
Abstract
Carbapenem-resistant Enterobacterales (CRE), particularly carbapenemase-producing CRE (CP-CRE) are a growing global threat in health care. Intestinal colonization increases infection risk and facilitates transmission in the hospital. We aimed to determine intestinal colonization of CRE and CP-CRE among hospitalized patients in Addis Ababa, Ethiopia. A longitudinal study was conducted on 165 patients from February 2023 to April 2024 at Tikur Anbessa Specialized Hospital. Microbial identification and antimicrobial susceptibility testing were done using VITEK 2. Carbapenemase production was confirmed using the modified carbapenem inactivation method, and Polymerase Chain Reaction (PCR) was used to detect carbapemase genes. CRE colonization was detected in 19.4% of patients at admission and 18.8% during follow-up, showing no significant change (p = 0.65). CP-CRE colonization was increased from 10.3% at admission to 16.4% (p = 0.03) during follow-up. The most frequently identified genes were blaNDM (71.0%) and blaOXA-48 (53.0%) at admission. These genes were detected in (74.1%) and (48.1%) during follow-up, respectively. A substantial burden of CRE and CP-CRE colonization was found, with a high persistence rate. Screening high-risk patients and strengthening infection prevention measures are urgently needed.
Introduction
The emergence of carbapenem-resistant Enterobacterales (CRE) represents a significant public health concern, as carbapenems are often considered the last-resort treatment choice in treating severe bacterial infections. 1 Hospitalized patients are particularly at risk of CRE infection due to their weakened immune systems. 2 These infections frequently result from asymptomatic colonization of the gut by carbapenem-resistant Escherichia coli and Klebsiella pneumoniae or through the transmission of these bacteria between patients. Such infections are associated with prolonged hospital stay, frequent antibiotic use, chronic diseases, and invasive procedures. 3 Most CRE infections are caused by carbapenemase-producing carbapenem resistant Enterobacterales (CP-CRE). 4 Carbapenemases are enzymes that confer resistance, encoded by mobile genetic elements capable of spreading between bacterial species. Notable carbapenemases include K. pneumoniae carbapenemase-producing (blaKPC), New Delhi metallo-beta-lactamase (blaNDM), oxacillinases (blaOXA-48-like), Verona-encoded integron metallo-beta-lactamase (blaVIM), and imipenemase (blaIMP). 5
Fecal carriage of carbapenem-resistant E. coli and K. pneumoniae is frequently reported in health care settings worldwide, posing significant challenges to clinical management. 6 Studies in Ethiopia have reported CP-CRE fecal carriage rates of 2%, 7 13.6%, 8 and 7%. 9 However, data regarding phenotypic and genotypic characterization of CRE and CP-CRE intestinal colonization among patients at the time of admission and during their hospital stay are scarce in Ethiopia. Therefore, this study aimed to determine intestinal colonization of CRE and CP-CRE using both phenotypic and genotypic methods among patients at admission and after 14 days of hospitalization in Addis Ababa, Ethiopia.
Materials and Methods
Study design and setting
A longitudinal cohort study was carried out at Tikur Anbessa Specialized Hospital (TASH) from February 2023 to April 2024. TASH is the largest specialized teaching hospital in Addis Ababa, Ethiopia. TASH has over 800 beds and provides diagnostic and treatment services for more than 500,000 patients annually.
Study population, sample size, and sampling procedure
We included patients ≥18 years old admitted to internal medicine ward. Patients who were unable to give a specimen, such as critically ill patients were excluded from the study. Patients admitted with a variety of clinical conditions, including neurological disorders, cardiovascular disease, and hematological abnormalities, were included. The majority of the patients were referral cases from multiple regions of the country. The sample size was calculated using the two dependent proportion formula by considering the previous prevalence at admission (50%) and during hospitalization (65%) in Rwanda.
10
With a 5 margin of error, Zα/2 = 1.96 and Zβ = 0.84.

Patients were recruited using systematic random sampling. Based on hospital records, 624 patients were admitted to internal medicine wards in the past 6 months (used as a sampling frame). The sampling interval was K = N/n = 624/184 = 3. A random start was chosen from the first three admissions, and every third patient was subsequently enrolled until the desired sample size was achieved (Supplementary Data S1).
Data collection
A structured questionnaire was used to collect clinical and demographic data from study participants (Supplementary Data S2). The recorded information included age, sex, underlying conditions, duration of hospitalization, and number of beds in a single room, presence of invasive medical devices, previous antibiotic exposures, and previous admission history. Hospital-acquired infection (HAI) was defined as infection occurring ≥48 hours after admission.
Specimen collection
After obtaining written consent from each participant, a data collector conducted interviewer-led interviews using a questionnaire in the Amharic language. Fresh fecal specimens (formed, soft, or diarrheal), each weighing about 2g, were collected from patients using sterile containers at admission and after 14 days of hospitalization. Approximately 1 g of each fecal sample was transferred into a Cary–Blair transport medium and delivered to the Ethiopian Public Health Institute (EPHI) within 4 hours of collection, maintaining a temperature range of 2°C–4°C.
Bacterial isolation and identification
Fecal samples were inoculated on MacConkey agar and incubated aerobically at 35°C–37°C for 24 hours. Colonies were characterized based on their morphology, and pure colonies were subcultured on tryptic soya agar and subjected to biochemical tests, including indole, urease, oxidase, citrate, lysine, mannitol, and triple sugar iron. In addition, bacterial identification was performed by the VITEK 2 Compact system (bioMe′rieux, France) with Gram-negative bacteria identification cards. Briefly, 3–5 bacterial colonies were suspended in 3.0 mL of sterile saline and adjusted to a 0.50 McFarland standard.
Antimicrobial susceptibility testing
The tested antimicrobials included ampicillin, amoxicillin-clavulanic acid, ampicillin/sulbactam, cefazolin, ceftazidime, ceftriaxone, cefepime, ertapenem, imipenem, gentamicin, ciprofloxacin, tobramycin, nitrofurantoin, trimethoprim-sulfamethoxazole. Antimicrobial susceptibility testing (AST) was performed using VITEK 2 AST-GN cards. A 0.50 McFarland suspension prepared from 3 to 5 colonies was used, and the results were interpreted according to CLSI protocol. 11
Phenotypic detection of carbapenemase production
All isolates non-susceptible to imipenem and/or ertapenem were tested for carbapenemase production by modified carbapenem inactivation method. 11 About 1–4 loops full of isolates were suspended in 2 mL of tryptic soy broth, and a 10 μg meropenem disk was submerged in each tube and incubated at ambient temperature for 4 hours ± 15 minutes. ATCC25922 E. coli isolates were suspended in sterile saline solution and adjusted for an equivalent 0.50 McFarland standard and spread onto Mueller–Hinton agar. Then, meropenem was placed on Mueller–Hinton agar and incubated at 35°C ± 2°C for 18–24 hours, after which the result was interpreted based on CLSI 2023 guideline. 11 A measure of inhibition zone with a diameter of 6–15 mm or pinpoint colonies was considered positive for carbapenemase enzyme production, and a zone of inhibition ≥19 mm was considered to be negative for carbapenemase enzyme production.
Molecular detection of CP-CRE genes
DNA extraction and amplification
DNA was extracted from all CRE isolates using the boiling lysis method. 24 A loop-full of fresh colonies was suspended in 100 µL Tris–acetate–ethylenediaminetetraacetic acid (EDTA) buffer and heated at 100°C for 10 minutes, and centrifuged at 14,000 g for 5 minutes. About 50 µL of the supernatant was transferred into a nuclease-free Eppendorf tube and stored at −20°C.
PCR was used to detect CP-CRE encoding genes at Armauer Hansen Research Institute (AHRI), Addis Ababa, Ethiopia, using protocols from the previous study. 12 CP-CRE genes were detected using three multiplex reactions: carba group-1 multiplex (blaKPC blaNDM, blaOXA, blaBIC), carba group-2 multiplex (blaVIM, blaSPM, blaIMP), and carba group-3 multiplex (blaAIM, blaGIM, blaSIM, blaDIM).
Amplification reactions were performed in a final volume of 25 μL containing 12.5 μL 2× Tag plus PCR Master Mix (Thermo Scientific, Lithuania, EU), 1 μL of DNA primers (0.5 μL forward plus 0.5 μL reverse), 5.5 μL of nuclease-free water, and 5 μL of the template DNA. Then, DNA was denatured at 95°C for 5 minutes, followed by 40 cycles of 95°C for 20 seconds, 61°C for 30 seconds, and 72°C for 1 minute, and a final extension of 72°C for 7 minutes. After PCR amplification, 2.5 μL of each reaction was used to separate the individual amplicons by gel electrophoresis in 1.5% agarose gel. CP-CRE genes were detected using specific primers as indicated in Supplementary Data S3. 12
Quality control
ATCC 25922 E. coli and ATCC 700603 K. pneumoniae were used as negative and positive control strains, respectively, based on CLSI guidelines. 11 K. pneumoniae ATCC BAA-1705 and K. pneumoniae ATCC BAA-1706 strains were used as positive and negative quality controls, respectively, to check the quality of antibiotic disks. Known E. coli and K. pneumoniae strains carrying blaKPC, blaNDM, and blaOXA-48 genes were used for antibiotic resistance gene detection.
Ethical approval
This study was reviewed and approved by the Institutional Review Board of the College of Health Science, Addis Ababa University (Protocol number 072/22/DMIP). A permission letter was obtained from TASH. Written informed consent was obtained from the study participants before sample collection. The aim of the study, the study procedures, possible risks/benefits, and the right to withdraw from the study at any time were explained to the study participants. This study was carried out based on the Declaration of Helsinki.
Statistical analysis
All data were entered into Microsoft Excel 2016 and exported to SPSS version 25 (IBM Corporate, USA). Descriptive statistics such as frequencies and percentages were used to summarize the magnitude of gut colonization. The detection rate of bacterial isolates and the associated factors of CRE colonization were determined using a binary logistic regression model. McNemar’s test was used to compare the proportions of CRE at admission and during hospitalization. p Value less than 0.05 is considered statistically significant.
Result
Sociodemographic characteristics
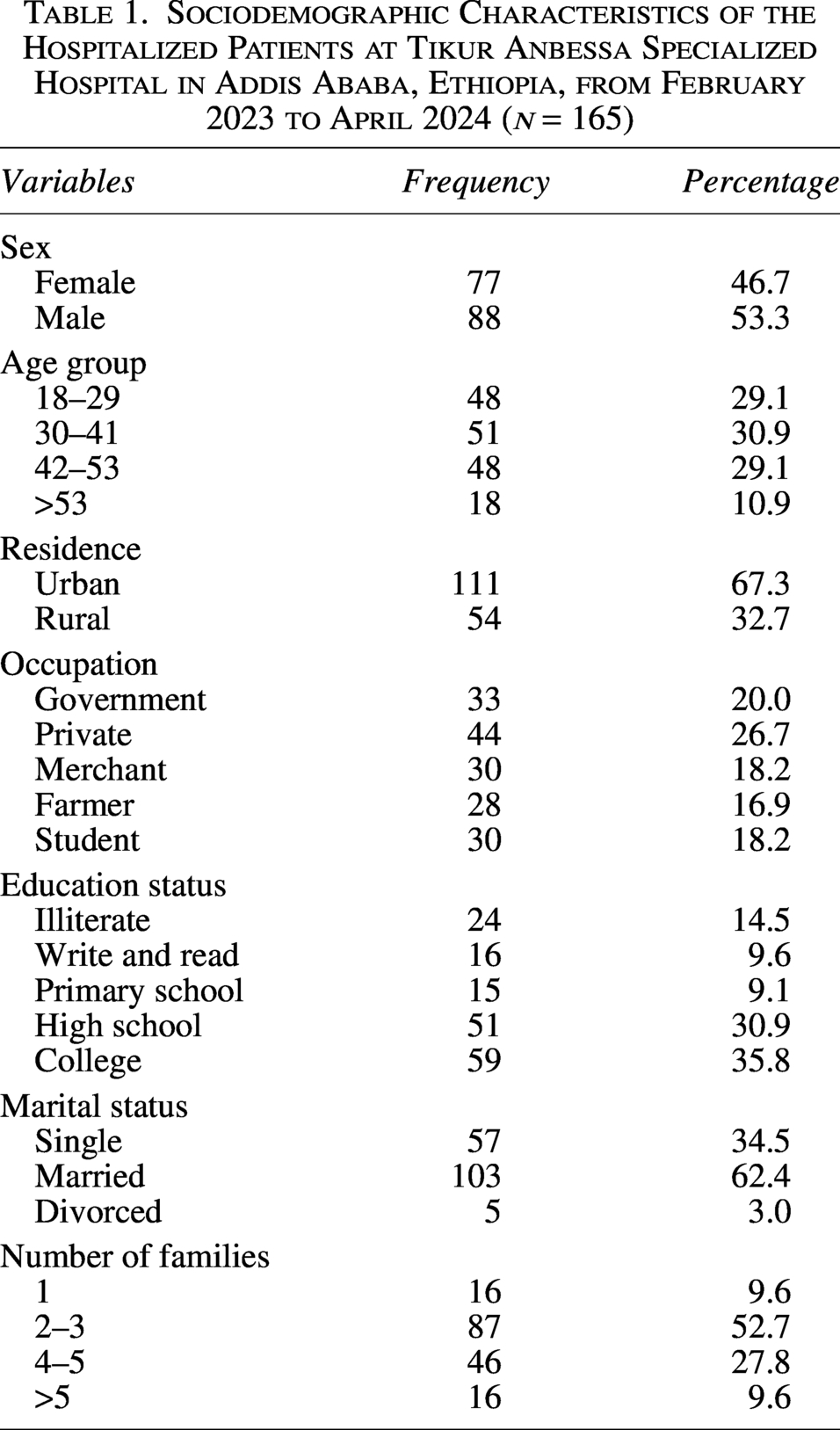
Among the 184 study participants enrolled in the study, 89.7% (165) gave fecal samples both at admission and after 14 days of hospitalization. No response rate was recorded at 10.3% (19/184)′ 9 patients due to early discharge, 8 patients refused to participate, and 2 patients died. The majority of the study participants were males, 53.3% (88/165). The median age of the study participants was 38 (ranging from 18 to 63 years old) (Table 1).
Sociodemographic Characteristics of the Hospitalized Patients at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, from February 2023 to April 2024 (n = 165)
Clinical characteristics of study participants
The majority of medical wards were allocated for hematological patients, and there was also a case mix in the medical ward during the study period. Accordingly, the majority of admitted patients had acute lymphoid leukemia, 33.3% (55/165), followed by acute myeloid leukemia, 21.8% (36/165), and cardiac disease, 8.5% (14/165), as the primary cause of admission in the hospital (Fig. 1).
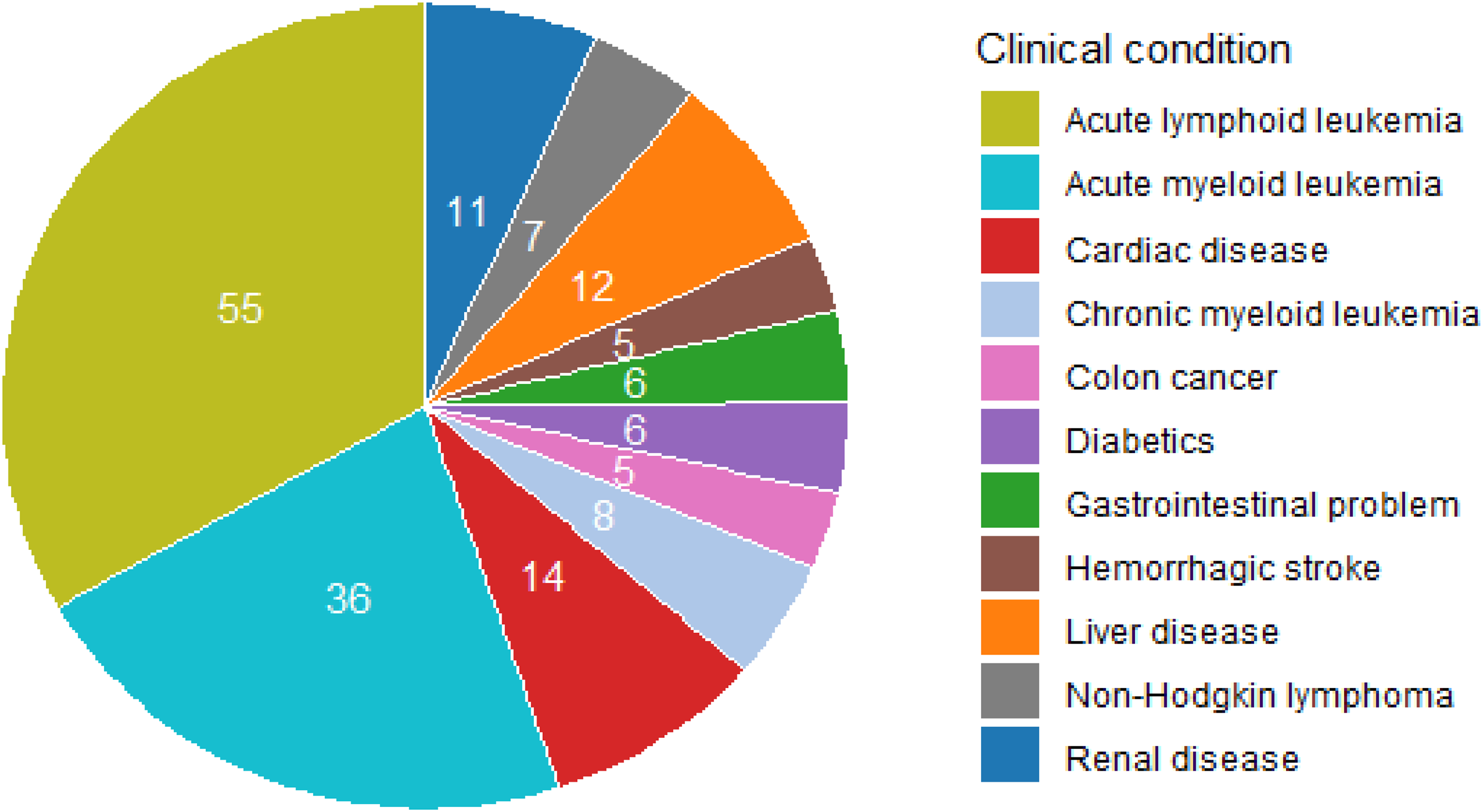
Number of cases among hospitalized patients based on clinical conditions at Tikur Anbessa Specialized Hospital from February 2023 to April 2024 (n = 165).
Frequency of Enterobacterales
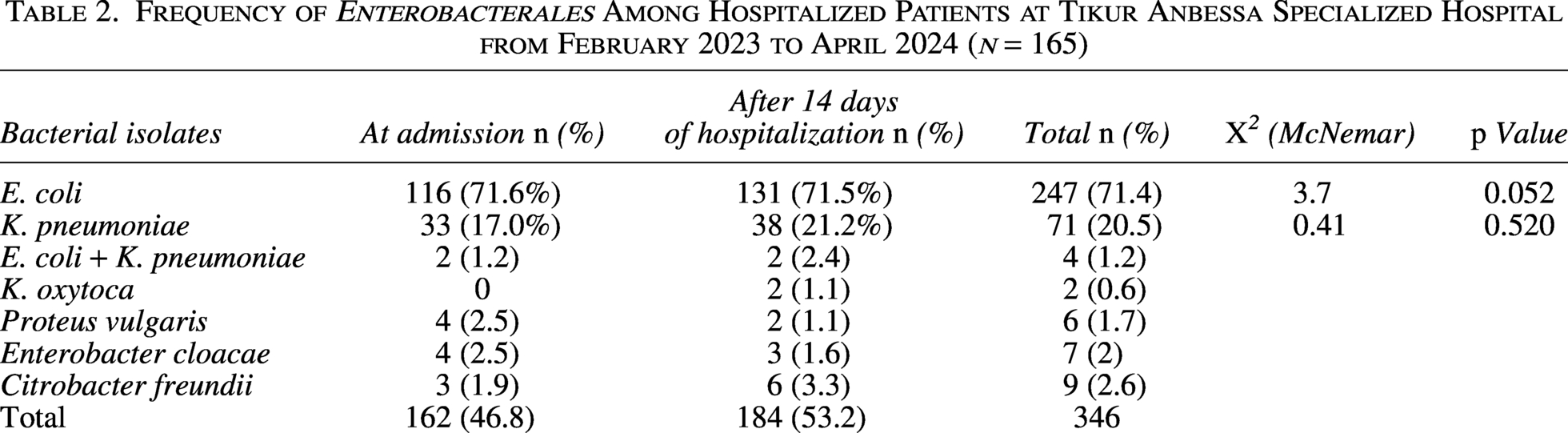
A total of 346 Enterobacterales were isolated from 330 stool samples collected, both at the time of admission and after 14 days of hospitalization. The most frequently isolated bacterium at both time points was E. coli, accounting for 71.6% (116/162) of isolates at admission and 71.2% (131/184) at day 14 of hospitalization. Among 131 E. coli isolates detected after 14 days of hospitalization, 25.9% (34/131) were newly acquired, while 74.0% (97/131) were persistent, showing no significant change (p = 0.052). The second most common bacterium was K. pneumoniae, 20.3% (33/162) at admission and 20.6% (38/184) after 14 days of hospitalization. Of the 38 K. pneumoniae isolates at day 14, 58% (22/38) were newly detected, while 42.0% (16/38) isolates were persistent at the two sampling time points (p = 0.520) (Table 2).
Frequency of Enterobacterales Among Hospitalized Patients at Tikur Anbessa Specialized Hospital from February 2023 to April 2024 (n = 165)
Frequency of CRE and CP-CRE
A total of 63 CRE isolates were identified, 18.2% (63/346), where 32 of them were detected at admission and 31 after 14 days of hospitalization. Carbapenem-resistant E. coli was 52.0% (22/42) and 48.0% (20/42) at admission and after 14 days of hospitalization, respectively. Carbapenem-resistant K. pneumoniae was detected at admission in 48.0% (10/21) and 52.0% (11/21) after 14 days of hospitalization. Among the 42 carbapenem-resistant E. coli, 66.7% (28/42) were CP-CRE. Likewise, among the 21 carbapenem-resistant K. pneumoniae, 76.0% (16/21) were CP-CRE (Fig. 2). The gel electrophoresis analysis reveals the PCR amplification products of CP-CRE encoding genes (Fig. 3).
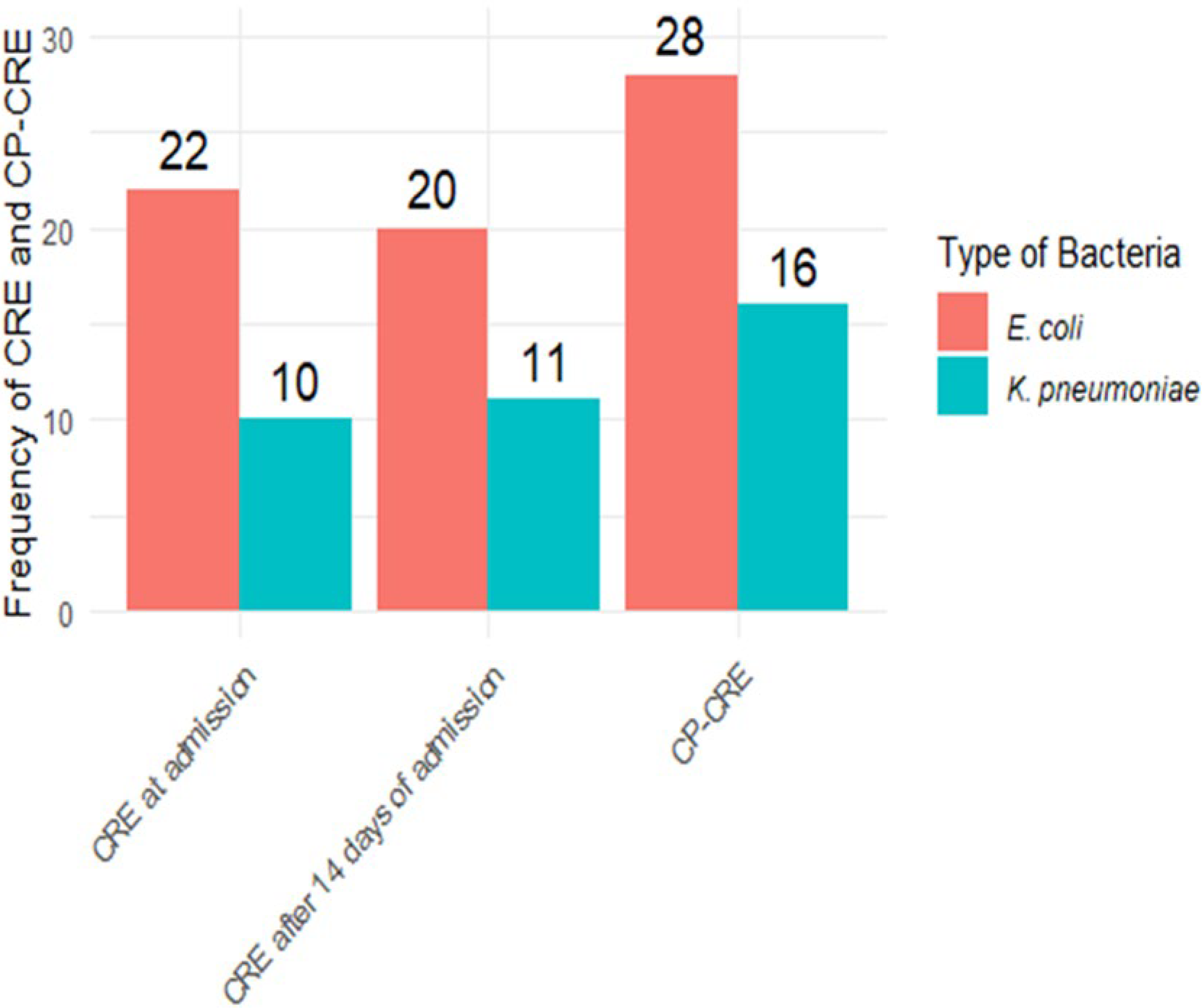
Frequency of CRE among hospitalized patients at admission and after 14 days of admission, and of CP-CRE at both time points at Tikur Anbessa Specialized Hospital from February 2023 to April 2024 (n = 165). CP-CRE, carbapenemase-producing carbapenem-resistant Enterobacterales.
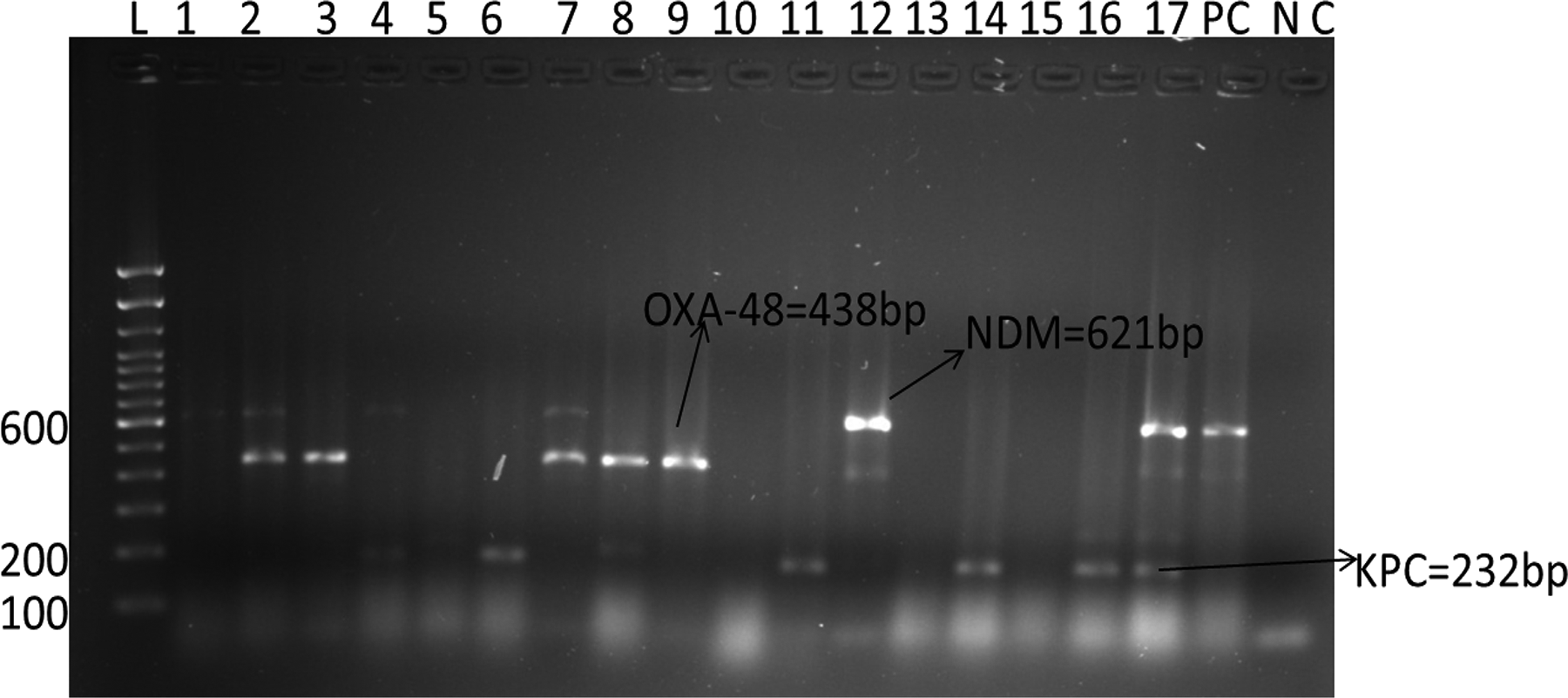
Gel electrophoresis image of blaOXA-48, blaNDM, and blaKPC in E. coli and K. pneumoniae among hospitalized patients at Tikur Anbessa Specialized Hospital from February 2023 to April 2024 in Addis Ababa, Ethiopia (n = 165). Numbers 1–17 indicate the patients’ ID. bp, base pair; L, ladder; NC, negative control; PC, positive control.
Colonization, acquisition, and persistence of CRE among hospitalized patients
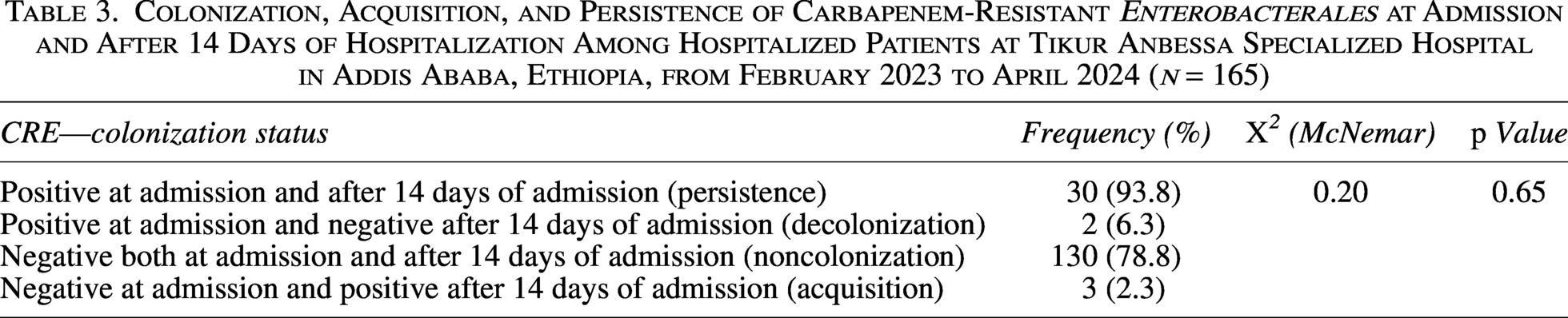
CRE colonization was found at admission in 19.4% (32/165) and 18.8% (31/165) after 14 days of hospitalization. Three patients who were negative at admission became positive after 14 days of hospitalization, 2.3% (3/133). Thirty patients remained colonized with CRE at both time points, 93.8% (30/32), while two patients who were colonized with CRE at admission were negative after 14 days of hospitalization. McNemar’s test showed no significant difference in CRE colonization status between admission and after 14 days of hospitalization (X2 = 0.2, p = 0.65) (Table 3).
Colonization, Acquisition, and Persistence of Carbapenem-Resistant Enterobacterales at Admission and After 14 Days of Hospitalization Among Hospitalized Patients at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, from February 2023 to April 2024 (n = 165)
Antimicrobial susceptibility profile of carbapenem-resistant E. coli and K. pneumoniae
All carbapenem-resistant K. pneumoniae isolates (100% [10/10]) were resistant to ceftazidime and ceftriaxone at both time points. Similarly, carbapenem-resistant E. coli isolates were resistant to ceftazidime at the rate of 100% (22/22) and 95.0% (19/20) on admission and after 14 days of hospitalization, respectively.
Furthermore, carbapenem-resistant E. coli and K. pneumoniae were highly resistant to gentami at admission at the rate of 77.2% and 80.0%, respectively. However, after 14 days of hospitalization, these rates changed to 90.0% and 82.0%, respectively. High resistance rate of carbapenem-resistant E. coli and K. pneumoniae to sulfonamides was observed at 81.8% and 90.0%, respectively, at admission, whereas the rates remained more-or-less similar after 14 days of admission at 85.0% and 91.0%, respectively (Table 4).
Antimicrobial Resistance in Carbapenem-Resistant Enterobacterales and Klebsiella pneumoniae on Admission and During 14 Days of Hospital Stay Among Hospitalized Patients at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, from February 2023 to April 2024 (n = 165)
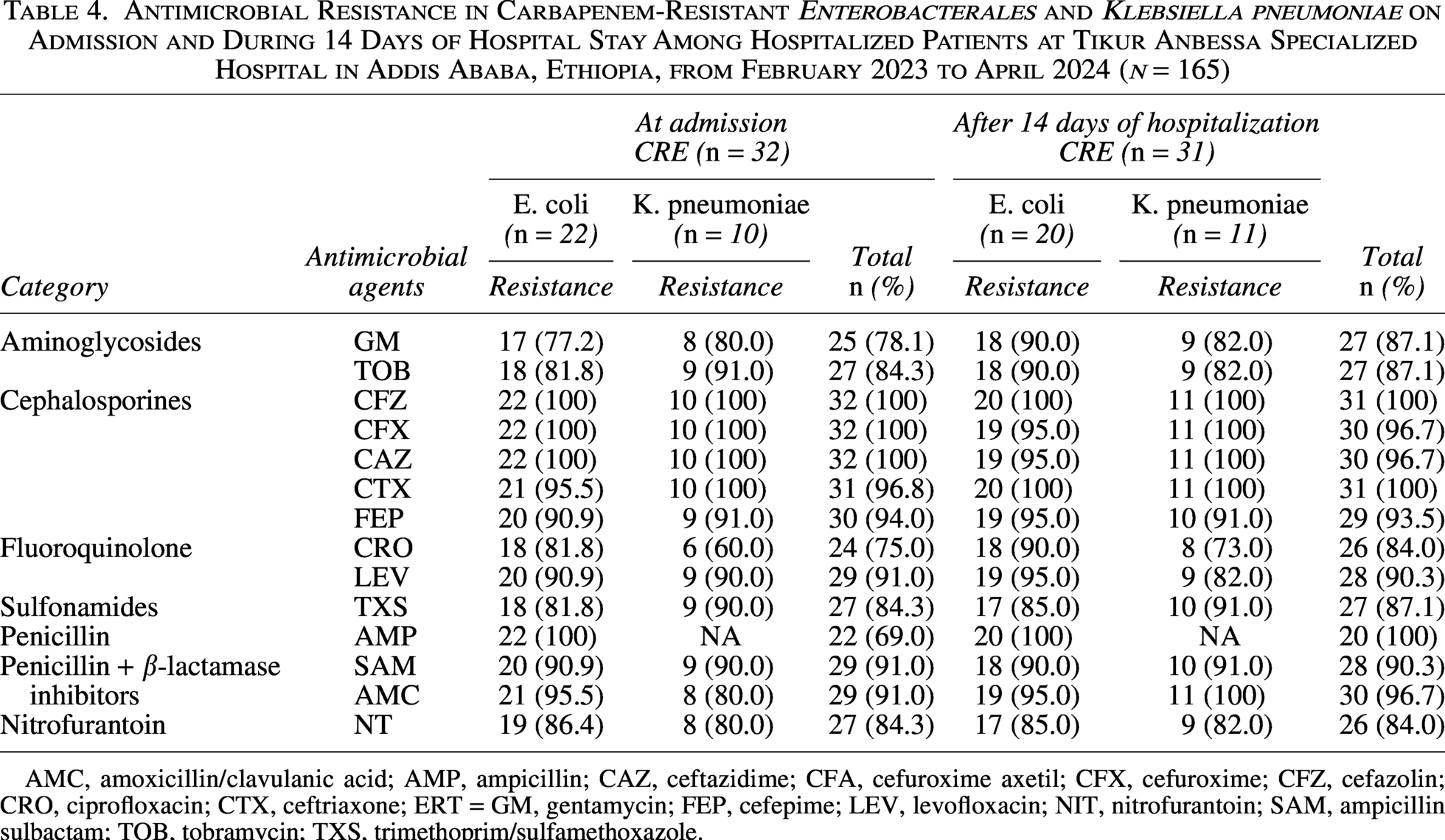
AMC, amoxicillin/clavulanic acid; AMP, ampicillin; CAZ, ceftazidime; CFA, cefuroxime axetil; CFX, cefuroxime; CFZ, cefazolin; CRO, ciprofloxacin; CTX, ceftriaxone; ERT = GM, gentamycin; FEP, cefepime; LEV, levofloxacin; NIT, nitrofurantoin; SAM, ampicillin sulbactam; TOB, tobramycin; TXS, trimethoprim/sulfamethoxazole.
Frequency of CP-CRE genes upon admission and during hospital stay
Of the 63 CRE isolates, 69.8% (44/63) were phenotypically identified as CP-CRE, and 63.5% (40/63) carried at least one carbapenemase gene.
Among the CP-CRE isolates, 38.6% (17/44) were detected on admission, while 61.4% (27/44) were identified after 14 days of hospitalization. The most frequently identified CP-CRE genes were blaNDM, 71.0% (12/17), blaOXA-48, 53.0% (9/17), and blaKPC, 24.0% (4/17) at admission, with similar proportions observed after 14 days of hospitalization, 74.1% (20/27), 48.1% (13/27), and 26.0% (7/27), respectively. In E. coli, these genes were detected at admission in 64.0% (7/11), 55.0% (6/11), and 18.2% (2/11) of isolates, while they changed to 72.2% (13/18), 44.4% (8/18), and 17.0% (3/18) of the isolates after 14 days of hospitalization, respectively. In K. pneumoniae, blaNDM, blaOXA-48, and blaKPC were detected at admission in 67.0% (4/6), 50.0% (3/6), and 33.3% (2/6) and increased to 78.0% (7/9), 56.0% (5/9), and 44.4% (4/9) after 14 days of hospitalization, respectively. Less common genes, such as blaVIM in 24.0% (4/17), and blaIMP in 29.4% (5/17) were detected at admission, with similar proportions detected after 14 days of hospitalization, 22.2% (6/27) and 26.0% (7/27), respectively (Fig. 4).
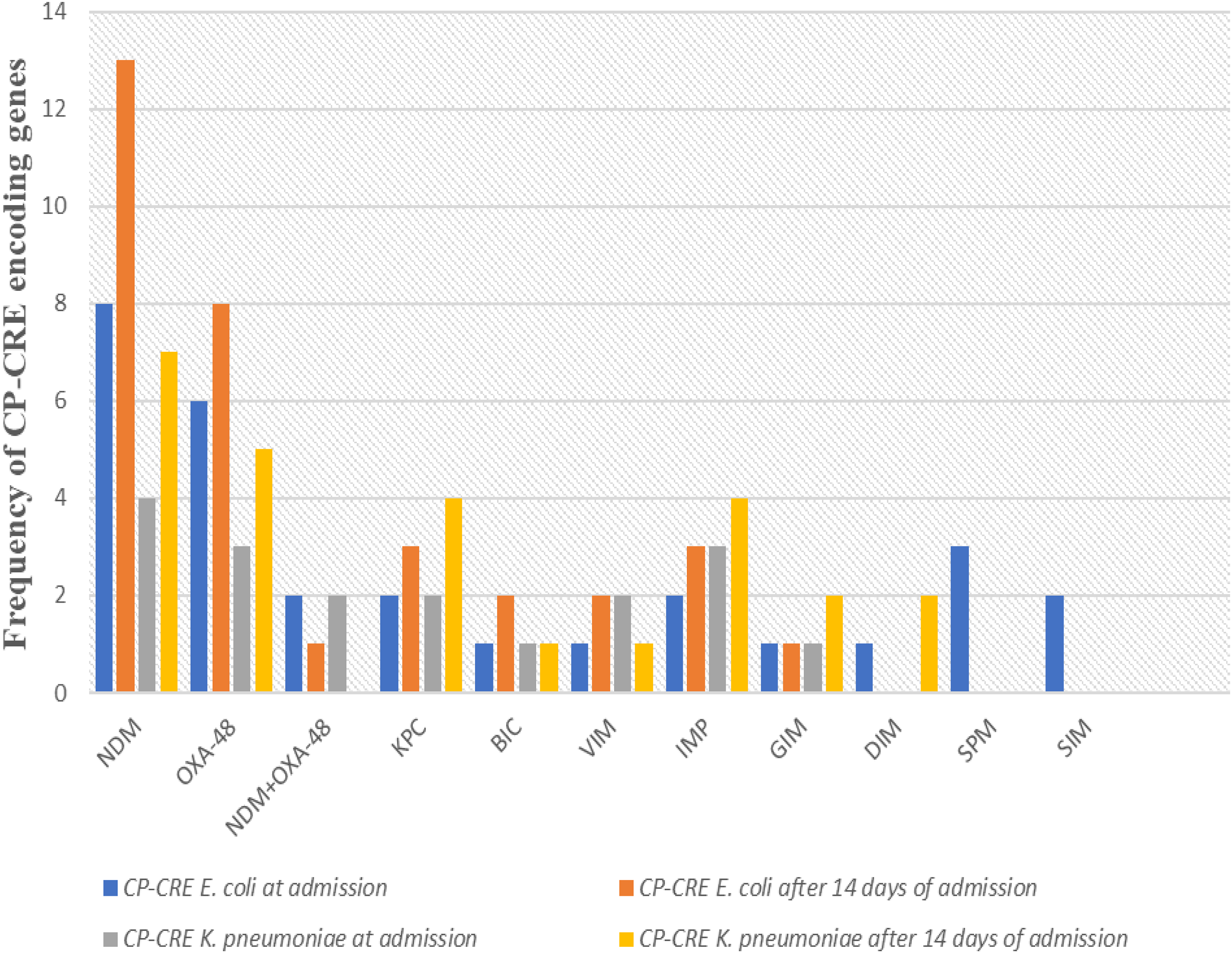
Frequency of CP-CRE encoding genes isolated from Enterobacterales among hospitalized patients in Addis Ababa, Ethiopia, from February 2023 to April 2024 (n = 165).
Factors associated with CRE colonization
Patients who had renal disease as a comorbidity were more likely to be colonized with CRE (adjusted odds ratio = 4.2, 95% confidence interval [CI] = 1.31–13.70, p = 0.02), while other comorbidity, sociodemographic factors, and potential risk factors such as venous catheterization showed no significant association. However, comorbidity involving liver disease showed a strong association with CRE colonization, although the level of association marginally failed for statistical significance (p = 0.07) (Table 5).
Associated Factors of Carbapenem-Resistant Enterobacterales Colonization Among Hospitalized Patients at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, from February 2023 to April 2024 (n = 165)
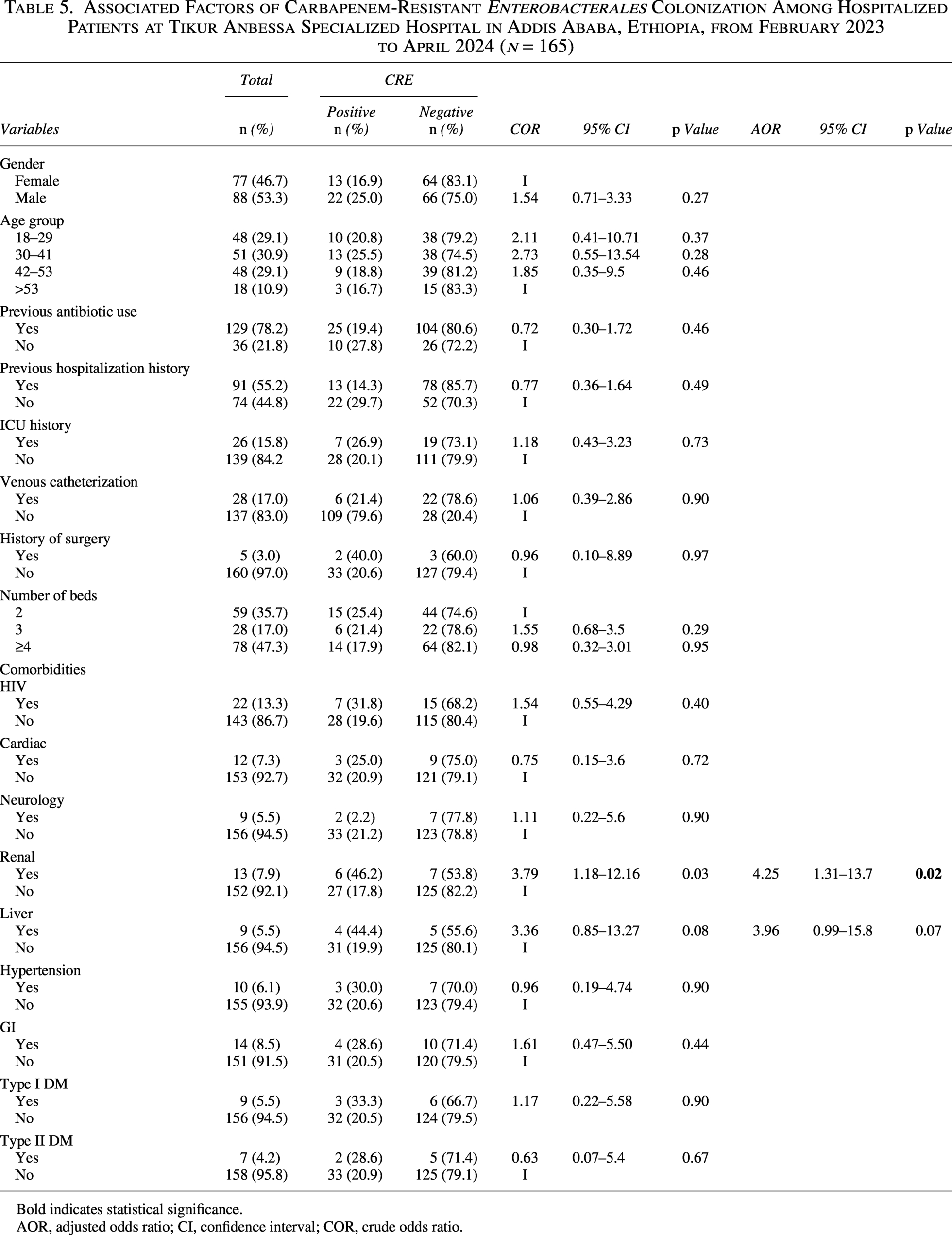
Bold indicates statistical significance.
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio.
HAI and patients’ outcome
HAIs occurred 20.6% (34/165) of the patients. Of these, 26% (9/34) were CRE positive; no association was observed between CRE colonization and HAI (p > 0.05). Pneumonia was the most common HAI, 50.0% (17/34), followed by urinary tract infection (UTI), 32.4% (11/34), and sepsis, 17.6% (6/34). Due to the limited number of CRE positive cases in each HAI category, further analysis was not performed. Moreover, a total of 12/165 (7.3%) deaths were recorded during the study period. Among HAIs patients, 15% (5/34) were CRE-positive, with no significant association between CRE colonization and death (Table 6).
Association of Carbapenem-Resistant Enterobacterales with Hospital-Acquired Infection and Infection Outcome Among Hospitalized Patients at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, from February 2023 to April 2024 (n = 165)

HAI, hospital-acquired infection; UTI, urinary tract infection.
Discussion
In this study, CRE colonization at admission and after 14 days of hospitalization was found to be 19.4% (32/165, 95% CI: 13.8–26.4) and 18.8% (31/165, 95% CI: 13.3–25.8), respectively, with no significant change (p = 0.65). The majority of patients who tested positive for CRE at admission continued to be CRE positive after 14 days of hospitalization (93.8%), while new acquisition was negligible (2.3%). This may suggest that many patients were already colonized prior to hospital admission, indicating a possible prior exposure in the community or from previous antibiotic use and hospitalization. Our findings were comparable to previous studies in Addis Ababa and Jimma, Ethiopia, which reported CRE at 17.1% 9 and 19.0%, 13 respectively. Comparable findings were reported from Egypt, with a 28% CRE colonization rate, 14 and from Nigeria, with a 17.5% CRE colonization rate. 15 However, our results were significantly lower than those reported from a 4-year study conducted in Palestine (22–57%) on admission and from 43% to 77% during hospitalization. 16 Another finding from Thailand reported a comparable (15.5%) CRE result to our reported rate at admission, but a higher acquisition rate (28%) during hospitalization. 17 The short period and only a one-time follow-up sample analysis in our study may be one attribute to this variation. The other reason could be due to differences in CRE detection methods used by the studies, where our detection method was VITEK 2 system, whereas the other two studies used chromogenic selective media.
K. pneumoniae (29.6%) was the most common carbapenem-resistant isolate in our study both at admission and after 14 days of hospitalization, followed by E. coli (17.0%). The fact that K. pneumoniae and E. coli were the two most predominant carbapenem-resistant isolates is consistent with previous studies both within Ethiopia (where 15.4% of K. pneumoniae and 12.4% of E. coli 9 ) and outside Ethiopia (e.g., in Thailand, where 83.3% of K. pneumoniae and 13.6% E. coli). 1 7
In our study, the overall frequency of CP-CRE at both times of sample collection was found to be 16.4% (27/165, 95% CI: 11.2–23.1). A similar finding was reported in Jimma, Ethiopia (11.2%), among oncology and nononcology patients. 18 In contrast, our finding was much higher than previous reports from studies in Addis Ababa (2.0%) from Tikur Anbesa Hospital 7 and 7.3% at St. Paul’s Hospital. 9
In this study, CRE E. coli was resistant at 77.2% to gentamicin at admission, which increased to 90.0% after 14 days of hospitalization. For sulfamethoxazole-trimethoprim, the resistance rate was 82.0% at admission and slightly increased to 85.0% after 14 days of hospitalization. Similarly, CRE K. pneumoniae showed 80.0% resistance to gentamycin at admission and 82.0% after 14 days of hospitalization, while resistance to sulfamethoxazole-trimethoprim was 90.0% at admission and 92% after 14 days of hospitalization. The slight increase in antimicrobial resistance during hospitalization may reflect antibiotic exposure and selective pressure favoring multidrug-resistant strains. In addition, these bacteria may have both enzymatic and nonenzymatic resistance mechanisms, which could account for the observed high levels of resistance. 19 Other studies in Ethiopia also found such high resistance rates; 95.5% and 90.6% against sulfamethoxazole-trimethoprim among E. coli and K. pneumoniae, respectively, although relatively low resistance rates were also observed against gentamycin at 43.9% and 59.4%,9,20 respectively.
In our study, blaNDM was detected at admission in 71.0% and 74.1% after 14 days of hospitalization, respectively. The high frequency of blaNDM may be attributed to its predominant presence on plasmids, which can easily be transferred to other bacteria via horizontal gene transfer. 21 These findings were lower than those of previous studies in Ethiopia (100%) 20 and in India (87.5%). 22 In contrast, our findings were markedly higher than reports from Jimma, Ethiopia (35%), 13 and Sudan (52%). 23 These variations might be due to differences in sample size, study population, laboratory detection methods, and specimen sources. Similarly, blaKPC was identified at admission in 24.0% and 26.0% after 14 days of hospitalization, which was higher than a previous study in Ethiopia (3.57%). 20 However, it was lower than that reported in another study from Ethiopia (100%). 13 Higher blaKPC detection rates have also been reported in Egypt (48.8%) 24 and India (37.5%). 22
Moreover, blaOXA-48 was detected in 53.0% of the patients on admission and 48.1% after 14 days of hospitalization, which was mainly carried by E. coli. Some previous studies have reported significantly less rate, such as 0.5% 13 from Ethiopia and 15.9% from Sudan. 25 However, higher values were observed from other previous studies in Egypt (66.7%) 14 and Iran (65%). 26 Sample size and geographical location might be responsible for these significant variations.
In addition, blaVIM (24.0%) and blaIMP (29.4%) genes were observed in our study at admission and 22.2% and 26.0% after 14 days of hospitalization, respectively. These findings may suggest the presence of travel-related acquisition or local emergence, which indicates the need for continuous monitoring, as these genes could replace the dominant once with passing time, further limiting the treatment options. Our results were consistent with a previous study in Ethiopia, which found a 24.0% blaVIM detection rate. 13 In other regions of the world, both higher and lower detection rates have been reported. For instance, in Iran, the detection rate of blaVIM and blaIMP were 49.0% and 43.0%, respectively, 27 while in Sudan, blaVIM was 0.9% and blaIMP, 3.4%. 23
In the present study, chronic kidney disease was significantly associated with CRE colonization (p = 0.02). This association may be explained by the frequent health care exposure among patients with end-stage renal disease. Other similar studies found that patients with chronic kidney disease had a higher likelihood of being colonized with CRE, which caused infection and mortality. 28 However, it was incongruent with studies in Ethiopia, which reported that chronic diseases were not linked to CRE colonization.8,9 Other potential risk factors showed no statistically significant association with CRE colonization in our study. The possible reason for the lack of association might be due to the limited sample size and the short follow-up period.
Limitation
Our findings were derived from a single hospital setting and a single sample source, which may limit their generalizability to other contexts. In addition, the short follow-up period and small sample size could have contributed to the lack of association between risk factors, CRE colonization, and clinical outcomes, as well as low acquisition rates. We, therefore, suggest future multicenter studies with multiple sampling, large sample size, and longer follow-up period.
Conclusion
Colonization rates of CRE and CP-CRE among hospitalized patients were high, the most commonly identified carbapenemase genes being blaNDM, blaOXA-48, and blaKPC. These results emphasize the importance of screening for fecal carriage of CRE and CP-CRE in patients at admission and during their hospital stay, so that evidence-based decision is made during HAI prevention and management efforts against the pathogens harboring these resistance genes. In addition, whole genome sequencing is highly recommended to investigate clonal relatedness of strains and the genetic bases of the resistance mechanisms.
Authors’ Contributions
D.A., W.E.A., A.A.N., and A.M. participated in conceptualization, design, data curation, and analysis of the study. D.A., W.E.A., and A.A.N. participated in writing the original draft; A.M., A.A.N., and W.E.A. involved in writing—review and editing the article. All authors reviewed the article.
Footnotes
Acknowledgments
We would like to express our gratitude to Addis Ababa University, EPHI, AHRI, and Arsho Diagnostic Laboratory for supporting the necessary materials for this research. We are also thankful to both the study participants and data collectors for their willingness to participate in this research.
Consent for Publication
Not applicable in this section.
Data Availability
All data generated or analyzed during this study are included in these published articles and supplementary information files.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.