
Abstract
Cross-sector collaboration is critical to improving population health, but data on partnership activities by children’s hospitals are limited, and there is a need to identify service delivery gaps for families. The aim of this study is to use public community benefit reports for all children’s hospitals in the United States to assess the extent to which children’s hospitals partner with external organizations to address five key health needs: health care access, chronic disease, social needs, mental health, and substance abuse. Strategies that involved partnering with community organizations were most common in addressing social needs and substance abuse. When adjusted for institutional and community characteristics hospitals in a multilevel regression model, hospitals had higher odds of partnering to address chronic illness and social needs. To encourage hospital engagement with complex social and behavioral health needs and promote health equity, support should be provided to help hospitals establish local population health networks.
Introduction
Cross-sector collaboration is critical to improving population health, reducing health disparities and preventable death, and improving the quality of health care services (Hogg & Varda, 2016; Mays et al., 2016). Strengthening these types of partnerships is a priority for many funding and advocacy organizations, including the Robert Wood Johnson Foundation, which lists it as one of the four priority areas in their Action Framework to build a Culture of Health in the United States (Trujillo & Plough, 2016). The goal of increasing this type of collaboration is to connect health care systems with organizations that address broader social and economic factors influencing health and well-being, resulting in more effective population health interventions.
The 2010 Patient Protection and Affordable Care Act (ACA) encouraged partnerships between nonprofit hospitals and community organizations by requiring hospitals to do community benefit reporting to the Internal Revenue Service (IRS; James, 2016; Rosenbaum et al., 2016). As a result, hospitals have become more interested in developing cross-sector partnerships in areas where they could collaborate with other organizations to improve local population health (Rosenbaum, 2016). Specifically, hospitals must perform a community health needs assessment (CHNA) every 3 years and develop implementation strategies for their programs, either independently or through partnerships, to address high-priority local health needs. The community benefit reporting requirements thus create a unique opportunity for researchers to examine the decisions and types of cross-sector partnerships in which hospitals are engaging to address the critical health needs in their communities.
Most studies to date on cross-sector partnerships between hospitals and community organizations have focused primarily on adult-serving hospitals; research on pediatric health care organizations remains limited (Henize et al., 2015). There are case studies of children’s hospitals engaging in upstream social determinants of health, which describe efforts to address housing, food access, environmental quality, and unemployment, but studies with more representative samples are needed (Franz et al., 2018; Kelleher et al., 2018; Sommer et al., 2011; Weier et al., 2017). As a field, pediatrics has historically embraced the idea of partnerships with families and various health and social agencies that are involved in the care of children (Sia et al., 2004). Children’s hospitals also have different characteristics when compared to adult-serving hospitals, such as being mostly located in major metropolitan areas and less in rural areas (Casimir, 2019; Franz & Cronin, 2020). The ways in which children’s hospitals engage in cross-sector partnerships are therefore likely to differ systematically from adult-serving hospitals.
New Contributions
Because children’s hospitals serve unique communities across the country, we assess the likelihood of adopting cross-sector partnerships with a national sample of children’s hospitals in the United States to address the five most commonly identified health needs from their IRS-mandated CHNAs: health care access, chronic disease, social needs, mental health, and substance abuse. We expect this study to contribute to our existing knowledge and practice on hospital–community collaborations and population health interventions in three ways. First, the study broadens our understanding of cross-sector partnerships between hospitals and community organizations to include the actions of children’s hospitals. Second, there is a clear need to identify the service delivery gaps that require more attention and robust public health partnerships, as the needs of families and their children are both vast and relatively heterogenous (Henize et al., 2015). Third, improvements to the social environments of children and families via cross-sector partnerships are also likely to have an outsized impact on reducing health disparities (Braveman & Barclay, 2009).
Conceptual Framework and Research Aims
In line with the ACA’s community benefit regulations, children’s hospitals must identify and respond to a range of health needs that exist in their surrounding communities. These health needs represent the key areas that hospitals may then choose to address by partnering in different ways with other organizations in their communities. Noh et al. (2016) found a pattern of hospital partnership behaviors with regard to whether they tend to adopt partnerships (a) inside the medical sector, (b) outside the medical sector, (c) both in and outside the medical sector, or (d) having no partnerships (i.e., being independent) when addressing population health). Building on this framework, we explore whether the nature of the health needs addressed increases the likelihood of adopting population health partnerships among children’s hospitals. This is important because although some health needs may align with services traditionally provided by hospitals, such as improving health care access and managing chronic disease, needs related to social or behavioral health may extend beyond traditional acute health care services. In these cases, partnerships may be particularly critical to helping hospitals move upstream and address the social determinants of health.
Most previous community benefit studies have focused on adult-serving hospitals, but there are likely similarities in how children’s hospitals utilize partnerships to address health needs in their surrounding communities. Existing studies, for example, suggest that hospitals have faced tremendous challenges in developing community-based partnerships after the ACA expanded community benefit requirements (Beatty et al., 2015; Pennel et al., 2015). There is some evidence, however, that these partnerships are beneficial in terms of improving the quality of CHNAs and implementation strategies (Pennel et al., 2015). A number of studies also suggest that adult-serving hospitals are less likely to address complicated health needs that extend beyond the provision of charity care in the hospital, such as the social determinants of health which underlie many chronic illnesses (Begun & Potthoff, 2017; Cramer et al., 2017; Franz, Cronin, et al., 2019; Franz, Skinner, et al., 2019; Singh et al., 2018; Young et al., 2018). Given evidence that external partnerships may help adult-serving hospitals address nonmedical or social needs, it is plausible that external partnerships may be more common when children’s hospitals are addressing specific types of needs, specifically those that transcend the provision of health care services. In this study, accordingly, we assess whether the type of need addressed by children’s hospitals is a key predictor of decisions to collaborate with an external, community-based partner.
Method
Sample
To construct our data set of hospital partnerships, we merged several sources of data on the strategies that hospitals have designed to address community health needs, organizational characteristics, and information on the surrounding county. We performed our analysis on all children’s hospital members of the Children’s Hospital Association (n = 234), which represents the vast majority of children’s hospitals in the United States (Casimir, 2019). We downloaded CHNAs and implementation strategies from the websites of each hospital; if these documents were not publicly available on hospital websites, we emailed and/or called the designated contact to request a copy of the reports. Hospitals with which we were unable to establish contact were excluded from the sample. After excluding hospitals with missing information, the total sample was 2,961 hospital strategies from 154 hospitals.
We examined the characteristics of our sample hospitals after dropping missing data to see if it was comparable to the entire universe of hospitals. For bed size, our hospitals were representative of the overall hospital population. Our sample did have a slightly higher percentage of freestanding hospitals, however. Freestanding hospitals can be part of systems, but are self-contained hospital organizations and not simply pediatric units located within a parent hospital. When conducting a t test between our sample and the hospitals with missing information, this difference was statistically significant suggesting that nonfreestanding hospitals may be less likely to make their community benefit documents publicly available.
Hospitals must complete regular community benefit reporting including annual financial reports on IRS Form 990 and Schedule H as well as complete CHNAs and implementation strategies every 3 years. Hospitals are required by tax law to make CHNA reports public, such as by posting them on their website, but not all hospitals are in compliance with this requirement. Because of the 3-year cycle, and the fact that hospitals had the option of starting this process for the first time in either 2012 or 2013, the most recent CHNAs and implementation strategies at the time that our data set was built ranged from 2015 to 2018. Data collection and coding of all CHNAs and implementation strategies occurred between 2018 and 2019.
Data on organizational characteristics were obtained from the 2015 American Hospital Association Annual Survey and 2015 Children’s Hospital Association Population Health Survey (American Hospital Association, 2015; Children’s Hospital Association, 2015). To assess community characteristics, we included the county in which each hospital is located. Data on county health characteristics came from the 2015 County Health Rankings database and the Centers for Disease Control and Prevention’s National Vital Statistics System (Centers for Disease Control and Prevention National Center for Health Statistics, n.d.; University of Wisconsin Population Health Institute, 2019). Additional community and county characteristics were sourced from the Area Health Resource File with data from 2015 (Health Resources & Services Administration, 2015) and the Northeast Regional Center for Rural Development’s Social Capital Variables for 2014 (Northeast Regional Center for Rural Development at Penn State University, n.d.; Rupasingha et al., 2006).
Coding
Two of the authors reviewed and coded each CHNA for the hospital’s list of prioritized community health needs and the corresponding implementation plan for whether a prioritized need was addressed with a specific program. CHNAs and implementation plans generally share a common structure, making it straightforward to identify the prioritized community health needs and accompanying implementation strategies to address them. In situations where the health needs and programs were not clear, we met as a research team to review the documents and collaboratively code them. In addition, we selected 10 CHNAs to code independently to ensure reliability. There was 100% agreement after coding documents independently. After coding the prioritized community health needs for all hospitals, we determined the five most commonly identified health needs in the community benefit reports to be health care access, chronic disease, social needs, mental health, and substance abuse. We then catalogued all hospitals’ implementation strategies to address each of these community health needs and created a dichotomous variable for whether hospitals undertook their strategies alone or mentioned a partnership with an outside community organization. Because hospitals have to demonstrate whether they address each identified need, we included all proposed strategies that hospitals presented in response to each need. Although proposed strategies were often multifaceted and addressed multiple needs, we catalogued strategies according to the primary need they addressed as defined by the hospital in their implementation strategy.
Measures
Our dependent variable is whether a hospital partnered with a community organization when implementing a strategy. Our unit of analysis is each individual strategy, nested within its hospital organization, which is in turn nested in a county. Our focal independent variables are whether each strategy addressed one of the four community health needs (chronic illness, mental health, substance abuse, and social needs) with health care access as the reference. We controlled for hospital size (measured by number of pediatric beds) and structure (free-standing as compared with hospitals that are colocated within adult hospitals; membership in a hospital system). We also included county-level demographic characteristics (mean income in the county with counties sorted into quintiles, the age-adjusted premature death rate, and the number of membership organizations per 10,000 residents as a measure of social connectedness). We selected this set of control variables based on prior conceptual work suggesting a relationship between community-level demographics and institutional investments to improve population health.(Franz, Cronin, et al., 2019) We also accounted for the number of nonprofit organizations per 1,000 residents in the county to control for a hospital’s partnership opportunities.
Analytic Strategy
To assess the relationship between hospital characteristics, county, state, and regional factors, and decisions to partner on addressing community health needs, we employed descriptive statistics to understand the percentage of hospitals partnering to address each need. We then performed multilevel logistic regression to understand the association between the multiple factors just described and hospital decisions to partner on each program. The multilevel logistic regression analysis included random effects to account for the nested structure of the data (i.e., strategies were nested within hospitals). Hospitals have multiple strategies but strategies within hospitals are likely to be more similar to each other than strategies across hospitals. Adjusted odds ratios (ORs) were used to report findings on the relationship between partnerships, specific health needs, organizational, and county-level characteristics. All statistical analyses were conducted using Stata 16.1 (StataCorp, 2020).
Results
The nature of the identified community health need was related to a children’s hospital’s decision to partner with a community organization. Descriptive statistics for the sample of children’s hospitals show us that hospitals have created numerous implementation strategies related to the five community health needs of interest. Of the 154 children’s hospitals in the analytic sample, there were 2,961 strategies to address the five community health needs. The average number of strategies per hospital was 19. More than half (62.07%) of the total 2,961 strategies indicated some form of community partnership outside of the organization (Table 1).
Descriptive Statistics of the Sample.
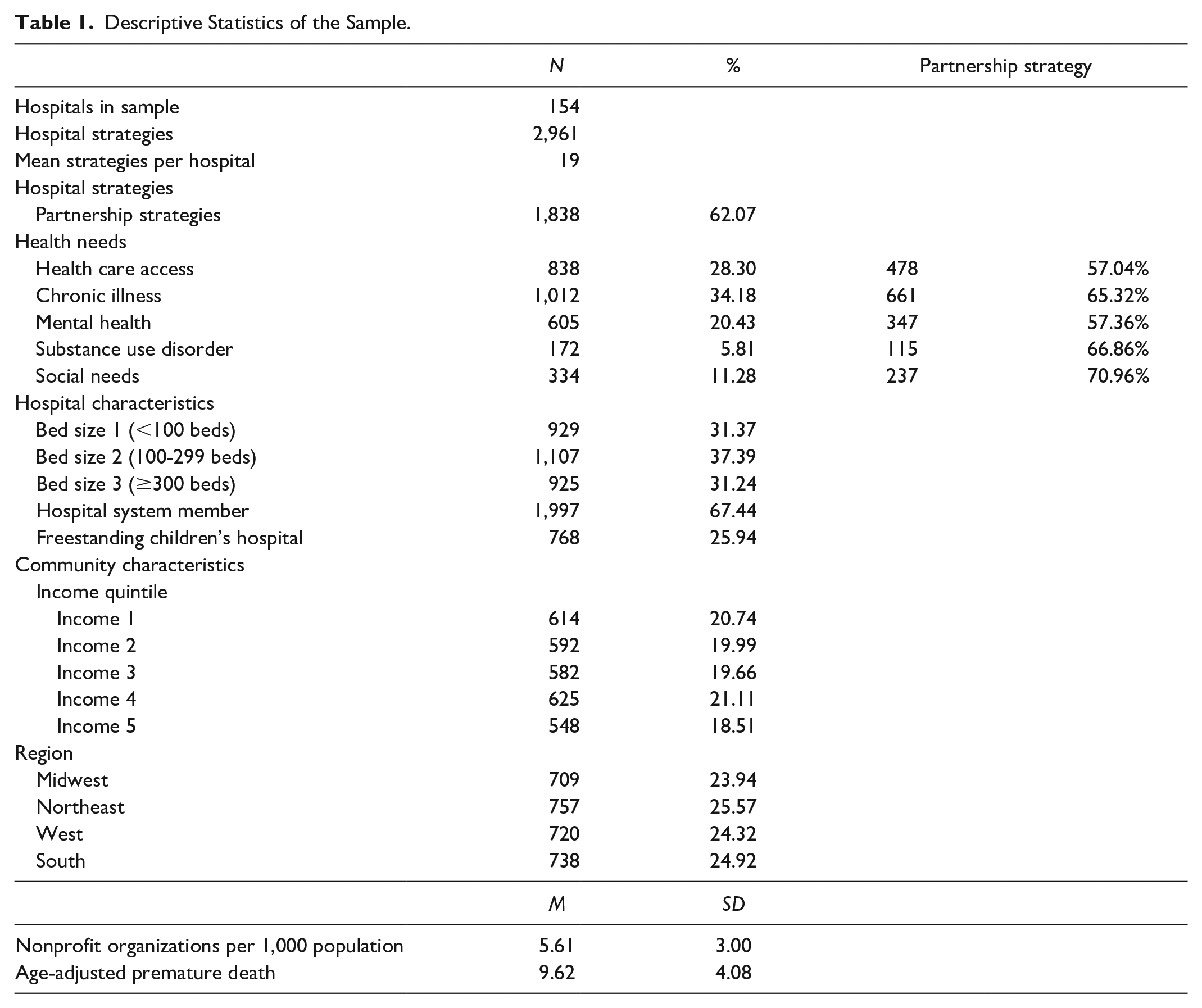
Because hospitals are not required to address all identified community health needs, we also assessed the extent to which hospitals developed strategies to address each type of need that was prioritized in their CHNA. Chronic illness was the most likely to have an implementation strategy associated with it (34.18%), followed by health care access (28.30%), mental health (20.43%), and social needs (11.28%). The health need that was least likely to be addressed by hospitals was substance use (5.81%). Among these strategies, hospitals most often indicated partnering in plans to address social needs (70.96%) and substance use (66.86%; Figure 1).
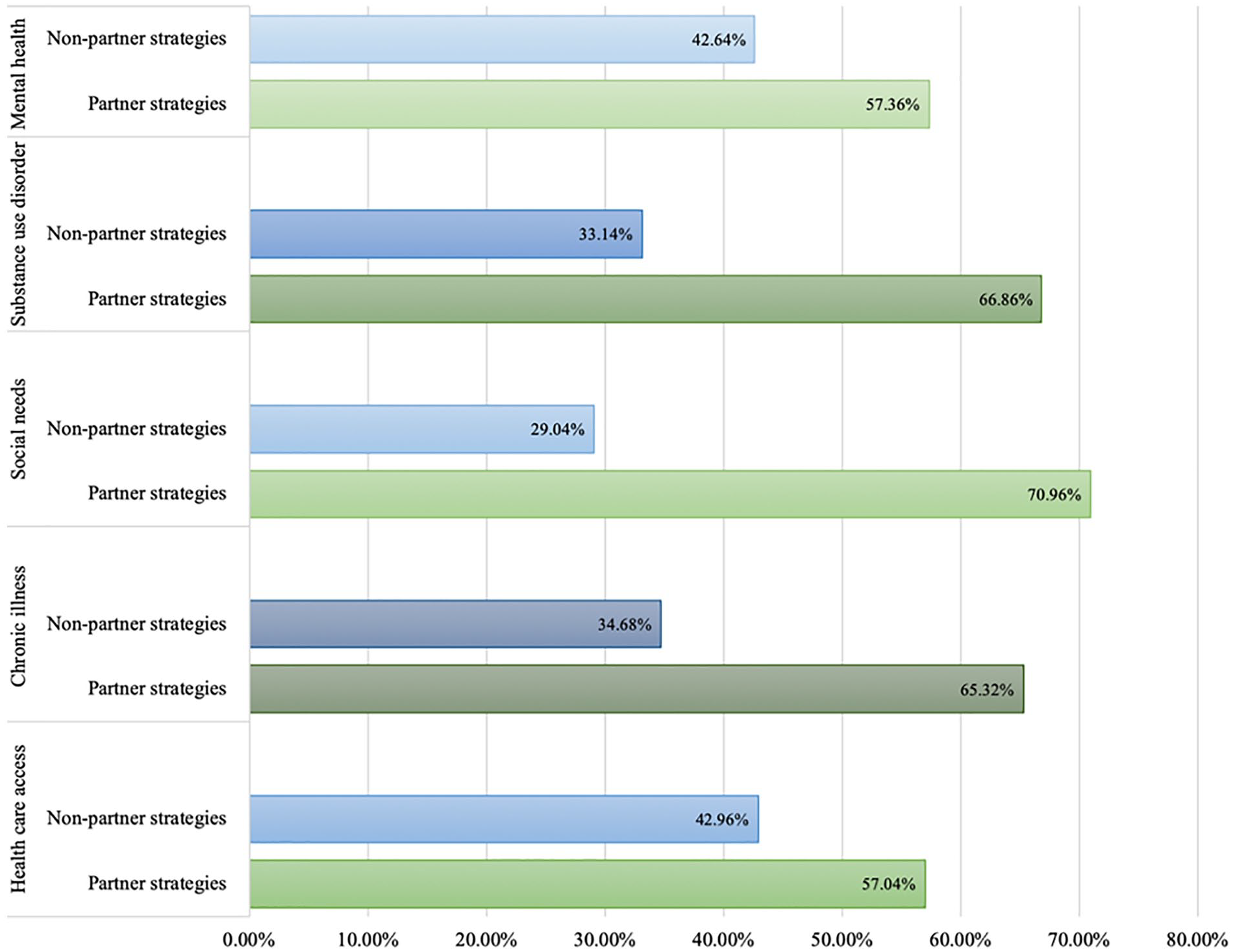
Partnering decisions by strategy type.
Table 2 reports the results from the multilevel logistic regression analysis of implementation strategies used by children’s hospitals to partner with community organizations. The multilevel logistic regression analysis indicates that when hospitals had strategies addressing social needs (as compared with health care access needs), a partnership arrangement was more likely to be used in the implementation strategy (OR = 1.77, 95% confidence interval [CI] = 1.25-2.51). Strategies addressing chronic illness similarly had higher odds of partnering with a community organization than children’s hospitals that identified needs related to health care access (OR = 1.43, 95% CI [1.13, 1.82]). Strategies carried out by Children’s hospitals in the West were more likely to partner with community organizations in their implementation strategies than children’s hospitals located in the South (OR = 2.03, 95% CI [1.08, 3.83]). Hospital characteristics, county, and state factors were not associated with the likelihood that strategies would involve a partnership approach. Table 3 contains a list of partnership strategies across the five community health needs.
Multilevel Logistic Regression of Partnering on Strategies.
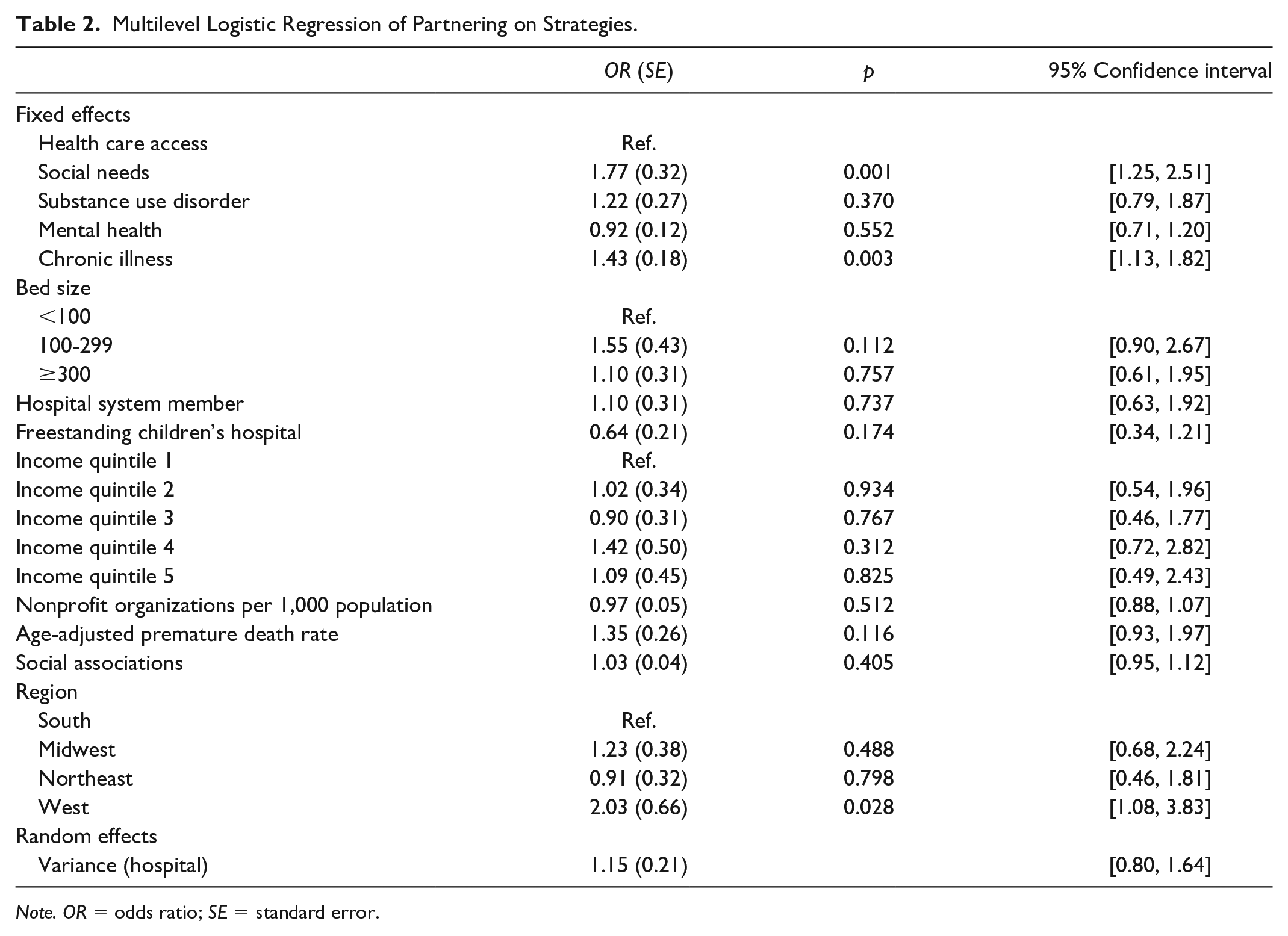
Note. OR = odds ratio; SE = standard error.
Examples of Partnership Strategies That Address the Most Common Health Needs.
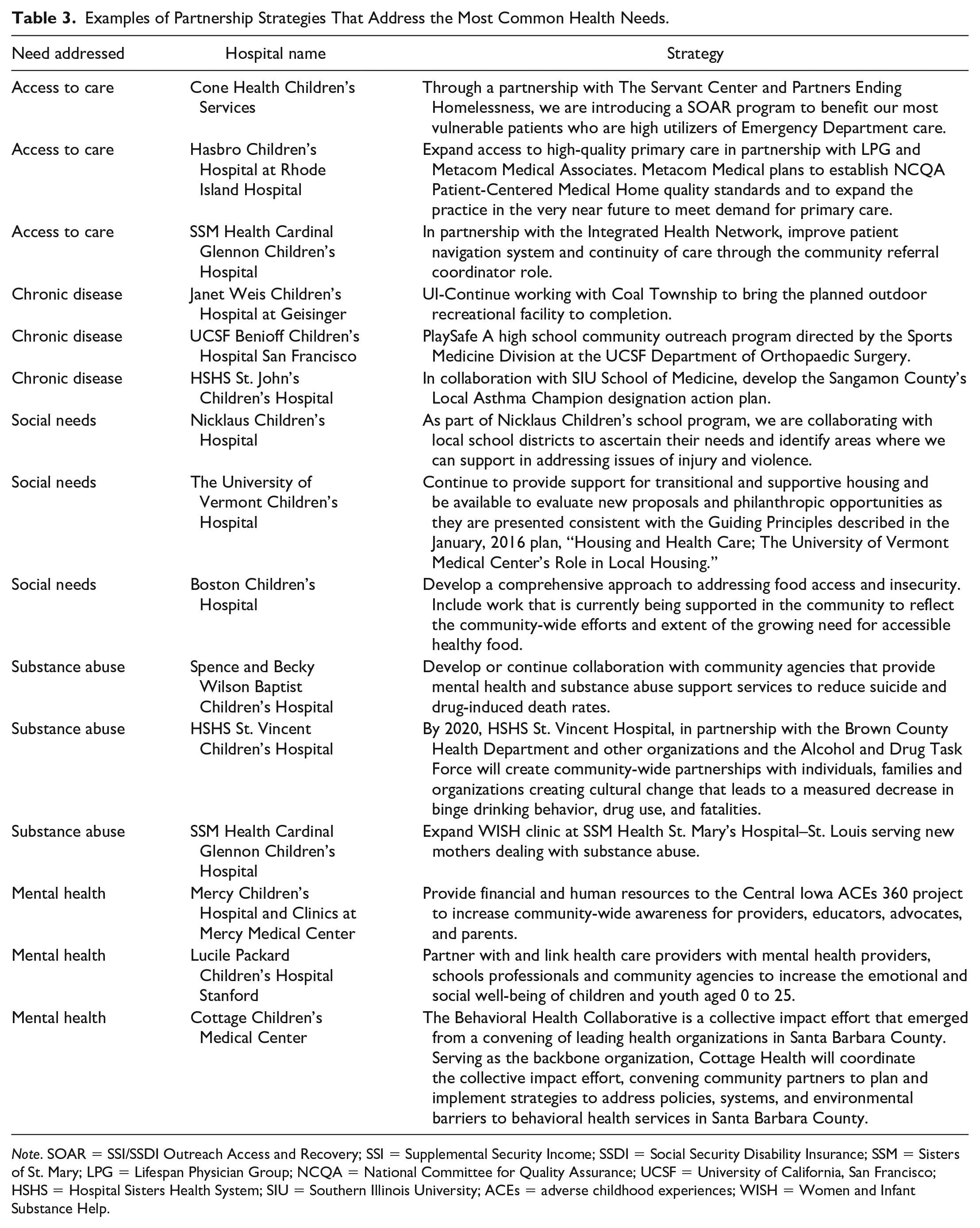
Note. SOAR = SSI/SSDI Outreach Access and Recovery; SSI = Supplemental Security Income; SSDI = Social Security Disability Insurance; SSM = Sisters of St. Mary; LPG = Lifespan Physician Group; NCQA = National Committee for Quality Assurance; UCSF = University of California, San Francisco; HSHS = Hospital Sisters Health System; SIU = Southern Illinois University; ACEs = adverse childhood experiences; WISH = Women and Infant Substance Help.
Discussion
Our results show that children’s hospitals in the United States are proposing to implement a large number of strategies to address their prioritized community health needs. Children’s hospitals had 19 strategies, on average, to address one or more of the five identified health needs, which correspond to a significant number of initiatives related to community health. Descriptive analyses showed that the most common implementation strategies were in response to chronic illness and health care access which aligns with existing evidence on adult-serving hospitals suggesting that most hospitals are not moving beyond the provision of traditional health care services in meeting community benefit requirements (Cramer et al., 2017; Young et al., 2018). Strategies that proposed partnering with community organizations were most common in addressing social needs and substance abuse. When adjusted for institutional, community, and regional characteristics, strategies were more likely to involve community partnerships when they addressed chronic illness and the social environment when compared with health care access. Taken together, these findings suggest that partnerships may be particularly critical when hospitals adopt strategies to address social and behavioral health needs. Building on our conceptual framework, we find that not only institutional characteristics, but the type of needs addressed are associated with decisions to partner with outside organizations. Our findings, in other words, extend the contextual factors that may shape partnering decisions and suggest that expanded public health partnership networks may provide additional support for hospitals to take on community benefit activities that expand beyond clinical care.
Children’s hospitals may be inclined to seek partnership support for social needs in particular given that social factors are typically beyond the scope of hospital services. In these cases, it is likely that children’s hospitals may gain value from the added expertise of social service agencies and community-based organizations. In terms of chronic illness, hospitals may seek external collaborations with public health departments or other agencies that foster health promotion and preventive efforts, although the nature of partnerships is not specified in the study data.
An important finding is that nearly two thirds of hospital strategies proposed partnering with some type of community organization. This number is encouraging given the promise shown by cross-sector public health networks, especially in underserved communities (Mays et al., 2016; Pennel et al., 2015). Partnering with outside organization may additionally bring more resources to that activity which may increase the likelihood of addressing health needs that historically have been underfunded. Coalition-building may also promote knowledge sharing on how to solve complicated health and social problems, especially when they are outside of hospitals’ traditional expertise.
One concern based on these study findings, however, is that some strategies that hospitals are likely to partner on, such as social needs, are not as commonly addressed in the implementation plans of hospitals. This suggests both that community partnerships are critical to the success of children’s hospitals in addressing these health needs and that hospitals may hesitate to commit to addressing these health needs at all, given the necessity to include external expertise to implement new programs. To encourage hospital engagement with complex social and behavioral health needs specifically, more support should be provided for establishing strong community public health networks where partners can be easily identified and leveraged.
Limitations
Our study findings are limited by the nature of the data extracted from the community benefit documents from children’s hospitals. It is unclear whether the hospitals in our sample have comprehensively included all activities related to their top five health needs in these documents. It is therefore possible that additional strategies related to each need are not captured in our data. In addition, our data do not contain specific information on the nature of partnerships developed by children’s hospitals, only whether they are involved some type of external partnership. Future research should specifically consider the types of organizations partnering with hospitals, and whether these relationships help hospitals adopt and implement evidence-based programs effectively. It is also possible that hospitals choose to identify community health needs based on existing partnerships rather than the nature of needs influencing the development of new partnerships. Given the cross-sectional design of our study, we are unable to determine the causal nature of this relationship. Finally, given that community benefit reports include only the strategies that hospitals project to occur in the future, there were no data on the effectiveness of these programs. Future studies should specifically assess the extent to which hospitals are adopting evidence-based strategies and whether partnerships help hospitals implement interventions effectively.
Public Health Implications
Many strategies adopted by children’s hospitals to address community health needs involve partnerships, but these hospitals are still less likely to address complicated health needs, potentially because it may require additional work to identify and establish relationships with external partners. Partnerships may help hospitals leverage additional resources and share knowledge on complex health issues, but initiating these relationships may be time intensive. Strong public health networks may increase the likelihood that partnerships can be leveraged to address critical local health needs. Amended community benefit guidance from the IRS could also require hospitals to partner on programs to address critical health needs and offer support and incentives for hospitals to partner with community organizations to address complex health needs, such as those related to substance abuse and the social environment.
Footnotes
Acknowledgements
We wish to acknowledge the Children’s Hospital Association for sharing institutional characteristics of member hospitals, and Haley Appelmann and Casey Hall-Jones for their assistance constructing the data set. We also wish to acknowledge the Honors Tutorial College at Ohio University for supporting three summer research assistantships related to hospital population health programs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.