
Abstract
This article is an investigation into the relationship between length of stay and readmission within 30 days of discharge from an acute care hospitalization. We estimated probability models for heart attack and for heart failure patients using generalized estimating techniques applied to hospital administrative data from California for calendar year 2008. The key independent variable was length of stay in the initial hospitalization. We found negative associations between length of stay and readmission probability, particularly in the case of heart attack. Simulated values of predicted readmissions based on a 1-day increase in length of stay yielded estimated reductions in readmission rates in the 7% to 18% range for heart attack patients and the 1% to 8% range for heart failure patients. Increasing length of stay for some patients may be a means of improving quality of care by reducing readmission during the 30-day postdischarge period.
Introduction
Hospital readmission rates often are used as indicators of quality of care. When patients are readmitted shortly after discharge, it may be due to low quality of care received during the initial hospital stay (Epstein, 2009; Keenan, Normand, & Zin, 2008; Medicare Payment Advisory Commission [MedPAC], 2007), fragmented discharge planning, or inappropriate assessment of readiness for discharge (Phillips et al., 2004). Over the past several years, the leading U.S. quality improvement organizations have expressed major interest in fostering reductions in readmission rates, and concern over readmissions has been a focus of MedPAC. More significantly for hospitals, readmission reduction is an important provision for large scale cost saving under the Patient Protection and Affordable Care Act (PPACA). As of fiscal year 2013, hospitals with “excessive” 30-day readmissions for certain conditions will incur financial penalties under the Medicare reimbursement system, with additional conditions potentially targeted for financial penalty in 2015 (PPACA, Section 3025, 2010). Moreover, the Bundled Payments for Care Improvement Initiative, currently being launched by the PPACA-established Center for Medicare & Medicaid Innovation, aligns payments across episodes of care. Under a bundled payments model, hospitals would receive a single payment for an entire episode of treatment that includes the initial admission and the readmission (Cutler, 2010), placing further pressure on hospitals to reduce readmissions.
Previous studies have contributed to a partial understanding of what modifiable factors are associated with the likelihood of readmission. These include prevention of adverse events during the initial admission (Bernard & Encinosa, 2004; Encinosa & Hellinger, 2005; Rosen, 2008), more careful review of medications at discharge (Coleman, Smith, Raha, & Min, 2005), and improved communication with patients about self-care following discharge (Coleman, Parry, Chalmers, & Lin, 2006; Kind, Smith, Frytak, & Finch, 2007; Naylor et al., 1999), among others (MedPAC, 2007). However, one explanation for high readmission rates that largely is absent from this literature is suboptimal length of stay following the initial admission (referred to as the index hospitalization). If in response to financial incentives of payers or providers, patients are discharged too soon, then as a result of their premature discharge, many patients may need to return to the hospital for additional inpatient care within a short period of time.
The predictors of readmission, reviewed elsewhere (Kansagara et al., 2011), generally have not explicitly examined length of stay of the index hospitalization. However, some population- and hospital-based studies of outcomes following implementation of Medicare’s Prospective Payment System, which resulted in sudden drops in hospital lengths of stay, suggested that such a linkage exists (Desharnais, Hogan, McMahon, & Fleming, 1991; Leibson, Naessens, Campion, Krishan, & Ballard, 1991). Still, the few patient-level studies that included length of stay have failed to find an inverse association. Krumholtz et al. (1997) analyzed Medicare patients treated for congestive heart failure in Connecticut from 1991 to 1994 and found higher within 6-month readmission rates for patients with index hospitalizations of greater than 7 days. Philbin and DiSalvo (1999) found no difference in index hospitalization length of stay between heart failure patients admitted to New York hospitals during 1995 who were readmitted before the end of that year and those who were not readmitted. A positive relationship between length of stay and 30-day readmission was found for 4,812 medical and surgical patients treated in 11 hospitals in Ontario (van Walraven et al., 2010). A study of general medical patients treated in six U.S. academic centers also showed a positive association between lengths of stay of greater than 2 days and 30-day readmissions (Hasan et al., 2010).
While patient-level evidence that longer stays reduce readmission has not appeared in the literature, some recent studies suggest that this may be the case. MedPAC recognized that reduction in length of stay is one aspect of hospitals’ practice patterns that influences the likelihood of patients being readmitted and recommended that “hospitals might consider keeping some patients an extra day to be more certain that their condition has stabilized” (MedPAC, 2007). In addition, the most recent comprehensive analysis of U.S. readmission rates found that rates had risen over time, with speculation that one explanation was the time trend toward shorter duration of index hospitalizations that was occurring over the same period (late 1970s to 2004; Jencks, Williams, & Coleman, 2009). Moreover, a recent international comparison of readmission rates for heart attack patients for whom the coronary artery was completely blocked found higher readmission rates in the United States, a difference that was attenuated after controlling for length of stay (Kociol et al., 2012). Finally, an observational study of 14-year (1993-2006) trends in outcomes for Medicare heart failure patients noted with interest the increase in 30-day readmissions that was occurring as length of stay was declining over this period (Bueno et al., 2010). However, these discussions are speculative and ignore possible simultaneous changes in acuity among patients.
New Contribution
This study is a retrospective examination of the association between length of stay in an index hospitalization and readmission within 7 days and within 30 days of discharge. It is the first study of U.S. hospital readmissions of which we are aware that explicitly focuses on index hospitalization length of stay. Previous studies are either dated or limited to a small number of hospitals. This study also is distinctive in examining this issue in the context of PPACA, under which hospitals recently have begun receiving Medicare reimbursement penalties for “excessive” 30-day readmissions for certain high-volume high-cost conditions. The implications for providers and for policy makers are significant as the Centers for Medicare and Medicaid Services currently is considering broadening the range of conditions subject to penalty.
Method
Data and Setting
We studied adult patients admitted to acute care hospitals in California during calendar year 2008, who were treated for heart attack or heart failure, and were discharged alive. We chose these two conditions because MedPAC recently identified them as the medical conditions having the highest Medicare readmission rates (MedPAC, 2007), and because these conditions currently are being penalized under Medicare for excessive readmissions. Patients were identified by the Medicare Severity (adjusted) Diagnosis Related Group (MS-DRG) classifications: 280-282 (heart attack) and 291-293 (heart failure and shock). We excluded patients who were admitted within 30 days of a prior admission (i.e., a hospitalization could not be both an index hospitalization and a readmission). If a hospitalization began on the same date as discharge from an index hospitalization, it was considered a readmission only if the source of admission for the rehospitalization was not “transfer.” Finally, we excluded patients whose length of stay was greater than 25 days, which are generally considered to be long-term stays (Kahn, Werner, Carson, & Iwashyna, 2012; MedPAC, 2004).
The primary sources of data were the State Inpatient Databases (SID) and the Supplemental Files for Revisit Analyses (Revisit Files) that are compiled by the Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project. The SID contains standard hospital discharge data. In compliance with Health Insurance Portability and Accountability Act privacy rules, the SID files do not indicate exact dates of admission or discharge. However, we were able to identify readmissions as well as the actual number of days to readmission using the Revisit Files. The Healthcare Cost and Utilization Project data were supplemented with the 2008 American Hospital Association Survey.
Analytic Technique
For each of the two conditions of interest, we performed two sets of probability regressions, one for 7-day readmissions and one for 30-day readmissions. The dependent variable was a binary variable for whether the patient was readmitted to an acute care hospital within 7 or within 30 days postdischarge, respectively. The 30-day window is the most common period of analysis in studies of readmission and will pick up a relatively high number of readmissions; however, the 7-day window is more likely to be related to the index hospitalization and the discharge process. Each set of regressions was estimated on all patients in the respective sample and on subgroups of patients for whom longer lengths of stay might be expected to be realized (Carey, 2002). We included two subgroups to test the sensitivity of results across groups: patients whose index hospitalization was less than 10 days and those with stays of less than 7 days.
We recognize that many readmissions will occur for reasons that are unrelated to the index hospitalization. Others will be indirectly related in the sense that the index hospitalization itself compromises the health of the patient who, for example, has been exposed to infection or has experienced lack of sleep. While it is not possible to identify these relationships empirically, we reduced confounding by indicating readmission only if the rehospitalization occurred in Major Diagnostic Category 5 (circulatory system). Among those, we included readmissions for all causes because it is not possible from administrative data to identify which specific readmissions were preventable and which were not. We also performed sensitivity analyses by estimating all models such that readmission to any MDC was defined as a readmission.
The key independent variable was the natural logarithm of length of stay for the index hospitalization measured in number of days (LNLOS). Predisposing variables included five age categories, gender, and race. Health maintenance organization (HMO) insurance status was included as a binary variable; this tests the hypothesis that patients enrolled in managed care organizations have lower probability of readmissions, possibly due to better postdischarge maintenance. We also incorporated a binary variable to control for patient access to an urban location, since accessibility to a hospital might increase the probability that a patient would return there. This was constructed using the rural–urban commuting area codes that are based on population size and commuting information collected by the Bureau of the Census. Clinical control variables are very important in this research design to identify a valid length of stay effect. We included two measures. The first was patient severity in the index hospitalization as categorized in the MS-DRG classification system as high severity (with major complications/comorbidities), medium severity (with complications/comorbidities), and low severity (with no complications/comorbidities). The second was the number of chronic conditions. These are identified in the SID according to whether the diagnosis codes for the hospitalization fall into the chronic or nonchronic category. Finally, at the hospital level, we included a measure of the hospital occupancy rate. Wennberg and colleagues at Dartmouth have found that the local bed supply is a significant factor in explaining hospital utilization (Fisher et al., 2000). The occupancy rate variable tests the theory here with regard to readmissions.
We specified linear probability models on LNLOS. This specification allows the magnitude of the effect of length of stay on readmission probability to decline with length of stay. We estimated the probability models using the generalized estimating equations (GEE) technique with robust standard errors accounting for correlation occurring within observations on the same hospital (Liang & Zeger, 1986; PROC GENMOD; SAS v9.1).
Results
For heart attack patients, the overall sample contains 19,811 observations with 18,711 and 17,420 in the subsamples of patients with index hospitalizations of 10 and of 7 or fewer days. For heart failure, the samples contain 47,563, 45,369, and 42,086 observations, respectively.
Descriptive statistics for the full samples and the smaller of the two subgroups are listed in Table 1. For the overall samples, 16.0% of heart attack patients were readmitted within 30 days and 8.8% were readmitted within 7 days. Heart failure readmission rates were considerably smaller, averaging 12.0% and 4.1% for 30-day and 7-day readmissions, respectively. Length of stay was similar for both conditions on average, 4.04 days for heart attack and 4.18 days for heart failure. The largest age group was between 70 and 84 years of age, accounting for approximately 37% of heart attack patients and 39% of heart failure patients. There were more males than females among heart attack patients, and slightly more female than male heart failure patients. Blacks accounted for approximately 8% of heart attack and 15% of heart failure patients. HMO insurance status was more prevalent among heart attack patients, accounting for 41% compared with 30% of heart failure patients. The two conditions were similar in other respects. For the subsamples, length of stay is approximately 1 day smaller for both conditions; readmissions are slightly higher in the heart attack subsample than in the overall sample. As expected, there was a smaller percentage of patients in the high severity class in the subsamples. Otherwise, the subsamples did not differ notably from the overall samples.
Means and Standard Deviations (in Parentheses) of Variables Used in Regression Analyses.
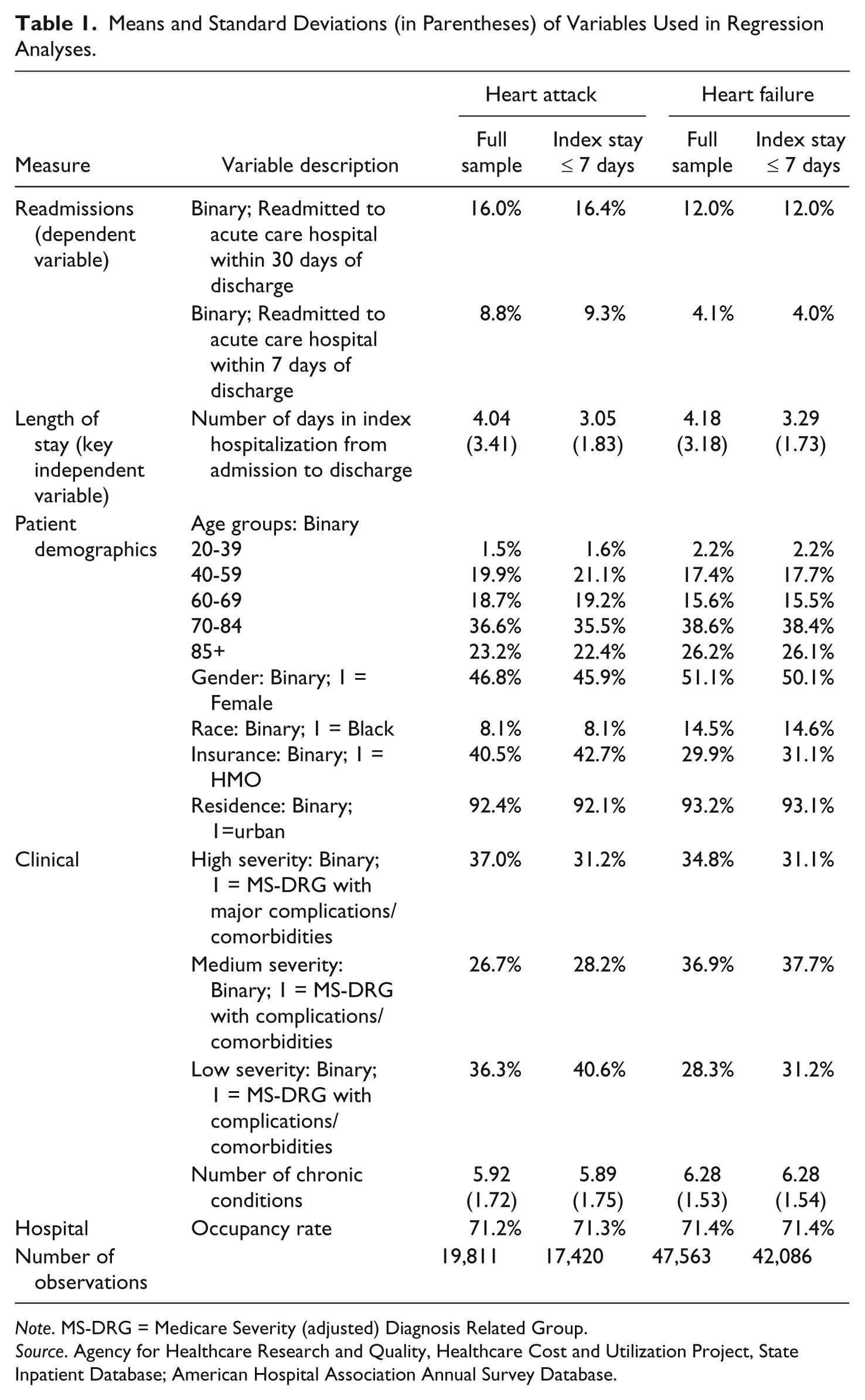
Note. MS-DRG = Medicare Severity (adjusted) Diagnosis Related Group.
Source. Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Database; American Hospital Association Annual Survey Database.
GEE regression results for heart attack are displayed in Table 2 for the overall sample and smaller subsample. The coefficients on LNLOS are negative and significant. The interpretation is that longer LOS is associated with a lower probability of readmission within 30 days or within 7 days. This is true in all four cases. The probability of 30-day readmission generally increases with age group up to age 84, but not the probability of 7-day readmission. Women are less likely to be readmitted; Black patients are less likely in the full sample. The HMO coefficient is also negative and significant in the 30-day readmission cases, suggesting that managed care organizations may be better at coordinating care of their enrollees in the 30-day postdischarge period. Interestingly, the coefficients on higher severity are not significantly different from zero, and for medium severity are negatively associated with 7-day readmissions. The number of chronic conditions, however, is positively associated and highly significant in all cases. Finally, the coefficient on occupancy rate is consistently negative and significant, lending support to the hypothesis that bed supply is a factor in explaining utilization.
Generalized Estimating Equation Results for Probability of Readmission: Heart Attack Patients.
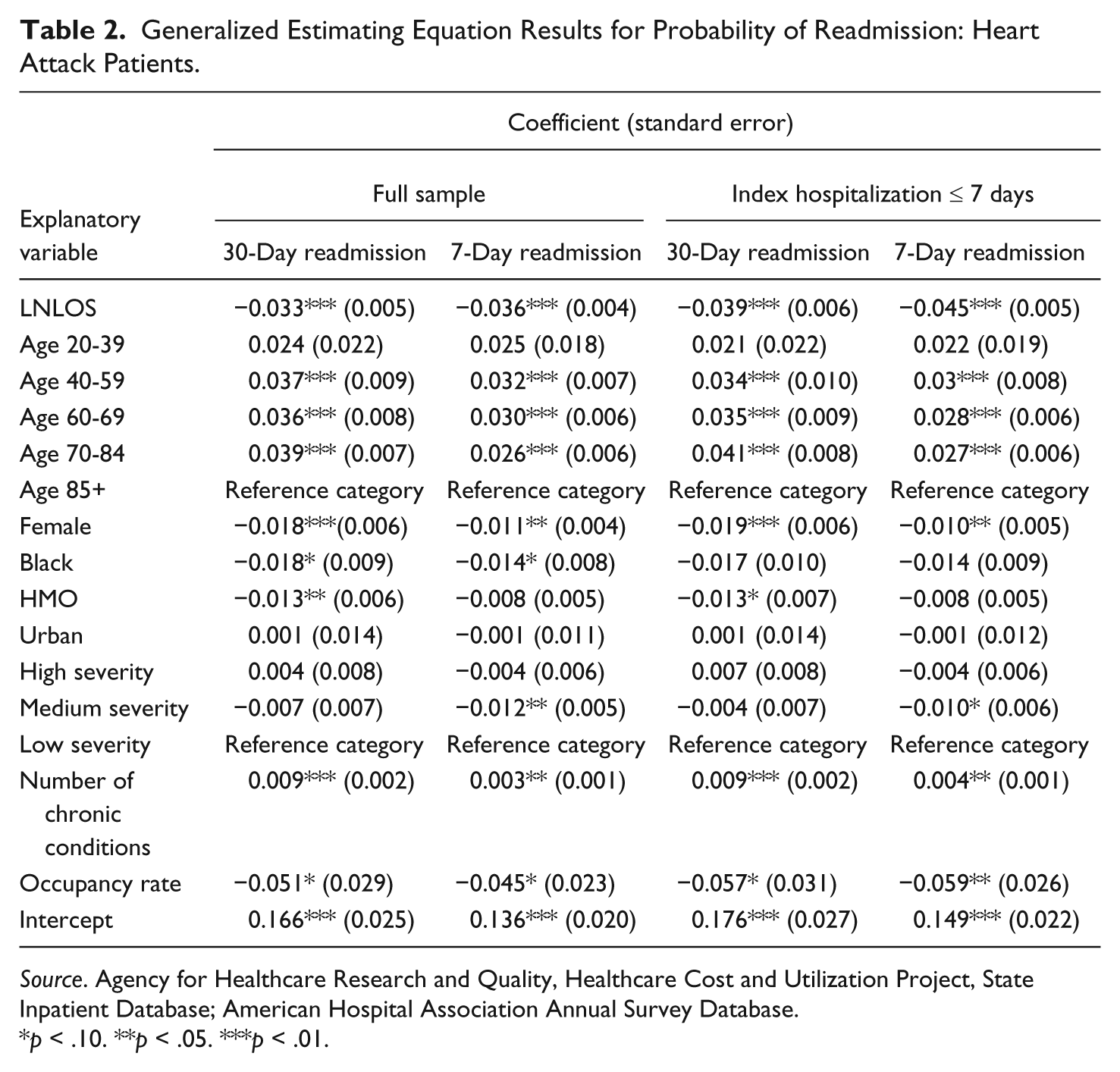
Source. Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Database; American Hospital Association Annual Survey Database.
p < .10. **p < .05. ***p < .01.
Table 3 presents the GEE regression results for heart failure patients. As with heart attack, the coefficient on LNLOS is consistently negative and statistically significant. Men are more likely than women to be readmitted within 30 days, but are no more likely to be readmitted than women within 7 days. Like men, Black patients are more likely to be readmitted within 30 days than other patients. As with heart attack patients, HMOs appear to be better at patient management and reducing the likelihood of readmission within 30 days, yet readmission probability within the 7-day window was no different for HMO patients. Patients with better access to an urban location were more likely to be readmitted within 30 days. Number of chronic conditions was consistently associated with readmission probability, but severity level was consistently not associated. Finally, occupancy rate did not appear to be a factor in explaining readmission for heart failure patients.
Generalized Estimating Equation Results for Probability of Readmission: Heart Failure Patients.
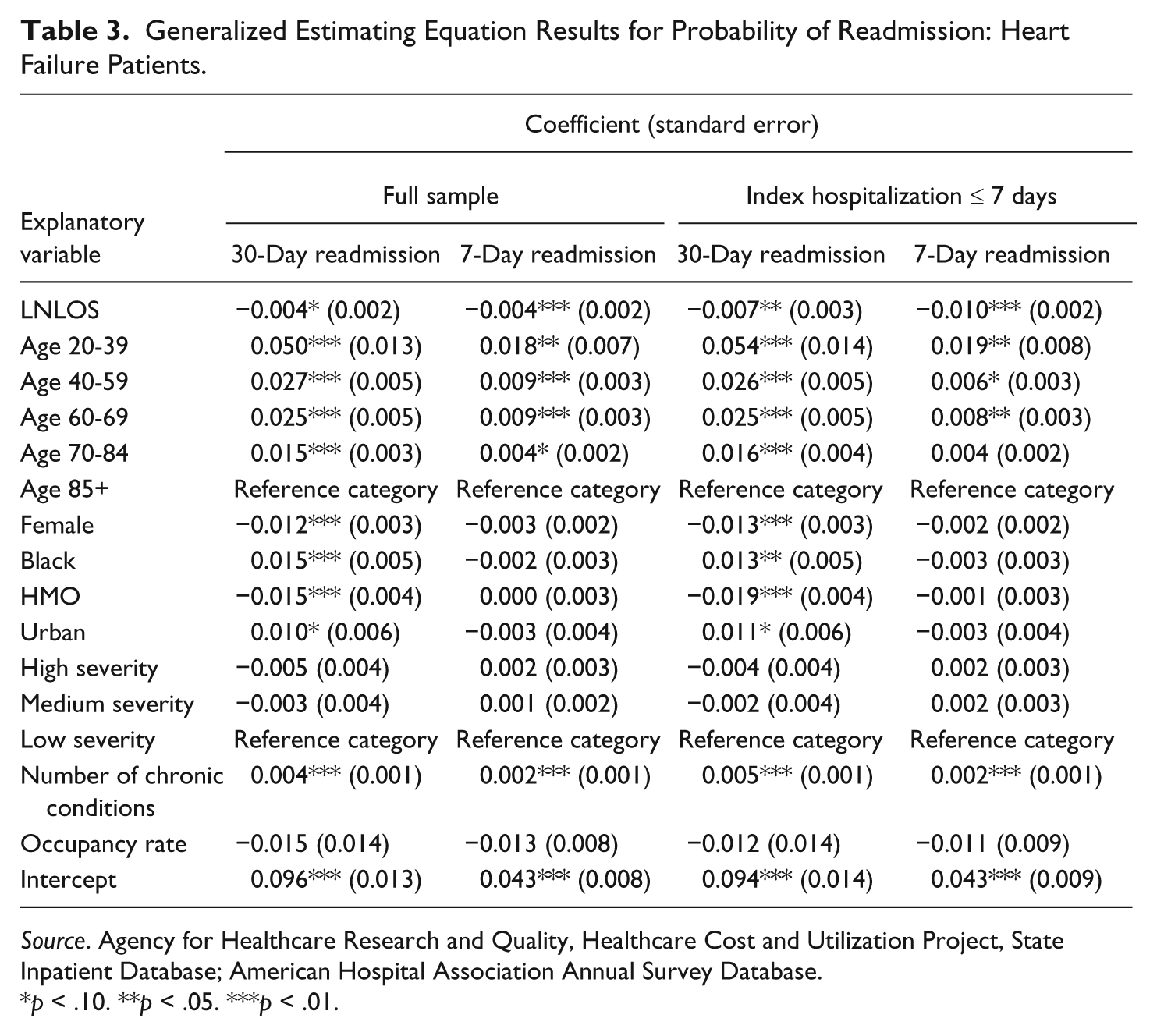
Source. Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Database; American Hospital Association Annual Survey Database.
p < .10. **p < .05. ***p < .01.
The coefficients on the key independent variable are not readily intuitive in themselves. However, the coefficients can be used to calculate marginal probabilities associated with a change in length of stay. To that end, we determined marginal probabilities for readmission by addressing the following question: How does the probability of readmission change if length of stay is increased by one day? To answer the question, we calculated the probability of readmission for each observation given individual patient and hospital characteristics, recalculated the probabilities after increasing the values of length of stay by one, and subtracted the latter probabilities from the former to obtain the marginal probabilities.
Table 4 displays the mean values of predicted probability and of marginal probability expressed as a change in percentage points and as a percentage of predicted probability, for all three samples. For heart attack, these range from 1.1 percentage points for 30-day readmissions based on the full sample results, to 1.16 percentage points for 7-day readmissions for the subsample of patients with index hospitalization of 7 or fewer days. As a percentage of readmission probabilities, these translate into a 6.5% reduction in the predicted values of readmission probability in the former case and a 17.9% reduction in the latter. For heart failure, the magnitudes were small; the respective marginal probabilities were 0.1 and 0.3 percentage points, translating into a range of 0.9% to 7.9% reductions in predicted readmission probabilities. For comparison, the results of estimations in which readmissions to any MDCs were considered. These are reported for cases in which there was a negative and significant association between LNLOS and readmission probability in Table 5. Since 72.3% of readmissions for heart attack were to MDC05, these results are not dramatically different from those in the restricted models. However, the magnitudes of the results are attenuated in all cases. Only 57.1% of heart failure readmissions were to MDC05. For these models, the association is either absent or very small. The contrast between Tables 4 and 5 imply that it is the circulatory readmissions that are possibly preventable with longer lengths of stay for some heart attack and heart failure patients.
Simulation Results: Readmissions Restricted to Same MDC as Index Hospitalization a .
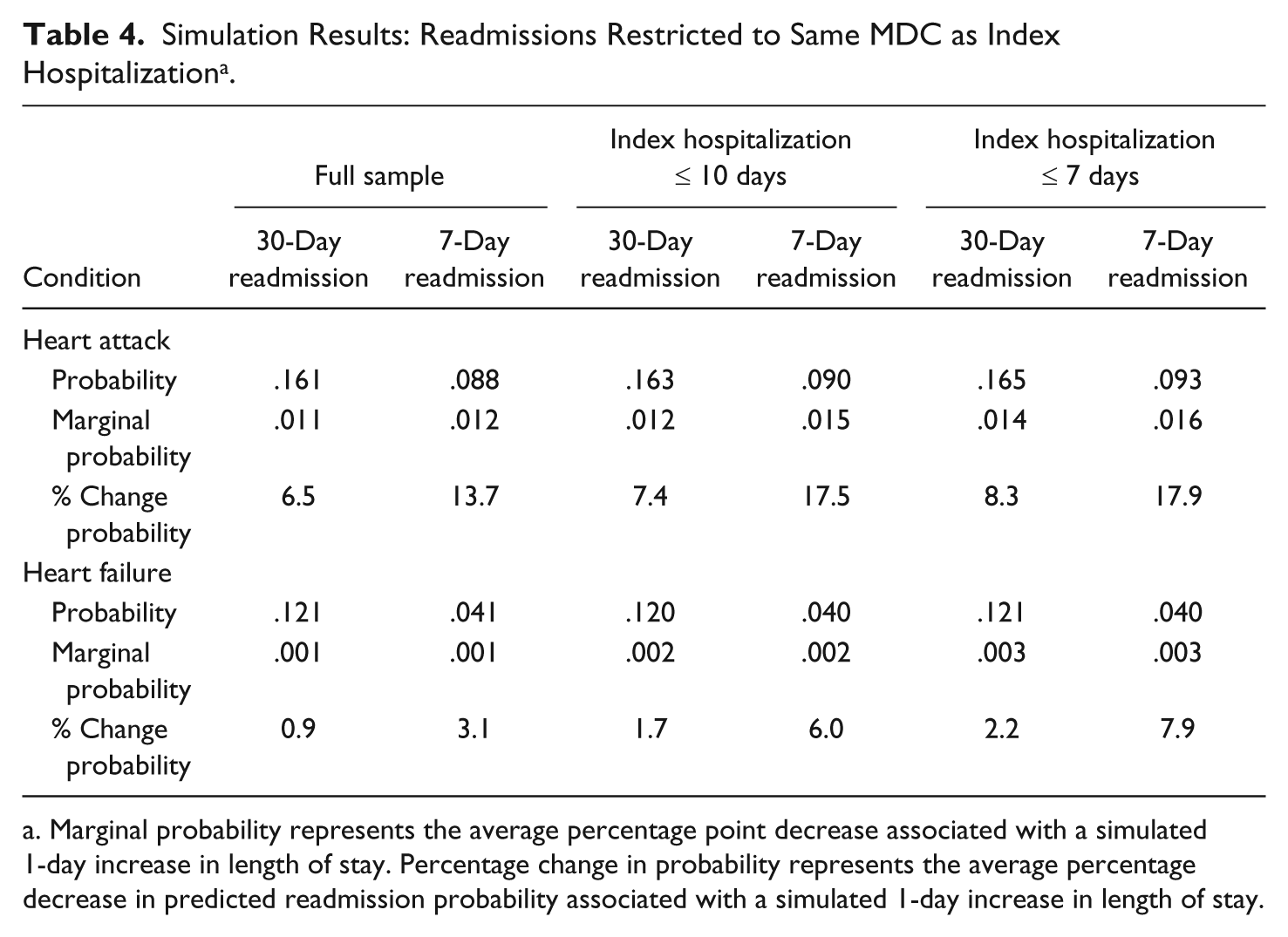
Marginal probability represents the average percentage point decrease associated with a simulated 1-day increase in length of stay. Percentage change in probability represents the average percentage decrease in predicted readmission probability associated with a simulated 1-day increase in length of stay.
Simulation Results: All Readmissions a .
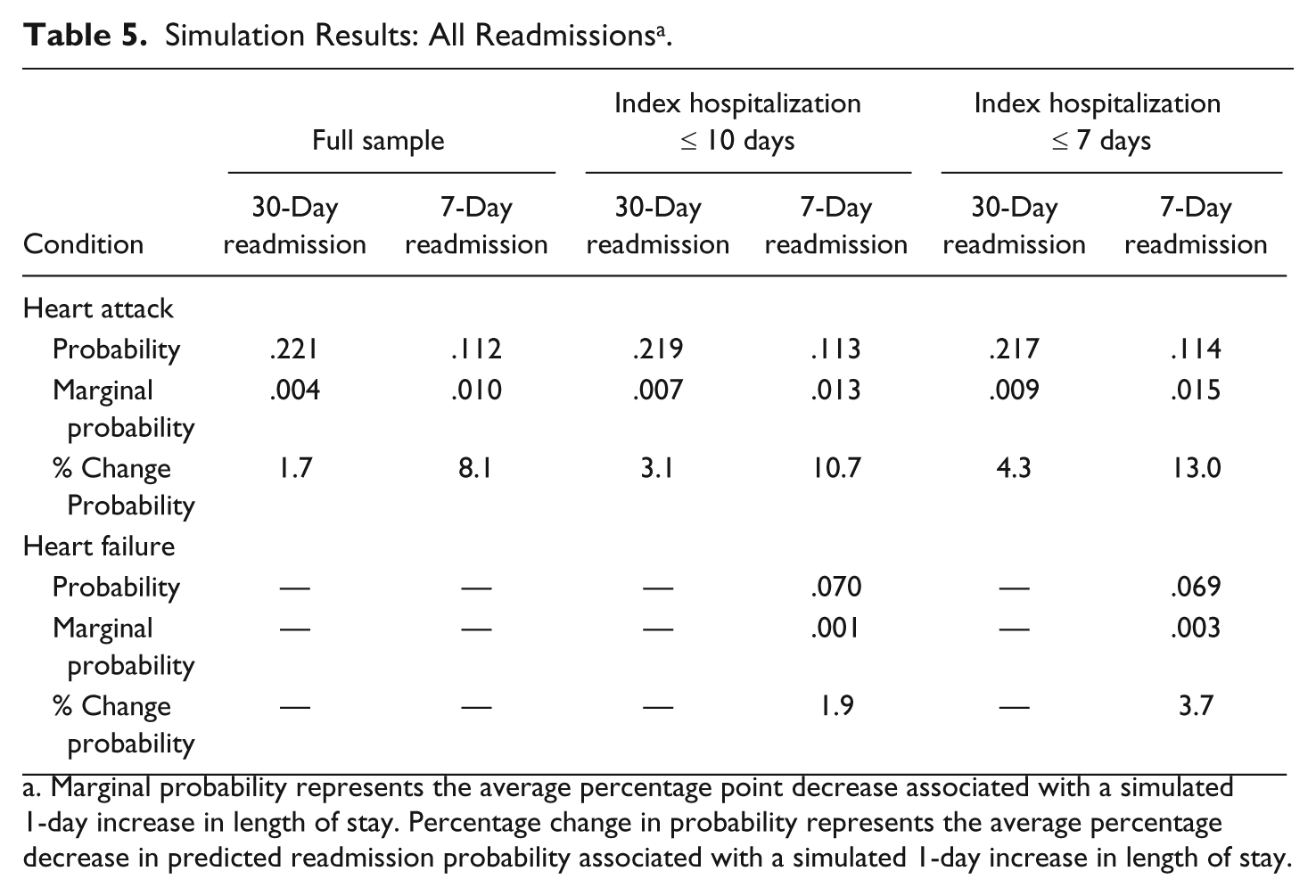
Marginal probability represents the average percentage point decrease associated with a simulated 1-day increase in length of stay. Percentage change in probability represents the average percentage decrease in predicted readmission probability associated with a simulated 1-day increase in length of stay.
Discussion
We investigated the relationship between patient length of stay and likelihood of readmission within 7 days and within 30 days of discharge by estimating patient-level models on samples of patients with an index hospitalization for heart attack or for heart failure. These medical conditions have both relatively high incidences and high rates of readmission, and also recently have been targeted by the Centers for Medicare and Medicaid Services for reimbursement penalties related to readmission rates.
We found negative associations between length of stay and readmission probability, particularly for heart attack patients. The magnitude of the effect was modest for heart attack; reductions in readmission rates following simulated increases in length of stay of 1 day ranged from 7% to 18%. For heart failure, the magnitude of the effect was very small, in the range of 1% to 8%. We also found evidence that HMOs may be better at patient management in the 30-day period following discharge, possibly resulting in fewer readmissions.
This study is an initial attempt at forging a link between hospital lengths of stay and readmissions, and it is subject to limitations. As is typical, the discharge data, while relatively complete and precise in measuring readmission and length of stay, contained only broad measures of severity of condition, and included no information on quality of the discharge planning process or the amount of follow-up care administered during the postdischarge period. Moreover, this is an observational study, such that the effect of length of stay on readmission is subject to parameter estimate bias to the extent of correlation between length of stay and omitted variables that also are significantly associated with readmissions. In particular, unmeasured patient severity could be positively correlated with both length of stay and readmission in our models. However, we maintain that this would lead to a conservative bias. Since length of stay is negatively associated with readmission, if we had been able to include better clinical controls, we expect that the association between length of stay and readmission would have been stronger than what we found. No method can completely identify causality from observational data, and the associations between length of stay and readmissions uncovered here need to be interpreted in that respect.
While PPACA takes a major step toward improving access to health care services in the United States, in doing so it heightens the critical challenge of improving on value for money achieved throughout the delivery system. An important provision for large-scale cost saving under the new law is reduction of hospital readmissions. As of October 2012, hospitals with “excessive” 30-day readmissions for certain high-volume/high-cost conditions (heart attack, heart failure, and pneumonia) began incurring financial penalties under the Medicare reimbursement system. Additional conditions will potentially be targeted for financial penalty beginning in 2015. This provision of the law creates powerful incentives for hospitals to identify ways of preventing readmissions in a manner that will not compromise quality of care. This article is an early investigation of the role of shorter lengths of stay in driving readmission rates. Optimal length of stay at the patient level is complicated by many clinical factors. However, the results achieved here suggest that longer length of stay for some patients might be considered as one factor in achieving the goal of readmission reduction.
While the scope of our results is modest, they support recent literature that suggests a link between shorter lengths of stay and readmission probability, and suggest that further study is important. Length of stay has cost consequences per se, but should it be linked to the likelihood of readmission, its cost implications become much more complicated. For some patients, assuming that the marginal cost of a day in the index hospitalization declines with each additional day, it is possible that an extra day of stay could reduce costs over the total episode if a readmission was avoided. At the current policy juncture, indentifying and understanding new opportunities for cost savings that can preserve quality of care delivery is critical to the success of health care reform.
Footnotes
Acknowledgements
The authors thank Cindy L. Christiansen for helpful comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Agency for Healthcare Research and Quality (#R03 HS020995-01), Kathleen Carey, Principal Investigator.