
Abstract
Oral and maxillofacial space infections (OMSIs) are potentially life-threatening polymicrobial conditions requiring timely and appropriate antimicrobial therapy. We conducted a systematic review and meta-analysis of 53 studies (12,408 cases) to evaluate microbial epidemiology and resistance patterns. Streptococcus was the predominant pathogen (45.51%), followed by Prevotella (15.89%) and Porphyromonas (15.61%). Methicillin-resistant Staphylococcus aureus (MRSA) accounted for 19.18% of S. aureus isolates. Diabetic patients exhibited a higher prevalence of Klebsiella (27.09% vs. 8.13% in nondiabetics). Antimicrobial resistance was lowest for levofloxacin (11.03%) and cephalosporins (16.83%), and highest for gentamicin (39.66%) and erythromycin (39.35%). The microbiological landscape and antimicrobial resistance patterns were influenced by multiple factors, including infection source, diabetic status, diagnostic methods, national income level, and temporal trends. Incorporating these variables with local antimicrobial surveillance data can support more targeted and effective empirical therapy. Well-designed, representative studies across diverse settings are urgently needed to optimize antimicrobial use amid rising resistance.
Keywords
Background
The superficial fascial spaces, anatomically adjacent to the oral cavity, constitute the primary sites of oral and maxillofacial space infections (OMSIs).1,2 The pathogen can disseminate rapidly along interconnected fascial planes. 3 OMSIs progress rapidly and can lead to life-threatening complications such as descending airway obstruction, necrotizing mediastinitis, craniocervical necrotizing fasciitis, and systemic inflammatory response syndrome, presenting significant challenges for clinical management.4–6
Antimicrobial therapy represents a cornerstone of OMSIs management. The selection of appropriate antibiotic regimens presents clinical challenges due to the polymicrobial nature of OMSIs, which frequently involve mixed aerobic and anaerobic microorganisms derived from the complex oral microbiota. Culture-based analyses consistently show that Streptococci are the predominant pathogens in OMSIs. Staphylococcus and anaerobic organisms like Prevotella follow. Gram-negative bacilli (notably Klebsiella and Pseudomonas) have been detected in purulent specimens.7–10 The isolation of methicillin-resistant Staphylococcus aureus (MRSA) is of significant clinical concern,11,12 highlighting the complex etiological nature of OMSIs.
In clinical practice, there is a growing trend of combining vancomycin with broad-spectrum antibiotics (such as meropenem) as empirical therapy, due to the critical situation caused by OMSIs and the concerns related to gram-negative bacilli and MRSA infections.12–14 However, antibiotic overuse accelerates the emergence of antimicrobial resistance, which poses a grave and multidimensional threat to global health security, affecting human health while undermining socioeconomic development. 15 Current evidence is still scarce concerning the distribution of pathogens and associated antimicrobial resistance patterns in OMSIs. This systematic review and meta-analysis therefore aims to (1) characterize the microbial epidemiology of OMSIs and (2) analyze resistance patterns of OMSIs to optimize evidence-based therapeutic strategies.
Materials and Methods
Data sources and search strategy
A comprehensive literature search was conducted in the Web of Science, PubMed, EMBASE, Scopus, and the Cochrane Library from database inception until August 19, 2025. The following search terms were used: “maxillofacial space infections,” “maxillofacial infections,” “oral and maxillofacial space infections,” “Ludwig’s angina,” “angina, Ludwig’s,” “ludwig angina,” “ludwigs angina,” “submandibular space infection,” “submandibular space infections,” “culture*,” “microbio*,” “bacteria*,” “isolate*,” “pathogen*,” “sequenc*,” “swab*.” The detailed search strategy for each database is provided in Supplementary Data S1. The meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 16 This meta-analysis has been registered in PROSPERO (registration number: CRD420251124385).
Inclusion and exclusion criteria
Clinical studies were eligible for inclusion if they reported concurrent microbiological culture results, next-generation sequencing (NGS) data, or antimicrobial resistance rates in patients with OMSIs. We excluded reviews, case reports, conference abstracts, and other non-original articles. Studies were also excluded if they presented ambiguous microbiological data, were duplicate publications, or focused solely on a single specific bacterium. For multiple studies reporting on isolates with the same patient population, time period, and geographic origin, only the one involving the largest number of strains was included.
Literature screening and data extraction
The study selection was performed independently by two reviewers (Y.L. and L.Y.) using EndNote version X9. After deduplication, they screened the titles and abstracts of the remaining studies using the inclusion and exclusion criteria. Subsequently, the full texts of studies deemed potentially eligible were retrieved and assessed. Data extraction was performed independently by two investigators using Excel (Office 2019; Microsoft, Redmond, WA, USA). The extracted data included: (1) study characteristics: first author, publication year, country, and title; (2) participant demographics: sample size, sex, age, prevalence of smoking, and diabetes; (3) microbiological outcomes: number of isolated bacterial genera/species and proportion of resistance. Discrepancies during the process were resolved by consensus with a third reviewer (C.W.).
Assessment of literature quality
Two investigators independently evaluated the methodological quality of the included studies using the Joanna Briggs Institute checklist, 17 scoring each item as “yes,” “no,” “unclear,” “not applicable”; any discrepancies were resolved through consensus discussion.
Statistical analysis
All statistical analyses were conducted using R version 4.2.3 with the “meta” package and employing the “metaprop” function. Before pooling, the proportions from individual studies were transformed using the Freeman–Tukey double arcsine transformation to stabilize variances and approximate normality. Random-effects meta-analyses were used to generate the pooled prevalence of the bacterial species and weighted pooled resistance rate estimates with 95% confidence intervals (CIs). Heterogeneity was evaluated through Cochran’s Q test and quantified using the I2 statistic. Publication bias was quantitatively detected by funnel plots and the Egger’s test. Sensitivity analysis was conducted to examine the robustness of the model, including the potential influence of individual studies and other sources of bias.
Results
Study selection and characteristics
The systematic search initially identified 1,434 citations. Following deduplication (n = 618 excluded), 816 records underwent title/abstract screening, which excluded 679 studies; 8 additional studies were unavailable for retrieval. Of the remaining 128 full-text articles assessed, 53 were excluded due to incomplete bacterial infection data, and 22 lacked confirmed OMSIs. As illustrated in Figure 1, a total of 53 studies ultimately met the inclusion criteria.7–10,13,14,18–64
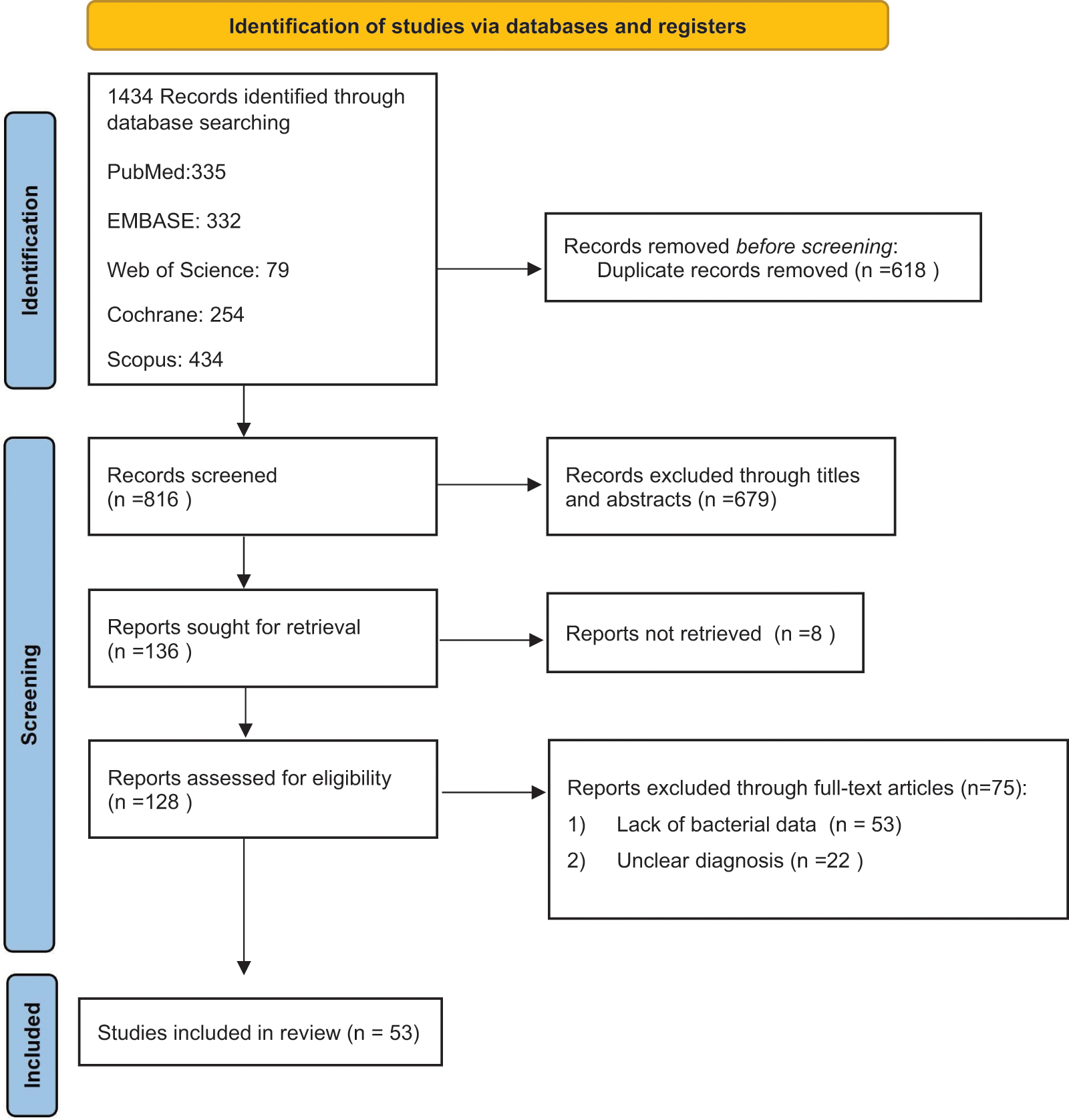
Flowchart of the meta-analysis.
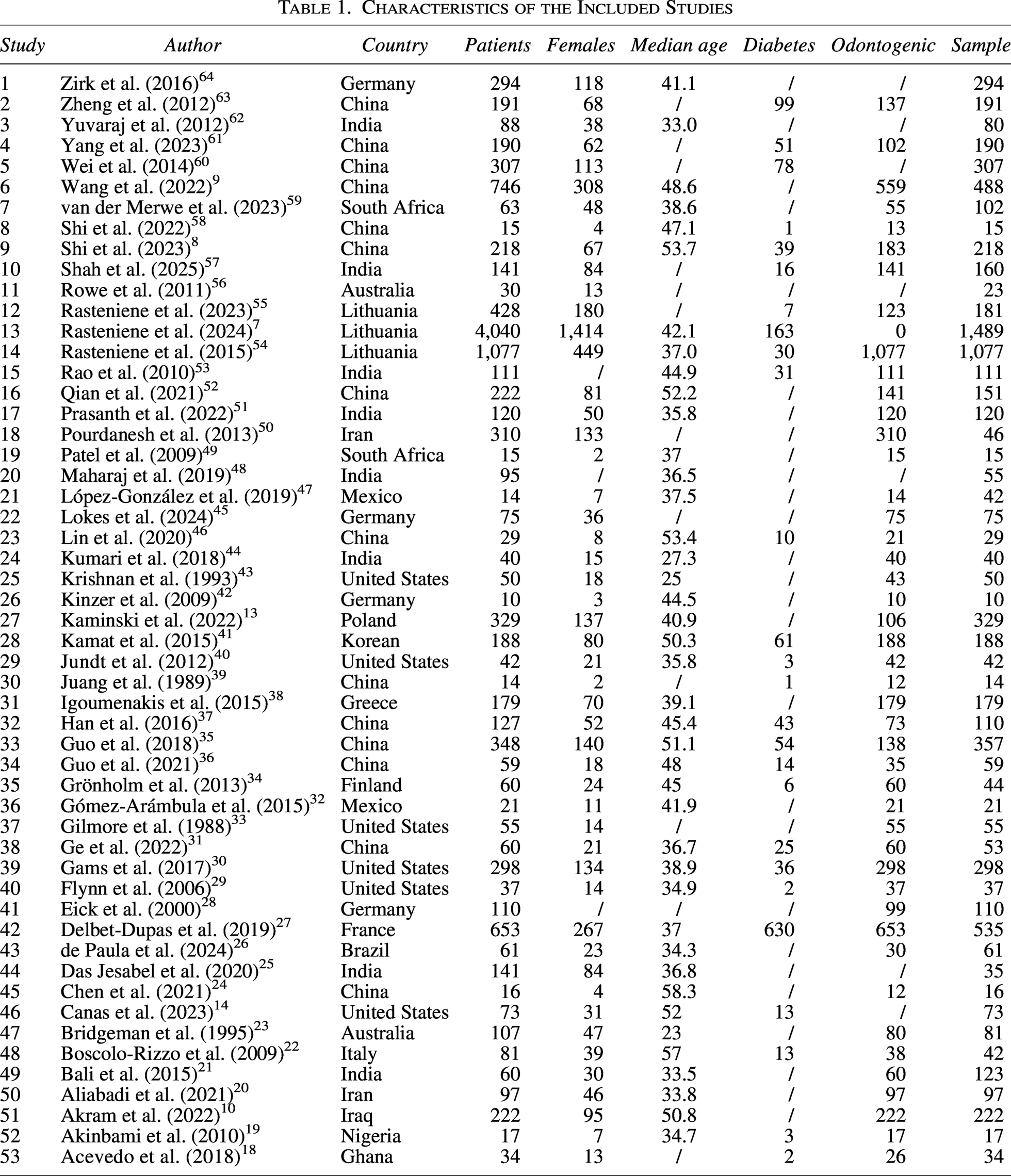
The 53 included studies were published between 1988 and 2025. The most frequent study locations were China (n = 14); India (n = 8); and the United States (n = 6), followed by Germany (n = 4); Lithuania (n = 3); Australia, Iran, Mexico, and South Africa (n = 2 each); and single reports from Poland, Iraq, Greece, France, Finland, Italy, Brazil, Nigeria, Ghana, and Korea (n = 1 each). These studies included 12,408 patients with confirmed OMSIs. The mean age was 41.31 ± 8.50 years, with 4,743 (38.23%) female participants. Odontogenic infections constituted the predominant etiology (89.69%; 95% CI: 88.94–90.41). Among 8,838 patients with documented medical histories, diabetes mellitus represented the most prevalent underlying comorbidity (19.95%; 95% CI: 12.10–29.10). Table 1 summarizes the characteristics of the included studies.
Characteristics of the Included Studies
All 53 included studies were assessed using the JBI Critical Appraisal Checklist for Prevalence Studies. Overall, the majority demonstrated appropriate sampling frames, recruitment strategies, sample sizes, and detailed descriptions of study participants and settings. However, 33 studies provided only minimal information on microbiological methods—typically stating that samples were “cultured” without detailing culture conditions or identification procedures. Although this limits comparability, the omission was not deemed sufficient to justify exclusion (Supplementary Data S2).
Synthesis of results
Microbiological testing protocols of OMSIs utilized two principal methodologies: purulent exudate cultures (48 studies)7,9,10,13,14,19–23,25–64 and nucleic acid amplification techniques (3 studies).8,24,58 The microbial profile revealed Streptococcus as the predominant pathogen (45.51%; 95% CI: 38.34–52.77), followed by anaerobic organisms including Prevotella (15.89%; 95% CI: 7.57–26.38) and Porphyromonas (15.61%; 95% CI: 1.69–38.33). Among aerobic isolates, Streptococcus viridans (29.65%; 95% CI: 20.90–39.19) was the most prevalent. Other isolates from OMSIs included S. aureus (9.03%; 95% CI: 5.77–12.86), coagulase-negative staphylococci (10.63%; 95% CI: 6.41–15.71), and gram-negative bacilli such as Klebsiella (7.56%; 95% CI: 4.73–10.90), Escherichia coli (4.14%; 95% CI: 1.09–8.54), and Pseudomonas (1.77%; 95% CI: 0.77–3.06). The forest plot in Figure 2 illustrates the prevalence data, with detailed information provided in Supplementary Data S3. Among 1,082 cultured samples, 34 S. aureus isolates were identified, including 8 MRSA isolates, corresponding to a prevalence of 0.23% (95% CI: 0.00–1.49) among all specimens. Among the S. aureus isolates, MRSA accounted for 19.18% (95% CI: 0.00–59.56).14,19,21,23,30,34,40,42,52,59
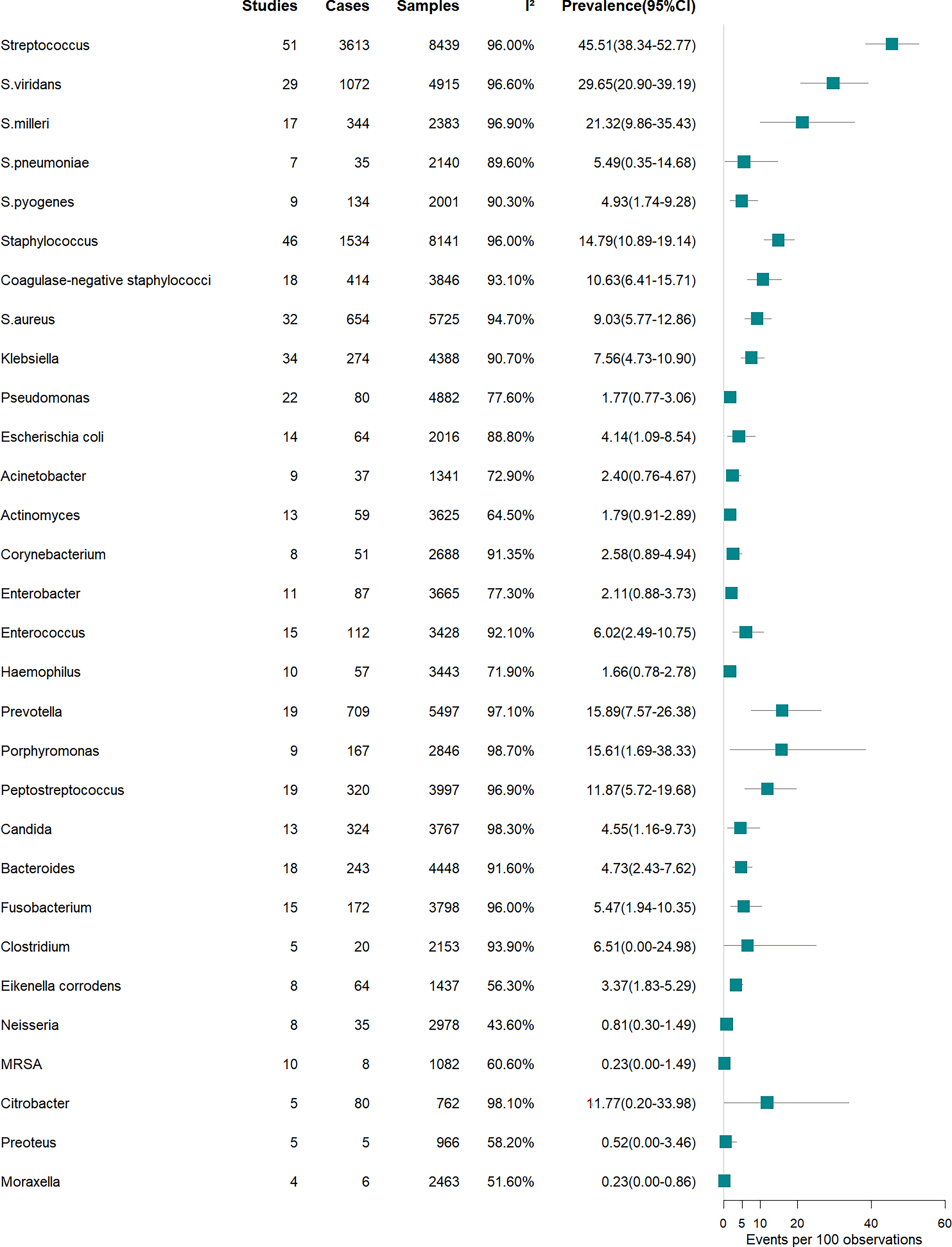
Prevalence of microorganisms in patients with oral and maxillofacial space infections. CI, confidence interval; MRSA, methicillin-resistant Staphylococcus aureus.
Nineteen included studies provided antimicrobial susceptibility profiles of pathogens isolated from OMSIs, with weighted pooled resistance rates across 11 antibiotics, ranging from 11.03% to 39.66% (Fig. 3, Supplementary Data S4). Levofloxacin demonstrated the lowest resistance rate (11.03%; 95% CI: 0.00–39.73), whereas β-lactam exhibited intermediate resistance: cephalosporin (16.83%; 95% CI: 3.44–37.01), ampicillin/amoxicillin (18.50%; 95% CI: 7.43–32.73), and amoxicillin/clavulanate (19.66%; 95% CI: 5.12–40.21). The highest resistance rates were observed for gentamicin (39.66%; 95% CI: 9.85–74.51), erythromycin (39.35%; 95% CI: 18.65–62.22), penicillin (26.72%; 95% CI: 16.69–38.05), metronidazole (28.29%; 95% CI: 13.68–45.65), and tetracycline (28.22%; 95% CI: 4.40–61.69).
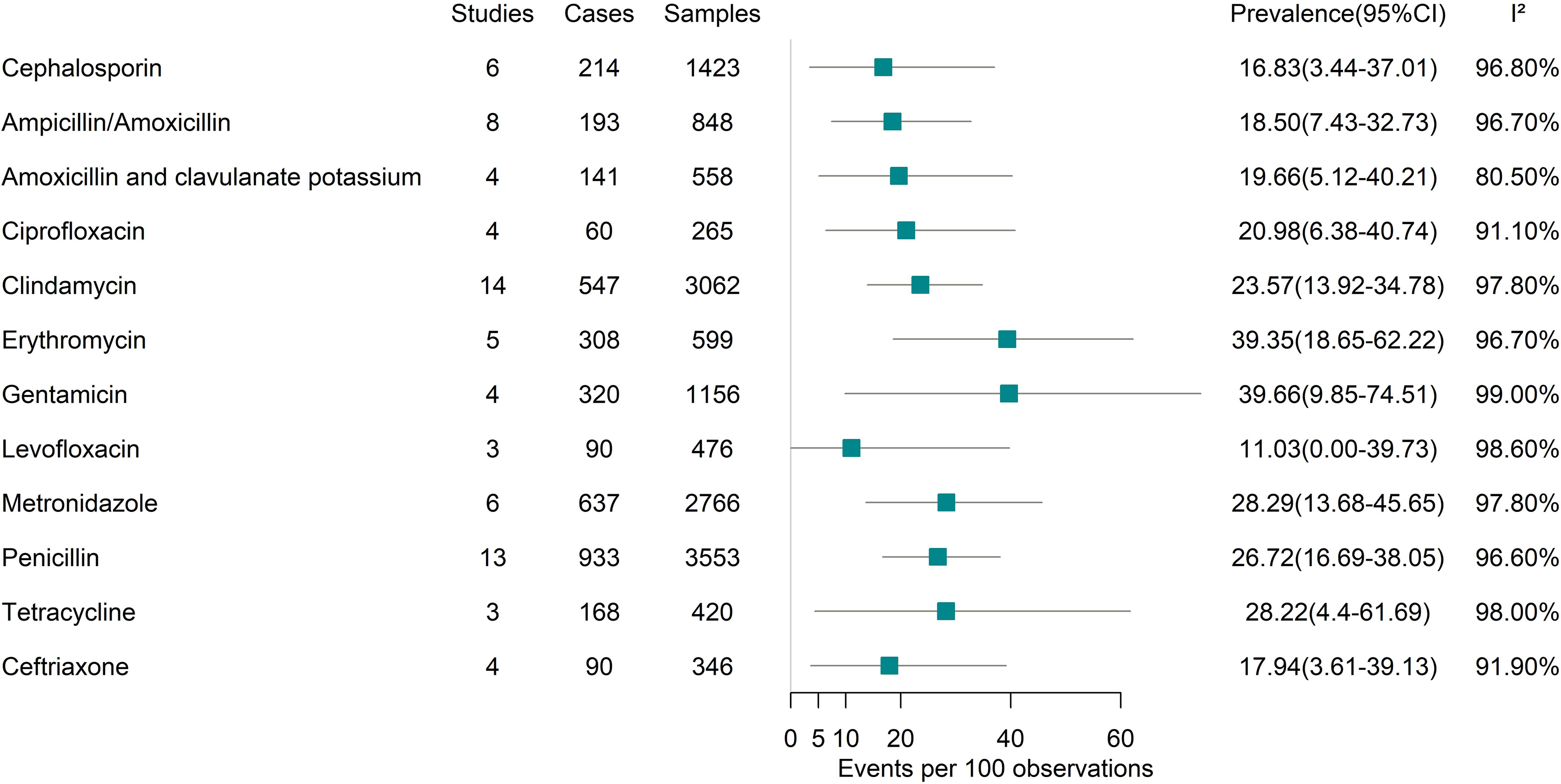
Forest plot for the antimicrobial resistance profiles of clinical isolates.
Subgroup analysis of microorganisms
Methods used for the identification of microorganisms
Studies employing NGS revealed that anaerobic bacteria including Prevotella (72.26%; 95% CI: 50.23–90.07), Porphyromonas (60.89%; 95% CI: 48.76–72.43), and Peptostreptococcus (54.05%; 95% CI: 20.34–85.94) were major pathogens in OMSIs. In contrast, culture-based methods reported substantially lower detection rates for Prevotella (9.30%; 95% CI: 5.63–13.70) and Peptostreptococcus (7.01%; 95% CI: 4.38–10.11) (Table 2).
Subgroup Analysis of Microorganisms in Patients with Oral and Maxillofacial Space Infections
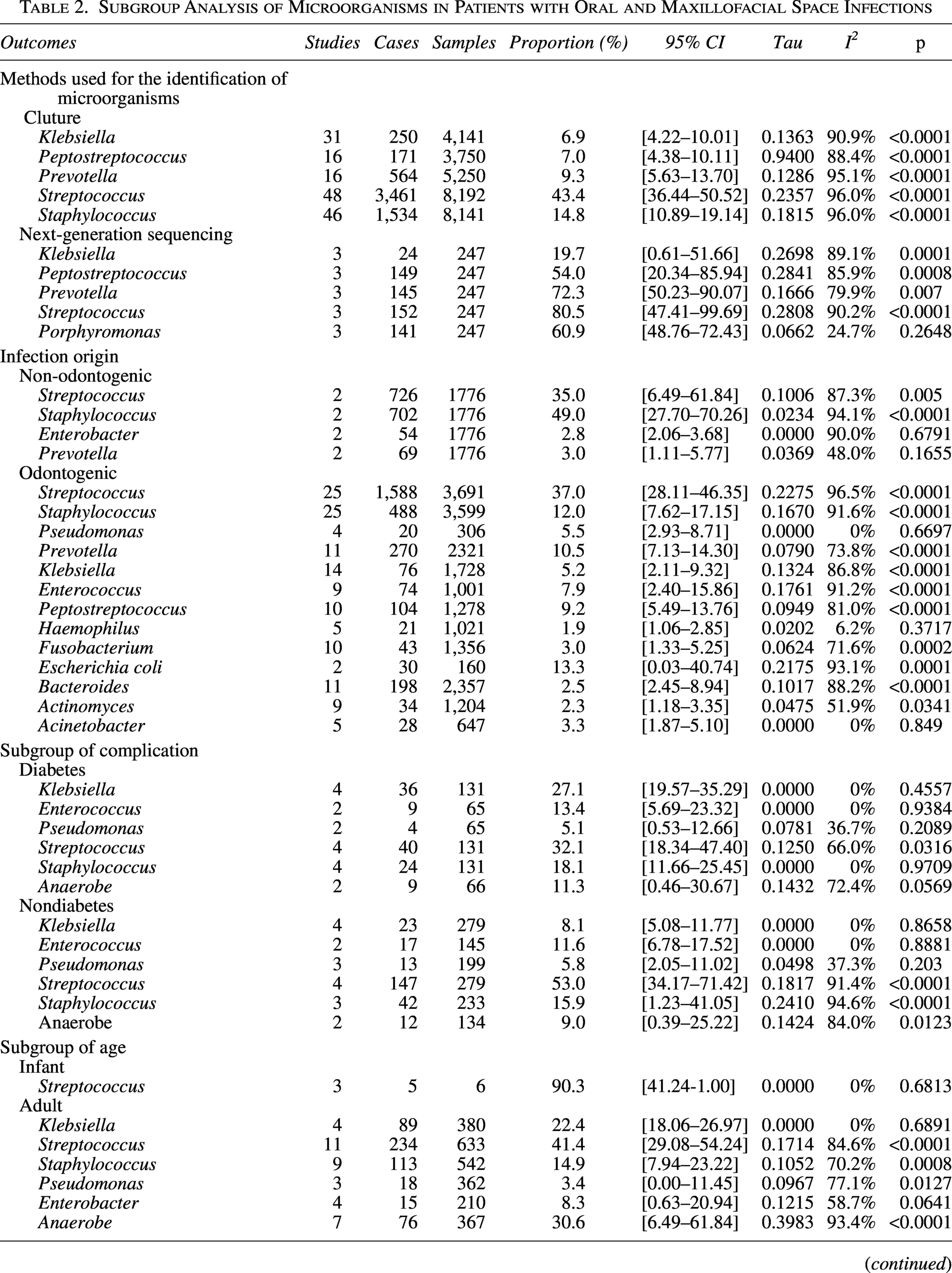
CI, confidence interval.
Odontogenic versus non-odontogenic OMSIs
In odontogenic cases, Streptococcus predominated (37.00%; 95% CI: 28.11–46.35), followed by Staphylococcus (12.01%; 95% CI: 7.62–17.15), Prevotella (10.46%; 95% CI: 7.13–14.30), Peptostreptococcus (9.24%; 95% CI: 5.49–13.76), Enterococcus (7.90%; 95% CI: 2.40–15.86), Pseudomonas (5.53%; 95% CI: 2.93–8.71), and Klebsiella (5.19%; 95% CI: 2.11–9.32). Non-odontogenic infections were primarily associated with Staphylococcus (48.88%; 95% CI: 27.70–70.26) and Streptococcus (34.97%; 95% CI: 6.49–61.84), and Prevotella was detected in a relatively limited proportion of isolates (3.04%; 95% CI: 1.11–5.77) (Table 2).
Diabetic versus nondiabetic patients
To evaluate the impact of diabetes, we performed a subgroup analysis comparing diabetic and nondiabetic patients. The results demonstrated a significantly higher prevalence of Klebsiella in OMSIs among diabetic patients (27.09%; 95% CI: 19.57–35.29) than in nondiabetic individuals (8.13%; 95% CI: 5.08–11.77) (Table 2).
National income level
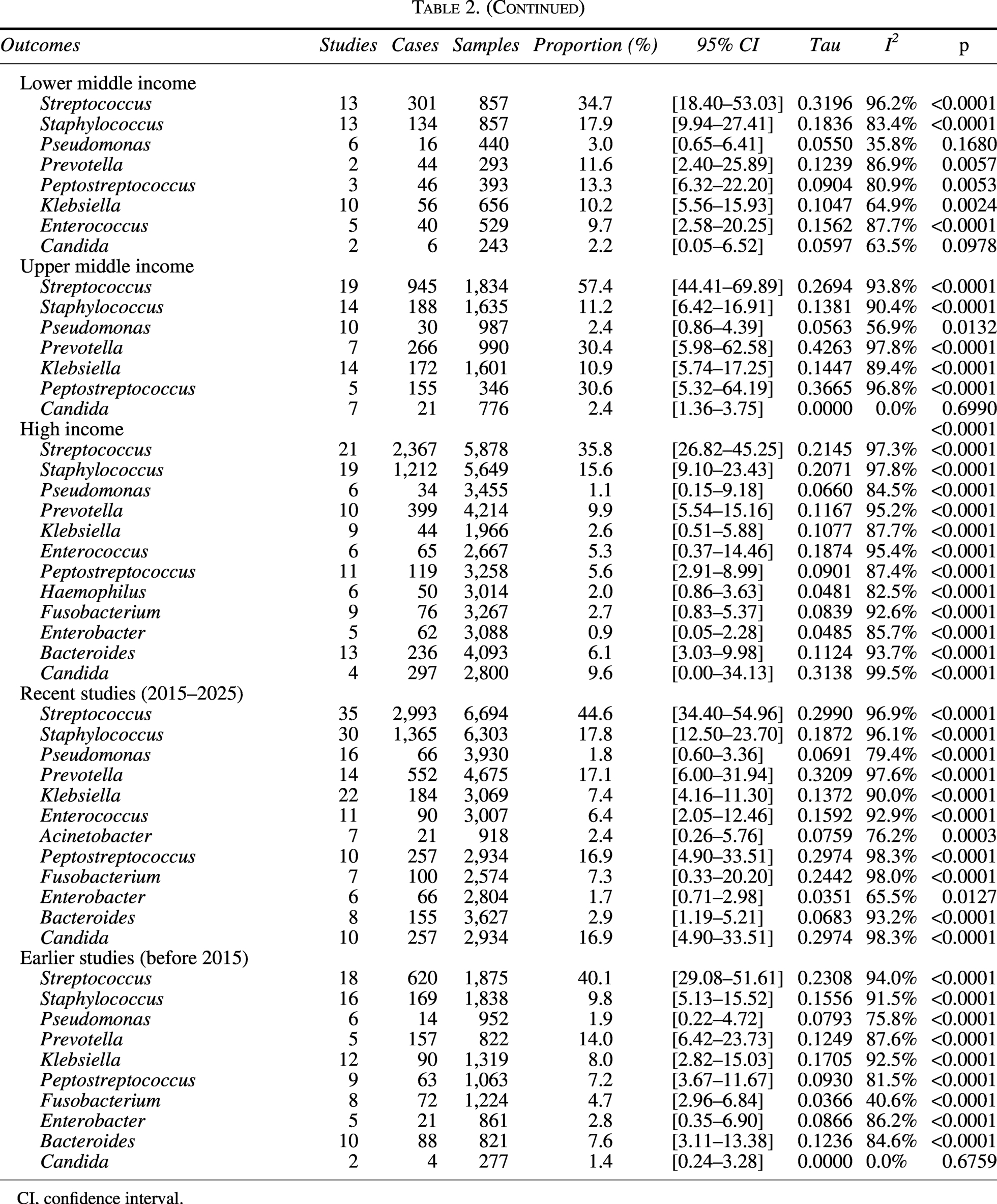
Klebsiella was more frequently reported in lower-middle-income (10.22%; 95% CI: 5.56–15.93) and upper-middle-income countries (10.90%; 95% CI: 5.74–17.25) than in high-income countries (2.60%; 95% CI: 0.51–5.88). In contrast, Candida was predominantly identified in high-income countries (9.55%; 95% CI: 0.00–34.13), with lower pooled prevalences in lower-middle-income (2.22%; 95% CI: 0.05–6.52) and upper-middle-income settings (2.44%; 95% CI: 1.36–3.75) (Table 2).
Time period
Subgroup analysis by publication period (before 2015 vs. 2015–2025) revealed notable temporal trends in the microbial etiology of OMSIs (Table 2). The pooled prevalence of Staphylococcus nearly doubled in recent studies (17.77%; 95% CI: 12.50–23.70) compared to earlier reports (9.76%; 95% CI: 5.13–15.52). Similarly, certain anaerobic bacteria showed higher detection rates in the recent period, including Peptostreptococcus (16.85%; 95% CI: 4.90–33.51 vs. 7.21%; 95% CI: 3.67–11.67) and Prevotella (17.06%; 95% CI: 6.00–31.94 vs. 14.01%; 95% CI: 6.42–23.73). Candida was markedly more prevalent in recent studies (16.85%; 95% CI: 4.90–33.51) than in studies published before 2015 (1.41%; 95% CI: 0.24–3.28).
Subgroup analysis of antimicrobial susceptibility
Antimicrobial susceptibility testing according to Clinical and Laboratory Standards Institute guidelines
Based on the subgroup analysis restricted to studies that adhered to Clinical and Laboratory Standards Institute (CLSI) guidelines for antimicrobial susceptibility testing, the highest pooled resistance was observed for erythromycin (53.30%; 95% CI: 27.45–78.25), followed by clindamycin (28.35%; 95% CI: 12.64–47.28) and penicillin (22.65%; 95% CI: 8.00–41.78). Resistance to ampicillin/amoxicillin was similarly high at 22.60% (95% CI: 8.10–41.48), whereas cephalosporins showed a lower resistance rate of 15.52% (95% CI: 2.47–36.06) (Table 3).
Subgroup Analysis of the Antimicrobial Resistance Profiles
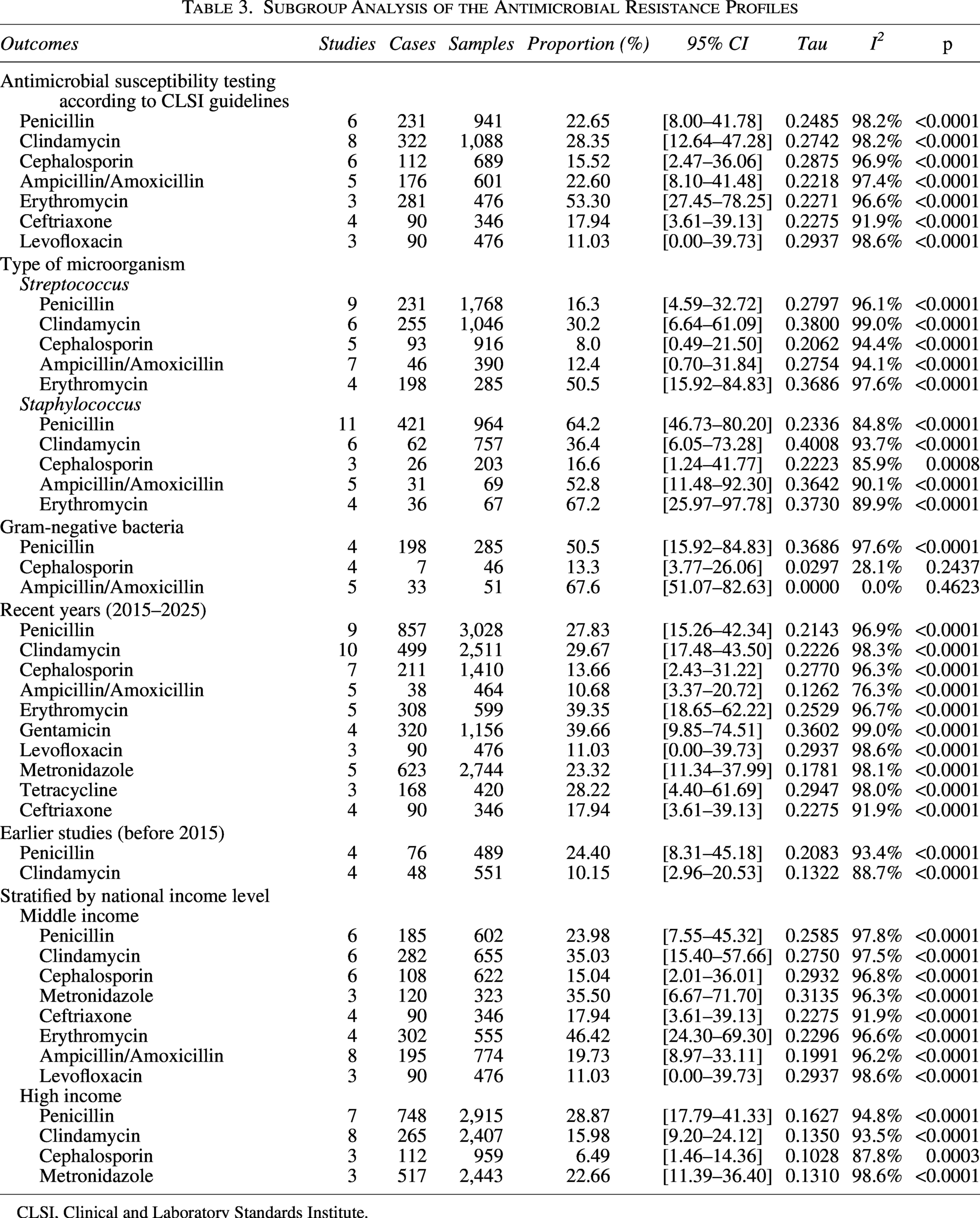
CLSI, Clinical and Laboratory Standards Institute.
Antibiotic resistance based on bacterial species
Subgroup analysis of antibiotic resistance patterns revealed species-specific profiles. Streptococcus exhibited pronounced resistance to erythromycin (50.51%; 95% CI: 15.92–84.83) and clindamycin (30.19%; 95% CI: 6.64–61.09), but remained susceptible to β-lactams, including penicillin (16.28%; 95% CI: 4.59–32.72), ampicillin/amoxicillin (12.42%; 95% CI: 0.70–31.84), and cephalosporins (7.95%; 95% CI: 0.49–21.50). Non-MRSA Staphylococcus showed high resistance rates to penicillin (64.22%; 95% CI: 46.73–80.20) and erythromycin (67.15%; 95% CI: 25.97–97.78), followed by ampicillin/amoxicillin (52.77%; 95% CI: 11.48–92.30) and clindamycin (36.43%; 95% CI: 6.05–73.28), while demonstrating greater susceptibility to cephalosporins (16.60%; 95% CI: 1.24–41.77). Gram-negative bacteria exhibited relatively low resistance to cephalosporins (13.29%; 95% CI: 3.77–26.06) (Table 3).
Antibiotic resistance patterns by publication period
Subgroup analysis by publication period revealed a significant increase in clindamycin resistance among OMSIs-associated pathogens in recent years (29.67%; 95% CI: 17.48–43.50) compared to the pre-2015 period (10.15%; 95% CI: 2.96–20.53). In contrast, penicillin resistance remained persistently high across both eras (27.83%; 95% CI: 15.26–42.34 in 2015–2025 vs. 24.40%; 95% CI: 8.31–45.18 before 2015). Resistance to erythromycin, gentamicin, and metronidazole was also substantial in recent studies; however, insufficient data from earlier publications precluded meaningful comparison with the pre-2015 era.
Antimicrobial resistance patterns by national income level
Subgroup analysis by national income level showed that resistance to clindamycin (35.03%; 95% CI: 15.40–57.66 vs. 15.98%; 95% CI: 9.20–24.12), metronidazole (35.50%; 95% CI: 6.67–71.70 vs. 22.66%; 95% CI: 11.39–36.40), and cephalosporins (15.04%; 95% CI: 2.01–36.01 vs. 6.49%; 95% CI: 1.46–14.36) was consistently higher in middle-income than in high-income countries. Notably, resistance to the third-generation cephalosporin ceftriaxone was reported exclusively in middle-income countries (17.94%; 95% CI: 3.61–39.13).
Risk of bias
Funnel plots (Supplementary Data S5) and Egger’s test (Supplementary Data S6) did not indicate significant publication bias for several microorganisms, including Streptococcus, Staphylococcus, Prevotella, S. aureus, coagulase-negative staphylococci, S. milleri, Enterobacter, Fusobacterium, Bacteroides, and Candida. In contrast, significant funnel plot asymmetry was observed for Haemophilus (p = 0.0447), Enterococcus (p = 0.0020), Actinomyces (p = 0.0334), E. coli (p = 0.0372), Pseudomonas (p = 0.0005), Klebsiella (p = 0.0014), S. viridans (p = 0.0072), Peptostreptococcus (p = 0.0343), and MRSA (p = 0.0400), suggesting a potential risk of publication bias for these nine microorganisms. Among antibiotics, no significant publication bias was detected for penicillin and clindamycin. For the remaining nine antibiotics, publication bias was not assessed due to an insufficient number of included studies (k < 10). To assess the influence of individual studies on the pooled estimates, we performed a leave-one-out sensitivity analysis. The results demonstrated that the effect estimates remained stable upon the sequential exclusion of each study (Supplementary Data S7 and S8), suggesting that our findings are not overly dependent on any single literature source.
Discussion
OMSIs may rapidly progress to life-threatening complications when polymicrobial pathogens disseminate through interconnected fascial planes. In the context of escalating global antimicrobial resistance, empirical therapy often relies on broad-spectrum antibiotics. In this systematic review and meta-analysis, we delineate the microbial epidemiology of OMSIs and characterize their associated antimicrobial resistance patterns, providing a foundation for more targeted and evidence-based antimicrobial strategies.
Our analysis reveals that OMSIs are typically characterized by polymicrobial infections featuring synergistic interactions between aerobic and anaerobic bacteria. Streptococcus—particularly the viridans groups—emerged as predominant aerobic pathogens, with Prevotella and Staphylococcus frequently isolated as co-pathogens. These findings are consistent with global surveillance data. 65 Our study shows that Streptococcus predominates in odontogenic OMSIs, whereas Staphylococcus are the primary pathogen in non-odontogenic infections, with a markedly lower prevalence of Prevotella in the latter. This pattern aligns with the established understanding of oral microbial ecology and the etiological specificity of infection sources.66,67 The detection rate of Klebsiella in diabetic patients was more than threefold higher than in nondiabetic patients, consistent with previous studies reporting an increased risk of Klebsiella infection in diabetic hosts.68,69 This finding suggests that empirical antimicrobial therapy in diabetic patients with OMSIs may warrant enhanced coverage against gram-negative organisms. However, it should be noted that few studies reporting on non-odontogenic OMSIs and diabetes were included in our analysis. This limited evidence base may affect the robustness and generalizability of findings for this subgroup, underscoring the need for additional high-quality studies to confirm these observations. Klebsiella was more frequently isolated in OMSIs in middle-income countries than in high-income countries, consistent with prior reports on regional disparities in the epidemiology of Klebsiella. 70 However, conventional culture-based techniques are prone to missing fastidious or unculturable anaerobes, which may lead to an underestimation of their true prevalence. It may therefore be beneficial for future research to explore the use of NGS to enable a more comprehensive and accurate characterization of the microbial landscape in OMSIs.
This study systematically evaluated the overall antimicrobial resistance profiles of 11 commonly used antibiotics based on data from 19 studies reporting antimicrobial susceptibility testing of pathogens isolated from OMSIs. The pooled resistance rate was lowest for levofloxacin (11.03%), whereas β-lactam antibiotics—including cephalosporins, ampicillin/amoxicillin, and amoxicillin/clavulanate—exhibited moderate resistance rates (16.83–19.66%). In contrast, substantially higher resistance was observed for gentamicin (39.66%), erythromycin (39.35%), metronidazole (28.29%), tetracycline (28.22%), and penicillin (26.72%). However, these findings should be interpreted with caution. Analyses for certain antibiotics—such as levofloxacin and tetracycline—were based on only three studies each. Moreover, heterogeneity exists across real-world settings due to variations in susceptibility testing methodologies, pathogen composition, and regional antibiotic prescribing practices, all of which contribute to uncertainty in the estimates. For example, non-MRSA Staphylococcus exhibited a markedly high penicillin resistance rate (64.2%), compared with only 16.3% in Streptococcus, a pattern highly consistent with the well-documented capacity of staphylococci to produce β-lactamase. 71 Additionally, clindamycin resistance increased significantly in the post-2015 period (29.67%) compared with the pre-2015 era (10.15%), further underscoring the dynamic evolution of antimicrobial resistance.72,73 Notably, metronidazole resistance was considerably higher in middle-income countries (35.50%) than in high-income countries (22.66%), likely reflecting prolonged and often unregulated use of this agent in resource-limited settings. 74 Antimicrobial therapy for OMSIs is facing increasingly complex resistance challenges. There is an urgent need to strengthen microbiological diagnostics, promote standardized susceptibility testing, and tailor empirical regimens according to infection origin, comorbidities, and national health care capacity.
Despite extensive subgroup analyses, high heterogeneity persisted across most subgroups—a common feature in prevalence-based meta-analyses with deep epidemiological and statistical roots. 75 First, real-world variability inherently drives heterogeneity: pathogen prevalence and resistance are shaped by time, geography, and population characteristics, further amplified by (1) evolving antimicrobial susceptibility testing methods and interpretive criteria over decades; (2) advances in microbiological diagnostics—from aerobic-only culture to anaerobic techniques and molecular methods (e.g., 16S ribosomal RNA sequencing)—which alter detection sensitivity and spectrum; (3) regional differences in antibiotic use that selectively enrich or suppress specific pathogens; (4) variations in patient demographics, comorbidities, and health care access; and (5) inconsistent sample collection protocols. Second, statistical properties of proportion data contribute to inflated I2: non-comparative prevalence estimates naturally yield high apparent heterogeneity even with modest absolute differences, unlike comparative effect measures. 75 Third, low I2 values in a few subgroups (e.g., Klebsiella prevalence in diabetic vs. non-diabetic patients, both I2 = 0%) should be interpreted cautiously—they stem from limited study numbers (k ≤ 5), where I2 lacks power to detect heterogeneity. 76 Notably, despite statistical homogeneity, the pooled prevalence differed more than threefold (27.1% vs. 8.1%), revealing underlying epidemiological divergence. In summary, the high heterogeneity observed is characteristic of prevalence-based meta-analyses. Future high-quality primary studies with standardized methods and stratified reporting by clinical and demographic factors are essential to improve the precision and generalizability of meta-analyses on prevalence.
In this study, publication bias concerning less common pathogens in OMSIs—such as Enterococcus, E. coli, Pseudomonas, Klebsiella, Haemophilus, and Actinomyces—likely stems from two interrelated factors. First, the majority of studies report these organisms as “not detected” and such negative findings are seldom published. Second, high-throughput sequencing can detect microbial DNA at extremely low abundances but cannot reliably distinguish between true infection, colonization, and contamination. This limitation may lead to overestimation of pathogen prevalence in the literature. The pooled prevalence of Peptostreptococcus was initially estimated at 11.87%. After the trim-and-fill analysis imputed 10 potentially missing studies, the adjusted estimate decreased to 2.26%. Similarly, the pooled prevalence of S. viridans was initially 29.0% and fell to 13.04% following the imputation of 13 studies. However, this apparent “overestimation” likely reflects the fact that our meta-analysis only included studies that explicitly identified and reported these organisms at the species level. In practice, many studies that detected such bacteria may have reported them under broader categories—such as “anaerobic gram-positive cocci” or “streptococci”—or used updated taxonomic names (e.g., Parvimonas or S. anginosus). Consequently, these cases would be difficult to capture with our search and extraction strategy. Therefore, the true burden of these common oral microbes in OMSIs is likely underestimated in the existing literature.
Although MRSA remains a major global health threat,77,78 our analysis reveals a low burden of MRSA in OMSIs. Among 1,082 cultured specimens, only 8 MRSA isolates were identified (0.23%; 95% CI: 0.00–1.49),14,19,21,23,30,34,40,42,52,59 a finding consistent with the recommendations in references79,80 that routine empirical anti-MRSA therapy is generally unnecessary for most OMSI patients in the absence of specific risk factors. Nevertheless, when restricted to S. aureus isolates, the MRSA proportion was 19.18% (95% CI: 0.00–59.56). Thus, in cases of Ludwig’s angina where Gram staining shows gram-positive cocci in clusters, adding vancomycin—as suggested by the Sanford Guide to Antimicrobial Therapy—remains a reasonable precautionary measure. 81 It should be noted that MRSA epidemiology exhibits heterogeneity across regions and settings, and clinical decisions should also be guided by local antimicrobial resistance patterns and institutional surveillance data.
Conclusion
This systematic review suggests that OMSIs are generally polymicrobial, with Streptococcus, Staphylococcus, and Prevotella among the pathogens most frequently identified. Levofloxacin and cephalosporins appear to have the lowest resistance rates among the antimicrobial agents evaluated, whereas penicillin, erythromycin, and metronidazole tend to show higher resistance rates. MRSA remains uncommon in OMSIs, consistent with current guidance advising against routine anti-MRSA therapy. A higher prevalence of Klebsiella has been observed in diabetic patients, which may indicate a potential need for broader gram-negative coverage in this group; however, this finding is based on a limited number of included studies, and further high-quality prospective research across different geographic regions would be helpful to better understand this association. In light of geographic variation in resistance patterns, limited susceptibility data for antibiotics, and heterogeneity across studies, empirical antibiotic choices might best be informed by antibiograms, the likely source of infection, and relevant comorbidities. Conventional culture-based methods may underestimate fastidious or unculturable anaerobes; therefore, future high-quality, population-based studies should prioritize integrating NGS with traditional methods to enable a more comprehensive understanding of the polymicrobial epidemiology of OMSIs and to inform evidence-based empirical antibiotic strategies in diverse clinical settings.
Authors’ Contributions
Y.L. conceived and designed the study, analyzed the data, wrote the article, and reviewed the article. L.Y. and C.W. analyzed the data and reviewed the article. All authors read and approved the final article.
Footnotes
Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
The authors declare that no funds, grants, or other support were received during the preparation of this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.