
Abstract
Introduction
Hemophilia A and B, which are characterized by the deficiency of blood clotting factors VIII and IX, progress with bleeding and related complications. In our study, we aimed to investigate the emotional state and appearance anxiety of these patients and the emotional state of their spouses who are responsible for their care.
Materyal method
We included 44 adult patients (age 18–57) with severe hemophilia A or B and 28 spouses. Psychological assessments were performed using the Beck Depression Inventory (BDI), Social Appearance Anxiety Scale (SAAS), and Oxford Happiness Questionnaire (OHQ). Cutoff values were applied: BDI >20 indicates depression; SAAS higher scores reflect greater anxiety; OHQ scores >140 indicate high happiness, 100–139 moderate, and <100 low happiness. Correlation analyses between annual bleeding frequency and psychological outcomes were conducted using Spearman’s rho.
Results
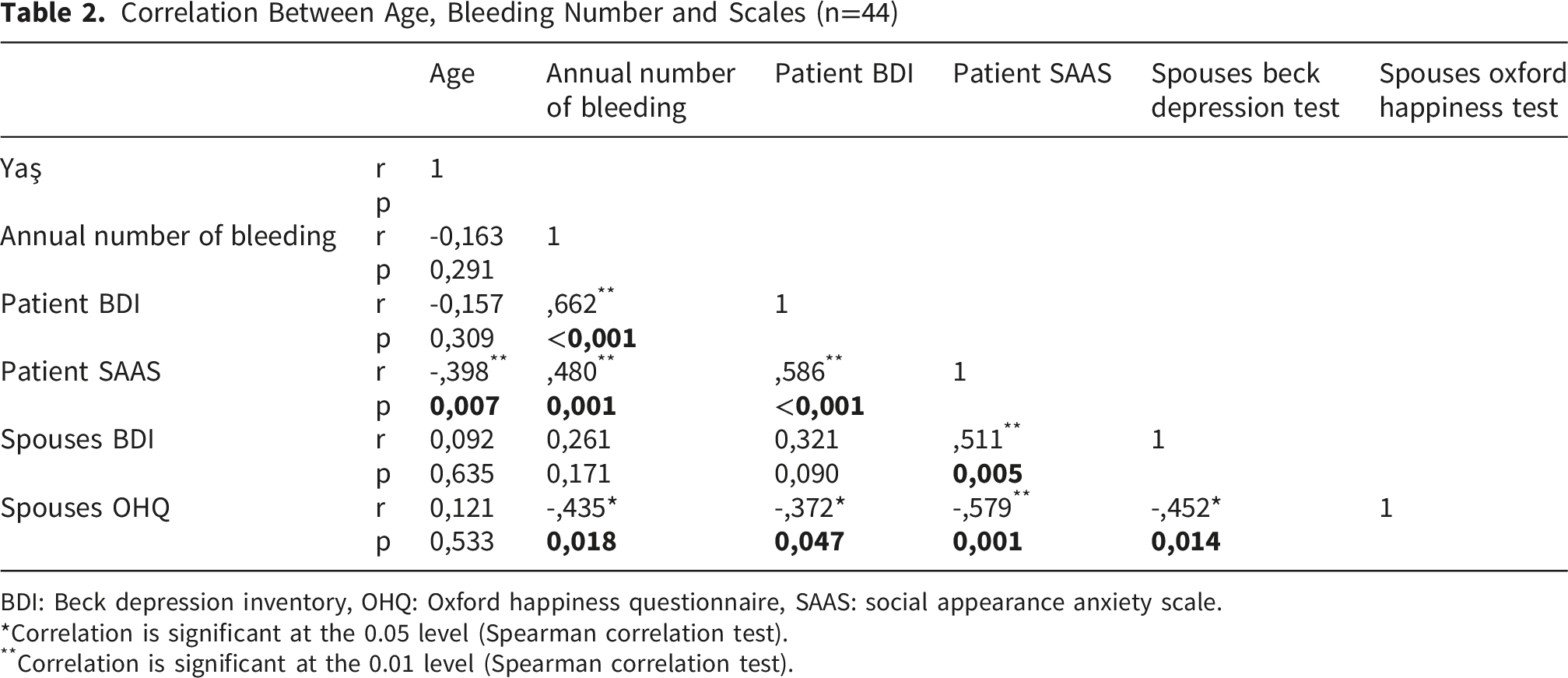
Patients had a mean BDI score of 23.7 (depression range), mean SAAS score of 42, and spouses had a mean BDI score of 21.6 (depression range) with OHQ mean of 120 (moderate happiness). Annual bleeding frequency was positively correlated with patient BDI (r=0.662, p<0.001) and SAAS (r=0.480, p=0.001), and negatively correlated with spouse OHQ (r=-0.435, p=0.018).
Discussion
Bleeding complications significantly affect patients’ emotional state and appearance anxiety, and in our cohort appearance anxiety was negatively correlated with age; however, subgroup analyses were not performed. Spouses also experience reduced happiness. These findings highlight hemophilia as a family-wide burden requiring integrated psychosocial support. Future longitudinal and interventional studies are needed to confirm these findings and guide comprehensive care models.

Introduction
Hemophilia A and B, resulting from deficiencies in coagulation factors VIII and IX, affect approximately 1 in 5,000 and 1 in 30,000 live births, respectively. 1 Musculoskeletal bleeding, particularly into joints, remains the predominant clinical manifestation and a major driver of long-term morbidity. Despite substantial therapeutic advances that have extended life expectancy to near-normal levels, the persistent burden of bleeding-related complications continues to compromise patients’ functional capacity and overall quality of life.2,3
Adults living with hemophilia continue to experience persistent functional limitations and perceived risks inherent to their chronic condition. The current standard of care—prophylactic or therapeutic replacement of factor VIII or IX—has markedly improved clinical outcomes, yet substantial challenges remain 4 . Patients frequently confront financial strain, emotional distress, physical disability, and social disruption. From early childhood onward, hemophilia exerts a pervasive influence on family dynamics, peer interactions, psychological development, and behavioral adjustment. Importantly, unless systematically addressed, these psychosocial dimensions are often neglected within routine clinical management.3-5
Enhancing quality of life in hemophilia necessitates a dual focus on physical health and psychological well-being. Consistent evidence indicates that individuals with hemophilia report significantly lower quality of life compared to the general population.6,7 Developmental transitions during puberty further shape autonomy, sexual relationships, and personality formation, amplifying vulnerability to psychosocial stressors. Concerns regarding body image and physical appearance, particularly in youth, may predispose patients with deformities to psychosomatic disorders, diminished self-esteem, academic challenges, depression, and heightened anxiety.8-10 Pain, a central clinical manifestation of bleeding disorders, demonstrates strong associations with depression, anxiety, and reduced health-related quality of life. Patients experiencing recurrent pain frequently report impaired physical functioning, elevated psychological distress, and weakened social connectedness.10,11 Moreover, anxiety and depression have been linked to increased hospitalization rates among individuals with hemophilia. 12
In adulthood, caregiving responsibilities are frequently assumed by partners, who themselves face considerable social pressures and heightened anxiety stemming from the demands of continuous care and recurrent hospitalizations.13,14 Although the association between hemophilia and depression has been extensively documented, investigations into social appearance anxiety among adult patients remain scarce. Existing research has predominantly focused on adolescents, leaving a critical gap in understanding the psychosocial burden in adult populations. Moreover, the emotional well-being and happiness of partners providing care for adult patients with hemophilia have not been systematically examined alongside patient outcomes. Accordingly, the present study seeks to evaluate depression, social appearance anxiety, and happiness in adult patients with hemophilia and their partners, and to analyze their relationship with bleeding episodes and related complications.
Materials and Methods
Subjects
This cross-sectional study was conducted between November 1, 2023, and February 1, 2024. A total of 44 adult patients with severe hemophilia A or B (factor activity <1%), aged 18–57 years, were consecutively enrolled from tertiary care centers. In addition, 28 spouses of patients who consented to participate were included. Spouses were included only if they were the partners of enrolled patients and consented to participate. Patients without a spouse or whose spouse did not agree to participate were excluded from the spouse cohort. The flow of patient and spouse inclusion is summarized in Figure 1, which depicts the parallel assessment and exclusion processes. All assessments were performed individually in standardized, private settings to ensure confidentiality and adequate time. Exclusion criteria comprised a history of psychiatric disorders, comorbidities, or medication use that could predispose to bleeding. Ethical approval was obtained from XXX University Clinical Research Ethics Committee (decision no: HRÜ/23.10.02), and all procedures complied with the Declaration of Helsinki. Flowchart of Patient and Spouse Inclusion Process - Flow diagram depicting participant inclusion. Of 69 individuals initially screened, 49 were diagnosed with severe hemophilia (factor activity <1%). Following exclusions, 44 patients and 28 spouses were assessed under standardized conditions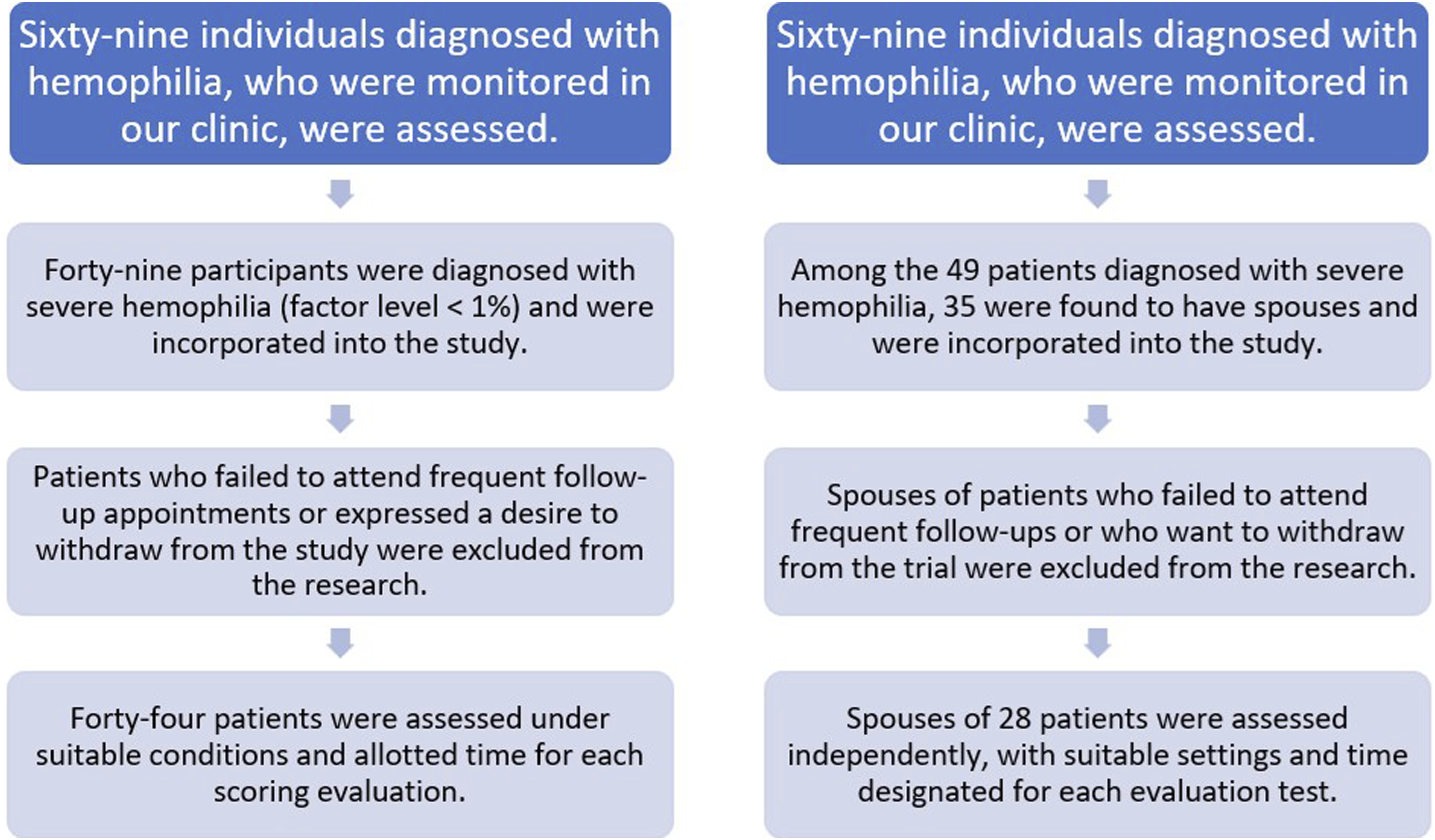
Measures
Psychological assessments were administered by a trained psychologist. Patients completed the Beck Depression Inventory (BDI) and the Social Appearance Anxiety Scale (SAAS), while spouses completed the Oxford Happiness Questionnaire (OHQ) and the BDI.
Beck Depression Inventory (BDI): Developed by Beck in 1961, the BDI is a 21-item self-report scale scored from 0–3 per item. Scores >20 indicate borderline depression, and >40 indicate severe depression. Reliability and validity coefficients in Turkish adaptations have been reported as satisfactory. 15
Social Appearance Anxiety Scale (SAAS): Developed by Hart (2008) and adapted into Turkish by Doğan (2010), the SAAS consists of 16 items rated on a 5-point Likert scale. Higher scores reflect greater social appearance anxiety. Reliability coefficients (Cronbach’s α = 0.93; test-retest r = 0.85) confirm strong internal consistency and validity.16,17
Oxford Happiness Questionnaire (OHQ): Developed by Hills and Argyle, the OHQ includes 29 items (19 positive, 10 negative) rated on a 6-point Likert scale. Higher scores indicate greater happiness. Reliability coefficients (Cronbach’s α = 0.91; split-half r = 0.86) demonstrate high reliability. The Turkish version has been validated with strong psychometric properties.18,19
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Normality was assessed with the Kolmogorov–Smirnov test. As data did not meet normal distribution assumptions (p<0.05), nonparametric methods were applied. Spearman correlation coefficients were calculated to examine associations between continuous variables. Confidence intervals and effect sizes were reported where appropriate to enhance interpretability.
Results
Participant Characteristics
Among the 44 patients with hemophilia enrolled, 10 (23%) had hemophilia B and 34 (77%) had hemophilia A. All were diagnosed with severe disease (factor activity <1%) and received routine prophylactic care. Twenty-eight spouses also participated. The mean age of the overall cohort was 32.2 years (SD ± 8.4).
Primary Outcomes
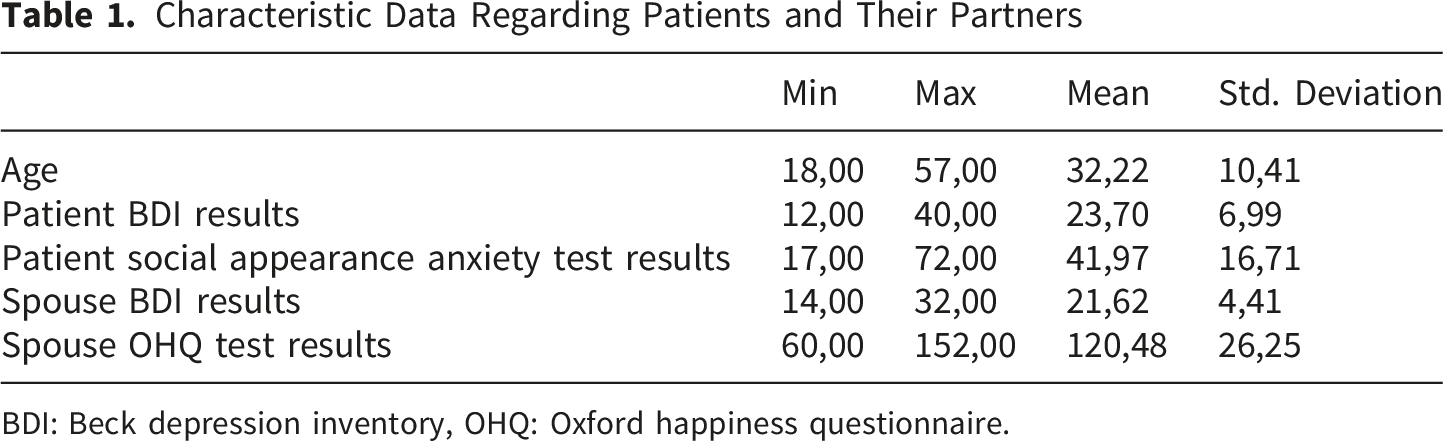
Patients demonstrated a mean Beck Depression Inventory (BDI) score of 23.7 (95% CI: 21.4–26.0), consistent with clinically significant depressive symptoms. Spouses reported a mean BDI score of 21.6 (95% CI: 19.1–24.1), also within the depression range (see Figure 2), highlighting that depressive symptoms were consistently elevated across both groups. The mean Social Appearance Anxiety Scale (SAAS) score among patients was 42.0 (95% CI: 38.5–45.5). Spouses had a mean Oxford Happiness Questionnaire (OHQ) score of 120.0 (95% CI: 114.2–125.8), indicating moderate levels of happiness. The OHQ was administered only to spouses, not to patients, as social appearance anxiety was assessed in patients using the SAAS, which was considered more relevant for evaluating appearance-related concerns. Descriptive statistics are summarized in Table 1, which demonstrates that both patients and spouses reported mean BDI scores above the clinical threshold, while patients also exhibited elevated social appearance anxiety and spouses moderate levels of happiness. Depression Levels in Patients and Spouses Mean Beck Depression Inventory (BDI) scores in patients and spouses. Both groups scored above the clinical cut-off of 20, indicating clinically significant depressive symptoms and highlighting the shared psychological burden of hemophilia Characteristic Data Regarding Patients and Their Partners BDI: Beck depression inventory, OHQ: Oxford happiness questionnaire.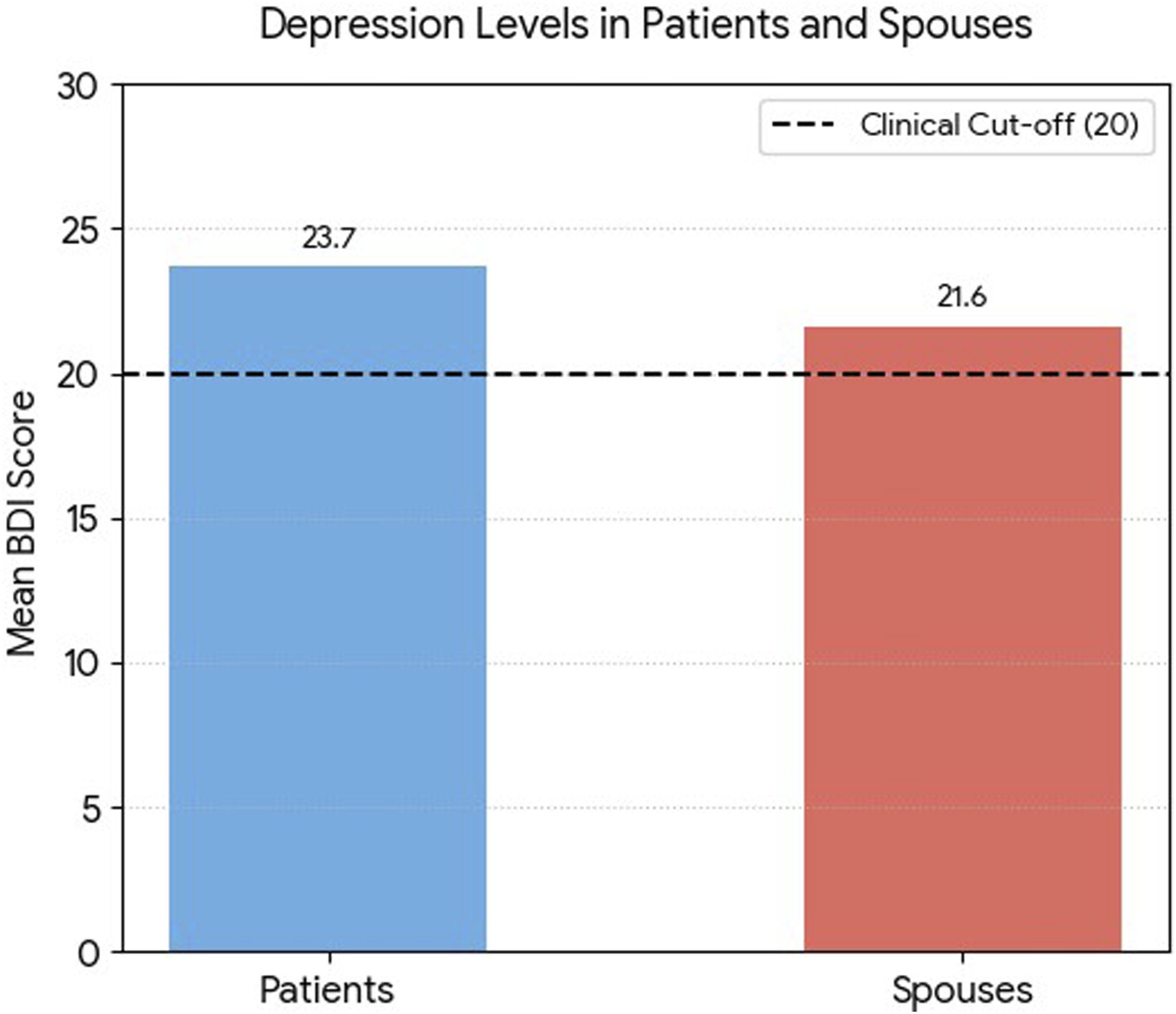
Correlation Analyses
Correlation Between Age, Bleeding Number and Scales (n=44)
BDI: Beck depression inventory, OHQ: Oxford happiness questionnaire, SAAS: social appearance anxiety scale.
*Correlation is significant at the 0.05 level (Spearman correlation test).
**Correlation is significant at the 0.01 level (Spearman correlation test).
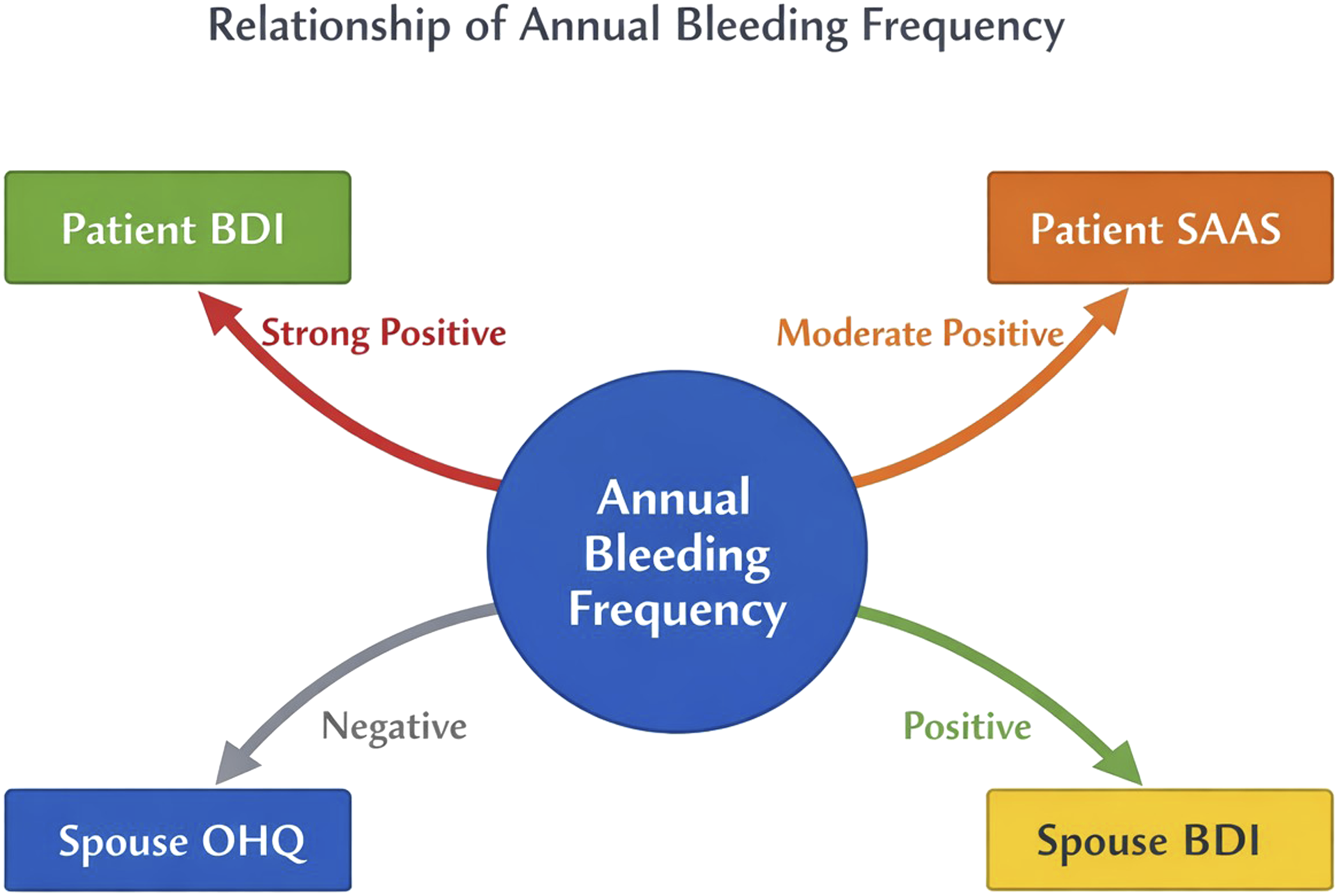
Relationship Map of Annual Bleeding Frequency Schematic representation of correlations between annual bleeding frequency and psychosocial outcomes. Strong positive associations were observed with patient depression (BDI), moderate positive associations with social appearance anxiety (SAAS), and negative associations with spouse happiness (OHQ). Patient appearance anxiety was further linked to increased depression in spouses
Secondary Associations
Secondary associations are detailed in Table 2. Patient BDI scores were positively correlated with SAAS scores (r = 0.586, p = 0.001) and negatively correlated with spouse OHQ scores (r = –0.372, p = 0.047). Patient SAAS scores were positively correlated with spouse BDI scores (r = 0.511, p = 0.001) and negatively correlated with spouse OHQ scores (r = –0.579, p = 0.001). Finally, spouse BDI scores were negatively correlated with spouse OHQ scores (r = –0.452, p = 0.014). Collectively, these findings (Table 2) underscore the interconnected psychosocial burden within families, linking patient distress directly to spouse well-being.
Clinical Relevance
These findings indicate that higher bleeding frequency is associated with greater depressive symptoms and appearance-related anxiety in patients, as well as reduced happiness in spouses. The strength of correlations (r > 0.5 for several associations) underscores the clinical relevance of these psychosocial outcomes.
Discussion
Hemophilia treatment has progressed from fresh frozen plasma to individualized regimens with novel products, including emicizumab prophylaxis as demonstrated in the HAVEN trials, and ongoing gene therapy studies, which have transformed patient-reported outcomes.20-22 These advances are consistent with recent World Federation of Hemophilia (WFH) Guidelines (2020–2023), which emphasize the integration of modern prophylaxis and patient-reported outcome measures into routine care. 23 Nevertheless, bleeding episodes and joint damage continue to affect patients’ physical appearance and performance, which are central to self-concept formation. 24 Frequent hospital admissions and bleeding-related complications impair quality of life not only for patients but also for their relatives. While depressive symptoms in patients with hemophilia have been widely studied, research on social appearance anxiety in adult patients and depressive states in spouses remains scarce and often outdated. 25 To our knowledge, this is the first study to apply the Social Appearance Anxiety Scale (SAAS) in adult patients with hemophilia, extending prior adolescent-focused work and situating our findings within contemporary psychosocial frameworks.10-27
Our findings demonstrate that both patients and spouses reported mean BDI scores above the clinical threshold (Figure 2, Table 1), underscoring the shared psychological burden of hemophilia. Similar impairments in psychosocial outcomes were reported by Álvarez-Román et al., who found reduced quality of life in adult hemophilia A patients even in the absence of inhibitors. Importantly, social appearance anxiety decreased with age among patients, suggesting that younger individuals are more vulnerable to appearance-related concerns. 28 This aligns with prior work indicating that bleeding and complications influence emotional states and self-image. Notably, our study is the first to apply the SAAS in adult PWH. Köker et al. examined self-image in adolescents with hemophilia using the OSIQ and found no correlation between bleeding frequency and self-concept, possibly due to the broader scope of the instrument and the younger age group. 10 Similarly, Khair et al. reported reduced appearance anxiety after regular exercise in young adults, although bleeding frequency was not evaluated in their study. 29 This supports the potential role of structured exercise programs in mitigating appearance-related concerns among patients with hemophilia. By integrating recent multicenter and registry data, 30 our study highlights that psychosocial burden persists despite modern prophylaxis, reinforcing the need for systematic patient-reported outcome (PRO) assessments.
Our findings are consistent with recent literature emphasizing the psychosocial burden of hemophilia. Álvarez-Román et al. 28 reported impaired psychosocial outcomes in adult patients with hemophilia A, even in the absence of inhibitors. Peng et al. highlighted high rates of depression and anxiety among hemophilia patients enrolled in clinical trials, underscoring the persistence of psychological distress despite modern therapies. 31 Koseoglu et al. demonstrated elevated depression and anxiety scores in both hemophilia A and B cohorts, consistent with our findings. 32 Von Mackensen et al. further emphasized that psychosocial support remains an unmet need in hemophilia centers, supporting our recommendation for integrated care models. 33
The observed associations can be understood within a biopsychosocial framework. Biologically, recurrent bleeding leads to joint damage and visible deformities, which heighten appearance-related anxiety, particularly among younger patients. Psychologically, these physical changes contribute to depressive symptoms and diminished self-esteem. Socially, the burden extends to spouses, who experience reduced happiness and emotional strain in parallel with patient distress. This biopsychosocial cascade is consistent with global frameworks for quality of life in hemophilia, and underscores how biological complications translate into psychological and social domains. 30
We also observed that higher annual bleeding counts were strongly associated with increased depressive symptoms and moderately associated with appearance-related anxiety in patients (Table 2, Figure 3). These findings are consistent with the meta-analysis by Al Hunuti et al., which demonstrated that hemophilia complications elevate anxiety and depression risk. 34 In contrast, no direct relationship was found between bleeding frequency and depression in spouses, although Triemstra et al. reported higher depression levels in spouses of frequently bleeding patients in a cohort that included mild and moderate hemophilia cases during an era of on-demand treatment. 25
Finally, our study revealed that increased bleeding frequency in patients was associated with lower happiness scores in spouses, as measured by the OHQ (Table 2). This represents the first investigation of OHQ in spouses of adult PWH. Arab et al. assessed OHQ in parents of pediatric patients and found no relationship with social conditions such as visit frequency or marital status, highlighting differences in caregiver roles between parents and spouses. 35 It should be noted, however, that these associations are correlational and do not imply causation. While our findings suggest a link between bleeding frequency and reduced spouse happiness, causal inferences cannot be drawn from this cross-sectional design. Moreover, although our study extends previous caregiver research to adult partners, the novelty of partner-related findings should be interpreted cautiously and requires replication in larger, longitudinal cohorts.
These clinical recommendations are aligned with recent World Federation of Hemophilia (WFH) Guidelines (2020–2023), which emphasize the integration of modern prophylaxis, multidisciplinary care, and systematic patient-reported outcome monitoring. 23 Our findings carry important clinical implications. Routine psychosocial screening should be integrated into hemophilia care, including validated measures for depression, anxiety, and appearance-related concerns. Multidisciplinary care models—combining hematologists, psychologists, psychiatrists, and physiotherapists—are essential to address both physical and emotional outcomes. Family-centered interventions should be prioritized, as spouse well-being is directly linked to patient distress. Rehabilitation programs and structured exercise interventions may mitigate appearance anxiety and improve psychosocial resilience, consistent with prior evidence in young adults. 29
Despite several strengths, including sample size, inclusion criteria, and the use of validated assessments, certain limitations must be acknowledged. Psychiatric diagnoses were not formally evaluated; however, reliable and validated scales were employed to quantify psychological outcomes. The relatively small sample size and cross-sectional design restrict generalizability and preclude assessment of longitudinal changes before and after treatment. Moreover, the absence of multivariate or regression modeling limits the ability to control for confounders such as age, disease severity, and treatment modality (e.g., emicizumab versus factor replacement). Future studies should incorporate advanced statistical approaches to better delineate the independent contributions of bleeding phenotype and psychosocial outcomes. Additionally, the cross-sectional design prevents causal inference, underscoring the need for longitudinal and interventional studies to confirm and expand our findings.
Conclusion
This study highlights the substantial psychosocial burden of hemophilia on both patients and their spouses. Patients demonstrated clinically significant depressive symptoms and elevated appearance-related anxiety, particularly among younger individuals, while spouses reported reduced happiness in parallel with patient distress. Notably, this represents the first application of the Oxford Happiness Questionnaire in spouses of adult PWH, underscoring the interconnected nature of patient–partner well-being. Despite strengths in design and validated assessments, limitations include the cross-sectional approach, modest sample size, and reliance on self-report measures. Future research with larger, longitudinal cohorts and interventional strategies is warranted to further elucidate these dynamics and to inform comprehensive care models that integrate psychological support alongside medical management.
Footnotes
Ethical Considerations
Ethics committee approval was obtained for our article with the application numbered HRÜ/23.10.02. from the Non-Invasive Clinical Research Ethics Committee of Harran University Faculty of Medicine.
Consent to Participate
All patients and volunteers participating in the study were informed about the study and appropriate study conditions were provided, and this was also stated in the ethics committee application. All procedures were carried out in accordance with the ethical rules and the principles of the Declaration of Helsinki.
Author Contributions
Cem Selim is the corresponding author and participated in the design of the study, data collection, and statistical analysis. Rafiye Çiftçi participated in approving the final version, critically appraising the manuscript, and performing statistical analysis. Sadice Kızgın participated in preparing the appropriate environment for the psychiatric tests and in administering and evaluating the tests and interpreting the statistical results.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: The funder had no role in the design, data collection, data analysis, and reporting of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data of all patients included in the study are available in the data archives of the Ministry of Health of the Republic of Türkiye, and the authors undertake to share this information with the editor if requested.