
Abstract
Globally, Acinetobacter baumannii has emerged as an important nosocomial pathogen and as highly resistant to clinically relevant antibiotics, namely, carbapenems. In this study, we aimed to determine the epidemiological profile and the imipenem (IPM) resistance rate of a clinical collection of A. baumannii isolates. This study was carried out at the Central Laboratory of the Oran Regional University Military Hospital (Hôpital militaire régional universitaire d’Oran) over a period of 7 years (January 2010–December 2016). The frequency of A. baumannii isolates was not constant over the 7 years; however, an increasing trend was observed. Among the 168 isolates, the majority was isolated from male patients (n = 131, 78%). Patients in the intensive care unit had a higher risk of developing A. baumannii infection (76%) compared to other hospital services, and protected distal pulmonary samples were the main site of isolation of A. baumannii isolates (34%). Among the collected isolates, 106 were IPM resistant and exhibited multidrug phenotypes. These results confirm the multidrug-resistant nature of A. baumannii and its nosocomial behavior. The emergence of this bacterial species represents a serious therapeutic and epidemiological problem, hence the need for the establishment of a system for monitoring the microbial environment of the hospital and the strict application of hygiene measures.
Introduction
Acinetobacter baumannii is a glucose-nonfermentative, nonmotile, nonfastidious, catalase-positive, oxidative-negative, aerobic Gram-negative coccobacilli. 1 It is an opportunistic human pathogen that primarily affects critically ill patients, making it a major nosocomial organism associated with a wide range of clinical infections. These include ventilator-associated pneumonia, bloodstream infections, wound infections, urinary tract infections, and meningitis.1–3 Unlike many other human pathogens, A. baumannii lacks identifiable toxins or specific molecular determinants that clearly explain the virulence of individual strains. 4 However, the rise of A. baumannii as a redoubtable human pathogen is largely attributed to its remarkable ability to persist and withstand diverse stress conditions, including host immune defenses, environmental challenges, and exposure to antimicrobial agents.4,5 In clinical settings, A. baumannii is a highly successful nosocomial pathogen capable of colonizing both biotic and abiotic surfaces. Its strong ability to form biofilms gives it notable resistance to disinfectants and desiccation.6–8
Globally, carbapenems (e.g., imipenem [IPM], meropenem) are considered the treatment of choice for severe A. baumannii infections.9–12 However, high rates of carbapenem-resistant A. baumannii have now been reported worldwide. 13 In A. baumannii, carbapenem resistance is primarily mediated by acquired OXA-type carbapenem-hydrolyzing β-lactamases (oxacillinases [OXAs]), mediated by blaOXA-23-like, blaOXA-40-like, blaOXA-58-like, blaOXA-143-like, and blaOXA-235-like genes.13,14 Less commonly, resistance is conferred by metallo-β-lactamases (MBLs), including IMP (Imipenemase), NDM (New Delhi metallo-β-lactamase), SIM (Seoul imipenemase), and VIM (Verona integron-encoded metallo-β-lactamase), whereas Klebsiella pneumoniae carbapenemase (KPC) and Guiana extended-spectrum β-lactamase (GES) are only rarely detected. 14 In addition, some variants of the intrinsic OXA-51-like carbapenemase confer carbapenem resistance when overexpressed via the insertion sequence ISAbaI.13,15 It is noteworthy that overexpression of drug efflux pumps, modifications or novel forms of penicillin-binding proteins, and changes in porin expression or in the genes encoding porins (e.g., OMP, OprD) also contribute significantly to carbapenem resistance in A. baumannii. 16 Alarmingly, several studies indicate that carbapenem-resistant strains are frequently multidrug-resistant (MDR) or even pan-drug-resistant (PDR), particularly against aminoglycosides and quinolones/fluoroquinolones, further limiting therapeutic options.17,18
The emergence and dissemination of carbapenem-resistant A. baumannii have been reported both in clinical samples and on inanimate surfaces in several Algerian hospitals.19–24 These studies, along with others, highlight alarming increases in clinical carbapenem-resistant A. baumannii and underscore the need for heightened attention in health care settings. In this context, the present investigation was undertaken. The main objective of this study was to retrospectively assess, over a 7-year period (2010–2016), the prevalence and resistance profile of A. baumannii to IPM, as well as the evolution of its epidemiological patterns at the Oran Regional University Military Hospital (Hôpital Militaire Régional Universitaire d’Oran, HMRUO), Algeria.
Materials and Methods
Study setting and isolates collection
This retrospective study was conducted at the Oran Regional University Military Hospital (HMRUO), Oran, Algeria, from January 1, 2010, to December 31, 2016. In accordance with the Declaration of Helsinki (2013), clinical specimens were obtained as part of routine diagnostic care from patients with clinical and/or biological suspicion of bacterial infection, in addition to hygienic/environmental swabs collected from hospital surfaces and laboratory equipment as part of routine microbiological surveillance. Only the first nonduplicate A. baumannii isolate recovered from each patient or sampling site was included in the analysis.
Clinical specimens included blood cultures, protected distal pulmonary (PDP) samples, pus, urine, catheter tips, cerebrospinal fluid (CSF), and throat swabs. All isolates were included only when considered clinically or epidemiologically significant according to standard microbiological criteria and in conjunction with the patient’s clinical presentation. Significant bacteriuria was defined as ≥105 CFU/mL. Bloodstream infection was considered in cases of positive blood culture associated with compatible clinical signs of infection. Respiratory samples, including PDP specimens, were interpreted as significant when predominant bacterial growth was observed in association with inflammatory cells and a compatible clinical context. CSF and catheter-related isolates were interpreted according to established diagnostic criteria and clinical relevance.
The distribution of collected A. baumannii isolates was analyzed according to specimen type, patient sex, hospital department, and antimicrobial resistance profile. Phenotypic identification of isolates was performed using morphological and biochemical tests (Gram staining, oxidase, catalase, and motility). Confirmation of A. baumannii identification was performed using the bioMérieux API 20 NE system (France). API 20 NE results were analyzed according to the manufacturer’s instructions using APIWEB software version 4.1.
Antimicrobial susceptibility testing
The antibiotic susceptibility of the isolates was assessed using the Kirby–Bauer disk diffusion method on Mueller–Hinton agar plates (Bio-Rad, Marnes-la-Coquette, France), following Clinical and Laboratory Standards Institute (CLSI) standards. 25 The used antibiotics were: ampicillin (AMP); ticarcillin (TIC), ticarcillin + clavulanic acid (TTC), imipenem (IPM), cefotaxime (CTX), ceftazidime (CAZ); Cefalotin/cefazolin (Cz) or (kz), cefoxitin (FOX), piperacillin + tazobactam (TZP), cefepime (FEP), gentamicin (GN), kanamycin (K), netilmycin (Net), ofloxacin (OFX), levoflaxcin (Lev); norfloxacin (NOR), trimethoprim/sulfamethaxazole (SXT), rifampicin (RD), tetracycline (TE), and furan (F) (nitrofurantoin). In addition, colistin susceptibility was determined using the broth microdilution method for all isolates, in accordance with CLSI recommendations. 25 Quality control was ensured using two standard reference strains, Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853. MDR isolates were defined as resistant to at least three classes of antimicrobial agents. 26
Statistical analysis
Statistical analyses of the data were made using Access and Excel software (Microsoft Office 2010).
Results
Number of collected isolates, demographic data, and specimens
During the study period, 168 A. baumannii isolates were identified from different samples and from different departments of the HMRUO. Over the 7 years, the evolution of A. baumanni showed a marked increase during the first 3 years, being 11 isolates in 2010 (13%), 22 in 2011, and 37 in 2012. Then, a decrease in frequency in 2013 with 15 isolates, then an increase in 2014 with collection of 25 isolates, followed by 31 isolates in 2015 and 27 isolates in 2016 (Table 1).
Occurrence of Acinetobacter baumannii by Sex, Age, and Nature of the Sample and Departments Between 2010 and 2016
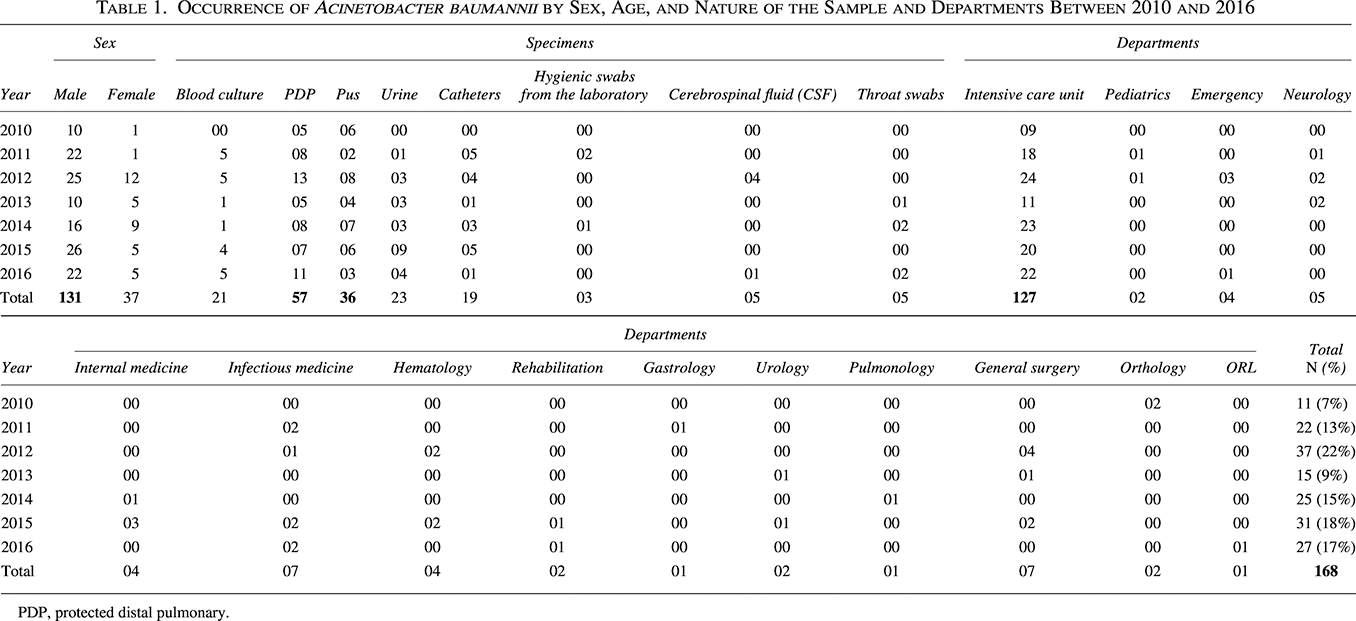
PDP, protected distal pulmonary.
The distribution of A. baumannii isolates according to gender showed that the majority of isolates were collected from males (n = 131, 78%), the M/F sex ratio was 3.54. Isolates were collected from various services in the hospital; however, the majority were collected from patients in the intensive care unit (ICU; n = 127; 76%) (Table 1). The distribution of isolates according to samples types revealed the predominance of the isolates derived from PDP samples (n = 57; 34%), followed by pus (n = 36; 21%), urine samples (n = 23; 17%), blood cultures (n = 21; 13%), catheters (n = 19; 11%), CSF (n = 5; 3%), and throat swabs (n = 5; 3%) (Table 1).
Antimicrobial susceptibility
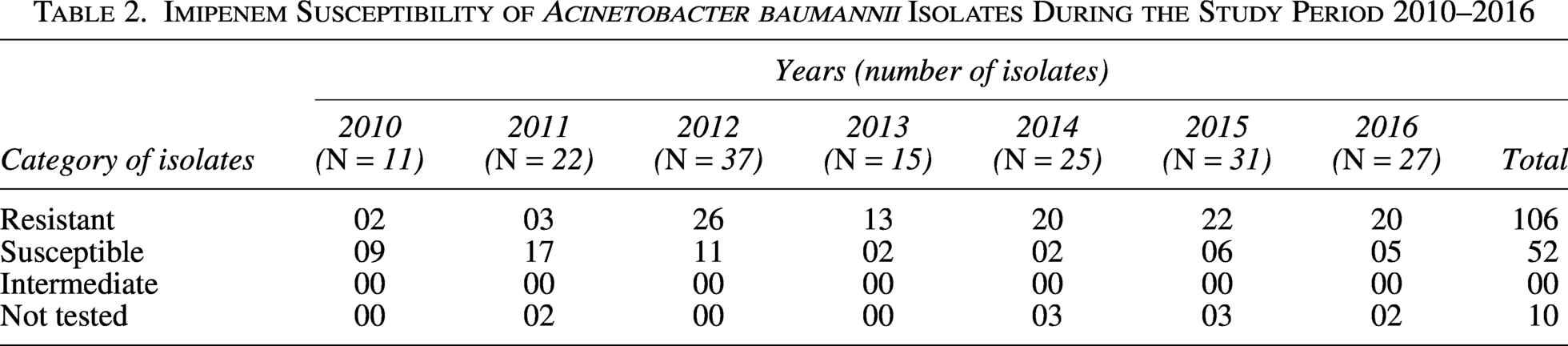
Among the 168 A. baumannii isolates, 158 were tested for their susceptibility to IPM, from which 106 (67%) were IPM-resistant (Table 2). Interestingly, all IPM-resistant isolates were MDR, where IPM resistance was associated to resistance toward several other antibiotics belonging to different families, including beta-lactams, aminoglycosides, quinolones, and fluroquinolones. However, these A. baumannii isolates were susceptible to colistin and/or RD. The IPM resistance rates increased from 2010 until 2014, ranging from 18% in 2010, 15% in 2011, 70% in 2012, 87% in 2013, and 91% in 2014, then a decrease in frequency in 2015 (79%), and then an increase in 2016 (80%) (Fig. 1).
Imipenem Susceptibility of Acinetobacter baumannii Isolates During the Study Period 2010–2016
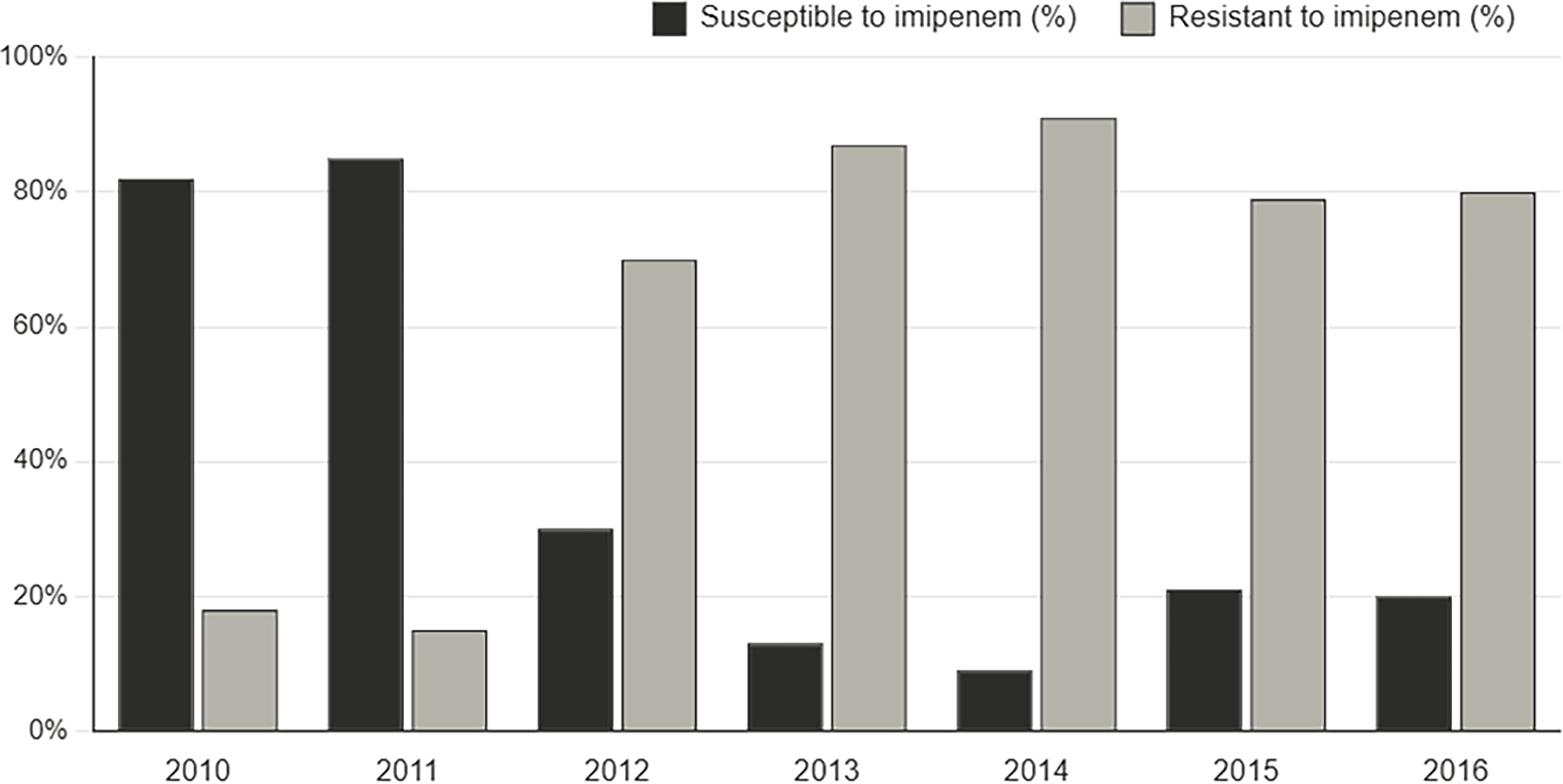
Evolution of imipenem-resistant Acinetobacter baumannii isolates to imipenem during the study period 2010–2016.
Discussion
Globally, antibiotic-resistance to clinically relevant antibiotics is a global threat to human health, which particularly concerns the ESKAPE pathogens. Clinical MDR and PDR A. baumannii isolates are increasingly reported worldwide, including Algeria, making the treatment of A. baumannii associated infections problematic. 11 In Algeria, little is known about the epidemiology of A. baumannii isolates in clinical settings, despite few local studies have reported high rates of antibiotic-resistant isolates, especially resistance to carbapenems.21,27,28 Therefore, more data are needed to objectively assess the status and epidemiology of carbapenem resistance among clinical A. baumannii isolates.
In our study, conducted over a 7-year period (from January 1, 2010, to December 31, 2016), a total of 168 A. baumannii isolates were identified in the bacteriology laboratory of the Oran Regional University Military Hospital. Although the number of A. baumannii isolates varied between years, the average was 24 isolates per year. This rate remains relatively low compared with that reported in a study conducted in Tlemcen (Algeria), where 155 isolates were recovered over a 4-year period. 29 In contrast, in Morocco, 546 isolates were collected from clinical samples at the University Hospital Center of Marrakech over a 6-year period (January 1, 2012, to December 31, 2017), corresponding to an average of 91 isolates per year 30 ; however, in the same country, 183 isolates were collected over 5 years (January 1, 2010, to December 31, 2015), with an average of 36.6 isolates per year. 31 In addition, a study from Kenya reported 590 A. baumannii isolates collected over a 3-year period, corresponding to 196.6 isolates per year. 32 These differences in annual isolation rates are likely related to variations in hospital size, health care infrastructure, and the number of hospitalized patients across countries.
Analysis of the temporal evolution of A. baumannii over the study period revealed a nonconstant trend, with fluctuations characterized by alternating increases and decreases across the 7 years. Similar patterns were reported in a study conducted in three hospitals in western Algeria (Tlemcen, Oran, and Sidi Bel Abbes), where the incidence curves varied according to the presence and magnitude of outbreak episodes and showed no consistent overall trend. 29 These fluctuations may be attributed to the challenges associated with controlling A. baumannii outbreaks within hospital settings. The dissemination of A. baumannii is often facilitated by patient or health care worker movement and exposure to common sources of contamination in hospitals, as well as by several predisposing factors, including recent surgery, the use of central venous catheters, tracheostomy, parenteral nutrition, hygiene practices, and antibiotic use.12,33,34 Nevertheless, despite this irregular temporal pattern, a notable increase was observed in 2016, with the number of isolates (n = 27) being nearly threefold higher than that recorded in the first year of the study in 2010 (n = 11).
According to patient demographics, infections were more frequent in males than females, consistent with previous reports.31,34 This predominance may be associated with higher exposure to risk factors such as smoking, alcohol consumption, diabetes, and chronic pulmonary disease in male patients.35–37 A striking finding in our study was the predominance of isolates recovered from ICUs, which accounted for 76% of all isolates. These findings are consistent with published data indicating that ICUs remain the primary source of A. baumannii infections, although reported rates vary.35,38 Patients admitted to ICUs are at higher risk of developing A. baumannii infections due to the severity of underlying diseases, prolonged hospital stays, extensive use of broad-spectrum antibiotics, and frequent exposure to invasive procedures, including mechanical ventilation, urinary catheterization, and central venous catheter placement.35,36,39 In this setting, A. baumannii isolation is clinically significant and is most frequently associated with health care-associated infections, particularly ventilator-associated pneumonia, bloodstream infections, and device-related infections, although colonization may also occur.
Regarding specimen type, PDP samples represented the most frequent source of isolation (34%). This finding is consistent with previous studies reporting respiratory tract infections as the predominant clinical manifestation of A. baumannii in hospital settings, with comparable or higher rates, including 33% in Morocco (2012–2017), 30 54% (2010–2015), 31 and 48.3% in Spain (two multicenter studies conducted in 2000 and 2010). 35 Pus specimens constituted the second most frequent source of isolation (21%), followed by blood cultures and urine samples. These findings reflect the predominantly nosocomial nature of A. baumannii infections, particularly in ICUs, where ventilator-associated pneumonia represents the most common clinical presentation, largely driven by environmental contamination and the use of mechanical ventilation. In addition, bloodstream infections, urinary tract infections, and suppurative infections are frequently encountered in ICU settings, mainly associated with invasive procedures such as central venous catheterization and urinary catheterization.35,40
The rate of IPM-resistant isolates was alarmingly high (67%), with increasing trends observed over the study period. Similar findings have been widely reported across different regions, confirming the global emergence of carbapenem-resistant A. baumannii.13,20–23,41 Consequently, the role of carbapenems as first-line agents for the treatment of A. baumannii infections has been increasingly questioned, particularly in light of numerous outbreaks caused by IPM-resistant strains worldwide. In Mediterranean countries, including Algeria, carbapenem resistance is mainly driven by the production of carbapenemases, particularly class D OXAs, although other enzyme families have also been described, including KPC, GES, IMP-like, VIM-like, SIM-like, and NDM groups.13,14,42,43 The dissemination of resistance genes, often plasmid-mediated, further facilitates their rapid spread in hospital environments. 44 Due to financial constraints and limited laboratory resources, we were unable to perform molecular screening for these carbapenemase-encoding genes in our collection. This limitation highlights the need for well-funded surveillance programs to comprehensively assess the genetic mechanisms driving carbapenem resistance in the region.
Notably, a high proportion of MDR isolates was observed among IPM-resistant isolates (n = 106, 67%). This MDR phenotype of A. baumannii is defined by resistance to CAZ and/or IPM in combination with resistance to other antibiotic classes, particularly aminoglycosides and fluoroquinolones.6,10 Previous studies have reported similarly high resistance rates among carbapenem-resistant A. baumannii isolates and have linked these patterns to prolonged hospital stays and the extensive use of broad-spectrum antibiotics. 45 Moreover, epidemic strains have been shown to exhibit higher levels of antimicrobial resistance compared with strains responsible for sporadic infections. 19
Globally, in response to the alarming rise of MDR A. baumannii, increasing attention has been directed toward alternative, nonantibiotic therapeutic strategies. Promising approaches include bacteriophage therapy, which exploits highly specific viruses to lyse bacterial cells, 46 and antimicrobial peptides (AMPs) that disrupt bacterial membranes while minimizing resistance development. AMPs, whether naturally occurring or engineered, have shown antibacterial and antibiofilm activity against A. baumannii in experimental models, and recent studies (including those involving the microbiome) have identified promising candidates capable of reducing bacterial load in vivo; however, systemic toxicity and pharmacokinetic stability remain challenges that must be addressed before large-scale clinical trials can be conducted. 47 Other innovative options encompass immunotherapies aimed at enhancing host defenses, 48 quorum sensing inhibitors that interfere with bacterial communication and virulence, 49 and nanoparticle-based systems that improve drug delivery or exert intrinsic antibacterial activity. 50 In addition, natural plant-based antimicrobial chemicals are promising substitutes for conventional antibiotics. Strong inhibitory effects against bacteria and fungi have been shown by many plant parts, including stems, roots, fruits, flowers, leaves, and seeds. 51 In fact, plant extracts and their essential oils have demonstrated significant efficacy in treating MDR-A. baumannii infections in a number of studies, such as essential oils of Cinnamomum zeylanicum (Cinnamon), the phenolic secondary metabolites of Zingiber officinale roscoe (Ginger), essential oils and extracts of Coriander sativum (Coriander), and extracts of Actinidia deliciosa (Kiwi).52–54 While many of these approaches remain at the experimental or preclinical stage, they represent a crucial avenue of research to complement or replace conventional antibiotics in the fight against MDR A. baumannii.
Conclusion
This 7-year analysis highlights a sustained increase in the frequency of A. baumannii isolates and a high rate of IPM-resistant, MDR strains, particularly in ICUs. These findings underline the critical need for continuous local and national surveillance systems to better characterize the extent, incidence, and temporal trends of A. baumannii resistance. Surveillance data are essential to guide infection prevention and control strategies, optimize antimicrobial stewardship programs, and support evidence-based treatment guidelines. Strengthening routine microbiological monitoring, combined with strict hygiene measures and rational antibiotic use, is crucial to limit the spread of MDR A. baumannii and reduce its public health impact in hospital settings.
Authors’ Contributions
N.B.: Formal analysis, methodology, investigation, and writing—original draft; M.H.: Conceptualization and formal analysis; B.R.: Conceptualization and investigation; L.B.: Conceptualization and formal analysis; M.S.A.: Formal analysis and review and editing.
Footnotes
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No financial support was provided for this article.