
Abstract
Ventilator-associated pneumonia (VAP) caused by carbapenem-resistant Acinetobacter baumannii (CRAB) poses a significant therapeutic challenge with high mortality rates. This study evaluated the clinical efficacy of high-dose ampicillin–sulbactam combined with colistin compared to standard colistin-based regimens. This retrospective study was conducted on 83 patients with CRAB-VAP at Hanoi Medical University Hospital, Vietnam, from May 2024 to May 2025. Patients were divided into an intervention group (n = 33) treated with high-dose ampicillin–sulbactam combined with colistin and a control group (n = 50) receiving other antibiotic regimens combined with colistin. Primary outcomes included 28-day mortality and total ventilation duration. The intervention group achieved significantly lower 28-day mortality (6.1% vs. 38.0%; p < 0.001) and higher microbiological clearance rates by day 14 (93.9% vs. 30.0%; p < 0.001). While early acute kidney injury was more frequent in the intervention group (66.7% vs. 24.0%), renal function outcomes were comparable by day 14. Multivariable analysis identified day-14 microbiological clearance as the strongest independent predictor of survival (hazard ratio [HR] = 13.03; p < 0.001). High-dose ampicillin–sulbactam combined with colistin significantly improves microbiological clearance and survival in patients with CRAB-VAP. Despite a higher incidence of transient nephrotoxicity, the regimen provides a substantial survival benefit.
Introduction
Ventilator-associated pneumonia (VAP) caused by carbapenem-resistant Acinetobacter baumannii (CRAB) represents one of the most challenging and life-threatening bacterial infections confronting clinicians in intensive care unit settings worldwide today. 1 A. baumannii has been officially designated by the World Health Organization as a critical priority-1 pathogen that urgently requires new antimicrobial therapeutic agents for treating resistant infectious diseases. 2 This Gram-negative opportunistic pathogen is notorious for its remarkable ability to persist on environmental surfaces and cause severe nosocomial infections through multiple acquired antimicrobial resistance mechanisms. 3 In intensive care unit settings, A. baumannii ranks among the most frequently isolated pathogens causing VAP, with reported prevalence rates exceeding 36–37% in Asian countries.4,5 These A. baumannii infections are associated with exceedingly high morbidity and mortality rates, with attributable mortality approaching 35%. 6
Carbapenem resistance in A. baumannii is driven by several mechanisms, notably carbapenem-hydrolyzing enzymes, altered membrane proteins, increased efflux pumps, and changes to penicillin-binding proteins. 7 These mechanisms restrict treatment, often leaving clinicians with colistin, which poses toxicity concerns. 8 Though colistin remains a common therapy, increasing evidence shows it may be inadequate for treating VAP in critically ill patients. 9
Key limitations of colistin therapy include its poor penetration into lung tissue, which restricts the drug’s ability to reach the site of infection, and the frequent occurrence of subtherapeutic concentrations in epithelial lining fluid, resulting in reduced antibacterial efficacy. 9 During the treatment course with colistin, resistance may emerge in A. baumannii populations as a consequence of antibiotic pressure and genetic changes. This emergence of resistance often leads to reduced treatment efficacy and can result in clinical failure, with persistent infection despite continued colistin administration. 10
Nephrotoxicity associated with colistin therapy represents a significant clinical concern, as a substantial proportion of patients experience varying degrees of renal impairment ranging from mild increases in creatinine to severe acute kidney injury (AKI). This adverse effect can limit the ability to optimize colistin dosing and may necessitate treatment modification or discontinuation, ultimately compromising the effectiveness of antimicrobial therapy in high-acuity patients. 11
Sulbactam, a β-lactamase inhibitor with direct action on penicillin-binding proteins, is effective against A. baumannii. 12 High-dose ampicillin–sulbactam regimens are able to achieve markedly higher concentrations within lung tissue and epithelial lining fluid compared to colistin, resulting in more favorable pharmacokinetic and pharmacodynamic profiles. This superior tissue penetration allows for consistent attainment of therapeutic drug levels at the site of infection, potentially leading to enhanced microbiological clearance and improved clinical outcomes in patients with severe respiratory tract infections. 13
Combining high-dose ampicillin–sulbactam and colistin offers complementary mechanisms and has shown synergistic effects in laboratory studies. 14 Despite promising early results, more comparative evidence is needed to determine the best treatment strategies for these resistant infections. 15
Methods
Study subjects
Patients eligible for enrollment in this study were individuals over 16 years of age who had undergone invasive mechanical ventilation for a minimum duration of 48 hours. To be included, patients were required to meet the 2023 Centers for Disease Control and Prevention (CDC) diagnostic criteria for VAP. 16 Clinically, inclusion required at least one systemic sign—fever of >38°C without another cause, leukopenia/leukocytosis, or altered mental status in patients >70 years—together with at least two respiratory findings such as purulent sputum, worsening gas exchange, or a new radiographical infiltrate. Microbiological confirmation required a positive lower respiratory tract culture for A. baumannii. Finally, participants must have had a specific clinical indication for treatment with high-dose ampicillin–sulbactam combined with colistin, specifically for CRAB strains exhibiting a meropenem MIC >8 µg/mL17,18 and a colistin MIC of <2 µg/mL.
The study excluded any patients or families who requested discharge against medical advice. Additionally, individuals who discontinued the prescribed treatment regimen <48 hours following study enrollment were removed from the final analysis to ensure data integrity regarding treatment response.
Study design and setting
This research was conducted as a retrospective descriptive cross-sectional study at the Department of Emergency and Intensive Care, Hanoi Medical University Hospital, from May 2024 to May 2025. Data were collected via a retrospective review of medical records using a convenience sampling method. The study population comprised two distinct cohorts of patients treated for CRAB-VAP: Those receiving a high-dose ampicillin–sulbactam regimen combined with colistin and a comparison group treated with alternative antibiotic regimens combined with colistin.
Dosing protocols
Antibiotic administration adhered strictly to established clinical guidelines. Colistin dosing followed the European Society of Clinical Microbiology and Infectious Diseases and Infectious Diseases Society of America recommendations, stratified by glomerular filtration rate (GFR). 19 Patients with normal renal function received a loading dose of 9 million international units (MIU), followed by a maintenance dose of 4.5 MIU every 12 hours, with appropriate dose reductions implemented for patients with renal impairment or those undergoing dialysis. Similarly, ampicillin–sulbactam was dosed according to renal function, with a standard regimen of 3 g every 6–8 hours in patients with normal creatinine clearance and adjusted dosing frequencies for those with impaired renal function or undergoing continuous or intermittent hemodialysis. 20
Study procedure
The study protocol commenced with a retrospective screening of all patients mechanically ventilated during the study period to identify those satisfying the diagnostic criteria for VAP. From this initial pool, cases with A. baumannii positive cultures were isolated, and their antibiograms were reviewed to select participants meeting the inclusion and exclusion criteria. Data collection began on Day 0, marking the initiation of targeted treatment, where baseline demographics, comorbidities, and clinical severity scores such as SOFA 21 and Acute Physiology and Chronic Health Evaluation II 22 were recorded. Throughout the treatment period, specifically from Day 1 to Day 14, clinical parameters including vital signs, fluid balance, and laboratory markers were monitored daily. Repeat endotracheal cultures were obtained on Day 7 and within the second week to assess microbiological clearance. The primary endpoint assessment was conducted on Day 28 to determine mortality outcomes, along with a calculation of the total duration of mechanical ventilation.
Clinical and microbiological response
Clinical efficacy was evaluated based on a composite of four criteria: (1) patient survival, (2) hemodynamic stability without the need for increasing vasopressor support, (3) stabilization or improvement in Sequential Organ Failure Assessment (SOFA) scores, and (4) improved respiratory parameters as indicated by the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2 ratio). A patient was classified as a nonresponder if they failed to meet any single one of these criteria.
Microbiological response was categorized as clearance if follow-up cultures of blood and respiratory specimens were negative for CRAB or as failure if the initial pathogen persisted.
Renal failure
AKI was assessed using the Risk, Injury, Failure, Loss, and End-stage kidney disease criteria, defined as a serum creatinine increase of more than 1.5 times baseline or a GFR decrease of more than 25% sustained for at least 24 hours. The time to AKI was recorded as the earliest point of renal injury following treatment initiation.
Survival outcomes
Treatment outcomes were classified as survival—defined as discharge or transfer with clinical improvement—or mortality, which included any in-department death or discharge for palliative care due to poor prognosis.
Study variables
Baseline characteristics encompassed patient demographics, source of admission, comorbid conditions, and specific risk factors, including recent surgical procedures or immunosuppressive states. Clinical parameters included vital signs, neurological status as evaluated by the Glasgow Coma Scale, infection biomarkers such as procalcitonin, and initial illness severity. The primary outcomes were defined by microbiological and clinical response rates, whereas secondary outcomes comprised 28-day mortality, total duration of mechanical ventilation, and the incidence of AKI.
Statistical analysis
All statistical analyses were performed using R software. Continuous variables were expressed as mean and standard deviation for normally distributed data or as median and interquartile range for nonnormally distributed data. Categorical variables were presented as frequencies and percentages. Comparative analysis between groups utilized Fisher’s exact test for categorical variables, while continuous variables were assessed using Student’s t test or the Mann–Whitney U test as appropriate. Survival analysis was conducted using the Cox proportional hazards model, with statistical significance defined as a p value of <0.05 at a 95% confidence interval.
Study ethics
The study utilized the standard biochemistry, hematology, and diagnostic imaging infrastructure of Hanoi Medical University Hospital. Microbiological identification and antimicrobial susceptibility testing, including E-test for MIC determination, were performed according to the hospital’s standard protocols. Regarding ethical considerations, the research was designed to enhance patient care and treatment efficacy. The study posed no risk to participants, and strict protocols were implemented to protect the rights and safety of vulnerable subjects. All personal data were anonymized and kept strictly confidential, used solely for the purposes of this research. The study was conducted after the protocol had been defended at the institutional committee, and the research project, including the assignment of academic supervisors for the master’s thesis, was approved in Decision No. 452/QĐ-ĐHYHN dated February 20, 2025, by Hanoi Medical University.
Results
The baseline demographic and clinical characteristics of the control group (n = 50) and the intervention group (n = 33) were generally comparable across all assessed variables. The median age in the intervention group was 67.0 years, and 78.8% were male, with no notable difference compared to the control group. Mean body mass index (BMI) values were similar between groups (21.5 ± 3.7 vs. 21.9 ± 3.8). The Charlson Comorbidity Index had a median of 2.0 [1.0; 4.0] in both groups. Comorbidity rates were comparable, and recent exposures to chemotherapy, corticosteroids, or surgery showed no meaningful differences between groups (Table 1).
Baseline Characteristics of Study Participants
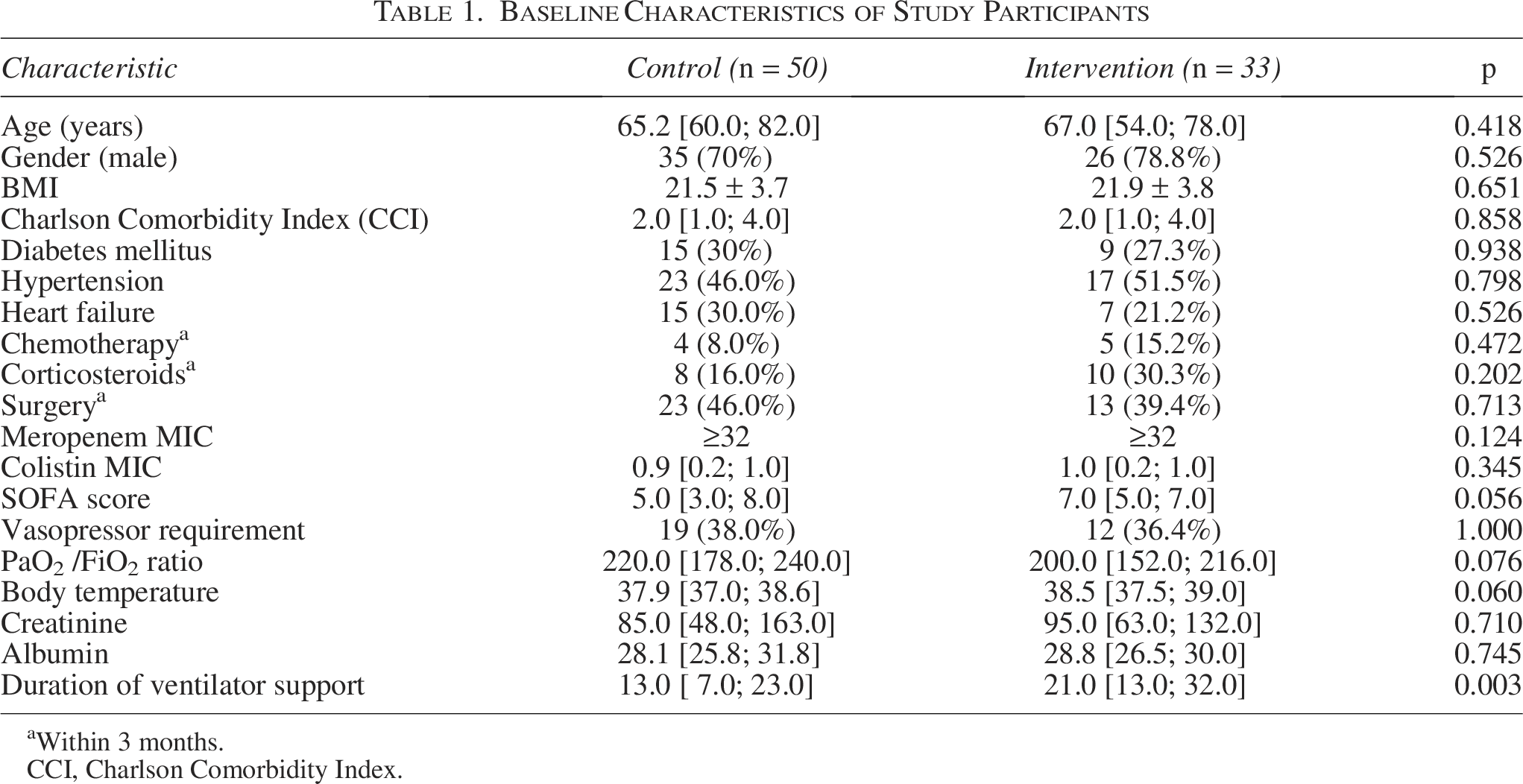
aWithin 3 months.
CCI, Charlson Comorbidity Index.
Resistance profiles, including meropenem MIC (≥32 in both groups; p = 0.124) and colistin MIC (0.9 [0.2; 1.0] vs. 1.0 [0.2; 1.0]; p = 0.345), were similar. Median SOFA scores (5.0 vs. 7.0), vasopressor requirements (38.0% vs. 36.4%), PaO2/FiO2 ratios (220.0 vs. 200.0), creatinine levels (85.0 vs. 95.0), and albumin concentrations (28.1 vs. 28.8) showed no significant differences. The intervention group required a significantly longer duration of ventilator support compared with the control group (p = 0.003; Table 1).
Table 2 shows notable differences in microbiological and clinical outcomes between the control and intervention groups. At day 7, microbiological positivity was higher in the control group (88.0%) than in the intervention group (72.7%), though not statistically significant (OR = 0.36; 95% confidence interval (CI): 0.11–1.13; p = 0.08). By day 14, microbiological clearance strongly favored the intervention group, with only 6.1% remaining positive compared to 70.0% in the control group (odds ratio (OR) = 0.03; 95% CI: 0.00–0.11; p < 0.001).
Microbiological and Clinical Outcomes
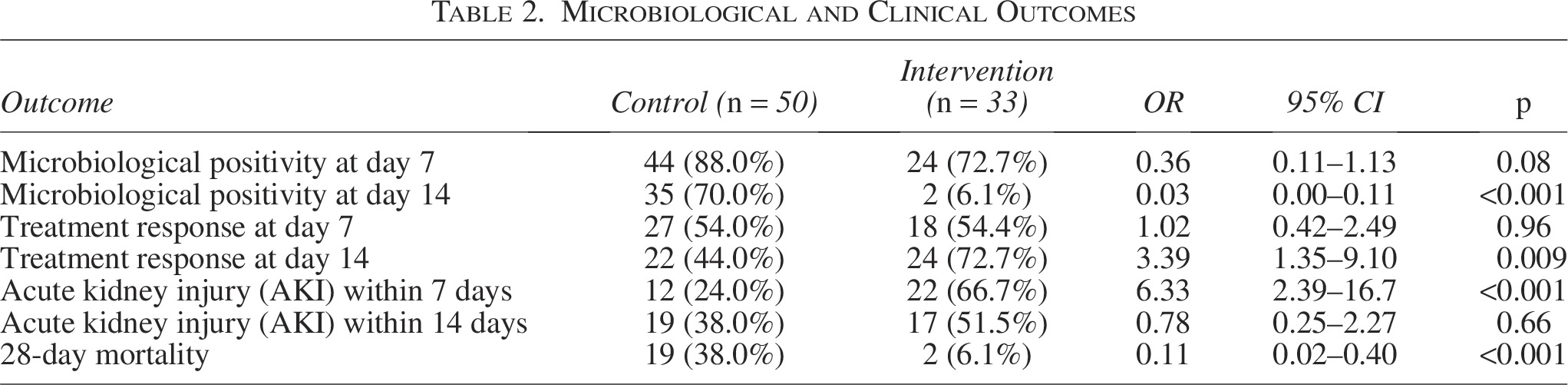
Clinical response was similar at day 7, but by day 14 the intervention group showed a significantly higher response rate (72.7% vs. 44.0%; OR = 3.39; 95% CI: 1.35–9.10; p = 0.009).
Regarding renal safety, AKI within 7 days occurred much more frequently in the intervention group (66.7% vs. 24.0%; OR = 6.33; 95% CI: 2.39–16.7; p < 0.001). However, by day 14, the incidence of AKI was not significantly different (51.5% intervention vs. 38.0% control; OR = 0.78; 95% CI: 0.25–2.27; p = 0.66).
Importantly, 28-day mortality was substantially higher in the control group at 38.0% compared to 6.1% in the intervention group (OR = 0.11; 95% CI: 0.02–0.40; p < 0.001). These findings highlight significant improvements in microbiological clearance, clinical response, and mortality favoring the intervention group, despite a higher rate of early AKI.
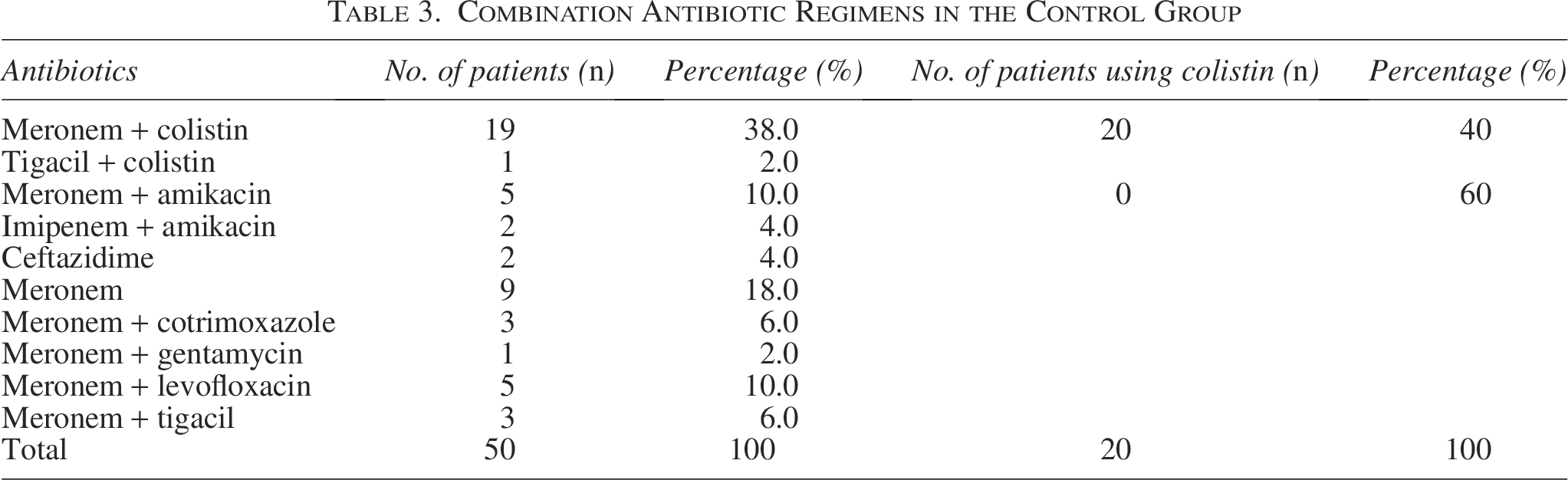
In the control group, 20 patients received combination antibiotic therapy that included colistin, and 7 patients received combinations containing amikacin (Table 3). Notably, 23 patients (46.0%) were treated with other antibiotics that did not include these nephrotoxic agents. This may partly explain why the incidence of AKI was lower in the control group.
Combination Antibiotic Regimens in the Control Group
The Kaplan–Meier curve in Fig. 1 shows a clear difference in 28-day survival between the two groups. Survival in the control group declined steadily, reaching about 60% by day 28, whereas the intervention group maintained a consistently high survival rate of over 90% throughout the follow-up. The wide separation between the curves highlights the marked survival benefit associated with the intervention.
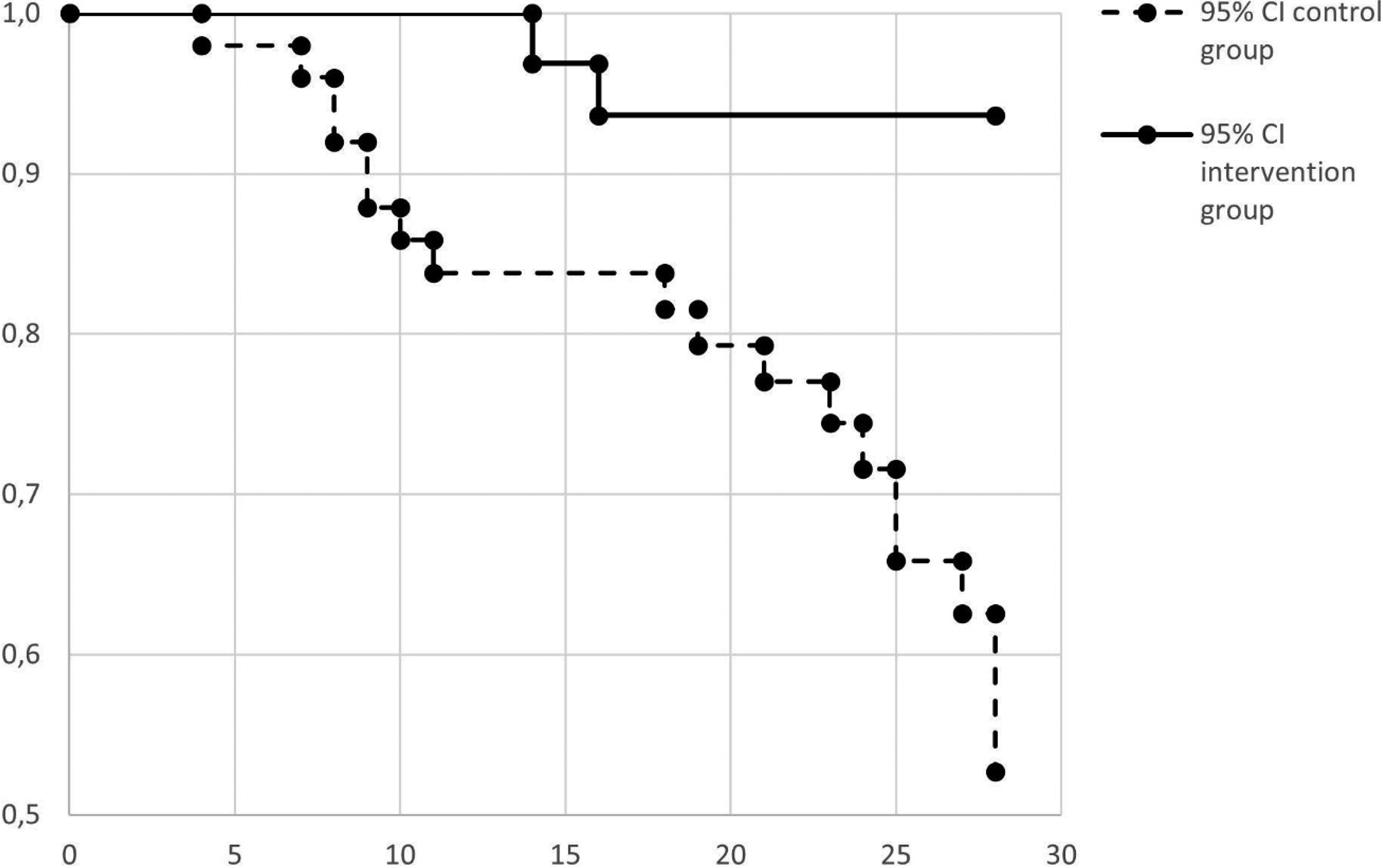
Twenty-eight-day survival rate after treatment.
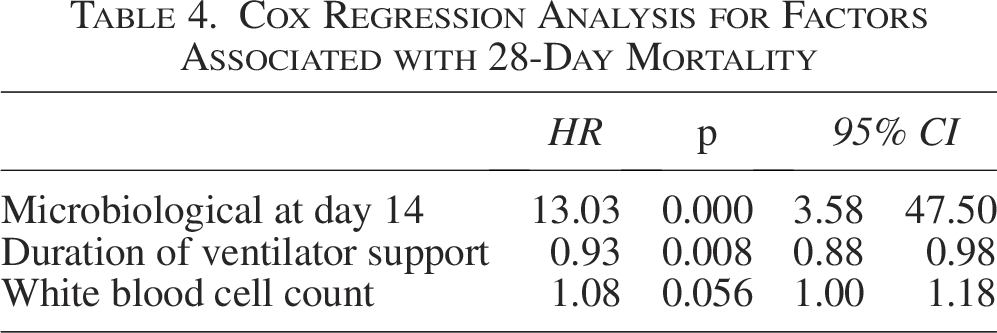
In the multivariable analysis, microbiological clearance at day 14 was strongly associated with achieving the primary outcome (HR = 13.03; 95% CI: 3.58–47.50; p < 0.001). Longer ventilator duration showed a modest but significant negative association with the hazard (HR = 0.93; 95% CI: 0.88–0.98; p = 0.008). Elevated white blood cell count demonstrated only a borderline, nonsignificant association (HR = 1.08; 95% CI: 1.00–1.18; p = 0.056; Table 4).
Cox Regression Analysis for Factors Associated with 28-Day Mortality
Discussion
The findings of this retrospective cross-sectional study demonstrate that high-dose ampicillin–sulbactam combined with colistin represents a clinically meaningful therapeutic approach for VAP caused by CRAB, achieving markedly superior microbiological and clinical outcomes compared to alternative antibiotics. The intervention group exhibited dramatically improved 28-day mortality rates of 6.1% relative to the control group’s 38.0%, coupled with significantly enhanced microbiological clearance by day 14 (6.1% vs. 70.0%), despite encountering a higher incidence of AKI during the initial treatment phase.
The robust clinical response documented in the intervention group aligns with emerging evidence supporting combination antimicrobial therapy as the optimal therapeutic strategy for multidrug-resistant A. baumannii infections. The intervention group achieved a clinical response rate of 72.7% by day 14, compared to only 44.0% in the control group, representing a three-fold increase in treatment efficacy. This outcome reflects the potent bactericidal activity of high-dose ampicillin–sulbactam in the treatment of A. baumannii. Sulbactam, functioning both as a β-lactamase inhibitor and intrinsic antimicrobial compound through inhibition of A. baumannii cell wall synthesis, demonstrates synergistic interactions with colistin through distinct molecular pathways. Studies showed that colistin and various β-lactam combinations also achieve synergistic or additive effects against multidrug-resistant A. baumannii isolates. 23 Several studies have suggested that prolonged colistin therapy (>14 days), as well as adjunctive inhaled colistin, may provide clinical benefit in the treatment of CRAB infections.24,25
The superior microbiological clearance in the intervention group by day 14 (6.1% positive vs. 70.0% in the control group) represents a critical mechanistic advantage. This pronounced microbiological clearance was independently associated with a 13-fold increase in likelihood of achieving the primary survival outcome in the multivariable Cox regression analysis, establishing microbiological clearance as a robust predictor of clinical success. This finding underscores the pathophysiologic importance of achieving adequate microbiological clearance within the pulmonary compartment to prevent treatment failure and persistent infection, particularly in critically ill patients where the inflammatory cascade triggered by residual bacterial burden perpetuates organ dysfunction and prolongs mechanical ventilation requirements. 26 The results also align with previous research showing that microbiological clearance was independently associated with recurrent pneumonia or death among patients with bacterial pneumonia following clinical cure, with an adjusted odds ratio of 1.56 (95% CI, 1.04–2.35) at 90 days in patients with pneumonia. 27
Additionally, microbiological clearance has been consistently associated with clinical success, with 55.5% of patients in previous severe pneumonia studies achieving total or partial microbiological clearance while experiencing favorable clinical outcomes. 28
A fundamental mechanistic distinction between the intervention regimen and colistin monotherapy relates to pulmonary pharmacokinetics and drug distribution to the primary site of infection. High-dose ampicillin–sulbactam achieves substantially higher concentrations within lung tissue and epithelial lining fluid compared to colistin, particularly when administered by continuous infusion or extended-interval regimens. It enables consistent attainment of therapeutic drug levels required to suppress bacterial growth and achieve microbiological clearance, thereby establishing more favorable pharmacokinetic and pharmacodynamic profiles. 29 This distinction becomes clinically important since colistin suffers from poor penetration into lung tissue, restricting the achievement of therapeutic concentrations at the site of pulmonary infection.5,8 Consequently, colistin epithelial lining fluid concentrations often remain subtherapeutic, limiting antibacterial efficacy and potentially contributing to clinical failure despite systemic administration.
A clinically significant finding emerges from the differential AKI patterns observed between treatment groups. The intervention group experienced a substantially higher incidence of AKI within the first 7 days of treatment (66.7% vs. 24.0%), yet this early renal dysfunction did not translate into worse mortality outcomes and appeared to stabilize by day 14 without persistent divergence between groups. This paradoxical dissociation between early AKI and improved clinical outcomes warrants careful consideration within the mechanistic framework of colistin-induced nephrotoxicity. Colistin nephrotoxicity represents a well-established adverse effect occurring in a substantial proportion of critically ill patients receiving intravenous colistin, with mechanisms involving direct tubular toxicity, oxidative stress, and inflammatory activation within renal tissue. The higher early AKI incidence in the intervention group may reflect greater cumulative colistin exposure or more aggressive dosing strategies required to achieve therapeutic levels in the context of clinical deterioration requiring intensified antimicrobial therapy.29,30
The modest negative association of prolonged ventilator support (HR = 0.93) reflects previously reported observations that extended mechanical ventilation often represents both a marker and consequence of disease severity rather than an independent mortality driver. Numerous variables associated with poor outcomes in patients who require extended ventilation reflect pre-existing or ongoing systemic dysfunction. In a prospective cohort study of 300 patients ventilated for at least 21 days, 1-year mortality was closely linked to clinical indicators of severe illness, including the requirement for vasopressors (1-year mortality odds ratio: 8.8, 95% CI = 1.6–48.4), hemodialysis (OR = 2.9, 95% CI = 1.1–7.7), platelet count ≤150 × 109/L (OR = 14.5, 95% CI = 4.1–50.8), and age of ≥50 years (OR = 5.6, 95% CI = 2.4–12.9). Notably, these factors reflect the extent of multiorgan failure or diminished physiological reserve, rather than the act of mechanical ventilation alone. 31
The strengths of this study lie in its comprehensive evaluation of both microbiological clearance and clinical survival in a high-risk patient population infected with a critical priority pathogen. However, several limitations must be acknowledged. First, the single-center, retrospective design utilizing convenience sampling inherently limits the generalizability of our findings to other health care settings with differing local resistance patterns and antibiotic stewardship protocols. Second, the relatively small sample size may restrict the statistical power to detect subtle differences in secondary outcomes or rare adverse events. Third, although baseline characteristics were comparable, the nonrandomized nature of the study precludes the complete elimination of selection bias and unmeasured confounders inherent to observational research. Consequently, future research should prioritize large-scale, multicenter randomized controlled trials to validate these findings. Additionally, further pharmacokinetic and pharmacodynamic studies are warranted to optimize high-dose ampicillin–sulbactam regimens, aiming to maximize microbiological clearance while mitigating the risk of nephrotoxicity when combined with colistin.
Conclusions
The combination of high-dose ampicillin–sulbactam and colistin demonstrated superior efficacy compared to other colistin-based regimens for treating VAP caused by CRAB. This regimen significantly improved pulmonary microbiological clearance and drastically reduced 28-day mortality (6.1% vs. 38.0%). Although the incidence of AKI was higher in the first week of treatment, it was transient and did not negatively impact overall survival outcomes. The study highlights that achieving early microbiological clearance is a robust predictor of survival, supporting the use of this combination therapy as a potential therapy for critically ill patients, particularly in settings where access to newer agents is limited. Besides, given the retrospective design and potential residual confounding, these findings should be confirmed in prospective studies.
Authors’ Contributions
H.B.H., T.K.N., and T.H.T.B.: Conceptualization, methodology, analysis, writing, reviewing, and supervision. L.K.N., S.T.D., T.H.T.B., and T.T.N.: Methodology and investigation. All authors contributed to the article and approved the submitted version.
Footnotes
Disclosure Statement
No competing interests exist.
Funding Information
No funding was received for this article.