
Abstract
Pregnancy-related complaints are a significant driver of emergency room (ER) utilization among women. Because of additional time for patient education and provider relationships, group prenatal care may reduce ER visits among pregnant women by helping them identify appropriate care settings, improving understanding of common pregnancy discomforts, and reducing risky health behaviors. We conducted a retrospective cohort study, utilizing Medicaid claims and birth certificate data from a statewide expansion of group care, to compare ER utilization between pregnant women participating in group prenatal care and individual prenatal care. Using propensity score matching methods, we found that group care was associated with a significant reduction in the likelihood of having any ER utilization (–5.9% among women receiving any group care and –6.0% among women attending at least five group care sessions). These findings suggest that group care may reduce ER utilization among pregnant women and encourage appropriate health care utilization during pregnancy.
Keywords
Introduction
Policymakers have targeted nonurgent or avoidable emergency room (ER) visits as a potential source of cost-saving because a significant share of ER visits are not considered medical emergencies (Agarwal et al., 2017; Agency for Health care Research and Quality, 2020; DeVries et al., 2013; Kilfoyle et al., 2017; Raven et al., 2013; Uscher-Pines et al., 2013; Serrano et al., 2018). Despite higher rates of insurance and access to routine visits, many pregnant women seek care in emergency departments (Kilfoyle et al., 2017). In a national study of ER usage, pregnancy-related complaints were among the top 10 reasons for ER visits for women between the ages of 15 and 64 years (Rui & Kang, 2017). Medicaid covers more than half of maternal/neonatal ER encounters, of which the most common drivers are hemorrhage, spontaneous abortion, early or threatened labor, delivery, and complications due to hypertension (Moore et al., 2017). Some evidence suggests that pregnant women with comorbid conditions are more likely to access ER visits, particularly if they have two or more comorbidities; however, little is known about the determinants of ER use among pregnant women, their likelihood of engaging in avoidable ER visits, or opportunities to reduce avoidable ER visits (Cunningham, Grilo, et al. 2017; Cunningham, Magriples, et al. 2017; Magriples et al., 2008; Malik et al., 2017; Vladutiu et al., 2019).
Group prenatal care is one of several evidence-based models aimed to enhance care delivery, appropriate care use, and maternal and infant outcomes. These models include birth centers, enhanced care management for pregnant women (often referred to as Maternity Care Homes), doula services, and home visitation services (Kozhimannil et al., 2013, 2016; Olds, 2006; Urban Institute, 2018). These interventions have in common an emphasis on addressing women’s needs for education and support and connecting women to other resources, with the practitioner spending more time with participants than the typical medically focused prenatal appointment (Urban Institute, 2018).
While several group-based models are in use, the CenteringPregnancy model has the largest research base. In this model, beginning in Weeks 16 to 20 of pregnancy, 6 to 12 women with similar due dates participate in 10 group sessions during their pregnancy. Group Sessions 1 and 2 are scheduled 1 month apart, followed by visits every 2 weeks for Sessions 3 through 10. Sessions begin with an individual routine medical examination for all women during the first 30 min and then transition to a 60- to 90-min facilitated group discussion led by a health care provider.
Women participating in the CenteringPregnancy model demonstrate increased participation in preventive health services during and after pregnancy, suggesting that the group model may increase health literacy or patient engagement (DeCesare et al., 2017; Grady & Bloom, 2004; Hale et al., 2014; Heberlein et al., 2020; Kennedy et al., 2009; Picklesimer et al., 2012; Roussos-Ross et al., 2020; Schellinger et al., 2017). Research investigating associations between group prenatal care participation and ER utilization is limited. An evaluation of group prenatal care implementation across multiple sites found that group prenatal care participants had lower prenatal health care costs and fewer ER visits after delivery, but no difference in ER visits prenatally (Urban Institute, 2018). Although a rigorously designed quasi-experimental study, this impact evaluation was limited to seven practices (529 births) where women were automatically enrolled in group care (vs. opting in) and did not examine both overall and avoidable ER utilization.
Group medical visits, where patients receive education, counseling, medical assessment, and clinical support from health care providers in a group setting, have been used to address a range of conditions, including diabetes, heart disease, chronic obstructive pulmonary disorders, dementia, and mood and anxiety disorders (Housden & Wong, 2016). While studies demonstrate substantial variation in context, implementation, and outcome measures, group medical visits now have an emerging body of evidence supporting their efficacy in improving patient trust, quality of care, self-management activities, and biophysical outcomes, with some studies of patients with diabetes demonstrating positive impacts on ER visits and hospital admissions (Edelman et al., 2012; Housden & Wong, 2016; Kirsh et al., 2017; Wadsworth et al., 2019). Our study investigates whether women participating in group prenatal care will have fewer total ER visits and fewer avoidable ER visits. Because the CenteringPregnancy curriculum is split up over 10 sessions, each with a distinct focus, we expect that the relationship between group prenatal care participation and ER utilization will be stronger among women with greater treatment exposure.
Conceptual Framework
The CenteringPregnancy model is based on a set of essential elements that align with national calls to improve prenatal care and with the Institute of Medicine’s tenets for redesigning health care (Rising et al., 2004). These essential elements include group facilitation principles (i.e., facilitative leadership, sessions have a plan, and group composition is stable), require that women are involved in self-care activities (i.e., learning to take their blood pressure), and that opportunity for socialization is provided. Theoretical underpinnings for the model include the self-efficacy theory, which posits that outcomes are influenced by perceptions of agency, and social support theory, where lack of support in pregnancy is associated with worse outcomes. CenteringPregnancy also follows principles of the midwifery model of care and feminist ideals, where patient–provider relationships are prioritized and power imbalances between clinicians and women are removed (Rising, 1998; Rising et al., 2004). In a synthesis of literature on shared medical appointments, including group prenatal care, multiple mechanisms explain how group visits work; of particular interest for this study, group visits can lead to patients’ increased health knowledge, confidence in managing their health, and relationships and trust of providers (Kirsh et al., 2017). A conceptual model of the relationship between group prenatal care and health care utilization is presented in Figure 1.
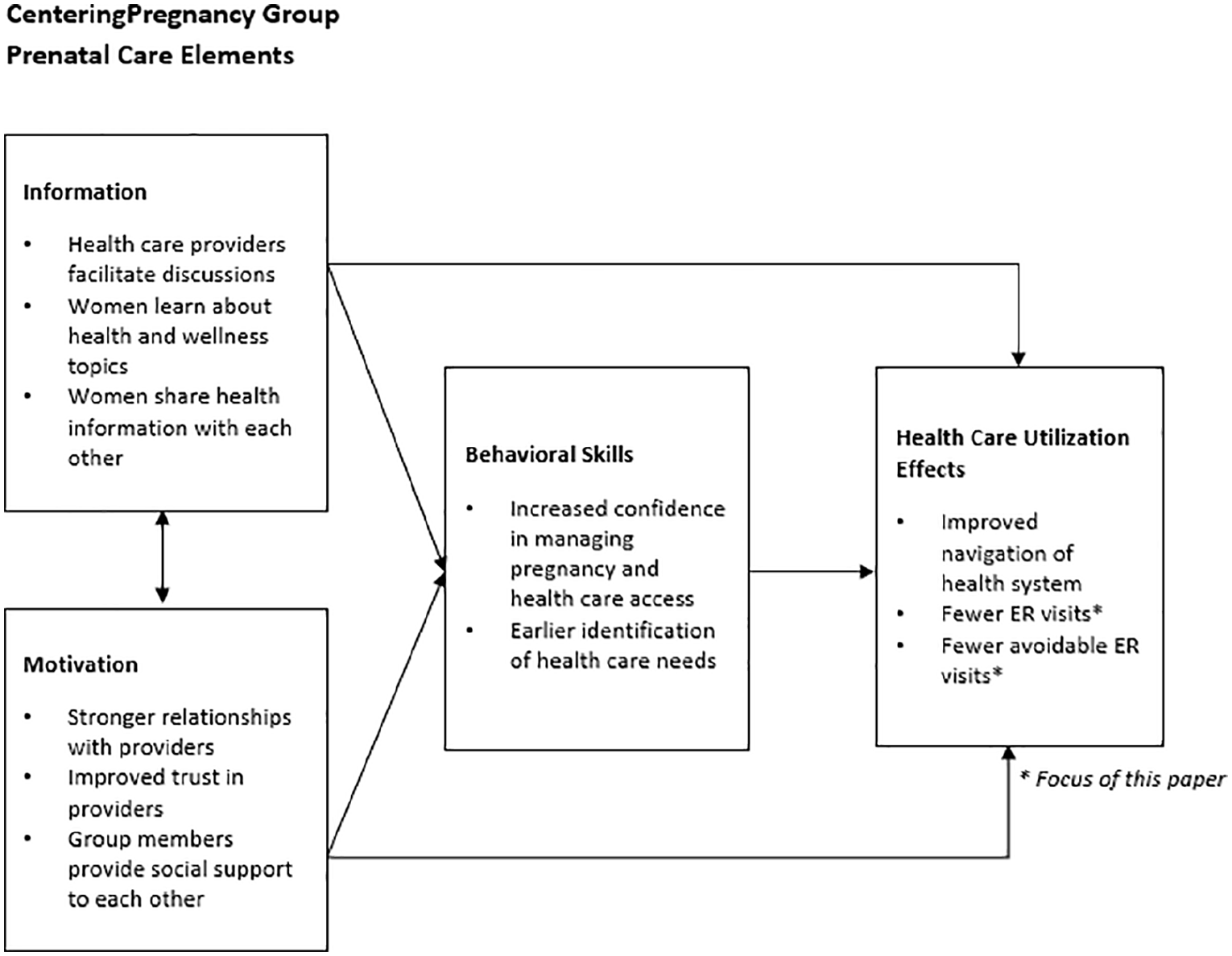
Conceptual Model of Group Prenatal Care and Health Care Utilization.
This model of group prenatal care uses an established curriculum covering a variety of topics, including not only those typically covered in traditional prenatal care (family planning, nutrition, and weight gain) but also those covered in childbirth preparation classes (breastfeeding, readiness for labor) (Rising, 1998; Rising et al., 2004). Topics of particular relevance to ER utilization are discussed at multiple times during the 10-session CenteringPregnancy curriculum. These sessions include information on when to seek emergency care versus calling the office for an appointment (Sessions 1, 4, 5, 7, 8, and 10), managing common discomforts of pregnancy (Session 2), recognizing preterm labor (Session 4), and preparing for labor and birth (Sessions 5, 6, 8, and 10). The established curriculum and additional time with providers may help pregnant women strengthen patient–provider relationships and improve health care literacy, enabling participants to better navigate the health care system, identify appropriate care settings, and reduce their stress and risky health behaviors.
In addition, participation in group care provides an opportunity to engage with other pregnant women during prenatal care visits, which may increase social support, encourage participants to change norms related to their health behaviors, and facilitate the sharing of information and experiences with one another. Family members and partners are also encouraged to attend sessions, creating another layer of support and imparting companions with knowledge that enables them to guide women to appropriate care settings during pregnancy.
New Contributions
In this article, we add to the existing literature by studying a large cohort of women receiving group prenatal care to evaluate their behavior in utilizing ER services, as well as being the first to examine the relationship between group prenatal care and avoidable ER visits. Using propensity score matching methods and administrative data from a multiyear initiative expanding access to group prenatal care in South Carolina, we compare ER utilization among pregnant Medicaid recipients participating in group prenatal care with those receiving traditional individual prenatal care. Our outcomes of interest include an indicator for any ER utilization, any avoidable ER utilization, total number of ER visits, and total number of avoidable ER visits. We identify avoidable ER visits using an updated version of the New York University (NYU) Emergency Department Visit Algorithm (Johnston et al., 2017). An additional contribution of this work is testing for heterogeneity in these relationships by stratifying the sample into low- versus high-risk pregnancies and restricting our study sample to women entering care prior to Month 5 of their pregnancy. After 5 months’ gestation (20 weeks), women entering care are often ineligible for group care as practices prioritize forming groups early in pregnancy to promote group cohesion and early pregnancy health education. In addition, restricting early entry to prenatal care increases the likelihood that the results represent a comparison of ER use after women begin prenatal care.
Method
Study Data and Population
Since 2012, the South Carolina CenteringPregnancy Expansion Project (SCCPEP) initiative has provided start-up funding, training, and technical assistance to 24 obstetric and family medicine practices to implement the CenteringPregnancy model of care (Crockett et al., 2019). All practices offer both CenteringPregnancy group prenatal care and individual prenatal care for patients who chose not to participate in group prenatal care or who are not eligible due to medical comorbidities, pregnancy complications, or late entry to prenatal care. Twenty-one of the 24 practices had data available for this study; previous research found that SCCPEP’s group prenatal care was associated with decreased rates of preterm birth and low birth weight births and increased rates of postpartum visit attendance (Crockett et al., 2019; Heberlein et al., 2020).
Practices maintained lists of group prenatal care participants, including patient identifiers and the total number of sessions attended. Biannually, each practice submitted their list of patients and the National Provider Identifiers of their obstetric care providers to the South Carolina Revenue and Fiscal Afairs (RFA) Office. The state office matched patient lists with birth certificates and identified a comparison group of births during the same month and year, which were delivered by the same providers using National Provider Identifiers. Medicaid claims for services delivered to the women in group prenatal care and the matched comparison group during pregnancy were linked to birth certificate data, and a de-identified data set was provided to the study team. We excluded duplicated births, pregnancies that were delivered at less than 20 weeks’ gestation or birth weight less than 350 g, multiple gestations, those with more than one birth during the study period, and women with missing values for any covariates of interest. Because claims data were only available for Medicaid-covered women, our sample excludes privately insured or uninsured women (Figure 2). The Prisma Health Institutional Review Board determined that informed consent was not required for the use of preexisting administrative data.
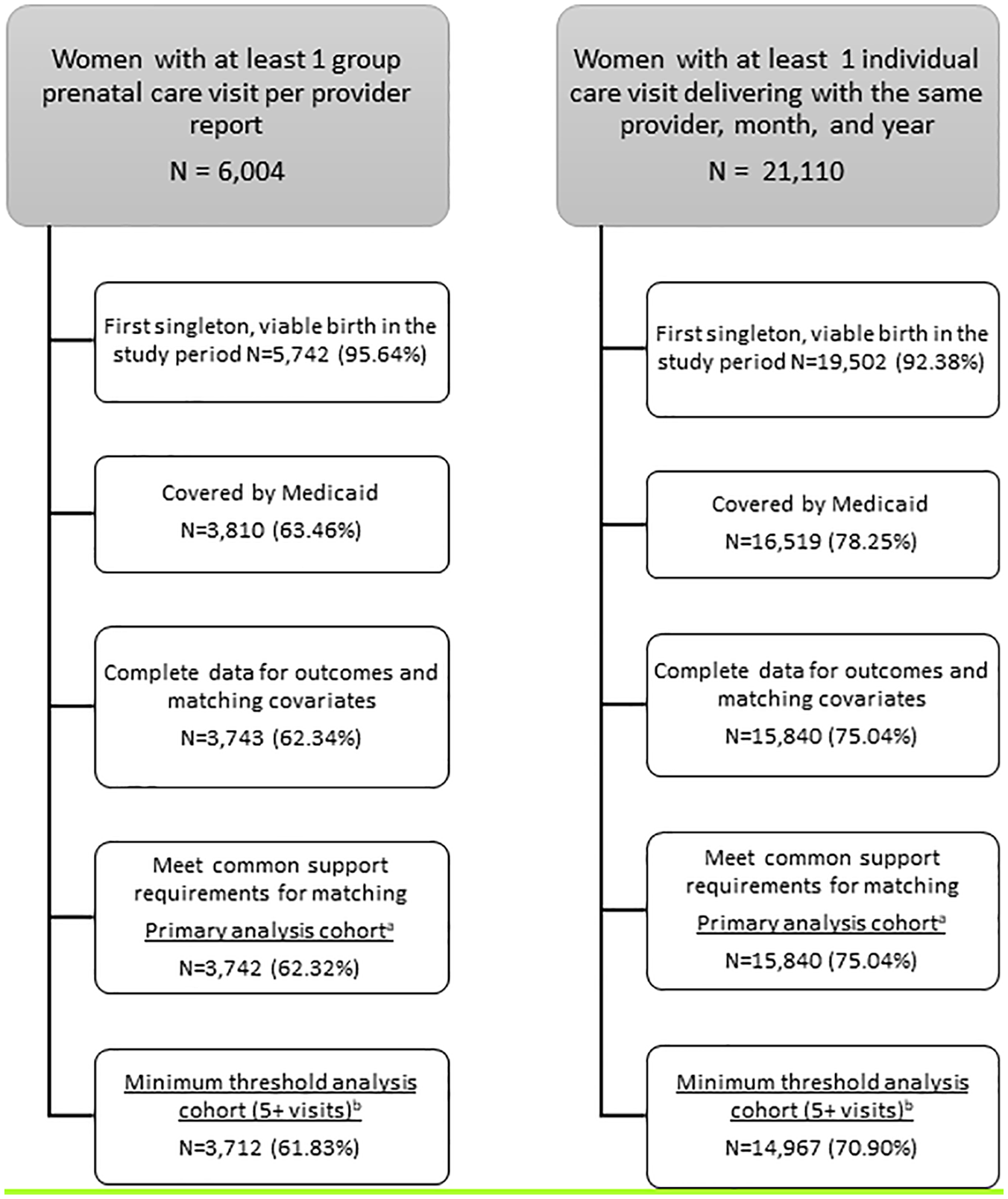
Group Prenatal Care and Individual Care Samples.
Treatment and Control Groups
It is expected that women with greater exposure to group prenatal care will experience greater benefits from the model’s health education and social support; therefore, we generated two levels of group prenatal care exposure a priori. In our primary analyses, we compare pregnant women participating in at least one group prenatal care session with women receiving individual prenatal care only. This is our “intent-to-treat” primary analysis group—if a woman attended any group care, she is included in the treatment group; if she attended individual care exclusively, she is in the control group. In our “minimum threshold” analyses, we compare pregnant women participating in five or more group prenatal care sessions with those who participated in less than five group prenatal care sessions, with at least five prenatal visits in total. As the group prenatal care curriculum is for 10 sessions, the five-visit threshold, which has been utilized in other studies, indicates that women attended a minimum of 50% of group sessions (Crockett et al., 2017; Cunningham, Grilo, et al. 2017; Cunningham, Magriples, et al. 2017; Ickovics et al., 2016). In the “minimum threshold analysis,” women included in the treatment group under the “intent-to-treat” primary analysis may cross over to the control group if they attended less than five group sessions. This results in a control group that includes women with a mix of group care and individual care visits and women receiving individual care exclusively. Women with less than five prenatal care visits (group care, individual care, or a combination of both) are excluded from the “minimum threshold” analysis.
Because participation in group prenatal care was not random, we employed propensity score matching methods to reduce differences in observable characteristics between the group prenatal care cohort and the individual cohort. This approach helps to ensure that differences between groups are attributable to their “treatment” status as opposed to other potentially confounding characteristics (Crockett et al., 2017; Hale et al., 2014; Rosenbaum & Rubin 1983, 1985; Crockett et al., 2019; Rubin, 2007). Following the previous literature, we performed a bivariate correlation analysis with each potential predictor variable versus the treatment variable (an indicator for participating in group prenatal care) and each outcome of interest to identify matching variables (Crockett et al., 2019). If the correlation between a predictor and group prenatal care indicator or any outcome was greater than |0.10| and the previous literature supported its inclusion, we included that predictor as a matching variable (Tanner-Smith et al., 2012). Matching variables (Xi) in the propensity scores included mother’s race, mother’s age, mother’s education, number of previous live births, month prenatal care was initiated, previous preterm birth, previous cesarean, body mass index greater than 45, and mother’s participation in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Other potential matching variables we considered but did not include due to the lack of a sufficient correlation with the group prenatal care indicator and our ER outcomes of interest were mother’s county of residence, mother’s diabetes status, mother’s hypertension status, infections during pregnancy, and two measures of mother’s smoking status. After settling on our matching variables, the resulting propensity score (psi) is the predicted probability of participating in group prenatal care (GPNCi) considering the values for each of these variables (psi = P(GPNCi = 1| Xi)).
We then applied a preferential-within, nearest neighbor matching approach in which group prenatal care participants were matched to individual prenatal care participants with similar propensity scores within the same practice site. Our matching approach applied a caliper width of 0.25 SDs of the estimated propensity score and allowed for matching replacement and ties. If no site-level match was identified, the matching algorithm found a suitable individual prenatal care participant at another practice to match with group prenatal care patients. This matching approach was selected for its ability to (a) account for the nested nature of the data by matching primarily at the site-level, (b) reduce the number of unmatched cases that would result from within-site only matching, and (c) improve the balance of covariates and confounders compared with pooled matching (Arpino & Cannas, 2016; Bryson et al., 2002).
Outcomes Measures
We identified ER visits from the Medicaid claims data using Current Procedural Technology (CPT) codes 99281–99285. We based our indicator for avoidable ER visits on an update to the original NYU Emergency Department Visit Algorithm that is widely reported in the literature (Billings et al., 2000; Johnston et al., 2017). This algorithm uses both International Classification of Diseases–Ninth revision (ICD-9) and ICD–Tenth revision (ICD-10) codes to give probabilities that a given ER visit fits into a set of emergent versus non-emergent categories whose definitions are both given below. These categories are also illustrated in Figure 3, along with a set of categories pulled out of the standard NYU classification scheme and tabulated separately. This figure and the category descriptions below are taken directly from the NYU Algorithm webpage (Billings et al., n.d.):
Non-emergent: Patient’s initial complaint, presenting symptoms, vital signs, medical history, and age indicated that immediate medical care was not required within 12 hr of the visit.
Emergent—Primary Care Treatable: Based on information in the record, treatment was required within 12 hr of the ER visit, but care could have been provided effectively and safely in a primary care setting. The complaint did not require continuous observation and no procedures were performed or resources used that are not available in a primary care setting (e.g., Computed tomography (CAT) scan or certain lab tests).
Emergent—ER Care Needed—Avoidable: ER care was required based on the complaint or procedures performed/resources used, but the emergent nature of the condition was potentially preventable/avoidable if timely and effective ambulatory care had been received during the episode of illness (e.g., the flare-ups of asthma, diabetes, and congestive heart failure).
Emergent—ER Care Needed—Non-avoidable: ER care was required, and ambulatory care treatment could not have prevented the condition (e.g., trauma, appendicitis, and myocardial infarction).
In our analysis, we defined any ER visit before delivery as avoidable if the updated algorithm assigned a positive probability of the visit being in the category of “Emergent—ER Care Needed/Avoidable.”
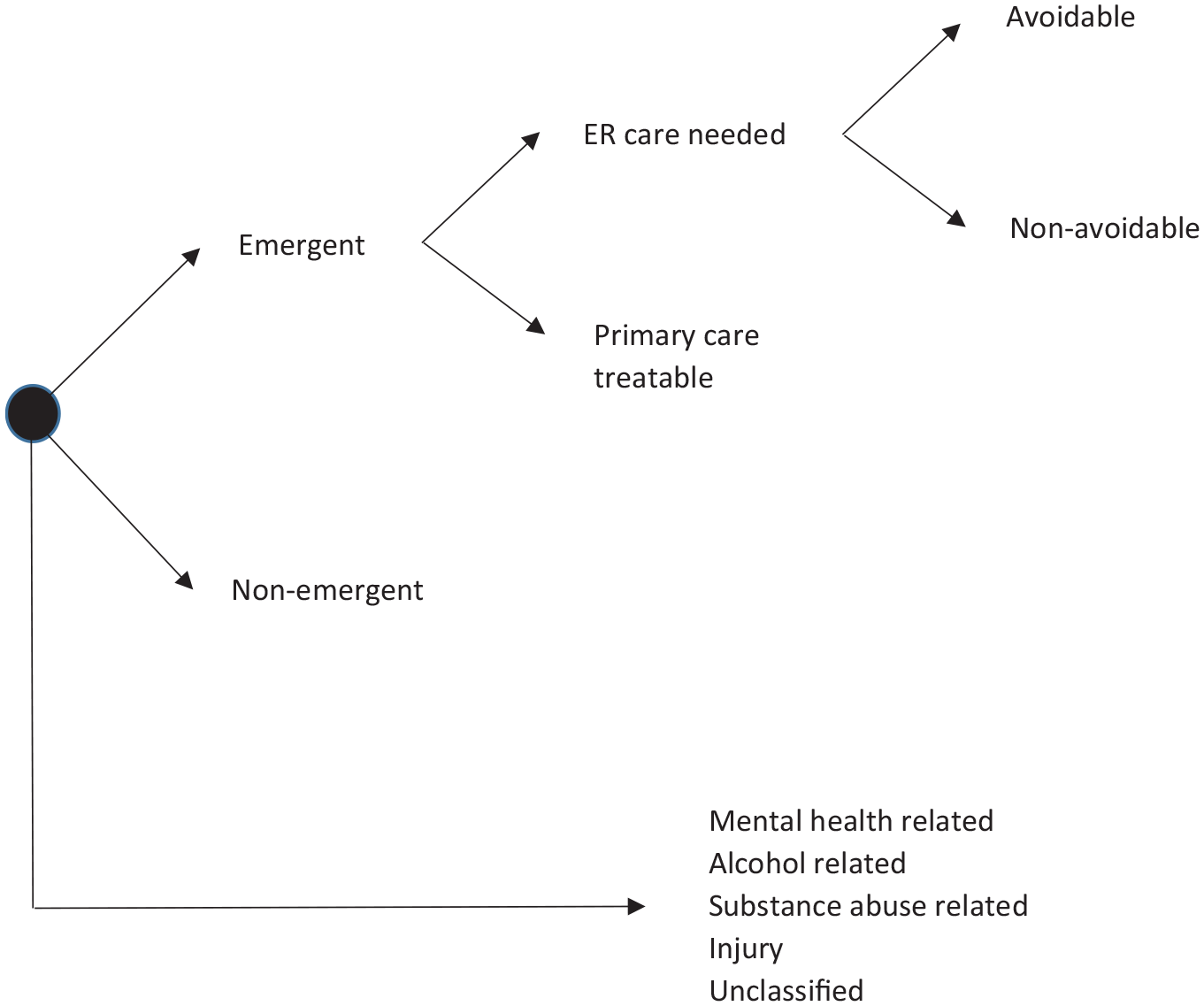
New York University (NYU) Emergency Room Visit Algorithm.
To assess the validity of the avoidable ER classification for a sample of pregnant women, we compared the distribution of the ICD-9 and ICD-10 codes associated with our ER indicator and avoidable ER indicator. Table A1 presents the top 75% of ICD-9 codes associated with our ER indicator for the pregnant women in our sample and Table A2 presents the top 75% of ICD-9 codes associated with our avoidable ER indicator. These tables show that many of the ICD-9 codes associated with our overall ER indicator for the pregnant women in our sample are pregnancy-related, such as “THREATENED PREMATURE LABOR ANTEPARTUM,” and some would be considered avoidable and others non-avoidable. Conversely, the ICD-9 codes associated with our avoidable ER indicator represent conditions or needs that could be treated in a primary care setting rather than an ER, consistent with the NYU algorithm. The frequency distributions associated with the relevant ICD-10 codes are similar, so they are not reported in the appendix.
Statistical Analysis
We examined the relationship between group prenatal care and ER utilization prior to delivery by estimating linear probability models for the binary outcomes of “any ER utilization” and “any avoidable ER utilization.” For the count outcomes of the number of ER visits and the number of avoidable ER visits, negative binomial models were estimated, given the number of observations with a count of 0. In each of these models, we weight the regressions with our preferential-within, nearest neighbor matching weights (psi) previously described. As mentioned, individuals in the treatment group are matched to those with similar propensity scores at the same site. If no site-level match is identified, then the matching algorithm found a suitable participant at another site to match with the treated individual.
Using birth certificate data, we also stratified the analysis of the primary and minimum threshold cohorts by high versus low-risk pregnancies and by the timing of entry to care. High-risk pregnancies were defined as those occurring for women with diabetes, hypertension, or a body mass index greater than 45 as indicated on birth certificates. We defined early entry to care as entering prenatal care at less than 5 months’ gestational age. All analyses are performed separately for the primary and minimum threshold cohorts.
Results
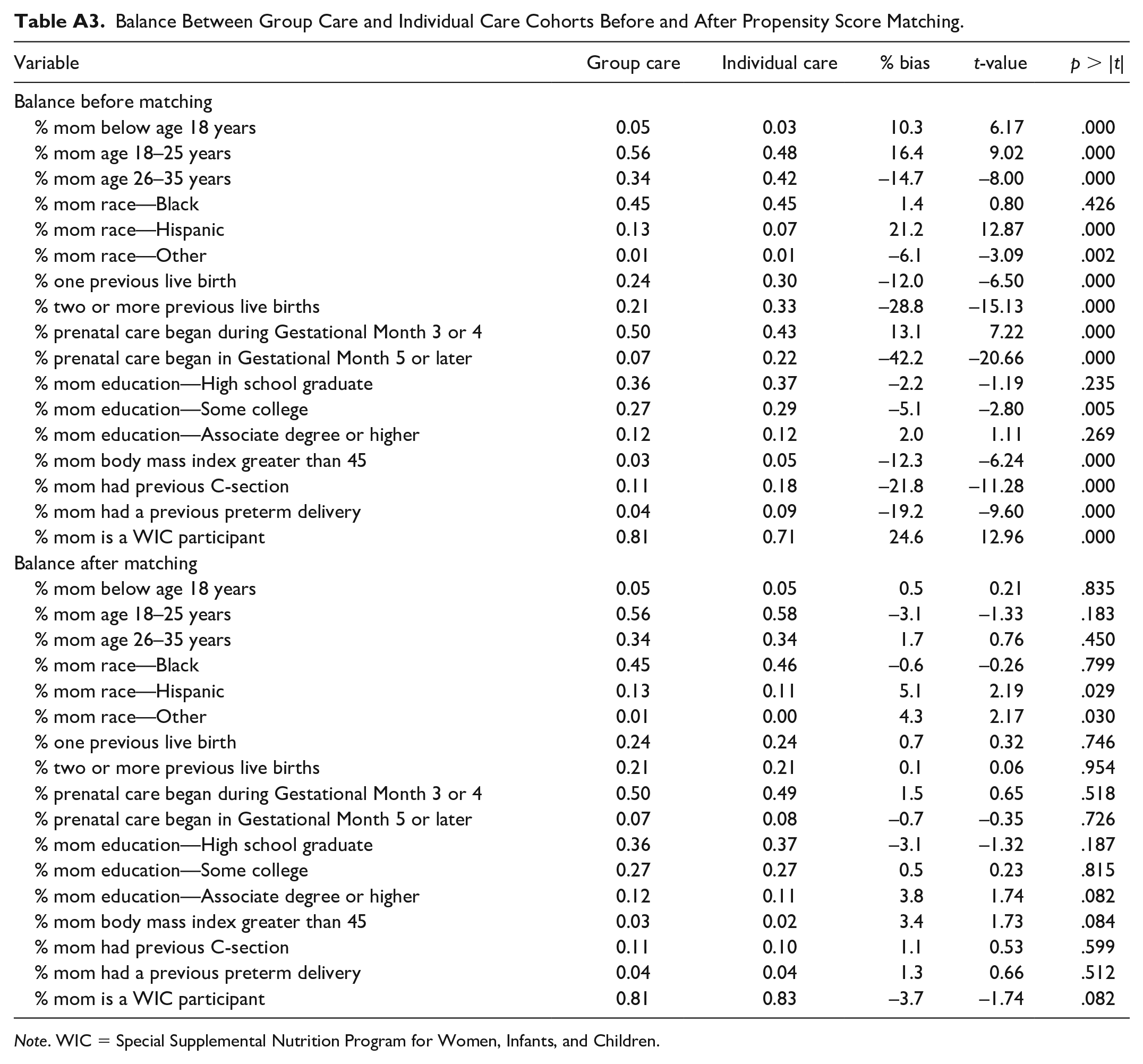
Table 1 provides descriptive statistics for our primary analytic sample prior to propensity score matching. Pregnant women in the group prenatal care cohort were more likely to be younger, be non-White, have a body mass index less than or equal to 45, and be a WIC participant compared with pregnant women in the individual prenatal care cohort. In addition, pregnant women in the group prenatal care cohort were less likely to start prenatal care in Gestational Month 3 or later, have a previous live birth, have a previous C-section, or have a previous preterm delivery compared with the individual prenatal care cohort. Propensity score matching substantially reduced the absolute standardized bias present in the unmatched samples, resulting in a matched sample with well-balanced characteristics for each set of analyses. Table A3 reports the means of the matching variables for each group, along with bias levels, before and after matching.
Unadjusted Sample Characteristics of Primary Analysis Group Prenatal Care and Individual Care Cohorts.
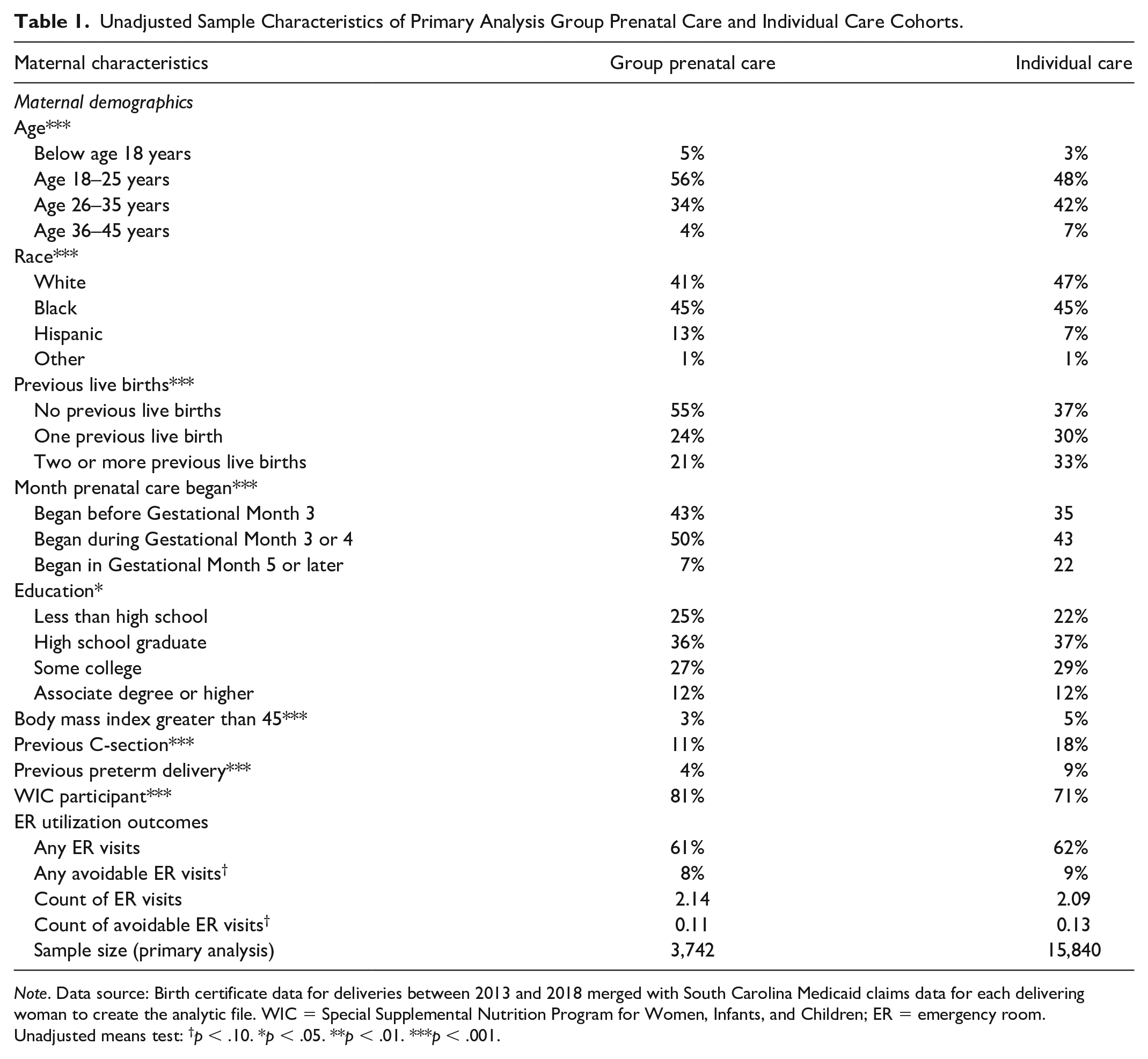
Note. Data source: Birth certificate data for deliveries between 2013 and 2018 merged with South Carolina Medicaid claims data for each delivering woman to create the analytic file. WIC = Special Supplemental Nutrition Program for Women, Infants, and Children; ER = emergency room.
Unadjusted means test: †p < .10. *p < .05. **p < .01. ***p < .001.
The unmatched group prenatal care and individual prenatal care cohorts demonstrated similar use of ER visits; 61% of group prenatal care versus 62% of individual prenatal care participants had at least one ER visit, and the group prenatal care cohort averaged 2.14 ER visits in comparison with an average of 2.09 ER visits for the individual prenatal care cohort. Table 1 shows that 8% of the pregnant women in group prenatal care had at least one avoidable ER visit and averaged 0.11 avoidable ER visits. In comparison, 9% of pregnant women in the individual prenatal care sample had at least one avoidable ER visit and averaged 0.13 avoidable ER visits.
Table 2 presents our main regression results. Our primary analysis, given in the top panel, suggests that group prenatal care participation is associated with a reduction in the probability of any ER utilization (–3.8 percentage points, 95% confidence interval [CI] = [–6.7, –1.0], p = .01; a 5.9% decrease) and avoidable ER utilization (–1.4 percentage points, 95% CI = [–2.7, –0.1], p = .04; a 15.1% decrease). Our primary models also suggest that group prenatal care is associated with lower counts of ER and avoidable ER visits. More specifically, group prenatal care is associated with a statistically significant reduction of 0.055 in the log of the expected count of ER visits (95% CI = [–0.104, –0.006], p = .027). The incident rate ratio (IRR) associated with this coefficient suggests that the ER visit incident rate for group prenatal care participants is 0.946 that of individual prenatal care participants. In addition, group prenatal care is associated with a reduction in the expected count of avoidable ER visits (–0.195, 95% CI = [–0.416, 0.027], p = .085), although this result is not statistically significant at conventional levels.
Propensity Score–Matched Regression Results for Primary Analysis and Minimum Threshold Analysis.
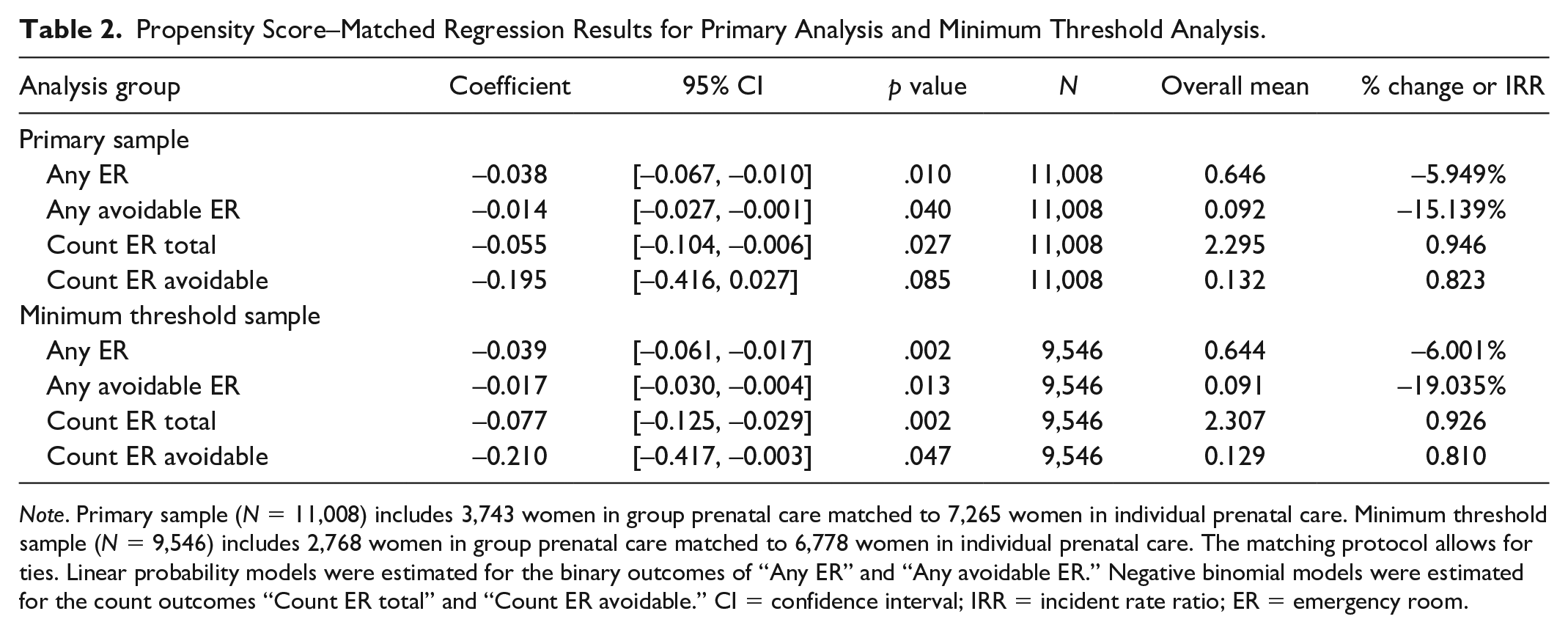
Note. Primary sample (N = 11,008) includes 3,743 women in group prenatal care matched to 7,265 women in individual prenatal care. Minimum threshold sample (N = 9,546) includes 2,768 women in group prenatal care matched to 6,778 women in individual prenatal care. The matching protocol allows for ties. Linear probability models were estimated for the binary outcomes of “Any ER” and “Any avoidable ER.” Negative binomial models were estimated for the count outcomes “Count ER total” and “Count ER avoidable.” CI = confidence interval; IRR = incident rate ratio; ER = emergency room.
The bottom panel of Table 2 presents the results of our minimum threshold analysis. Here, we see that group prenatal care is associated with a statistically significant reduction in the probability of any ER utilization (–3.9 percentage points, 95% CI = [–6.1, –1.7], p = .002; a 6.0% decrease) and the probability of any avoidable ER utilization (–1.7 percentage points, 95% CI = [–3.0, –0.4], p = .013; a 19.0% decrease). We also observe statistically significant numerical reductions in the count of any ER visits and the count of avoidable ER visits in the group care sample.
Sub-Analyses
The CenteringPregnancy model of care was originally developed for medically low-risk women and many practices continue to limit group participation based on medical exclusion criteria (Mazzoni & Carter, 2017). However, health education, social support, and facilitated group discussions offered in the group prenatal care model may benefit women with complex health conditions. In addition, women with high-risk pregnancies tend to have more ER visits than those with low-risk pregnancies, so there may be more opportunities for group prenatal care to reduce ER visits among those with high-risk pregnancies. Table 3 reports a replication of the analysis presented in Table 2 separately for high versus low-risk pregnancies. We see a statistically significant reduction in the probability of any ER visit (–3.6 percentage points, 95% CI = [–6.9, –0.4], p = .03; a 5.7% decrease) and a reduction in the expected number of ER visits –(0.082, 95% CI = [–0.131, –0.032], p = .001; IRR = 0.922) associated with the low-risk pregnant women in our primary sample participating in group prenatal care. Findings for high-risk participants were not statistically significant, but the directionality of the coefficients suggests that group prenatal care may be associated with reductions in the likelihood of any ER and any avoidable ER encounters. The magnitude of the coefficients for the high-risk participants in the primary sample are similar to those in the low-risk participants.
Propensity Score–Matched Subanalysis Regression Results: Stratified by Pregnancy Risk for the Primary and Minimum Threshold Samples.
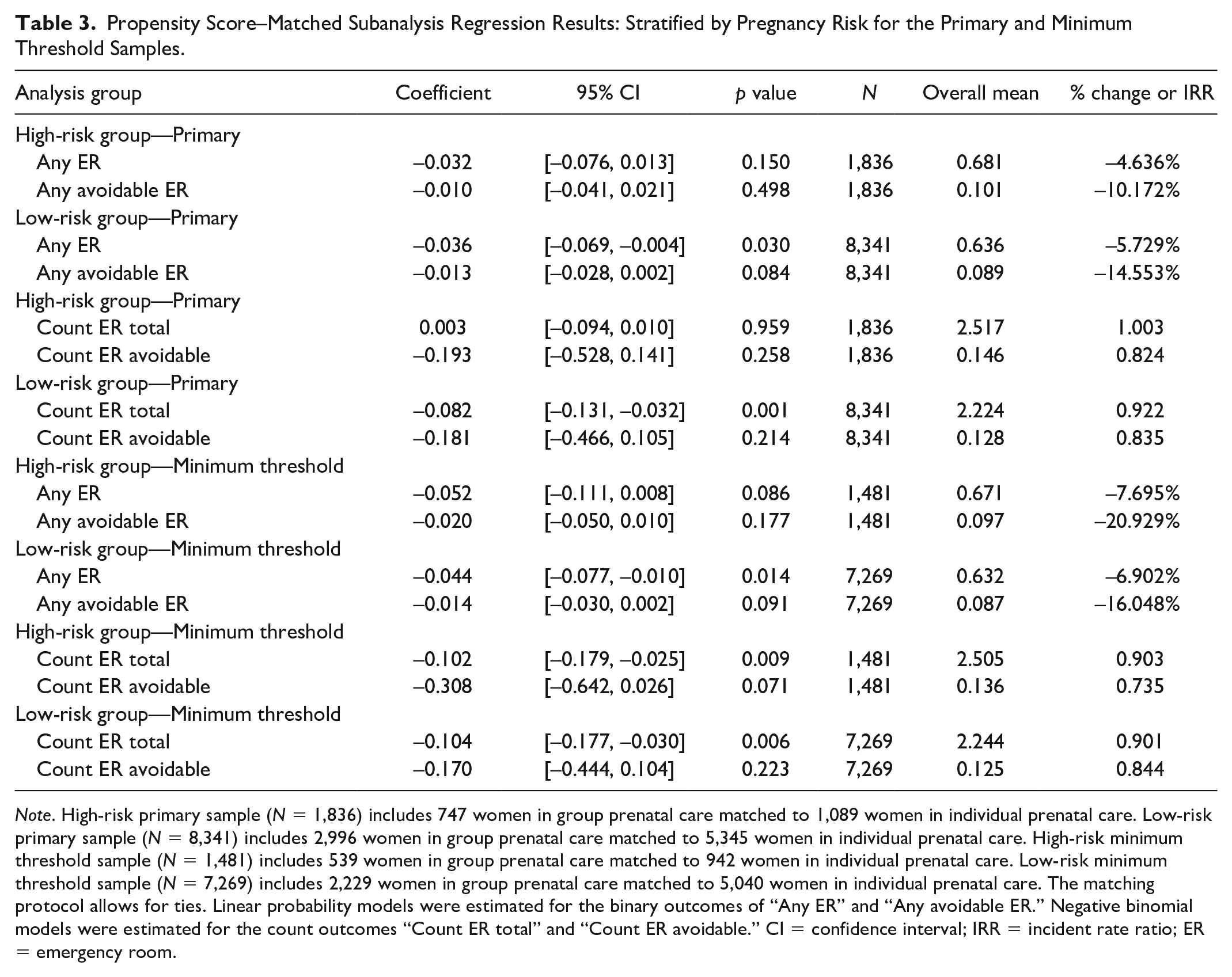
Note. High-risk primary sample (N = 1,836) includes 747 women in group prenatal care matched to 1,089 women in individual prenatal care. Low-risk primary sample (N = 8,341) includes 2,996 women in group prenatal care matched to 5,345 women in individual prenatal care. High-risk minimum threshold sample (N = 1,481) includes 539 women in group prenatal care matched to 942 women in individual prenatal care. Low-risk minimum threshold sample (N = 7,269) includes 2,229 women in group prenatal care matched to 5,040 women in individual prenatal care. The matching protocol allows for ties. Linear probability models were estimated for the binary outcomes of “Any ER” and “Any avoidable ER.” Negative binomial models were estimated for the count outcomes “Count ER total” and “Count ER avoidable.” CI = confidence interval; IRR = incident rate ratio; ER = emergency room.
The findings observed in the “minimum threshold” sample are similar although with one additional statistically significant finding. We see a statistically significant reduction in the expected number of ER visits among the high-risk pregnant women participating in group prenatal care. Overall, in several cases, the estimated relationship between group prenatal care and ER utilization is stronger in our “minimum threshold” sample as compared with our primary sample.
Table 4 reports the results after restricting the sample to women who initiated care prior to Month 5 of their pregnancy. According to Table 4, group prenatal care is associated with somewhat larger reductions in the likelihood of any ER utilization among women who started prenatal care prior to Month 5 compared with the full sample. This is true for both the primary and “minimum threshold” analysis.
Propensity Score–Matched Subanalysis Regression Results: Includes Only Women Who Initiated Care Prior To Month 5 of Their Pregnancy in the Primary and Minimum Threshold Samples.
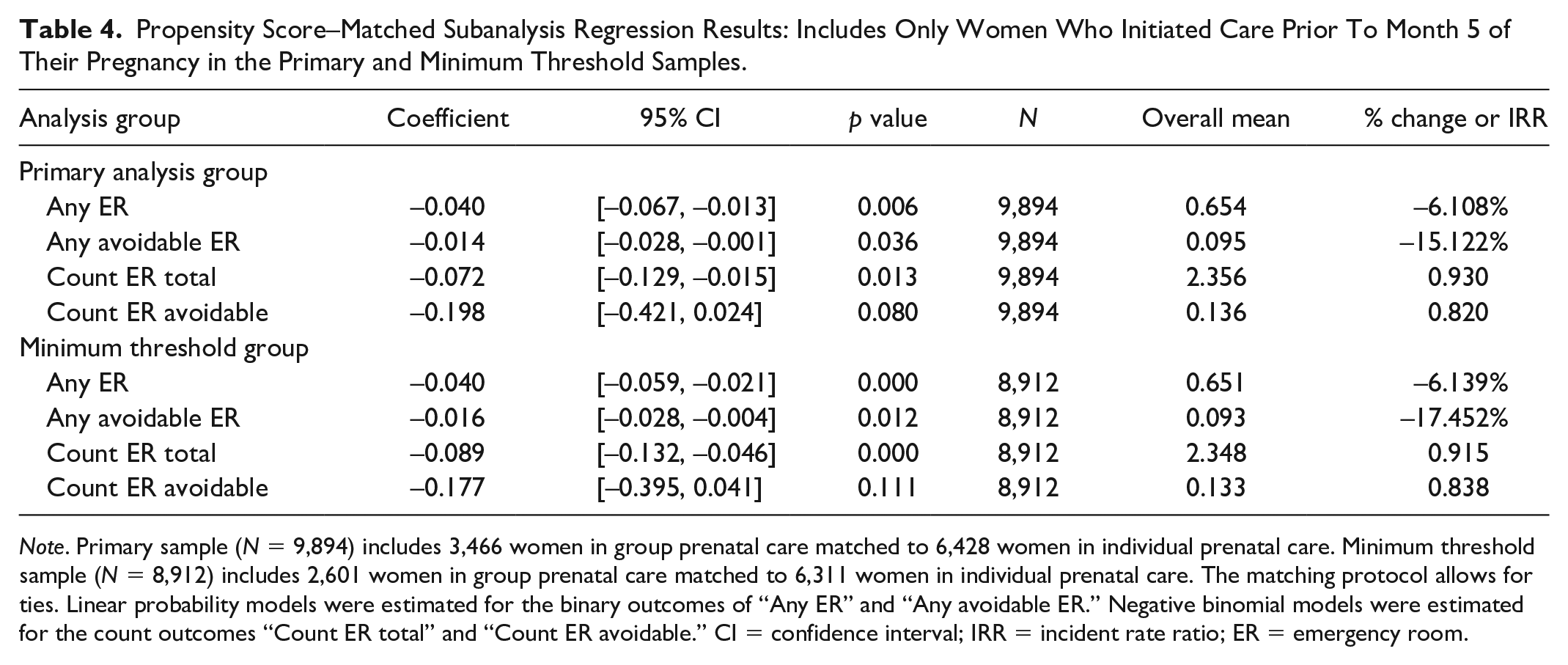
Note. Primary sample (N = 9,894) includes 3,466 women in group prenatal care matched to 6,428 women in individual prenatal care. Minimum threshold sample (N = 8,912) includes 2,601 women in group prenatal care matched to 6,311 women in individual prenatal care. The matching protocol allows for ties. Linear probability models were estimated for the binary outcomes of “Any ER” and “Any avoidable ER.” Negative binomial models were estimated for the count outcomes “Count ER total” and “Count ER avoidable.” CI = confidence interval; IRR = incident rate ratio; ER = emergency room.
Discussion
Participation in group prenatal care programs, such as CenteringPregnancy, is associated with reductions in overall and avoidable ER utilization. Our primary analysis suggests that group prenatal care is associated with a 5.9% reduction (3.8 percentage points) in the likelihood of having any ER utilization, a 15.1% (1.4 percentage points) reduction in the likelihood of having any avoidable ER utilization, and a reduction in the number of overall ER visits. Our “minimum threshold” analysis, restricted to women with at least five prenatal care visits, suggests that group prenatal care is associated with a 6.0% reduction (3.9 percentage points) in the likelihood of having any ER utilization and a 19.0% reduction (1.7 percentage points) in the likelihood of having any avoidable ER utilization. Finally, our subsample analysis implies stronger potential correlations for women with high-risk pregnancies in our minimum threshold analysis and somewhat stronger correlations for those entering group prenatal care in the first 5 months of pregnancy. Thus, our findings provide suggestive evidence that group prenatal care may lead to reductions in both overall ER and avoidable ER utilization among pregnant women.
Our study’s strengths include the use of a widely established algorithm to analyze avoidable ER utilization and data from the multisite, real-world expansion of group prenatal care in South Carolina. Each of these sites uses the same model of group prenatal care and have all been certified by the Centering Healthcare Institute, thus assuring a level of consistency in curriculum covered and model implementation. In addition, this cohort is one of the largest existing for evaluation of outcomes of group care.
Previous studies on ER utilization for pregnant women primarily examined incidence of, and patient characteristics associated with, ER visits but did not distinguish between urgent and nonurgent/avoidable visits (Cunningham, Grilo, et al. 2017; Cunningham, Magriples, et al. 2017; Magriples et al., 2008; Malik et al., 2017). In addition, these studies were not typically focused on interventions, such as group prenatal care, that might impact ER utilization. One study assessing avoidable versus non-avoidable ER visits among pregnant women examined the characteristics of those with and without such visits but did not consider the relationship between any sort of intervention and ER utilization (Kilfoyle et al., 2017). That study found that 35.6% of pregnant women in their sample had at least one nonurgent ER visit, as compared with 9% in our sample (Kilfoyle et al., 2017). A direct comparison is difficult because the previous study used patient recall to determine whether or not self-reported ER visits were nonurgent/avoidable, rather than our approach of using claims data and the NYU Emergency Room Algorithm (Johnston et al., 2017; Kilfoyle et al., 2017).
Our analysis does have several limitations. First, we are hesitant to give results a causal interpretation as the “treatment” of participation in group prenatal care was not randomly assigned at any site. Second, the structure of our data prohibited us from reliably determining when, during pregnancy, a mother received care in the ER or how many prenatal care encounters occurred before an ER visit; this level of information would provide more insight into how and when the timing of group prenatal care visits impacts ER utilization. Third, there are concerns associated with self-selection bias that our propensity scores should mitigate, but may not fully account for, particularly for women in the group care cohort. For example, by allowing group prenatal care women attending less than four group sessions to cross over into the control cohort in the minimum threshold analysis, we create a sample more reflective of real-world treatment but risk diluting the effect of group prenatal care relative to individual prenatal care. Finally, we have a general concern with single-state studies about external validity, as these findings may not be equally applicable in other areas of the United States.
Future research should be designed to explore the pathways by which group prenatal care may work to reduce ER utilization. We speculate that it could be due to specific characteristics of the model that yield stronger patient–provider relationships and therefore lead patients to avoid the ER to seek consistency in their source of health care or potential improvements in their health care literacy, which help patients better navigate the health care system and identify appropriate care settings.
Our findings add to the growing body of evidence surrounding the value of group prenatal care programs, such as CenteringPregnancy, as a potentially cost-effective intervention to encourage appropriate health care utilization among pregnant women and improve pregnancy-related outcomes (Gareau et al., 2016). According to the Agency for Health Care Research and Quality, the average total individual expense associated with a single ER visit in 2017 was more than US$1,400, and the mean hospital charge for women aged 18 to 64 years is US$47,431 (Agency for Healthcare Research and Quality, 2010, 2016). Thus, if group prenatal care is associated with reductions in such expensive episodes of care, as our findings suggest, then this could lead to additional, previously undocumented cost savings to offset the expense associated with the program.
Our study offers several clinical and policy implications. Although the CenteringPregnancy model focuses on prenatal care, clinicians and policymakers have demonstrated interest in group medical visit models to improve outcomes and reduce costs across a broad range of chronic diseases and health conditions for different populations. Group visits may be one strategy to meet the quadruple aim of optimizing health systems: improving population health, enhancing patient care experiences, reducing costs, and improving work life of health care providers (Bodenheimer & Sinsky, 2014). If group care can positively impact both care experiences and costs through increasing patient use of non-ER settings, health systems and payers may have greater incentives to support the implementation of these innovative models of care (Stiefel & Nolan, 2012). Findings from this study should therefore be understood in the broader context of literature on group medical visits, and future CenteringPregnancy research may incorporate standardized patient, provider, and system outcomes, where appropriate, to contribute not only to the field of obstetrics but also to overall preventive and primary care.
Footnotes
Appendix
Balance Between Group Care and Individual Care Cohorts Before and After Propensity Score Matching.
| Variable | Group care | Individual care | % bias | t-value | p > |t| |
|---|---|---|---|---|---|
| Balance before matching | |||||
| % mom below age 18 years | 0.05 | 0.03 | 10.3 | 6.17 | .000 |
| % mom age 18–25 years | 0.56 | 0.48 | 16.4 | 9.02 | .000 |
| % mom age 26–35 years | 0.34 | 0.42 | –14.7 | –8.00 | .000 |
| % mom race—Black | 0.45 | 0.45 | 1.4 | 0.80 | .426 |
| % mom race—Hispanic | 0.13 | 0.07 | 21.2 | 12.87 | .000 |
| % mom race—Other | 0.01 | 0.01 | –6.1 | –3.09 | .002 |
| % one previous live birth | 0.24 | 0.30 | –12.0 | –6.50 | .000 |
| % two or more previous live births | 0.21 | 0.33 | –28.8 | –15.13 | .000 |
| % prenatal care began during Gestational Month 3 or 4 | 0.50 | 0.43 | 13.1 | 7.22 | .000 |
| % prenatal care began in Gestational Month 5 or later | 0.07 | 0.22 | –42.2 | –20.66 | .000 |
| % mom education—High school graduate | 0.36 | 0.37 | –2.2 | –1.19 | .235 |
| % mom education—Some college | 0.27 | 0.29 | –5.1 | –2.80 | .005 |
| % mom education—Associate degree or higher | 0.12 | 0.12 | 2.0 | 1.11 | .269 |
| % mom body mass index greater than 45 | 0.03 | 0.05 | –12.3 | –6.24 | .000 |
| % mom had previous C-section | 0.11 | 0.18 | –21.8 | –11.28 | .000 |
| % mom had a previous preterm delivery | 0.04 | 0.09 | –19.2 | –9.60 | .000 |
| % mom is a WIC participant | 0.81 | 0.71 | 24.6 | 12.96 | .000 |
| Balance after matching | |||||
| % mom below age 18 years | 0.05 | 0.05 | 0.5 | 0.21 | .835 |
| % mom age 18–25 years | 0.56 | 0.58 | –3.1 | –1.33 | .183 |
| % mom age 26–35 years | 0.34 | 0.34 | 1.7 | 0.76 | .450 |
| % mom race—Black | 0.45 | 0.46 | –0.6 | –0.26 | .799 |
| % mom race—Hispanic | 0.13 | 0.11 | 5.1 | 2.19 | .029 |
| % mom race—Other | 0.01 | 0.00 | 4.3 | 2.17 | .030 |
| % one previous live birth | 0.24 | 0.24 | 0.7 | 0.32 | .746 |
| % two or more previous live births | 0.21 | 0.21 | 0.1 | 0.06 | .954 |
| % prenatal care began during Gestational Month 3 or 4 | 0.50 | 0.49 | 1.5 | 0.65 | .518 |
| % prenatal care began in Gestational Month 5 or later | 0.07 | 0.08 | –0.7 | –0.35 | .726 |
| % mom education—High school graduate | 0.36 | 0.37 | –3.1 | –1.32 | .187 |
| % mom education—Some college | 0.27 | 0.27 | 0.5 | 0.23 | .815 |
| % mom education—Associate degree or higher | 0.12 | 0.11 | 3.8 | 1.74 | .082 |
| % mom body mass index greater than 45 | 0.03 | 0.02 | 3.4 | 1.73 | .084 |
| % mom had previous C-section | 0.11 | 0.10 | 1.1 | 0.53 | .599 |
| % mom had a previous preterm delivery | 0.04 | 0.04 | 1.3 | 0.66 | .512 |
| % mom is a WIC participant | 0.81 | 0.83 | –3.7 | –1.74 | .082 |
Note. WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: South Carolina Department of Health and Human Services and the South Carolina Chapter of the March of Dimes supported the statewide expansion of CenteringPregnancy.