
Abstract
This study assesses individual- and area-level predictors of racial/ethnic disparities in mental health care episodes for adults with psychiatric illness. Multilevel regression models are estimated using data from the Medical Expenditure Panel Surveys linked to area-level data sets. Compared with Whites, Blacks and Latinos live in neighborhoods with higher minority density, lower average education, and greater specialist mental health provider density, all of which predict lesser mental health care initiation. Neighborhood-level variables do not have differential effects on mental health care by race/ethnicity. Racial/ethnic disparities arise because minorities are more likely to live in neighborhoods where treatment initiation is low, rather than because of a differential influence of neighborhood disadvantage on treatment initiation for minorities compared with Whites. Low rates of initiation in neighborhoods with a high density of specialists suggest that interventions to increase mental health care specialists, without a focus on treating racial/ethnic minorities, may not reduce access disparities.
Introduction
While overall prevalence rates of mental illness are similar across racial/ethnic groups (Breslau et al., 2006), the burden of mental illness is greater for minority populations. Latinos and Blacks with mood disorders and Blacks with anxiety disorders are more likely to be persistently ill than Whites with these psychiatric disorders (Breslau et al., 2005). In addition, major depressive disorder is more likely to become chronic among Blacks and Latinos than among Whites (Breslau et al., 2005; Williams et al., 2007) and leads to a higher degree of functional limitation among Blacks than among Whites (Williams et al., 2007). In the presence of these disparities in the burden of mental illness, mental health care disparities have persisted, with a widening of Latino–White disparities (Blanco et al., 2007) from 1993 through 2002 and persistent Black–White disparities between 2000 and 2004 (Cook, McGuire, & Miranda, 2007). Toward these ends, there have been numerous calls to reduce service gaps (U.S. Department of Health and Human Services, 2000).
Improving access to mental health treatment has the potential to reduce disparities in persistence and severity because evidence-based care works as well for minorities as it does for Whites (Miranda et al., 2005; Schraufnagel, Wagner, Miranda, & Roy-Byrne, 2006). Despite this potential, we know little about area-level influences on disparities in mental health treatment, while efforts to engage patients at the individual level are often costly and difficult to reproduce at the population level (Alegria, 2009). To this end, this study extends prior work in understanding episodes of mental health care by incorporating individual-, census block group-, county-, and state-level factors to clarify the influence of pathways at multiple levels underlying racial/ethnic disparities in episodes of mental health care. Because the magnitude of disparities in the initiation of mental health care are extremely large, we further decompose the relative contribution of each of these factors by racial/ethnic group, thus guiding policymakers toward areas for which policy changes may have greater relative impact.
Conceptual Models
Individual-level behavioral approaches to understanding who seeks mental health treatment, and why, overlook contextual factors beyond the control of the individual (Pescosolido, Wright, Alegría, & Vera, 1998) and make the assumption that decisions to seek treatment are rationally undertaken based on need for care and availability of services. Our work is guided by two conceptual models incorporating multilevel factors that influence mental health care. First, the social-ecological model (Stokols, 1996) recognizes that health behaviors change because of not only individual-level factors but also those at the social and physical environment and the policy level. Second, the network episode model (Pescosolido, 2006) recognizes that understanding mental health care access requires not only understanding behavior change but also the interrelationships among the social context, individual episode factors, the illness history of the individual, social supports/networks, and the health care delivery system that lead people to formal treatment.
Recent studies have found contextual variables such as provider supply and provider characteristics to be important predictors of mental health care access (Cook, Doksum, Chen, Carle, & Alegria, 2013) and compositional variables such as neighborhood segregation to have an important influence on the type of mental health care provider seen during treatment (Dinwiddie, Gaskin, Chan, Norrington, & McCleary, 2013). However, more information about the joint influence of compositional and contextual characteristics of neighborhoods is needed to better understand how health care policies, the social environment, and community networks influence disparities in initiation and retention in care. Factors at the individual, neighborhood/county, and state levels can all influence disparities via multiple and interacting pathways. We thus explore how the distributions and effects of predictors vary by race/ethnicity, after adjustment for variables at multiple levels: (1) the individual level (predisposing characteristics, e.g., patient perception/stigma of mental health care; enabling characteristics, e.g., health insurance and language proficiency; and need characteristics, e.g., depressive symptoms and psychological distress; Andersen, 1995; Andersen & Aday, 1978); (2) the neighborhood level (e.g., census block group differences in insurance status, poverty, and population distribution of racial/ethnic minorities); (3) the county level; and (4) the state level (e.g., differences in state mental health care policies and Medicaid eligibility).
Individual-Level Factors
Racial/ethnic minorities are likely to be disadvantaged compared with Whites on many characteristics known to influence mental health care. For example, Blacks and Latinos are more likely to be uninsured, a strong negative predictor of receiving mental health care (Cook et al., 2007; McGuire, Alegria, Cook, Wells, & Zaslavsky, 2006; Zuvekas & Taliaferro, 2003). Multiple barriers contribute to this disparity in coverage, including the greater likelihood that racial/ethnic minorities will be uninsured (Alegria et al., 2012), have jobs that are less likely to offer coverage, and ineligible for public insurance coverage due to citizenship or legal residence requirements (Schur & Feldman, 2001). Limited English-language proficiency among certain Latino subgroups also may lead to mental health care disparities given that limited English-language proficiency individuals are less likely to report having a usual source of care (Ponce, Hays, & Cunningham, 2006) and report lower scores for timeliness of care, provider communication, and staff helpfulness than their English-speaking counterparts (Weech-Maldonado et al., 2003). Prior studies have also identified the significant associations among socioeconomic status (SES), age, gender, and urban residence on mental health care access (Alegria et al., 2002; Cook et al., 2007; Cook et al., 2014; Kirby, Taliaferro, & Zuvekas, 2006).
Neighborhood- and County-Level Factors
A significant association exists between mental health care and neighborhood characteristics (Diez-Roux & Mair, 2010; Truong & Ma, 2006), with significant variation across regions of the United States in the assessment and treatment of mental health conditions (Edlund, Belin, & Tang, 2006). Evidence is mixed as to whether these neighborhood characteristics influence racial/ethnic disparities in health care. Geographic differences in quality of care explain most of the difference between racial and ethnic groups for a number of medical (nonmental health) procedures among Medicare beneficiaries (Baicker, Chandra, Skinner, & Wennberg, 2004). However, for mental health care access, mental health care provider density, the existence of a community mental health center, and health maintenance organization (HMO) penetration at the county-level explain some, but not all, of the racial/ethnic disparity (Cook et al., 2013). Area differences in disparities may also be attributed to differential area levels of poverty and segregation. Living in segregated communities with greater levels of poverty and lower levels of political empowerment may contribute to feelings of powerlessness, hopelessness, and alienation from societal institutions, thereby impeding health care seeking and other healthy behaviors (Braithwaite & Lythcott, 1989; LaVeist, 1992). Living in neighborhoods with greater residential segregation, defined as the separation of minorities and Whites in their place of residence, school, work, or places of worship (LaVeist, Rolley, & Diala, 2003), has been shown to account for a large percentage of the Black–White differences in access to medical services (Kirby et al., 2006). These neighborhood-based disparities in health care resources may be especially predictive of racial and ethnic disparities in the unmet need for services given that minorities living in segregated and impoverished neighborhoods are more likely to experience social disorder (Cohen, Farley, & Mason, 2003) and psychological distress (Galea & Vlahov, 2005) and be diagnosed with depression (Weich et al., 2002). We extend our prior studies to focus on correlates of mental health care within more finely defined areas, assessing the role of neighborhood characteristics at the census block group level and health care resources at the county level.
State-Level Factors
State Medicaid policies may influence access to mental health services both in determining income standards for Medicaid eligibility as well as in determining the scope and types of mental health services covered in Medicaid programs. State regulation of private insurance markets may also influence access to mental health services, for example, via state mental health parity mandates.
We continue a line of health services research centered on identifying place-based health care variations (Fisher, Goodman, & Chandra, 2008), identifying how racial/ethnic minorities differ from Whites on individual-, neighborhood-, and state-level predictors of mental health care; how the effects of these predictors differ by race/ethnicity; and whether these differences persist after adjustment for multilevel factors. In doing so, we provide an assessment of the significant predictors of racial/ethnic disparities in mental health care initiation derived from all levels of the social-ecological model (Stokols, 1996), providing information relevant to policymakers and administrators. We separately identify how the composition of a neighborhood contributes to mental health care disparities (via sociodemographic makeup, exposure to community-level supply factors, and state policies) and how these factors influence care differentially for racial/ethnic minority groups (i.e., the moderating effect [interaction] of race/ethnicity and area-level variables).
Method
Data Source and Study Sample
We used responses from Panels 9 to 13 (corresponding to years 2004-2009) of the Medical Expenditure Panel Survey (MEPS). The MEPS data provide an in-depth, comprehensive look at health care use and expenditures for a nationally representative sample of the community population during a 2-year time period, including details on individuals’ psychotherapy, outpatient, inpatient, emergency room, and office-based visits and prescription drug use. In the MEPS Household Component, respondents were interviewed about all household members’ sociodemographic information, clinical characteristics, and health care use and expenditures. Information regarding health care use and expenditures was verified directly from individual user’s medical care providers and pharmacy records in the Medical Provider Component. Through a data use agreement with the U.S. Census Research Data Center, census block group, county, and state identifiers were linked to MEPS participants. Analyses were conducted at the Boston Census Data Center and at the Agency for Healthcare Research and Quality.
Our sample includes non-Latino White, non-Latino African American or Black, and Hispanic or Latino adults 18 years and older with probable psychiatric disorder (N = 13,211 episodes of mental health care representing 10,399 individual respondents). Racial/ethnic categories (referred to as White, Black, and Latino from here on) are based on U.S. Census definitions; because of sample sizes, we were unable to include Native Americans or Asian/Pacific Islanders. We restricted the sample to adults who had probable depressive disorder using the Patient Health Questionnaire–2 (PHQ-2) depression symptom checklist (score ≥2) or had severe psychological distress on the K-6 scale (score ≥13; Kessler et al., 2003). Limiting the sample to those with clinical need for mental health care was done in an attempt to exclude individuals who may be overusing or receiving inappropriate care. PHQ-2 scores ≥2 have strong sensitivity (86%) and specificity (78%) to a diagnosis of major depressive disorder (Arroll et al., 2010). The K-6 scale was designed to maximize the ability to discriminate cases of serious mental illness from noncases while being amenable to quick and easy administration in national population surveys such as the MEPS. The K-6 is predictive of serious mental illness defined as any individual with a DSM-IV diagnosis and severe impairment by the Alcohol, Drug Use, and Mental Health Administration Reorganization Act (Kessler et al., 2003). Both the PHQ-2 and K-6 scales have been validated in Spanish-speaking populations (Reuland et al., 2009; Stolk, Kaplan, & Szwarc, 2014; Valencia-Garcia, 2012). The populations captured via PHQ-2 and K-6 did not differ significantly by race/ethnicity.
Outcomes of Interest: Initiation and Length of Mental Health Care Episodes
Dependent variables are the probability of initiation of care (among 13,211 mental health care episodes of respondents with probable psychiatric disorder) and the number of days in a mental health care episode (among 4,474 mental health care episodes of respondents who had probable psychiatric disorder and initiated mental health treatment). A mental health care event was defined similar to a prior study (Cook et al., 2014): (1) primary care physician (PCP) or mental health specialist visits (psychiatrist, psychologist, counselor, or social worker) with International Classification of Diseases-9 (ICD-9) Codes 291, 292, or 295-314 (Zuvekas, 2001); (2) prescription drug fills associated with any of these ICD-9 codes; or (3) drug fills from the psychotropic drug class as defined by the Multum Lexicon Drug Database (Multum Information Services, 2009). New episodes of mental health care were defined as any mental health treatment that was separated by 12 weeks or more from a previous mental health care event (Cook et al., 2014; Keeler, Manning, & Wells, 1988; Tansella, Micciolo, Biggeri, Bisoffi, & Balestrieri, 1995). Assessing mental health care by episodes of care is one way to more accurately capture the complex treatment patterns seen with mental illness (Cook et al., 2014; Jimenez, Cook, Chen, Bartels, & Alegria, 2013; Saloner, Carson, & Cook, 2014). Episodes allow for a more targeted analysis of underlying care-seeking behaviors that drive disparities in mental health care than do cross-sectional averages. Furthermore, episodes allow us to more effectively capture treatment behaviors such as the decision to initiate care (as opposed to a count of mental health care visits over a calendar year) that are directly amenable to policy change.
Predictor Variables: Individual-Level Factors
Individual-level covariates are education, income, marital status, region of the country, residence in a metropolitan statistical area (MSA), citizenship status, insurance coverage type (private insurance, Medicaid, Medicare, or other public insurance), and participation in an HMO. Variables indicating individual-level need are self-reported mental and physical health, the mental and physical health components of the Short Form (SF-12) questionnaire, as well as gender and age. Physical health variables, which are also indicators of need given the high rates of comorbidity between physical ailments and mental disorders (Afari, Schmaling, Barnhart, & Buchwald, 2001; Alexopoulos et al., 1997; Clarke & Meiris, 2007; de Groot, Anderson, Freedland, Clouse, & Lustman, 2001), are any limitation due to physical health, body mass index, and the presence of 0, 1, or 2 plus chronic physical health illnesses out of a list of 11 priority physical health conditions queried of all respondents in the MEPS.
Predictor Variables: Neighborhood-, County-, and State-Level Factors
Two main sources of area-level data were merged with the MEPS: the 2005-2009 U.S. American Community Survey (census block group level; Matheson et al., 2006; Silver, Mulvey, & Swanson, 2002) and the 2007 Area Health Resource File (county level). Census block groups are used as proxy representations of neighborhoods and are typically the best approximation of neighborhoods within epidemiological research (Silver et al., 2002). The U.S. American Community Survey census block group variables considered as part of the model specification were median household income and percentage of residents who are living below the poverty level, college graduates, Black, Latino, unemployed, on public assistance, living in female-headed households, foreign-born, and recent immigrants. These factors were chosen because neighborhood structural characteristics of disadvantage and affluence, racial/ethnic composition, residential mobility/instability, among other neighborhood-level factors, are likely to influence health and mental health outcomes (Diez-Roux, 1998; Robert, 1999; Williams & Collins, 2001). We also considered the following list of county-level factors: number of active medical doctors (primary care or any other specialty) per 10,000 county residents, number of active mental health specialists per 10,000 county residents, number of community mental health centers, percentage of Medicaid- and privately insured populations enrolled in managed care, and the existence of an academic training center in the county, based on prior studies demonstrating their significant association with mental health care access (Cook et al., 2013). Because of the high collinearity among neighborhood variables and county-level supply variables, we reduced the list of variables by retaining variables that were conceptually distinct from other area-level variables or were consistently significantly associated with episode initiation and episode length in stepwise regression models (reverse and forward). The final specification includes at the block group level the percentage of residents who are college graduates, Black, Latino, foreign-born, and unemployed; and at the county level, it shows the density of general health care providers and mental health specialists and the existence of an academic training center in the county. By including testing for interactions between area-level characteristics and individual-level race/ethnicity, we assess whether area characteristics affect individuals differently based on race/ethnicity, for example, whether living in a community with fewer health care providers reduces initiation more for Black than White community members. State-level variables considered in the models were indicators of specific state-level Medicaid policies (i.e., eligibility thresholds, co-pay amounts, medication coverage). Because none of the state-level indicators were statistically significant, we opted instead for a state-fixed effects approach, including an indicator for each identifiable state.
Accounting for Missing Data
The final sample included 13,211 episodes among 10,399 individuals with probable psychiatric disorder. On average, each respondent had 1.30 episodes of mental health care (1.35 episodes per person for Whites, 1.17 episodes per person for Blacks, and 1.15 episodes per person for Latinos). Less than 1% of this sample had missing data on self-reported mental health, the physical and mental health components of the SF-12, and education. These missing data were imputed using the mi procedure in Stata (StataCorp, 2014). We created five complete data sets, imputed missing values using a chained equations approach, analyzed each data set, and used standard rules to combine the estimates and adjust standard errors for the uncertainty due to imputation (Little & Rubin, 2002; Rubin, 1998).
Statistical Analyses
First, we compared Whites, Blacks, and Latinos on sociodemographic characteristics and then examined the characteristics of the census block groups (neighborhoods), counties, and states where they live. Second, we estimated multilevel regression models of initiation and duration (days) of mental health care episodes for those with probable psychiatric disorder (determined by having a PHQ-2 ≥2 representing significant depressive symptoms or a K-6 ≥13 representing severe psychological distress). For each response, we estimated linear multilevel random effects models following the basic structure:



where Yijk is a measure of mental health care use of individuals i within census block group j and county k (the full model is actually a four-level model that includes nesting of mental health care episodes within individuals within Census Block Groups within Counties, but we present a three-level model here to simplify the presentation), Ri the race/ethnicity of the ith individual, HSi the vector of individual health status characteristics, SESi the vector of individual socioeconomic status variables, Statei a vector of dummy variables indicating the respondent’s state of residence, cbgj the vector of census-block-group-level characteristics, and Ck a vector of county-level characteristics. Assessment of variance components at each level (i.e., σ cbg 2 and σ C 2) in models without covariates allows for an initial assessment of the partitioning of variance by individual, census block group, county, and state levels. We estimated linear multilevel models using the xtmixed command in Stata 14. Linear models were used in estimation for ease of interpretation and because nonlinear models did not converge when incorporating all levels. Significance and direction of covariates were nearly identical in three-level nonlinear models estimated using xtlogit for initiation and xtpoisson for episode length, and so are not presented here.
The model coefficients test the significance of the association among initiation and individual, census block group, county, and state characteristics. The hierarchical nature of the models measures variability across the multilevel structure and accounts for the nonindependence of individuals living in the same area (Raudenbush & Bryk, 2002).
To assess underlying area-level mechanisms of disparities, we first identified whether significant predictors differ in distribution by race/ethnicity (suggesting that disparities arise because minorities live in areas with greater disadvantage) and next examined whether there are significant interactions between significant predictors and race/ethnicity (suggesting that the disadvantage is greater for minorities). We reestimated the model in Equation (1) removing individual-level race/ethnicity and SES variables to address the issue that including individual-level covariates correlated with significant neighborhood-level variables may cause the significance of neighborhood-level coefficients to be underestimated (Bingenheimer & Raudenbush, 2004). All standard errors account for MEPS sampling design characteristics using the balanced, repeated replication method (Agency for Healthcare Research and Quality, 2012).
We also used the Blinder–Oaxaca decomposition method (Blinder, 1973; Oaxaca, 1973), using the oaxaca command in Stata (StataCorp, 2014), to quantify to what extent the individual-, neighborhood-, and county-level characteristics and states are associated with the racial and ethnic disparities in initiation of mental health care and what parts of the difference are unexplained in the model. A linear regression model of initiation of mental health care (described above) is estimated separately for each racial/ethnic group and used to generate predicted probabilities of initiation. To assess the contribution of each variable, we calculated the change in the average predicted probability by replacing the minority mean with the White mean of that variable while holding the distributions of the other variables constant. Summing together, variables’ contribution at each level allows us to calculate how much of the overall difference between groups is explained by each level.
Results
Descriptive Analysis
Blacks and Latinos with probable mental illness were significantly less likely than Whites with probable mental illness to initiate care. There were no significant Black–White and Latino–White differences in duration of treatment (Table 1). Compared with Whites, Blacks and Latinos were less likely to be married, insured, or live in the West and Midwest but more likely to be publicly insured, younger, of lower income, having lower educational attainment, living in an urban setting (MSA), and reporting higher (healthier) scores on the mental health component of the SF-12 and greater self-reported mental health. Latinos were more likely than Whites to have the MEPS administered in Spanish and to be noncitizens, less likely to have a comorbid physical health disorder, and less likely to have a limitation of activity. Blacks had lower (less healthy) scores on the physical health component of the SF-12, had higher average body mass index, and were more likely to live in the South compared with Whites.
Descriptive Statistics of Individual-Level Variables, County-Level Variables, and Census Block Group Characteristics by Race/Ethnicity (N = 13,211 Mental Health Treatment Episodes/10,399 Individuals).
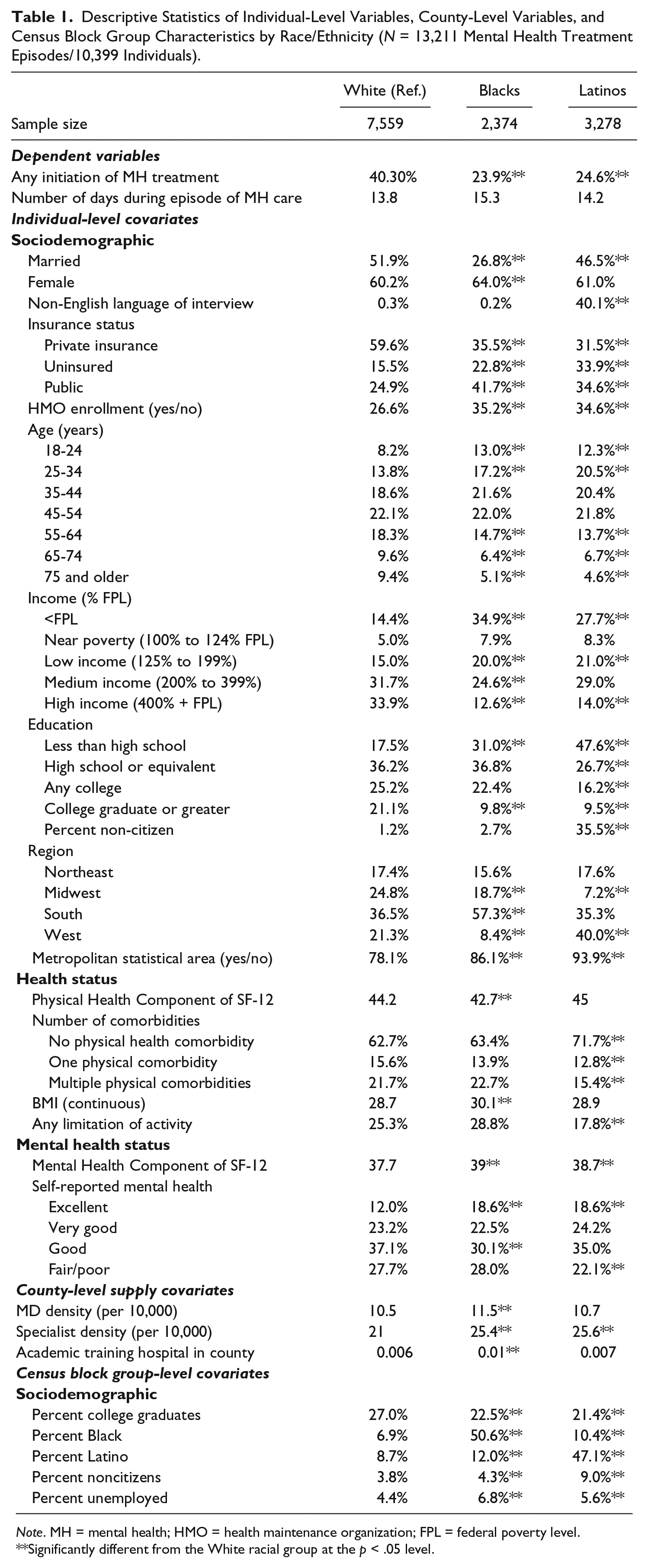
Note. MH = mental health; HMO = health maintenance organization; FPL = federal poverty level.
Significantly different from the White racial group at the p < .05 level.
Compared with Whites, Blacks and Latinos lived in census block groups with higher unemployment rates, fewer college graduates, a greater percentage of noncitizens, and a greater percentage of Black and Latino residents (Table 1). Black residents with probable mental illness lived in counties with a greater density of general MDs, mental health specialists, and training hospitals per 10,000 residents than the counties where Whites with probable mental illness lived. Latinos also lived in counties with a greater density of mental health specialists.
Predictors of Initiation of Mental Health Care
The variance components corresponding to the individual, census block group, county, and state were significant, suggesting that there is significant variation in mean initiation at each level (Table 2). The null multilevel model found that 23.7%, 1.9%, 1.4%, and 0.2% of the variance is attributable to the individual, census block group, county, and state levels, respectively.
Random Intercepts Multilevel Linear Regression Models of Any Mental Health Treatment Episode Initiation (N = 13,211).
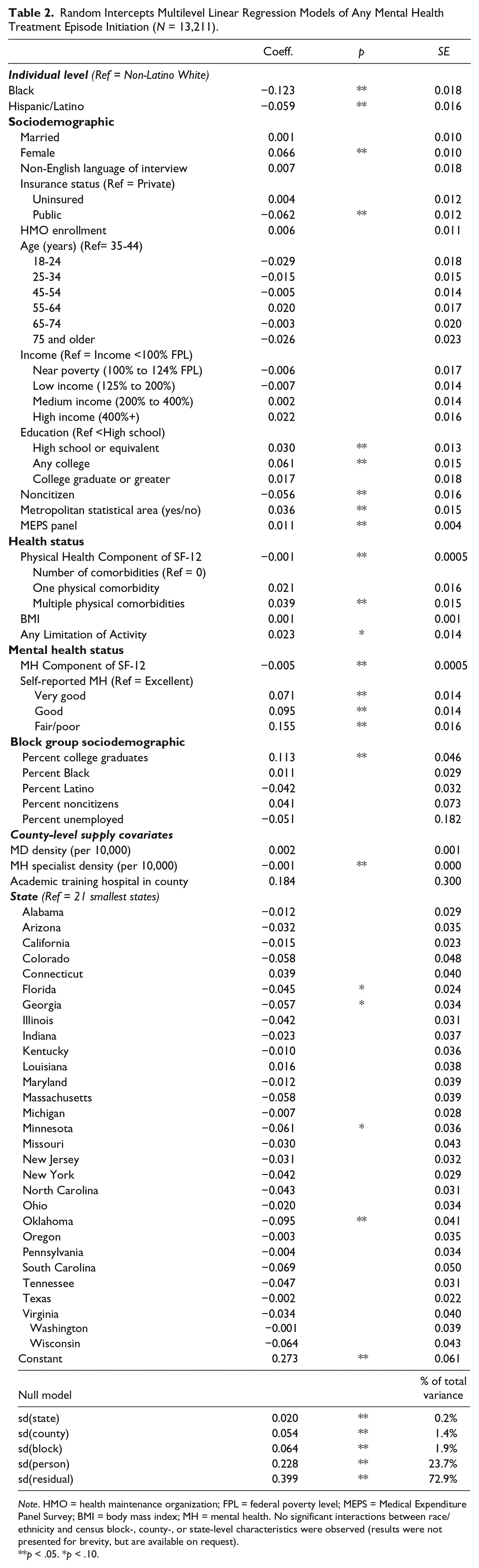
Note. HMO = health maintenance organization; FPL = federal poverty level; MEPS = Medical Expenditure Panel Survey; BMI = body mass index; MH = mental health. No significant interactions between race/ethnicity and census block-, county-, or state-level characteristics were observed (results were not presented for brevity, but are available on request).
p < .05. *p < .10.
Individual-level factors that predicted greater likelihood of initiating mental health care were being female, having higher education, living in an MSA, being surveyed in more recent MEPS panels, having physical comorbidities or limitation of activity, and reporting poorer mental health. Individual-level factors that predicted lower initiation were being Black or Latino, being publicly insured (vs. privately), being a noncitizen, and scoring higher (healthier) on the physical and mental health components of the SF-12 (Table 2).
At the neighborhood level, living in census block groups with a greater percentage of college graduates, where Whites were more likely to reside, was positively associated with mental health treatment initiation. Individuals in counties with greater mental health specialist density, where Blacks and Latinos were more likely to reside, were significantly less likely to initiate treatment. Living in Oklahoma (p < .05), Florida, Georgia, and Minnesota (p < .10) was associated with less initiation of mental health care compared with the 21 smallest states in the United States.
No significant interactions between race/ethnicity and census block-, county-, or state-level characteristics were observed. In models adjusted for age, insurance, health status, and area-level measures (but not individual-level race/ethnicity or SES), higher percentages of Blacks and Latinos in a neighborhood were negatively associated with initiation of mental health services (results are available on request).
Predictors of Episode Length (Number of Days per Episode)
In multilevel analyses of number of days per episode, the variance components corresponding to the individual, census block group, and state, but not the county, were significant in null models (Table 3). The multilevel model finds that approximately 42%, 9%, 0.3%, and 0.5% of the variance is attributable to the individual, census block group, county, and state levels, respectively.
Random Intercepts Multilevel Linear Regression Model of Number of Days of Treatment During Episode Among Those Receiving Any Mental Health Treatment (N = 4,474).
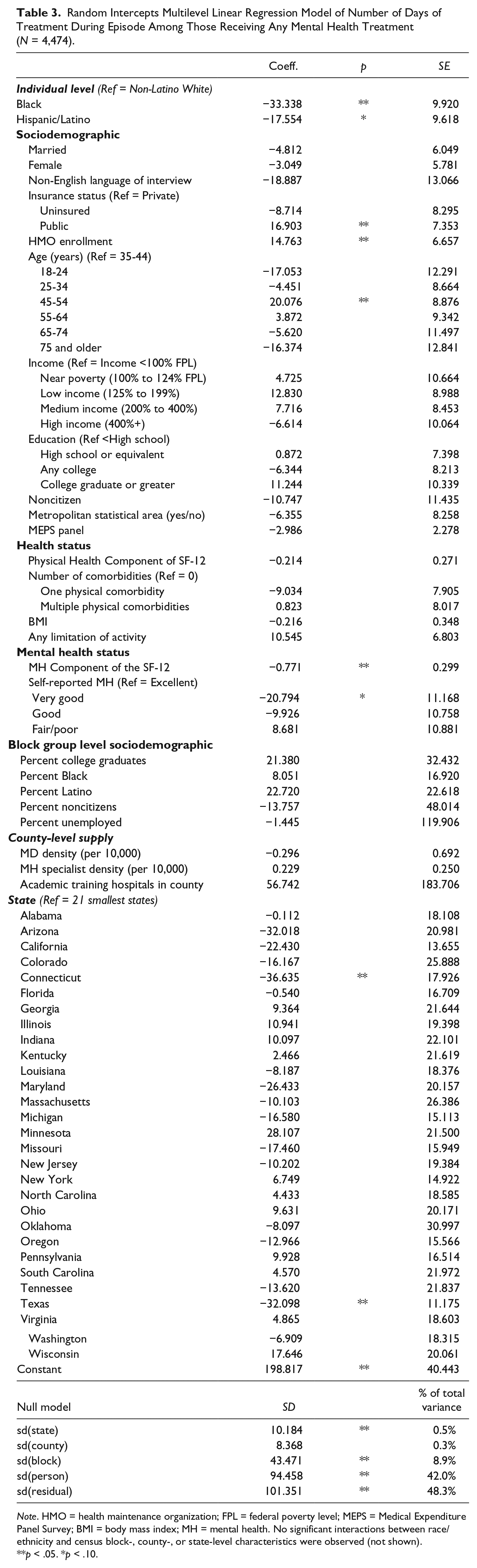
Note. HMO = health maintenance organization; FPL = federal poverty level; MEPS = Medical Expenditure Panel Survey; BMI = body mass index; MH = mental health. No significant interactions between race/ethnicity and census block-, county-, or state-level characteristics were observed (not shown).
p < .05. *p < .10.
Adjusting for individual-, census block group-, county-, and state-level characteristics, Blacks with probable mental illness who initiated care had a shorter length of episode than their White peers (Table 3). The Latino–White disparity was marginally significant. Individual-level factors that predicted greater number of days per treatment episode were public (vs. private) insurance, HMO enrollment, and between the ages of 45 and54 years (compared with 35-44 years). Meanwhile, factors that predicted fewer days per treatment episode were higher (healthier) scores on the mental health components of the SF-12 and very good (compared with excellent) self-reported mental health status. Individuals living in Texas or Connecticut had shorter episode lengths compared with individuals living in the 21 smallest states.
No significant interactions between race/ethnicity and census block-, county-, or state-level characteristics were observed. In models adjusted for age, insurance, health status, and area-level measures (but not individual-level race/ethnicity or SES), higher percentages of Blacks in a neighborhood was a significant negative predictor of number of days in an episode of mental health care (results are available on request).
Decomposition of Disparities in Initiation of Mental Health Care
The predicted likelihood of initiation for Whites (the reference group), Blacks, and Latinos was 40%, 24%, and 25%, respectively (Table 4). The observed population characteristics explained 31% of the disparity between Whites and Blacks and 67% of the disparity between Whites and Latinos.
Oaxaca–Blinder Decomposition of Initiation of Mental Health Treatment (N = 13,211).
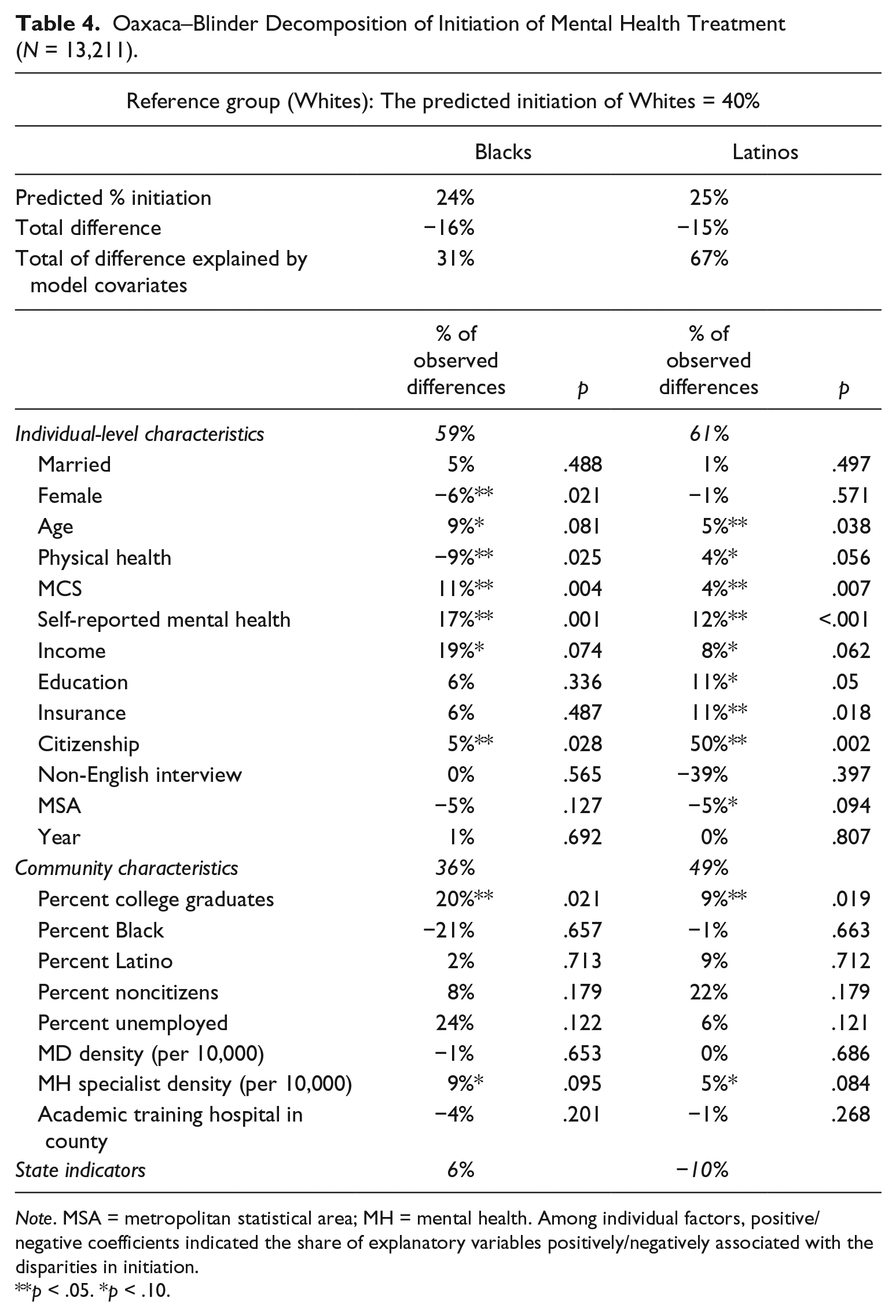
Note. MSA = metropolitan statistical area; MH = mental health. Among individual factors, positive/negative coefficients indicated the share of explanatory variables positively/negatively associated with the disparities in initiation.
p < .05. *p < .10.
Individual-level factors accounted for 59% of the observed Black–White difference. Respondents’ gender, age, physical health, mental health, income, and citizenship were major factors associated with the observed disparity in initiation among Whites versus Blacks. Area-level characteristics accounted for 36% of the observed Black–White difference. The smaller percentage of Blacks living in neighborhoods with college-educated residents was a significant contributor to the disparity in initiation. The fact that Blacks lived in neighborhoods with greater mean mental health specialist density was a marginally significant contributor (p < .10) to the Black–White disparity in initiation. State differences accounted for only 6% of the observed difference.
Individual-level factors accounted for 61% of the observed Latino–White difference. Age, mental health status, insurance status, and citizenship were major individual factors associated with the observed differences in initiation among Whites versus Latinos. Area-level characteristics accounted for 49% of the observed Latino–White difference. The smaller percentage of Latinos living in neighborhoods with college-educated residents was a significant contributor to the disparity in initiation. The fact that Latinos lived in neighborhoods with greater mean mental health specialist density was a marginally significant (p < .10) contributor to the Latino–White disparity in initiation. State differences accounted for −10% of the observed differences in treatment initiation, meaning that Latinos were more likely than Whites to live in states with greater mental health care initiation.
Discussion
Similar to a prior study of disparities in mental health treatment episodes among individuals with probable mental illness (Cook et al., 2014), we identified significant Black–White and Latino–White disparities in initiation of mental health care, and additionally, we found that these disparities persist even after adjustment for individual-, census block group-, county-, and state-level characteristics. Furthermore, Blacks with probable mental illness had significantly fewer days per mental health episode than did Whites, and Latinos had fewer days by a marginally significant margin. Finding no significant interactions between race/ethnicity and area-level factors suggests that Black–White and Latino–White disparities in initiation of mental health treatment emerge because Blacks and Latinos on average are more likely than Whites to reside in areas of disadvantage and not because living in an area of disadvantage is more detrimental to Blacks and Latinos than Whites.
Racial/ethnic differences in mental health care were explained by both compositional and contextual place-based differences, suggesting that the incorporation of a social-ecological perspective and the network episode model enhances our ability to identify critical influences on disparities in the receipt of mental health care and potential policy levers. The compositional finding that neighborhoods with residents with lower education levels have lower rates of mental health care access reinforces the importance of the association between neighborhood SES and racial/ethnic disparities in accessing care. Families with greater education may be better able to link to quality mental health services and have networks with greater access to medical information and resources (Pescosolido, 2006). Individuals in these neighborhoods are also more likely to obtain more comprehensive health insurance coverage and the means to purchase quality mental health care (Dinwiddie et al., 2013).
In addition, the contextual effect of availability of mental health treatment is reflected in mental health specialist density, which may have important and underexamined impacts on treatment seeking and receipt of care. The low rates of initiation of mental health care for individuals living in areas of high density of mental health specialty care may seem counterintuitive but echoes prior studies demonstrating that specialists choose not to work with disadvantaged urban patients because of the complexity of their physical and mental health problems, low reimbursement for Medicaid-insured populations, or no reimbursement for uninsured individuals (Fiscella, Franks, Doescher, & Saver, 2002; Fiscella & Williams, 2004; Komaromy et al., 1996). Specialist providers, particularly those associated with large urban teaching hospitals, may not be accessible to local residents due to closed panels, a disproportionate number of psychiatric specialists situated in inpatient modalities as opposed to outpatient care, greater involvement in research or supervision of trainees that limits clinical hours, or because they include a high number of trainees who may see fewer patients.
Other studies have identified that respondents in majority Black communities were more likely to be treated by nonpsychiatrists and general doctors and that respondents in majority Latino neighborhoods were more likely to be treated by general doctors when compared with neighborhoods with a lower concentration of racial/ethnic minorities (Dinwiddie et al., 2013). Health care providers may also be reluctant to practice in low-income segregated areas (Gaskin, Dinwiddie, Chan, & McCleary, 2012). While Latinos may live in close proximity to major teaching and safety net hospitals, these areas are often limited in the number of available mental health services for individuals with subsidized insurance such as Medicaid (Alegria et al., 2002). In addition to the issue of apparent versus actual availability of mental health specialists, there tends to be higher stigma among racial/ethnic minority groups toward seeking mental health care (Ferrari et al., 2015; Latalova, Kamaradova, & Prasko, 2014). Treatment in primary care settings may not carry the same stigma as psychiatric treatment by specialty mental health care providers, and PCPs may therefore be better positioned to improve initiation for mental health treatment for racial/ethnic minorities.
Similar to a prior study, we identified significant Black–White and borderline-significant Latino–White disparities in length of mental health treatment episode (Cook et al., 2014), but we did not identify any significant neighborhood-level correlates of episode length. Other unmeasured area-level factors are likely to explain these disparities in length of mental health care episodes, given that census block group factors are very important, explaining nearly a third of the variation in length of episode (results not shown). Mechanisms such as proximity to treatment, social networks, and familiarity of specialists with neighborhood norms may operate to increase retention in care and should be investigated in future studies.
We identified that racial/ethnic makeup of a census block group was a significant predictor of mental health care access and episode length after removing individual-level race/ethnicity and SES variables from model specifications. This discrepancy in results is evidence of the context versus composition quandary inherent to multilevel modeling (Bingenheimer & Raudenbush, 2004), where it is difficult to interpret whether contextual differences are due to differences in the individuals who make up the neighborhood (i.e., there are more Blacks living in a neighborhood and Blacks are less likely to initiate care) versus differences in attributes specific to the neighborhood (neighborhoods with a high density of Black individuals reflect a history of residential segregation, a factor that limits access to mental health care). For the latter, adjustment of individual-level variables may absorb important variation at the neighborhood level. For example, individual-level self-rated health may be a proxy for the allostatic load individuals incur over time in certain social and community networks (McEwen, 1998; Todorova et al., 2013) and thus may absorb much of the neighborhood variation that might be important. Future qualitative studies may disentangle these contextual and compositional influences.
Results from the Oaxaca–Blinder decomposition for initiation of mental health treatment echo an earlier study decomposing racial/ethnic differences in any ambulatory health care services (Kirby et al., 2006) that observed variables explain a small percentage (31% in our study) of the difference between initiation for Blacks and Whites. Observed variables explained more of the Latino–White difference in initiation (67%) compared with the Black–White explained difference (31%). There is thus a need for improved data at all levels to better understand what deters racial/ethnic minority residents from initiating mental health treatment in their own communities. Prior literature suggests that incorporation of additional variables related to health care experiences, medical knowledge, resources of the social networks of respondents (Pescosolido, 2006), levels and types of perceived discrimination (Burgess, Ding, Hargreaves, van Ryn, & Phelan, 2008), and cultural attitudes and beliefs toward mental health care (Kirby et al., 2006) might improve our ability to identify contributors to mental health care access disparities and then determine how these factors interrelate across different socioecological levels.
The Oaxaca–Blinder analysis suggests important differences between Blacks and Latinos with respect to which individual factors significantly contribute to disparities between each minority group and Whites in the sample. Citizenship is a stark example in that it accounted for 50% of the observed Latino–White difference but accounted for only 5% of the observed Black–White difference, suggesting as in previous decomposition studies using MEPS data that immigration status presents a significant barrier to accessing mental health care for Latinos (Chen & Vargas-Bustamante, 2011). There was a similar contrast in how insurance status predicts access differences in that it accounted for 11% (p = .02) of the Hispanic–White disparity but only 6% (n.s.) of the Black–White disparity, highlighting the importance of reducing the extremely high rates of uninsurance in the Hispanic population (34% in our sample, compared with 23% for Blacks and 16% for Whites). Expanding Medicaid eligibility in states that have opted out of ACA Medicaid expansion is a possible policy solution given the large number of uninsured Hispanics living in states that have opted out of expansion (Garfield & Damico, 2016). Both Black and Hispanic SF-12 mental health component scores and self-reported mental health status were on average better (healthier) than those for Whites and were significant contributors to the lower access to mental health care among Blacks and Latinos compared with Whites. The large contribution of mental health status to racial/ethnic differences in mental health care access highlights the importance of the analyst’s decision to adjust or not to adjust for measures of clinical need in disparities measurement (Cook, McGuire, & Zaslavsky, 2012; McGuire et al., 2006) and suggests the need for future studies that assess the impact of access disparities on mental health outcomes.
A limitation of the study is that the PHQ-2 and K-6 scales used to measure probable psychiatric illness, while having reasonable sensitivity and specificity, are not as precise as diagnostically related instruments. Nor was it possible to disentangle initiation of care for those with varying diagnoses. In the MEPS, only those who initiate care receive an ICD-9 diagnosis code. Second, we do not have detailed information on a number of factors related to mental health specialist service provision (e.g., whether or not they accept new patients/Medicaid patients, whether they work in highly specialized or more integrated primary care/specialty settings, whether they are trainees or involved in training) to help us understand how specialist mental health care provider density relates to initiation of mental health care access. The use of density of specialty mental health providers as a measure of quality needs to be improved before it will be helpful in identifying policy levers for reducing disparities.
Despite these limitations, we provide further evidence that racial/ethnic disparities in initiation and duration of mental health care persist. Our results suggest underlying mechanisms of disparities related to both compositional and place-based effects. At the neighborhood level, the average education of the neighborhood residents and the density of specialist mental health care providers are associated with disparities in initiation of mental health care. The presence of specialists already practicing in areas of substantial Black and Latino need suggests that greater access to existing resources could reduce disparities. Potential policies to increase access include greater Medicaid reimbursements and incentivizing better integration of primary and specialist mental health care through the Accountable Care Organizations, bundled payments, and other integrated care payment mechanisms.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors, and no official endorsement by the Agency for Healthcare Research and Quality or the Department of Health and Human Services is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge funding from the Agency for Healthcare Research and Quality (R01 HS021486; PI Cook) and the National institute of Mental Health (R01-MH091042; PI Cook).