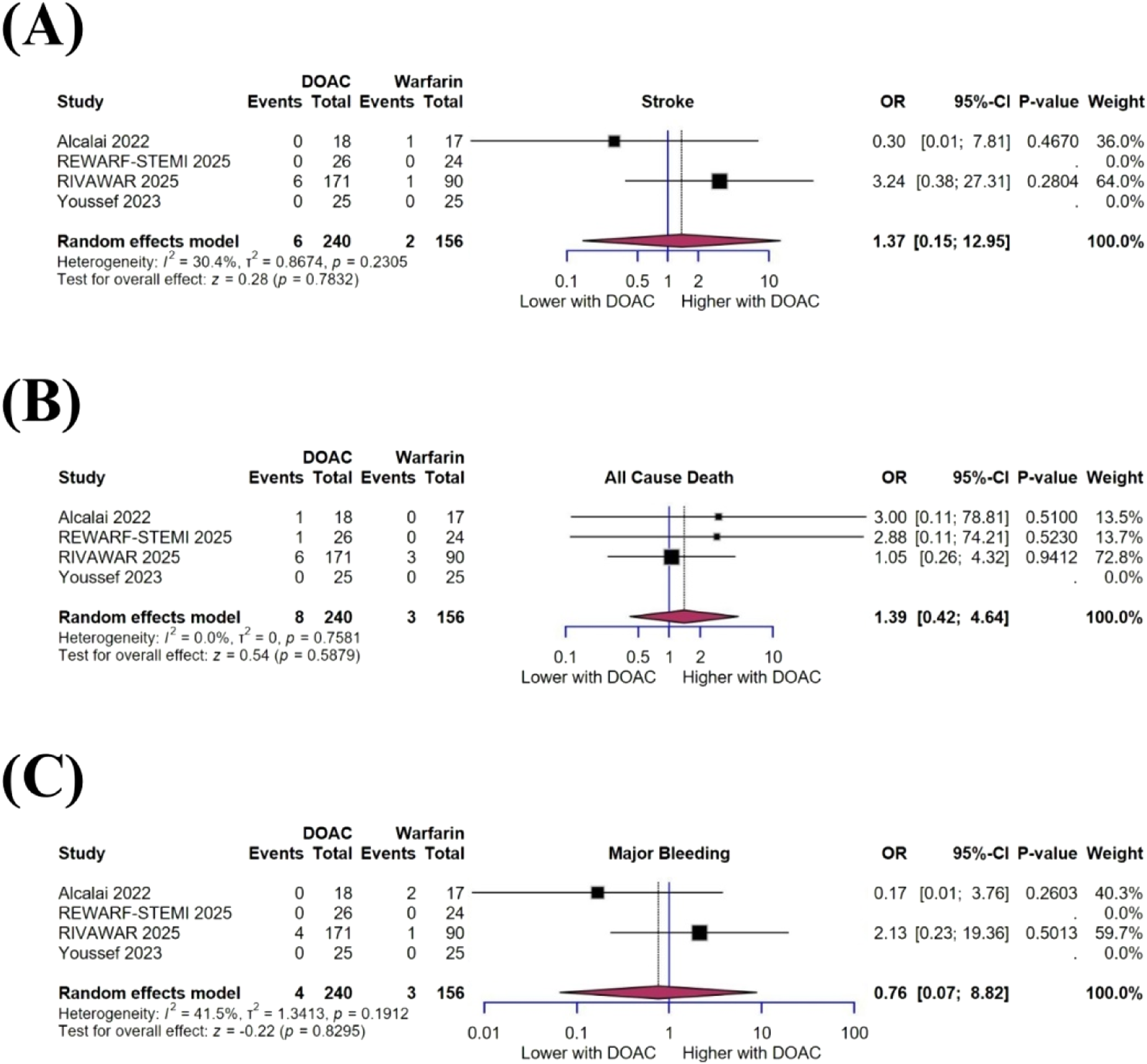
Finally, major bleeding rates was 1.6% (4 of 240) in the DOAC group, compared to 1.9% (3 of 156) in the warfarin with no significant difference between the two groups (OR = 0.76, 95% CI [0.07– 8.82], p = 0.82; I2 = 41.5%, p = 0.19) (Figure 5C).
3.5. Certainty of Evidence
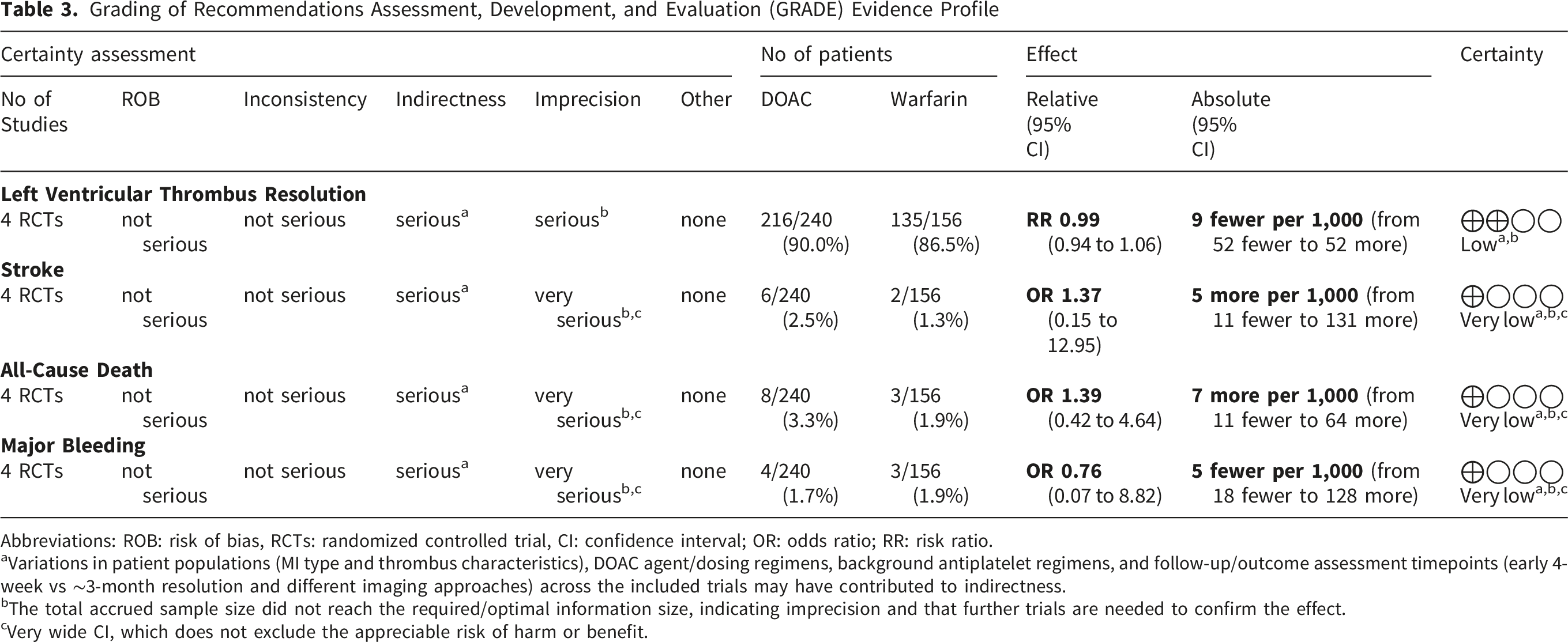
Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Evidence Profile
Abbreviations: ROB: risk of bias, RCTs: randomized controlled trial, CI: confidence interval; OR: odds ratio; RR: risk ratio.
aVariations in patient populations (MI type and thrombus characteristics), DOAC agent/dosing regimens, background antiplatelet regimens, and follow-up/outcome assessment timepoints (early 4-week vs ∼3-month resolution and different imaging approaches) across the included trials may have contributed to indirectness.
bThe total accrued sample size did not reach the required/optimal information size, indicating imprecision and that further trials are needed to confirm the effect.
cVery wide CI, which does not exclude the appreciable risk of harm or benefit.
4. Discussion
This meta-analysis tested the hypothesis that DOACs provide similar outcomes to warfarin for managing LVT. Across four randomized controlled trials enrolling 396 patients, thrombus resolution was achieved in approximately 90% of those treated with DOACs, a rate slightly higher yet broadly comparable to the 87% observed with warfarin. Importantly, stroke events were uncommon in both groups, affecting only 2–3% of patients receiving DOACs and about 1% of those on warfarin, with no significant difference between arms. Mortality followed a similarly low pattern, occurring in 3% of patients treated with DOACs compared with 2% in the warfarin group. Finally, major bleeding events were rare, observed in fewer than 2% of patients in each arm, and occurred at nearly identical rates with both anticoagulant strategies.
Post-MI LVT develops when all components of Virchow’s triad act hand in hand within the infarcted ventricle. Following Endocardial injury from transmural necrosis exposes collagen and tissue factor, accelerating platelet adhesion and thrombin generation, especially in large anterior or apical infarcts, where the surface is highly thrombogenic.4,21 As the necrotic region loses contractility, regional stasis from severe wall-motion abnormalities such as apical akinesis, dyskinesis, or aneurysm creates low-shear zones that promote fibrin-rich clot formation, explaining the association between reduced ejection fraction, anterior location, and LVT in imaging studies.1,4 In addition, a transient pro-coagulant state after MI, driven by inflammation, increased fibrinogen, and platelet hyperactivity, enhances thrombus formation during the early post-infarct period. 4 These processes are compounded by reperfusion-related microvascular obstruction and intramyocardial hemorrhage, which sustain local stasis, extend tissue injury, and are consistently linked with larger infarcts, adverse ventricular remodeling, and higher LVT risk.22,23 According to current AHA/ACC guidelines, patients with LVT are routinely treated with oral anticoagulation in clinical practice. 5 The duration of therapy depends on follow-up imaging, and DOACs are now more accepted as an alternative to vitamin K antagonists. For patients who develop LVT after MI, the 2025 American Heart Association scientific statement suggests about 3 months of anticoagulation, followed by repeat imaging to confirm that the clot has resolved. In these cases, DOACs may be used instead of warfarin if drug interactions and bleeding risks are carefully considered. 5 The European Society of Cardiology (2017 STEMI guideline, updated in the 2023 ACS guideline) recommends at least 6 months of anticoagulation, with repeat imaging to weigh the benefits against bleeding risk. 24 On the other hand, giving anticoagulation to prevent clots after a large anterior MI without a documented thrombus is not routinely advised, though in certain high-risk patients, a shorter course of 1–3 months may be considered. 5
Interestingly, our pooled analysis showed that DOACs achieved similarly high rates of complete LVT resolution compared with warfarin at about 3 months (90.0% vs 86.5%), with no meaningful difference between groups (RR 0.99, 95% CI 0.94–1.06; I2 = 0%). These results are in line with those of REWARF-STEMI trial, which observed that complete LVT resolution was achieved in approximately 81% of patients treated with DOACs compared with about 71% in those receiving VKAs, corresponding to a relative risk of 1.14 (95% CI 0.98–1.32), a difference that was not statistically significant but pointed toward a favorable trend. 19 Consistently, Chi et al in their meta-analysis reported no significant difference in resolution. 25 At the individual-trial level, Mansouri et al demonstrated rivaroxaban to be non-inferior to warfarin with similar reductions in thrombus size and no excess risk, while RIVAWAR trial reported >95% resolution in both arms of a contemporary post-MI RCT. 11 This effect can be understood through the action of factor Xa inhibition. By blocking thrombin generation, apixaban and rivaroxaban produce fibrin networks that are looser and more permeable, which makes it easier to break down and promote thrombus shrinkage. Gauer et al confirm that DOACs increase clot dissolution and shift fibrin structure toward thicker fibers with greater permeability. 26 More generally, reducing thrombin generation changes fibrin ultrastructure in ways that enhance susceptibility to lysis, linking the drug’s pharmacology to the neutral or favorable resolution outcomes observed in clinical trials. 27
Just as with thrombus resolution, ischemic outcomes in our pooled analysis were infrequent and showed no meaningful differences between DOACs and VKAs, consistent with findings from the REWARF-STEMI trial and Chi et al19,25 While the RIVAWAR trial reported >95% resolution in both groups without excess embolic events, and Alcalai et al confirmed apixaban’s non-inferiority to warfarin 8 and 10. In contrast, a few studies suggest a modest advantage for DOACs, with Hu et al and Vorla et al reporting fewer stroke/TIA events.28,29 The risk of embolism from LVT is greatest early, when stasis, endocardial injury, and a prothrombotic state overlap after MI. Anticoagulation with either DOACs or VKAs reduces thrombin generation, prevents thrombus growth, and stabilizes friable components, which explains the low event rates and lack of difference between drugs in short-term RCTs. That is why current AHA guidance recommends about 3 months of oral anticoagulation for post-MI LVT 5
Perhaps most reassuring for clinicians and patients alike, survival outcomes were similar regardless of whether DOACs or warfarin were used. Mortality was low and not different between the two groups in our analysis, consistent with the Chi et al and the randomised synthesis by REWARF-STEMI trial with short-term follow-up. Some broader meta-analyses across all study designs suggest numerically lower mortality with DOACs, possibly due to fewer severe intracranial bleeds and less over-anticoagulation, though results vary by study type and duration.28,29 This pattern may be explained by the fact that early deaths after MI-associated LVT are mainly determined by infarct size, heart failure, and arrhythmias, factors that anticoagulant choice cannot directly change. As a result, short-term mortality differences are minimal. Where differences do appear in larger datasets, they often reflect DOACs’ link to smaller intracranial hemorrhage volumes and lower ICH-related mortality compared with VKAs.30,31
One of the most debated concerns in anticoagulant therapy, major bleeding, proved far less dramatic in practice. Major bleeding was uncommon and similar between groups in our RCT-only analysis, consistent with the findings of Chi et al. Larger meta-analyses, however, often point to a safety advantage for DOACs, Vorla et al found significantly less overall bleeding, while Hu et al reported that DOACs provided non-inferior efficacy with superior safety compared with VKAs in LVT cohorts.28,29 Although LVT-specific studies include too few intracranial hemorrhage events for precise comparisons, broader anticoagulation data consistently demonstrate smaller hematomas and lower short-term mortality in DOAC-associated ICH than with VKAs.31,32
The necessity of concomitant antiplatelet therapy after primary PCI complicates LVT management. While our analysis showed no significant difference in major bleeding between DOACs and warfarin (OR 0.76; 95% CI 0.07–8.82), the choice of the specific P2Y12 inhibitor and the duration of triple therapy remain critical. The predictable pharmacokinetics of DOACs may offer a safer profile for long-term combination therapy compared to the INR variability associated with VKAs, though clinician vigilance regarding bleeding remains paramount in the early post-PCI period. 33 DOACs provide stable and targeted anticoagulation, with fewer food and drug interactions and no INR variability. Unlike VKAs, they do not deplete vitamin-K-dependent proteins important for vascular hemostasis, and by reducing thrombin amplification at the factor Xa level, they help account for the lower severity of ICH observed across indications without loss of thromboprophylaxis effect.34,35
When tested by DOAC type, the results tell a clear and consistent story, or the rivaroxaban showed no benefit over warfarin for LVT resolution (RR 1.07, 95% CI 0.82–1.39; p=0.62; I2=47%), and apixaban produced nearly identical findings (RR 0.98, 95% CI 0.87–1.11; p=0.78; I2=0%). These results are consistent with previous evidence where Youssef et al, demonstrated apixaban to be non-inferior to warfarin at three months, 9 while studies on rivaroxaban also showed similar outcomes at same period. 10 The absence of separation between rivaroxaban and apixaban suggests a class effect, as both agents inhibit activated factor Xa with comparable potency, making major differences in thrombus resolution unlikely, supports a shared effect of factor Xa inhibitors rather than molecule-specific differences. 36
4.1 Clinical Implications and Future Directions
This study confirms that DOACs work as well as warfarin in managing LVT. Their fixed dosing, minimal monitoring, and easier use improve patient comfort and adherence. Clinicians can rely on them as a safe and practical alternative that reduces hospital workload and follow-up needs, though cost and availability remain challenges.
4.2. Strengths
This study adds valuable information to an area where data have been limited, by comparing the effectiveness of DOACs and warfarin in treating left ventricular thrombus. A major strength is that only randomized controlled trials were included, which reduces bias and makes the results more reliable. The analysis also used sensitivity checks, showing that no single trial changed the overall outcome, which strengthens confidence in the findings. In addition, the similar results across important outcomes, LVT resolution, stroke, death, and major bleeding, give a clear and balanced picture of the safety and effectiveness of DOACs compared with warfarin. We also conducted a subgroup analysis by DOAC type, which adds further strength to the study. A key strength of this review is the use of a structured GRADE approach to transparently rate the certainty of evidence across outcomes.
5. Limitations
Nevertheless, some limitations warrant consideration. First, the overall sample size was modest, with fewer than 400 patients included, limiting the statistical power to detect small but clinically meaningful differences in rare outcomes such as stroke or major bleeding. Second, heterogeneity in trial design, patient characteristics, and follow-up duration may have introduced variability that cannot be fully accounted for, even with pooled analysis. Third, the limited reporting of subgroup data (e.g., type of underlying cardiomyopathy, concomitant therapies) restricts the generalization of findings across diverse clinical populations. Finally, the relatively short follow-up periods in some trials constrain the assessment of long-term efficacy and safety. Consistent with these limitations, the GRADE assessment rated the certainty of evidence as low for LVT resolution and very low for stroke, all-cause death, and major bleeding, reflecting concerns related to indirectness and substantial imprecision from sparse events and very wide CIs.
6. Conclusion
In summary, this meta-analysis of RCTs demonstrates that DOACs provide efficacy and safety similar to warfarin in managing LVT. Rates of thrombus resolution, ischemic events, mortality, and major bleeding were consistently comparable between groups, supporting the role of DOACs as a reliable alternative to VKAs. Given their ease of use, predictable dosing, and favorable patient adherence profile, DOACs represent a practical option in clinical practice, although larger and longer-term studies are still needed to confirm these findings and extend their applicability to broader patient populations.
Supplemental Material
Supplemental Material - DOACs vs Warfarin for Post-Myocardial Infarction Left Ventricular Thrombus: A GRADE-Assessed Meta-Analysis with Trial Sequential Analysis of Randomized Trials
Supplemental Material for DOACs vs Warfarin for Post-Myocardial Infarction Left Ventricular Thrombus: A GRADE-Assessed Meta-Analysis with Trial Sequential Analysis of Randomized Trials by Ahmed Elbataa, Ameer Awashra, Ahmed Elazab, Noha Hammad, Ahmed Mansour, Amro Ali, Mohamed Yasser Elnaggar, Elsayed Balbaa, Abdalhakim Shubietah, Mohamed S. Elgendy, Mohammed A. Elbahloul, Fawzi Zghyer, Mohammed Al-Sadawi and Amr Salama in Clinical and Applied Thrombosis/Hemostasis.
Footnotes
Author Contributions
A.E., N.H., A.M., A.A., M.Y.E., E.B., M.E., M.A.E., and A.S. contributed to conceptualization, data curation, formal analysis, investigation, methodology, and software. M.A.-S., F.Z., and A.Sa. were responsible for project administration, supervision, and validation. A.Eb. and A.Aw. prepared the original draft. All authors reviewed and approved the final manuscript. The authors declare that all data were generated in-house, that no paper mill was used and that no AI tool has been used for the generation of text or figures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
AI Use
The authors confirm that no artificial intelligence was used.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.