
Abstract
Patient involvement in decisions is central to patient-centered care. Yet many important decisions must be made in complex, ambiguous clinical situations in which all possible options cannot be known, evidence is inadequate to inform patients’ preferences fully, and/or patients are unclear about their desired level of involvement. In these situations, preferences are shaped by affect, framing, and “collaborative cognition” among clinicians, patients, and their families; thus, decisions are often relational, dynamic, iterative, provisional, and/or conditional. Clinicians can help patients achieve greater autonomy by engaging both intuitive and deliberative decision-making processes (“whole mind”) and involving others in exploring, clarifying, and co-constructing patients’ preferences (“shared mind”). Clinical and interpersonal relationships can promote effective decision making through developing a shared attentional focus, tailoring information, and identifying conditions under which provisional preferences might change. Information technology and health systems offer untapped potential to deepen the relationships and conversations within which decisions are made.
Introduction: Context, Evidence, Preferences, and Decisions
A key feature of patient-centered care is meaningful participation of patients and families in decisions regarding their care (Institute of Medicine, 2001). Sometimes, patients, families, and clinicians face decisions where high-quality clinical evidence is available and clear. In these situations, participants can weigh the established harms and benefits of a complete list of available approaches in light of clearly defined goals of care and thus inform patient’s treatment preferences sufficiently to make a decision. Commonly, though, important decisions must be made in complex, ambiguous clinical situations, in which clinical evidence is insufficient, goals and options are not clearly defined, and preferences are contextual, provisional, and conditional. In this article, we focus on approaches for promoting patient-centered decision making under these types of complex and ambiguous conditions. In the first part of the article, we examine several factors that affect decision making in the face of unclear or inadequate evidence. These factors include the level of complexity of the clinical situation, the applicability of clinical evidence to the patient’s situation, other influences on patients’ preferences (e.g., family input, religious beliefs), and the degree to which their decisions are provisional and conditional. In the second part, we propose some ways that patients, clinicians, and health systems can arrive at decisions that are more likely to be viewed by clinicians and patients as approaching optimal decisions. We take the perspective of practicing clinicians aspiring to patient-centered care, avoiding the extremes of paternalism (persuading the patient to adopt a particular view) and “naïve consumerism” (blindly acceding to patients’ expressed but yet unexamined preferences; Epstein & Peters, 2009).
The Clinical Context: Simple, Complicated, and Complex Situations
More than 50 years ago, Lindblom (1959) described the differences in approach required by simple and complex situations. According to Lindblom, in simple situations goals are relatively well defined. In such situations, it is possible to chart a course to achieve desired goals from the outset. This is in contrast to complex situations, in which attainable goals cannot be known fully at the outset—goals often come into focus only after having embarked on a course of action. Thus, in complex clinical situations, actions are undertaken provisionally and conditionally, intermediate goals and outcomes are assessed, and another provisional action is decided on. Often, though, the parties involved never feel that the information they have is complete, and no one is “fully informed.” With the distal goals not completely in focus, actions serve two aims—to achieve an intermediate goal and to bring more distal goals into focus. In choosing to undergo cancer surgery, for example, a patient and his or her surgeon might endorse a general approach (e.g., complete excision) and provisional goals (e.g., cure) prior to starting an operation, but this approach is conditional; anatomical variants, tumor characteristics, and patient factors may prompt the need to slow down, reconsider, and reformulate the goals of the procedure (Moulton, Regehr, Mylopoulos, & MacRae, 2007). Further along, the decision to embark on a course of chemotherapy is also provisional and conditional—the patient’s response to a first cycle of chemotherapy may influence the patient’s and the oncologist’s willingness to stay the course or consider primarily palliative options. Multiple parties with different perspectives and different types of expertise might contribute to incremental decisions over time as the situation evolves to offer a “diversity of analytic attacks” (Lindblom, 1958) on a situation. In health care, these individuals may have a common focus on the patient’s situation even if they never meet, form a “team,” or come to consensus (Haidet, Fecile, West, & Teal, 2009; Lindblom, 1958).
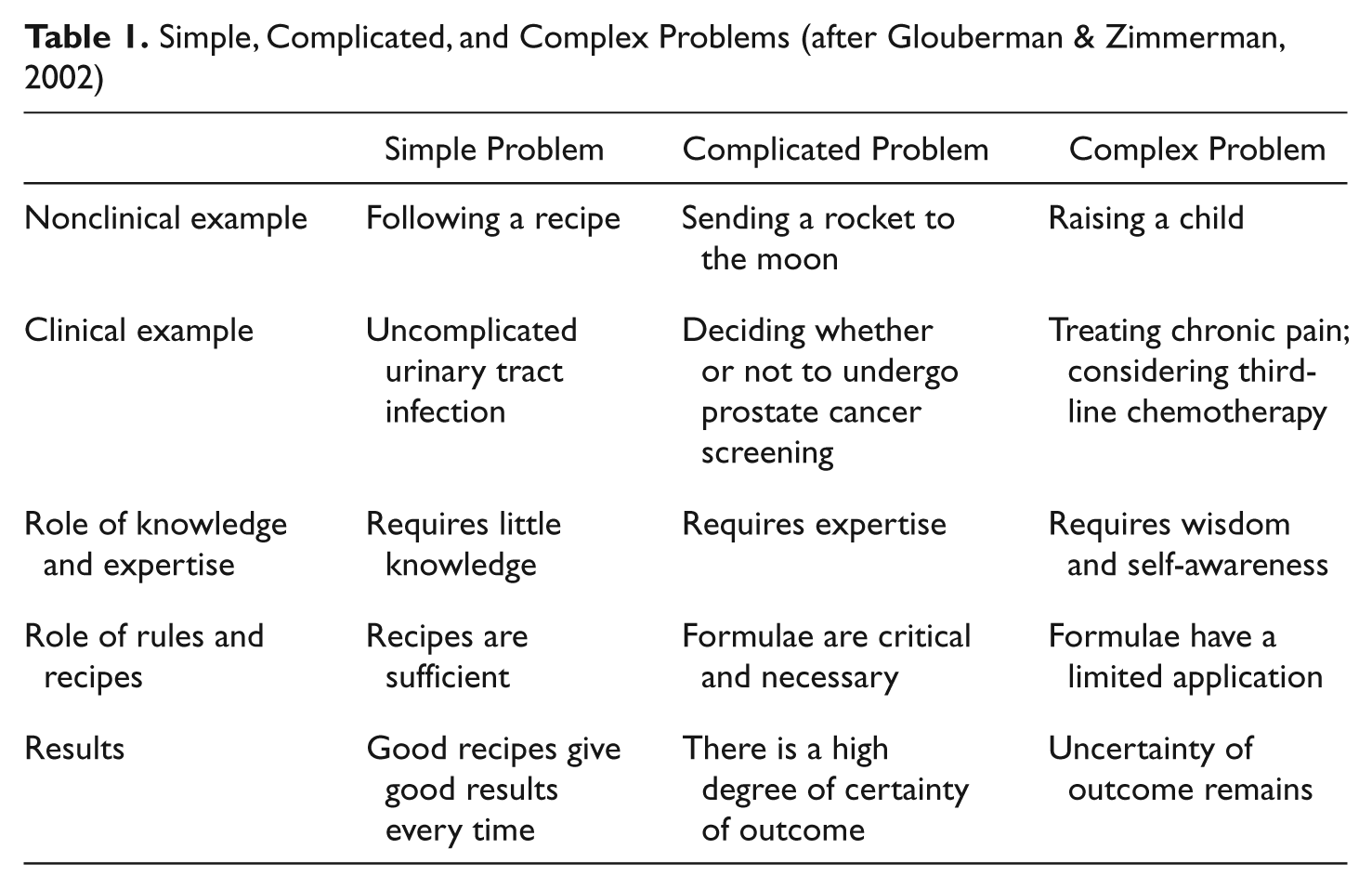
This “muddling through” (Good, 2011; Lindblom, 1959) approach to complex problems has been the subject of intense debate and revision over the 50 years since it was originally proposed. An important elaboration by Glouberman and Zimmerman (2002) in the context of health care also describes “complicated” situations (Table 1)—which represent solvable problems that require training and expertise, as distinguished from those that do not require training and expertise (simple) and those for which training and expertise are insufficient (complex; Glouberman & Zimmerman, 2002). Glouberman and Zimmerman suggest that problems arise when situations that are complex are treated as if they were merely complicated. Considering one complex situation (e.g., deciding whether to change a patient’s chronic low back pain treatment plan). Falzer et al. (2012) suggest that often clearly stated preferences (“I understand that I still have pain but I don’t want to change my pain medications”) often prove to be conditional over time. The situation is often reevaluated as the context changes (e.g., worsening symptoms, worry, or existential distress), prompting a change in preference. Knowing that a situation is complex could prompt clinicians to introduce specific questions about context to help make explicit the conditions under which preferences might change (“What if I could find a pain medication that did not make you sleepy or constipated?”). These questions might also enhance patients’ self-awareness, access to gut feelings (Gigerenzer, 2007), and affective forecasting (Halpern & Arnold, 2008; Wilson & Gilbert, 2010) that help guide future decisions.
Simple, Complicated, and Complex Problems (after Glouberman & Zimmerman, 2002)
The Role of Evidence
In both simple and complicated situations in which clinical options are clearly defined, applying clinical evidence can improve quality of care, reduce unwarranted variations in practice, and highlight concerns for which the patient’s voice is sought (Epstein, Alper, & Quill, 2004). However, because clinical evidence is about populations, even when it is of high quality, individual factors still must be considered. For every guideline, even the most “noncontroversial” ones, there are exceptions—it may not be in a patient’s best interest to have standard chemotherapy for early breast cancer, screening for colon cancer, or “optimal” blood sugar control. Furthermore, evidence is more than a prescriptive mandate (“Treatment A is better than Treatment B at achieving a particular outcome, therefore it is preferred”); it is also descriptive (“With Treatment A, Outcome X is more likely to occur; with Treatment B, Outcome Y is more likely to occur”), requiring some judgment about whether for this patient Outcome X is actually preferred. For example, a patient receiving hospice care may choose to forgo evidence-based empirical antibiotic treatment for presumed bacterial pneumonia, knowing that treatment would only prolong death rather than improve quality of life. In another case, an elderly man may refuse standard hormonal treatment to prevent spread of prostate cancer because the treatment itself has previously caused cognitive and functional decline.
Awareness of the unique characteristics of each clinical situation (e.g., patient age, treatment affordability, patient and family beliefs, patient’s level of literacy, comorbidities) is essential for the wise application of clinical evidence (Boudon, 1991; Flyvbjerg, 2001). For example, determining at what point to start insulin in a person with type 2 diabetes mellitus is a complex decision. While clinical evidence suggests that insulin can prevent complications of diabetes, insulin is also associated with risk of hypoglycemia, and other physical and psychological complications (e.g., weight gain, adopting a “sick role”). In particular, elderly patients and those with serious comorbidities (e.g., advanced cancer, heart failure, untreated depression) may be at greater risk for dangerous side effects and experience fewer benefits from tight control of diabetes, suggesting different parameters for optimal blood sugar levels (Ismail-Beigi et al., 2011). Clinical evidence may provide little wisdom as to exactly when and how the transition to insulin should occur for a particular individual. In these complex situations, an “acquaintance with particulars often makes us wiser than the possession of abstract formulas, however deep” (James, 1902/1961, p. xvii). Eliciting data about these “particulars” requires an ability to adopt multiple perspectives and effective communication with patients and families (McWhinney, 1989); yet this communication often does not occur (Weiner et al., 2007).
Influences on Patients’ Preferences
Preferences are “statements by individuals regarding the relative desirability of a range of health experiences, treatment options and health states” (Brennan & Strombom, 1998, p. 259). Patients and families may have preferences regarding the structure, process, and/or outcome of health care (Donabedian, 1968; Street, Elwyn, & Epstein, 2012). Ideally, patients, families, and clinicians move from uninformed preferences, often based on hypothetical considerations, to informed preferences that reflect a deeper understanding of the situation. Preferences may be uninformed because of lack of basic medical knowledge or ignorance of the full range of options and their attributes. Uninformed preferences may also be because of misunderstandings. For example, clinicians commonly ask patients with serious illnesses whether they wish to have “everything” done (Quill, Arnold, & Back, 2009). Patients, frightened and fearing being abandoned, often acquiesce rather than ask for clarification—not realizing that from a clinician’s perspective, “everything” might signify prolonged, burdensome, and often ineffective efforts at extending life (Quill et al., 2009). Alternatively, expressed preferences for a process (e.g., antibiotics) might not comport with the intended outcome (e.g., symptomatic relief in upper respiratory infections for which antibiotics are ineffective); yet these disconnects often go unquestioned.
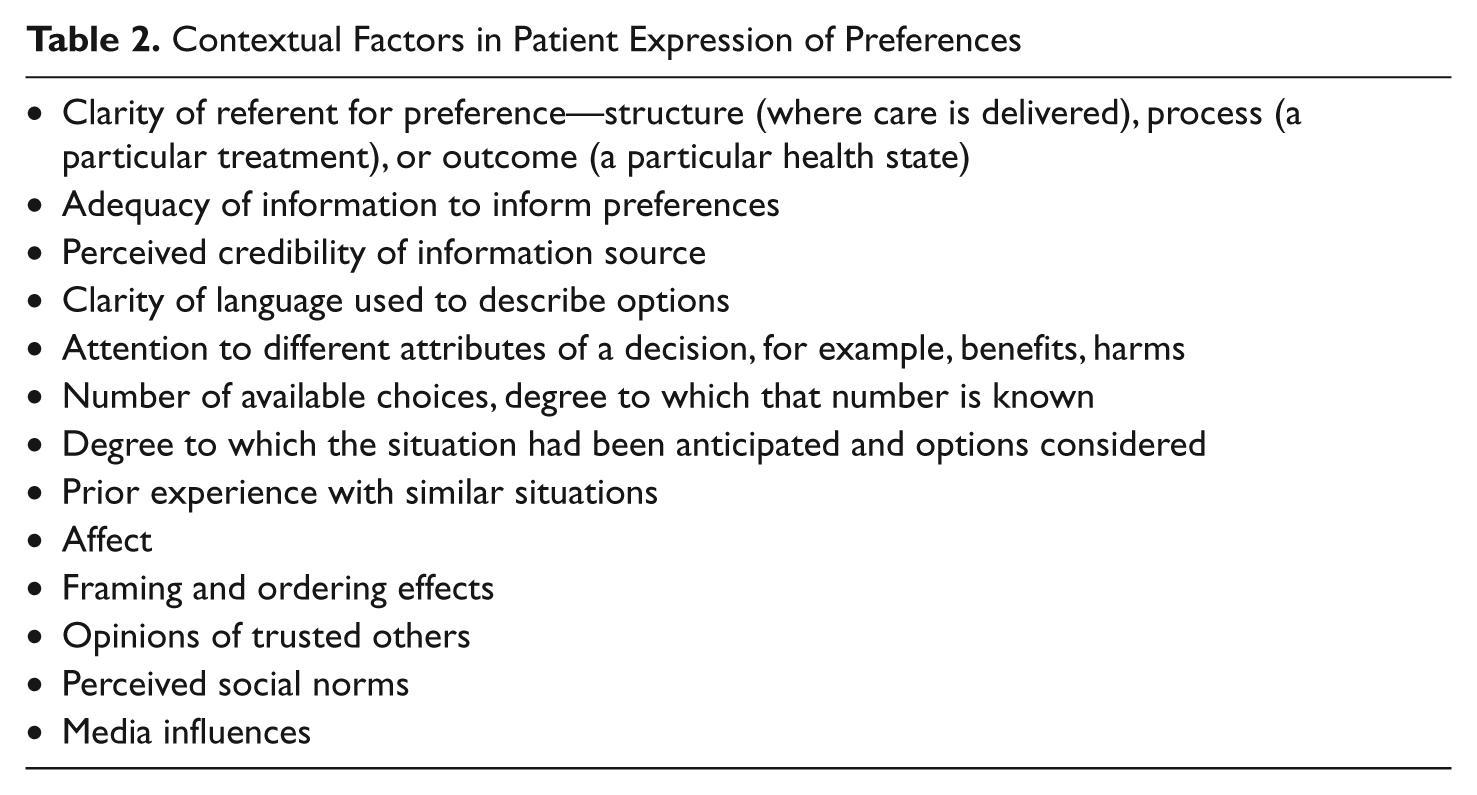
Medical decision-making research has typically considered situations in which preferences are stable and based on known values. Preferences tend to be stable in situations that are familiar and anticipated, and characterized by a limited range of known potential outcomes. Conversely, preferences tend to be unstable (i.e., contextual, conditional, provisional) when patients are anxious, when they confront unanticipated and unfamiliar circumstances, when the situation is affectively charged, and when there are numerous options that are not mutually exclusive (Epstein & Peters, 2009; Lichtenstein & Slovic, 2006; Slovic, 1995). In these situations, common in clinical medicine, preferences are more prone to change; preferences are influenced to a greater degree by context, framing, ordering, affect, unrelated recent events, perceived credibility of the source of information, perceived social norms, and numerous other factors (Table 2; Epstein & Peters, 2009; Fischhoff, 2005; Lichtenstein & Slovic, 2006; Little et al., 2008; Slovic, 1995; Ubel, Loewenstein, Schwarz, & Smith, 2005). In complex situations it is common for decisions to be conditional—depending on disease activity, symptoms, and the personal meaning of the illness (Falzer et al., 2012).
Contextual Factors in Patient Expression of Preferences
These observations might generate a sense of hopelessness about ever being able to define an individual preference in a complex situation and to enact the preference wisely. Fortunately, three concepts borrowed from recent work in cognitive psychology now shed light on how to help clinicians and patients “muddle through” to achieve wise, if not perfect, choices.
First, decision making is optimized when people engage both intuition and deliberation. Intuition involves low-effort, rapid, nonanalytic mental processing (Kahneman, 2003; Norman, Young, & Brooks, 2007), making use of “fuzzy traces” (Reyna, 2008), gut feelings (Gigerenzer, 2007), and mental shortcuts based on tacit rules that have been internalized through experience (Kruglanski & Gigerenzer, 2011). Intuitive processes are most efficient and accurate with relatively familiar clinical situations in which these internalized rules comport with demands of the situation and environment (Norman et al., 2007). However, unexamined use of these mental shortcuts can result in expressed preferences that would change if more closely examined. In contrast, deliberative mental processing is more explicitly analytic, slow, and effortful (Evans, 2008; Kahneman, 2003; Kruglanski & Gigerenzer, 2011). Rather than choosing one mode of thinking, “dual processing” models propose using both modes of cognitive processing to promote the best possible judgments under uncertainty (Evans, 2008; Kahneman, 2003). Clinical expertise thus depends on the ability to move back and forth between the two modes (Moulton & Epstein, 2011). For patients, too, wise choices depend on use of intuitive and deliberative processing—and on the ability to move efficiently between them. Less well understood is how dual processing capabilities are optimized and learned.
Second, exploration of health beliefs can assist with decision making (Falzer et al., 2012), especially beliefs relating to specific illnesses rather than more general health beliefs (Fischhoff, 1991). Consider a patient whose parent had an amputation shortly after having been started on insulin for diabetes. This patient may associate the initiation of treatment with the adverse event (i.e., amputation) that occurred rather than understanding that earlier initiation of insulin therapy may have helped avoid the need for amputation. Exploring such perceptions and experientially informed beliefs can uncover dissociations between intended outcomes (avoidance of amputation) and expressed preferences (avoiding insulin). Another common example is patients’ and families’ decision to refuse increases in pain medications when they believe that pain inevitably accompanies cancer and that addiction would result from use of opioids, however appropriate opioid use may be.
Finally, patients can engage others to help them make decisions. Patients rarely think and feel their way through difficult decisions alone. Normally, the patient’s network of family, friends, and health professionals contribute to the deliberation, such that preferences to some extent reflect the “shared mind” among individuals rather than the cognitions and emotions of a single person (Epstein & Street, 2011). When preferences are shaped by coercive or controlling relationships, they have the potential to diminish patient autonomy, but when shaped by trusting relationships, socially constructed preferences may actually enhance patient autonomy (autonomy-in-relation; Candib, 2002; Entwistle, Carter, Cribb, & McCaffery, 2010). These social influences are especially important when patients are overwhelmed and cognitively overloaded—or when they wish to be assertive but do not know how to assert themselves. As clinicians, we are acutely aware of the serious barriers to creating trusting relationships and effective communication in clinical settings; the challenges include communicating information, involving patients in deliberations regarding their care, and promoting mutual understanding and endorsement of clinical decisions. Here, though, we point to what might be possible and desirable in health care.
Making Better Decisions: Complexity, Preferences, Relationships, and Autonomy
Engaging patients in constructing preferences in the face of complexity, inadequate evidence, and irreducible uncertainty involves more than provision of information and an invitation to choice. It also involves dialogue about the communication process itself; that is, what patients want to know, what information is relevant, how patients prefer to be informed, patients’ roles in decision making, and who else (if anyone) should be present. Seen this way, constructing preferences is relational, dynamic, iterative, provisional, and conditional—it involves building relationships, providing information, and exploring preferences, which then strengthen relationships, understanding, and involvement in decisions. This iterative view amends more linear decision-process models, which describe a stepwise progression from providing tailored information, to identifying choices, reviewing evidence, and then agreeing on an action plan (Charles, Gafni, & Whelan, 1997, 1999; Elwyn, Edwards, Kinnersley, & Grol, 2000; Towle, Godolphin, Greenhalgh, & Gambrill, 1999).
Implied in this relational and dynamic view of decision making is that clinical care is both a set of human interactions as well as a transaction of goods and services (Beach & Inui, 2006; Engel, 1980; Epstein & Street, 2011; Politi & Street, 2011; Tresolini & Pew-Fetzer Task Force, 1994). Patients are embedded in social relationships with friends and family (some of whom might also be health professionals). When well or ill, they encounter representatives of the health care system, who themselves are embedded in relationships with other health professionals. Relationships among health professionals occasionally constitute teams—cohesive self-contained groups—but more often are “communities of care,” reflecting their diffuse nature yet with a focus on an individual patient and his or her illnesses. While these human interactions are relegated to the contextual background when considering episodic or relatively minor illnesses, these relationships grow in importance when considering serious or chronic illness and/or behavior change related to health.
Next, we suggest eight ways to promote relational engagement that in turn can promote effective decision making in complex situations in which clinical evidence does not provide clear answers:
Developing a shared attentional focus
Tailoring information
Informing preferences
Co-constructing preferences
Using “whole mind”
Articulating provisional preferences
Using information technology
Reorienting health systems
Developing Shared Attentional Focus
Shared construction of preferences requires that all parties involved consider the same data as relevant. However, in complex situations, relevant parties often attend to different issues. Facing a choice about prostate cancer treatments, a patient might focus on side-effects, his spouse on cure, and his physicians on technical and procedural aspects of care (Volk et al., 2004). The definition of “effective” might differ, with patients more focused on quality of life, clinicians on survival (Crawford et al., 1997). Thus, it would not be surprising that each would favor a different treatment approach. Attentional focus may be influenced by cultural, religious, and health beliefs, each of which provides a framework for assigning meaning to health-related information. To make attentional focus more explicit, clinicians might say, “It seems that each of us is focusing on a particular aspect of this situation,” and propose ways to achieve a shared focus. Pathways to achieving a shared focus need not be overly complex and typically involve methods that are the foundation for sound communication of evidence in any clinical situation. These methods include using techniques that build patient–clinician partnerships and checking periodically for understanding and agreement between the parties (Epstein et al., 2004).
Tailoring Information
In high-stakes situations, patients usually want control over the timing and delivery of information. They also are concerned that their values and preferences be taken into account but may not want to make the actual decision (Charles et al., 1997; Charles, Whelan, Gafni, Willan, & Farrell, 2003; Strull, Lo, & Charles, 1984). Some patients may prefer information that is actionable (i.e., that would change a plan of care). If so, clinicians should focus on determining, with the patient, how much information is needed to reach a threshold of action, as well as the degree to which it is possible to change course after action is undertaken. Alternatively, patients may want information that helps them make sense of an illness that is experienced as chaotic and meaningless, even if it involves no changes in the clinical management approach. Furthermore, patients not only have preferences for the message and the delivery but also for the messenger; strong trusting relationships set the stage for partnership while lending credibility to the message (Politi & Street, 2011).
Informing Preferences
Often a few questions can help clinicians and patients distinguish between informed and uninformed preferences. A patient’s fear that surgery spreads cancer or his irrational belief that surgery “gets it all” can promote a preference that does not comport with the patient’s underlying values (e.g., for quality of life) in the context of prostate cancer (Zeliadt et al., 2006). In such situations, clinicians might choose to introduce uncertainty and doubt by gently challenging the patient’s assumptions, proposing another way of looking at the situation, while also being aware of the clinician’s potential to manipulate information in such a way that a patient elects a particular option.
Because the mind tends to simplify when cognitive load is high (Oei, Everaerd, Elzinga, van Well, & Bermond, 2006), patients and clinicians risk engaging in premature closure before actively considering relevant options (Croskerry, 2003). Yet for situations in which there are multiple options (e.g., diabetes, HIV, lupus) considering all options at once can be overwhelming. A skilled clinician will not present too much detail and too many options all at one time, perhaps presenting a few examples and waiting for the patient to assimilate them. Clinicians can periodically ask patients to restate their understanding (“teach back”), judge how well they were able to take in and synthesize information, and ask if they would like further information. Based on patients’ reactions, clinicians can then present additional aspects of the situation (Back, Arnold, Baile, Tulsky, & Fryer-Edwards, 2005). As clinician and patient work their way through the preference-construction process, the discussion leads to an evolving shared view of the situation and thresholds for action. Such an approach is also potentially efficient in that the clinician does not waste time presenting information that is neither wanted nor assimilated. As clinical teachers and communication researchers, we have listened to countless mini-lectures by clinicians to patients in which it is not clear what information is desired, understood, and recalled or even recallable when it is needed by the patient. Importantly, although patients might ask for clarification to correct physicians’ mistaken assumptions, few do; more often they back off, feeling misunderstood and disengaged. Efforts to help patients be appropriately involved in clinical care often involve “patient activation” through coaching or information technology (Dimoska, Tattersall, Butow, Shepherd, & Kinnersley, 2008; Kinnersley et al., 2007). Clinicians and patients also need to decide which of the myriad decisions that they face warrants more explicit deliberation and exploration of options in order to make the best use of limited time.
Constructing Preferences
Autonomy can be enhanced through trusting relationships with family, friends, and health professionals (Entwistle et al., 2010). In the context of risk communication, Collins and Street (2009) describe several elements of dialogic process, in which parties in conversation share and reconcile multiple understandings and meanings. These elements are naturally occurring and are common and include defining the nature of the situation, clarifying the goal of the conversation, describing individual perspectives, and managing differences before taking action. In addition, the parties also reconcile intuitions and affects, which in turn, are fundamental to rational judgment (Damasio, 1994). Thus, the construction of preferences involves sharing relevant intuitions, feelings, and emotions as well as logical formulations (Epstein & Peters, 2009).
Decision making, and by implication preference construction, is often distributed across individuals (Rapley, 2008). The term shared mind refers to how ideas can originate through dialogue among two or more individuals (Epstein & Street, 2011; Zlatev, Racine, Sinha, & Itkonen, 2008). A related concept, “collaborative cognition” (Meegan & Berg, 2002), suggests that individuals help each other recall and sort through complex information and choices and reduce the anxiety that often accompanies complex mental tasks—effectively sharing the cognitive load. This naturally occurring process is often effective in clarifying difficult dilemmas. However, when the involvement of others in the preference construction process is implicit, there are dangers of persuasion and coercion. For that reason, transparency and self-awareness are important, for example, distinguishing between what clinicians might want for themselves and what others might desire, or indicating which data they attend to and which they consider less relevant. Mutual recognition that preferences are socially constructed can act as a corrective in power-discordant relationships, such as between doctor and patient. When patients are deferential, for example, clinicians can encourage that decisions be “made together,” opening the door for each participant to bring their expertise, experience, and wisdom to the table.
Using Whole Mind: Engaging Deliberative and Intuitive Modes
Expert clinicians invoke broad principles of care alongside their evolving understanding of the particulars of each patient’s situation (McWhinney, 1989). In primary care and many clinical specialties, clinicians have multiple contacts with patients and build a basis of personal knowledge of the patient and his or her circumstances. Because personal knowledge is always in part tacit (Polanyi, 1983), it tends to inform decisions in unconscious ways. Thus, expert clinicians’ automatic processing is accompanied by a “subsidiary awareness” (Polanyi, 1983). Subsidiary awareness refers to a state of mind in which there is an “attentiveness in automaticity” (Moulton & Epstein, 2011; Moulton, Regehr, Lingard, Merritt, & MacRae, 2010) during routine tasks (e.g., riding a bicycle; removing a gall bladder) that alerts them to tacit assumptions (e.g., the road is smooth and without potholes; the patient’s biliary anatomy is normal) that do not comport with the reality of the situation (e.g., a pothole in the road; aberrant anatomy that raises risk of surgical error). Such alerting, in expert practitioners, prompts the need to slow down and switch temporarily to more deliberative processing. This judicious combination of (or alternation between) automatic and deliberative mental processing appears to help avoid errors and optimize the construction of preferences.
Clinicians can help patients use their whole mind as well. Clinicians have three sets of capabilities they can bring to complex situations:
Interoceptive capabilities—Monitoring their own thoughts, feelings, assumptions, and mental processes that might inform their care of the patient
Exteroceptive capabilities—Engaging in active listening and watching for other indications (e.g., body language, facial expressions, voice tonality) that provide clues to patient understanding and receptivity
Interactive capabilities—Helping patients be aware of their own grasp of the information, assumptions about the meaning of the messages, and willingness to consider alternative approaches
Using these three capabilities, that are in part teachable (Krasner et al., 2009), has been referred to as “mindful practice” (Epstein, 1999). Employing techniques of mindful practice is efficient—they do not appear to lengthen consultations. Yet the skills of mindfulness are rarely modeled or taught explicitly in clinical training.
Articulating Provisional Preferences: Time-Limited Trials
Because preferences in complex situations are often provisional, conditional, and evolving, the desired outcome may not come into focus until after having started on the journey. In many situations, this may be desirable; an 80-year-old and her physician may not know how tightly to control her diabetes until having attempted to do so, and after having experienced positive (e.g., improvements in neuropathy) and negative (e.g., hypoglycemic episodes) effects. Also, provisional preferences may help patients adjust for peoples’ generally poor ability to predict how they will feel subsequently about a decision (affective forecasting)—especially when considering negative health states (e.g., disability, disfigurement; Ubel et al., 2005). Thus, it would be expected that provisional preferences would reverse, adjust, and/or accommodate as information becomes available and health states change.
Enacting treatment decisions that are based on provisional preferences requires doctors and patients to “check in” periodically to reassess the effectiveness of the plan and whether that plan continues to reflect preferences as clinical situations change. Without vigilance to ongoing reassessment, patients run the risk of making decisions that lose sight of their values; decisions that would have been considered conditional inadvertently become irrevocable. For example, medications are often continued without ongoing assessment of whether they are still helpful and needed, resulting in accumulation of low-benefit medications (Moloney, Konrad, & Zimmer, 2011). Similarly, continuing screening tests in people who otherwise have poor prognoses confers no medical benefit yet can contribute to morbidity and anxiety (Sima, Panageas, & Schrag, 2010). “Checking in” is straightforward in concept, but competing clinical demands, pervasive distractions, and discontinuity in the clinician–patient relationship threaten the likelihood that such reassessments will occur. Formalizing reassessment using clinical processes such as “time-limited trials” (Quill & Holloway, 2011) can document a provisional decision and schedule a time to reevaluate that decision. Time-limited trials are most commonly seen in intensive-care settings (e.g., ventilator use), but are applicable to many other decision-making settings (e.g., initiating warfarin with an elder who is at some risk of falling; pharmacotherapy for sleeplessness).
Optimizing Information Technology
Decision support technology is specifically designed to provide, tailor, and help patients tailor disease-specific information and apply information to their current situation (Elwyn, Stiel, Durand, & Boivin, 2010; Hesse, 2005; Nelson, Han, Fagerlin, Stefanek, & Ubel, 2007; O’Connor et al., 2001). Decision aids help patients recognize, inform, and revise their preferences based on information that is relatively free of individual and contextual biases. Tailored formats help patients access and interpret information that they consider relevant in quantities and formats that suit their cognitive styles (Jerant et al., 2007; Kreuter, Farrell, Olevitch, & Brennan, 2000; Street et al., 2009). However, in the authors’ view, information technology has unrealized potential to help patients engage in a deeper dialogue with their clinicians by bringing patients’ perspectives to clinicians’ attention, providing information prior to clinical visits, and helping patients be more effective communication partners, thus making best use of limited time. Importantly, the implementation of information technology can widen (through differential access) or narrow (through targeted interventions) social disparities in patient participation in care (Campbell & Quintiliani, 2006). Along with information provision, the next generation of decision aids can be developed in such a way that they strengthen relationships within which decisions are made and help patients to bring up important questions, concerns, and opinions with clinicians (Epstein, Fiscella, Lesser, & Stange, 2010). This might be accomplished using a range of technologies for purposes that might include
Electronic prompting to help patients formulate questions prior to office visits
Interactive media applications that allow patients to inform physicians of their concerns
Audio-recording patient–physician encounters for later review by patients and clinicians
Monitoring patient symptoms electronically using mobile devices, which can provide alerts to the health care team at appropriate thresholds
Reorienting Health Systems
Increasingly, health care is a team activity, focused on patient-centeredness, safety, and effectiveness (Institute of Medicine, 2001). Yet many health systems initiatives have focused on simple and complicated problems, such as computerized order entry systems to reduce medication errors and implementing protocols for medications following a heart attack. Systems efforts to promote “patient-centered care” have focused on structural and technological enhancements and information provision, while in a relative sense, ignoring the importance of healing relationships in promoting high-quality care (Epstein et al., 2010; Levinson, Lesser, & Epstein, 2010). To address complex problems, patients should not merely be the objects of the team’s attention; patients must be active participants in the team in a meaningful way. In addition to using checklists and protocols (Gawande, 2009), health care teams can also be oriented around promoting mindfulness of and attentiveness to patients’ preferences, as well as deliberativeness in honoring them (Epstein et al., 2010; Epstein, Siegel, & Silberman, 2008; Moulton & Epstein, 2011; Sibinga & Wu, 2010). Hospitals and clinics should provide spaces within which patients’ concerns can actually be heard, rather than having to discuss personal concerns and life-and-death decisions with patients who are separated from their neighbors only by a flimsy curtain in a shared room, amidst the noise of blaring televisions and beeping monitors. Some health systems have implemented financial rewards for clinicians that are based not only on through-put of patients but also on measures of the quality of interpersonal care. Respect for persons and their informed preferences is less likely to occur if doing so means that individual clinicians and health systems suffer economically. Yet it is clear that in some circumstances good communication does take more time; and health systems must be prepared to invest in relationships in the same way they invest in technology.
Perils and Promise
Interactive, relational care can promote greater clarity about preferences and thus enhance autonomy. However, there are potential pitfalls, the greatest of which is self-deception. Clinicians can firmly believe that they are acting in the patient’s best interest, yet have a poor grasp of the patient’s motivations, values, and preferences. Power can create illusions of agreement and suppress open discussion. Clinicians can confuse a patient’s passive assent with true endorsement of a plan of action. Clinicians’ certainty, persuasiveness, and charisma can overwhelm the patient’s voice so that both believe that they share a common frame of reference. Patients can be silenced by anxiety, to which clinicians may inadvertently contribute. Disagreements may manifest in actions (e.g., not taking one’s pills) rather than words (a discussion about why).
While these critiques might lead some patients and families to reject partnerships with health professionals, the alternative—militant individualism—can backfire by leading to mindless enactment of uninformed preferences and leaving patients feeling abandoned and alone. A three-pronged approach, involving clinicians, patients, and health systems, that is focused on mindfulness, activation, and healing relationships, has potential to help. For clinicians, practice incentives, restructured health care teams, and medical education can promote greater mindfulness, teamwork, and patient centeredness. For patients and families, coaching and information technology can help ensure that their voices are heard, that they genuinely and meaningfully share in deliberation and decisions, and ultimately that they achieve greater autonomy and self-determination in setting the course of their own or their family member’s health care. For health care systems, focus on human interactions—not just clinical transactions—will direct the clinician’s gaze to what really matters to patients and their families.
Footnotes
Acknowledgements
The authors thank Richard L. Street Jr., PhD, Vikki Entwistle, PhD, and an anonymous reviewer for their thoughtful comments on the article.
Authors’ Note
The Eisenberg Conference Series 2011 Meeting on Differing Levels of Clinical Evidence: Exploring Communication Challenges in Shared Decision Making was conducted by the John M. Eisenberg Center for Clinical Decisions and Communications Science at Baylor College of Medicine, Houston, Texas, under contract to the Agency for Healthcare Research and Quality, Rockville, MD (Contract No. HHSA290200810015C). The authors of this article are responsible for its content. No statement may be construed as the official position of the Agency for Healthcare Research and Quality of the U.S. Department of Health and Human Services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A stipend covering a portion of the lead author’s work on this article was provided by the John M. Eisenberg Center for Clinical Decisions and Communications Science at Baylor College of Medicine with funding support from the Agency for Healthcare Research and Quality under Contract No. HHSA290200810015C, Rockville, MD.