
Abstract
Consumer cost-sharing has been shown to diminish utilization of preventive services. Recent efforts, including provisions within the Affordable Care Act, have sought to increase use of preventive care through elimination of cost-sharing for clinically indicated services. We conducted a rapid review of the literature to determine the impact of cost-share elimination on utilization of preventive services. Searches were conducted in PubMed, Scopus, and CINAHL Complete databases as well as in grey literature. A total of 35 articles were included in qualitative synthesis and findings were summarized for three clinical service categories: cancer screenings, contraceptives, and additional services. Impacts of cost-sharing elimination varied depending on clinical service, with a majority of findings showing increases in use. Studies that included socioeconomic status reported that those who were financially vulnerable incurred substantial increases in utilization. Future investigations on additional clinical services are warranted as is research to better elucidate populations who most benefit from cost-sharing elimination.
Introduction
The cost of health care in the United States has skyrocketed over the past half-century. In 2018, total national health expenditures exceeded $3.7 trillion, compared with the $27.2 billion spent in 1960 (adjusted for inflation; Peterson-KFF Health System Tracker, n.d.). As aggregate health care expenditures have risen, out-of-pocket consumer costs have also increased. Among those with employer-sponsored insurance, the average general annual deductible for single coverage was 162% higher in 2019 compared with 2009 ($1,396 compared with $533, respectively; Kaiser Family Foundation, 2019). There is significant evidence that the presence of cost-sharing, even if the amount is relatively modest, deters patients from receiving care (Goldman et al., 2004; Lohr et al., 1986). Decreases in care utilization are not limited to services with little clinical benefit for patients. High-value preventive and chronic disease management services are also received less frequently when cost-sharing is imposed, even if high-value services themselves are exempt from cost-share (Busch et al., 2006; Solanki & Schauffler, 1999).
There have been efforts to reduce cost-sharing for high-value services among private and public health insurance plans since the relationship between cost-sharing and limited use of services was elucidated. In March 2010, the Patient Protection and Affordable Care Act (ACA) was enacted. This multifaceted health care reform law was designed to increase the affordability of health insurance, expand state Medicaid programs to cover all adults with incomes under 138% of the federal poverty level, and support the development of innovative health care delivery methods to reduce health care costs (ACA, n.d.-a). Section 2713 of the ACA eliminated out-of-pocket costs for high-value preventive care services among private, nongrandfathered health insurance plans. High-value services considered exempt from cost-share under Section 2713 are determined by the U.S. Preventive Services Task Force (USPSTF), the Advisory Committee on Immunization Practices, and the Health Resources and Services Administration (Coverage of Certain Preventive Services Under the Affordable Care Act, 2015). The ACA also eliminated cost-sharing in Medicare plans for USPSTF-recommended preventive services and required colorectal cancer screenings to be covered predeductible for Medicare enrollees (Tolbert, 2015). Through eliminating cost-sharing for these services, it was hoped that utilization of preventive care would increase, helping to reduce the incidence of chronic disease and thus limit spending on more costly secondary interventions.
Ten years after the enactment of the ACA, assessments have provided mixed results on the impact of the cost-sharing elimination mandate on utilization of preventive services. Some reports have shown that some utilization rates have increased, such as rates of blood pressure checks and flu vaccinations (Han et al., 2015; Hong et al., 2017). Others have demonstrated that the mandate improved the utilization of some services among subgroups of the population, such as increased colonoscopy use among Medicare recipients, but made no impact on utilization rates generally (Richman et al., 2015). Additional analyses have concluded the ACA is not associated with changes in utilization for select services, including long-acting reversible contraceptives (LARCs) and breast, cervical, and colorectal cancer screenings (Alharbi et al., 2019; Han et al., 2015; Jensen et al., 2015; Pace et al., 2016). The ACA has even been shown to correspond with decreases in the utilization of mammography (Carlos et al., 2019; Jena et al., 2017). These manuscripts normally examine a handful of services, such as cancer screenings or contraceptive methods, with many looking at utilization changes for only one service. As of December 2019, 68 preventive services were listed as exempt from cost-sharing on HealthCare.gov. Furthermore, some analyses of private health insurance claims inferred that the ACA is responsible for changes in utilization without specifying whether claims came from grandfathered or nongrandfathered health insurance plans (Alharbi et al., 2019; Han et al., 2015). Without this specification, changes in utilization for privately insured populations cannot be directly linked to the ACA elimination mandate as those in grandfathered plans may still have cost-sharing provisions in place for preventive services.
To our knowledge, no review has been published that examines the direct impact of eliminating cost-sharing on utilization for an extensive list of preventive services, such as those covered under Section 2713 of the ACA. We conducted a rapid review to determine the effects of cost-share elimination on the utilization of preventive care. Services of interest included all services listed on HealthCare.gov as of December 20th, 2019, as this comprehensive list includes most services that are exempt from cost-share in most health plans. We included studies that occurred pre-ACA, are directly linked to the ACA mandate, or are unrelated to the ACA mandate as we wanted to report general changes in preventive service use due to cost-share elimination.
New Contributions
Following a search of the existing literature, this is the first rapid review examining the utilization of a broad range of preventive services following the elimination of cost-sharing. This is of notable importance as the 10-year anniversary of the passage of the Patient Protection and ACA was observed in 2020. An extensive review of service utilization at this point in time is paramount in determining the impact of this specific policy on preventive care use, and more broadly, how the removal of cost-sharing in the United States may affect health care use and long-term patient-centered outcomes.
Conceptual Framework
This narrative review of the impacts of cost-sharing on the utilization of high-value preventive services is based on the tenets of value-based insurance design (V-BID). In 2001, Fendrick et al. (2001) proposed that the cost-sharing amount for a service should be based on a patient’s potential clinical benefit, and laid the groundwork for the concept of V-BID. Within V-BID plans, there would be minimal to no cost barrier for high-value services to incentivize use. V-BID principles have been incorporated by several employer plans to reduce employees’ out-of-pocket costs for preventive and chronic disease management services (Busch et al., 2006; Chernew et al., 2008; Choudhry et al., 2010; Hirth et al., 2016). Copayment elimination has also been the focus of experimental trials, such as the MI-FREEE trial, which eliminated out-of-pocket costs for patients after myocardial infarction in the hopes of increasing medication adherence (Choudhry et al., 2011). Throughout the first decade of the 21st century, employer plans were the main areas of V-BID implementation as large, self-insured employers had significant control over their plans’ benefit design (Chernew et al., 2007). Since V-BID principles had been incorporated in plan design for years prior to the enactment of the ACA, we chose to review studies that examined the elimination of cost-sharing outside of the ACA mandate as well as those that directly analyzed the impact of the ACA to best understand how V-BID has improved access to high-value preventive services.
V-BID principles were also considered as we defined the key terminology for our review. Preventive services were broadly defined as “routine health care that includes screenings, check-ups, and patient counseling to prevent illnesses, disease, or other health problems,” to reflect the potential V-BID has to provide clinical benefit to a wide variety of patients (HealthCare.gov, n.d.-b). We defined utilization using the 2013 edition of the Encyclopedia of Behavioral Medicine, which states that “Health Care Utilization is the quantification or description of the use of services by persons for the purpose of preventing and curing health problems, promoting maintenance of health and well-being, or obtaining information about one’s health status and prognosis” (Carrasquillo, 2013). Finally, in keeping with the original intent of V-BID, we defined elimination of cost-sharing as the complete removal of out-of-pocket costs (such as copayments, coinsurance, or payments prior to meeting a plan deductible) for a given preventive service.
Guided by the core principles of V-BID, we aim to inform the development of future V-BID policies, contribute new findings to the health care research landscape, and allow practitioners to be better informed on how benefit design can affect patient behavior and outcomes.
Method
Study Design
We conducted a rapid review informed by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA; Moher et al., 2009). The protocol for this review can be found in the University of Michigan’s digital repository, Deep Blue. Guided by the research question, “What is the impact of the elimination of cost-sharing for preventive care services on utilization?” this review aims to provide insight into how the practice of eliminating cost-sharing for key preventive care services affects beneficiaries.
Search
Search strategies were created by four team members (HN, HR, BS, and JES). The primary search strategy was created in PubMed (NLM, Washington, DC). Additional searches in Scopus (Elsevier, New York, NY) and CINAHL Complete (EBSCOhost; EBSCO, Ipswich, MA) were translations of that primary search. Search concept blocks were: cost-sharing, elimination, and preventive services as defined by HealthCare.gov and the USPSTF A and B recommendations. See Appendix A (available in the online supplement material) for a list of those services. Searches combined keywords in the title and abstract, such as “cost sharing” and “out of pocket,” and “early detection of cancer.” Controlled subject headings were used when available (e.g.., MeSH terms: cost sharing, and preventive health services). Databases were searched from their inception to the date of search: January 22, 2020. No other search filters were applied. Complete search strategies are available in Appendix B (available in the online supplement material). Results were exported to EndNote 8 and duplicates were removed.
Team members (HN, HR, MB, and BS) reviewed reference lists and citation tracked (in Scopus) articles meeting inclusion criteria. A final search strategy was to conduct limited searches of grey literature within the Kaiser Family Foundation, Commonwealth Fund, and Health Affairs Blog websites. As with any rapid review methodology, the team made intentional decisions about which portions of the systematic methodology to abbreviate while keeping any possibility of bias to a minimum. One abbreviation to note was the decision to choose three databases to search rather than several. The team also determined the search would be strengthened by citation tracking and searching reference lists.
Inclusion/Exclusion Criteria, Study Selection, Quality Appraisal, Data Extraction
Team members used DistillerSR software (Evidence Partners, Ottawa, Ontario, Canada) provided by the University of Michigan Taubman Health Sciences Library to conduct the screening and data extraction processes. Studies were included if they analyzed privately or publicly insured enrollees using at least one preventive service, and discussed utilization as it relates to the elimination of cost-sharing. For the scope of this article, preventive services were included in the review if they appeared on HealthCare.gov’s (2019) list of preventive health services as of December 20, 2019 (Appendix A [available in the online supplement material]). Exclusion criteria were: studies not about the American health care system; studies that did not measure utilization, but measured cost; or studies that were not primary research studies. It is important to note that recent changes in USPSTF guidelines regarding mammography and cervical cancer screenings influenced the impacts of elimination on utilization of these two services. This likely affected breast cancer and cervical cancer screening utilization findings reported in our review.
For the title and abstract screening, citations were randomly assigned to reviewers in DistillerSR, and each citation was reviewed by at least two team members (HN, HR, MB, and BS); conflicts were resolved throughout the initial screening phase in meetings with all reviewers present. At the full-text level, 191 articles were screened following the same protocol. Reasons for exclusion are noted in Figure 1. At the end of the screening process, 35 articles were selected for inclusion in the review.
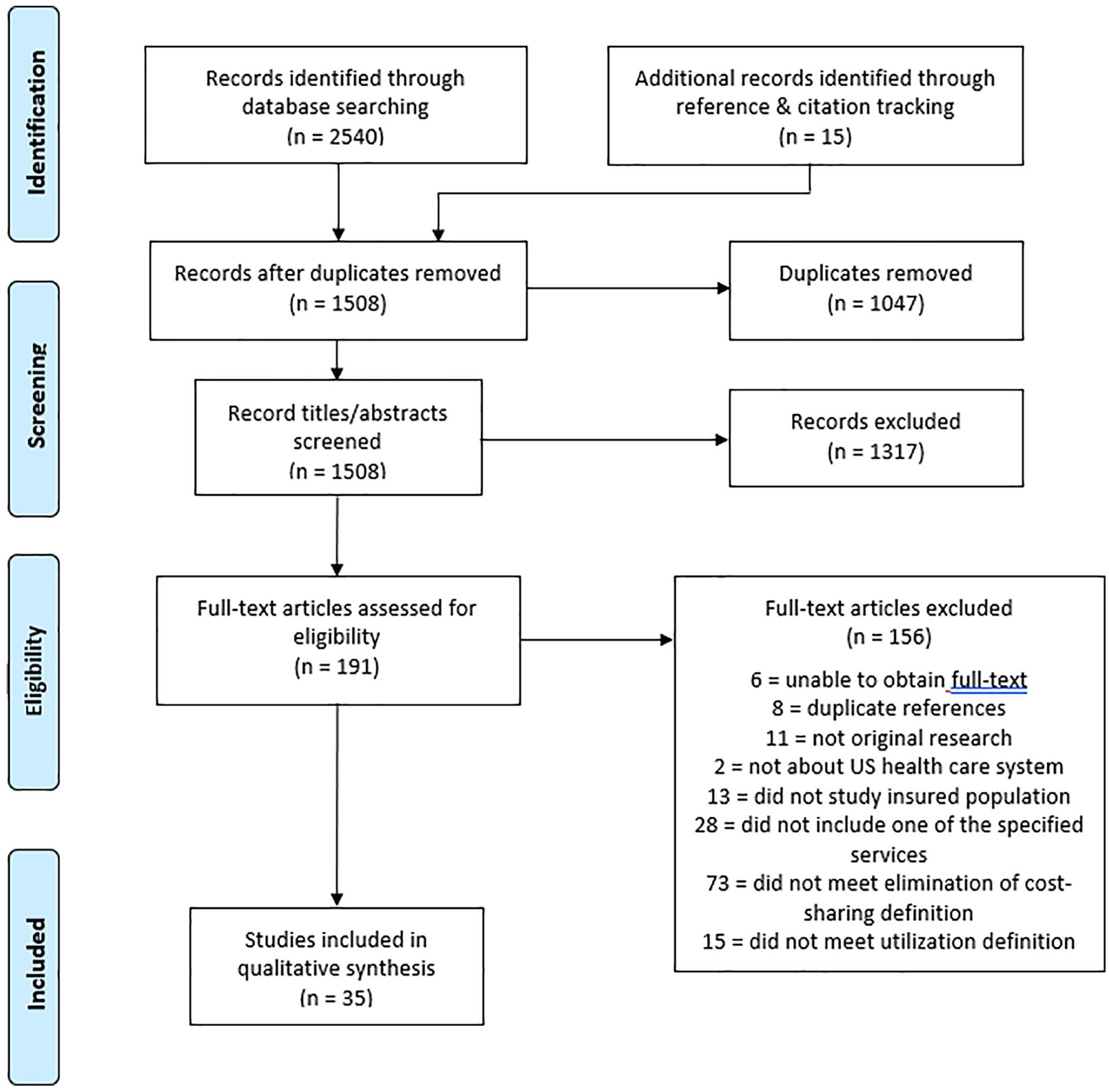
PRISMA 2009 flow diagram (Moher et al., 2009).
Articles selected for inclusion were appraised for methodological quality at the study level using the JBI Critical Appraisal Tools (Joanna Briggs Institute, Adelaide, Australia; checklists accessible at https://jbi.global/critical-appraisal-tools). As this review included articles with a variety of study designs, the critical appraisal tools for analytical cross-sectional studies, cohort studies, quasi-experimental studies, and randomized controlled trials were utilized to appraise quality as appropriate. A complete list of questions used to assess methodological quality is included in Appendix D (available in the online supplement material).
All articles were appraised by at least two team members; one team member (HN) reviewed all articles included in the review, with one of three team members (HR, MB, and BS) serving as a second reviewer on each article. Conflicts were resolved in meetings with all reviewers present. Levels of quality were assigned to articles based on the following criteria: good quality = more than 80% of items on checklist satisfied; moderate quality = between 41% and 80% of items on checklist satisfied; fair quality = less than 40% of items on checklist satisfied. These standards have been used by previous research to determine levels of methodological quality (dos Santos et al., 2019).
The following data points were extracted from each study: reference, characteristics of the population (race, gender, SES, type of health plan, education, age, geography, number of participants), preventive service(s), study setting, study design type, study timeline, utilization measurement, results and outcomes, conclusions, and secondary outcomes and results. For each study, one reviewer extracted the aforementioned data, and another performed quality control to confirm accurate reporting.
Results
Summary of Findings
A total of 35 articles were included; 19 were analytical cross-sectional studies, 12 were retrospective cohort studies, 3 were randomized controlled trials, and 1 was a quasi-experimental study. The complete list of included studies can be found in Appendix C (available in the online supplement material). Study characteristics can be found in Table 1. The included studies relied on various data sources: 17 using national claims or health plan data, 9 using national surveys, 6 using regional claims or health plan data, and 3 using point-of-service information. The majority (19) of the studies in the final search analyzed private health plans, followed by 14 studies on Medicare beneficiaries (2 of which focused on Medicare Advantage), 1 on Medicaid, and 1 on Veterans Affairs beneficiaries.
Study Characteristics.
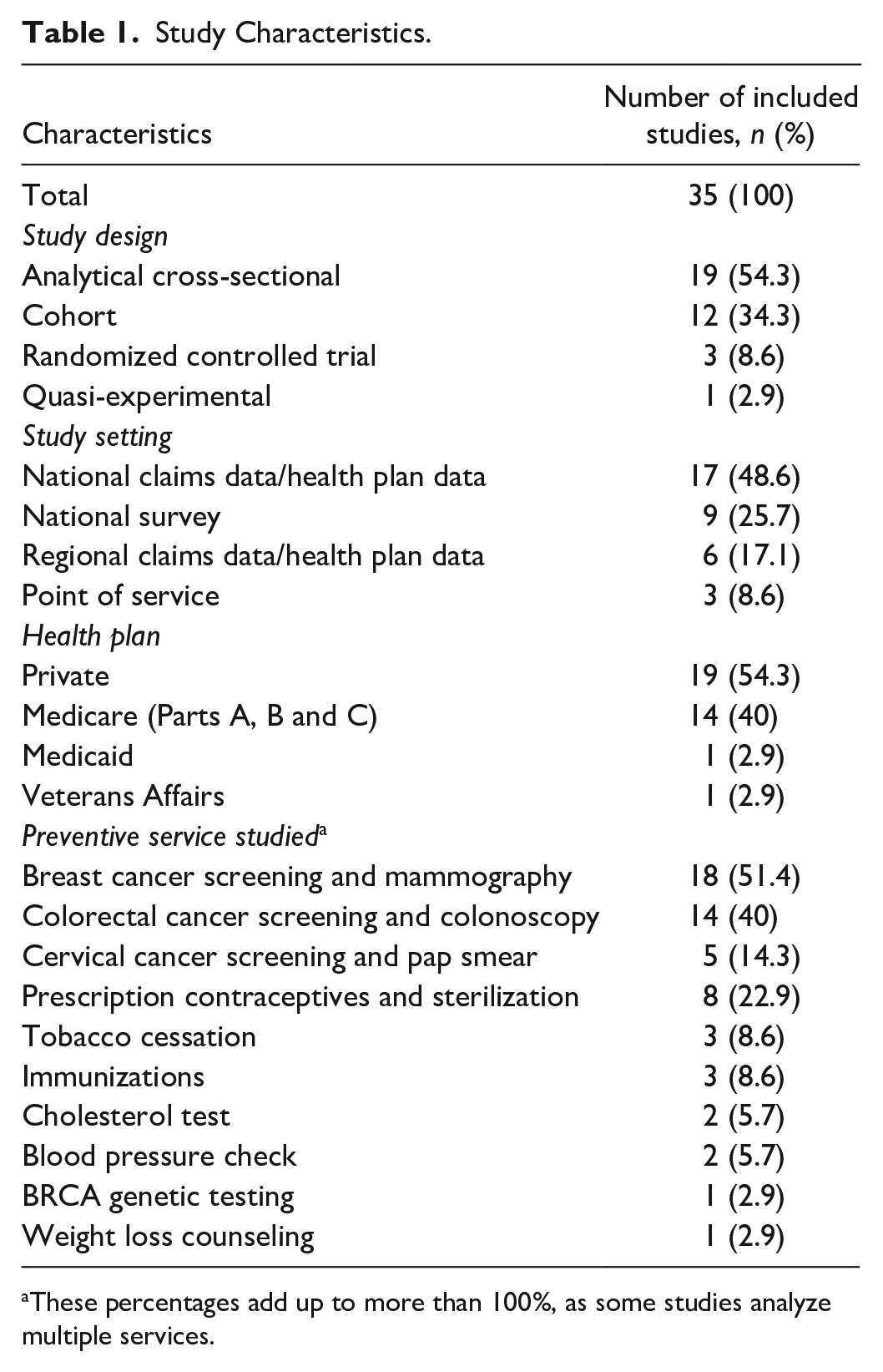
These percentages add up to more than 100%, as some studies analyze multiple services.
After conducting the quality assessment, the majority of articles included in our review were rated “good” quality (20 out of 35, or 57.1%). Fifteen articles were of “moderate” quality (42.9%). None of our included articles received a fair quality rating. Summary charts with results of the methodological quality assessment can be found in Appendix E (available in the online supplement material).
Of the 19 analytical cross-sectional studies, 8 received a “moderate” quality rating and 11 received a “good” quality rating. All analytical cross-sectional studies included clearly defined inclusion criteria; used objective, standard criteria for measuring elimination of cost-sharing; and used appropriate statistical methods. However, 17 articles identified and stated strategies to deal with confounding factors. 16 articles described study subjects and setting in detail. Only 12 articles measured the elimination of cost-sharing in a valid and reliable way, and 11 measured health care utilization in a valid and reliable way. Some cross-sectional studies utilized self-reported data from national or regional surveys to determine information on health insurance status, cost-sharing, and care utilization, which is considered an unreliable method of measurement.
Seven of the 12 retrospective cohort studies in our review were rated “good” quality, and the other 5 were rated “moderate” quality. For all retrospective cohort studies, exposures were measured similarly for the exposed and unexposed groups; outcomes were measured in a valid and reliable way; and appropriate statistical methods were used. A total of 11 studies identified confounding factors, and 10 stated methods of addressing confounding factors. Nine studies used exposed and unexposed groups that were recruited from the same population; measured exposure in a valid and reliable way; and followed participants for a significant amount of time to observe utilization of the preventive services of interest. Since all included cohort studies were retrospective, questions on the completeness of follow-up were not applicable.
The one quasi-experimental study included in our review, Jena et al. (2017), received a “good” quality rating. Jena et al. (2017) fulfilled all listed criteria for a quasi-experimental study, other than the requirement that participants included in comparisons be similar to one another: women with individual subscriber Medicare Advantage plans were slightly older, lived in poorer neighborhoods, and were more likely to be white and healthier than women in employer-supplemented Medicare Advantage plans. In addition, while Jena et al. utilized claims data to determine utilization of mammography in their population of interest, claims data were not explicitly mentioned as the data source in their published paper. One team member (HN) contacted the corresponding author to determine the data source (A. Jena, personal communication, March 9, 2021). Although claims data is a valid and reliable form of measuring exposure to cost-sharing and utilization, the omission of data source in the original article has the potential to impact interpretations of findings and applications to novel contexts if the corresponding author is not contacted.
Two of the randomized controlled trials were rated “moderate” quality, and one was rated “good” quality. All three studies used true randomization to assign participants into groups; had complete follow up or analyzed differences in follow up between experimental and control groups; analyzed participants according to group assignment; measured outcomes in the same way for all groups; used appropriate statistical methods; and used an appropriate trial design. Two out of three studies concealed allocation to treatment groups; stated explicitly that treatment groups were similar at baseline; blinded those delivering treatment to treatment assignment; explicitly stated that treatment groups were treated identically besides the treatment itself; and measured outcomes in a reliable way. Only one study explicitly blinded participants to treatment assignment. None of the randomized controlled trials stated that outcomes assessors were blinded to treatment assignment.
The search results of our literature review gathered utilization data for ten different services listed in the HealthCare.gov glossary. Some of the 35 studies mentioned more than one service, therefore resulting in a percentage of more than 100% within Table 1. Half of studies (18) included information about breast cancer screening and mammography, 14 about colorectal cancer screening and colonoscopy, 8 about prescription contraceptives and sterilization, 5 about cervical cancer screening and pap smears, 3 about tobacco cessation, 3 about immunizations, 2 about cholesterol tests, 2 about blood pressure checks, 1 about BRCA genetic testing, and 1 about weight loss counseling. Our findings are organized into three main result categories: cancer screenings, contraceptives and sterilization, and additional services, and are detailed below.
Cancer Screenings
Many of our included articles reported on the impact of eliminating cost-sharing on screenings for cancer—specifically breast cancer, colorectal cancer, and cervical cancer.
Breast Cancer Screening and Mammography
Breast cancer screenings were the most frequent service of interest among our literature search items. Eighteen of 35 articles (51.4%) examined at least one form of breast cancer screening. Mammography was the most common form, and often the only form, of breast cancer screening reported. Eight studies focused entirely on screening mammography (44.4% of articles that included breast cancer screening; 22.9% of all included articles). Two studies provided information on rates of clinical breast exams in addition to rates of mammography (Jensen et al., 2015; Toseef et al., 2020). The data sources varied for each article, with eight using national claims data, six using results from national surveys, two using regional claims data, and one using point-of-service information. A summary of changes in breast cancer screening and mammography can be found in Table 2.
Summary of Changes in Utilization: Breast Cancer Screening and Mammography (n = 18).
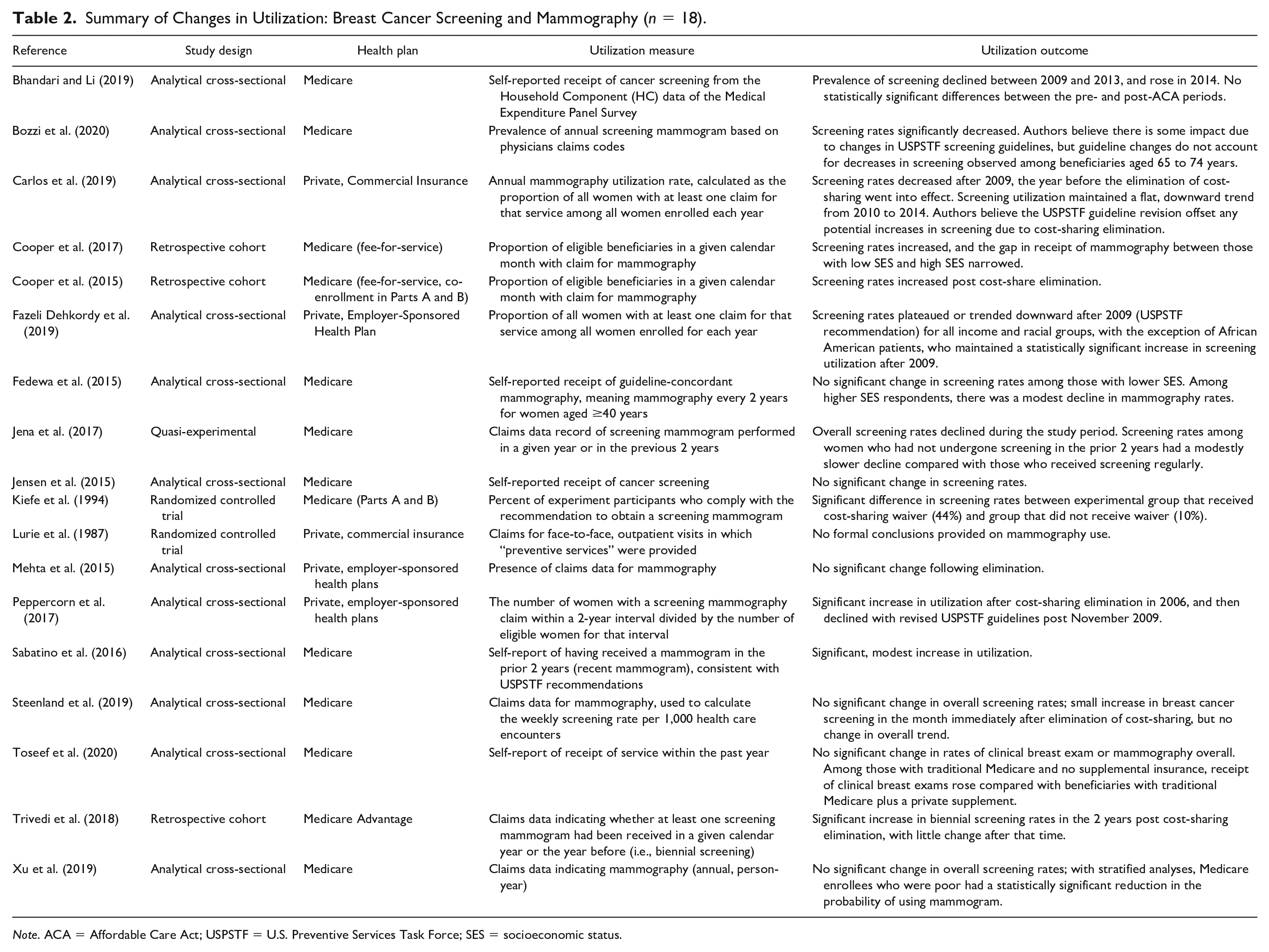
Note. ACA = Affordable Care Act; USPSTF = U.S. Preventive Services Task Force; SES = socioeconomic status.
Six studies conclude the removal of cost-sharing resulted in increased rates of screening, including four that focused on the effects of ACA implementation on mammography among Medicare populations (Cooper et al., 2015; Cooper et al., 2017; Sabatino et al., 2016; Trivedi et al., 2018). In two retrospective cohort studies, Cooper and colleagues determined that among a sample of Medicare beneficiaries older than 70 years, there was a statistically significant increase in the odds of mammography use in the 2 years following the ACA mandate (Cooper et al., 2015; Cooper et al., 2017). Mammography rates increased between the pre-ACA and post-ACA periods for all socioeconomic groups, contributing to a narrower gap in receipt of mammography between low and high SES groups, although having a lower SES was associated with lower odds of mammography in general (Cooper et al., 2017). Their data also suggest an association between use of wellness visits and preventive screenings, and that previously having a mammogram increases the likelihood of subsequent screening (Cooper et al., 2015). Both retrospective cohort studies received “good” quality ratings, and the only missing criteria was that the measurement of cost-sharing elimination was not reliable; dual-eligible beneficiaries or beneficiaries with supplemental insurance were not analyzed separately from beneficiaries only enrolled in traditional Medicare.
Through their analyses of survey data in an analytical cross-sectional study, Sabatino et al. (2016) observed a 3.5 percentage point increase in reported mammography screening for Medicare beneficiaries between 2010 and 2013, with 74.7% of survey respondents between ages 65 and 74 years reporting a mammogram in 2013. Sabatino et al. (2016) received a “moderate” quality rating as the study relied on self-reports of insurance status and utilization of mammography. In their retrospective cohort study, Trivedi et al. (2018) analyzed the Medicare Beneficiary Summary File and also reported a nearly 6 percentage point increase in mammography rates for the 2-year period post-ACA for women in Medicare Advantage plans that eliminated cost-sharing, a significant increase compared with screening rates for those in plans that did not impose cost-sharing before the ACA. Trivedi et al. (2018) received a “good” quality rating, fulfilling all criteria for a retrospective cohort. Both Trivedi et al. (2018) and Sabatino et al. (2016) note that despite the observed increases in screening, less than three quarters of eligible beneficiaries received mammography during their respective study time periods, and suggested that ensuring beneficiaries are aware of cost-share eliminations could increase the impact of policy change.
The remaining articles that reported increases in breast cancer screenings following cost-share removal took place outside of the context of the ACA. Peppercorn et al. (2017) observed a natural experiment when a large rural health insurance provider eliminated out-of-pocket costs for screening mammography in 2006. Annual and biennial screening rates rose significantly following the policy change: annual screening rates experienced a 5 percentage point increase overall post-2006 and increased the most among younger women (Peppercorn et al., 2017). Peppercorn et al.’s (2017) analytical cross-sectional study was given a “moderate” quality ranking, as the authors did not identify or state strategies to account for confounding factors. Kiefe et al. (1994) conducted a randomized controlled trial where Medicare-enrolled women at an inner-city general medicine clinic were recommended to obtain a mammogram at a nearby facility, and half of patients received a voucher for free screening mammography. The study was considered to be “moderate” in quality, as participants, providers, and outcomes assessors were not blind to which women were given a voucher. 44% of women who received a voucher for mammography obtained screening mammograms, whereas only 10% of patients without vouchers did so, resulting in an adjusted odds ratio of 7.4 following multiple logistic regression (Kiefe et al., 1994). The main reason women without vouchers reported not receiving screening was due to cost, leading Kiefe and colleagues to conclude that copayments were significant financial barriers to receiving mammography for low-income Medicare enrollees.
Three papers determined overall breast cancer screening rates decreased following the ACA elimination of cost-sharing for Medicare Advantage, Medicare, and commercially insured populations, respectively. In their quasi-experimental study, Jena et al. (2017) compared post-ACA annual and biennial screening rates between women with individual-subscriber Medicare Advantage insurance, who previously had a $20 copay for mammography, and employer-supplemented group Medicare Advantage insurance, who always had full screening coverage. They concluded that screening rates decreased for both groups between 2009 and 2012, with those who experienced the new cost-share elimination experiencing 1.4 percentage points lower decline compared with the full-coverage group (Jena et al., 2017). While Bozzi et al. (2020) found that the proportion of annual screening mammograms increased for Medicare beneficiaries between 2001 and 2007, prior to cost-sharing elimination, the prevalence of annual screening mammograms among women ages 65 to 74 years began to decline after 2007 and did not increase after the ACA mandate. For women aged 65 to 74 years, the adjusted odds of annual screening mammograms post-ACA was 25% lower than the odds of screening mammograms pre-ACA (Bozzi et al., 2020). In their interrupted time series analyses of utilization trends, Carlos et al. (2019) reported that annual screening utilization rose from 36.0% in 2004 to a peak of 42.2% in 2009 among their commercially insured population, before experiencing a steady rate of decline after 2010, eventually reaching 39.9% in 2014. All three studies were given a “good” quality ranking, with Carlos et al. (2019) fulfilling all the critical appraisal tool criteria for an analytical cross-sectional study and Bozzi et al. (2020) meeting all criteria besides measuring exposure in a valid and reliable way. A discussion of Jena et al.’s quality criteria can be found in the Summary of Findings section. The results of these studies counter the expectation of moral hazard following the removal of financial barriers.
All three studies drew connections between changes in USPSTF guidelines in 2009, which modified screening mammography recommendations to biennial instead of annual for women aged 50 to 74 years and no longer recommended screening mammography among women older than 74 years, and their observed decreases. Bozzi et al. and Carlos et al. noted that the reductions in screening mammograms occurred indiscriminately of beneficiary age and could have been due changes to physician specialty guidelines instead of changes to USPSTF guidelines (Bozzi et al., 2020; Carlos et al., 2019; Jiang et al., 2015). Carlos et al. additionally suggested that few plans required cost-sharing for mammography before the ACA, and those plans that did require cost-sharing only charged patients a small amount. Carlos et al. (2019) proposed that there could be “a ceiling effect in further responses of screening rates to patient financial incentives to reduce screening cost” (p. 793). Jena et al. (2017) saw the effect of the ACA mandate as protective for mammography screening rates, concluding that “full coverage for screening mammography had a slight positive impact among new women undergoing screening” and helped slow the screening rate decline that may have been precipitated by the USPSTF guideline changes (Jena et al., 2017, p. 201).
Four analytical cross-sectional studies reported that breast cancer screening rates did not significantly change among Medicare beneficiaries after the ACA-related elimination of cost-sharing (Bhandari & Li, 2019; Fedewa et al., 2015; Jensen et al., 2015; Steenland et al., 2019). Among these studies, Steenland et al. (2019) was the only group to use claims data (from the Massachusetts All-Payer Claims Database between 2009 and 2012) in their analyses, and the study was assigned a “good’ quality rating for meeting all criteria besides providing a detailed description of study subjects. Bhandari and Li (2019) and Jensen et al. (2015) both used data from the Medical Expenditures Panel Survey to determine rates of mammography among Medicare beneficiaries. Fedewa et al. (2015) also utilized self-reports, specifically from the National Health Interview Survey between 2008 and 2013, to determine screening rates. Because of their uses of self-reported data, Bhandari and Li (2019), Fedewa et al. (2015), and Jensen et al. (2015) were given “moderate” quality rankings. In addition to the analyses of Medicare beneficiaries, Mehta et al. (2015) conducted a retrospective cross-sectional analysis of claims data for commercially insured Humana beneficiaries, also concluding that there were no significant changes in mammography utilization between those enrolled in grandfathered and nongrandfathered plans. Mehta et al.’s (2015) analytical cross-sectional study met all criteria on the JBI Critical Appraisal Tool and received a “good” quality rating.
Some groups proposed that minimal changes in screening rates could have been due to already low out-of-pocket costs for mammography prior to the complete elimination of cost-sharing, as Medicare only required a low coinsurance for mammography and many private plans exempted mammography from cost-share already (Mehta et al., 2015; Steenland et al., 2019). Multiple sets of authors also suggested that beneficiaries were not aware of the cost-share elimination, leading utilization to remain stagnant (Bhandari & Li, 2019; Jensen et al., 2015; Mehta et al., 2015; Steenland et al., 2019).
Additional articles infer that the ACA cost-sharing elimination had some impacts on breast cancer screening rates, but utilization overall was unchanged. Toseef et al. (2020) found that eliminating copayments for Medicare beneficiaries did not result in changes in overall breast cancer screening utilization for their population; however, the authors determined that traditional Medicare beneficiaries without supplemental insurance were more likely to report receipt of a clinical breast exam postelimination compared with their counterparts with supplemental insurance. Another research group, using claims information for commercially insured individuals, indicated that screening rates increased slightly during a 5-year period preceding the elimination of cost-sharing (2004 to 2009), but then plateaued in 2009 (Fazeli Dehkordy et al., 2019). When stratifying data by race, African Americans maintained a statistically significant increase in utilization post-2009 that was not observed among other racial groups, helping close the racial gap in patterns of screening mammography (Fazeli Dehkordy et al., 2019). Fazeli Dehkordy et al. (2019) believed overall utilization rates among their sample could have been influenced by the 2009 USPSTF revised recommendations for mammography screening. They also echoed Carlos et al.’s sentiment that there may be a ceiling effect on changes in screening rates in response to financial incentives, and inferred that the effect may be similar among race/ethnicity and income groups.
Xu et al. (2019) reported in their analytical cross-sectional study that there was no statistically significant difference in a beneficiary’s probability of receiving mammography after the ACA eliminated cost-sharing for Medicare enrollees based on self-report and fee-for-service claims data. With stratified analyses, they determined that poor Medicare enrollees had a statistically significant reduction in the odds of using mammography after the ACA mandate (Xu et al., 2019). This finding was not expected by the authors, as one of the defining goals of cost-share elimination is to reduce financial barriers to health care for low-income individuals with the hope of improving rates of utilization. Xu et al. (2019) was considered to be a “good” quality article that fulfilled all criteria on the JBI Critical Appraisal Tool.
Finally, Lurie and colleagues provided some findings on mammography use during the RAND Health Insurance Experiment, including that only 2% of eligible adult women received a screening mammogram during the study period, but made no formal conclusions on the relationship between cost-sharing and care utilization (Lurie et al., 1987). This randomized controlled trial was assigned a “moderate” quality rating as some of the study design, such as whether the treatment groups were similar at baseline and whether blinding was used, was unclear from the description of methods.
Cervical Cancer Screening and Pap Smear
Five studies (14.3%) provided information on the utilization rates of cervical cancer screening, most commonly Pap smear, following the elimination of cost-sharing. No study solely reported on changes in cervical cancer screening rates. Of these five studies, one analyzed national claims data, one used national survey data, one linked national claims data and survey data, one looked at regional claims data, and one utilized data from the RAND Health Insurance Experiment.
Two studies reported that cervical cancer screening rates increased with the elimination of cost-sharing for the service (Bhandari & Li, 2019; Lurie et al., 1987). Pap smear was the most common cancer screening procedure among adult beneficiaries in the RAND Health Insurance Experiment, and more women enrolled in the free care plan received at least one Pap smear compared with women in cost-sharing plans during the 3-year study period (a difference of 13.1%; Lurie et al., 1987). Bhandari and Li (2019) found in their “moderate” quality analytical cross-sectional study that self-reported use of Pap smear increased among women with Medicare-only insurance following the ACA cost-sharing mandate, and the adjusted prevalence of Pap tests among Hispanic women with Medicare-only insurance increased from 0.47 in 2009 to 0.91 in 2011. However, these increases were limited to the time period immediately following ACA implementation, as no additional increases were statistically significant following 2011 (Bhandari & Li, 2019).
The remaining items from our literature search suggested that the removal of out-of-pocket costs for Pap smear did not significantly impact utilization. In their retrospective cohort study, Busch et al. (2006) observed no significant change in Pap smear rates or trends after employer Alcoa eliminated cost-share for preventive services in employee plans. Busch et al. (2006) was of “moderate” quality, as treatment and control groups had different demographic characteristics and their observation period may have been too short to observe changes in screening utilization following cost-sharing removal. Steenland et al. (2019) and Xu et al.’s (2019) analytical cross-sectional studies determined that Pap smear rates decreased for Medicare beneficiaries post-ACA, but found no significant association between cost-sharing elimination and utilization rates of cervical cancer screenings. In their conclusions, both sets of authors linked decreases to changes in screening guidelines by the USPSTF prior to the implementation of cost-sharing elimination, suggesting that the shift to recommending triennial screening instead of annual screening for women older than 30 years overrode any changes cost-sharing manipulations may have enacted (Steenland et al., 2019; Xu et al., 2019). The changes in cervical cancer screenings and Pap smear utilization can be found in Table 3.
Summary of Changes in Utilization: Cervical Cancer Screening and Pap Smear (n = 5).
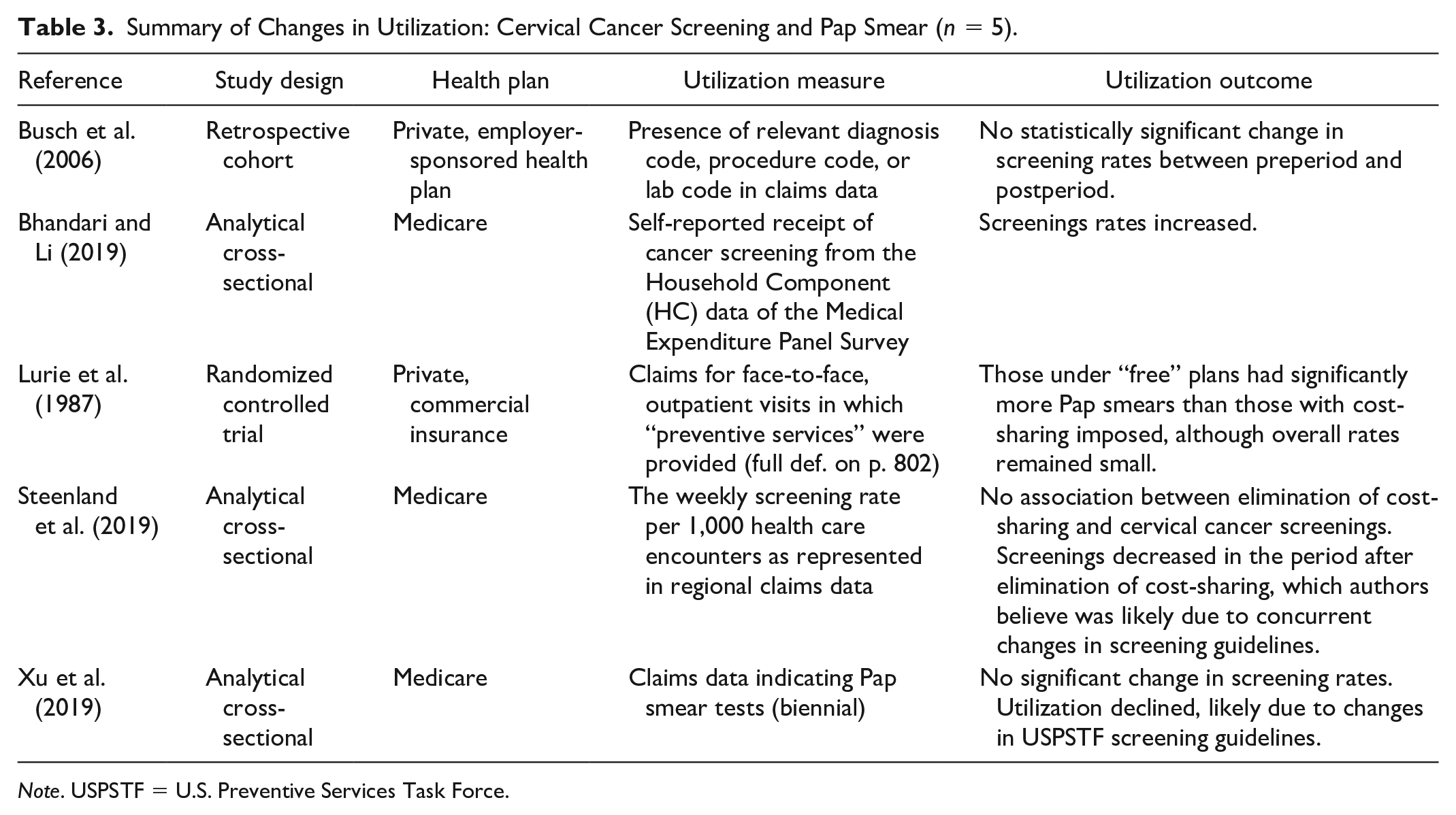
Note. USPSTF = U.S. Preventive Services Task Force.
Colorectal Cancer Screening and Colonoscopy
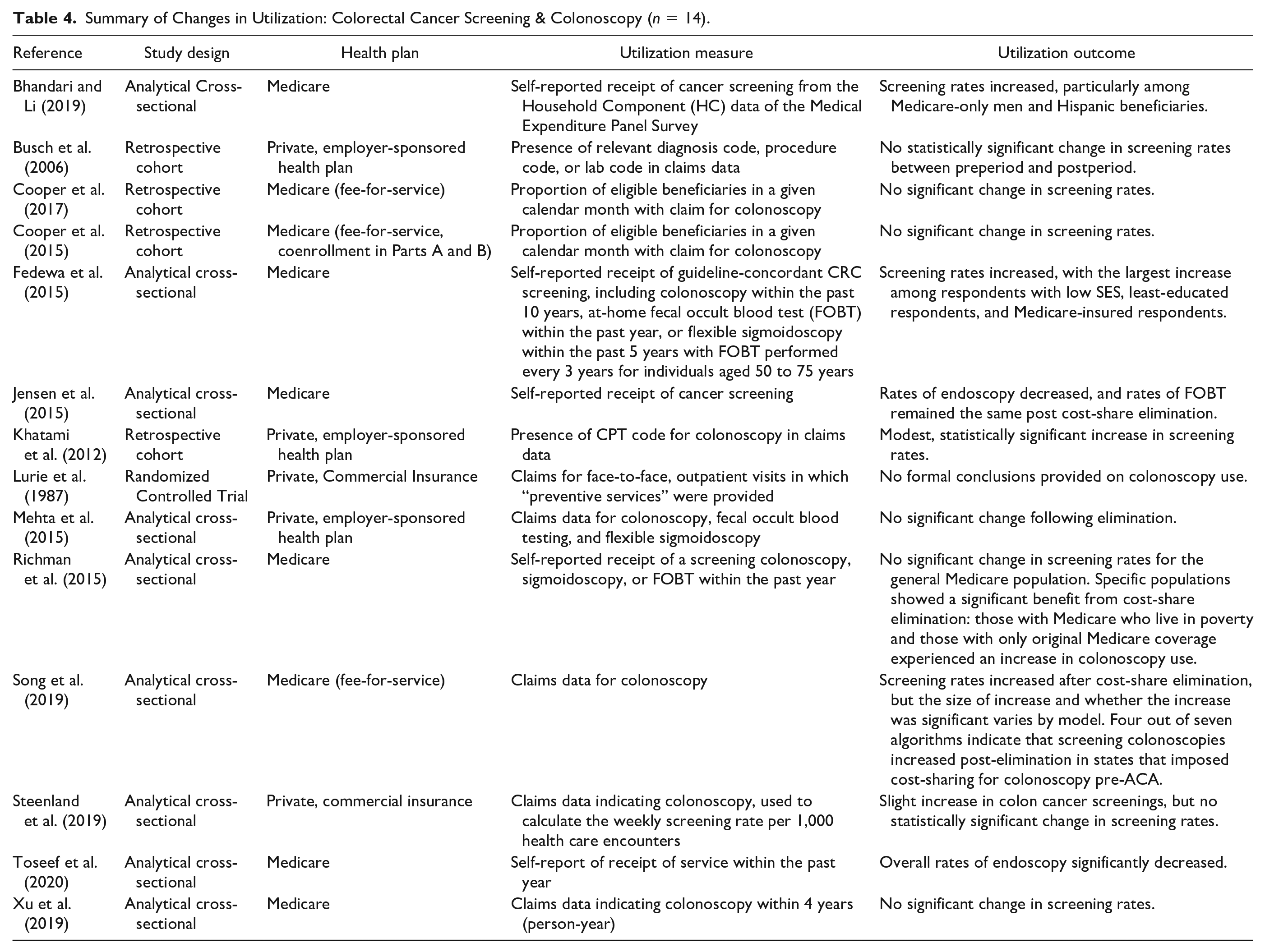
Fourteen of 35 (40%) articles from our literature search discussed colorectal cancer screening utilization, 3 of which (21.4% of colorectal cancer screening articles, 8.6% of total articles) only studied colorectal cancer screenings. The most studied form of colorectal cancer screening was colonoscopy, although some articles also provided findings on sigmoidoscopy. Some studies use the term “endoscopy” instead of colonoscopy. The data analyzed in the included studies varied, with five studies having used national survey data, another five used national claims data, two analyzed regional claims data, one looked at linked survey/claims data, and one analyzed health plan data from the RAND Health Insurance Experiment.
Most studies examining changes in colorectal cancer screenings determined that eliminating cost-sharing did not significantly affect utilization. Looking at beneficiaries of a single employer-sponsored health plan from 2003 to 2004, the cohort study by Busch et al. (2006) found no significant change in the rate of colorectal cancer screening after associated out-of-pocket costs were removed. However, cost-sharing for nonpreventive care rose at the same time cost-sharing for colorectal cancer screening was eliminated, confounding results and suggesting that the elimination of cost-sharing may have served as a protective factor for colorectal cancer screenings (Busch et al., 2006). Busch et al. (2006) was determined to be of “moderate” quality, with the main issues being an insufficient follow-up time for colorectal cancer screenings to occur in response to removal of cost-sharing, and lack of clarity around participants’ receipt of colorectal cancer screening prior to the study period.
Three studies that examined rates of colonoscopy in Medicare fee-for-service beneficiaries before and after the ACA cost-sharing mandate found no significant changes in utilization (Cooper et al., 2015; Cooper et al., 2017; Xu et al., 2019). All three articles were rated as “good” quality, but retrospective cohort studies Cooper et al. (2015) and Cooper et al. (2017) failed to detail how or if identified confounding factors were dealt with in their analysis. Both Cooper et al. (2015) and Cooper et al. (2017) looked at Medicare claims data from 2009 to 2010 and 2011 to 2012, but Cooper et al. (2017) looked specifically at men and women over 70 with an increased risk of colorectal cancer screening and who had not received a colonoscopy in the last five years. Cooper et al. (2015) simply looked at beneficiaries 70 or older who were due for screening. In their analytical cross-sectional study, Xu et al. (2019) looked at national survey data tied to claims data and measured the use of colonoscopy in a year for Medicare enrollees older than 50 years. Using grandfathered plans as a comparison group, Mehta et al. (2015), an analytical cross-sectional study, found that the ACA-mandated elimination of cost-sharing did not significantly change utilization of colonoscopy for men and women aged 50 to 64 years who were enrolled in small business health plans between 2008 and 2012. The authors noted that only preventive-coded colonoscopies were exempt from cost-share, with about 60% of eligible colonoscopies in the study being coded as preventive after the ACA mandate (Mehta et al., 2015). Mehta et al. was also given a “good” quality rating, with no concerns identified.
Busch et al. (2006), Cooper et al. (2015), Xu et al. (2019), and Mehta et al. (2015) all concluded that elimination of cost-sharing might not be a strong enough financial incentive to significantly increase utilization of colorectal cancer screening. Cooper et al. (2015) and Mehta et al. (2015) cited that other nonfinancial barriers remain for beneficiaries, like lost wages, fear of complications, and the invasive nature of the test. Mehta et al. (2015) also noted that patients and physicians may have been unaware of the cost-sharing elimination, as it is a relatively infrequent test (generally every 10 years). When looking at other secondary outcomes, both Xu et al. (2019) and Cooper et al. (2017) noted that disparities in colorectal cancer screening rates for low-income populations persisted, with Xu et al. (2019) finding that use of colonoscopy among poor Medicare enrollees further declined after the ACA.
Using data from the Massachusetts All-Payer Claims Database from 2009 to 2012, Steenland et al. (2019) found that despite an apparent increase in colon cancer screenings, the ACA-mandated elimination of cost-sharing did not significantly change the rate of utilization. Interestingly, the authors reported that the percentage of colon cancer screenings associated with a copay were strongly decreasing throughout the study period, and that the rate of decline was lessened after the mandate. This observation, however, was not robust in sensitivity analysis (Steenland et al., 2019). This analytical cross-sectional study was determined to be of “good” quality, but did not provide enough information describing the study subjects and setting in detail.
While most findings suggested that cost-sharing elimination had no effect on colorectal cancer screening rates, three studies from our literature search concluded that rates of colorectal cancer screening increased when cost-sharing was removed. Bhandari and Li (2019) and Fedewa et al. (2015) both reported that self-reported screening rates increased among Medicare beneficiaries following the ACA cost-sharing mandate. Among men with only Medicare coverage in 2011, the adjusted prevalence ratio of self-reported colonoscopy receipt in 2011 compared with 2009 was 1.13, which was statistically significant (Bhandari & Li, 2019). Among Hispanic Medicare beneficiaries, the adjusted prevalence ratio of self-reported colonoscopy receipt was statistically significant for the entire post-ACA observation period (2011-2014) relative to 2009 levels, with the adjusted prevalence ratio ranging from 1.28 to 1.44 during this period (Bhandari & Li, 2019). Fedewa et al. (2015) determined that the prevalence of colorectal cancer screenings increased by 9.8 percentage points among Medicare-only insured beneficiaries and by 5.9 percentage points among Medicare beneficiaries that had supplemental private insurance. After stratified analyses, Medicare beneficiaries with low socioeconomic status and the lowest self-reported education levels experienced the biggest increases in colorectal cancer screenings (Fedewa et al., 2015). Both analytical cross-sectional studies (Bhandari & Li, 2019; Fedewa et al., 2015) were determined to be of “moderate” quality, as both articles failed to demonstrate valid and reliable measurements of exposure and the outcome of interest. In a retrospective cohort study, Khatami et al. (2012) observed colorectal cancer screening rates after the University of Texas eliminated colonoscopy copayments for their employee health plan beneficiaries in fiscal year 2009, prior to the ACA mandate. The copay waiver was significantly associated with greater use of colonoscopy among enrollees, even after adjusting for age, sex, and beneficiary status (Khatami et al., 2012). The annual incidence of screenings in 2009 was 9.5%, a 1.5 percentage point increase compared with the expected incidence of 8.0% based on screening trends between 2002 and 2008 (Khatami et al., 2012). Khatami et al. (2012) presented no issues in the quality assessment and was given a “good” rating.
Additionally, in Richman et al.’s analytical cross-sectional analysis of data from the Medical Expenditure Panel Survey, the total population of Medicare enrollees did not experience a significant change in colonoscopy or sigmoidoscopy use following the ACA; however, Medicare enrollees who lived in poverty had a 5.7 percentage point higher rate of colonoscopy use post-ACA, and Medicare enrollees that did not have supplemental coverage had a 12 percentage point increase in colonoscopy use (2015). While significant, Richman and colleagues encourage their results to be interpreted with caution, as they examined multiple subgroups and there is uncertainty about their effect size estimates. Additionally, this article was assessed as “moderate” quality due to a lack of detailed information about the study subjects and setting, and a failure to provide valid, reliable measurements of the exposure and outcomes.
In their conclusions, Bhandari and Li (2019), Fedewa et al. (2015), Khatami et al. (2012), and Richman et al. (2015) all highlighted additional factors that need to be addressed when aiming to increase colorectal cancer screening rates to desired levels. Khatami et al. (2012) and Fedewa et al. (2015) suggested informing patients of the importance of colorectal cancer screenings and increasing rates of physician recommendations for testing as methods to improve screening utilization. Fedewa et al. (2015) and Richman et al. (2015) emphasized patients’ potential fears, embarrassment about screening methods, and feelings of inconvenience as barriers to receiving colorectal cancer screenings. Beneficiaries’ awareness of coverage for colorectal cancer screenings was also cited as an area that requires improvement, as many may not be aware of the ACA’s cost-sharing elimination for select preventive services (Bhandari & Li, 2019; Fedewa et al., 2015; Richman et al., 2015).
Song et al. (2019) was unique among included studies on colorectal cancer screenings as the outcomes of interest were the sensitivity and specificity of different published algorithms for classifying colonoscopies in addition to determining colonoscopy utilization rates among Medicare fee-for-service beneficiaries following the ACA mandate. This analytical cross-sectional study met all criteria outlined by JBI and received a “good” rating. The authors found that screening rates increased after cost-share elimination, but the magnitude of increase and whether the increase was significant varied by model. There was over a 30-fold difference in estimated magnitude of increase across the models (between 1.1 and 34 colonoscopies per 10,000 eligible persons; Song et al., 2019). Four out of seven algorithms indicated that screening colonoscopies significantly increased post-elimination in states that had imposed cost-sharing for colonoscopy pre-ACA (Song et al., 2019).
Two analytical cross-sectional studies reported significant decreases in self-reported colorectal cancer screenings among Medicare beneficiaries following cost-sharing elimination (Jensen et al., 2015; Toseef et al., 2020). Both studies were given a “moderate” quality rating, not meeting the criteria for valid and reliable measures of exposure and outcomes. Jensen et al. (2015) observed a 2.3 percentage point decrease in endoscopy receipt for Medicare seniors when comparing 2008-2010 and 2012 percentages, and Toseef et al. (2020) found a 3.17 percentage point reduction in endoscopy receipt between 2006-2010 and 2012-2016 time periods. Both studies highlighted the fact that nearly four fifths of Medicare beneficiaries already had supplemental health insurance that reduced or completely covered their out-of-pocket costs for preventive services pre-ACA mandate. They also echoed many of the additional factors other studies in this section have suggested for low colorectal cancer screening rates, such as lack of awareness of cost-sharing elimination, discomfort with some procedures, and the need for physicians to recommend or refer patients to the service. It is notable that Toseef et al. (2020) intended their study as a follow-up to Jensen et al. (2015), and utilized much of the same methodology.
Similar to their reporting of mammography, Lurie et al. (1987) included colorectal cancer screenings as one of their services of interest during the RAND Health Insurance Experiment randomized controlled trial but did not include formal conclusions on the effect of cost-share elimination on rates of utilization. They did report that 3% of adults aged 45 to 65 years received sigmoidoscopies during the study period, and less than 1% were considered preventive (Lurie et al., 1987). This study received a “moderate” quality score due to a lack of clarity around the measurement of exposure, condition, and outcomes. The changes in colorectal cancer screenings and colonoscopy utilization are summarized in Table 4.
Summary of Changes in Utilization: Colorectal Cancer Screening & Colonoscopy (n = 14).
Contraceptives and Sterilization
Of the 35 articles yielded by our search and subsequent screening process, eight discussed prescription contraceptives and sterilization (22.9%). All articles looked at populations with private health insurance plans. While Bell et al. (2018) also looked at study populations with other types of insurance, those aspects of the study were not included in our analysis because they did not meet stated criteria. Six of the eight studies that looked at contraceptives and sterilization utilized national data (Becker, 2018; Dalton et al., 2018; Heisel et al., 2018; Pace et al., 2016; Snyder et al., 2018; Weisman et al., 2019), one looked at a specific gynecology practice (Bell et al., 2018), and one analyzed longitudinal claims data from a regional health plan operating in the Midwest (Carlin et al., 2016). Refer to Table 5 for a summary of changes in contraceptive utilization following cost-share elimination.
Summary of Changes in Utilization: Prescription Contraceptives and Sterilization (n = 8).
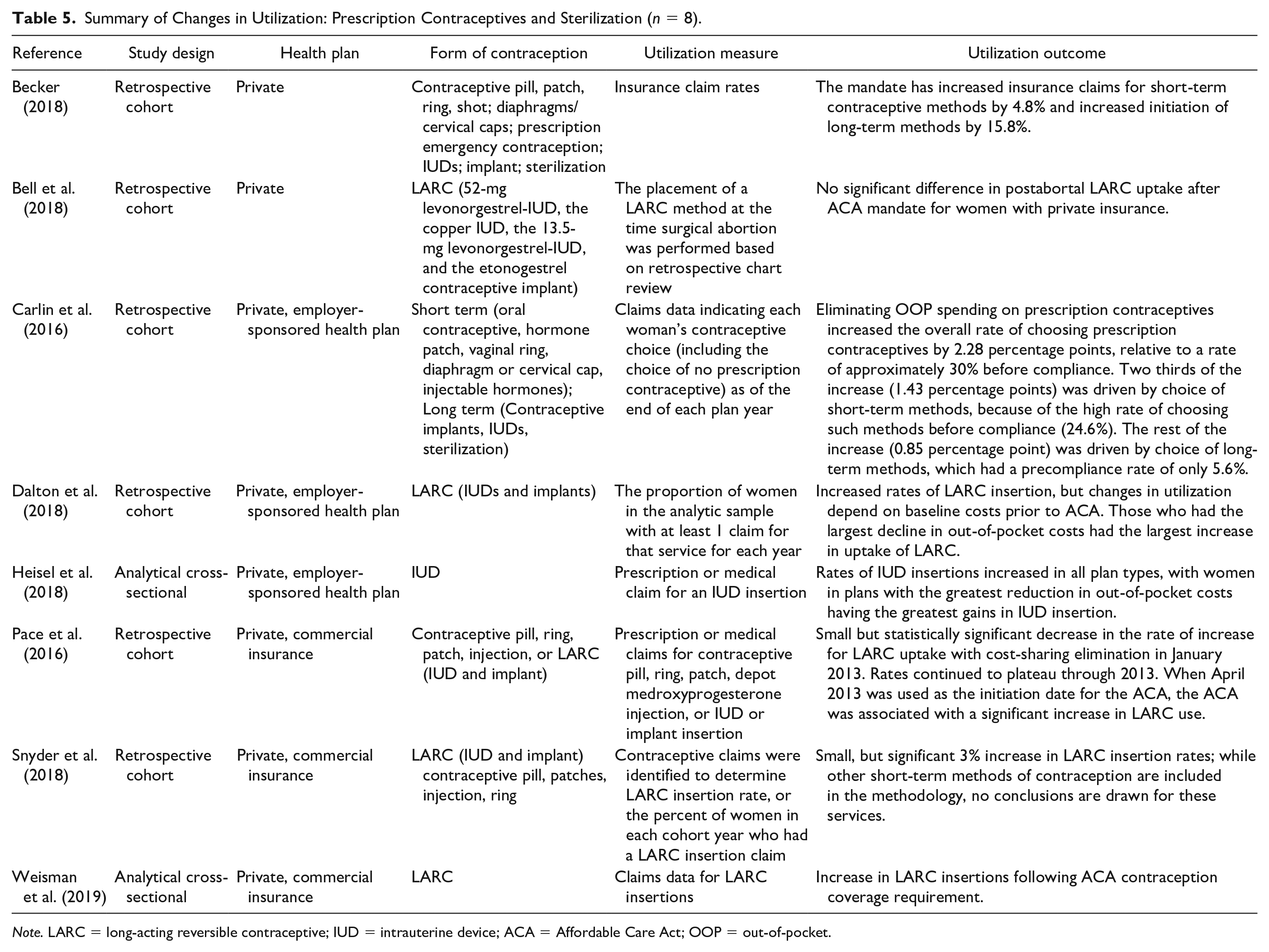
Note. LARC = long-acting reversible contraceptive; IUD = intrauterine device; ACA = Affordable Care Act; OOP = out-of-pocket.
Of the eight articles that analyzed contraceptives and/or sterilization, six reported increases in long-term birth control (intrauterine devices [IUDs], implants, or sterilization) uptake after cost-sharing elimination (Becker, 2018; Carlin et al., 2016; Dalton et al., 2018; Heisel et al., 2018; Snyder et al., 2018; Weisman et al., 2019), and two articles reported increases in short-term birth control methods’ (pill, patch, ring, shot, diaphragms or cervical caps) utilization after cost-sharing elimination (Becker, 2018; Carlin et al., 2016). Using claims data from a large national insurer, Becker (2018) compared women enrolled in plans that came into compliance with the ACA cost-sharing mandate to those enrolled in plans that did not and found that the elimination of cost-sharing led to 4.8% and 15.8% relative increases in short and long-term birth control claim rates, respectively. This retrospective cohort study was determined to be “good” quality, meeting all applicable criteria. The retrospective cohort study conducted by Carlin et al. (2016) analyzed claims data from a single insurer in the Upper Midwest and reported that the rate of women choosing any prescription birth control increased by 2.28 percentage points after the mandate, with 1.43 percentage points of the increase being driven by choice of short-term methods, and 0.85 percentage points by long-term methods. This study was determined to be of “moderate” quality due to unaddressed confounding variables and participants not being free of the outcome of interest prior to the study period. Both Becker (2018) and Carlin et al. (2016) found that long-term methods of contraception saw disproportionately greater increases than short-term methods.
Looking at LARC claims data for women aged 15 to 45 years and enrolled in an employer-sponsored health plan, the retrospective cohort study by Dalton et al. (2018) reported increased insertion rates, but changes in utilization were dependent on baseline costs prior to the ACA mandate. Those who had the largest decline in out-of-pocket costs had the largest increase in odds of uptake of LARC (Dalton et al., 2018). This article received a “moderate” quality assessment score, meeting all applicable criteria except for a lack of clarity around whether participants were free from the outcome prior to exposure. In their cross-sectional pre–post analysis using claims data, Heisel et al. (2018) had similar findings: rates of IUD insertions increased in all plan types after cost-sharing was eliminated, with women in plans with the greatest reduction in out-of-pocket costs seeing the greatest gains in IUD insertion. Heisel et al. (2018) was determined to be of “good” quality, meeting all criteria outlined by JBI for analytical cross-sectional studies. Both Dalton et al. (2018) and Heisel et al. (2018) noted that out-of-pocket costs represent only one barrier to utilization of long-term methods of birth control. Snyder et al. (2018) conducted a retrospective cohort study using national claims data from 2006 to 2014 to analyze how the utilization of contraception changed before and after the ACA cost-sharing mandate went into effect, and reported small, but statistically significant increases of LARC uptake following cost-sharing elimination. This article was given a “good” quality rating and met all applicable criteria except that participant demographics varied slightly between the cohorts. Weisman et al. (2019), an analytical cross-sectional study, found that insertions of IUDs and implants increased after the ACA mandated cost-sharing elimination. The authors also reported that even though median costs for LARCs remained zero each year after the mandate, there was an increase in mean out-of-pocket costs for IUDs in 2015-2016, as well as a decrease in the percentage of women paying $0 over the same time frame. The article cited three reasons for why this may have occurred: new IUDs may not have been covered, more employers may have been exempt from contraceptive coverage requirements in 2015-2016, and more employers may have been noncompliant with the mandate during this time frame. Weisman et al. (2019) was determined to be “moderate” in quality; the study participants and setting were not described in enough detail, and the authors did not identify potential confounding variables.
Two retrospective cohort studies reported no significant change or decreases in utilization of contraception after the elimination of cost-sharing (Bell et al., 2018; Pace et al., 2016). Looking at LARC uptake for privately insured women at the time of receiving a surgical abortion at a specific gynecology practice, Bell et al. (2018) found no change before and after the elimination of cost-sharing. The authors noted that they had a high number of beneficiaries with full LARC coverage before the ACA mandate took effect, but privately insured women with full or partial coverage were more likely to utilize a postabortal LARC method than privately insured women with no coverage after the mandate. They also stated that their unique study population of postabortion patients may have contributed to their results, citing the possibility that patients may have not wanted to discuss contraception on the day of the abortion, or may have wanted to follow up with their primary gynecologists (Bell et al., 2018). Bell et al. (2018) received a “moderate” quality rating, failing to identify and account for potential confounding factors and not having a sufficient follow-up time. Pace et al. (2016) conducted a retrospective cohort study similar to that of Snyder et al. (2018), but over a more limited time period (2010 to 2013). The study was assessed to be “good” quality, meeting all applicable criteria except for participants being clear of the outcome prior to exposure. The authors found that despite successful, significant decreases in cost-sharing following the mandate, LARC initiation rates did not increase as expected. Similar to the conclusions of Dalton et al. (2018) and Heisel et al. (2018), Pace et al. (2016) note that reducing out-of-pocket costs may not be sufficient to make LARCs accessible to everyone who needs them.
Additional Services
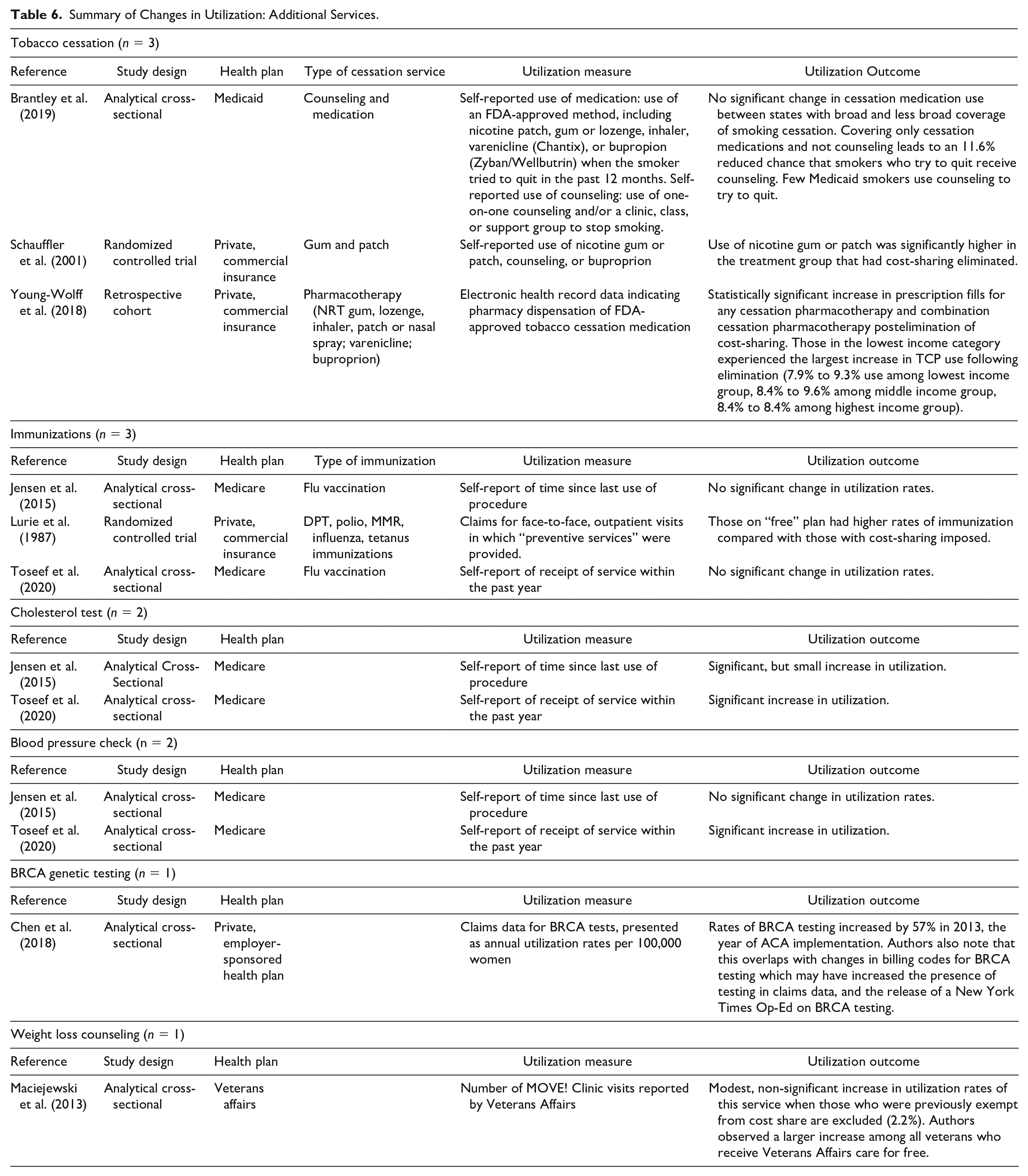
Eight articles (22.9%) analyzed the utilization of additional preventive services on the HealthCare.gov list, including tobacco cessation, immunizations, cholesterol tests, blood pressure checks, BRCA genetic testing, and weight loss counseling. A summary of changes in utilization rates for these services within our literature search can be found in Table 6. The articles featured data from a variety of sources - three utilized national survey data, one used regional survey data collected during a randomized experiment, two obtained data from national claims datasets, one used data from a regional claims dataset, and one utilized measurements collected at point-of-service.
Summary of Changes in Utilization: Additional Services.
Tobacco Cessation
Out of the three studies found on tobacco cessation, two of them found statistically significant increases in utilization of tobacco cessation pharmacotherapy, such as the nicotine gum and patch, following the elimination of cost-sharing. Schauffler et al. (2001) conducted a randomized control trial (RCT), which received a “good” quality ranking due to the inherent validity and reliability of randomized experiments and the study design meeting stringent requirements of RCTs, except for the blinding of outcome assessors. Researchers divided 1,200 participants into a treatment and control group, with the control group receiving a self-help kit and the treatment group receiving fully covered tobacco cessation benefits. Study results determined a higher utilization rate of nicotine patches and gum among the treatment group, with an adjusted odds ratio of 2.3 for the use of nicotine patch and/or gum in the treatment group, compared with the control group (Schauffler et al., 2001). Similarly, a retrospective cohort study by Young-Wolff et al. (2018) found that smokers enrolled in Kaiser Permanente Northern California were more likely (9.1% utilization vs 8.2% utilization) to use tobacco pharmacotherapy (gum, patches) following the elimination of cost-sharing in 2015 than in 2014. Furthermore, among patients that already had one tobacco cessation prescription, the percentage utilizing combination pharmacotherapy increased from 37.9% in 2014 to 42.3% in 2015 (Young-Wolff et al., 2018). This article was considered “moderate” in our quality assessment, as the cohorts were not recruited from the same group and smoking status was based on self-reported measures. An analytical cross-sectional study by Brantley et al. (2019) examined National Health Interview Survey data to determine the effect of Medicaid coverage policies on tobacco cessation programs and found no notable changes in the utilization of cessation medications as a result of Medicaid policies. This paper’s JBI quality was considered “good” as its main limitation, like most cross-sectional studies, was the reliance on self-reported measures to determine smoking status.
Immunization
With regard to the utilization of immunizations, a randomized control trial found that elimination of cost-sharing significantly increased the use of any immunization, with the highest increase found in children aged 0 to 6 years. However, 58.9% of children in this age group received immunizations in the free plan group, compared with 49.1% of children in the cost-sharing group (Lurie et al., 1987). The immunizations studied included diphtheria-pertussis-tetanus, polio, measles-mumps-rubella, tuberculosis skin testing, tetanus, and a yearly influenza vaccine for high-risk adults (Lurie et al., 1987). It is important to note that treatment allocation was not concealed in this study, and there was uncertainty regarding blinding and the similarity of groups at baseline, hence its “moderate” quality rating. Two analytical cross-sectional studies based on self-reported use of influenza vaccinations in a national survey found no significant change in utilization following the elimination of cost-sharing (Jensen et al., 2015; Toseef et al., 2020). In their study, Jensen and colleagues analyzed data from 3,042 traditional Medicare patients and found a slight but insignificant increase in the percentage of beneficiaries receiving a flu shot, with 70.4% of beneficiaries reporting receipt of a flu shot in the past year between 2012 and 2016, up from 66.3% between 2008 and 2010. It is important to note that services such as flu shots were mostly already covered prior to 2011, therefore explaining the stagnant utilization levels. Using data from the Medical Expenditure Panel Survey, Toseef et al. studied 27,124 Medicare beneficiaries and their use of certain preventive services and determined the proportion of beneficiaries receiving flu shots was unchanged following elimination of cost-sharing (Toseef et al., 2020). Both papers were given a “moderate” quality rating since using self-reporting in cross-sectional studies inhibits valid measurement of exposures and outcomes.
Cholesterol Test and Blood Pressure Check
A study analyzing the self-reported utilization of preventive services among Medicare beneficiaries determined that the elimination of cost-sharing resulted in a 2.35 percentage point increase in cholesterol tests and a 1.15 percentage point increase in blood pressure checks, relative to usage prior to the elimination of cost-sharing (Toseef et al., 2020). A similar study by Jensen and colleagues also found a slight increase in cholesterol tests following the elimination of cost-sharing. 90.2% of respondents reported receipt of the service in the postperiod, up from 84.1% during the preperiod (Jensen et al., 2015).
BRCA Genetic Testing
Research conducted by Chen et al. (2018) analyzed BRCA testing trends, which identifies genetic markers for breast cancer risk, among women aged 18 to 64 years in national claims data between 2003 and 2014. This analytical cross-sectional study found an increase in BRCA testing after elimination of cost-sharing, such that 2.68/100,000 women were tested in 2003 compared wiwth 240.99/100,000 in 2014. Using claims data, it was found that BRCA testing utilization experienced a relative increase of 57% in the span of 1 year, between 2012 and 2013. Comparatively, annual utilization rates had experienced relative increases of only 9%, 10%, and 13% in the 3 years leading up to 2012 (Chen et al., 2018). A “good” quality rating was given to this article; authors met objective JBI Critical Appraisal Tool standards, except for the lack of validity in their outcome measurement.
Weight Loss Counseling
Another preventive service of interest, weight loss counseling, experienced a slight increase in utilization rates on the elimination of a copayment (Maciejewski et al., 2013). The authors of this analytical cross-sectional study examined the use of a weight loss clinic among patients in the Veterans Affairs, and determined a nonsignificant 2.2% relative increase in the number of clinic visits for patients newly exempt from copayments. This article met every JBI requirement for cross-sectional studies, receiving a quality rating of “good,” and reinforcing the validity of their findings.
Discussion
To the best of our knowledge, this is the first rapid review examining the utilization of a broad range of preventive services following elimination of cost-sharing. Due to the wide variety of services, differences in study populations, and various methods of measuring utilization rates, it is challenging to develop a single conclusion on the impacts of eliminating cost-sharing on the utilization of preventive care services. Our goal in conducting this rapid review was to provide an overview of current literature studying the interaction of cost-sharing elimination as defined in our conceptual framework, and in doing so produce evidence for the effectiveness of V-BID implementation. The majority of findings in our literature conclude that cost-sharing elimination led to increases in utilization for select preventive services.
Cost-share elimination produced a wide array of changes in care utilization depending on the type of service analyzed. Out of 18 articles on breast cancer screening, 8 (44.4%) reported increases in screening rates following cost-share elimination for either the entire study population or a population subgroup, while 5 (27.8%) reported no significant change in screening rates, and 4 (22.2%) reported decreases in screening rates among the study population or population subgroup. Two (40%) of the five articles reporting on cervical cancer screening rates found that screening rates increased following cost-share removal, while the remaining three (60%) observed no significant change in screening rates. Several studies reporting on breast cancer and cervical cancer screenings conducted in response to the ACA cost-sharing mandate highlighted how changes in USPSTF guidelines in 2009 and 2010, respectively, may have influenced utilization rates for these services in addition to the removal of financial barriers. The 14 studies on colorectal cancer screenings also had mixed conclusions, with 6 studies (42.9%) indicating no change in screening rates, 5 (35.7%) reporting increases in screening rates among some or all of the study population, and 2 (14.3%) finding that screening rates decreased for their study population. Among the eight studies on contraceptives and sterilization methods, six (75%) reported increases in the use of at least one form of prescription contraceptive following cost-share elimination, with the largest observed increases observed in long-acting contraceptive use, while two groups (25%) observed no significant change in IUD placement with cost-share removal. For the remaining services represented in our literature search, the elimination of cost-sharing was associated with significant increases in cholesterol screening (two out of two articles), blood pressure checks (two out of two articles), and BRCA genetic testing (one article). Two out of three (66.6%) articles examining cost-share removal and tobacco cessation methods reported increases in cessation resource utilization, while the remaining article found no change in utilization. For immunizations, one study (33%) determined cost-share removal increased their utilization, while two (66%) more recent publications indicated there was no significant change in immunization rates postelimination. As the outcomes of cost-share elimination varied widely by service among items from our literature search, it is evident that additional research is needed to determine the impacts of removing cost-sharing on utilization of preventive services.
When evaluating the effects of cost-share elimination, it is essential to consider who will benefit the most from the removal of financial barriers. Many studies from our literature search, especially those focusing on cancer screenings, observed minimal or no changes in utilization following cost-share elimination for their study populations (Busch et al., 2006; Jensen et al., 2015; Mehta et al., 2015; Steenland et al., 2019). However, on conducting stratified analyses, several studies determined that select groups within their population benefited from the removal of these financial barriers (Dalton et al., 2018; Fazeli Dehkordy et al., 2019; Richman et al., 2015; Toseef et al., 2020). Changes in utilization may be localized or augmented among specific populations, including low-income individuals, Medicare beneficiaries lacking supplemental insurance, and those with high levels of cost-sharing for a service pre-elimination (Cooper et al., 2017; Dalton et al., 2018; Fedewa et al., 2015; Richman et al., 2015; Toseef et al., 2020). These findings suggest that low-socioeconomic groups and those who experience the greatest financial barriers to care appear to benefit the most from cost-sharing elimination. This is similar to prior research on eliminating cost-sharing for prescriptions following myocardial infarctions, which indicated that cost-share removal increased medication adherence and reduced rates of major vascular events or revascularization for vulnerable non-White populations (Choudhry et al., 2014).
Furthermore, many articles from our literature search highlighted that cost is not the only barrier, or even necessarily the most important barrier, to accessing preventive services. Carlos et al. (2019) and Fazeli Dehkordy et al. (2019) link their findings on breast cancer screening utilization to a potential ceiling effect, where financial incentives like copayment elimination will only be effective at raising screening rates to a certain level. It is possible that a similar financial ceiling effect exists for other preventive services as well. In addition to cost, discomfort with procedures, patients’ unawareness of what services are exempt from cost-share, misperceptions of the importance of preventive care, and a lack of physician recommendation for some services are all additional barriers to care for patients; additional interventions are needed to assist those facing these barriers in accessing the preventive services they need (Bhandari & Li, 2019; Cooper et al., 2015; Fedewa et al., 2015; Jensen et al., 2015; Mehta et al., 2015; Richman et al., 2015; Steenland et al., 2019). We will need innovative financial and alternative motivators to further encourage the use of preventive services.
Limitations
As of December 2019, 68 preventive services were listed as exempt from cost-share on the HealthCare.gov webpage used to design our inclusion criteria. However, our search results only report on changes in utilization for ten services from this list—less than one sixth of the total services available for consideration. Twenty-nine of our 36 articles studied at least one form of breast cancer screening, colorectal cancer screening, or prescription contraceptive. The overrepresentation of cancer screenings and contraceptives in our literature search starkly contrasts with a dearth of current information on the utilization of other effective preventive services and screenings, such as childhood immunizations, aspirin use for adults at high-risk of cardiovascular disease, and screenings for alcohol misuse (Maciosek et al., 2017). More research must be conducted on preventive service use beyond screening for cancer and prescriptive contraception methods, especially in the wake of the COVID-19 pandemic. Many health services, including preventive and elective care, were deferred in the first months of the COVID-19 pandemic (Whaley et al., 2020). The pandemic has also resulted in an economic downturn, and many Americans report trouble affording regular household expenses such as health care (Garner et al., 2020). Understanding the influence cost-sharing has on the utilization of preventive services will be especially relevant as we seek to improve health care delivery and mitigate adverse health outcomes following the COVID-19 pandemic.
Since included studies did not encompass all preventive services, with most studies focusing on contraceptives, mammograms, and colonoscopies, we could not generalize the results to all preventive services. Additionally, our research question relies on continuously evolving data and policy changes, so articles published after we began screening may not have been included in our final review. Similarly, changes in the USPSTF guidelines, such as those addressing breast cancer and cervical cancer screenings, may impact which preventive services are covered. Our review can therefore only accurately reflect the guidelines that were in place at the time this was written. Furthermore, our literature review search rationale included both primary and secondary research, as we considered all original research, independent of whether the author collected the data themselves. This may have resulted in challenges regarding the quality of our literature.
Last, while the majority of articles included in our review were considered to be of “good” quality, most included articles had observational study designs, which provide weaker evidence of effectiveness compared with experimental study designs (Porritt et al., 2014). Furthermore, half of the randomized controlled trials and quasi-experimental studies were rated as “moderate” in quality. Some of the limitations in study quality are related to the nature of research on cost-sharing; experiments on patients’ ability to afford potentially life-saving medical care could pose a significant ethical dilemma, and thus the feasibility of conducting these studies is limited. However, many of the “moderate” quality observational articles were rated as such because of unreliable methods of measuring exposure to cost-sharing or utilization of care. Future observational research into this topic must ensure that measures of exposure and outcomes are as accurate, valid, and reliable as possible to better elucidate the relationship between cost-sharing and use of preventive care.
Strengths of our review included a carefully scoped grey literature search; citation and reference tracking to increase search sensitivity and reduce publication bias; and a thorough appraisal of methodological quality for included articles. Furthermore, the broad scope of our literature review is a strength in itself, and the extensive results add value to a continuously changing health care landscape.
Conclusion
This extensive analysis of original research articles indicates a significant level of variability regarding utilization rates of preventive care following the elimination of cost-sharing. Within the categories of preventive service for which literature was available, the results were inconsistent, making it difficult to establish definitive conclusions. A majority of findings showed increases in use following cost-share elimination, and studies that included socioeconomic status reported that those who were financially vulnerable incurred substantial increases in utilization. More research needs to be conducted to broaden the types of services represented in the literature, and to provide more clarity on how coverage of a service impacts its utilization. This review suggests that additional factors beyond cost-sharing may affect service access, including educating patients and practitioners, addressing health care access and systemic health inequities, and informing beneficiaries of their available benefits and how to navigate a complex health care system.
Supplemental Material
sj-pdf-1-mcr-10.1177_10775587211027372 – Supplemental material for Utilization Impact of Cost-Sharing Elimination for Preventive Care Services: A Rapid Review
Supplemental material, sj-pdf-1-mcr-10.1177_10775587211027372 for Utilization Impact of Cost-Sharing Elimination for Preventive Care Services: A Rapid Review by Hope C. Norris, Haley M. Richardson, Marie-Anais C. Benoit, Beth Shrosbree, Judith E. Smith and A. Mark Fendrick in Medical Care Research and Review
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A. Mark Fendrick reports compensated consulting relationships with AbbVie Inc, Amgen Inc, Bayer Centivo, Community Oncology Association, Covered California, EmblemHealth, Exact Sciences Corporation, Freedman Health System, GRAIL, Harvard University, Health & Wellness Innovations, Health at Scale Technologies, MedZed, Merck & Co., Inc., Montana Health Cooperative, Penguin Pay, LLC, Phantom Pharmaceuticals, Risalto Health, Sempre Health, Inc, the State of Minnesota, US Department of Defense, Virginia Center for Health Innovation, Wellth, Inc, Yale-New Haven Health System and Zanzors; receiving research support from the Agency for Healthcare Research and Quality (AHRQ), Boehringer-Ingelheim, Gary and Mary West Health Policy Center, Arnold Ventures, National Pharmaceutical Council, Patient-Centered Outcomes Research Institute, Pharmaceutical Research and Manufacturers of America, Robert Wood Johnson Foundation, and the State of Michigan Centers for Medicare and Medicaid Services; serving as co-editor of the American Journal of Managed Care; and being a member of the Medicare Evidence Development and Coverage Advisory Committee and VBID Health, outside the submitted work. The remaining authors report no conflict of interest. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.