
Abstract
Medical assistants (MAs) are a flexible and low-cost resource for primary care practices and their roles are swiftly transforming. We surveyed MAs and family physicians in primary care practices in North Carolina to assess concordance in their perspectives about MA roles, training, and confidence in performing activities related to visit planning; direct patient care; documentation; patient education, coaching or counseling; quality improvement; population health and communication. For most activities, we did not find evidence of role confusion between MAs and physicians, physician resistance to delegate tasks to properly trained MAs, or MA reluctance to pursue training to take on new roles. Three areas emerged where the gap between the potential and actual implementation of MA role transformation could be narrowed—population health and panel management; patient education, coaching, and counseling; and scribing. Closing these gaps will become increasingly important as our health care system moves toward value-based models of care.
Background
Medical assistants (MAs) are a flexible, low-cost and redeployable resource for primary care practices and their roles are swiftly transforming (Chapman & Blash, 2017). As payment and care delivery models change, MAs are increasingly taking on expanded roles in chronic disease management, health promotion, patient coaching, and population health (Bodenheimer et al., 2014; Chapman & Blash, 2017; Chapman et al., 2015). Increased pressure on primary care practices to lower costs, address patients’ social determinants of health, provide preventive care, and document quality outcomes has spurred interest in redesigning workflows to delegate more tasks to MAs. These changes are being undertaken in hopes of improving patient and population health outcomes, improving access to care, enhancing patient satisfaction, and reducing provider burnout (Dill et al., 2019; Jerzak, 2019; Willard-Grace et al., 2014).
Despite the rapid pace of change in MA role and deployment, their training is highly variable and often inadequate to prepare them for new roles and responsibilities (Chapman et al., 2015). Licensure is not required, and certification requirements vary by state and employer organization. The absence of educational pathways and career lattices that reward increased MA skill development with career mobility and improved compensation may limit MAs’ willingness to take on additional training for new tasks. Previous work suggests that physician resistance to delegate tasks can also be a barrier and stems from concerns about MA training and competence to take on new tasks. Physicians in small primary care offices report restricting MA clinical autonomy in answering patient questions and providing education, yet MAs report having confidence in their ability to perform these tasks and regularly undertake these roles (Elder et al., 2014).
Even in primary care practices that have redesigned roles, confusion remains about how to optimize task sharing among physicians, nurses, medical assistants, and other providers (Edwards et al., 2018). Successful team optimization and efficient task distribution depend on the degree to which there is a shared understanding of roles, confidence in the training and competence of team members, a willingness by physicians to delegate tasks, and an opportunity for MAs to receive training to take on new roles. Physician trust in MAs and other team members is critical to navigating the culture shift from the physician-centric model of care delivery to a team model. Once physicians are assured that MAs are trained, they are more willing to trust and delegate responsibilities (Ladden et al., 2013).
Conceptual Framework
The ability of a team—in this case, a family physician and medical assistant—to “share the care” (Ghorob & Bodenheimer, 2012) is dependent on how team members distribute patient care functions between themselves (Bodenheimer, 2019). To effectively distribute tasks, physicians and MAs must share a common understanding of the MA’s role, the tasks that she or he will undertake and the MA’s competence to undertake these functions. Even with this shared understanding in place, the physician must be willing to delegate tasks and the MA willing to take on new functions and receive training for new roles. Team-based models have been shown to improve patient outcomes, access to care and patient satisfaction as well as increase the practice’s capacity to provide preventive and chronic care services (Bodenheimer & Smith, 2013; Grumbach & Bodenheimer, 2004; Sinsky et al., 2013). Effective task delegation from physicians to other team members can also increase staff engagement and satisfaction (Bodenheimer & Sinsky, 2014; Chapman & Blash, 2017; Sheridan et al., 2018). These dynamics operate at the individual level, but macro- and practice-level forces also affect the MA-physician dyad, including scope of practice regulations, payment models, and practice culture and workflows (Figure 1).
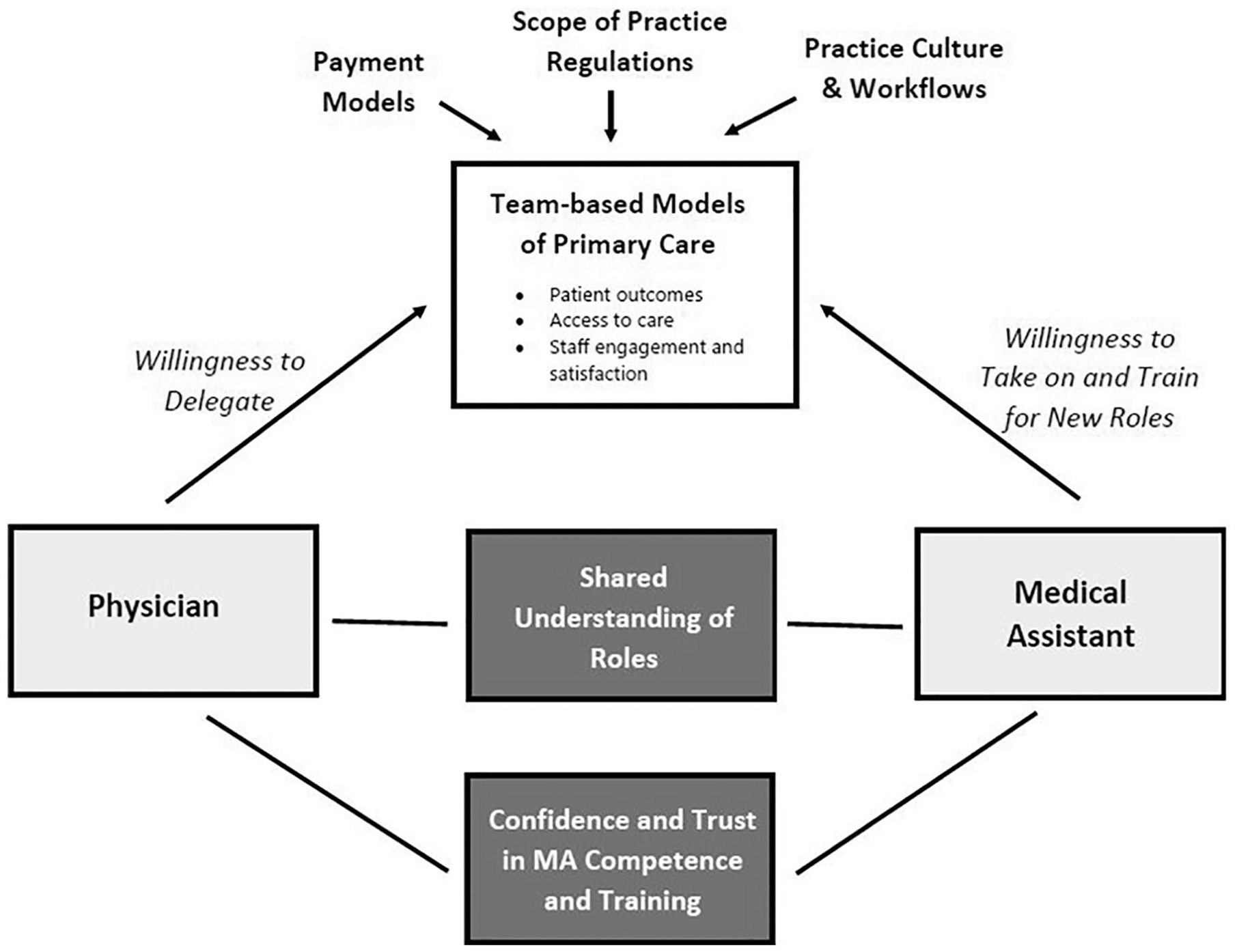
Factors influencing medical assistant and physician teamwork.
New Contributions
A robust literature identifies a gap between the full potential of MA role expansion and its implementation in primary care practice. This gap has been attributed to role confusion, shortcomings in MA training, physician resistance to delegate tasks, and MA reluctance to take on new roles. This study sought to investigate each of these dimensions of teamwork from the perspectives of both MAs and physicians in primary care. We surveyed MAs and family physicians to gauge whether they agreed on the roles MAs were currently performing and identify their level of confidence in MAs’ ability to perform these tasks. For those tasks not currently being performed, we assessed physician willingness to transition tasks to MAs with additional training and MA willingness to pursue that training.
Method
Sampling Frame
Surveys were administered to MAs and family physicians in primary care practices in North Carolina between May and September 2017. We sought to sample a representative group of MAs and family physicians employed in primary care practices, but this proved challenging because the underlying sampling frame of primary care practices in the state was unknown. Therefore, we employed two different convenience sampling methods to reach MAs and physicians. MA surveys were delivered to primary care practices by practice facilitators employed by the North Carolina Area Health Education Centers (NC AHEC) program. Since 2007, the NC AHEC has supported approximately 1,100 primary care practices across North Carolina in becoming certified as patient-centered medical homes. NC AHEC deploys practice facilitators to support quality improvement initiatives, assist with electronic health record (EHR) implementation and provide technical assistance in using clinical performance data to improve patient outcomes and lower costs in these practices (Agency for Healthcare Research and Quality, 2013; Lefebvre et al., 2017). Study authors (Erin P. Fraher and Dana Neutze) met with practice facilitators during two of their meetings and explained the study purpose. Practice facilitators as a group then agreed to deliver the surveys to MAs in the practices they supported because they saw the study as an important way to better understand the roles and skill gaps of MAs in their practices. Facilitators gave MAs the choice of filling out hard or electronic copies of the survey; the majority of MA survey respondents (96%) used the electronic survey link provided by the facilitator. Family physicians were reached through the North Carolina Academy of Family Physicians newsletter. Every 2 weeks, on June 1st, 15th, and 29th, a notice about the study appeared in the newsletter, giving family physicians a link to complete the survey. By partnering with NC AHEC and the North Carolina Academy of Family Physicians, we are were able to survey a diverse group of primary care practices from across the state.
The MA and family physician surveys were administered through Qualtrics. MA and family physician respondents were eligible for five $100 Visa gift cards that were distributed to randomly selected MAs and physicians who completed the survey. This study was determined to meet the federal “exempt” criteria for human subjects review by the University of North Carolina at Chapel Hill Institutional Review Board (Study #16-2735).
Questionnaire
The MA and physician surveys were developed based on previous work conducted by one of the authors (Dana Neutze), a family physician who practices in a family medicine clinic in an academic medical center serving 21,000 patients annually (see supplementary Appendices A and B for MA and provider survey instruments [available online]). In an effort to redesign MA roles and workflow in that clinic, 12 MAs were surveyed to assess the frequency with which they performed a range of administrative and clinical activities and to identify the roles for which they felt they needed additional training. Thirty-three providers were also surveyed to gauge their expectations, confidence, and hopes regarding MA expanded roles. The success of this project in MA and workflow redesign led to the current study which sought to extend the sample to a broader group of family medicine clinics.
The original surveys were modified based on learning from the earlier work and literature findings about evolving MA roles in primary care practices (Chapman & Blash, 2017; O’Malley et al., 2015). The revised surveys included parallel questions for both MAs and family physicians about their demographic characteristics, practice type, practice affiliation with hospital or health care system, length of time in organization, and MA to provider ratio. MA surveys included questions about the length of time worked as an MA, certification status, and their highest level of education (on-the-job training, vocational training, community college, 4-year program). MAs were asked how frequently (never, infrequently, most days) they performed activities related to visit planning; direct patient care; documentation; patient education, coaching or counseling; quality improvement; population health and communication. They were also asked whether they had taken courses or received training from their employer to perform each activity (yes/no) and about their level of confidence in performing each activity (not confident, somewhat confident, confident). Family physicians were asked, for the same set of activities, whether the MA performed the task in their practice (yes/no) and their level of confidence in the ability of the MA to perform the activity at their current level of training activity (not confident, somewhat confident, confident). For those activities that were not performed by MAs in their practices, family physicians were asked whether they would be willing to transition the activity to MAs if the MAs had proper training.
Data were collected in Qualtrics, downloaded to an excel spreadsheet and imported to Stata. All statistical analyses were performed using Stata SE v. 14.0 (StataCorp, 2015).
Results
Response Rate
A total of 118 MAs and 175 family physicians responded to the surveys. Although different sampling approaches were used to reach MAs and family physicians, their practice characteristics were similar (Table 1). Half (50%) of physicians and 47% of MAs worked in group practices with fewer than 10 providers, while nearly one third of MAs and physicians worked in practices with 10 or more providers. Two thirds of physicians and 55% of MAs worked in practices affiliated with hospitals or health care systems. The majority of MAs (62%) and family physicians (59%) worked in a one-to-one MA to provider ratio, but about one fifth (20% of MAs and 22% of physicians) worked with an MA to provider ratio of less than 1. Approximately three quarters (71%) of MAs and nearly two thirds (64%) of physicians reported almost always working with the same team.
Demographic and Practice Characteristics of MAs and Physicians Surveyed.
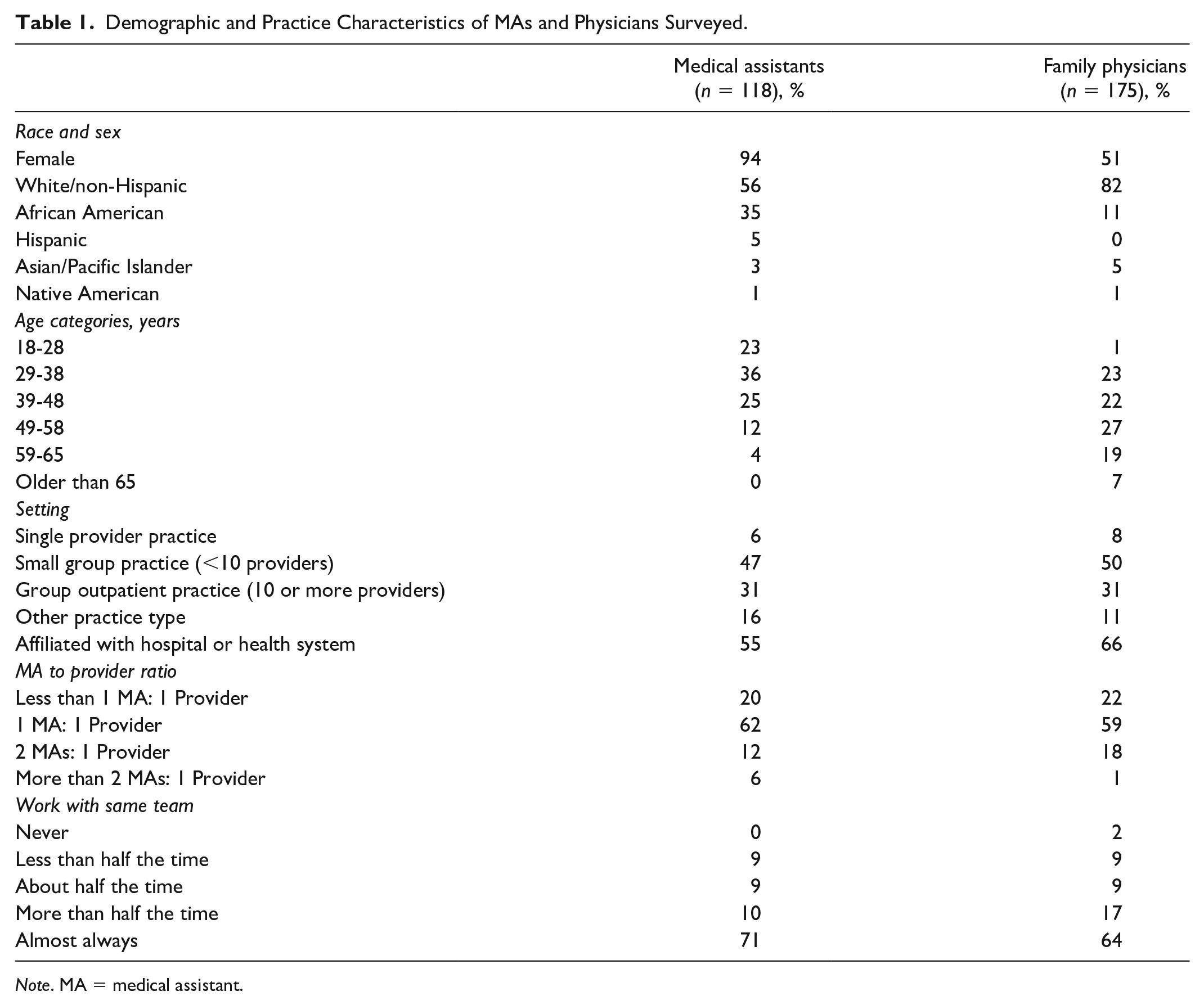
Note. MA = medical assistant.
Despite using a convenience sample to reach family physicians in North Carolina, survey respondents were generally representative of the demographic and practice characteristics of the 2,700 family physicians in practice in North Carolina in 2017. Data on actively practicing physicians in the state are drawn from the North Carolina Health Professions Data System which houses annual licensure data from the North Carolina Board of Medical Examiners. The data reflect a complete census of family physicians in active practice in the state. Survey respondents were more likely to be female and more diverse than the underlying population of family physicians in practice in the state. The age distribution of family physicians responding to the survey was generally representative, although respondents were more likely to be between 49 and 65 years of age and less likely to be older than 65 years. Survey respondents were in similar practice settings with 8% in a single provider practice and 81% in group practices compared with 10% and 78% of practicing family physicians in North Carolina, respectively.
While national data on the demographic, practice, and education characteristics of MAs are scant, a 2016 report suggests that MA survey respondents were generally representative of the national population (Skillman Dahal et al., 2016). Like their national counterparts, MA respondents were predominantly female, aged 29 to 48 years and had completed some college. Representing the state’s population demographics, NC MAs were more likely to be African American and less likely to be Hispanic than MAs nationally (Table 1).
MA Education and Certification
The majority (75%) of MAs surveyed were certified, with the highest percentage (46%) credentialed as Certified Medical Assistants by the American Association of Medical Assistants (Table 2). Consistent with data reported in the Washington survey (Skillman et al., 2018), nearly half of MAs surveyed had been working for 5 or fewer years and another 22% reported having worked as a MA for between 5 and 19 years. About half (52%) of the MAs reported they had trained in an associate degree program at a community college, 14% through vocational training, 12% through a certificate program, and 9% on-the-job. Fifty-nine percent of MAs reported that their job had undergone change since they started with their current organization.
Medical Assistant Practice, Certification, and Education Characteristics.
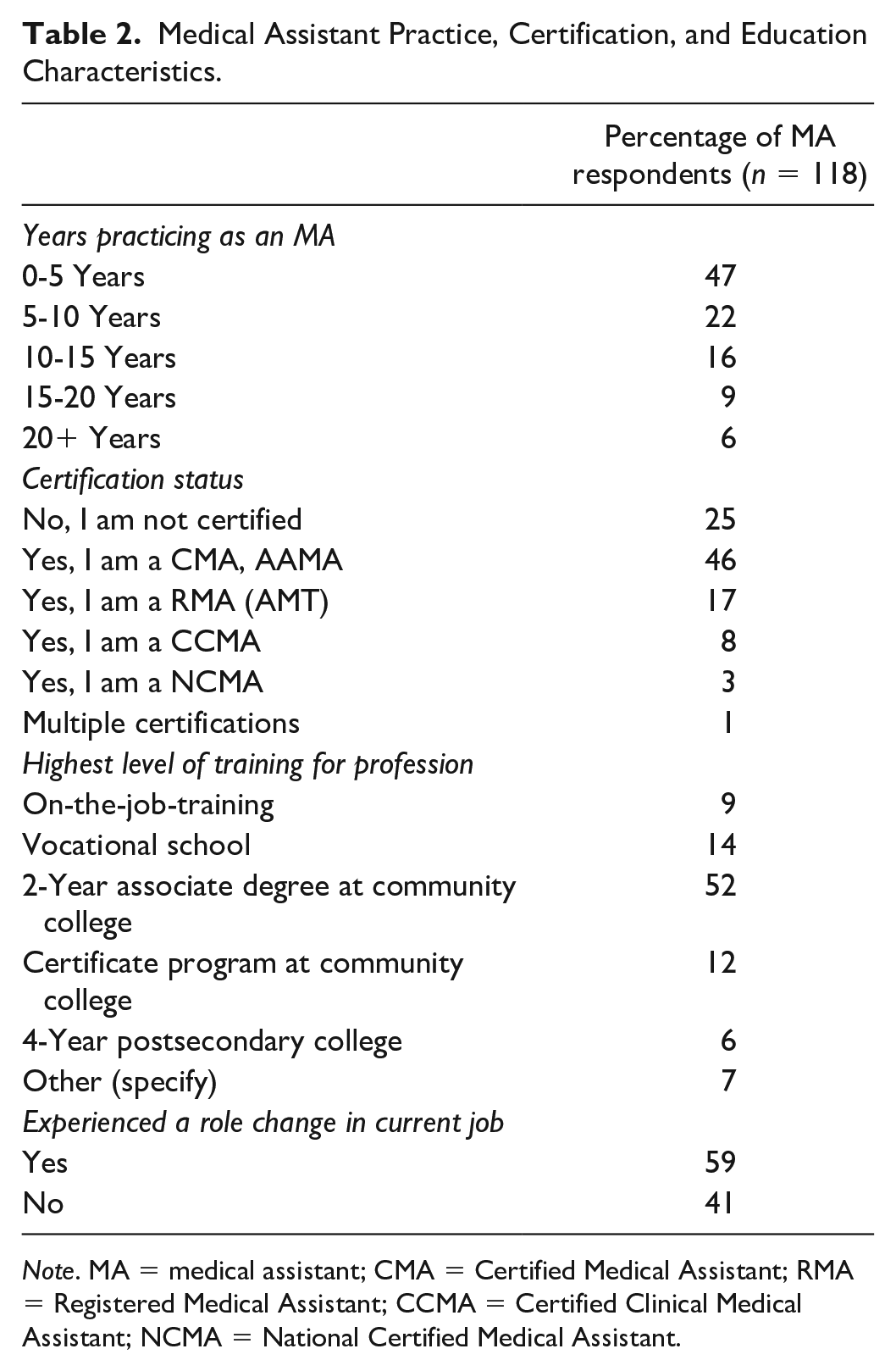
Note. MA = medical assistant; CMA = Certified Medical Assistant; RMA = Registered Medical Assistant; CCMA = Certified Clinical Medical Assistant; NCMA = National Certified Medical Assistant.
MA Roles
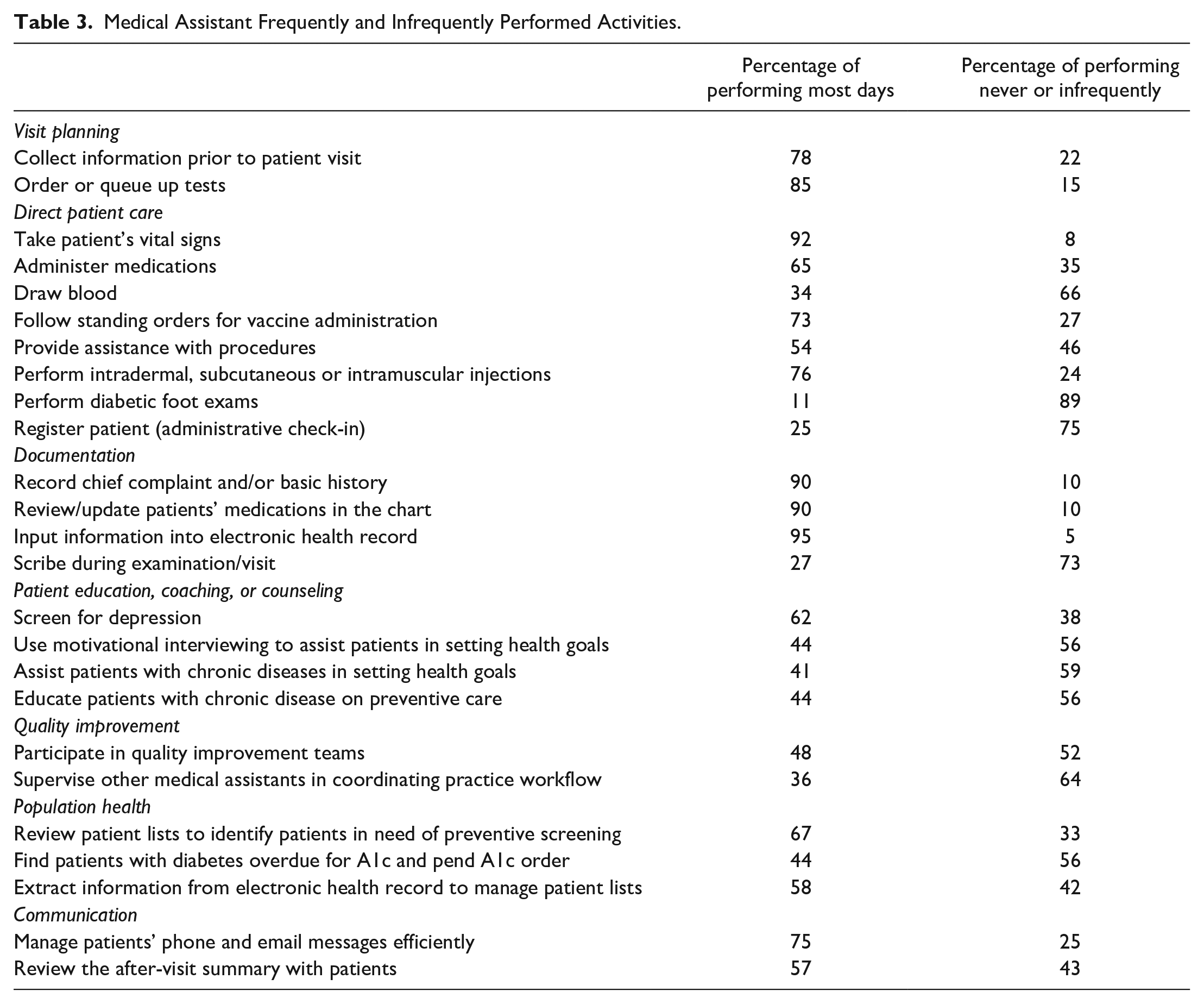
MAs performed most activities related to visit planning and direct patient care, documentation, and communication on most days (Table 3) and generally had high levels of confidence in tasks they reported performing frequently (data not tabled). MAs reported being engaged in some population health activities, particularly identifying patients for preventive screenings (67%) and extracting information from EHRs (58%), but less than half (44%) reported finding patients with diabetes who were overdue for A1c tests and pending the order. While 90% of MAs were engaged in documentation and 95% said they input information into the EHR, only 27% reported scribing. There was also variation in patient education, coaching, and counseling activities. Although 62% of MAs reported screening patients for depression, less than half (44%) reported using motivational interviewing (MI) to help patients set health goals, 41% assisted patients with chronic disease in setting goals, and 44% were engaged in educating patients with chronic disease about preventive care. They were less likely to be engaged in a “cross training rotation” (Chapman & Blash, 2017) with only 34% performing phlebotomy and 25% registering the patient. The least performed activity in our sample was diabetic foot exams with only 11% of MAs reporting they performed this activity.
Medical Assistant Frequently and Infrequently Performed Activities.
Divergence in MA and Physician Perceptions of Role and Confidence
MAs and physicians generally agreed on the tasks currently being performed by MAs, but they had diverging perceptions of MA roles on tasks related to patient education, coaching, and counseling except screening for depression (Table 4). Some of this divergence may be explained by the fact that physicians are often not in the room when MAs interact with patients so may not see the activities they are performing and the skill with which they are performing them. While 44% of MAs reported performing MI, only 13% of physicians said MAs in their practices currently perform MI. Forty-one percentage of MAs reported assisting patients with chronic diseases in setting goals compared with 18% of physicians who believe their MAs do this; 44% of MAs said they educated patients with chronic disease about preventive care while only 25% of physicians reported MAs took on this role. Similarly, a much higher percentage of MAs (57%) reported reviewing the after-visit summary with patients compared with physicians (32%).
MAs’ and Physicians’ Divergent Perceptions in Role and Confidence for Patient Education, Coaching, and Counseling.
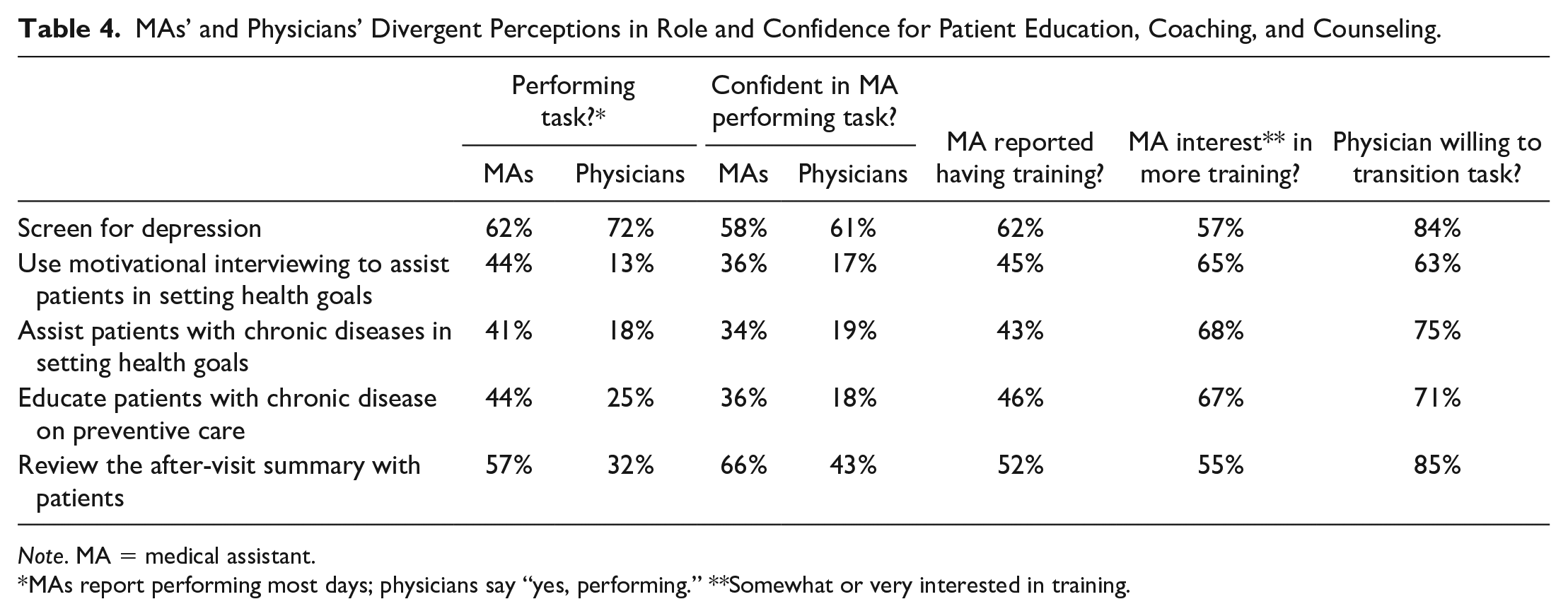
Note. MA = medical assistant.
MAs report performing most days; physicians say “yes, performing.” **Somewhat or very interested in training.
MAs were less confident in their ability to perform MI, goal setting and patient education than other activities reported in the survey, and physicians reported the lowest levels of confidence in MAs’ competence in the survey for these activities. However, the majority of physicians would be willing to transition these tasks to MAs not currently performing these activities in their practice if they received proper training and most MAs were somewhat or very interested in receiving more training.
Tasks in the survey that physicians indicated that they would be most willing to delegate to MAs that MAs are currently not performing in their practice were population health activities such as identifying patients in need of preventive screening (mammography, colorectal screening, etc.); finding patients with diabetes who are overdue for A1c tests and pending the order; and extracting data from the EHR to manage patient lists (Table 5). More than half of MAs reported either having prior training to perform these activities or being somewhat or very interested in receiving additional training.
Tasks Physicians Most Willing to Transition Were Population Health Activities.
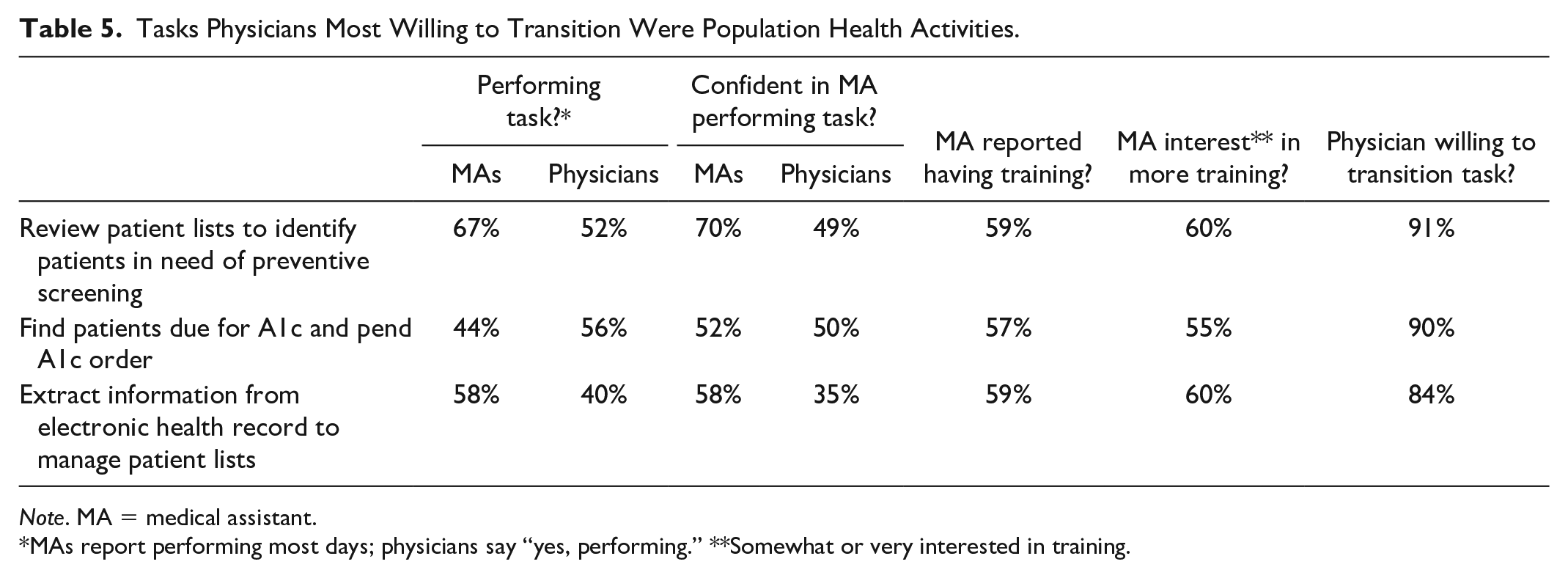
Note. MA = medical assistant.
MAs report performing most days; physicians say “yes, performing.” **Somewhat or very interested in training.
Physicians and MAs agreed on tasks that MAs perform least frequently (Table 6). Only 9% of physicians and 27% of MAs reported that MAs performed scribing. Thirty-nine percentage of MAs reported being confident to scribe, 31% reported previous training and 56% were somewhat or very interested in receiving more training in scribing. One quarter (25%) of physicians reported that MAs in their practices performed diabetic foot exams, but only 11% of MAs reported performing this activity. Fewer than one in four MAs (23%) felt confident doing foot exams, the lowest confidence level reported by MAs in the survey. Slightly over two thirds of physicians were willing to transition both tasks to MAs with training and the majority of MAs are willing to undertake training.
MA and Physician Agreement on Tasks Least Performed by MAs.
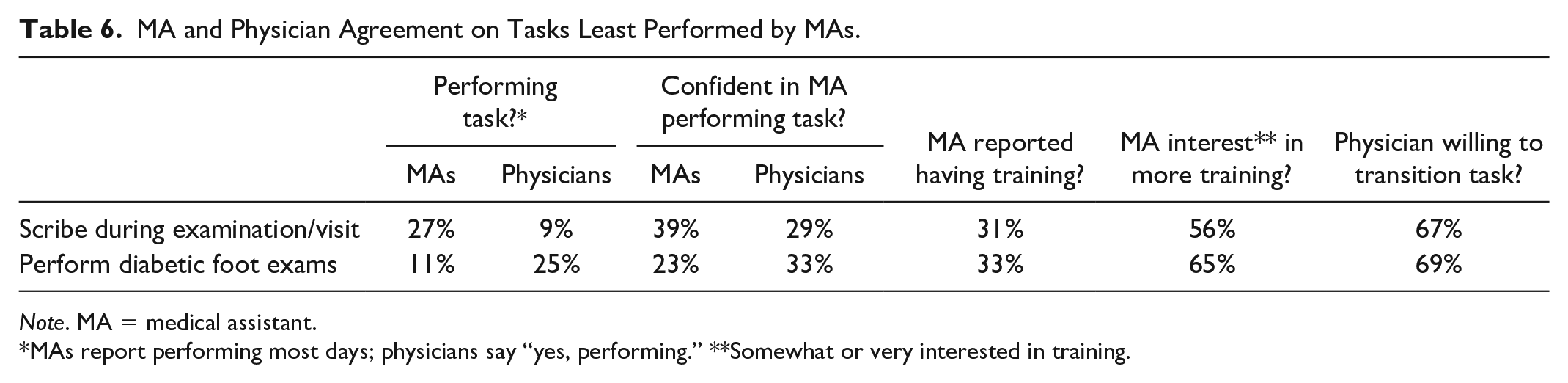
Note. MA = medical assistant.
MAs report performing most days; physicians say “yes, performing.” **Somewhat or very interested in training.
Discussion
The majority (59%) of MAs in our sample reported experiencing a role change since beginning their current position. Findings from this study suggest that many of the activities related to visit planning, direct patient care, and documentation that were once considered extended roles (Taché & Chapman, 2006) are now routinely performed by MAs on most days. For most activities, we did not find evidence of role confusion between MAs and physicians, physician resistance to delegate tasks to properly trained MAs, or MA reluctance to pursue training to take on new roles. However, we did identify three areas where the gap between the potential and actual implementation of MA role transformation could be narrowed—population health and panel management; patient education, coaching and counseling; and scribing. Closing these gaps will become even more important as our health care system moves toward value-based and risk-based payment models that emphasize addressing the upstream, preventive, and chronic care needs of patients.
Population Health
Our findings suggest that the activities physicians were most willing to transition to properly trained MAs relate to panel management, including identifying patients in need of preventive screening (mammography, colorectal screening, etc.); finding patients with diabetes who are overdue for A1c tests and pending the order; and extracting data from the EHR to manage patient lists. While physicians are interested in delegating these functions, an individual provider’s ability to do so is dependent on higher level administrative decisions about workforce policies that impact task delegation (Dill et al., 2019). For example, an MAs’ ability to take on panel management tasks depends on both staffing ratios and clinic scheduling. Most practices in our sample were operating in a 1:1 MA to provider ratio, but this would need to be increased to two or more MAs per provider to take on more population health tasks. Clinics operating in a fee-for-service model may be reluctant to take on this increased staffing cost, but models have shown that it can be offset by an increase of 2.5 visits per day per MA (Eden, 2016). To operationalize the kind of data extraction from the EHR needed for population health and risk stratification, the clinic would have to allow MAs to have protected administrative time, either in conjunction with, or separate from, the physicians with whom they work.
Patient Education, Coaching, and Counseling
While MAs and physicians generally agreed on the tasks currently being performed by MAs, the greatest divergence in perceived roles related to patient education, coaching, and counseling and these were activities for which MAs reported the lowest level of confidence on the survey. Physicians also reported low levels of confidence with MAs’ current level of training. These findings are not surprising, as sharing the health coaching role with MAs requires an even greater level of physician trust than panel management tasks (Ladden et al., 2013), yet the majority of physicians in our sample were willing to transition these tasks to MAs with proper training. These findings and other studies suggest that enhanced training is needed for MAs in foundational educational programs, and through continuing education programs to support the enhanced use of MAs as patient educators and health coaches (Naughton et al., 2013; Wagner et al., 2017).
Increased training in chronic disease management, MI, self-management, and patient education has the potential to narrow the gap between MAs’ current and potential use in population health roles and to increase physician confidence and willingness to delegate these tasks. About two thirds of MAs indicated an interest in pursuing additional training and over 70% of physicians indicated they were willing to transition these tasks to appropriately trained MAs.
Documentation and Scribing
Physicians and MAs were in strong agreement about MAs’ role in documentation. However, only 9% of physicians and 27% of MAs reported that MAs were scribing during the patient visit, which represents another gap that could be closed to enhance care and improve patient and provider satisfaction. Practices that deploy MAs as scribes have lower rates of physician burnout in part because it decreases the burden on physicians of completing patient notes “after hours” (Jerzak, 2016). Scribes’ notes for patients with diabetes have been shown to be more up-to-date, thorough, useful, and comprehensible for diabetic patients than when physicians wrote them alone (Misra-Hebert et al., 2016). Using MAs as scribes has also been associated with enhanced patient satisfaction because providers can devote more time to patients during the visit (Jerzak, 2016).
More than half of MAs (56%) in our sample indicated a willingness to pursue additional training for scribing and two thirds of physicians (67%) said that they would be willing to delegate scribing to an MA with proper training. While these results are promising, deploying MAs as scribes requires hiring additional staff, retraining existing staff, and redesigning workflows. The incremental costs incurred by using MAs as scribes may be offset by increased provider productivity, accuracy of clinical documentation and billing, as well as enhanced patient outcomes and satisfaction, measures which are increasingly important under value-based payment models (Campbell et al., 2012; Shultz & Holmstrom, 2015).
Successfully transitioning MAs into new roles—including population health management; patient education, coaching, and counseling; and scribing—hinges on having a physician leader to champion the proper utilization and retraining of MAs to meet evolving primary care practice needs (Chapman & Blash, 2017; Jerzak, 2019). Physician resistance to new MA roles due to concerns about their training has been identified as a key challenge to MA role expansion (Eden, 2016). Our findings suggest that the majority of physicians are willing to delegate tasks to MAs with proper training. This is important because physicians are key champions in MA role redesign, both within the practice and in making the business case for role expansion to higher level administrators. Physicians are more likely to gain confidence in, and champion, MAs’ expanded roles when they work in stable teams. Our findings suggest that they generally do work in stable teams with 71% of MAs and 64% of physicians reporting they almost always work with the same team.
Some physicians in our study were unwilling to delegate tasks even if the MA received additional training (data not tabled). Thirty-three percent of physicians said they would only be willing to delegate 5 or fewer of the 26 tasks in the survey even if MAs had additional training. These more “resistant” physicians were more likely to be male (p < .01) and aged 59 years and older (p < .01). Practice setting and health system affiliation were not associated with physician willingness to delegate.
Nearly half (47%) of the MAs in our study and the Washington study (46%) were in practice for fewer than 5 years which may contribute to providers’ lower confidence in MA training and ability to perform expanded roles in panel management and patient education, coaching, and counseling. Even when physicians and MAs consistently work on the same team, physicians and administrators who set workforce policy for the practice may need education about allowable MA scope of practice. Lack of clarity on MA scope of practice regulations can lead to situations where the practice puts more stringent restrictions on MA practice than state regulations, particularly for standing protocols and injections (Chapman & Blash, 2017).
Our convenience sampling methodology may have introduced selection bias into our study. Family physician respondents were younger than the underlying population of physicians in North Carolina. Their younger age, combined with the fact that the survey was administered electronically, may have biased respondents toward more innovative physicians likely to deploy MAs in new roles in practice. Data on the percentage of the MA workforce nationally that is certified is difficult to obtain but, in our sample, 75% of MAs reported being certified. Higher certification rates in our sample may cause the study to overestimate the amount of training MAs have, their willingness to take on new trainings and their confidence in their skills compared with the true population. The MAs in our sample may also have had higher career aspirations since 47% reported that they had plans to pursue additional education for a different health profession in the future.
Conclusions
There were nearly 674,000 MAs in practice in the United States in 2018 and 76% (516,030) were employed in ambulatory care (Bureau of Labor Statistics, 2019). As payment models continue to drive care to outpatient settings and emphasize population health and panel management strategies, MA roles will continue to expand. Efforts to assure this workforce is “fit for purpose” need to focus both on the baseline competencies MAs acquire through training before they are hired (Dill et al., 2019) and on retooling the 674,000 MAs already employed in the health care system.
This study focused on the MA–physician dyad, but team composition in primary care is diverse. Jabbarpour et al. found that in 2018, 56% of family physicians reported working with nurse practitioners (NPs), 54% with registered nurses (RNs), and 43% with physician assistants (PAs; Jabbarpour et al., 2020). The most surprising finding was the growing percentage of family physicians who reported working with licensed practical nurses (LPNs) which increased from 34.5% in 2014 to 49.3% in 2018. Given the potential overlap in functions between MAs and LPNs in primary care, these data suggest that some primary care practices may be employing LPNs to take on many of the functions MAs also perform. This raises a question for future research about whether patterns of task delegation to MAs and LPNs differ and, if they do, why these differences exist.
Previous work suggests that primary care staffing is not the result of an explicit plan, but evolves from macro-level forces such as payment and regulatory policy, organizational-level decisions about roles and workflow and individual preferences (Leach et al., 2017). In our current fee-for-service environment, studies of task delegation have often focused on the roles of physicians in relation to other staff, but as payment models shift, we will need to investigate the roles of the growing number of other health professionals found in value-based payment models. For example, as integrated primary care and behavioral health care delivery models expand, more evidence will be needed on task delegation between social workers and other team members, especially RNs whose roles in care coordination, care management, patient education, and managing patients’ social care needs often overlap. An example of this type of research, conducted by Donelan et al. (2019), investigated RN and social worker roles in caring for frail elderly in primary care and geriatrics practices. The authors found that when social workers and RNs worked in the same practice, social workers were more likely than RNs to participate in social needs assessment and RNs were more likely than social workers to participate in care coordination. Future workforce research needs to emulate these types of analyses that move beyond enumerating the supply of different types of providers to understanding the evolving and dynamic roles of health professionals on health care teams. One immediate opportunity is investigating how the roles of MAs, RNs, social workers, physicians, and other providers have changed with the sweeping changes to telehealth. Such evidence is needed to support decision making about the sustainability of telehealth provisions that expand the types of providers and settings that can bill for telehealth.
Supplemental Material
sj-pdf-1-mcr-10.1177_1077558720966148 – Supplemental material for The Evolving Role of Medical Assistants in Primary Care Practice: Divergent and Concordant Perspectives from MAs and Family Physicians
Supplemental material, sj-pdf-1-mcr-10.1177_1077558720966148 for The Evolving Role of Medical Assistants in Primary Care Practice: Divergent and Concordant Perspectives from MAs and Family Physicians by Erin P. Fraher, Allison Cummings and Dana Neutze in Medical Care Research and Review
Supplemental Material
sj-pdf-2-mcr-10.1177_1077558720966148 – Supplemental material for The Evolving Role of Medical Assistants in Primary Care Practice: Divergent and Concordant Perspectives from MAs and Family Physicians
Supplemental material, sj-pdf-2-mcr-10.1177_1077558720966148 for The Evolving Role of Medical Assistants in Primary Care Practice: Divergent and Concordant Perspectives from MAs and Family Physicians by Erin P. Fraher, Allison Cummings and Dana Neutze in Medical Care Research and Review
Footnotes
Authors’ Note
Dr. Cummings was a medical student conducting research in the Carolina Health Workforce Research Center at the time this work was conducted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Bureau of Health Workforce (BHW), National Center for Health Workforce Analysis (NCHWA), Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $450,000, with zero percent financed with nongovernmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by HRSA, HHS, or the U.S. Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.