
Abstract
Background
Rapid assessment of rivaroxaban exposure is clinically critical for older patients with atrial fibrillation in scenarios such as acute bleeding, urgent invasive procedures, or thrombolysis decision-making. This study evaluated rivaroxaban-calibrated anti-factor Xa activity (anti-FXa activity), prothrombin time (PT), and activated partial thromboplastin time (APTT) for identifying clinically relevant rivaroxaban concentrations in older atrial fibrillation patients.
Methods
In this prospective multicenter diagnostic accuracy study, older patients with atrial fibrillation receiving rivaroxaban were enrolled. Liquid chromatography–tandem mass spectrometry (LC-MS/MS) was used as the reference standard, with ≥50 ng/mL defined as the primary diagnostic threshold. Anti-FXa activity, PT, and APTT were evaluated as index tests. Diagnostic performance was assessed using receiver-operating-characteristic analysis, Youden-derived cut-offs, and patient-level clustered bootstrap resampling.
Results
A total of 183 patients were included, contributing 350 LC-MS/MS samples. Anti-FXa activity showed the highest discrimination for identifying LC-MS/MS-measured rivaroxaban concentrations ≥50 ng/mL, with an area under the receiver-operating characteristic curve (AUC) of 0.980 (95% confidence interval [CI], 0.960–0.993), followed by PT (0.904; 95% CI, 0.869–0.938) and APTT (0.825; 95% CI, 0.779–0.869). At Youden-derived cut-offs, anti-FXa activity had sensitivity of 94.0% and specificity of 96.1%, compared with 84.8% and 85.4% for PT, and 74.4% and 81.0% for APTT. Spearman correlations with LC-MS/MS were strongest for anti-FXa activity, followed by PT and APTT.
Conclusion
In this cohort of older patients with AF, anti-factor Xa activity showed the highest diagnostic accuracy for identifying rivaroxaban concentrations ≥50 ng/mL, whereas PT provided moderate discrimination and APTT was less informative.
Introduction
Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia and an important cause of ischemic stroke. 1 Direct oral anticoagulants (DOACs) are recommended as the preferred option for stroke prevention in AF by contemporary clinical guidelines,2,3,4 and rivaroxaban is among the most widely used factor Xa inhibitors. Although routine laboratory monitoring is not required for most patients receiving DOACs, measurement of rivaroxaban exposure may be clinically relevant in selected situations. 5 This issue is particularly relevant in older patients with AF, who often have multimorbidity, polypharmacy, and age-related changes in renal and hepatic function that may increase variability in drug exposure.6,7 Current guidance 8 also recognizes advanced age, urgent bleeding, and invasive procedures as settings in which DOAC measurement may be considered, although test results should be interpreted in clinical context rather than used for routine dose adjustment.
Several laboratory approaches may be used to assess rivaroxaban exposure. Liquid chromatography–tandem mass spectrometry (LC-MS/MS) is regarded as the reference method for measuring plasma rivaroxaban concentrations, but its routine use is limited by batch-based workflows, technical requirements, and longer turnaround time. Chromogenic anti-factor Xa activity assays, 9 particularly when calibrated for the specific drug, provide a more accessible functional approach for estimating factor Xa inhibitor exposure. Routine coagulation assays, including prothrombin time (PT) and activated partial thromboplastin time (APTT), are widely available and rapidly performed in clinical laboratories. PT reflects the extrinsic and common coagulation pathways, whereas APTT reflects the intrinsic and common pathways. Rivaroxaban can prolong PT and, to a lesser extent, APTT, but the magnitude of these changes depends on reagent sensitivity, analytical platform, drug concentration, and patient-related factors.10,11 The clinical utility of PT and APTT for identifying clinically relevant rivaroxaban exposure remains uncertain and requires evaluation against a reference concentration method.
Although the relationships between rivaroxaban exposure and individual coagulation assays have been previously described, direct comparative evidence regarding their ability to identify clinically relevant rivaroxaban levels remains limited in older patients with AF. Therefore, using LC-MS/MS as the reference method, we directly compared the diagnostic performance of anti-factor Xa activity, PT, and APTT for identifying rivaroxaban concentrations ≥50 ng/mL in this clinically vulnerable population.
Methods
Study Design
The present investigation is a sub-study of the RIVAroxaban Genetic Association in Patients with atrial fibrillation (RIVA-GAP, trial registration number of ChiCTR2300074934), which is a prospective observational multicenter study in older patients with atrial fibrillation treated with rivaroxaban. The study protocol was reviewed and approved by the ethics committees of the participating hospitals. The study was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants.
Patients
Qualified patients were enrolled consecutively in the RIVA-GAP cohort. The inclusion criteria were as follows: (1) patients of age over 65; (2) patients diagnosed as NVAF according to the European Society of Cardiology criteria; (3) treated with rivaroxaban for at least 3 consecutive days. The exclusion criteria were as follow: (1) severely impaired renal function with creatinine clearance <30 mL/min; (2) moderate-severe hepatic dysfunction (considered Child–Pugh class B and class C); and (3) incomplete medical information.
Rivaroxaban dose was determined by the treating clinicians before enrollment and was not assigned by the study protocol. For determination of plasma rivaroxaban concentration (LC-MS/MS method), trough samples were collected at 24 hours after the last dose, and peak samples were collected at 2 to 4 hours after drug ingestion, both using EDTA-anticoagulated tubes. For anti-FXa activity and hemostasis tests, plasma samples were collected at the same time points as those for LC-MS/MS analysis in vacuum tubes containing 3.2% trisodium citrate. Blood samples were centrifuged for 15 min at 3000 rpm, and 0.5 mL of the upper layer of platelet-poor plasma was aspirated. All blood samples were frozen and stored at -80 °C in the institutional biobank for further analysis.
LC-MS/MS Method
Rivaroxaban concentrations in plasma samples were quantified using LC-MS/MS. Human plasma samples were directly protein precipitated by acetonitrile, and rivaroxaban-d4 was used as the internal standard. The separation was carried out on a Kinetex® 5 μm XB-C18 100A, (50 × 2.1 mm) column with a gradient elution using a 5 mmoL/L, ammonium acetate solution containing 0.2% formic acid (A)-acetonitrile (B) as the mobile phase, at a flow rate of 0.6 mL/min, and a column temperature of 40°C. The ionic reactions used for quantitative analysis were m/z 436.1 (parent ion) → m/z 145.0 (rivaroxaban) and m/z 440.1 (parent ion) → m/z 145.0 (internal standard) using an electrospray ionization source, the positive ionization mode, and multiple reaction monitoring (MRM) scanning mode. The standard curve equation of rivaroxaban in human plasma was y=0.00728x+0.000389 (r=0.9981), with good linearity in the range of 0.5∼600 ng/mL, the lower limit of quantification was 0.5 ng/mL. The methodological validations were performed to ensure the reliability of the detection results, shown in Supplementary Tables S1 and S2.
Chromogenic anti-FXa Activity Assay
The peak and trough anti-FXa activity of rivaroxaban were determined using a commercially available anti-FXa activity assay with rivaroxaban-specific setup using rivaroxaban calibrator on the MDC7500 automatic coagulation analyzer (Beijing Jiuqiang Biotechnology Co., Ltd., Beijing, China). The anti-FXa activity reagent used was the Jiuqiang Anti-Xa Assay Kit (Chromogenic Substrate Method), specifically optimized for rivaroxaban quantification. The results of rivaroxaban calibration of anti-FXa activity were expressed in ng/mL. The lower limit of quantification of the FXa activity bioassay was 25 ng/mL, which was adopted from the manufacturer’s validated data and further verified locally.
Hemostasis Tests
Prothrombin time (PT) and activated partial thromboplastin time (APTT) were performed using the Jiuqiang PT Reagent Kit and Jiuqiang APTT Reagent Kit on the MDC7500 automatic multiparameter hemostasis analyzer (Beijing Jiuqiang Biotechnology Co., Ltd., Beijing, China). The thromboplastin source of PT reagent is rabbit brain powder (20 g/L), while the APTT reagent contains ellagic acid (2.85 g/L), phenol (2.5 g/L), and rabbit brain phospholipid (1 g/L), with ellagic acid acting as the contact activator to initiate the intrinsic coagulation pathway and rabbit brain phospholipid providing a platelet-mimicking surface for cascade activation. The reference ranges for PT and APTT are 10–15 s and 24–40 s respectively.
Index Tests, Reference Standard, and Blinding
LC-MS/MS-measured rivaroxaban concentration was used as the reference standard. Rivaroxaban-calibrated anti-FXa activity, PT, and APTT were evaluated as index tests. All index tests and LC-MS/MS measurements were performed according to prespecified laboratory protocols using samples collected at the same peak or trough time points. Laboratory personnel performing the index tests were blinded to the LC-MS/MS results, and personnel performing LC-MS/MS were blinded to the anti-FXa activity, PT, and APTT results. Index-test results were not used to define the reference-standard classification, and LC-MS/MS results were not available when the index tests were performed.
Statistical Analyses
Patient characteristics were summarized using descriptive statistics. Categorical variables are expressed as n (%). Continuous variables were expressed as mean ± SD (standard deviation) if normally distributed, or median (25th percentile [Q1] – 75th percentile [Q3]) otherwise. The primary diagnostic target was defined as a clinically relevant rivaroxaban concentration of ≥50 ng/mL, measured by LC-MS/MS. For the diagnostic accuracy analyses, each paired blood sample was classified as positive if the LC-MS/MS-measured rivaroxaban concentration was ≥50 ng/mL and negative if it was <50 ng/mL. Anti-FXa activity, PT, and APTT were evaluated as index tests for identifying samples with rivaroxaban concentrations ≥50 ng/mL. The blood sample was used as the unit of analysis. Because some patients contributed both peak and trough samples, within-patient correlation was addressed using patient-level clustered bootstrap resampling.
The Spearman’s rank correlation coefficient was used to assess the monotonic association between LC-MS/MS-measured rivaroxaban concentrations and each index test, with Spearman correlations ≥ 0.9 indicating a high correlation. Agreement between rivaroxaban-calibrated anti-FXa activity and LC-MS/MS-measured rivaroxaban concentrations was further evaluated using Bland–Altman analysis. Median bias and percentile-based 95% limits of agreement (LoA) were reported. Deming regression was used to assess the linear relationship between rivaroxaban-calibrated anti-FXa activity and LC-MS/MS-measured concentrations, accounting for measurement error in both methods. Because replicate measurements were not available to estimate method-specific error variances, the error variance ratio was set to 1.
Receiver operating characteristic curves were constructed to evaluate the ability of anti-FXa activity, PT, and APTT to identify LC-MS/MS-measured rivaroxaban concentrations ≥50 ng/mL. This threshold was selected a priori because expert guidance considers DOAC concentrations >50 ng/mL clinically relevant in patients with serious bleeding when reversal may be considered.12-14 Therefore, the 50 ng/mL threshold was used as a marker of clinically relevant residual rivaroxaban exposure, rather than as a prospectively validated safety threshold for clinical outcomes. The area under the receiver operating characteristic curve (AUC) and its corresponding 95% confidence interval (CI) were calculated for each index test. The optimal cut-off value for each index test was determined by maximizing Youden’s index. Based on the corresponding cut-off values, 2 × 2 contingency tables were constructed, and sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, negative likelihood ratio, and overall accuracy were calculated.
To account for within-patient correlation caused by paired peak and trough samples, 95% confidence intervals for diagnostic performance measures were estimated using patient-level clustered bootstrap resampling with 1,000 iterations. In each bootstrap iteration, patients rather than individual samples were resampled with replacement, and all available peak and/or trough samples from selected patients were retained. Pairwise differences in AUCs among anti-FXa activity, PT, and APTT were also estimated using the same patient-level clustered bootstrap approach. Two-sided bootstrap P values were calculated from the empirical distribution of AUC differences.
To reduce optimism caused by deriving Youden cut-off values and estimating diagnostic performance in the same dataset, internal validation was performed using out-of-bootstrap validation. In each bootstrap iteration, the optimal cut-off was determined in the bootstrap training sample, and its diagnostic performance was evaluated in the corresponding out-of-bootstrap validation sample when available. Internally validated estimates of AUC, sensitivity, specificity, positive predictive value, and negative predictive value were summarized across bootstrap iterations.
Sensitivity analyses were performed separately in peak samples and trough samples. Exploratory subgroup analyses stratified by rivaroxaban daily dose (10 mg and 15 mg) were additionally conducted. The same ROC-based diagnostic accuracy framework and patient-level clustered bootstrap procedure were applied to the peak-only and trough-only datasets. Missing or invalid LC-MS/MS or index-test results were not imputed; analyses were performed using available paired results. All statistical tests were two-sided, and P values <0.05 were considered statistically significant. Analyses were performed using R software, version 4.3.3. The study was reported in accordance with the STARD 2015 guidelines for diagnostic accuracy studies. 15
Results
Patient Characteristics
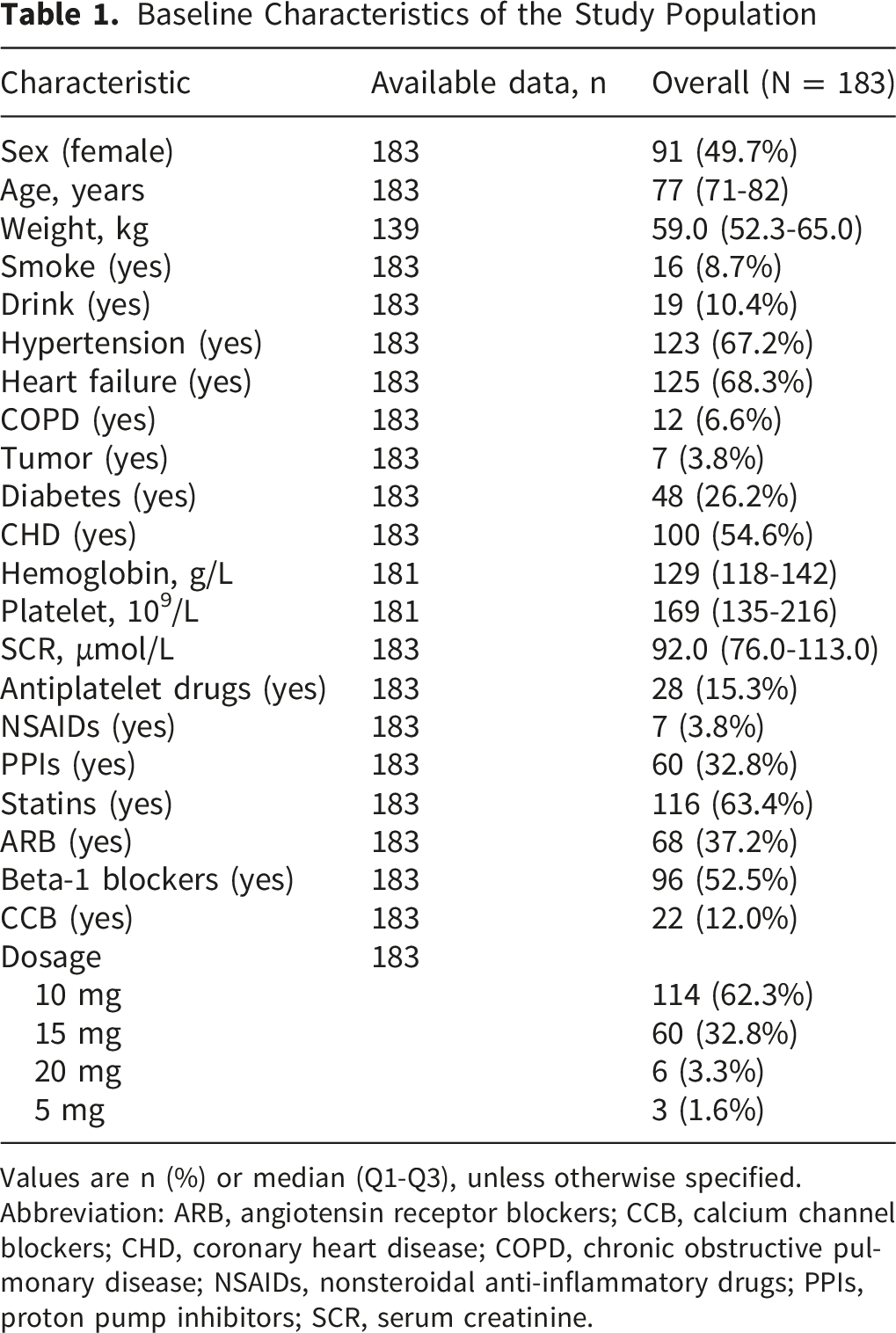
Of 207 potentially eligible participants, 183 were included in the analysis after 24 were excluded because of lost samples or missing test results. A total of 350 LC-MS/MS samples were available, with final paired analysis sets comprising 348 anti-FXa activity, 342 PT, and 343 APTT measurements (Figure 1). Among the 183 patients included in the analysis, the median age was 77 years (Q1–Q3, 71–82), and 91 patients (49.7%) were women. Cardiovascular comorbidity was common: 123 patients (67.2%) had hypertension, 125 (68.3%) had heart failure, and 100 (54.6%) had coronary heart disease. Diabetes was present in 48 patients (26.2%). Concomitant cardiovascular medications were frequently used, including statins in 116 patients (63.4%) and beta-1 blockers in 96 patients (52.5%). Rivaroxaban was most commonly prescribed at 10 mg in 114 patients (62.3%), followed by 15 mg in 60 patients (32.8%). Other demographic characteristics, comorbidities, laboratory measures, concomitant medications, and lifestyle factors are summarized in Table 1. Study flow and analysis sets. Abbreviations: LC-MS/MS, liquid chromatography–tandem mass spectrometry; anti-FXa activity, rivaroxaban-calibrated anti-factor Xa activity; PT, prothrombin time; APTT, activated partial thromboplastin time Baseline Characteristics of the Study Population Values are n (%) or median (Q1-Q3), unless otherwise specified. Abbreviation: ARB, angiotensin receptor blockers; CCB, calcium channel blockers; CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; NSAIDs, nonsteroidal anti-inflammatory drugs; PPIs, proton pump inhibitors; SCR, serum creatinine.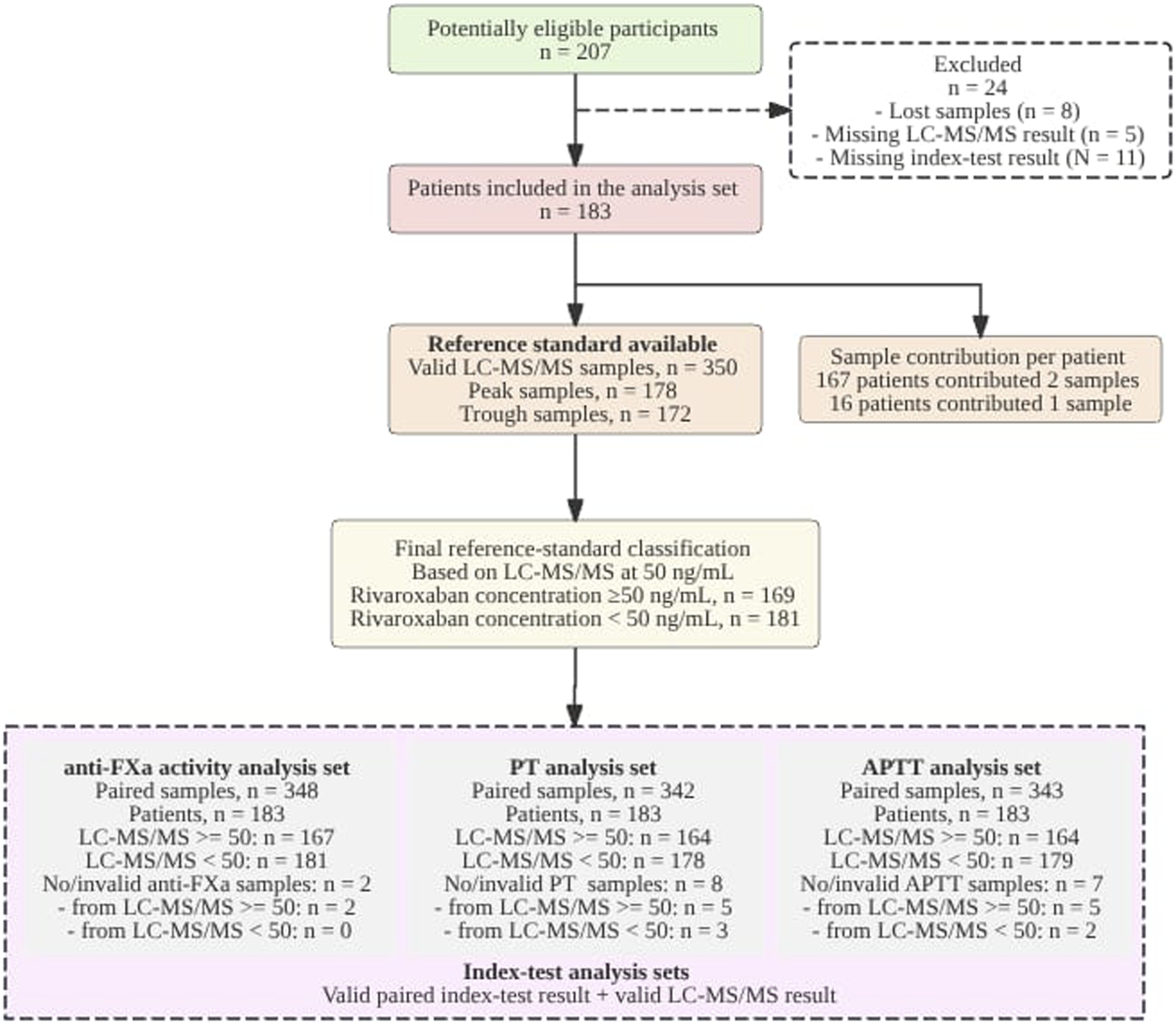
Diagnostic Performance for Identifying Rivaroxaban Concentrations ≥50 ng/mL
The diagnostic unit was the blood sample, whereas clustered resampling was performed at the patient level to account for non-independence of peak and trough samples. At the prespecified LC-MS/MS threshold of ≥50 ng/mL, anti-FXa activity showed the highest discrimination among the three index tests, with PT showing intermediate performance and APTT showing the lowest performance. The AUC was 0.980 (95% CI, 0.960–0.993) for anti-FXa activity, compared with 0.904 (95% CI, 0.869–0.938) for PT and 0.825 (95% CI, 0.779–0.869) for APTT. Patient-level clustered bootstrap comparisons showed larger AUCs for anti-FXa activity than PT, with a median difference of 0.075 (95% CI, 0.046–0.109; P<0.001), and for anti-FXa activity than APTT, with a median difference of 0.155 (95% CI, 0.114–0.202; P<0.001). PT also had a larger AUC than APTT, with a median difference of 0.075 (95% CI, 0.041–0.116; P<0.001). These findings indicate a consistent diagnostic hierarchy at the 50 ng/mL threshold: anti-FXa activity had the strongest discrimination, PT retained moderate discrimination, and APTT provided the least separation among the tested assays (Figure 2A; Table 2; Supplementary Table S4). Diagnostic performance of index tests for identifying LC-MS/MS-measured rivaroxaban concentrations ≥50 ng/mL (A) Receiver-operating-characteristic curves for anti-FXa activity, PT, and APTT in identifying LC-MS/MS-measured rivaroxaban concentrations ≥50 ng/mL. Anti-FXa activity showed the highest discrimination, followed by PT and APTT. (B–D) Distribution of anti-FXa activity, PT, and APTT values according to LC-MS/MS-measured rivaroxaban concentration <50 ng/mL or ≥50 ng/mL. Dashed horizontal lines indicate the Youden-derived cut-offs: 46.59 ng/mL for anti-FXa activity, 12.85 s for PT, and 41.65 s for APTT. Individual points represent paired samples. Abbreviations: LC-MS/MS, liquid chromatography–tandem mass spectrometry; anti-FXa activity, rivaroxaban-calibrated anti-factor Xa activity; PT, prothrombin time; APTT, activated partial thromboplastin time; ROC, receiver-operating-characteristic Diagnostic Performance of Index Tests for Identifying LC-MS/MS-Measured Rivaroxaban Concentrations ≥50 ng/mL Values are apparent point estimates with patient-level clustered bootstrap 95% confidence intervals in parentheses, unless otherwise specified. The reference standard was LC-MS/MS-measured rivaroxaban concentration ≥50 ng/mL. Positive and negative samples were defined as LC-MS/MS ≥50 ng/mL and <50 ng/mL, respectively. Valid paired samples indicate samples with both LC-MS/MS and the corresponding index test available. Cut-offs were determined by maximizing Youden’s index in the apparent dataset. Abbreviation: anti-FXa activity, rivaroxaban-calibrated anti-factor Xa activity; APTT, activated partial thromboplastin time; AUC, area under the receiver operating characteristic curve; CI, confidence interval; LC-MS/MS, liquid chromatography-tandem mass spectrometry; LR+, positive likelihood ratio; LR-, negative likelihood ratio; NPV, negative predictive value; PPV, positive predictive value; PT, prothrombin time.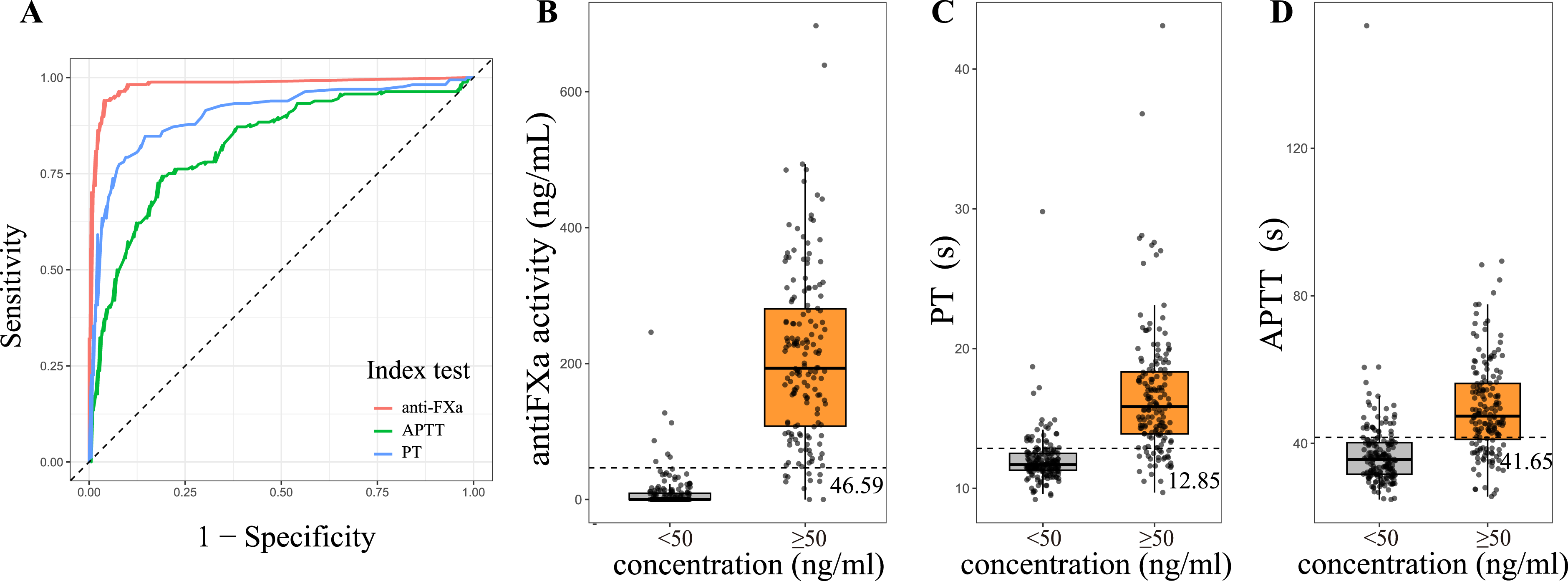
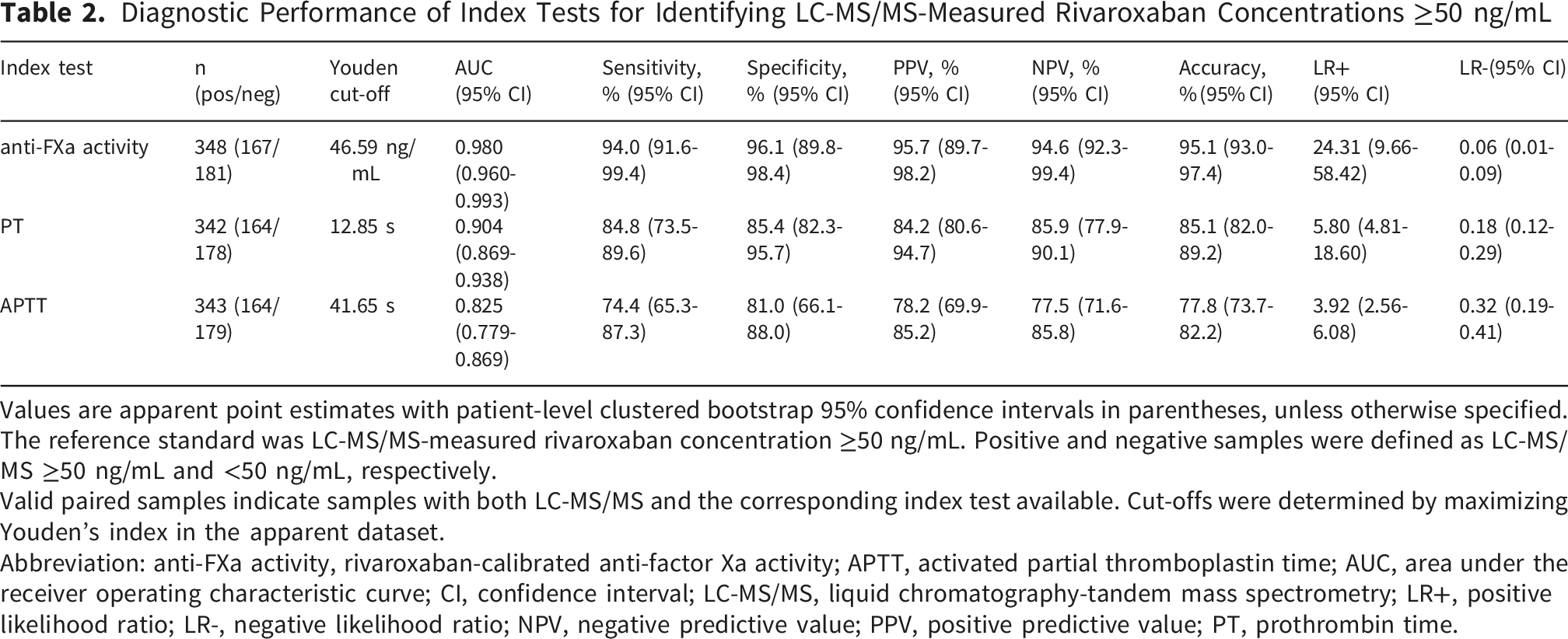
Using Youden-derived cut-offs, anti-FXa activity showed the most balanced diagnostic performance for identifying LC-MS/MS-measured rivaroxaban concentrations ≥50 ng/mL. At a cut-off of 46.59 ng/mL, anti-FXa activity had a sensitivity of 94.0% (95% CI, 91.6–99.4), specificity of 96.1% (95% CI, 89.8–98.4), accuracy of 95.1% (95% CI, 93.0–97.4), LR+ of 24.31 (95% CI, 9.66–58.42), and LR− of 0.06 (95% CI, 0.01–0.09). PT showed intermediate performance at a cut-off of 12.85 s, with sensitivity of 84.8% (95% CI, 73.5–89.6), specificity of 85.4% (95% CI, 82.3–95.7), accuracy of 85.1% (95% CI, 82.0–89.2), LR+ of 5.80 (95% CI, 4.81–18.60), and LR− of 0.18 (95% CI, 0.12–0.29). APTT showed the lowest performance at a cut-off of 41.65 s, with sensitivity of 74.4% (95% CI, 65.3–87.3), specificity of 81.0% (95% CI, 66.1–88.0), accuracy of 77.8% (95% CI, 73.7–82.2), LR+ of 3.92 (95% CI, 2.56–6.08), and LR− of 0.32 (95% CI, 0.19–0.41). The boxplots showed higher index-test values among samples with LC-MS/MS concentrations ≥50 ng/mL, with the clearest separation for anti-FXa activity and progressively greater overlap for PT and APTT (Figure 2B–D; Table 2).
Internal Validation and Sensitivity Analyses
The performance hierarchy was consistent across validation and sensitivity analyses. In out-of-bootstrap validation, median AUCs were 0.980 for anti-FXa activity, 0.904 for PT, and 0.824 for APTT; repeated 5-fold cross-validation yielded similar values of 0.981, 0.907, and 0.828, respectively. Sampling-time sensitivity analyses showed the same ranking in both peak-only samples (AUCs, 0.957, 0.847, and 0.791) and trough-only samples (AUCs, 0.981, 0.816, and 0.729). In the one-random-sample-per-patient analysis, anti-FXa activity also retained the highest AUC, followed by PT and APTT (0.976, 0.898, and 0.812, respectively), supporting the robustness of the primary diagnostic ranking under alternative validation and sampling assumptions (Supplementary Tables S5–S8). Exploratory subgroup analyses stratified by rivaroxaban dosage showed the same diagnostic ranking: in the 10 mg subgroup, AUCs were 0.985 for anti-FXa activity, 0.897 for PT, and 0.801 for APTT; the corresponding values in the 15 mg subgroup were 0.973, 0.923, and 0.883, respectively (Supplementary Table S9).
Correlation and Agreement Analyses
Across all paired samples, LC-MS/MS-measured rivaroxaban concentrations correlated most strongly with anti-FXa activity, followed by PT and APTT (Spearman’s rho, 0.910, 0.753, and 0.595, respectively; all P<0.001), with the same ordering observed in trough and peak samples. For anti-FXa activity versus LC-MS/MS, Bland–Altman analysis showed a median bias of −4.58 ng/mL, with percentile-based 95% limits of agreement from −32.54 to 181.62 ng/mL. Deming regression yielded an intercept of −21.543 (95% CI, −32.197 to −13.312) and a slope of 1.405 (95% CI, 1.267–1.571), indicating that anti-FXa activity was closely aligned with LC-MS/MS in rank-based analyses but showed measurable bias and wide limits of agreement in absolute concentration estimates (Supplementary Tables S10–S12; Supplementary Figures S1–S2).
Discussion
In this prospective multicenter diagnostic accuracy study of 183 older patients with atrial fibrillation receiving rivaroxaban, the rivaroxaban-calibrated anti-FXa activity assay showed the strongest overall performance for identifying LC-MS/MS-measured rivaroxaban concentrations ≥50 ng/mL. Anti-FXa activity had the highest discrimination, with an AUC of 0.980, followed by PT and APTT, with AUCs of 0.904 and 0.825, respectively; this hierarchy was supported by patient-level clustered bootstrap comparisons and remained consistent in internal validation, peak-only, trough-only, and one-random-sample-per-patient sensitivity analyses. The principal contribution of this study is the direct, within-cohort comparison of anti-factor Xa activity, PT, and APTT against LC-MS/MS-measured concentrations at a clinically relevant threshold in older patients with AF. Our findings provided population-specific estimates of diagnostic accuracy and practical cutoff values that may support rapid assessment when LC-MS/MS is not immediately available.
Chromogenic anti-FXa activity assay, specifically calibrated with the drug to be tested, has been recommended for rivaroxaban detection by national and international guidelines.10,13 A strong positive association between anti-FXa activity and rivaroxaban concentration (rho = 0.910 across all samples, 0.842 in peak samples, and 0.715 in trough samples.) was observed in current research, consistent with previous findings.12,16,17 The corresponding categorical result of clinical thresholds is the most crucial information, which might directly prompt clinical decision making. Anti-FXa activity exhibited the highest AUC for identifying LC-MS/MS-measured concentrations ≥50 ng/mL, with an AUC of 0.980 and balanced sensitivity and specificity at the Youden-derived cut-off of 46.59 ng/mL. The Bland–Altman and Deming findings indicated that anti-FXa activity-derived values should not be regarded as numerically interchangeable with LC-MS/MS across the full concentration range. This is consistent with Studt et al, 17 who found high correlations between anti-Xa assays and HPLC-MS but also reported systematic bias, wider limits of agreement, and concentration-dependent variation across reagents and platforms.
At the 50 ng/mL LC-MS/MS threshold, PT had an AUC of 0.904, with sensitivity and specificity both approximately 85% at the Youden-derived cut-off of 12.85 s. Spearman analysis also showed a moderate-to-strong association between PT and LC-MS/MS concentration across all samples, with rho = 0.753. The diagnostic and correlation findings together support PT as a potential qualitative adjunct for identifying clinically relevant rivaroxaban exposure when anti-FXa activity is unavailable, rather than as a quantitative substitute for LC-MS/MS or anti-FXa activity. This distinction is important because PT responses to rivaroxaban are reagent- and platform-dependent, and the cut-off identified in this study lies close to commonly used PT reference intervals. 18 It may serve as a qualitative screening tool, where a prolonged result suggests the presence of an anticoagulant, but a normal PT may not reliably exclude clinically relevant rivaroxaban concentrations.
APTT had the weakest overall performance among the three index tests. Although APTT values tended to increase with higher LC-MS/MS-measured rivaroxaban concentrations, its diagnostic discrimination was lower than that of anti-FXa activity and PT, with an AUC of 0.825 at the 50 ng/mL threshold. These findings indicate that APTT reflects some concentration-related signal but with substantial dispersion and limited reliability, which aligns with guideline recommendations against the use of APTT for monitoring Xa inhibitor activity.19,20 Furthermore, APTT prolongation may also result from coagulation factor deficiencies, inhibitory substances, or global hemostatic impairments. In this context, the present findings support the conclusion that APTT should not be used to exclude clinically relevant rivaroxaban exposure. A simple and rapid test has been proposed for the functional assessment of DOAC, the MRX PT DOAC. 21 This test measures the effect of DOACs on the extrinsic coagulation pathway rather than its concentration, using a single reagent.
Several methodological features strengthen the interpretation of this study. LC-MS/MS was used as the reference standard, and the analytical validation data supported the reliability of the concentration measurements. The study also addressed two issues that are often insufficiently handled in diagnostic accuracy studies using paired peak and trough samples. First, because samples from the same patient are not independent, patient-level clustered bootstrap and one-random-sample-per-patient sensitivity analyses were performed. Second, because Youden-derived cut-offs may overestimate apparent diagnostic performance when derived and evaluated in the same dataset, out-of-bootstrap and repeated 5-fold cross-validation analyses were used to assess internal validity. The relative ranking of the three assays was consistent across these analyses, which reduces the likelihood that the primary findings were driven only by sample-level dependence or apparent-sample cut-off optimization.
There were several limitations that should be acknowledged in this study. First, we did not evaluate clinical outcomes such as bleeding, thrombosis, perioperative decisions, reversal-agent use, or procedural complications. Therefore, the findings should be interpreted as diagnostic accuracy results against LC-MS/MS-defined rivaroxaban concentration thresholds, rather than evidence that testing improves clinical outcomes. Second, our cohort was limited to older Chinese patients with atrial fibrillation, predominantly receiving low-dose rivaroxaban (10 mg once daily), with a smaller subset on 15 mg once daily and very few patients on the standard 20 mg once-daily regimen. Therefore, our results should not be extrapolated to younger or non-Asian populations, other clinical indications, other direct oral anticoagulants, or patients receiving standard-dose rivaroxaban without further validation. Third, PT and APTT are reagent- and platform-dependent, and the cut-offs reported here may not be transferable to laboratories using different coagulation systems. Finally, although internal validation and sensitivity analyses were performed, external validation in independent laboratories and with different assay platforms remains necessary before broad implementation.
Conclusion
In this cohort of older patients with AF, anti-factor Xa activity showed the highest diagnostic accuracy for identifying rivaroxaban concentrations ≥50 ng/mL, whereas PT provided moderate discrimination and APTT was less informative. These findings support anti-factor Xa activity as the most reliable of the evaluated readily available assays when LC-MS/MS is unavailable, although external validation is required.
Supplemental Material
Supplemental Material - Diagnostic Accuracy of Anti-factor Xa Activity, PT, and APTT for Clinically Relevant Rivaroxaban Levels in Older AF Patients
Supplemental Material for Diagnostic Accuracy of Anti-factor Xa Activity, PT, and APTT for Clinically Relevant Rivaroxaban Levels in Older AF Patients by Qiang Zhao, M.S., Guoquan Chen, M.S., Haiping Wang, B.S., Jiale Chen, M.S., Xianqing Hu, M.D. in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Ethical Considerations
The RIVA-GAP study protocol was reviewed and approved by the Medical Ethics Review Committee of Jinhua Municipal Hospital and Longyan Second Hospital.
Consent to Participate
Written informed consent was obtained from all participants included in the study.
Author Contributions
Qiang Zhao, Haiping Wang, and Guoquan Chen conceived and designed the study. Qiang Zhao, Haiping Wang, Guoquan Chen, and Jiale Chen contributed to data collection and manuscript drafting. Qiang Zhao and Haiping Wang participated in the development of the methodology. Guoquan Chen performed the statistical analysis and generated the figures. Haiping Wang and Guoquan Chen acquired funding for the study. Xianqing Hu supervised the study and critically revised the manuscript. All authors revised the manuscript and approved the final version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Jinhua Central Hospital Youth Research Foundation (Grant No. JY2024-2-14), the Health Project of Longyan Joint Fund for Scientific and Technological Innovation (Grant No. 2023LYF17089), and the Key Science and Technology Plan Projects of Jinhua (Grant No. 2023-3-122).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Trial Registration
RIVAroxaban Genetic Association in Patients with Atrial Fibrillation (RIVA-GAP). Trial registration number: ChiCTR2300074934.
Prior Presentation
This manuscript has not been presented at a professional meeting.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.