
Abstract
Although the importance of safety regulations is highly emphasized in hospitals, nurses frequently work around, or intentionally bypass, safety regulations. We argue that work-arounds occur because adhering to safety regulations usually requires more time and work process design often lacks complementarity with safety regulations. Our main proposition is that mindfulness is associated with a decrease in occupational safety failures through a decrease in work-arounds. First, we propose that individual mindfulness may prevent the depletion of motivational resources caused by worrying about the consequences of time lost when adhering to safety regulations. Second, we argue that collective mindfulness may provide nursing teams with a cognitive infrastructure that facilitates the detection and adaptation of work processes. The results of a multilevel analysis of 580 survey responses from nurses are consistent with our propositions. Our multilevel analytic approach enables us to account for the unique variance in work-arounds that individual and collective mindfulness explain.
Background
Occupational safety is a prominent issue in the management of organizations; indeed managers in 118 countries contend that occupational safety is the number one social issue that needs to be addressed (Kiron, Kruschwitz, Rubel, Reeves, & Fuisz-Kehrbach, 2013). Although occupational safety is a costly and pervasive problem in many organizations (Zohar, 2010), the prevalence of occupational safety failures in hospitals is particularly striking. Nurses, for instance, are 30 times more likely to experience an occupational injury than workers in other industries (Lucian Leape Institute, 2013). A survey of nurses in the United States revealed that almost one third had experienced back or musculoskeletal injuries in the past year, and 13% reported unprotected contact with blood-borne pathogens (Ulrich, Buerhaus, Donelan, Norman, & Dittus, 2005). Frequently cited reasons for these alarming statistics include a turbulent work environment, the increasing demands of the job, the complex and dynamic problems that nurses face, and the need for continuous adaptation and learning (Katz-Navon, Naveh, & Stern, 2005; Lucian Leape Institute, 2013).
In response to this prevalence of occupational injuries and inspired by the belief that organizational reliability can be achieved through standardization and routines (Hannan & Freeman, 1984), hospitals and both national and international organizations have enacted safety regulations for all types of actions (Brunsson & Jacobsson, 2000). Previous research, however, has documented that nurses often work around these safety regulations. Some authors go as far as characterizing nurses as “masters of work-arounds,” recognizing that work-arounds are a common practice in health care contexts (Morath & Turnbull, 2005). Consider, for example, nurses who attempt to lift a patient on their own despite the safety regulations that call for either assembling additional nurses to assist or using assistive equipment (e.g., a ceiling mounted or portable lift). Such safety work-arounds, defined as the intentional bypassing of existing safety regulations (Halbesleben, Wakefield, & Wakefield, 2008), are strong predictors of the frequency and severity of occupational injuries in hospitals (Halbesleben, 2010; Halbesleben & Rathert, 2008; Halbesleben, Savage, Wakefield, & Wakefield, 2010). Notably, a single safety work-around may or may not lead to an occupational injury; nevertheless, consistent engagement in safety work-arounds does increase one’s risk of experiencing an occupational injury (Halbesleben et al., 2008).
Hospitals strive for high levels of reliability in a context where even a small safety failure can have detrimental consequences, making increasing occupational safety a major concern. Prior research shows that safety-related behaviors are driven by individual-level variables, such as personality characteristics and job attitudes, and team-level antecedents, such as safety climate and leadership (Christian, Bradley, Wallace, & Burke, 2009). Despite the fact that the interest in organizational and managerial cognition has increased in the past two decades, the literature on occupational safety has largely ignored the role of cognition. Because several scholars have suggested that team and individual cognition is key to assuring high performance in uncertain and complex environments such as hospitals, it is important to examine whether and how cognition-related constructs influence occupational safety in hospitals (Walsh, 1995; Weick, Sutcliffe, & Obstfeld, 1999).
Recently, mindfulness has been proposed as a promising cognition-related construct for predicting job performance (Dane & Brummel, 2013) and work-related errors (Dane, 2011, 2013). A central aim of this article is thus to provide an empirical account of the role of mindfulness in affecting occupational safety in hospitals. Specifically, this study applies both individual and collective mindfulness as cognitive antecedents to occupational safety. This multilevel perspective allows us to account for the fact that both individual-level and team-level antecedents can drive occupational safety failures. We posit that mindfulness will decrease the occurrence of work-arounds and, as such, increase occupational safety in hospitals. Unraveling the relationship between mindfulness and occupational safety is important as some evidence suggests that the degree of team and individual mindfulness can be increased through implementing particular HR practices (Vogus & Welbourne, 2003) and through mindfulness training (Brown & Ryan, 2003; Chambers, Lo, & Allen, 2008). However, despite these studies, presently there is a lack of empirical evidence supporting the efficacy of collective and individual mindfulness to improve safety outcomes in hospitals making it difficult for hospital managers to make well-informed decisions about whether to implement mindfulness-inducing HR practices and mindfulness training.
New Contributions
Using multilevel modeling to separate between-subject effects (i.e., individual mindfulness) and between-group effects (i.e., collective mindfulness) as distinct sources of variance in work-arounds, we tested our hypotheses on survey responses from 580 nurses (across 54 teams) to make two main contributions. First, we contribute to the literature on occupational safety by providing empirical evidence for the role of team and individual cognition in understanding occupational safety in hospitals. While previous research has documented that individual-level and team-level constructs are important for understanding occupational safety (Christian et al., 2009), the cognitive processes that influence occupational safety are understudied. By focusing on individual and collective mindfulness as cognition-related constructs, our study addresses this void to highlight the pivotal role of work-arounds in the relationship between mindfulness and occupational safety in hospitals. We found evidence that, while work-arounds make occupational safety failures more likely, both individual and collective mindfulness are associated with lower rates of occupational safety failures through fewer work-arounds. Importantly, we did not find a significant direct effect for individual or collective mindfulness on occupational safety failures. This emphasizes the significance of work-arounds as a lever to better understanding how mindfulness can reduce occupational safety failures.
Second, this study adds to the growing evidence on the benefits of mindfulness in organizations in general and hospitals in particular. Our results are in line with the view that individual and collective mindfulness explain unique variance in work-arounds and occupational safety failures in hospitals. Importantly, collective and individual mindfulness affect occupational safety but in relation to different constraints. Overall, the results of this study suggest that increasing collective and individual mindfulness in hospitals via mindfulness-inducing HR practices and mindfulness training may be worthwhile interventions to improve occupational safety. Our aim is for the study’s insights to have a considerable impact on the management of occupational safety in hospitals.
Conceptual Framework
Individual Mindfulness
Given the high frequency of work-arounds in hospitals, a natural question to ask is how a work environment replete with safety regulations might prompt nurses to work around these regulations. One proposed explanation is that adhering to safety regulations often entails the immediate cost of a slower pace (Naveh, Katz-Navon, & Stern, 2005; Zohar, 2002). The slower pace caused by close adherence to safety regulations increases the time pressure that nurses experience and may induce nurses to start worrying about how they will be able to complete their work on time.
The main consequence of worrying about the future consequences of close adherence to safety regulations is that the nurses’ motivational resources to adhere to the safety regulations may be depleted (Halbesleben & Bowler, 2007). Because a lack of motivational resources is a core predictor of work-arounds (Halbesleben, 2010), it can be argued that the time-consuming characteristic of occupational safety regulations can prompt nurses to work around them. We argue that individual mindfulness will prevent the depletion of motivational resources caused by worrying about the future consequences of adhering to safety regulations, thereby reducing work-arounds and occupational safety failures.
Individual mindfulness has its roots in Buddhist philosophy and can be understood as a state of consciousness in which one’s attention is focused on present-moment internal and external phenomena. Individual mindfulness also manifests itself through an accepting, open, and nonjudgmental attitude toward phenomena that are perceived in the present moment (Brown & Ryan, 2003; Brown, Ryan, & Creswell, 2007; Dane, 2011; Glomb, Duffy, Bono, & Yang, 2011). Like other psychological concepts, individual mindfulness is a trait-level construct as well as a psychological state that varies from moment to moment within individuals (Dane, 2011; Vogus, 2011). Hulsheger, Alberts, Feinholdt, and Lang (2013), for instance, report that 62% of the variance in mindfulness occurs between individuals and 38% within individuals. Contrary to previous research about attention, which has predominantly focused on the direction of attention, mindfulness addresses the quality of attention and emphasizes the richness of the interpretations that are based on perceiving present-moment phenomena (Dane, 2013; Langer & Moldoveanu, 2000; Weick et al., 1999).
Shifting the line of inquiry from the direction of attention to the quality of attention improves our chances of addressing why nurses work around the safety regulations. Specifically, we argue that focusing attention on the present moment and approaching the present moment with an accepting, open, and nonjudgmental attitude will reduce the tendency of nurses to start worrying about the future consequences of adhering to time-consuming occupational safety regulations. Consequently, the depletion of the nurses’ motivational resources is reduced implying that nurses will have more motivational resources available to closely follow the safety regulations. That is, we expect that individual mindfulness will enable nurses to closely adhere to the occupational safety regulations, ultimately resulting in a decrease in work-arounds. Overall, we expect individual mindfulness will be related to fewer occupational safety failures among nurses through a reduction in work-arounds.
Collective Mindfulness
A second explanation for the prevalence of work-arounds is that the design of work processes may conflict with newly developed safety regulations (Edmondson, 2004; Halbesleben et al., 2008). For example, given the high degree of interdependence among hospital departments, the design of work processes in other departments may prevent nurses from adhering to the safety regulations in their own department (Nembhard & Tucker, 2011; Tucker, Heisler, & Janisse, 2014). Working around safety regulations is the dominant response of nurses in such situations, and previous research shows that 10% to 15% of nurses’ work time is lost to managing the lack of complementarity between safety regulations and the design of work processes (Tucker & Edmondson, 2002, 2003; Tucker et al., 2014). We argue that work-arounds, and relatedly, occupational safety failures, may be better understood when they are considered from the perspective of collective mindfulness.
Collective mindfulness, also called mindful organizing, refers to an entirely different construct than individual mindfulness. Collective mindfulness is defined as a team’s capacity to develop a rich awareness of discriminatory details about internal and external processes and to regulate team behaviors accordingly (Vogus, 2011; Vogus & Sutcliffe, 2012; Weick et al., 1999; Weick & Sutcliffe, 2006). Collective mindfulness can be identified through five team processes (Weick & Sutcliffe, 2007): (a) preoccupation with failure in noticing when something goes wrong, (b) reluctance to simplify so that heuristics and “quick fixes” are avoided, (c) sensitivity to operations to prevent automated processes from occurring in unexpected and undesirable ways, (d) commitment to bounce back from failure and inaction, and (e) deference to expertise to ensure that the person with the right qualifications executes the job.
Collective and individual mindfulness share an emphasis on an increased attention to internal and external present-moment phenomena and on approaching the present moment with an accepting, open, and nonjudgmental attitude. Like individual mindfulness, collective mindfulness is as much about what teams do with what they notice as it is about the act of noticing itself (Weick et al., 1999). A notable distinction, however, is that collective mindfulness is a social process that exists only to the extent that it is collectively enacted (Levinthal & Rerup, 2006; Vogus & Sutcliffe, 2007b).
We posit that collective mindfulness will provide the nursing team the cognitive infrastructure that is necessary to develop an increased situational awareness of the work processes, the safety regulations, and how the combination of the two may potentially lack complementarity. Also, the accepting, open, and nonjudgmental attitude that characterizes collectively mindful nursing teams is expected to induce nursing teams to search for structural solutions rather than opting for “quick fixes.” Specifically, collective mindfulness will enable nursing teams to consider a detailed root-cause analysis of the occupational safety failures (or signals that may lead to occupational safety failures) and to come up with structural solutions that incorporate the expertise of every individual team member. Such a pattern of behavior is expected to reduce the number of occupational safety failures through a reduction in work-arounds caused by the lack of complementarity between work-process design and safety regulations.
Method
Participants and Procedure
Data were collected from four general hospitals. The number of beds varied from 217 to 811 and none of the hospitals were university teaching hospitals. We surveyed 580 nurses in 54 nursing departments with different specializations, including surgery, geriatrics, emergency medicine, pediatrics, maternity, psychiatry, revalidation, dental care, oncology, cardiology, gastroenterology, orthopedics, radiography, and polyclinics. We defined a team as a minimum of two nurses operating under the direct supervision of one head nurse (i.e., minimally, as a three-person work group). Participating nursing departments had an average of 11 nurses who provided care for an average of 19 patients. The nurses who participated in the study were, on average, 38 years old (SD = 11), had worked in the hospital for 14 years (SD = 11), and had worked as a nurse for 15 years (SD = 10). On average, nurses worked in the hospital for 33 hours per week (SD = 8). A total of 75% of the nurses were female.
We received permission from the nursing directors in each hospital to conduct our survey and then presented the purpose of the study to the head nurses to stimulate participant recruitment. We did not reveal the hypotheses of our study and we guaranteed confidentiality. Paper surveys were distributed in large envelopes to each nursing department, and nurses were asked to deposit the completed surveys in a locked box placed in the coffee room of each nursing department. Surveys were deposited in sealed envelopes to assure anonymity. We visited the nursing departments 2 weeks after the distribution of the surveys to collect the completed surveys.
Data were collected in the nursing departments in two stages. In Stage 1, we collected 580 surveys from nurses in four hospitals, a response rate of 70%. We used the data from these surveys for our multilevel analyses. In Stage 2, 6 months later, we used the same procedure to collect survey data from the head nurses on the number of occupational safety failures obtaining a 100% response rate. We used the data from these surveys to assess the reliability of the number of occupational safety failures the nurses reported in Stage 1. To avoid survey fatigue, the hospital management did not permit us to distribute the survey to all nurses in Stage 2.
While the use of self-report data has limitations, we found it to be an essential method of reporting the measures we collected. It is very difficult for individuals to accurately report on the extent to which another individual may engage in mindful or work-around behavior, or the extent to which they experience incidents related to occupational safety. Individuals are not likely to widely articulate that they decided to work-around an official safety regulation. Relatedly, it would be difficult for others to ascertain the cause of an individual’s injury, if they noticed it at all. Following this rationale, we found that self-report data were an appropriate means of obtaining the data of interest, particularly individual error.
Measures
Individual Mindfulness
We used the Mindful Attention and Awareness Scale (MAAS) to assess individual mindfulness (Brown & Ryan, 2003). The MAAS measures the absence of attention and awareness in thoughts, emotions, physical sensations, and behaviors. Given our focus on predicting workplace behaviors rather than on individual well-being (Dane, 2011), we chose to include only the behavioral items of the MAAS and asked respondents to what extent these items reflected their work-related experiences. Items were measured on a 6-point Likert-type scale ranging from almost never to nearly always and are thus reverse-scored. The items are (a) “I could break or spill things because of carelessness, not paying attention, or thinking of something else”; (b) “I rush through activities without being really attentive to them”; (c) “I do jobs or tasks automatically, without being aware of what I’m doing”; (d) “It seems I am running on automatic pilot without much awareness of what I’m doing”; and (e) “I find myself doing things without paying attention.” The Cronbach’s alpha value for this measure was .83.
Collective Mindfulness
We used the Safety Organizing Scale to take a safety-specific measure of collective mindfulness (Vogus & Sutcliffe, 2007b). This scale includes nine items measured on a 5-point Likert-type scale ranging from not at all to to a very great extent. Example items include “We spend time identifying activities we do not want to go wrong” and “When errors happen, we discuss how we could have prevented them.” The Cronbach’s alpha value for these items was .92. Because we are interested in team levels of collective mindfulness, we checked whether we could aggregate this measure to the team level of analysis. Supporting the aggregation of this measure (Bliese, 2000), we found an average rwg of .92 (Mdn = .92), an ICC(1) of .26 and an ICC(2) of .80, and a significant amount of between-group variance F(53, 579) = 4.93, p < .01. Please note that, in this study, collective mindfulness is not defined as the aggregate of individual mindfulness at the group level; instead, it refers to distinct group processes and is measured at the group level of analysis. Because we are testing a multilevel model, we separate the between-subject and between-group effects as distinct sources of variance in work-arounds.
Work-Arounds
We used a validated four-item scale to measure work-arounds (Halbesleben, 2010). Example items include “I bypass safety rules in order to get work done” and “I follow safety procedures, even if it causes my work to take longer” (reverse-scored). Items were scored on a 5-point frequency scale from 1 (never) to 5 (everyday). We obtained a Cronbach’s alpha value of .87.
Occupational Safety
We collected occupational safety failures from the nurses by means of a checklist based on the Bureau of Labor Statistics system and of an existing survey from the Centers for Disease Control and Prevention (2004), with some modifications to address the specific injuries health care professionals face in a hospital setting (Halbesleben, 2010; Halbesleben et al., 2013). Items included the frequency with which nurses experienced “allergic skin reactions,” “bruises,” “back pain,” “needle sticks,” and “chemical splashes (bodily fluid)” as a result of their work during the past 6 months. Over 6 months, nurses experienced an average of 8 incidents (SD = 7.00).
A meta-analysis conducted by Beus, Payne, Bergman, and Arthur (2010) indicates that self-reports and cross-sectional data can artificially strengthen the relationship between safety attitudes and safety outcomes. To assess the reliability of our outcome variable, we asked head nurses to report the number of safety failures 6 months after we collected the other measures (Mitchell & James, 2001). The correlation between the number of occupational safety failures reported by the head nurse and the sum of the number of occupational safety failures reported by the members of the nursing team is .40 (p < .05, N = 54 teams). Although this statistic does not substitute for longitudinal data, it gives us some confidence that our outcome measure is reliable. Furthermore, it corroborates our earlier argument that self-reported data may be more accurate for capturing this information since it may be difficult for others to accurately assess another person’s experience related to safety and error reporting. Also note that each theoretical construct in our multilevel analyses requires individual-level data, making it impossible to use the number of occupational safety failures reported by the head nurses in the survey administered in Stage 2.
Control Variables
We controlled for characteristics of the nurses, the nursing teams, and the hospitals to account for nonspecific effects. First, we controlled for characteristics of the nurse such as age, tenure in the hospital, and tenure in the nursing department. Second, we included the average number of patients cared for by the nursing teams, as occupational safety may be a function of nurse workload (Katz-Navon et al., 2005). Third, we measured the average complexity of patient conditions in the work unit using six items (Hofmann & Mark, 2006) to control for the fact that occupational safety may also be a function of more complex patient conditions. An example item from this measure is “How many patients on your unit have complex problems that are not well understood?” These items were measured on a 5-point Likert-type scale ranging from a few (<20%) to most (>80%). Fourth, we controlled for potential differences between the hospitals by controlling for hospital size, which is measured by the total number of beds (Katz-Navon et al., 2005). We derived each nurse’s hospital affiliation from the data collection. We found that adding these controls did not meaningfully change our results. Therefore, following the recommendations of Becker (2005), we omitted these variables from subsequent analyses.
Analyses
We analyzed the data using structural equation modeling in two steps (McDonald & Ho, 2002). First, we conducted a confirmatory factor analysis on our measurement model. The measurement model showed a good fit to the data (Hu & Bentler, 1998, 1999): χ²(168) = 510.82 (p = .00), standardized root mean square residual = .05, root mean square error of approximation = .06, and comparative fit index = .95. When we alternately constrained each pairwise factor to unity, we found that, in each case, constraining the factor correlation significantly worsened the model (p < .05). Because multilevel structural equation models are too parameter intensive for our data, we proceeded with testing the structural relationships using aggregated measures in a multilevel path model (Grizzle, Zablah, Brown, Mowen, & Lee, 2009). The results obtained using the multilevel path model are similar to those obtained through hierarchical linear modeling (Grizzle et al., 2009).
To assess our hypothesized cross-level model, we followed the procedures described by Hofmann (1997) and Hofmann, Griffin, and Gavin (2000) and adopted by Walumbwa, Wang, Weng, Schaubroeck, and Avolio (2010). Specifically, we first tested the main effects in our model. In hierarchical linear modeling terminology, this consists of an intercept-as-outcome model. We established the mediating effects by testing alternative models that specify a direct link between individual mindfulness, collective mindfulness, and occupational safety (James, Mulaik, & Brett, 2006; Preacher, Zyphur, & Zhang, 2011). These alternative models indicate whether a residual direct effect remains after work-arounds are included in the model.
Finally, because the teams in our data set are further nested within organizations, we accounted for nonindependence in our data at the organizational level by including the “type=COMPLEX” command in Mplus. This command corrects standard errors and the chi-square test of model fit for nonindependence of observations (Satorra, 2000).
Results
Table 1 shows the means, standard deviations, and correlation coefficients for the study variables. The correlations are in the direction consistent with our hypotheses. Specifically, the correlation between collective mindfulness and work-arounds and between individual mindfulness and work-arounds are both significantly negative (r = −.30, p < .05, for individual mindfulness; r = −.32, p < .05, for collective mindfulness). The correlation between work-arounds and the number of occupational safety failures is significantly positive (r = .20, p < .05). To assess our hypothesized cross-level model, we first examined the degree of between-group variance for work-arounds and occupational safety failures. Results for a null model showed that 22% of the variance in work-arounds and 25% of the variance in safety failures was between-group variance.
Means, Standard Deviations, and Intercorrelations Among Study Variables.
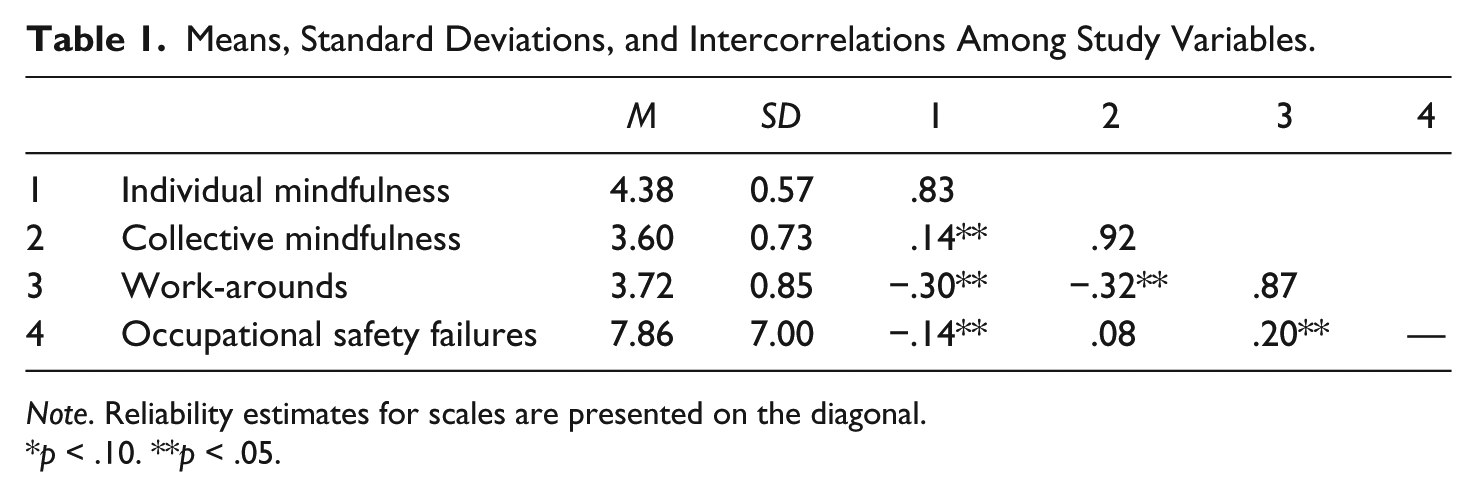
Note. Reliability estimates for scales are presented on the diagonal.
p < .10. **p < .05.
When assessing group-level effects, we applied grand mean centering to partial out variance in individual-level variables (e.g., individual mindfulness; Hofmann & Gavin, 1998). Figure 1 shows the standardized parameter estimates for our hypothesized model. Both individual mindfulness (ŷ = −.27, p < .05) and collective mindfulness (ŷ = −.62, p < .05) were significantly negatively related to safety work-arounds, and safety work-arounds further predicted the number of occupational safety failures (ŷ = .13, p < .05).
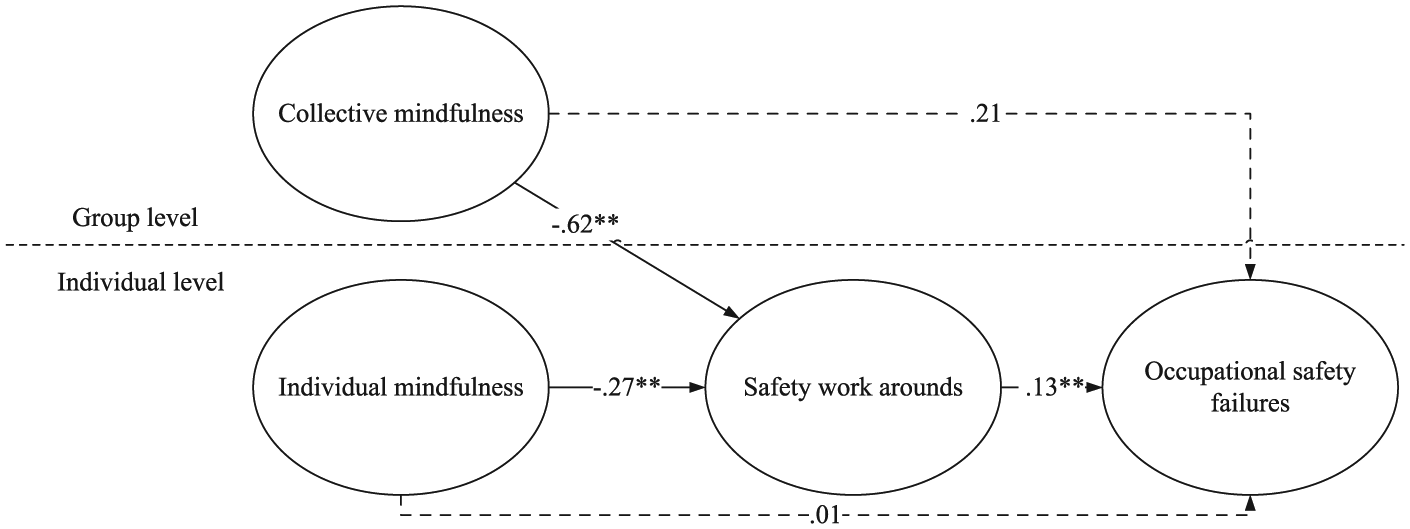
Hypothesized model.
Next, we tested our mediation hypotheses by specifying a direct effect for collective mindfulness (ŷ = −.21, p = .21) and individual mindfulness (ŷ = .01, p = .88) on occupational safety failures. To test the cross-level mediation effect, we followed the recommendations of Zhang, Zyphur, and Preacher (2009), who argued that cross-level mediation effects may be confounded if one looks at between-subject, rather than between-group, effects as mediators. These results confirm that the effects of individual and collective mindfulness operate through safety work-arounds.
Discussion
Individual and team cognition are important in complex and uncertain environments such as hospitals. Indeed, reliability often results from stable processes of cognition that help individuals and teams develop a detailed understanding of the situation (Weick et al., 1999). In this study, we seek to address the lack of research concerning the role of cognition for improving occupational safety in hospitals by examining how individual and collective mindfulness are related to occupational safety in hospitals. Work-arounds, defined as the intentional bypassing of existing safety regulations, have a pivotal role in our theoretical model as we posit that individual and collective mindfulness influence occupational safety through a reduction in work-arounds. We expect individual mindfulness to reduce the depletion of nurses’ motivational resources caused by worrying about the future consequences of adhering to time-consuming safety regulations. As such, nurses have more motivational resources available for adhering to the safety regulations, leading to less work-arounds and more occupational safety.
We posit that collective mindfulness will provide the nursing team with a cognitive infrastructure that enables detailed root cause analyses of occupational safety failures and the development of structural solutions for occupational safety failures. Thus, nursing teams that are more collectively mindful should engage less in working around existing safety regulations, leading to a higher degree of occupational safety. The results of a multilevel analysis of survey responses of 580 nurses support the hypothesized relationships between individual and collective mindfulness, work-around, and occupational safety.
This study contributes to research and practice in two ways. First, by providing empirical support for the positive effects of mindfulness on occupational safety in hospitals, this study contributes to a better understanding of the role of cognition in occupational safety. By using work-arounds to explain the relationship between mindfulness and occupational safety failures, this study also helps clarify the underlying mechanism that drives the effect of mindfulness. While the pioneering work of Vogus and Sutcliffe (2007a) has already documented that collective mindfulness reduces medication errors, it does not address the unique underlying processes through which collective mindfulness influences safety outcomes. As documenting these underlying mechanisms is a next step toward better understanding the effects of mindfulness, our study advances knowledge about the role of mindfulness in the workplace and has the potential to change the way in which occupational safety is managed in hospitals.
Second, to our knowledge, this study is the first to consider individual and collective mindfulness simultaneously and to investigate the unique variance accounted for by each construct in predicting work-arounds and occupational safety. Although some researchers have advocated for viewing occupational safety as a function of individual-level and team-level antecedents, studies that focus on both are scarce (Christian et al., 2009). Our study fills this gap and provides an empirical toolkit that should stimulate further research in this area.
Managerial Implications
This study provides guidance on how hospital managers can improve occupational safety. We believe that such guidance is important as occupational safety plays a pivotal role in the efficient and effective functioning of hospitals. For example, hospitals often develop performance indicators related to occupational safety and use them for the evaluation of nurse managers because nursing turnover and/or exit from the profession are clear outcomes if occupational safety is ignored or downplayed. In other words, the immense costs of recruiting and training new nurses can be obviated, at least in part, by improving nurses’ occupational safety. Also, a lack of occupational safety often results in negative media attention and reputational damage for the health care organization.
We believe that our results suggest two implications for hospital managers. First, hospital managers should consider emphasizing mindfulness when designing policies for improving occupational safety. A natural response to occupational safety failures is to implement new safety regulations (Hannan & Freeman, 1984). Although safety regulations are necessary to ensure reliability, the effectiveness of these safety regulations is reduced when employees work around them. This study shows that individual and collective mindfulness can reduce the tendency to work around a safety regulation, leading to a safer work environment. Note that we do not suggest that hospitals should reduce the emphasis on safety regulations. Instead, we argue that hospitals may benefit from simultaneously focusing on mindfulness to increase the effectiveness of implementing safety regulations.
Second, our study suggests that hospital managers should focus on improving both individual and collective mindfulness rather than making a choice between the two. One potential way to increase individual mindfulness is by offering mindfulness training, a practice already observed in other organizations tasked with delivering an error-free service in dynamic, complex, and time-pressured conditions (such as aircraft carrier flight desks and nuclear power control rooms). Collective mindfulness can be improved by implementing mindfulness-inducing HR practices. Positive employee relations and emphasizing training have been shown to induce collective mindfulness as they stimulate sensitivity to operations and commitment to resilience, which are two of the five underlying processes of collective mindfulness (Vogus & Welbourne, 2003). Creating an environment where employees feel safe to speak up also has the potential to induce more collective mindfulness (Edmondson, 1999). Previous research suggests that particular leadership styles, such as authentic leadership, and particular behavioral patterns in the leader’s behavior, such as word-deed alignment, help develop an environment where employees feel safe to speak up (Leroy et al., 2012).
Finally, recent research suggests that collective mindfulness is more likely to emerge when team members experience emotional ambivalence and prosocial motivation (Vogus, Rothman, Sutcliffe, & Weick, 2014). Although empirical evidence concerning the relationship between emotional ambivalence, prosocial motivation, and collective mindfulness is lacking, hospitals can incorporate these insights into their employee selection procedures. Importantly, the different approaches outlined in this article to stimulate collective mindfulness also complement lean and other quality improvements initiatives in hospitals.
Limitations and Future Research
A brief mention of some limitations of this study should be made to place our results in perspective. First, our data are cross-sectional and derived from a single source: hospital nurses. We therefore must be careful with the conclusions we draw regarding the causality of our arguments. An alternative explanation for our results could be that nurses who have experienced an occupational safety failure are more likely to say that they or their team should be more mindful. Our data does not allow for the disentanglement of this alternative explanation from the theoretically grounded explanation we have developed and tested in this study. That said, the effect of experiencing an occupational safety failure on individual and collective mindfulness is an unexplored research area and deserves more attention in future research.
We must also be careful with the conclusions we draw regarding the strength of our cross-sectional findings (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). Although the common method bias may have biased these relationships, it would likely have influenced all relationships in the same way and therefore would not influence our test of the mediation hypotheses. Longitudinal research, in any case, may help overcome these issues.
Second, research is needed to determine the extent to which the relationships we document are generalizable to other health care settings. Such generalization rests on the assumption that the use of safety regulations to enhance occupational safety and the prevalence of safety work-arounds are not unique to hospital settings. Although empirical evidence supports this assumption (see Christian et al., 2009, for an overview), establishing the boundary conditions of our argumentation by investigating the role of individual and collective mindfulness in other health care settings, such as nursing homes, is an important next step that should be taken.
Third, in our study, we measured individual and collective mindfulness and used differences between individuals and teams to investigate the effects of individual and collective mindfulness. Our decision to measure differences in mindfulness rather than to induce differences in mindfulness between individuals and teams by manipulating mindfulness with an intervention is in line with the majority of research in this domain. Furthermore, in previous research, measuring mindfulness differences yields similar outcomes as those derived from inducing differences in mindfulness (Chiesa & Serretti, 2009).
On the other hand, improving nurses’ occupational safety by focusing on mindfulness may occur via mindfulness training at both the individual and team level. Future research should thus examine whether mindfulness training or short inductions can increase occupational safety through a reduction in safety work-arounds. Given that the typical 8-week-long mindfulness training (e.g., Kabat-Zinn, 2002) is not always feasible in health care contexts, future research should also study whether and how shorter mindfulness inductions (Koole, Govorun, Cheng, & Gallucci, 2009) enhance performance outcomes.
Finally, the relationship between individual mindfulness and collective mindfulness should be further explored. In this study, we explicitly chose to study both concepts at different levels of analysis. We highlighted similarities as well as differences in both constructs and demonstrated the importance of including both when predicting work-arounds. Future research needs to clarify how both may be interrelated.
Conclusion
Previous research has already documented several benefits of mindfulness. Individual mindfulness has been shown to enhance positive outcomes in several important life domains, including mental health, physical health, behavioral regulation, and interpersonal behavior (see Brown et al., 2007, for an overview). The performance effects of collective mindfulness have also begun to emerge (Rerup, 2009; Vogus & Sutcliffe, 2007a). In this study, we examined the effects of individual mindfulness and collective mindfulness on occupational safety in hospitals and clarified how each type of mindfulness is linked to nurses’ occupational safety.
Overall, this study emphasizes the importance of mindfulness as one potential way to reduce nurses’ well-documented tendency to work around occupational safety regulations. Unpacking the roles of individual mindfulness and collective mindfulness in ensuring occupational safety may further advance our knowledge of how to create safer workplaces. At a broader level, this study speaks to the debate about the efficacy of introducing safety regulations to create safer workplaces (Lucian Leape Institute, 2013).
Footnotes
Acknowledgements
We are indebted to Jonathon Halbesleben, Kathleen Sutcliffe, and Timothy Vogus for helpful comments on earlier versions of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.