
Abstract
One reason that nursing homes are a primary source of COVID-19 infections and deaths in the United States may be that workers hold multiple jobs. We use 2010-2019 Current Population Survey data to document the rate of second jobholding among nursing and long-term care workers. On average, 6.41% of personal care and nursing aides and 6.23% of licensed practical nurses and registered nurses hold second jobs; second job holding rates are 35% and 32% higher than those of other workers, respectively. Both wages and hours in the primary job are negatively associated with the probability of holding a second job for personal care and nursing aides, while lower hours are more strongly correlated with a second job for registered nurses and licensed practical nurses. Many of these workers move across health settings from their first to second jobs, and 15% of second jobs for personal care and nursing aides are in other “essential” occupations.
Introduction
As cases of COVID-19 approach 7 million and deaths surpass 200,000 in the United States, it is becoming clear that nursing homes account for a large fraction of morbidity and mortality. A number of particularly severe cases have received attention in news media (Ivory et al., 2020; Tully, 2020), but the problem is widespread. As of August 13, 2020, nationwide, 8% of cases and 41% of deaths were linked to nursing homes, and in 20 states, at least half of all COVID-19 deaths have been linked to nursing homes. 1 To put that into context, nursing home patients represent less than a half a percent of the U.S. population and approximately 3% of the over-65 population. 2 Infections among staff are also important. For example, in New Jersey, as of July 6, 2020, a total of 12,385 workers in these facilities had confirmed cases of COVID-19, and this represented 7.1% of infections in the state. 3 Although workers have a much lower death rate, they are clearly a vulnerable group and one that has the potential to transmit the disease within and across facilities. And, in fact, a recent report by the New York State Department of Health (2020) identified staff transmission as a primary source of outbreaks in nursing homes.
In this study, we examine second job holding among workers employed in long-term care settings. Our sample consists of registered nurses (RNs), licensed practical nurses (LPNs), 4 certified nursing assistants (CNAs), and personal and home care aides (hereafter, the latter two groups are collectively referred to as direct care workers). These occupation groups are chosen because all of the workers can work in long-term care settings, and all but personal and home care aides can work in hospitals; this introduces the possibility for worker-based transmission of COVID-19 both from health facilities to long-term care settings, as well as between different long-term care settings.
There are several reasons why workers in these occupations, particularly the direct care workers, are important in the context of the spread of COVID-19 in nursing homes. First, the workers who provide the majority of hours of care to nursing home patients are CNAs, who perform physically and often emotionally intensive work for low wages. They are considered to be a part of the direct care workforce because their job is to provide personal care to patients via tasks such as bathing, feeding, and using the bathroom, rather than medical tasks such as administering medication. This regularly puts them in extremely close proximity to patients, and reports suggest that nursing home staff have had even less access to personal protective equipment (PPE) than hospital staff (Rau, 2020; Whoriskey et al., 2020).
Second, U.S. nursing homes themselves are generally poorly set up to contain the spread of contagious disease. Some of the reasons are outside the control of any nursing home director, including the number of extremely frail and at-risk individuals confined to a relatively small space. But other factors are not inherent to design of the facilities—or specific to the COVID-19 pandemic. A common, persistent problem in U.S. nursing homes is understaffing. Geng et al. (2019) analyze daily nursing home staffing data from April 2017 to March 2018. They find that the majority of nursing homes met the expected Centers for Medicaid and Medicare Services staffing levels for fewer than 20% of days in the year. And researchers have documented a relationship between understaffing and lower quality of care, including residents falling more frequently (Leland et al., 2012), being restrained more frequently (Miller et al., 2006) and other measures of poor quality (Collier & Harrington, 2008). In the context of the COVID-19 pandemic, understaffing has the potential to contribute to the spread of disease, as fewer workers means that each worker interacts with more patients per day.
The final unique characteristic of these workers is the focus of this study: the extent to which they work for more than one employer and in more than one long-term care or health care setting. Multiple job holding may occur because the primary job does not provide the desired number of weekly hours or pay enough, leading to financial constraints. When workers hold multiple jobs, particularly with insufficient PPE and testing, they are more likely to become infected because of exposure to more patients. Regardless of whether a worker with multiple jobs becomes symptomatic, they have the potential to transmit infection between various health and long-term care institutions. Transmission of infections from staff to patients has been documented (Barnam & Kerby, 1981; Harkness et al., 1992) and there is also a relationship between outbreak of contagious disease and worker “presenteeism,” or working while sick (High et al., 2007; Kobayashi et al., 2016).
New Contributions
There is a gap in our collective understanding of the extent of multiple job holding among direct care workers and nurses who work in long-term care. We are among the first to estimate the prevalence of multiple job holding in this workforce. This is especially important in the context of COVID-19, as nursing homes across the country have served as “hotspots” of contagion and, for many states, are the primary source of COVID-19 deaths.
To our knowledge, there are two existing papers on this topic. One is a study by Van Houtven et al. (2020), who analyze data from a 2012 survey of workers in 30 nursing homes in the Northeastern United States and find that one in six report holding multiple paid jobs and that many feel pressure to come to work even when they are sick. The second is by Chen et al. (2020), who use cell phone location data to estimate job holding in multiple nursing homes for workers from the Life Care Center in Kirkland, Washington. They find that 7% of workers from that center also appear in at least one other nursing facility and that the aggregate number of connections between nursing homes is high.
We build on this work by using a large national data set covering 10 years and including hospital and home health workers in our analysis. Using pre-2020 data, we estimate the rate at which direct care workers and nurses hold multiple jobs, the factors associated with multiple job holding, and the mix of employment across settings for those who do hold a second job. Our results are complementary to the studies discussed above, but not directly comparable, as the time period, sample and methods are very different. It is not possible at this point to measure the extent to which the spread of COVID-19 in nursing homes is driven by workers, due to incomplete testing and contact tracing, but it is now clear that nursing home workers and residents are a particularly vulnerable group during the pandemic. Our study is one of the first which looks at second job holding among workers in long-term care settings and our results have implications for policy design around COVID-19 and long-term care.
Method
We use data from the Current Population Survey (CPS), which collects data on second job holding for the Outgoing Rotation Groups each month, and limit our sample to only the 4th month that individuals are in the sample, so as to not double count any respondents. Given that we are focusing on specific occupation groups that represent a small fraction of the full CPS, we pool data for all months in the years 2010 through 2019 to generate a sufficient sample size.
Jobs in the CPS are defined at the level of the employer, and respondents are asked the industry of the employer, what kind of work they do for that employer (i.e., occupation) and their hours and earnings. We define primary and secondary jobs based on the order of the survey responses, which usually list the primary job as the one with the most weekly hours reported. The occupation and industry measures are the Census 2002 codes based on the North American Industry Classification System (NAICS) and the Standard Occupation Classification (SOC) manual. Direct care workers are defined as being either “nursing, psychiatric and home health aides” or “personal care aides.” Nurses are defined as being either “registered nurse” or “licensed practice or vocational nurse” (for simplicity, we refer to this group as LPN). Although these workers are able to work in a variety of settings, including various types of outpatient care and schools, when we look at combinations of primary and secondary jobs, we restrict our analysis to nursing homes and the two sectors which have been consistently open and functioning during the COVID-19 outbreak and employ these types of workers: hospitals and home health. Hospitals are defined in a straightforward way, as they have their own unique NAICS code. We define nursing homes as either “nursing care facilities” or “residential care facilities, without nursing.” Home health settings are defined as “home health care services” or “individual and family services.” For purposes of the analyses that follow, we create a sample of those who are working in at least one job, which we define as reporting an occupation and industry, as well as positive earnings and hours, for at least one job.
We start our analysis by estimating the mean probability of holding a second job in our focal occupation groups and in the full set of workers in the sample. We then compare the characteristics of single versus multiple job holders within each occupation group, estimating means for weekly earnings, full-time status and imputed wage, as well as demographic variables and education levels. We perform two-tailed t tests for significant differences between the groups and weight all descriptive statistics using CPS individual sampling weights. The CPS uses multistage adjustments to adjust for sex, age, and race coverage to ensure that valid comparisons can be made across major race/ethnicity, gender, and age groups. We then formalize the descriptive analysis of single versus multiple job holders by estimating logit regressions in which the dependent variable is equal to 1 if the individual reports a second job and 0 otherwise. All of the demographic and education variables in the descriptive analysis are included in all models. However, we estimate three separate models for each occupation group, one with weekly earnings, one with weekly earnings and a dummy variable for working full-time (or more than 35 hours), and another with just imputed wage. Finally, all of the logit models include dummy variables for each year in the sample to account for any changes in rates of second job holding over time caused by factors not in the model.
Results
Prevalence and Determinants of Multiple Job Holding
In Table 1, we show that the average probability of holding two or more jobs for all workers in the CPS during the 2010-2019 period is 4.73%. Direct care workers are 36% more likely to hold multiple jobs, with a probability of 6.41% (p < .01). Perhaps surprisingly, given their much higher wages, nurses are also likely to hold multiple jobs—32% above the sample of all workers—with a probability of 6.23% (p < .01). For purposes of comparison, we have also estimated second job holding rates in the first month of the 2014 Survey of Income and Program Participation and find slightly higher overall rates, but a similar pattern of 5.96% for all workers, 6.58% for direct care workers and 7.81% for nurses. Additionally, we have tabulated rates of second job holding in our CPS sample broken down by year and they range from 5.17 to 7.7 for direct care workers and from 5.39 to 7.34 for nurses, but there is no clear upward or downward pattern.
Fraction of Respondents Holding Second Job.
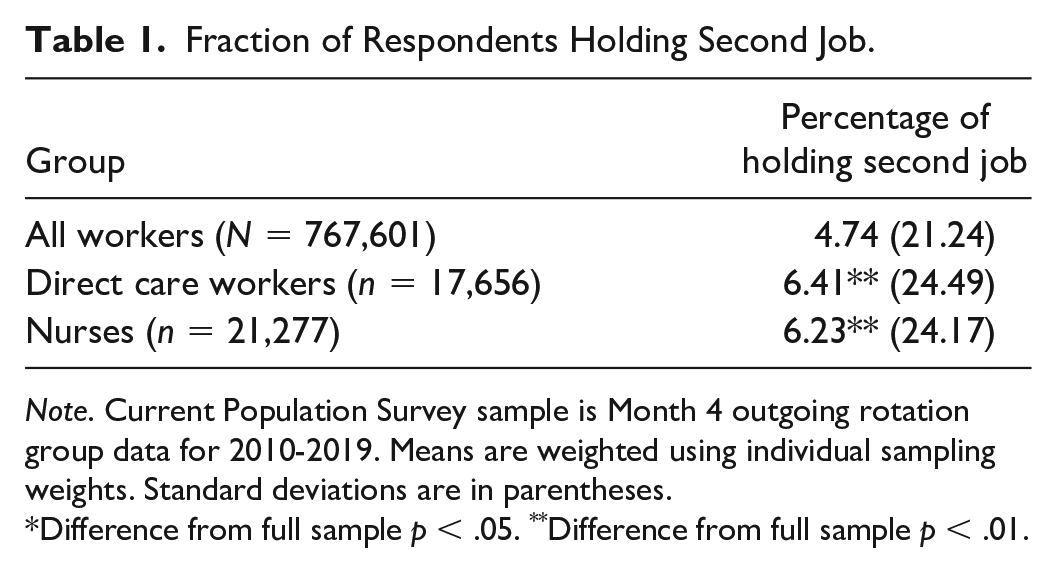
Note. Current Population Survey sample is Month 4 outgoing rotation group data for 2010-2019. Means are weighted using individual sampling weights. Standard deviations are in parentheses.
Difference from full sample p < .05. **Difference from full sample p < .01.
We next break apart the samples of direct care workers and nurses based on the setting of their primary jobs. Among direct care workers whose primary job is in a nursing home, the rate of second job holding is 6.84%, the highest of all settings. The rate for direct care workers with primary jobs in hospitals is 5.29%, a significant difference compared with nursing home workers (p < .05). The rate for those whose primary job is in home health is 6.65%, a difference that is not statistically significant. Among nurses, those in nursing homes are more likely to have second jobs than those in hospitals, but the highest rate (7.10%) is for home health nurses (p < .05).
We now restrict the sample to direct care workers and nurses. In Table 2, we compare the characteristics of workers with one and two jobs. It is clear that direct care workers are an economically vulnerable group. Their mean weekly earnings across the full sample are $442.32; this translates to $23,000 per year, assuming full-year work. Based on year and family size, 47.8% of workers who are the sole earners in their households would fall under the federal poverty threshold. More than two thirds would be eligible for Medicaid coverage under the Affordable Care Act expansions (68.23%).
Characteristics of Workers by Second Job Status.
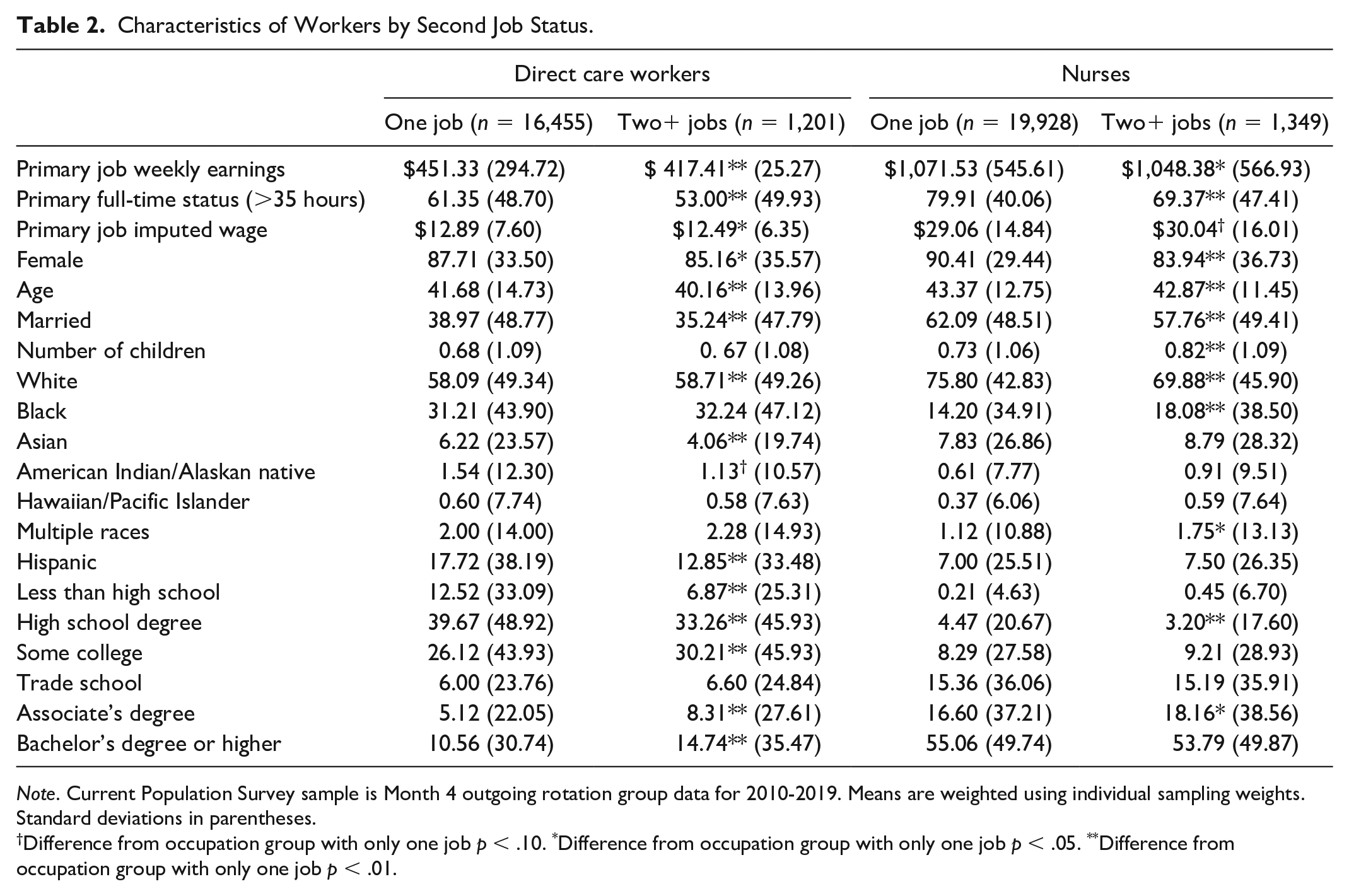
Note. Current Population Survey sample is Month 4 outgoing rotation group data for 2010-2019. Means are weighted using individual sampling weights. Standard deviations in parentheses.
Difference from occupation group with only one job p < .10. *Difference from occupation group with only one job p < .05. **Difference from occupation group with only one job p < .01.
Comparatively, second job holders are 8.3 percentage points less likely to work full-time (p < .01), and weekly earnings are approximately $34 lower (p < .01). This translates into hourly wages that are $0.40 or 3% lower (p < .05). Demographically, direct care second job holders are also significantly younger, less likely to be female and less likely to be married. White direct care workers are slightly more likely to have second jobs, while Asian, and American Indian/Alaskan Native and Hispanic workers are all less likely, controlling for all other characteristics.
There are also large and significant differences between direct care workers who hold one and multiple jobs in terms of education. One might expect more economically vulnerable workers with lower levels of education to be more likely to take second jobs, but it is actually the high-educated workers who are more likely. For example, direct care workers without a high school degree are only half as likely to hold a second job than those with a higher level of education. This makes sense from a job opportunity point of view, as most CNA programs require a high school diploma, some aides receive their training in a community college setting, and only CNAs are qualified to work in hospitals and many nursing homes.
Overall, nurses have significantly higher wages and earnings than direct care workers and they work almost 30% more hours. Among the nurses, those with more than one job also have slightly lower weekly earnings (p < .05) and are 10.5 percentage points less likely to work full-time p < .01). As was true with direct care workers, nurses with a second job are slightly younger and less likely to be married. Black nurses are more likely to hold second jobs than White nurses. And education is positively associated with second job holding, although not in a linear way. Nurses with associate’s degrees are about 10% more likely to hold second jobs than nurses with just a high school degree, but there is no significant difference for a bachelor’s degree. Given that LPNs and RNs have different educational requirements, we have estimated models (not shown) in which they are broken apart, but the results are very similar.
We formalize these descriptive statistics by estimating logit models in which the dependent variable is holding a second job relative to holding only one. Although these models do not necessarily produce causal estimates, they help better measure the relationships between second job holding and wages and hours by removing any correlations driven by demographic differences. For each occupation group, we run three specifications: (a) with only primary job weekly earnings, (b) with both earnings and a dummy for whether the primary job is full-time (greater than 35 hours), and (c) one in which only hourly wage is included. Hourly wage is imputed using earnings and hours. In Table 3, we present and discuss the results as marginal effects, which we have calculated from the logit coefficients; they are interpreted as the change in the dependent variable (in percentage points for dummy variables) for every unit change in the independent variable (or per $1,000 for earnings).
Logit Regression Results: Holding Two or More Jobs.
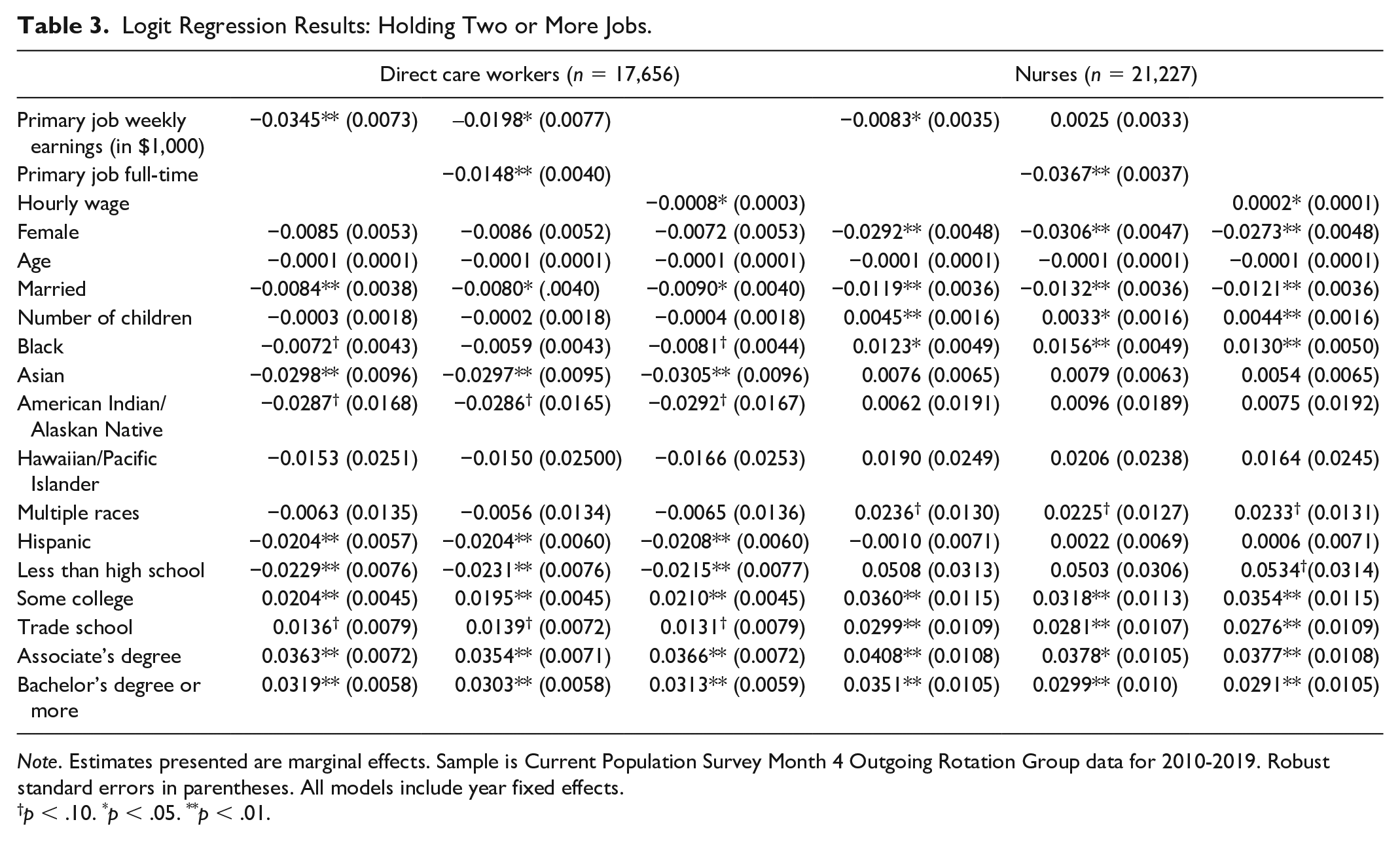
Note. Estimates presented are marginal effects. Sample is Current Population Survey Month 4 Outgoing Rotation Group data for 2010-2019. Robust standard errors in parentheses. All models include year fixed effects.
p < .10. *p < .05. **p < .01.
For direct care workers, earnings, full-time hours and wage are all significantly associated with the probability of holding a second job in the expected negative direction. The results in the first column show that for every additional $1,000 in weekly earnings, the likelihood of holding a second job decreases by 3.5 percentage points (p < .01); that translates to a 7% lower probability of second job holding associated with a 20% increase ($42) in the mean earnings of a 2nd job holder. The estimate decreases to 2 percentage points per $1,000 in earnings when we add a full-time primary job variable. Having a full-time primary job is associated with a 1.5 percentage point, or 23%, lower probability of holding a second job (p < .05). When we add wage into the model without earnings and hours (column 3), the likelihood of holding a second job decreases by 0.08 percentage points for every dollar increase in hourly wage (p < .05). This means that a 10% increase in the hourly wage (or about $1.20) is associated with a decrease in the probability of holding a second job of 0.09 percentage points or approximately 1.5%. This is a relatively small effect, but we note that because we are imputing wage, the resultant measurement error in the variable will tend to bias our estimate downward.
As in the descriptive statistics, married workers are significantly less likely to take second jobs, although there is no longer a statistically significant effect for age. Compared with White workers, Asian, American Indian, and Alaskan Native workers are all less likely to have second jobs. Black direct care workers are also less likely, but the effect is of a smaller magnitude and only statistically significant in the model that does not control for work hours. Hispanic workers are significantly less likely than non-Hispanics to hold second jobs. The positive effect of education on second job holding is similar to the one found in the descriptive statistics.
For nurses, weekly earnings in the primary job are associated with a significantly lower probability of holding a second job (p < .05), but the effect becomes insignificant when an indicator for full-time status is introduced into the model. However, there is a large and statistically significant 3.67 percentage point (62%) reduction in second job holding associated with having a full-time primary job. The effect of hourly wages is positive but very small. Female and married nurses are less likely to hold second jobs, while those with children and Black nurses are more likely. They are also more likely to hold a second job for each additional child they have. And, again, education is significantly and positively associated with second job holding.
Our evidence suggests that for nurses, constrained hours on the first job, or wishing to work more than the hours available, is the most likely explanation for multiple job holding. However, for direct care workers both wages and hours matter. This is not surprising, given that their mean wages are low relative to costs of living, and even relative to the federal poverty threshold.
Characteristics of Primary and Secondary Jobs
In the remaining analyses, we restrict our sample to direct care workers and nurses with second jobs and analyze the location of their primary and second jobs. For their primary job, direct care workers are most likely to work in home health settings (35.45%) and also nursing homes (29.74%); a smaller but nontrivial fraction work in hospitals (13.25%). Hospitals are the setting for 57.27% of primary jobs for nurses, with smaller fractions of primary jobs in nursing homes (11.46%) and nursing homes (5.92%).
For both direct care workers and nurses, the secondary occupation is most often the same as the primary one. Approximately one half of direct care workers work second jobs as direct care workers. The next three most common occupations are outside of health care but still in the service sector: cashier, retail, and janitor/maid. This is not surprising, as these are predominantly low-wage workers with low levels of education and high rates of turnover (Baughman & Smith, 2012; Duffy et al., in press). But these findings are extremely relevant to exposure to COVID-19. Cleaning workers and cashiers are disproportionately likely to have been designated “essential workers” and, therefore, interact with the public—outside of health care—more than the average worker. News reports and other sources have focused on cashiers as a particularly vulnerable group in the COVID-19 pandemic (Bhattarai, 2020; Kinder, 2020; North, 2020). In total, we estimate that 15.11% of direct care workers’ second jobs are in occupations that are defined as “essential,” following the methodology put forth in Folbre et al. (in press) based on the Department of Homeland Security advisory guidance which identifies “essential critical infrastructure workers” who “protect their communities, while ensuring continuity of functions critical to public health and safety, as well as economic and national security.” 5
Turning to the results for nurses, just over 50% take second jobs as either RNs or LPNs. The next most common second occupation is college instructor; these are most likely, nurses who are serving as clinical faculty in nursing programs. Additionally, a smaller fraction (5.5%)—but clearly relevant to COVID transmission—that have second jobs as direct care workers.
Finally, we turn to data on what may be the most important factor affecting transmission of COVID-19 by nurses and direct care workers: the overlap of settings of primary and secondary job. First, note that because of the way the survey questions are asked in the CPS, a job refers to a particular employer; therefore, workers who report two nursing home jobs are working in two different nursing homes. The same is true for home health workers, although it is less clear whether respondents are reporting working for an agency as an employer or a single client as an employer—in either case, these workers come into contact with more patients. 6
Panel A of Table 4 contains the results for direct care workers with more than one job. Those with primary jobs in a nursing home are most likely to take a second job in another nursing home (31.51%), although a sizeable number of second jobs (20.00%) are in home health. Second jobs in hospitals (3.06%) are rarer. For those with primary jobs in hospitals, the settings are more evenly distributed, although home health (15.06%) is actually more common than hospital (13.06). A substantial number of workers (11.99%) hold second jobs in nursing homes (11.99%). Those “bundles” of jobs may be of particular concern during an outbreak like COVID-19, where hospitals may be the primary source of infection. Finally, most home health workers (30.81%) hold second jobs in home health, while a small number work in nursing homes (6.83%) or hospitals (3.45%).
Setting of Primary and Secondary Job.
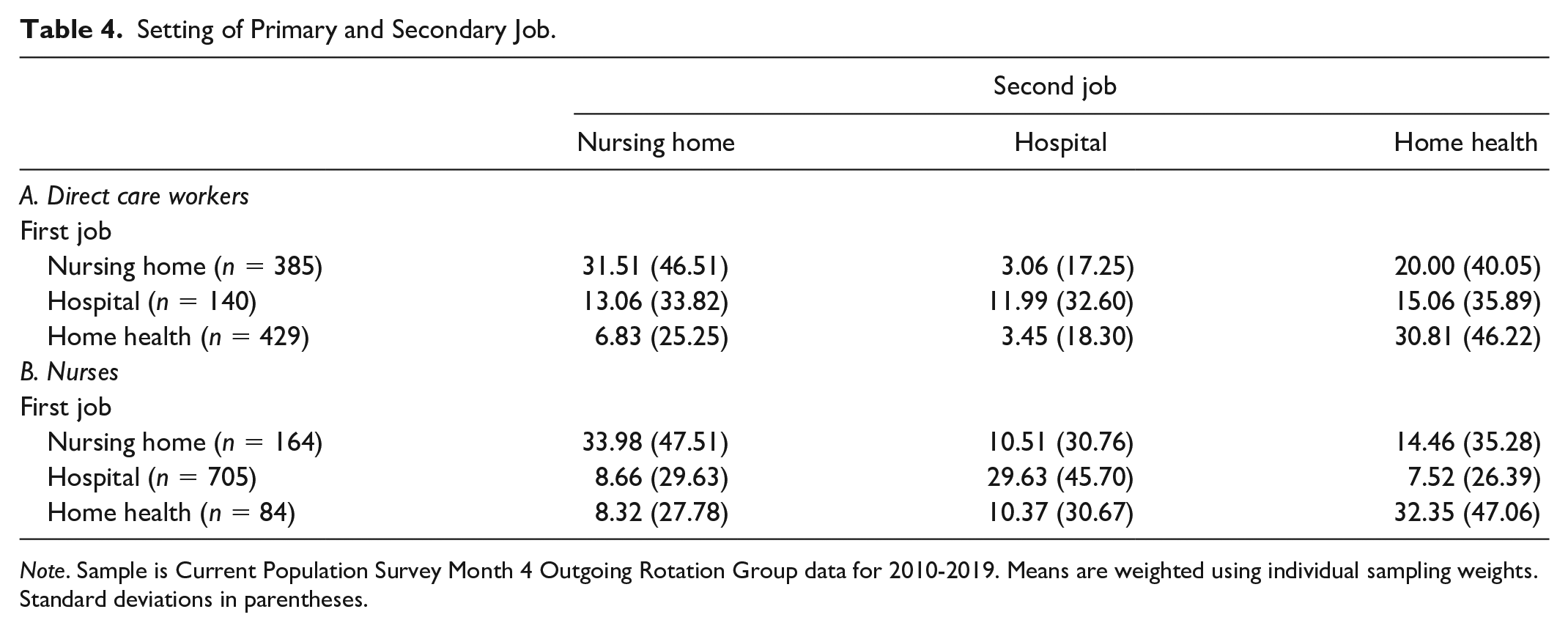
Note. Sample is Current Population Survey Month 4 Outgoing Rotation Group data for 2010-2019. Means are weighted using individual sampling weights. Standard deviations in parentheses.
The results for nurses are presented in Panel B of Table 4. The most likely “bundles” of primary and secondary jobs are in the same setting. Workers in nursing home settings in their primary jobs are most likely to take a job in another nursing home (33.98%), and those in hospitals are most likely to take another hospital job (29.63%). The same is true of home health workers (32.35%). However, a nontrivial number of nurses are working in a combination of hospitals and nursing homes, with 10.51% of primary job nursing home nurses holding a second job in a hospital and 8.66% of primary job hospital nurses holding a second job in a nursing home. Finally, 14.46% of nursing home nurses and 7.52% of hospital nurses also work in home health.
Discussion
In this study, we estimate the extent to which nurses (RNs, LPNs) and direct care workers (CNAs and personal care aides) hold multiple jobs, as, in theory, this has the potential to explain some part of the disproportionately high impact of COVID-19 on nursing homes, patients and workers alike. Over time, we are learning more about transmission of the virus and have learned that transmission is primarily from person to person either by direct contact or via particles transmitted through the air from coughing or sneezing (Rothan & Byrareddy, 2020). Close proximity to other individuals is therefore considered very dangerous, but is required in this type of work, putting nurses and direct care workers at increased risk of contagion. We also now understand that there are many infected individuals who do not exhibit symptoms but do transmit the disease, and that asymptomatic transmission may be particularly important in long-term care facilities (Gandhi et al., 2020). Movement of workers between various health and long-term care settings is therefore a cause for concern.
Overall, we find that although direct care workers and nurses are significantly more likely than other workers to hold second jobs, the absolute rates we measure in the CPS are not large. This begs the question of the extent to which second job holding explains COVID-19 outbreaks in nursing homes. We note that the epidemiological understanding of this disease is not that it is transmitted directly from one care provider to one patient, but that “super-spreaders” are likely to explain a large amount of total transmissions. Evidence suggests that a small number of contagious people, some of them asymptomatic and yet highly contagious, are responsible for a majority of infections (Beldomenico, 2020). The interpretation in our context could be that just one contagious nursing home worker could go into a new facility and transmit to coworkers and residents, they do not care for through networks of contact. And that is meaningful if poorly paid direct care workers are more likely to live in low-income areas where rates of COVID-19 infections are higher.
To the extent that multiple job holding becomes a public health concern during outbreaks of contagious disease, it is important to understand the factors associated with working for two or more employers. Theoretically, there are several motives for holding more than one job, including hours constraints and economic vulnerability driven by low wages. Among nurses, the former seems to be more relevant, as weekly hours at the primary job are negatively and significantly associated with the probability of holding another job, while wages and earnings have weaker effects. However, among direct care aides, earnings and wages are also significantly and negatively associated with second job holding. This makes sense given that their average wages are very low to begin with and fall below living wage standards in many parts of the country; they are likely to work second jobs to meet financial obligations.
Anecdotally, during the initial outbreak, some nursing home managers identified second job holding as a potential source of disease transmission and either required or incentivized workers to work in only one facility by paying bonuses (Crimaldi, 2020). In a more general sense, policy makers have also identified nursing and direct care labor supply as essential in the fight against COVID-19. For example, in New Hampshire, Governor Chris Sununu implemented a $300 weekly stipend for 25,000 frontline Medicaid workers caring for seniors to encourage them to continue working in long-term care settings from mid-April through the end of June 2020 (Landrigan, 2020). Federal legislators have proposed additional compensation for essential workers who are at increased risk of contracting COVID-19 through a temporary bonus of up to $12 per hour in “Patriot Pay” to ensure that essential workers in critical industries receive higher compensation than the unemployment insurance rate (Romney, 2020). Neither policy is aimed at reducing second job holding, but our results suggest that doubling the hourly wage of direct care workers, as the “Patriot Pay” plan would effectively do, would decrease the probability of holding a second job by 15%. Raising the wages of low-wage health care workers at their primary job could reduce the incentive for workers to attain a second job.
Of course, there are other steps nursing homes—and to a lesser extent hospitals and home agencies—can take to keep both patients and workers safe. We also find that having a primary job that is full-time is associated with a significantly lower likelihood of having a second one. While we are not able to flesh out the causal relationship (or possibility of joint choice of first and second job), the result suggests that offering full-time hours could reduce second job holding. Another step would be to improve average staffing levels. Understaffing in nursing homes has been a common problem that predates the COVID-19 pandemic, and during outbreaks of contagious disease, the more patients a worker has to take care of, the greater the possibility of transmission, even when they do not hold a second job. Additionally, the pandemic demonstrates that appropriate levels of PPE and regular testing are just as important in nursing homes as they are in hospitals. These measures protect the workers themselves, as well as their patients.
This study is an introductory exploration of multiple job holding by nurses and direct care workers in three settings that involve vulnerable patients and high prevalence of COVID-19. However, it has limitations and answers only some of the questions one might ask about the role of nursing homes and long-term care workers in the spread of COVID-19. First, the analysis we present is descriptive in nature, so to the extent that first and second jobs are chosen jointly, wages and hours may not be exogenous to the decision to hold more than one job. Additionally, we face data limitations. Because we focus on a very specific group of occupations and employment settings, our sample of nurses and direct care workers who hold a second job is relatively small, even with the pooling of monthly CPS data for 10 years. To address the concern that outliers or specific CPS questions might be producing unreliable results, we have conducted the same analyses presented in this article using data from the Survey of Income and Program Participation (SIPP), a data set that has a smaller sample size, but places more emphasis on collecting information for multiple jobs. And although the SIPP results are not always statistically significant, they present a pattern that is very similar to the CPS results we summarize in this article. Additionally, the CPS may be undercounting the true rate of second job holding because it misses gig work and self-employment (Rho & Fremstad, 2020). That suggests we may be missing some informal home health work. This is likely to be one reason why our estimated rates of second job holding are lower than those in Chen et al. (2020) and Van Houtven et al. (2020). Another difference is that our CPS measure defines jobs based on an employer and will not capture workers who move between nursing homes run by the same company; that may explain part of the difference between our estimates and the location-based estimates in Chen et al. (2020).
We also note that in our data, Black nurses have a higher likelihood of holding multiple job holding than White nurses, but do not find this same pattern among direct care workers. News reports show that nursing homes with higher representation of Black and Hispanic residents have been hit harder by COVID-19, due in part to disparities in nursing home quality but also due to the location of these nursing homes in Black and Hispanic communities where COVID-19 is more prevalent (Konetzka & Werner, 2020). Staff, who go in and out of the nursing home and potentially to other long-term care facilities, typically live in the community in which they work. We have not focused on the relationship between race, community, and second job holding, but this is clearly an area for further research.
Finally, given that our data precedes the COVID-19 pandemic, one could ask whether our results reflect behavior during the pandemic, particularly whether direct care workers and nurses continued to hold second jobs during the COVID-19 outbreak. Preliminary data suggest the increased likelihood of holding multiple jobs shown for these two occupation groups has not diminished as an effect of the pandemic. Data for March, April, and May of 2020 show even though second job holding rates fall across the board, direct care workers and nurses are still significantly more likely be dual job holders compared with the average worker. As policy makers look to limit the spread of COVID-19 in nursing home facilities, multiple job holding among nurses and direct care workers should be closely monitored in the upcoming months.
Conclusion
In this study, we explore the prevalence and factors associated with second job holding among nurses and direct care workers. We find that direct care workers are 35% more likely to hold multiple jobs than other workers and nurses are 32% more likely. Additionally, the pairing of first and second jobs in health and long-term care may be a cause for a concern. When these workers hold second jobs, they are most likely working in the same type of institutional setting, but for a different employer and at a different location. We also see pairs of jobs that span the three key settings in the study: nursing homes, hospitals, and home health. Approximately 9% of dual job holding nurses whose primary job is in a hospital work a second job in a nursing home, and 20% of direct care workers and 14% of nurses who hold a primary job in nursing homes also work in home health care. Third, even though the raw numbers are small, for direct care workers, we show that the next most common occupations for second jobs are in other essential, “front line” jobs such as cashier and cleaning worker. Taken together, the results suggest that reducing second job holding among workers in nursing homes and home health has the potential to reduce transmission of COVID-19.
Footnotes
Acknowledgements
We are grateful to Bianca Frogner and Joanne Spetz for helpful comments on an earlier version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.