
Abstract
Health insurers use narrow and tiered networks to lower costs by contracting with, or favoring, selected providers. Little is known about the contemporary effects of narrow or tiered networks on key metrics. The purpose of this systematic review was to synthesize the evidence on how narrow and tiered networks impact cost, access, quality, and patient steering. We searched PubMed, MEDLINE, and Cochrane Central Register of Controlled Trials databases for articles published from January 2000 to June 2020. Both narrow and tiered networks are associated with reduced overall health care costs for most cost-related measures. Evidence pertaining to access to care and quality measures were more limited to a narrow set of outcomes or were weak in internal validity, but generally concluded no systematic adverse effects on narrow or tiered networks. Narrow and tiered networks appear to reduce costs without affecting some quality measures. More research on quality outcomes is warranted.
Introduction
Many health insurers selectively contract with providers by forming narrow provider networks that typically include fewer than a third of eligible clinicians or hospitals in a given geographic area (Bauman et al., 2016; Hall & Fronstin, 2016; Jacobson et al., 2016, 2017; Polsky et al., 2017). These networks allow health insurers to negotiate lower prices in exchange for promised higher patient volumes to included providers. Due to the anticipated savings from lower prices, insurers can offer lower premiums to patients, making provider networks a key component of the payer’s value-added service.
Narrow provider networks grew in popularity in the 1980s when this approach was employed by Health Maintenance Organizations (HMOs; Morrisey, 2001). In the 1990s, a backlash against HMOs resulted in the abandonment of many cost-saving strategies as HMOs evolved into Preferred Provider Organizations (PPOs). However, PPOs retained the concept of narrow networks, given the evidence that selective contracting resulted in lower prices (Melnick et al., 1992; Morrisey, 2001; Wholey et al., 1995; Zwanziger et al., 2000). Importantly, in response to provider and consumer complaints about HMO and PPO structures, and the perceived disruptions to health care markets, several state and federal entities regulated how payers can construct their narrow networks (Howard, 2014). Subsequently, some insurers introduced an alternative to narrow networks known as tiered provider networks. In a tiered provider network, the insurer categorizes providers into tiers based on their prices and, in some cases, their quality relative to other providers (Sinaiko et al., 2017). Low-cost, high-quality providers are placed in the preferred tier. Patients incur lower out-of-pocket costs if they choose to utilize providers from the preferred tier.
Narrow and tiered provider networks gained even more attention with the passage of the Affordable Care Act (ACA) due to regulatory constraints on plan benefit design, including essential health benefits and modified community ratings (Buntin & Graves, 2020). Subsequently, narrow and tiered provider networks proliferated in the ACA Marketplaces, with approximately half of first-year insurers using these types of provider networks to offer competitive premiums (Buntin & Graves, 2020; Howard, 2014). Although the prevalence of plans with narrow provider networks in the ACA Marketplaces declined to 21% in 2017, narrow networks are common in other markets. For example, Medicare Advantage plans limited choice of providers for 33% of enrolled beneficiaries in 2017, with further projected increases (Feyman et al., 2019). Approximately, 14% of employers with 50 or more workers offered a tiered network plan in 2019 (Kaiser Family Foundation, 2019). Despite the growing popularity of narrow and tiered provider networks, little is known about their contemporary effects on key health care metrics. The purpose of our systematic review was to synthesize more recent evidence to examine the effects of narrow and tiered networks on a broad array of health care metrics.
New Contributions
Our systematic literature review provides a comprehensive synthesis and critical appraisal of the effects of narrow and tiered networks on access to care, costs, quality, and patient steering. A prior review of the literature focused on the effects of selective contracting used by HMOs in the 1990s (Morrisey, 2001). Although selective contracting is one of the key design features of narrow and tiered networks, our review includes a broader set of outcomes measures that were not studied in the context of selective contracting. Our review highlights contemporary and methodologically rigorous studies published since 2000. Finally, given changes in regulatory, payment, and overall market conditions since the early days of HMOs/PPOs, our review provides useful insights into whether and how narrow and tiered networks affect a wide range of outcomes. As such, our findings will be of interest to policy makers, health care purchasers, and other stakeholders interested in the effects of these specific insurance plan designs.
Conceptual Framework
Narrow and tiered networks are common strategies used by insurance companies to obtain greater market share, control costs, and offer competitive premiums to consumers. In narrow networks, consumers are offered a health plan that limits provider choice in exchange for lower premiums. Given their design, narrow networks may influence important health system outcomes, such as costs, access, and quality of care. Specifically, insurers negotiate lower prices with providers to be included in a narrow network. Providers make price concessions in exchange for promised higher patient volumes, or risk being excluded from the insurer’s network (Corlette & Volk, 2014). Insurers can then offer more competitive premiums, thus attracting more enrollees. Given the lower negotiated prices, narrow networks may lead to lower overall health costs or reduced expenditures in certain service areas. Reduced costs may also be attainable in narrow networks because patients who seek care from providers outside of the defined network are penalized with higher cost-sharing requirements, thereby steering enrollees toward providers with fewer out-of-pocket costs.
Beyond limiting access to all providers, narrow networks also exclude certain providers with high-cost specialized expertise (Schleicher et al., 2016). Subsequently, sicker patients or individuals who require highly specialized care are less likely to choose a narrow network plan. Thus, patients enrolled in narrow networks may have poorer access to care due to limited provider choices. Finally, because insurers using narrow networks are able to choose and negotiate with providers based upon quality performance or willingness to improve care (Burns, 2012; Corlette & Volk, 2014), narrow networks may be associated with higher quality of care.
Tiered networks are also based on a combination of quality, cost, efficiency, or some other factors. In tiered networks, consumers face lower cost-sharing requirements when seeking care from providers in the preferred tier and higher cost-sharing when care is obtained from providers in other less-preferred tiers. Insurers make decisions on which tier to assign providers based on cost and/or quality determinations. Insurers can further negotiate lower prices by threatening to place a provider into a disadvantageous market tier that makes them less appealing to patients due to higher cost-sharing requirements. Subsequently, providers may agree to lower prices and/or delivery of high-quality care in exchange for remaining in the preferred or most advantageous tier. As such, tiered networks may result in lower costs and/or higher quality of care. Finally, tiered networks incentivize patients to seek care by preferred providers—but their choice is not limited if they are willing to pay higher cost sharing. Thus, access to care may not be affected by tiered networks.
Method
Our study was conducted consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). We assessed the quality of evidence using modified Oxford Centre for Evidence-based Medicine framework (see Supplemental eTable 1; “Oxford Centre for Evidence-Based Medicine: Levels of Evidence,” 2020).
Identification and Selection of Studies
We included empirical, peer-reviewed, U.S.-based, English-language studies that examined how narrow or tiered provider networks effect key health care metrics, such as access to care, costs, quality, and patient steering outcomes. We excluded letters to the editor, research letters, policy briefs, and other publications that were either nonempirical or had not been peer reviewed. We also excluded studies that did not have a clearly described comparison or control group. For example, we excluded studies that solely focused on assessing the proportion of all providers available in narrow networks.
We searched PubMed, MEDLINE, and the Cochrane Central Register of Controlled Trials databases, using several keywords associated with narrow and tiered networks, for studies published from January 2000 to June 2020. The complete search strategy is presented in the Supplemental eAppendix 1. First, two reviewers (O.M. and H.T.) independently screened and reviewed the titles and abstracts based on the inclusion criteria described above. Next, the two reviewers conducted a full-text screening of studies that met the inclusion criteria. Finally, a snowball technique was used to screen the reference lists of included studies for additional articles that the database searches might have missed. At each stage, the reviewers met and discussed any disagreements that were then resolved through consensus with the third author.
Data Extraction
We developed a standard coding sheet to extract data from each included article. The coding sheet elements were selected based on study characteristics and outcomes that could vary from one study to the next, such as study design, data source, and type of network examined. The coding sheet was pilot tested by having the two reviewers independently extract all data elements from several randomly selected included studies. Refinements to the coding sheet were made until near-perfect inter-rater reliability was achieved on extracted elements. All included studies were then analyzed, and their data extracted by at least one reviewer. When challenges arose with using the coding sheet, the authors made group decisions based on consensus during regular meetings.
From each included study, we extracted the following information as captured on the coding sheet: study design (experimental or quasi-experimental [QE] vs. others (simple observational), network type (narrow vs. tiered), network scope (hospital, physician, or both), and type of insurance plan studied (employer-sponsored, ACA Marketplace, or Medicaid). In addition, we extracted data on all unique analyses reported in each included study. We considered an analysis unique if it examined a discrete outcome (e.g., outpatient costs, number of prescriptions) or examined the same outcome in a different population (e.g., change in premiums for single vs. family beneficiaries).
We also grouped all dependent variables from each of the included unique analyses into the following categories: access to care, health care costs, quality of care, or patient steering. Per the Agency of Health care Research and Quality (“Elements of Access to Health Care,” n.d.), we defined access to care as “having the timely use of personal health services to achieve the best health outcomes.” Thus, we grouped insurance coverage, use of health services, and timeliness of care-related outcomes in the access to care category. Outcomes such as insurance premiums and health expenditures were coded as health care costs. Using the Institute of Medicine’s definition, we defined quality of care as the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge (Institute of Medicine (U.S.) Committee to Design a Strategy for Quality Review and Assurance & Lohr, 1990). We grouped analyses under the patient steering category if they focused on such items as patient likelihood of switching providers, and provider market share. Finally, we extracted the reported effect of narrow/tiered networks on each discrete outcome by coding it as a “desirable” (e.g., lower costs, better quality), “undesirable” (e.g., increased wait times to see a provider, higher readmission rate), or “no effect” (e.g., no statistically significant difference in outcomes) based on the conclusions of each study’s authors.
Finally, two reviewers (O.M. and H.T.) applied the modified Oxford Centre for Evidence-based Medicine framework to appraise the quality of evidence in each study (“Oxford Centre for Evidence-Based Medicine: Levels of Evidence [March 2009],” 2020; see Supplemental eTable 1). Each study was given a numerical score, ranging from 1 to 5, with lower scores representing higher quality of evidence presented within the study. Given the lack of randomized controlled trials of the tiered/narrow network effects, we assigned the highest ranking of “2” to studies using a QE design. The “3” and “4” ratings were assigned to studies with designs weaker in internal validity. As we excluded expert opinions, none of our studies were given a “5” ranking. We used quality ratings to assess whether our findings may be driven by more rigorous studies. We conducted several robustness checks by limiting analyzes to QE studies, which received the highest quality appraisal score based on the Oxford Centre for Evidence-based Medicine Framework.
Data Analysis
We analyzed findings separately for articles that focused on narrow versus tiered networks. First, we used descriptive analyses to examine the distribution of key variables in individual analyses extracted from included articles. Next, we analyzed the percentage of analyses, by outcome category, associated with a change in the outcomes due to the reported effects of the narrow/tiered networks. We purposefully highlighted how the findings from analyses that used designs with stronger internal validity (e.g., experiments or QEs) differed from analyses that employed simple observation designs. To address the issue of variability in the number of analyses nested within articles, we examined the bivariate relationship between narrow or tiered networks and desirable outcomes using a logistic regression with robust clustering. All analyses were conducted in STATA Version 16.1 (StataCorp LLC, 2021).
Results
Our keyword searches identified 1,257 unique studies for title and abstract screening of which 36 studies were identified for further full-text review. Upon full-text review and the snowballing process, 24 studies met the inclusion criteria (see Supplemental eFigure 1 for the PRISMA flow diagram). In general, studies that were excluded tended to focus on outcomes outside the scope of our study, such as consumer valuation, consumer responsiveness, or equilibrium in health care markets (Ericson & Starc, 2015; Ho, 2009; Prager, 2020).
As shown in Table 1, most included studies focused on narrow networks (n = 17, 70.8%), whereas the remaining studies assessed tiered networks (n = 7, 29.2%). More than half of the included studies examined physician networks only (54.2%), with fewer studies focusing on hospital networks (20.8%) or both provider types (25%). The majority of studies examined employer-sponsored health insurance plans (n = 18, 75%). No included studies used an experimental study design, but 37.5% of studies (including 48.8% of included analyses) used a QE research design. The remaining were all simple observational studies and primarily consisted of descriptive, cross-sectional, or repeated cross-sectional study designs (n = 15; 62.5%). Overall, half of the studies examined access to care outcomes (n = 12, 50%) and several studies included analyses that examined more than one outcome measure. Studies examining cost of care (n = 9, 37.5%) or quality of care (n = 8, 33.3%) outcomes were also common. Most studies were conducted on populations from settings within a single state (n = 14, 58.4%).
Characteristics of Included Articles That Examined the Effects of Narrow or Tiered Networks on Outcomes (N = 24).
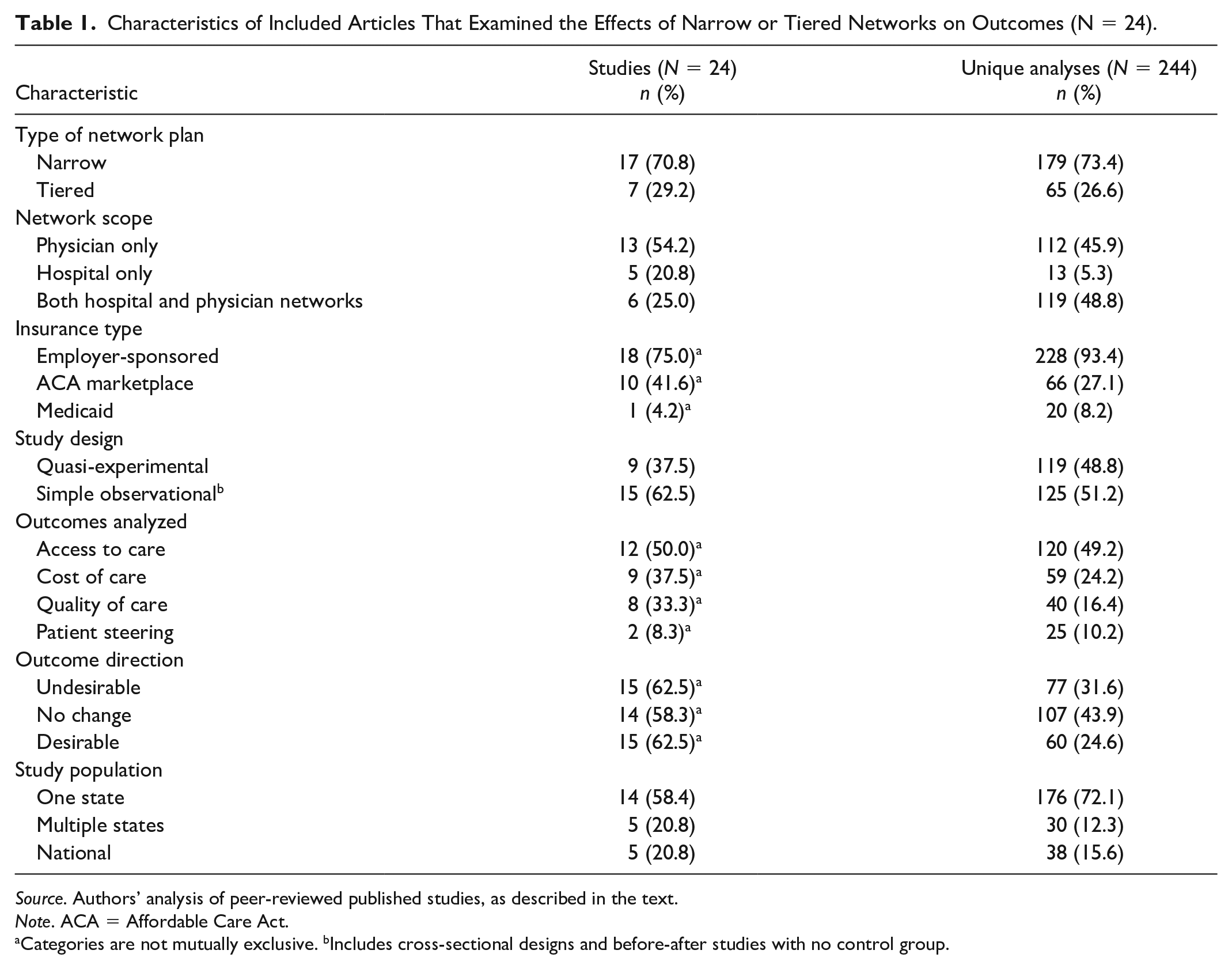
Source. Authors’ analysis of peer-reviewed published studies, as described in the text.
Note. ACA = Affordable Care Act.
Categories are not mutually exclusive. bIncludes cross-sectional designs and before-after studies with no control group.
We present our analyses for narrow and tiered networks separately and frame outcomes as either “desirable” (e.g., lower costs, better quality) or “undesirable” (e.g., increased wait times to see a provider, higher readmission rate) based on the nature of the measured effect or association. The results of the robust clustering analysis yielded similar findings to the simple bivariate analyses. As such, we present the bivariate analyses which are easier to understand.
Access to Care in Narrow Networks
Among studies focused on narrow networks, 116 analyses (65%) examined the effects on access to care (see Table 2; Atwood & Lo Sasso, 2016; Gillen et al., 2017; Gruber & McKnight, 2016; Haeder et al., 2015, 2016, 2019; Lo Sasso et al., 2006; McKenna et al., 2019; Polsky et al., 2018; Rosenthal et al., 2009; van den Broek-Altenburg & Atherly, 2020). The most common measure of access to care was “utilization of services” which included 58 analyses (Atwood & Lo Sasso, 2016; Gillen et al., 2017; Gruber & McKnight, 2016; Lo Sasso et al., 2006; McKenna et al., 2019; Rosenthal et al., 2009; van den Broek-Altenburg & Atherly, 2020). Of these, 35 analyses (60.3%; Atwood & Lo Sasso, 2016; Gillen et al., 2017; Gruber & McKnight, 2016; McKenna et al., 2019; Rosenthal et al., 2009; van den Broek-Altenburg & Atherly, 2020), including 29 QEs (Atwood & Lo Sasso, 2016; Gillen et al., 2017; Gruber & McKnight, 2016; Rosenthal et al., 2009), reported no difference in narrow versus broader networks. An additional 17 analyses (29.3%; Atwood & Lo Sasso, 2016; Gruber & McKnight, 2016; McKenna et al., 2019; van den Broek-Altenburg & Atherly, 2020), of which 11 were QEs (Atwood & Lo Sasso, 2016; Gruber & McKnight, 2016), reported a decrease in the service utilization attributable to narrow networks. Of note, approximately two-thirds (70.7%) of the QE analyses reporting a decrease in the service utilization came from two studies (Atwood & Lo Sasso, 2016; Gruber & McKnight, 2016). These two QE studies examined changes in the number of visits across several service (office, inpatient, outpatient, and laboratory visits) and provider types (primary care and specialty care). These two QE studies reported generally consistent findings, except regarding primary care utilization. Specifically, Gruber and McKnight (2016) reported an increase, whereas Atwood and Lo Sasso (2016) reported a decrease in primary care utilization following the narrowing of provider networks.
Proportion of Published Analyses Focused on Narrow Networks That Reported an Undesirable, Equivalent, or Desirable Outcome (N = 179 Analyses).
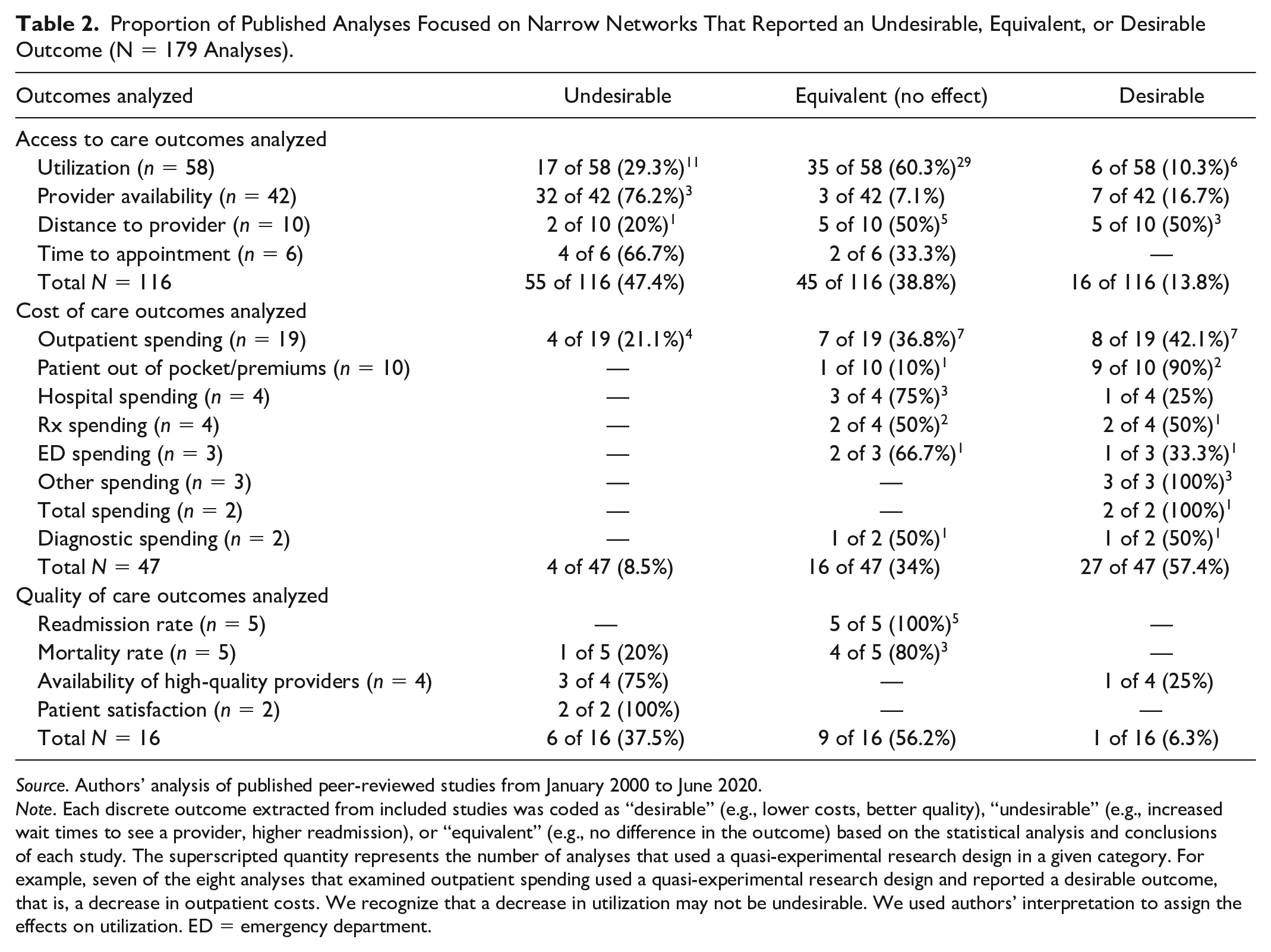
Source. Authors’ analysis of published peer-reviewed studies from January 2000 to June 2020.
Note. Each discrete outcome extracted from included studies was coded as “desirable” (e.g., lower costs, better quality), “undesirable” (e.g., increased wait times to see a provider, higher readmission), or “equivalent” (e.g., no difference in the outcome) based on the statistical analysis and conclusions of each study. The superscripted quantity represents the number of analyses that used a quasi-experimental research design in a given category. For example, seven of the eight analyses that examined outpatient spending used a quasi-experimental research design and reported a desirable outcome, that is, a decrease in outpatient costs. We recognize that a decrease in utilization may not be undesirable. We used authors’ interpretation to assign the effects on utilization. ED = emergency department.
The next most common access-related outcome in the literature was “provider availability,” which included all measures that examined the accessibility of providers to patients. Among the 42 analyses (Haeder et al., 2019; McKenna et al., 2019; Polsky et al., 2018; Rosenthal et al., 2009) that examined provider availability, 32 (76.2%), including three QEs (Rosenthal et al., 2009), reported undesirable effects. For example, patients who had previously seen a provider who was later excluded due to network narrowing, were more likely to discontinue visiting that provider (Rosenthal et al., 2009).
Other access-related outcomes included measures that examined “distance to a provider” (n = 10 analyses; Gruber & McKnight, 2016; Haeder et al., 2015) and “time to appointment” (n = 6 analyses; Haeder et al., 2016). Evidence from the studies that examined distance to provider had mixed results with 5 of 10 analyses (50%; Gruber & McKnight, 2016), all QEs, reporting no difference between narrow networks and their counterparts. Three of the remaining 10 analyses (30%; Gruber & McKnight, 2016), all also QEs, found that patients enrolled in narrow networks travelled shorter distances (a desirable effect) for primary care, outpatient hospital, and visits to their previous providers. Two remaining analyses (20%; Gruber & McKnight, 2016; Haeder et al., 2015), including 1 QE (Gruber & McKnight, 2016), reported an increase in patient distance to a provider (an undesirable effect). On the contrary, most of the analyses that focused upon time to appointment (n = 4; 66.7%; Haeder et al., 2016) reported an undesirable effect in narrow networks, whereby longer wait times were needed for a scheduled appointment with a requested provider (Haeder et al., 2016). Notably, all of these analyses used simple observational study designs.
Cost of Care in Narrow Networks
A total of 47 analyses examined the effects of narrow networks on health care costs (see Table 2; Atwood & Lo Sasso, 2016; L. Dafny et al., 2015; L. S. Dafny et al., 2017; Gillen et al., 2017; Gruber & McKnight, 2016; Polsky et al., 2016; Rosenthal et al., 2009; van den Broek-Altenburg & Atherly, 2020). The most common outcome studied was “outpatient spending” (n = 19 analyses; Atwood & Lo Sasso, 2016; Gruber & McKnight, 2016; van den Broek-Altenburg & Atherly, 2020). Most of these analyses found either no difference in costs (n = 7 analyses, all from QEs; Atwood & Lo Sasso, 2016; Gruber & McKnight, 2016) or a desirable (e.g., decrease) effect on spending (n = 8 analyses, seven QEs; Atwood & Lo Sasso, 2016; Gruber & McKnight, 2016; van den Broek-Altenburg & Atherly, 2020). A small fraction of analyses (n = 4; 8.5%; Gruber & McKnight, 2016), all from a single QE study, found that narrow networks were associated with increased spending in outpatient settings, specifically an increase in costs associated with visiting a new versus a previous provider.
The remaining cost-related outcomes included patient out-of-pocket costs or premiums, and costs from either hospital, prescription, emergency department, diagnostic, other, or total spending (Atwood & Lo Sasso, 2016; L. Dafny et al., 2015; L. S. Dafny et al., 2017; Gillen et al., 2017; Gruber & McKnight, 2016; Polsky et al., 2016; Rosenthal et al., 2009; van den Broek-Altenburg & Atherly, 2020). All of these analyses either found no difference in costs (n = 16 analyses including 15 QEs; Atwood & Lo Sasso, 2016; Gillen et al., 2017; Gruber & McKnight, 2016; van den Broek-Altenburg & Atherly, 2020) or a desirable effect resulting in decreased spending (n = 27, including 16 QEs; Atwood & Lo Sasso, 2016; L. Dafny et al., 2015; L. S. Dafny et al., 2017; Gruber & McKnight, 2016; Polsky et al., 2016; Rosenthal et al., 2009; van den Broek-Altenburg & Atherly, 2020).
Quality of Care in Narrow Networks
Overall, 16 analyses evaluated some measure of quality of care in narrow networks (see Table 2; Fortney et al., 2001; Gruber & McKnight, 2016; Haeder et al., 2015; Howard, 2008; Yasaitis et al., 2017). The most common quality of care outcomes included “readmissions” (n = 5 analyses; Gruber & McKnight, 2016) and “mortality rates” (n = 5 analyses; Gruber & McKnight, 2016; Haeder et al., 2015; Howard, 2008). Nine analyses (56.2%; Gruber & McKnight, 2016; Haeder et al., 2015), including eight QEs, found no difference in hospital readmissions or patient mortality rates in narrow networks.
Other quality-related outcomes included “availability of high-quality providers” (Haeder et al., 2015; Howard, 2008; Yasaitis et al., 2017) and “patient satisfaction” (Fortney et al., 2001). Four analyses, all from simple observational studies (Haeder et al., 2015; Howard, 2008; Yasaitis et al., 2017), evaluated whether narrow networks had similar availability of high-quality providers. Three of these four analyses (75%) reported fewer high-quality physicians or high-quality hospitals available within narrow networks (Haeder et al., 2015; Yasaitis et al., 2017). Two analyses examined patient satisfaction using simple observational designs and concluded that narrow networks were associated with an undesirable effect, particularly for enrollees living in rural areas (Fortney et al., 2001).
Tiered Networks
As shown in Table 3, a total of 65 analyses examined the effects of tiered networks (Brennan et al., 2008; Frank et al., 2015; Scanlon et al., 2008; Sinaiko, 2016; Sinaiko et al., 2017; Sinaiko & Rosenthal, 2014; Tackett et al., 2011).
Proportion of Published Analyses Focused on Tiered Networks That Reported an Undesirable, Equivalent, or Desirable Outcome (N = 65 Analyses).
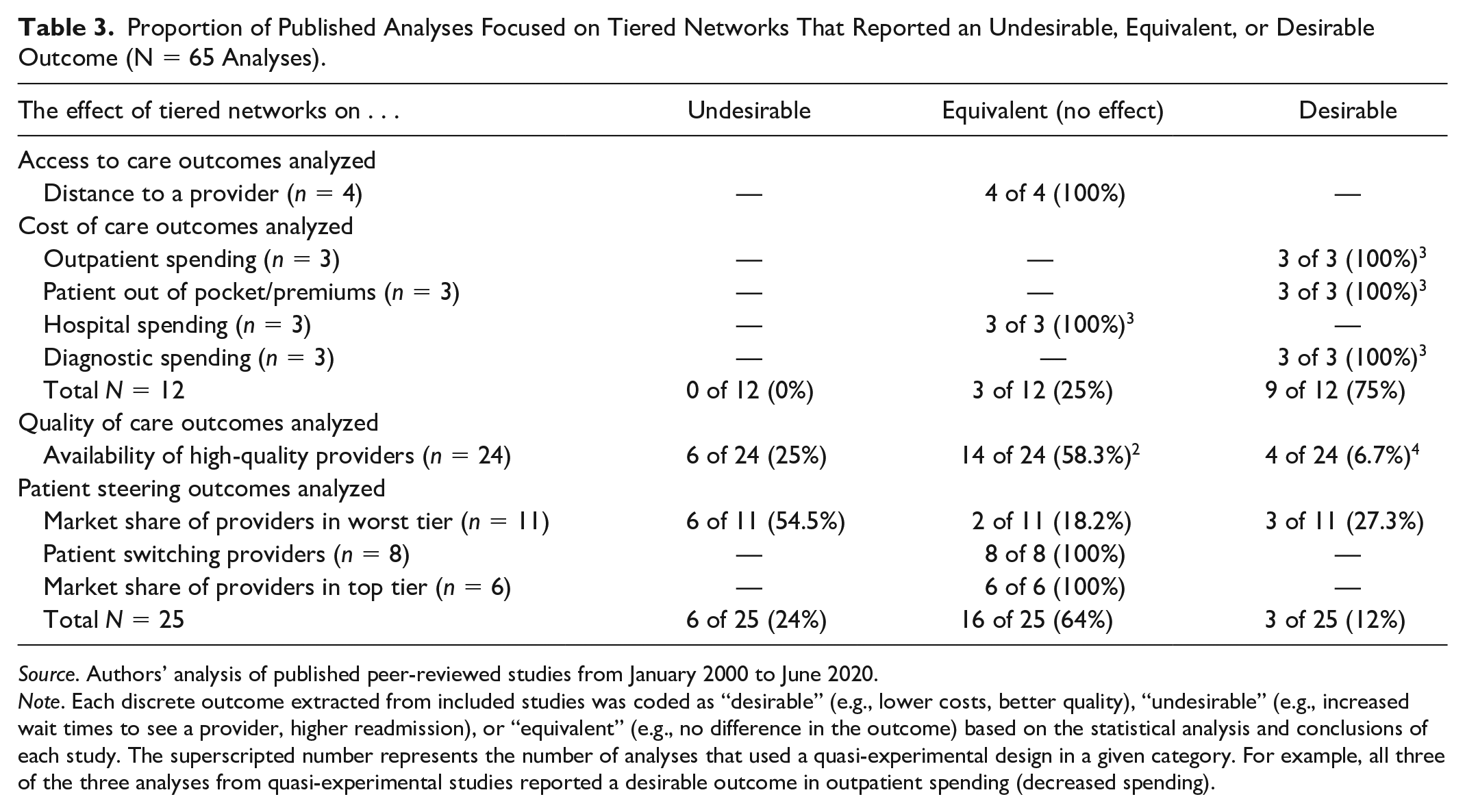
Source. Authors’ analysis of published peer-reviewed studies from January 2000 to June 2020.
Note. Each discrete outcome extracted from included studies was coded as “desirable” (e.g., lower costs, better quality), “undesirable” (e.g., increased wait times to see a provider, higher readmission), or “equivalent” (e.g., no difference in the outcome) based on the statistical analysis and conclusions of each study. The superscripted number represents the number of analyses that used a quasi-experimental design in a given category. For example, all three of the three analyses from quasi-experimental studies reported a desirable outcome in outpatient spending (decreased spending).
Access to Care in Tiered Networks
A single simple observational study (Tackett et al., 2011), including four analyses, found that enrollees had similar travel times to physicians in the preferred tier for four specialties, including adult primary care physicians, cardiologists, general surgeons, and obstetrician/gynecologists.
Cost of Care in Tiered Networks
All analyses that examined cost of care utilized QE designs. Tiered networks were associated with a decrease in outpatient spending (three of three analyses; Sinaiko et al., 2017), a decrease in out-of-pocket spending or premiums (three of three analyses; Sinaiko et al., 2017), and a decrease in diagnostic spending (three of three analyses; Sinaiko et al., 2017). Finally, tiered networks did not affect overall hospital spending (in three of three analyses; Sinaiko et al., 2017).
Quality of Care in Tiered Networks
Overall, 24 analyses examined the availability of high-quality providers in tiered networks (Brennan et al., 2008; Frank et al., 2015; Scanlon et al., 2008). Most of these analyses (58.3%; Brennan et al., 2008; Scanlon et al., 2008), including two QEs (Scanlon et al., 2008), found that the availability of high-quality providers was similar in tiered and non-tiered networks. In addition, four QE analyses (Frank et al., 2015; Scanlon et al., 2008) reported that patients enrolled in tiered networks were more likely to select higher quality hospitals for planned admissions relative to patients in non-tiered plans.
Patient Steering in Tiered Networks
Almost 40% of analyses that focused on tiered networks, all using simple observational designs, examined patient steering outcomes (Sinaiko, 2016; Sinaiko & Rosenthal, 2014). These analyses found no effect on patient likelihood of switching providers (eight of eight analyses; Sinaiko, 2016; Sinaiko & Rosenthal, 2014) and no effect on market share of providers in the top tier (six of six analyses; Sinaiko & Rosenthal, 2014). These findings suggest a null effect because tiered networks are intended to influence patient’s choice of provider. Similarly, two analyses that examined the market share of providers in the worst tier found no effect (Sinaiko, 2016). However, conflicting evidence, all from simple observational studies, found that providers in the worst tier have either a lower market share (n = 6 of 11 analyses; Sinaiko, 2016; Sinaiko & Rosenthal, 2014) or paradoxically a higher market share (n = 3 of 11 analyses; Sinaiko & Rosenthal, 2014) in tiered networks.
Additional Findings
Finally, we explored whether any extracted study characteristics, such as network scope (hospital, physician, or both) and insurance type (employer-sponsored, ACA Marketplace, or Medicaid) were associated with reported undesirable effects from narrow or tiered networks. We found that studies focused on ACA Marketplaces were more likely to report an undesirable effect attributable to narrow networks regardless of outcome studied (62.1% vs. 21.2%, p < .001). Furthermore, analyses that focus on physician networks only, whether narrow or tiered, were more likely to report undesirable outcomes (65.2% vs. 19.3%, p < .001).
Robustness Checks
We conducted several robustness checks by limiting analyzes to QE studies, which received the highest quality appraisal score based on the Oxford Centre for Evidence-based Medicine Framework. Among narrow networks, QE studies were more likely to find a desirable effect or no difference in access to care outcomes (69.0% vs. 25.9%, p < .001) and quality outcomes (100% vs. 25%, p = .002) than studies with simple observational designs and thus lower quality appraisal scores. We found no relationship between quality appraisal score and cost outcomes among narrow networks. We were unable to determine whether quality appraisal score was related to access to care, costs, or patient steering outcomes within tiered networks, due to a lack of studies with varying quality in these areas. Finally, we found no difference in outcomes related to quality of care among tiered networks regardless of the appraised quality of the study.
Discussion
Both narrow and tiered networks are associated with reduced overall health care costs for most, but not all, cost-related measures. Although the evidence is not as robust either methodologically (e.g., fewer QE designs) or in terms of the number of outcomes examined, quality and access do not appear to be affected by either type of network. Importantly, our findings are based on studies that used QE and simple observational designs commonly used in this literature. Nevertheless, QE studies were more likely to report a desirable effect or no difference in access to care and quality outcomes for narrow networks, thus strengthening our conclusion that narrow networks improve key outcomes.
Evidence reasonably strong in internal validity showed that narrow networks reduced out-of-pocket spending, as well as hospital, prescription, emergency department, diagnostic, and total spending, but not necessarily outpatient spending. Importantly, however, half of the analyses that examine cost of care in narrow networks were from a single QE study conducted on state employees in Massachusetts (Gruber & McKnight, 2016). Thus, existing evidence may have limited generalizability and future research should examine the effect of narrow networks on cost of care in other states or populations.
Although not always strong in internal validity, current evidence generally suggests narrow networks do not adversely affect access to care. Enrollees of narrow networks had similar rates of service utilization despite having fewer providers by design. Future studies should rigorously assess the relationship between provider availability and health care utilization among different patient subpopulations and determine whether this utilization adversely affects disease outcomes particularly among those with chronic conditions. Furthermore, there was contradictory evidence on how narrow networks affect travel distances from patients to providers. Importantly, studies using QE designs reported similar or sometimes shorter distances traveled by enrollees, thus suggesting an unanticipated desirable effect.
Narrow networks did not seem to negatively affect quality of care. Specifically, narrow network enrollees had similar readmissions and mortality rates relative to their counterparts in other health plans. Of note, studies that used QE designs were more likely to report desirable effects or no difference between quality of care between narrow and broader networks. However, the included studies were limited to a narrow set of quality outcomes and findings varied across studies. Subsequently, relatively little evidence exists regarding the effect of these networks among specific patient subpopulations and across a wider range of quality outcomes.
Similar to narrow networks, tiered networks reduced several cost measures, including patient out-of-pocket, outpatient, and diagnostic spending. However, tiered networks appeared to have no effect on overall hospital spending. Access to care and quality measures were unfrequently examined by existing studies in the context of tiered networks. Nevertheless, tiered network enrollees had similar access to high-quality providers, traveled similar distances for care, and were more likely to select high-quality providers for planned hospital admissions relative to patients in non-tiered plans. Furthermore, studies using simple observational designs found that tiered networks had no effect on patient likelihood of switching providers, which is contradictory to the intended effects of tiered networks. Given that tiered networks are intended to steer patients to high-value providers, additional studies are needed to better understand the mechanisms that drive patient choice in tiered networks. Of note, very few QEs have been published that examine effects of the tiered networks on various outcomes that appear in the literature focused on narrow networks.
Importantly, our findings were consistent when limiting our analyses to studies with the highest quality appraisal score (score = 2; see Supplemental eTable 1). In fact, limiting to studies with the highest quality appraisal score provided more frequent evidence of either desirable effects or no detrimental effects regarding access to care and quality outcomes within narrow networks. Thus, overall, the evidence with the strongest internal validity to date suggests that narrow networks do not adversely affect access or quality outcomes.
Our conclusions are based on a growing literature where a majority of studies used Marketplace data and other contemporary narrow and tiered networks. Of note, our findings are generally consistent with the main takeaways from the evidence on selective contracting from the 1990s (Morrisey, 2001). Our study provides a more comprehensive picture of the effects of narrow and tiered networks, given that we based our conclusions using studies that employed a broader set of access and quality outcomes, contemporary data, and a more granular approach to examining different types of networks. For instance, we found that studies using Marketplace data and those focused on physician-only networks were more likely to report undesirable effects of narrow and tiered networks. It is plausible that Marketplace networks, or their enrollees, have unique characteristics that drive a higher rate of undesirable effects among included studies. It is also plausible that the degree of network narrowness contributes to the undesirable effects. Recent evidence suggests that Marketplace networks tend to be narrower than employer-sponsored plans (Graves et al., 2020), thus potentially adversely affecting access and quality by increasing a patient’s likelihood for disrupting continuity of care. Future research should focus on assessing the reasons why studies of Marketplace networks report undesirable effects more commonly. Similarly, additional research is needed to understand why studies of physician-only networks reported undesirable effects more commonly.
It is worth noting a few limitations of our systematic literature review. First, given the variability in study designs, data sources, and different ways that previous authors have operationalized their dependent variables, we were unable to perform a traditional meta-analysis. Second, our search strategy may not have identified all relevant articles due to a wide range of synonyms used to describe narrow and tiered networks. To overcome this issue, we used a snowball technique to search and retrieve additional articles that may have used different terms to describe narrow or tiered networks, but recognize that some relevant articles may have been missed. Third, similar to other systematic reviews, our findings are susceptible to publication bias. In our review, 14 studies reported at least one nonsignificant result, but only two studies reported complete null results from all analyses. To the extent that academic journals preferentially publish studies with statistically significant findings, our systematic review is limited in its ability to fully consider the effects of narrow and tiered provider networks.
One of the key areas for further research should be examination of the effects of tiered networks, particularly when considering access to care and quality of care outcomes. Importantly, future studies should use outcome measures similar to those used in the literature that focused on narrow networks to facilitate comparisons of the effects of the two types of networks. Future studies should also use more granular measures of health outcomes or health status when assessing the effects of tired networks, including rates of appropriate preventive care, prenatal care, birth outcomes, and time from diagnosis to treatment for common conditions. Finally, given that studies often do not include detailed information regarding out-of-pocket cost differences between tiers, future research should comprehensively acknowledge and account for this information in analyses.
Conclusion
Based on the available evidence to date, narrow and tiered networks are associated with reductions in costs, without negative effects on access or quality of care. Thus, expanded use of narrow and tiered networks could contribute to higher value care in the United States.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587211055923 – Supplemental material for The Impact of Narrow and Tiered Networks on Costs, Access, Quality, and Patient Steering: A Systematic Review
Supplemental material, sj-docx-1-mcr-10.1177_10775587211055923 for The Impact of Narrow and Tiered Networks on Costs, Access, Quality, and Patient Steering: A Systematic Review by Olena Mazurenko, Heather L. Taylor and Nir Menachemi in Medical Care Research and Review
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was in part supported by the National Library of Medicine of the National Institutes of Health, under award number T15LM012502. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the National Library of Medicine.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.