
Abstract
Using data from the 2006 Medical Expenditure Panel Survey and the 2000 Census, the authors explored whether race/ethnic disparities in health care use were associated with residential segregation. They used five measures of health care use: office-based physician visits, outpatient department physician visits, visits to nurses and physician’s assistants, visits to other health professionals, and having a usual source of care. For each individual, the authors controlled for age, gender, marital status, insurance status, income, educational attainment, employment status, region, and health status. The authors used the racial–ethnic composition of the zip code to control for residential segregation. The findings suggest that disparities in health care utilization are related to both individuals’ racial and ethnic identity and the racial and ethnic composition of their communities. Therefore, efforts to improve access to health care services and to eliminate health care disparities for African Americans and Hispanics should not only focus on individual-level factors but also include community-level factors.
Keywords
African Americans and Hispanics tend to have lower rates of use of health care services than Whites (Mayberry, Mili, & Ofili, 2005; Shi, 1999; Smedley, Stith, & Nelson, 2003; U.S. Department of Health and Human Services & Agency for Healthcare Research and Quality, 2008). Race and ethnic differences in health insurance status, income, and educational attainment are factors often listed as contributors to observed disparities in health care use. In comparison to Whites, African Americans and Hispanics are more likely to be uninsured or covered by Medicaid and have lower incomes and lower levels of education (DeNavas-Walt, Proctor, Smith, & U.S. Census Bureau, 2010). Deficits in these enabling factors tend to reduce health care consumption even when comparing individuals with similar health needs (Andersen, 1995).
Researchers who have decomposed race and ethnic differences in health care use have found that race and ethnic differences in individual-level enabling factors and health status do not fully account for these observed differences (Gaskin et al., 2007; Hargraves & Hadley, 2003; Weinick, Zuvekas, & Cohen, 2000). The residual difference is usually attributed to unobserved factors such as patient preferences, cultural differences, medical mistrust, provider biases, stereotyping, and poor patient–provider communication (LaVeist, Nickerson, & Bowie, 2000; Smedley et al., 2003). While these patient-level and provider-level factors are important determinants of health care utilization, the Institute of Medicine also points to health care system–level factors as possible sources of health care disparities (Smedley et al., 2003). In particular, the Institute of Medicine report highlights differences in the way that health care systems are organized, financed, and the availability of services as contributors to lower utilization by racial and ethnic minorities.
In this article, we explore the association between residential segregation and health care use. Residential segregation is important because it is associated with social forces that shape culture and preferences regarding health care use, inequities in health care marketplace across community, and disparities in environmental risk factors that affect health needs. We contend that a portion of observed race and ethnic disparities are actually “place” disparities because geographic-level factors are correlated with the racial and ethnic composition of neighborhoods, towns, and communities. Typically, researchers control for geographic-level factors using regional and urban–rural indicators or sometimes with state-, city-, or county-level variables or fixed effects. However, the geographic areas covered by these variables are too large to adequately adjust for market-level factors that vary within these geographic units. Residential segregation is a phenomenon that occurs within these geographic units. People are not randomly distributed by race/ethnicity within counties, cities, or states. Consequently, adjusting for the availability of providers within these geographic units does not control for the variation in provider availability across African American, Hispanic, and White neighborhoods.
There is still much work to be done to understand the relationship between residential segregation and health care utilization. Sociologists have found that residential segregation affects minority access to quality jobs, housing, education, public safety, and social networks (Charles, 2003; Wilson, 1987). There are some studies that show segregation’s influence on access to health care. A few studies report that segregation in hospital care resulted in minorities receiving less care and lower quality care compared with Whites (Sarrazin, Campbell, & Rosenthal, 2009; Smith, 1998; Smith, Feng, Fennel, Zinn, & Mor, 2007). There is evidence that segregation reduced minority access to physicians and hindered physician referrals for other medical services (Bach, Pham, Schrag, Tate, & Hargraves, 2004; Bronstein, Adams, & Florence, 2004; Fossett, Chang, & Peterson, 1991; Fossett, Perloff, Kletke, & Peterson, 1991; Mitchell, 1991; Perloff, Kletke, Fossett, & Banks, 1997; Reschovsky & O’Malley, 2008). Hargraves and Hadley (2003) found that community-level characteristics accounted for some racial and ethnic differences in having a regular provider and seeing a doctor within the past year. African Americans and Whites in a low-income integrated community had similar rates of health care use in contrast with disparities reported nationally (Gaskin, Price, Brandon, & LaVeist, 2009). One study conducted in 1997 found that pharmacies located in minority communities in New York City were less likely to adequately stock opioids (Morrison, Wallenstein, Natale, Senzel, & Huang, 2000). The reasons pharmacists gave for inadequate supplies of opioids were low demand, fear of theft, and regulations regarding fraud, abuse, and disposal.
New Contribution
Prior research has demonstrated that individual-level factors contribute to racial and ethnic disparities in health care. Using data from the 1996 Medical Expenditure Panel Survey (MEPS), Weinick et al. (2000) reported that 23% to 45% of disparities between Whites, African Americans, and Hispanics were due to racial and ethnic differences in health insurance and income. Using data from the 1996-1997 and 1998-1999 Community Tracking Surveys, Hargraves and Hadley (2003) concluded that health insurance was the primary drivers of disparities between African Americans and Whites, and health insurance and income were the main drivers of disparities between Whites and Hispanics. They included community-level measures of physicians and safety net resources and found that they did not explain much of the disparities in access and use. They concluded that the supply of medical resources was not as important for minority groups. However, their study measured provider availability using metropolitan-level and county-level variables. These measures are too broad because they do not reflect the geographic variation in the availability of health services within cities and counties. We hypothesize that this variation is associated with the racial and ethnic composition of neighborhoods.
Our study explores the role of place at the neighborhood or community level. We hypothesize that community factors at the zip code level contribute to race and ethnic disparities. The literature on residential segregation makes the case that distribution of community-level resources within cities and counties is related to the racial and ethnic composition of neighborhoods (Massey & Denton, 1993; Williams & Collins, 2001; Wilson, 1987). Our study advances the literature on health care disparities by exploring the role of place at the zip code level and the interaction between race/ethnicity and place.
Conceptual Framework
Andersen and Aday (1978) provide the basic framework for understanding the determinants of health care utilization. They posit that predisposing factors (age, gender, race, and education), enabling factors (income, health insurance status, and provider availability), and health needs (overall health status, symptoms, and concomitant conditions) determined health care use. We hypothesize that the racial composition of neighborhoods potentially affects health care utilization through all three domains.
Racial composition of neighborhood may influence preferences and culture that are associated with racial identity. The racial composition of neighborhood affects the social networks available to individuals. Compared with Whites, minorities have less informal access to medical experts because of the size and composition of their social networks (Cornwell & Cornwell, 2008). Physicians and other health professionals may not be in their social networks because they do not reside in predominantly Black or Hispanic neighborhoods, particularly those that are low income (Wilson, 1987). Peers can influence the information that individuals use to make decisions and their preferences for providers. In particular, peers can affect relative rankings of choices because individuals may value the opinions of their neighbors. If, in general, the experiences of African Americans and Hispanics within health care tend to be different than the experiences of Whites then the information available to individuals in social networks that are predominantly African American or Hispanic will vary. Studies report that higher rates of perceived discrimination and low rates of trust in medical providers among African Americans and Hispanics compared with Whites contributed to disparities in health care use (Burgess, Ding, Hargreaves, van Ryn, & Phelan, 2008; Casagrande, Gary, LaVeist, Gaskin, & Cooper, 2007; Hausmann, Kressin, Hanusa, & Ibrahim, 2010; Johnson, Saha, Arbelaez, Beach, & Cooper, 2004; LaVeist et al., 2000; LaVeist, Rolley, & Diala, 2003). The impact of residential segregation could result in cultural preferences that discourage health care utilization and thus lower the demand for health care services in minority communities.
The racial composition of neighborhood influences the use of health care because of its impact on the supply of health care providers. Fewer providers locate in minority neighborhoods because of lower provider reimbursement rates. Higher proportions of African Americans and Hispanics are covered by Medicaid or are uninsured. Also, African Americans and Hispanics have lower incomes and are therefore less able to pay for services out of pocket. This should affect office-based providers differently from hospital-based providers because reimbursement policies vary by site of care. Hospital-based providers typically receive better Medicaid reimbursement and more generous uncompensated care payments. Also, differences in insurance coverage policies toward physician services compared with nonphysician services make the supply of the latter more sensitive to the patients’ ability to pay for service out of pocket.
The lower supply of physicians and other health care providers in minority neighborhoods may also be due to the lower quality of community amenities such as public safety, transportation services, garbage collection, public schools, and restaurants (Alba, Logan, & Bellair, 1994; Massey, Condran, & Denton, 1987; Massey & Denton, 1993; Massey & Fong, 1990). Fewer providers in minority neighborhoods increase the time price of using health care services because residents have to wait longer to see community providers or travel to providers outside their neighborhoods, affecting their work schedules. The lack of local providers increases the time price for residents in minority neighborhoods relative to persons living in predominantly White neighborhoods. While residents of White neighborhoods presumably have similar geographic access to providers outside their communities or near their places of work, they also have better geographic access to care at home.
At the structural level, sociological research has underscored the role of residential segregation as a primary institutional mechanism of racism and a fundamental cause of racial disparities in health (LaVeist, 1989; Massey & Denton, 1993; Williams & Collins, 2001). Residential segregation is considered an institutional mechanism of racism because it separates racial/ethnic groups into different neighborhoods, determines the type of resources (i.e., employment, social, economic, and health) available in those neighborhoods, and determines the type of goods and services (i.e., convenience vs. grocery stores) needed to improve life chances (Massey & Denton, 1993; Wilson, 1987). Since residential segregation patterns have not changed much since the 1970s, African Americans and Hispanics are more likely to live in racially homogenous communities.
Residential segregation can be regarded as a “fundamental cause of disease” since social factors account for 60% to 75% of the variance in disease vulnerability (Williams & Collins, 2001). Fundamental cause theory contends that social causes have a persistent association with disease despite changes in intervening mechanisms since fundamental causes involve access to resources and exposure to risk factors that can be used to avoid risk or to minimize the consequences of disease once it occurs (Link & Phelan, 1995). Fundamental causes such as socioeconomic status, race/ethnicity, and gender are tied to resources such as money, power, prestige, and social connectedness, where those with the most access and control over resources are in a better position to avoid risks, diseases, and the consequences of disease. Social groups that reside in residentially segregated neighborhoods often lack the health resources (i.e., doctors, health information, innovative technologies) needed to circumvent disease, since the majority of programs aimed to improve health have focused on behavioral interventions at the micro level. Minorities who reside in homogenous neighborhoods may be at a “double disadvantage” because society sometimes deprives them of opportunities (i.e., education, social advancement) because of their racial/ethnic identity, and they reside in neighborhoods that do not offer similar quality resources and public services available in White communities. For these reasons, residential segregation may increase the health needs of persons living in minority communities, thus increasing their demand for health care services.
Data and Method
We used data from the 2006 MEPS and the 2000 U.S. Census Summary File 1 to determine whether residential segregation was associated with health care use. MEPS is a longitudinal survey that covers the U.S. civilian noninstitutionalized population. The Agency Healthcare Research and Quality fields the MEPS based on a sampling frame of the National Health Interview Survey. The survey consists of five interviews conducted over a 2½-year period. MEPS is unique in its ability to link data on individuals and households (including demographics, health status, employment, and income) to information on their use of health services. This information includes sources of payment for specific medical services, health insurance status, and the details of individual/household health plans. Each of the five interviews conducted for the panel asked about all health care utilization and associated expenditures for a specific period of time, and these periods cumulatively covered the 2-year period.
There are 23,791 noninstitutionalized adults aged 18 years and older in the 2006 MEPS. We restricted this sample to non-Hispanic Whites, Hispanics, and non-Hispanic African Americans living in metropolitan statistical areas (MSAs) for which we had zip code–level data for a total of 17,514. (For ease of composition, we dropped the non-Hispanic suffix for Whites and African Americans.) We were unable to study Asians because there were only 48 Asians out of the 896 in the MEPS living in predominantly Asian zip codes. Sample includes 9,210 Whites, 3,286 African Americans, and 5,018 Hispanics. We divided the sample by racial and ethnic composition of the respondent’s zip code: predominantly White, predominantly African American, predominantly Hispanics, and integrated/other. The definitions for each of these categories are listed below. Table 1 displays the distribution of the sample adults.
Distribution of the Sample of Adults in Person Level Reported Metropolitan Statistical Areas in the 2006 Medical Expenditure Panel Survey by Racial Composition of Zip Code
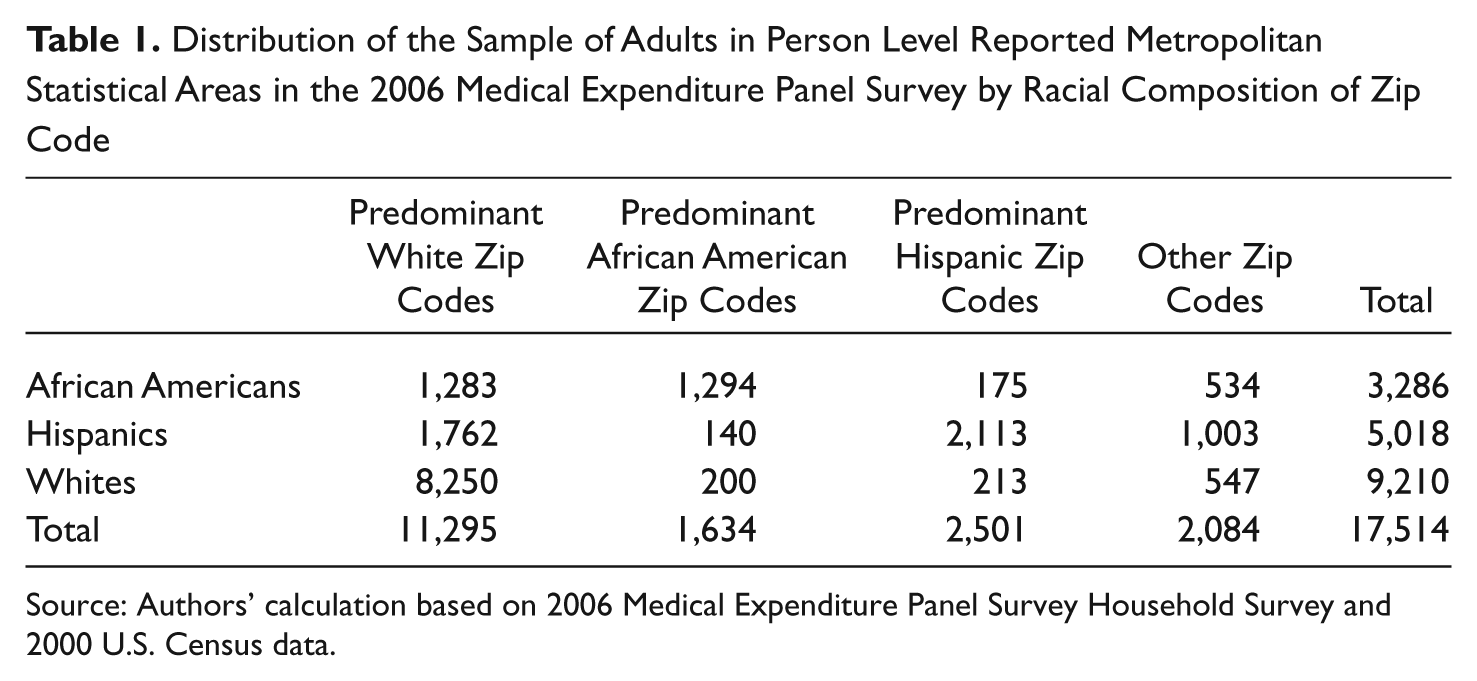
Source: Authors’ calculation based on 2006 Medical Expenditure Panel Survey Household Survey and 2000 U.S. Census data.
We used five measures of health care services use: office-based physician visits, outpatient department physician visits, visits to nurses or physician’s assistants, visits to other health professionals, and having a usual source of care (USC). Physician visits included services provided by primary care and specialty physicians. Visits to nurses or physician’s assistants included services provided by nurses and nurse practitioners, physician’s assistants, or midwives. Nurse and nurse practitioners provided the bulk of these services in this category. Other health professional visits included services provided by chiropractors, dentists, optometrists, podiatrists, physical therapists, occupational therapists, psychologists, social workers, acupuncturists, massage therapists, homeopathic/naturopathic/herbalists, or alternative/complementary care professionals. Chiropractors provided most of the services in this category, followed by physical therapists and psychologists. Our models controlled for age, gender, marital status, poverty status, insurance status, income, educational attainment, employment status, region, and health status.
We linked the MEPS data to the race–ethnic composition of the zip code. Race–ethnic composition was measured with four indicator variables that denoted whether the zip code was predominantly (50% or more) White, predominantly African American, predominantly Hispanic, or Integrated/Other (no predominant group or predominantly other). We used dichotomous variables to define the racial/ethnic composition of a zip code because the distribution of the percentage of minority residents across zip codes is skewed. Of zip codes in MSAs, only 5.0% were predominantly African American and 3.9% were predominantly Hispanic; however, large proportions of African Americans (40.9%) and Hispanics (37.7%) in MSAs reside in predominantly African American and Hispanic zip codes, respectively. We combined the respondents’ race/ethnicity with the race/ethnic composition of the zip code to create 12 race/ethnicity–place indicator variables, for example, Whites living in predominantly White zip codes, African Americans living in predominantly White zip codes, and Hispanics living in predominantly White zip codes.
We estimated four sets of logistic regression analyses to compute the odds of having a visit or a USC for African Americans and Hispanics relative to Whites. The first set of regressions is our base model that estimates disparities by race and ethnicity controlling only for individual-level characteristics. In this base model, Whites were the reference group and the coefficients of interest were the indicator variable for African American and Hispanic race/ethnic identity. We exponentiated the coefficients on the African American and Hispanic indicator variables to compute the odds of having a visit or USC relative to Whites. The second set of models adds place indicators to the base specification. In this model, predominantly White zip codes were the reference place and the coefficients of interest were the indicator variables for predominantly African American, predominantly Hispanic, and Integrated/Other zip codes. The third set of models estimated disparities by allowing interactions between race–ethnicity and place. These models tested whether the association of place was uniform across race and ethnic groups. For these models, instead using the African American and Hispanic indicator variables, we substituted 11 race/ethnicity–place indicator variables using Whites living in predominantly White zip codes as the reference category. The fourth set of models estimated disparities by race and ethnicity within place. We stratified the sample by racial and ethnic composition of the zip code and used the traditional specification to determine whether there were disparities in utilization within zip code type. We performed the analysis using the survey estimation procedures in STATA© 11 to control for strata and sampling units because the MEPS has a complex sampling design.
Findings
We report estimates of the rates of use (with 95% confidence intervals) by race/ethnicity and type of zip code in Table 2. Overall, we observed that African Americans and Hispanics have lower rates of use than Whites. This was true for all zip codes and regardless of the racial or ethnic composition of the zip code. We also observed that persons residing in African American and Hispanic zip codes had lower rates of use than persons in predominantly White zip codes. This was true for African Americans, Hispanics, and Whites. Generally, Hispanics had the lowest rates of use, and rates of use were lowest in predominantly Hispanic zip codes. Race and ethnic disparities were greatest for nonphysician services.
The Proportion of Persons Having Physician and Nonphysician Visit During the Year and Having a Usual Source by Race/Hispanic Origin and Racial Composition of Zip Code
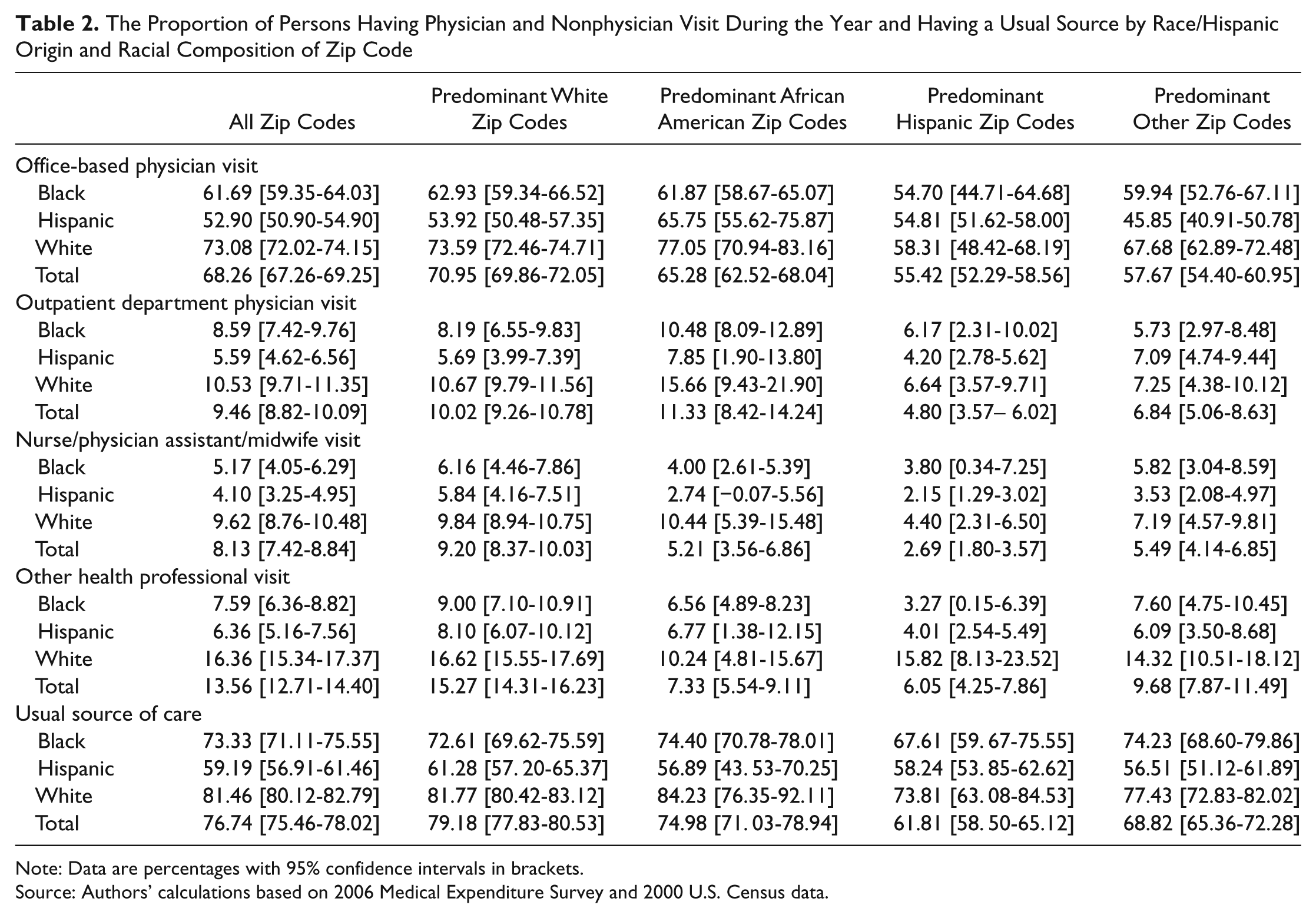
Note: Data are percentages with 95% confidence intervals in brackets.
Source: Authors’ calculations based on 2006 Medical Expenditure Survey and 2000 U.S. Census data.
In Table 3, we report race and ethnic disparities in health care use without controlling for the minority composition of the zip code. We found that African Americans were less likely to have office-based physician visits. The odds of African Americans having at least one office-based physician visit were almost 30% lower than Whites. We did not find a disparity in the use of physicians based in outpatient departments. African Americans and Hispanics were less likely to have a nurse or physician’s assistant visit. The odds of African Americans and Hispanics were about 50% lower than Whites. African Americans and Hispanics were a little more than 45% less likely to have a visit to other health professionals. Hispanics were less likely to have a USC. The odds of Hispanics having a USC were almost 25% lower than Whites.
The Association Between Race/Hispanic Origin and Having Physician and Nonphysician Visit During the Year and Having a Usual Source
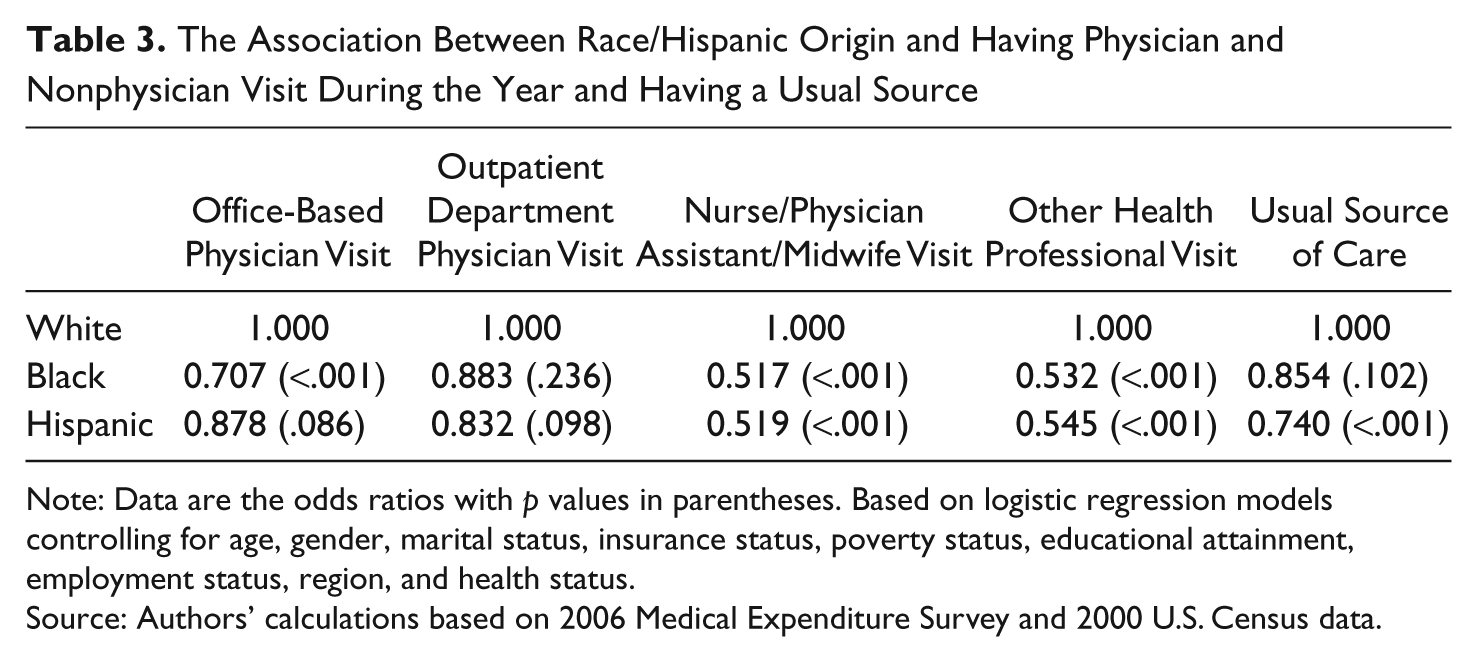
Note: Data are the odds ratios with p values in parentheses. Based on logistic regression models controlling for age, gender, marital status, insurance status, poverty status, educational attainment, employment status, region, and health status.
Source: Authors’ calculations based on 2006 Medical Expenditure Survey and 2000 U.S. Census data.
We report the associations of the racial–ethnic composition of place with utilization in Table 4. Adding the zip code variables to the models did not significantly change the estimates on race and ethnicity. Race and ethnicity still matters even when we consider place. Place matters but the associations were not uniform across the type of service or across predominantly minority zip codes. Compared with persons living in predominantly White zip codes, persons living in predominantly Hispanic zip codes had the greatest disadvantage with significantly lower odds of use in three of the five categories. Persons living in predominantly African American zip codes were not statistically different from persons living in predominately White zip codes. Persons living in integrated zip codes were less likely to have an office-based physician visit and nurse or physician’s assistant visit.
The Association Between Race/Hispanic Origin and Having Physician and Nonphysician Visit During the Year and Having a Usual Source
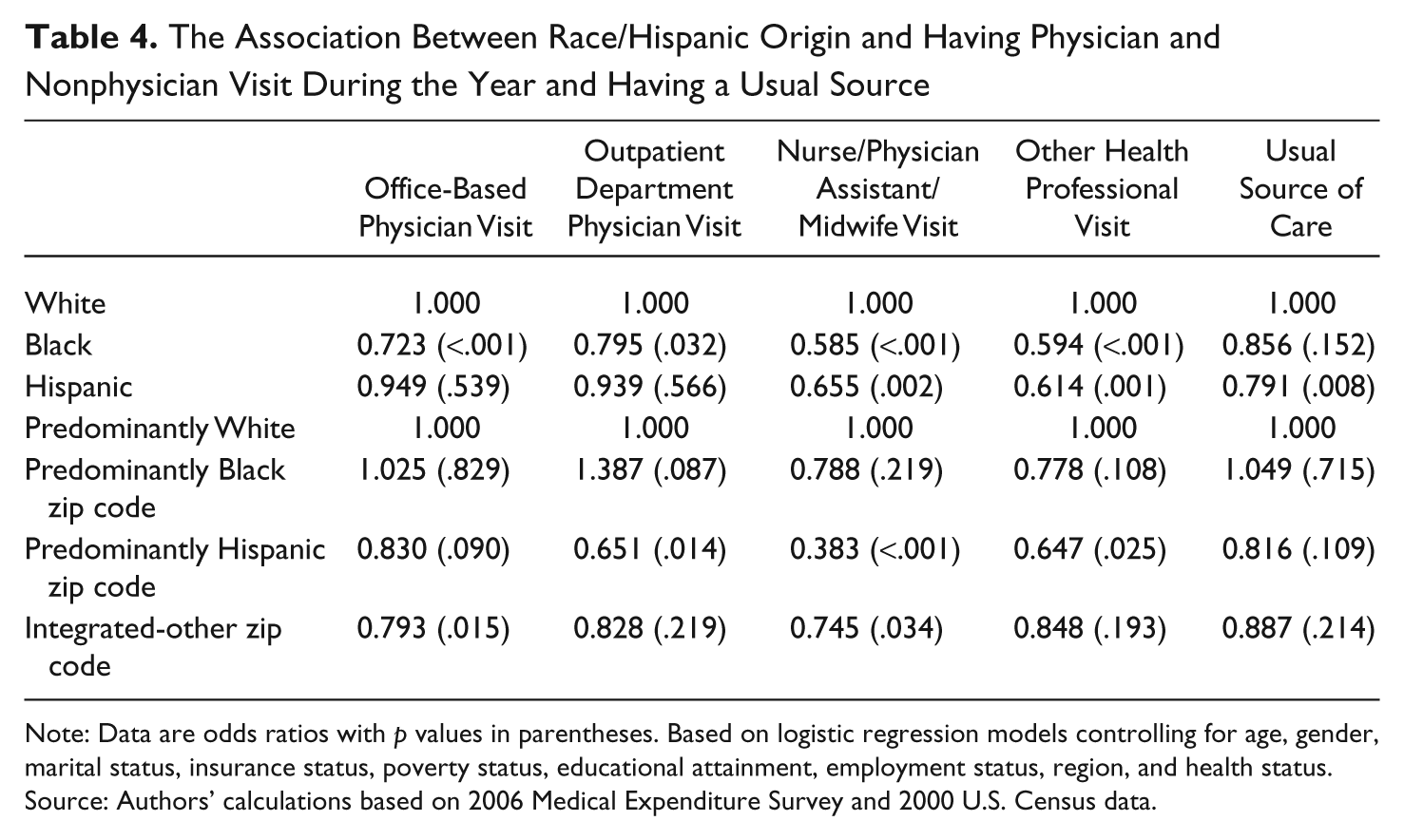
Note: Data are odds ratios with p values in parentheses. Based on logistic regression models controlling for age, gender, marital status, insurance status, poverty status, educational attainment, employment status, region, and health status.
Source: Authors’ calculations based on 2006 Medical Expenditure Survey and 2000 U.S. Census data.
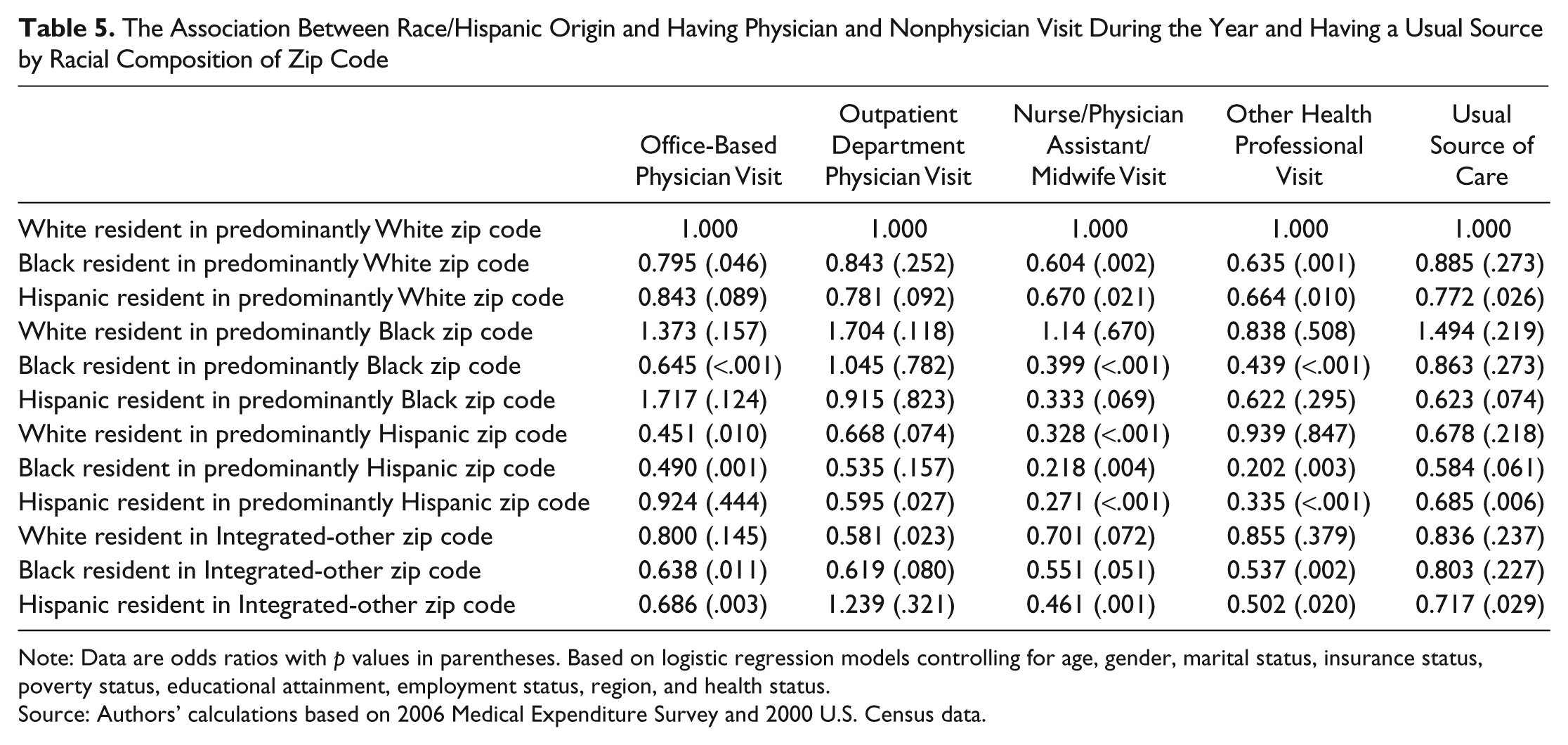
The impact of place was not uniform across racial and ethnic groups. In Table 5, we report the odds of health care use for each race and ethnicity group by the race/ethnic composition of the respondent’s zip code. The reference group was Whites residing in predominantly White zip codes. For office-based physician visits, we found that African Americans residing in predominantly White zip codes were less likely to have a physician visit compared with Whites residing in predominantly White zip codes. However, African Americans residing in predominantly African American, predominantly Hispanic zip codes, and integrated zip codes were at a greater disadvantage compared with Whites residing in predominantly White zip codes. The odds for African Americans having an office-based physician visit declined from 0.795 in predominantly White zip codes to 0.645 in predominantly African American zip codes, 0.638 in integrated zip codes, and 0.490 in predominantly Hispanic zip codes. Similar to the base model, Hispanics’ use of office-based physicians were not statistically different from Whites residing in predominantly White zip codes with the exception of Hispanics in integrated zip codes (odds ratio [OR] = 0.686). However, the odds of having an office-based physician visit for Whites residing in predominantly Hispanic zip codes were 55% lower compared with the odds for Whites residing in predominantly White zip codes. There were no significant differences between Whites residing in predominantly African American and integrated zip codes and Whites residing in predominantly White zip codes.
The Association Between Race/Hispanic Origin and Having Physician and Nonphysician Visit During the Year and Having a Usual Source by Racial Composition of Zip Code
Note: Data are odds ratios with p values in parentheses. Based on logistic regression models controlling for age, gender, marital status, insurance status, poverty status, educational attainment, employment status, region, and health status.
Source: Authors’ calculations based on 2006 Medical Expenditure Survey and 2000 U.S. Census data.
For outpatient department physician visits, the overall disparity between Hispanics and Whites appears to be due to, primarily, the disparity between Hispanics living in Hispanic zip codes and White living in White zip codes. The odds of having an outpatient department physician visit for Hispanics living in Hispanic zip codes were almost 40% lower compared with Whites living in White zip codes.
For nurse/physician’s assistant visits, we found that residing in predominantly African American, predominantly Hispanic, and integrated zip codes increased the disparities in use between the minorities and Whites. Both minority groups were less likely to use nurse/physician’s assistant services; however, their relative use declined significantly when they resided in predominantly African American or Hispanic zip codes. The odds ratio declined by 33% to 65% for both minority groups when they live in predominantly African American or Hispanic zip codes. In addition, Whites residing in Hispanic zip codes were less likely to use nurse/physician’s assistant services. Their disparity with Whites in White zip codes was almost as large as the disparities for their minority neighbors.
For African Americans the pattern of results for other health professional visits was similar to the results for office-based nonphysician visits. African Americans living in predominantly White zip codes were less likely to use other health professional services compared with Whites in White zip codes. The disparity was greater for African Americans in predominantly African American, predominately Hispanic, and integrated zip codes. For Hispanics, we found that Hispanics living in Whites zip codes were about 35% less likely to use other health professional than Whites living in White zip codes. This disparity in the use of other health professionals was larger for Hispanics living in predominately Hispanic zip codes (almost 65%) and integrated zip codes (about 50%). The disparity in having a USC between Hispanics and Whites was greater for Hispanics residing in predominantly Hispanic and integrated zip codes.
To explore whether disparities exist within zip codes of similar racial and ethnic composition, we stratified the sample by racial–ethnic composition and estimated the base models. The results are reported in Table 6. We found disparities between Whites and African Americans and Whites and Hispanics even within zip codes of similar race–ethnic composition. However, these disparities did not always match the overall disparities reported in Table 3. In the predominantly African American, Hispanic, and White zip codes the direction of the association was the same with two exceptions, but the significant odds ratios did not correspond to the overall race–ethnicity associations. In predominantly White zip codes, African Americans and Hispanics were less likely to use nurse/physician’s assistant services and other health professionals compared with Whites. In predominantly African American zip codes, African Americans were less likely to use physician and nurse/physician’s assistant services compared with Whites. In predominantly Hispanic zip codes, African Americans and Hispanics were less likely to use other health professionals compared with Whites. Integrated zip codes differed most from the results in Table 3. In integrated zip codes, we found only one significant disparity: Hispanics were more likely to have an outpatient department physician visit.
The Association Between Race/Hispanic Origin and Having Physician and Nonphysician Visit During the Year and Having a Usual Source by Racial Composition of Zip Code

Note: Data are the odds ratios with p values in parentheses. Based on logistic regression models controlling for age, gender, marital status, insurance status, poverty status, educational attainment, employment status, region, and health status stratified by racial composition of zip code.
Source: Authors’ calculations based on 2006 Medical Expenditure Survey and 2000 U.S. Census data.
Conclusions
Our findings suggest that disparities in health care utilization are related to both individuals’ racial and ethnic identity and the racial and ethnic composition of their communities. Therefore, efforts to improve access to health care services and eliminate health care disparities for African Americans and Hispanics should not only focus on individual-level factors but also include community-level factors. Furthermore, efforts to eliminate disparities have focused primarily on physician services. However, we found large disparities in use of nonphysician services that have been neglected by policy makers. Public policy should address individual- and community-level factors that contribute to these disparities in nonphysician services. These findings highlight the importance of community health and population-based approaches to improve minority health, and evidence suggests that these strategies can be effective. The Center for Disease Control and Prevention established the Racial and Ethnic Approaches to Community Health (REACH) in 1999 to address Center for Disease Control and Prevention’s Healthy People 2010 goals of improving minority health and eliminating health disparities (Collie-Akers et al., 2007). The REACH program empowers community-based organizations in 40 communities across the United States to address six priority health problems: cardiovascular disease, diabetes, breast and cervical cancer screening and prevention, asthma, immunizations, and infant mortality. REACH has four targeted populations: African Americans, Asians, Hispanics, and American Indians/Alaskan Natives. These community-based organizations are charged with planning, developing, and implementing effective interventions that improve minority health in their community. They achieve through health education, health promotion, training, advocacy, organizing, and implementing programs. The program consists typically of one community-based organization in collaboration with three other locally based organizations including an academic research center or local/state health department. Programs may address the negative effects of segregation on culture and preferences of residents in minority communities that discourage appropriate health care use. Evaluations of REACH found that it was effective in addressing cholesterol screening and diabetes-related amputations (Jenkins, Myers, Heidari, Kelechi, & Buckner-Brown, 2011; Liao, Tucker, Siegel, Liburd, & Giles, 2010), suggesting that community-based approaches can be effective for improving the health of minority populations.
We hypothesize that racial and ethnic composition of zip codes is a proxy for the impact of segregation on the availability of health care resources. Future studies should explore more thoroughly the relationship between health care disparities and measures of geographic availability of health care resources. The new health care law offers an opportunity to examine whether increasing health providers can reduce the persistent racial and ethnic disparities in health service use. The Patient Protection and Affordable Care Act (PPACA) provides $11 billion to expand community health centers and the National Health Service Corp that provide health care services in underserved areas. PPACA increases payments to primary care providers in Medicare and Medicaid, making primary physician practices more financially viable in minority communities. Most important, PPACA will reduce the number of uninsured from 49.9 million to an estimated 22.1 million by expanding Medicaid to persons below 133% FPL and give low-wage earners and small businesses access to coverage through health insurance exchanges (Buettgens, Garrett, & Holahan, 2010). Increasing the financial viability of office-based physician services in minority communities should encourage more health providers to locate in these communities, increasing access to services for its residents.
As a whole, residents in predominantly Hispanic neighborhoods, irrespective of race, tend to have low levels of access to ambulatory services, although some of these effects we measured were not statistically significant. However, it is interesting that the effect on the use of office-based physician services was more moderate for Hispanics living in predominantly Hispanic zip codes compared with their White and African American neighbors (see Table 5). We offer three possible explanations for this protective effect. Perhaps Hispanics living in predominately Hispanic neighborhoods have access to social networks that promote health services use. Also, Spanish speakers may have an advantage accessing physicians in Hispanic communities. Additionally, these communities may have a larger supply of language concordant providers encouraging greater use (Hart et al., 2007; Palloni & Elizabeth, 2004). Prior research has found that international medical graduates from Cuba, the Dominican Republic, and Central and South America are more likely to locate in states with large Hispanic populations (Hart et al., 2007), and thus, physicians trained in these countries may be more inclined to serve predominantly Hispanic communities. Our findings suggest that Hispanics living in predominantly Hispanic neighborhoods did not have a similar advantage over their White neighbors in the use of hospital-based physician and nonphysician services. This may be due to physicians’ ability to establish financially independent medical practices relative to other health care providers who are more dependent on hospitals, health centers, and clinics for practice settings and/or patient out-of-pocket payments for revenues.
The reduction in the use of nonphysician providers by minority residents is pronounced whether they reside in predominantly White, African American, or Hispanic neighborhood. This is consistent with a 2001 study indicating less use of complementary and alternative medical providers by African Americans and Hispanics (Bausell, Lee, & Berman, 2001). Studies have indicated greater trust and satisfaction among low-income African Americans and Hispanics with nurse practitioners and practices managed by nurse practitioners (Benkert, Peters, Tate, & Dinardo, 2008; Castro & Ruiz, 2009). This could be a lost opportunity to improve care for minorities. The overall reduction could be lack of familiarity with these providers, lack of supply within minority neighborhoods, or both. Public policy should develop models of health care that make preferred nonphysician services more accessible to minorities especially in their communities.
This study has a few limitations. Our measure of race and ethnic composition is from the 2000 Census while our utilization measures are from 2006. Some of the zip codes may have changed during this 6-year interval. However, these are the best data available given that zip code–level data are only available every 10 years, and we will not be able to evaluate the stability of zip codes until the 2010 Census is released. However, prior studies find that residential segregation is persistent in urban areas (Massey & Denton, 1989). Another limitation is our inability to identify the source of the community-level effects. We have a plausible hypothesis, but we are unable to distinguish whether the impact of segregation is due to the lack of health care resources in minority communities or possible cultural effects associated with persons who elect to live in racially and/or ethnically homogeneous communities who may have similar preferences about health care use. This should be the subject of future research. Despite these limitations, this study provides evidence that place matters. Efforts to eliminate disparities in health care should include community-level interventions.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant 1P60MD00214-07 from the National Institute of Minority Health and Health Disparities (NIMHD) of the National Institutes of Health (NIH).