
Abstract
The COVID-19 pandemic pushed hospitals to deliver care outside of their four walls. To successfully scale virtual care delivery, it is important to understand how its implementation affects frontline workers, including their teamwork and patient-provider interactions. We conducted in-depth interviews of 17 clinicians and staff involved with the COVID-19 Virtual Observation Unit (CVOU) in the emergency department (ED) of an academic hospital. The program leveraged remote patient monitoring and mobile integrated health care. In the CVOU (vs. the ED), participants observed increases in interactions among clinicians and staff, patient participation in care delivery, attention to nonmedical factors, and involvement of coordinators and paramedics in patient care. These changes were associated with unintended, positive consequences for staff, namely, feeling heard, experience of meaningfulness, and positive attitudes toward virtual care. This study advances research on reconfiguration of roles following implementation of new practices using digital tools, virtual work interactions, and at-home care delivery.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) pandemic accelerated the adoption of practices that leverage digital technology in novel ways, pushing hospitals to deliver care outside of their four walls. In particular, the need to treat a surge of patients, prevent contagion, and expand access to care provided an opportunity for emergency departments (EDs) to experiment with and adopt virtual care tools. Examples of these tools included the iPad deployment for virtual evaluation, virtual rounding, remote patient monitoring (RPM), and a hotline for COVID-19 screening (Jaffe et al., 2021; Uscher-Pines et al., 2021). Indeed, the adoption of such tools—within the ED and post-ED discharge—allowed facilities to conserve personal protective equipment (PPE; Bains et al., 2021; Callagy et al., 2021; Candel et al., 2021; Hamm et al., 2020), increase attention to staff safety (Bains et al., 2021), and improve throughput (Callagy et al., 2021; Chou et al., 2020). As uses of digital technologies continue even as the pandemic subsides (“Telehealth Is Here to Stay,” 2021), it is important to understand how their implementation affects care delivery processes as well as the interface between patients and health care professionals.
We conducted a qualitative study to describe the experiences of frontline clinicians and staff implementing a COVID-19 Virtual Observation Unit (CVOU) in the Massachusetts General Hospital (MGH) ED. This novel program leveraged RPM and mobile integrated health care (MIH). RPM refers to the digital transmission of disease-related and physiological data over the phone or videoconferencing, which facilitates remote clinical assessment of a patient (de Farias et al., 2020). MIH is a model of care delivery under which specially trained paramedics conduct home visits and provide routine health care services outside of a health care facility (Gregg et al., 2019). Together, pairing RPM and MIH via the CVOU enabled patients who tested positive for COVID-19 to be virtually monitored and receive care without leaving their homes. At home, patients would self-report symptoms using a mobile or web-based survey or receive daily calls from a nurse for symptom assessment. If their symptoms escalated, the nurse and physician would determine whether the patient should go to the ED for further testing and potential admission or whether the patient could remain at home and undergo an evaluation via the MIH platform.
To organize a system of out-of-hospital care for these COVID-positive patients, the CVOU necessitated the coordination of many professional role groups, including emergency medicine physicians, nurses, administrative coordinators, community paramedics, and administrative staff. We conducted in-depth interviews of 17 clinicians and staff of various role groups to explore their experiences related to teamwork and patient-provider interactions when implementing a CVOU.
Background Literature
Combining remote patient monitoring (RPM) and mobile integrated healthcare (MIH) is a novel model of care that facilitates virtual care delivery. RPM allows monitoring of patients outside of traditional clinical settings and makes uses of remotely collected patient data, such as temperature, respiration rate, heart rate, electrocardiogram reading, and others. It has been most commonly used to manage cardiovascular diseases, among other chronic conditions (de Farias et al., 2020), and shown to support self-management and prompt timely and accessible care (Walker et al., 2019). To achieve successful outcomes from RPM, studies have found that ensuring collaborative and coordinated care of a multidisciplinary team is critical (Thomas et al., 2021). As for MIH, it relies on paramedics to provide in-home medical assessments and often involves emergency physicians, nurses, and community health workers in program planning and execution (Gregg et al., 2019). Patients enrolled in MIH tend to have chronic diseases and/or frequently use ED services. According to a recent review, MIH was associated with reduced hospital admission, reduced ED visits, improved access to community resources, and patient satisfaction (Gregg et al., 2019). At the same time, however, another review found that without adequate formal education and clinical supervision, paramedics in MIH and MIH-like programs were not able to fully expand their existing role or build trusting relationships with patients and physicians (Eaton et al., 2021).
Most of the prior research on RPM and MIH was conducted before the pandemic and has not examined provider experiences. Existing literature on remote and virtual work highlights heightened challenges in exchanging and coordinating knowledge in virtual versus face-to-face work environments (Kanawattanachai & Yoo, 2007; Morrison-Smith & Ruiz, 2020; Raghuram et al., 2019; Sole & Edmondson, 2003). Implementing digital tools can also negatively impact care team dynamics and outcomes, at least in the short term (Edmondson et al., 2001; Gomez et al., 2021; Hayirli et al., 2021). To successfully scale virtual care delivery, it is important to understand how implementation affects frontline workers, including their teamwork and patient-provider interactions.
Shifting from in-person to virtual care delivery is expected to alter the process and patterns of interaction among clinicians, staff, and patients. Such interactions are embedded in routines, practices, and technology and comprise coordination; they facilitate information exchange and organize a collective set of interdependent tasks (Gittell, 2002; Okhuysen & Bechky, 2009; Schultz & McDonald, 2014). In health care organizations, effective coordination is key to favorable patient outcomes, high quality of care, and positive clinician experiences (Chen & Cheng, 2021; Gittell, 2002; Gittell et al., 2010; Kerrissey, Tietschert, et al., 2022). However, prior research on coordination has largely explored patient care delivered within the bounds of a hospital or clinic. Consequently, our current understanding of coordination is limited to how clinicians and staff interact with each other and with patients when these interactions take place in person rather than virtually.
Moreover, adoption of new technology can shift role boundaries and yield new or reconfigured process and patterns of interaction (Aristidou & Barrett, 2018; Barley, 1986; Pine & Mazmanian, 2017; Raj et al., 2021). Work activities are often coordinated through role-enacted interactions, as specific roles account for well-defined responsibilities and tasks (Bechky, 2006; Valentine & Edmondson, 2015). When role boundaries shift due to technology implementation that disrupts care delivery processes, relationships and interactions linked to those roles may also shift. Thus, enabling virtual care delivery via RPM and MIH has the potential to alter the roles of clinicians, staff, and patients; their interactions; and quality and outcome of care.
New Contributions
This research provides important new insights for health services researchers and managers of health care organizations implementing telehealth and virtual care delivery models. First, we examine a new model of care delivery—a virtual observation unit that leverages RPM and MIH—from the perspective of frontline clinicians and staff who implemented it. A program like the CVOU described in this study is novel, especially in the context of the ED, and is likely to be adopted by other organizations as virtual care offerings continue to expand.
Second, we explore and describe the teamwork and patient-provider interactions in the CVOU based on the perspectives of clinicians and staff representing all role groups involved. As implementation of new practices that leverage digital tools tends to have varying effects on professional workers by role (e.g., Aristidou & Barrett, 2018; Barley, 1986; Pine & Mazmanian, 2017), we intentionally interviewed participants from all role groups involved. This approach allowed us to compare the perceptions of changes in the work context (in the CVOU vs. the ED) as well as associated changes in teamwork and patient-provider interactions following the transition from in-person to virtual care delivery.
Third, our findings suggest that in addition to safely isolating patients to receive care at home by leveraging RPM and MIH capabilities, a virtual observation unit can have unintended, positive consequences on staff, such as fostering feelings of being heard, experience of meaningfulness, and positive attitudes toward virtual care, as their involvement in direct patient care and interactions with other care team members grew.
Method
Research Setting
The CVOU was implemented in MGH’s Department of Emergency Medicine in January 2021. The program temporarily discontinued in April in response to the downtrending number of COVID-19 cases in the hospital and region. A total of 402 patients enrolled in the CVOU between January 19 and March 18, 2021. Following its successful implementation, the MGH ED is implementing the next iteration of the virtual observation unit to manage conditions beyond COVID-19, including cellulitis (skin infection), heart failure, gastrointestinal illnesses, and urinary tract infections, including pyelonephritis (kidney infections).
Figure 1 illustrates the workflow process for the CVOU. Patients were eligible to enroll in the CVOU if they had a confirmed COVID-19 infection, were experiencing symptoms related to COVID-19, had access to a telephone, and were more than 18 years old. Without the CVOU, they would have had to stay in the hospital for a longer period of time. There was no language requirement for enrollment as medical interpreters were available. Following a discharge from the ED, inpatient unit, or respiratory clinics—all in-person care settings—patients were monitored daily for 14 days in the CVOU via either patient self-reporting using a mobile or web-based symptom survey or daily calls by a nurse who used a structured questionnaire for symptom assessment. In the middle of the program, patients began receiving pulse oximeters and thermometers at enrollment. If patients reported worsening symptoms, a nurse would assess the patient over the phone and engage the on-call physician to assess the patient. If the physician deemed that the patient did not need to go immediately to an ED, they could choose to send the community paramedic to the patient’s home. During such a visit, an emergency physician provided a video-based telehealth evaluation with the paramedic on scene and determined whether the patient could continue isolating at home or whether they needed to be transported to the hospital for further acute care or inpatient admission. Of the 402 CVOU patients, 30 had care escalations, for which a community paramedic was dispatched to the patient’s home for an MIH encounter. From the patient’s perspective, the only in-person component in the CVOU was when the paramedic visited the patient’s home to connect the patient to the ED physician.

The COVID-19 Virtual Observation Unit Process
The CVOU team comprised 13 nurses, who were responsible for daily symptom monitoring; three nurse leaders, who oversaw the nursing staff; 13 on-call ED physicians, who responded to escalated cases and dispatched and provided medical directions to MIH paramedics; two paramedics, who visited patients at home and virtually connected them to the physician; nine coordinators, who enrolled and consented patients into the CVOU and organized the paramedic dispatch requested by the on-call physician; and three project managers, who oversaw program administration. All clinicians and staff received standardized training prior to their work in the CVOU. They were also given access to a shared Dropbox (Dropbox, San Francisco, CA, USA) folder containing tip sheets and documents that describe the workflows, technology, and resources related to the CVOU. The virtual provision of care was new for most clinicians and staff, other than the attending physicians who had provided video-based urgent care since 2018. All physicians and coordinators had worked together prior to the CVOU while paramedics had not worked with the other role groups. Some of the nurses had worked with physicians and coordinators previously. During the CVOU shifts, nurses, physicians, and paramedics only covered the CVOU, whereas coordinators were located in the ED and covered both the CVOU and other ED-based programs.
Data Collection
We conducted 17 in-depth, semi-structured interviews using Microsoft Teams (Microsoft Corporation, Redmond, WA, USA), a cloud-based, videoconferencing platform. The interview sample was drawn purposively to include participants from all roles involved in the CVOU implementation. Interview participants included four physicians, four nurses, two nurse leaders, five coordinators, one paramedic, and one project manager. To mitigate the limitations of virtual interviews and build rapport with participants, we requested that the interviews were conducted using two-way video and audio features, asked participants to find a private room for the interview, and exchanged a number of emails prior to the interview in regard to the study goals and procedures (Archibald et al., 2019; Deakin & Wakefield, 2014; Sedgwick & Spiers, 2009). On average, interviews lasted 48 minutes and were transcribed using Microsoft Teams. Interviews took place from June to September 2021 (with nearly 90% of the interviews conducted in July and August; see Supplement 1 for timing of all interviews by role). The institutional review boards at Harvard University and MGH approved this study.
We used a semi-structured interview guide (Supplement 2). We sought to gather information on participants’ role and background, their experiences with the CVOU, and challenges or barriers encountered during implementation. The interview guide was drafted through iterative discussions among the research team, consisting of ED physicians and management and health services researchers with qualitative research experience. The interview guide was also informed by existing research and frameworks describing determinants of effective implementation in health care settings (Damschroder et al., 2009; Greenhalgh et al., 2004).
The first author, without a clinical background and unaffiliated with MGH ED, conducted all of the interviews. Lacking prior or tacit knowledge about the program and the clinical workflow in the ED, the interviewer was able to ask probing questions about the details of the program and encourage participants to share specific examples. Participants seemed to welcome such questions soliciting elaborate input. We continued our interviews until we reached theoretical saturation within roles, such that additional interviews did not reveal new information from each role group (Glaser & Strauss, 1967).
Analysis
We conducted a thematic analysis, which involves identifying and examining codes that describe important themes in the data (Corbin & Strauss, 2008). Our analysis involved deductive and inductive approaches (Berg, 2001; Miles & Huberman, 1994). The deductive approach entailed using the interview guide as the initial codebook. We first organized the data according to the domains in the interview guide (e.g., clinician/staff interactions, clinician-/staff-patient interactions, and general experiences). The inductive approach entailed reviewing and open coding the organized segments from the transcripts using NVivo, a qualitative analytic software (QSR International, Melbourne, Australia). We searched for specific patterns of changes associated with the CVOU implementation across roles. The first author coded all of the data and shared the codes and coded data segments with the research team. The team met regularly throughout the analytic process to review the emerging codes and themes, discuss apparent patterns, and resolve any discrepancies. Through iterative rounds of discussions, we categorized the changes in work context associated with the CVOU implementation and related changes in interactions among clinicians and staff and between patients and clinicians/staff. We present our findings below.
Findings
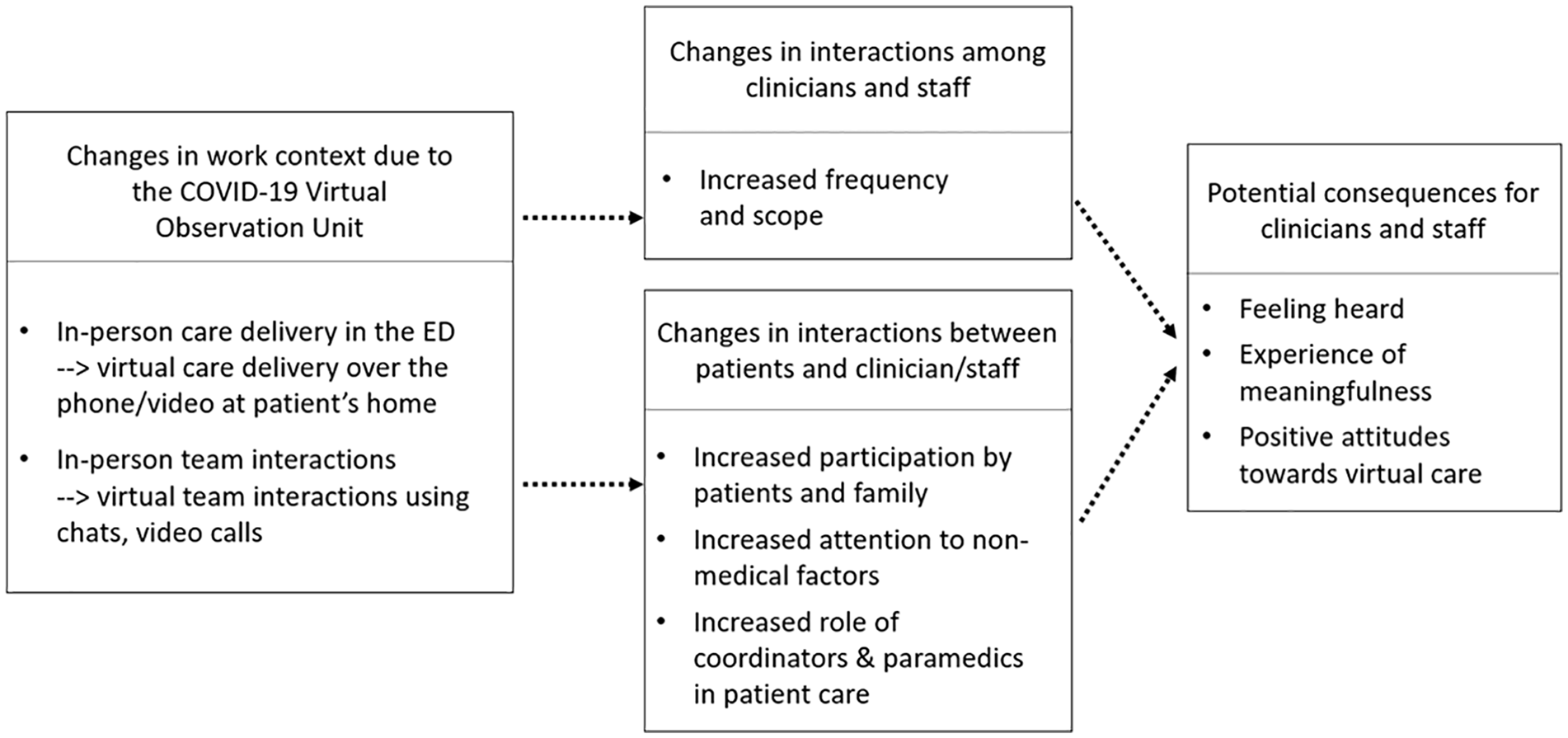
The implementation of the CVOU was associated with more frequent interactions among clinicians and staff, increased participation by patients and their family in care delivery, increased attention to nonmedical factors, and expanded role of coordinators and paramedics, compared with the in-person care in the ED. Respondents reported that these changes were associated with feeling heard by care team members, experience of meaningfulness, and positive attitudes toward virtual care. These findings are summarized in Figure 2; given that these are findings of an exploratory qualitative study, we represent relationships in dotted arrows. Below, we expound on each theme with illustrative quotes.
Effect of the COVID-19 Virtual Observation Unit Implementation on Work Context and Interactions Among Participants
Changes in the Work Context Due to the CVOU
Shift From In-Person Care in the ED to Virtual Care in the Patient’s Home
Prior to the implementation of the CVOU, patients were seen and treated in person as they walked in or were transported via an ambulance to the ED. In contrast, the care provided through the CVOU enabled patients to stay at home and receive care from a distance, away from the ED or other health care facilities. One physician described the contrast—getting to see patients in their home environment—as “eye-opening” as she could “see what patients’ homes look like and how that interplays with their symptoms, like where a patient has a flight of stairs and how much shortness of breath that could induce.” A coordinator similarly shared that, with the CVOU, she could “get inside of patients’ home life.” She added, “It wasn’t just the clinical setting you’d be dealing with—you’d be dealing with their home life, you’d be talking to family members. It’d be more intimate” (Coordinator2).
Shift From In-Person to Virtual Care Team Interactions
The doctors and nurses staffed on the CVOU worked remotely, either from home or in another setting away from the ED. Remote work implied that much of the care team interactions took place online rather than in person. To hold virtual huddles, coordinate paramedic dispatches, and discuss any questions or concerns, all CVOU clinicians and staff were given access to CVOU-specific channels on Microsoft Teams. One nurse explained how she and her colleagues used the platform: We had a chat with all of the nurses who were on for the day. Most of us worked in an acute setting before, and we were used to that face-to-face context and new to this virtual world. It helped to have a comfortable, safe setting to ask questions, share our screens to look at how to document things together. It was nice to have that channel of people to talk to. (Nurse2)
Prior to the CVOU, some nurses had worked with other nurses, physicians, and coordinators in person but not virtually. Both nurses who had worked together in person before working together virtually and nurses who had not worked together in person spoke positively about virtual interactions—especially around the convenience and timeliness of virtual information exchange. For many of the nurses and other clinicians and staff, particularly for whom the CVOU was their first time working away from the ED, this online platform was key to a smooth transition from in-person to virtual work.
Coordinators also described differences in in-person versus virtual communication with the care team in the ED and CVOU, respectively. One coordinator said, In the ED, everything is thrown at you at once so you don’t really have time to talk about the care with the providers. It is a chaotic environment. In the CVOU, when I called patients to consent them, we would have time for them to give me extra information. I could then relate that to the doctors and providers—patients mentioned this and that, so you may want to check into that. This was a good thing because the more information we collect, the better care the patient receives. (Coordinator 3)
In this case, the coordinator interviewee referred to the difference in the unpredictable type and amount of work in the ED versus the controlled type and amount of work in the CVOU.
Changes in Interactions Among Clinicians and Staff
Increased Frequency and Scope of Interactions Within the Care Team
Respondents observed that virtual coordination and delivery of care was associated with increased interactions between different role groups. One nurse shared that the use of Microsoft Teams allowed a constant flow of communication among nurses and physicians, more so than when they were working in the ED in person. She said, Most doctors were always on Teams. I could just type in a question or issue, and they’d get back almost instantaneously, every single time. It was nice to have that close contact—if you needed to run something by the doctors, when you are at home and making these clinical decisions alone. (Nurse1)
Respondents who were not as directly involved in patient care prior to the CVOU observed having more interactions with the clinicians in the CVOU (vs. the ED). For example, more interactions between physicians and paramedics took place, as paramedics set up videoconferencing in the patient’s home for physicians to provide care from afar. A paramedic explained that with the CVOU, I interacted more with physicians and nurses [in the CVOU than in the ED]. I am the only eyes on a patient, the one physically touching the patient. Physicians and other clinicians are much more dependent on my findings and assessments. They are more conscious of what my opinion is as a health care professional, versus just a paramedic who picked up someone off the street. (Paramedic1)
In line with this observation, a physician shared that Paramedics were people that I did not interact with frequently. We do see them regularly in the ED, when they drop off the patient. But with the CVOU, we got to know them more personally. It wasn’t just the few minutes when patients are dropped off, like, what happened, okay, thanks, bye. It was more like, what do you think about this, what do you think about that. (Physician4)
Similarly, there were increased interactions between physicians and coordinators in the CVOU, as coordinators would arrange and monitor the paramedic dispatches. One coordinator shared that in her job as a registrar in the ED, “communication with providers happens only if there is an error in the patient’s name or demographics,” whereas in the CVOU, there was more communication because “the paramedic couldn’t visit the patient unless someone in my role communicated with the patient and set it up for the providers” (Coordinator 5). Another coordinator commented that the increased frequency and scope of interactions with doctors inspired her “to learn to talk to doctors and learn the medical terminology they use with each other.” She added, To understand what needed to be done with the patient, I’d need to ask doctors questions. Sometimes I would be afraid of asking, but I had to get over that, for the sake of the patient. I would be afraid that I would look stupid with the little questions, like what is this medical abbreviation or terminology. (Coordinator1)
These experiences indicate that the increased frequency and scope of interactions among clinicians and staff may have allowed previously nonclinical staff, such as coordinators and paramedics, to be more integrated in the care delivery process and to closely work alongside other clinicians like physicians and nurses.
Potential Consequence: Feeling Heard
Our data suggest that increased frequency and scope of interactions among clinicians and staff were associated with reports of feeling heard by other care team members. Feeling heard refers to the belief that one’s ideas and input are acknowledged and valued (Kerrissey, Hayirli, et al., 2022). Interviewees from all role groups expressed that they felt more connected to the care team following their involvement in the CVOU. For nurses, the virtual monitoring and provision of care implied a heightened ability to speak up to ensure that the care team members were on the same page in regard to the care plan. One nurse said, “There is something about being able to speak directly to the doctors, who often have the final say in the care plan. I liked hearing about their thought process. It felt like I was playing a greater part in the plan of care” (Nurse4).
For paramedics, an interviewee shared that because paramedics are regarded as transportation rather than a part of the care team according to Medicare regulations, “we are always looking in from out the window, like, ‘we want to play in the health care sandbox.’” He added that “being able to interact with other care providers [in the CVOU] helped them to see the skills that we do have. I felt like our opinions and findings actually mattered and people listened to us” (Paramedic1).
Coordinators were able to play a more explicit part in patient care and within the care team in the CVOU than in the ED. They shared that “as coordinators, we are not a part of the clinical team but in the CVOU, we became a part of it” (Coordinator1) and that the CVOU “made me feel more like a part of the team, rather than someone on the sidelines” (Coordinator 2). In response to the increased exposure to coordinators via the CVOU, a physician expressed that she now has a “greater appreciation for the coordinators” and added that “I knew their names, but I didn’t really know who they were, what their personalities were like, or what they were bringing to the table as I do now” (Physician2).
Changes in Interactions Between Patients and Clinicians/Staff
Increased Patient Participation
Respondents shared the observations of increased participation of patients and their family in care delivery in the CVOU. RPM implied that clinicians had to learn from patient-generated data as they were not able to physically touch the patient. One nurse explained that she had never conducted a non-face-to-face assessment prior to the CVOU, which meant that she “had to listen to both how patients sounded on the phone and what they were saying to put together the clinical picture in my mind” (Nurse2). Another nurse said that “When I do a nursing assessment, I can tell a lot about a patient’s medical history and how they are feeling by just looking at them. But we didn’t have any of that. I couldn’t look at their hands or check the pulse” (Nurse1). Without physical, in-person interactions, patients “had to play an active part in their care than just lying in a hospital bed,” she added: In the hospital, you don’t have to rely on them as much. I can just figure it out. But when they’re home, I have to rely on them just as much as on my own knowledge or doctors instructing me on what to do.
Interviewees recalled that being able to interact with patients’ family members was a “big benefit” (Physician3) and that they were “eager to help, so willing and able to provide input” (Paramedic1). One nurse shared that family members offered an “extra set of eyes,” as they “could see what the patient looked like and could express their concerns and help with the assessment as we couldn’t see the patient on the phone” (Nurse4). The presence and engagement of family members were appreciated especially during this time as visitor restrictions were very strict for patients in the ED.
Increased Attention to Nonmedical Factors
By design, the CVOU monitored patients for 14 days while they isolated at home. In contrast, in the ED—a setting where optimizing throughput is critical—patients would be discharged in just a few hours or stay up to 2 days in an ED observation unit. The 14-day observation period in the CVOU meant that clinicians and staff could have more time with patients. One nurse shared that being able to see patients for “two weeks in a row” made her “feel like I actually established relationships with patients” (Nurse3). Similarly, a physician shared that virtual meetings with patients would be scheduled for 30 to 45 min, which was “in contrast to about 10 minutes per patient in the ED” and “not something we always have the luxury or ability to do in the ED” (Physician1).
Interviewees shared that they would hear more about chronic, nonmedical issues during calls and meetings with patients in the CVOU than in the ED, perhaps because they had more time with patients in the CVOU. A nurse leader shared, Nurses were calling patients to follow up with COVID symptoms, right? But then a patient would be like, well, I feel fine, but I don’t have any food. Or I can’t pay my bills because I can’t go to work. My wife is sick and I can’t get her medicine. (NurseLeader2)
Similarly, a paramedic said that in the CVOU, because he was not “bound by time constraints,” he did not have to “worry about getting a patient to the ED in 15 minutes because his coronary artery is blocked.” Instead, he could invite patients to Tell me your story. And they would tell me everything. A lot more than what I’d want to know, but it allowed me to figure out what I needed to do to mitigate what was going on with them. For example, understanding that they spend more money on cat food than on their medication. Then we’d brainstorm: Can we find a way to get her medications at a lower cost? How can we help so that she is not costing us $3,000 to $5,000 every time she goes to the ED? It’d be well worth for MGH to say, here’s a gift card for $500 of cat food for the year to keep you out of the ED. (Paramedic1)
Although addressing such nonmedical factors was “far outside of the intended scope of the program” (Physician2), it was not “something that we could just ignore” (Nurse4). Providing care outside of the walls of the ED extended the scope of care and tended to patients’ health more generally, possibly to the benefit of the patient and the health system.
Increased Role of Coordinators and Paramedics in Patient Care
Staff such as coordinators and paramedics reported being more involved in patient care in the CVOU (vs. prior to the CVOU). In the ED, while coordinators were “the first face you see when you come in,” in terms of patient interaction, “there’s not a lot,” one coordinator said (Coordinator4). Their role in the ED was limited to registering patients and ensuring that beds were clean and ready for use. “Sometimes a patient would be standing right next to me and I’d chat with them. I would get them a blanket if they were cold. But it was frustrating, because I felt like I couldn’t do more for them,” a coordinator said (Coordinator2). In contrast, the CVOU “allowed me to do more. I could see from start to finish, and be aware of what is going on with the patient and what happens to them,” she added. Coordinators became more involved in patient care in the CVOU, compared with in the ED, in the following ways: In the CVOU, coordinators would (a) consent and enroll patients—which tended to include more clinical information than when they obtained consent for general ED care; (b) organize paramedic dispatches and the accompanying virtual doctor-patient visits; (c) educate patients about these visits and follow up as needed; and (d) follow individual patients more closely, rather than overseeing the flow of 30 to 40 patients in the ED. A coordinator commented that, As coordinators in the ED, we don’t have to explain anything to the patient. That’s not our role. Nurses and doctors do that. With the CVOU, I’d tell patients why they are receiving the care and how the visit works. (Coordinator1)
Similarly, paramedics did not have a reason or time for much patient interaction prior to the CVOU. “As a typical paramedic, we don’t give a lot of thought and do a deep dive in trying to understand why something happened. It’s more like, it happened, so let’s get you moving and get you to the hospital. Then I’m onto the next case,” a paramedic shared (Paramedic1). With the CVOU, “it was much more than that.” He explained, For example, it’s not just, let’s get you to the hospital because your blood sugar level is 20, but more like, how can I prevent it from dropping to 20 again, so that you can stay at home and not be in the ED or on the back of my ambulance.
In these ways, the CVOU seemed to have expanded the ways that coordinators and paramedics interacted with patients and grew their involvement in patient care.
Potential Consequence: Experience of Meaningfulness
Our data indicate that clinicians and staff experienced meaningfulness or felt “worthwhile, useful, and valuable—as though they made a difference and were not taken for granted” (Kahn, 1990, p. 704), as their participation in patient care and team discussions grew. One coordinator shared feeling that she “could be more resourceful and helpful in the CVOU compared to being a registrar on any other normal day” and that she “had more tasks that I enjoyed [in the CVOU].” She attributed her positive experience to “more contact with patients, and definitely more contacts with paramedics and doctors” (Coordinator5). Nurses, too, expressed experiences of meaningfulness for being able to interact more with patients and contribute to team discussions. One nurse said, This program built my skills and confidence, in talking to my colleagues and asking questions like, what would you ask the patient in this circumstance? Does that sound unusual to you? Should I investigate a little bit further? This part was satisfying and fulfilling 100%. (Nurse4)
Others cited getting to play a greater role in patient care delivery in the CVOU as a reason for their positive experience. A coordinator shared that she enjoyed working in the CVOU, because: It broadened my knowledge of medicine. I learned what the diagnosis is when we send paramedics out, what patients need done with the doctors, and what the results are like. I’m very interested in medicine. But I’m not a doctor. I’m not a clinician. But I work here. Because of the CVOU, I became more aware of the clinical aspect of patient care. (Coordinator2)
She added that she believes coordinators’ increased involvement in patient care improved the quality of care because “If you understand what the patients are going through, you can be even more compassionate and interested in their well-being. It’s like the patient has gained another ally, another set of eyes watching out for them.”
Similarly, a paramedic shared that paramedics’ involvement in the CVOU “invigorated the department because we are getting involved in more patient care and fulfilling our desire to want to be involved in medicine” (Paramedic1). These data suggest that, particularly for the previously nonclinical staff, increased interactions with patients and other care team members in the CVOU enhanced their ability to meaningfully contribute to patient care and to the care team. Our data further suggest that increased interactions with patients and care team members were associated with more engaged, satisfied support staff.
Potential Consequences: Positive Attitudes Toward Virtual Care
Overall, positive experiences in the CVOU shaped clinicians’ and staffs’ opinions and attitudes toward virtual care. One physician said that while he used to be “old school in terms of thinking about what patient care interaction should physically look like,” after “a number of really positive interactions in the CVOU, how strongly I used to feel about the need to do a full physical exam in person has changed a bit” (Physician3). Another physician said that she signed up to help in the CVOU because it was a “new program that hadn’t been done before and I wanted to see whether it would work” (Physician4). She said that she was “surprised that it actually worked,” that “people whose symptoms could be managed at home, did stay at home.” Similarly, nurses also expressed being surprised by the “success of the CVOU.” One nurse leader said, Nursing is very hands-on. That’s how we work. We touch the patient. So, it was interesting to realize what you can do to keep patients at home. My initial thought was we can’t do this at home. There’s no way. But you can. You can do a lot of it at home. (NurseLeader2)
Implementation Challenges
While most respondents reported positive experiences with the CVOU, some did raise challenges related to implementation. These challenges primarily pertained to learning a new model of care during the pandemic. Several respondents referred to a “learning curve” associated with using Microsoft Teams, using the pager, making daily phone calls to patients (a new way of connecting with patients for ED nurses), and becoming familiar with new documentation processes on the electronic health record. Moreover, complicating the learning process were the conditions of the pandemic, which gave rise to a large number of COVID-19 cases at the time of implementation and the need for some clinicians to work remotely due to safety concerns. One nurse recalled, For the first month of the CVOU, we were on 12-hour shifts. You can have busy shifts like that in any clinical setting but this was a little crazy at first. We were on 8am-8pm shifts. I’d literally sit and not move for hours as I called patients. Sometimes I would still have more patients to call when 8 o’clock hit in the evening. (Nurse3)
Another nurse, who worked in her own home environment, shared, It was intimidating to be home by myself and figure out the new workflow. I’d wonder, am I asking these questions right [to patients], or, am I documenting this correctly? So much of nursing, specifically what I’ve done, has been in an acute care setting where you have a team of people around you and we troubleshoot things together. We’re sitting next to each other at a desk and could ask each other: Does my screen look normal? How do I answer this? How do I move past this screen? We didn’t have that in the CVOU. That was the biggest challenge for me. (Nurse2)
However, respondents also said that these challenges were not insurmountable. Over time, clinicians and staff all became familiar with new workflows and approach to clinical care that differed from the one in the ED. The same nurse who shared the challenges of implementing a new program in physical isolation said that uses of chats and videoconferencing helped her to connect with other nurses and figure out any uncertainties about the program as a group. Others described training documents that were “quite robust” and “helpful,” although “we couldn’t sit around and do the training together in person” (Physician3). A coordinator similarly mentioned benefiting from the training materials that “described step-by-step processes” (Coordinator1). Overall, there seemed to be a general sentiment that “everyone wanted to make this program work,” said one nurse (Nurse1). She added, “There was no huge hurdle that we couldn’t overcome. Anytime we ran into anything we thought as a group and would come to a decision, like this is a better way to do this, let’s do it this way.”
Discussion
This study investigated the experiences of frontline clinicians and staff implementing the virtual observation unit in the ED during the COVID-19 pandemic. The CVOU program was designed to isolate patients in their homes while providing care by leveraging RPM and MIH capabilities. These capabilities shifted care delivery from in-person to virtual and changed how clinicians and staff coordinate care and interact with patients.
The pandemic accelerated the adoption of new models of care—like the CVOU that combines RPM and MIH—that leverage technologies like the telephone, mobile app, and video-based telehealth. For example, while physicians in our setting had provided care via video-based telehealth previously, they had not cared for patients in their homes with another health care provider (e.g., a paramedic) present with the patient. This gave the physician the additional ability to obtain a robust set of vital signs, administer medication, and conduct diagnostics, among others. Studies on such efforts have been mostly descriptive, detailing how the virtual care or RPM was organized (e.g., Annis et al., 2020; Sitammagari et al., 2020) and how they affected clinical operations (e.g., Bains et al., 2021; Candel et al., 2021). More research is needed, therefore, on how the transition to virtual care affects frontline clinicians and staff who provide care, as its implementation requires the coordination of several professional role groups. Understanding how each group individually and collectively experiences new technology and practice can shed light on scaling and sustaining their proper and consistent use (Atkinson & Singer, 2021; Colquhoun et al., 2017). In the case of the CVOU, affected role groups included physicians, nurses, coordinators, and paramedics. In-depth interviews with individuals from every role group allowed us to explore how the CVOU implementation affected their practice and interaction processes and patterns.
In accordance with scholarship that evinces reconfiguration of professional roles following new technology and practice implementation (e.g., Aristidou & Barrett, 2018; Barley, 1986; Pine & Mazmanian, 2017), this study shows that implementing the CVOU expanded the roles of support staff in care delivery. Specifically, organizing virtual care delivery necessitated paramedics and coordinators to interact with patients more frequently and directly than they would in the ED, allowing them to become core members of the care team. Paramedics and coordinators, who used to play a limited role in patient care prior to the CVOU, welcomed such opportunities as increased patient interactions seemed to cause their jobs to feel more meaningful.
Like other health care workers around the world, CVOU team members had to adapt to a virtual work environment and expanded roles (particularly in terms of increased involvement in patient care) with limited training and learning on the job. Although this was not ideal, it was the reality for most health care providers during the COVID-19 pandemic. Our findings suggest that clinicians and staff appreciated the opportunity to learn new tasks and new ways of interacting with patients and team members. The new and reinforced interpersonal interactions in the CVOU led to vicarious learning on the job among clinicians and staff, which then seems to have led to building of trust and affective commitment (Myers, 2018). In this way, experiences of meaningfulness and feeling heard by other team members were an unintended byproduct of implementing a virtual care delivery model. Carefully designing virtual workflows to include more staff in care delivery and patient interactions—with adequate training—may serve to reinvigorate the health care workforce, as exhaustion and burnout have been a serious concern among paramedics and support staff (Au et al., 2018; Sporer, 2021). The increased opportunity to connect with patients may serve as a motivation for health care workers who want to make a positive difference in other people’s lives (Grant, 2007).
The CVOU equipped clinicians and staff to become a virtual team, as technology enabled them to work across locational, temporal, and boundaries (Martins et al., 2004; Morrison-Smith & Ruiz, 2020; Raghuram et al., 2019). Microsoft Teams served as the communication technology. It enabled the discussions that normally would have occurred in person on the ED floor. The enterprise-level version adopted by MGH was compliant with the Health Insurance Portability and Accountability Act (HIPAA).
While prior research on remote and virtual work points to heightened challenges in exchanging and coordinating knowledge compared with face-to-face work (Kanawattanachai & Yoo, 2007; Raghuram et al., 2019; Sole & Edmondson, 2003), in our context the CVOU enriched the interactions among care team members and allowed care team members to feel like their ideas and input were heard and valued by others. According to our findings, uses of chats and videoconferencing increased the frequency and scope of interaction between physicians, nurses, and coordinators. Two reasons may explain the open and constant information exchange in the CVOU. First, technology-based communications enabled asynchronous interactions, allowing busy clinicians to respond to questions and offer information based on their own availability. Second, it is possible that electronic, virtual interactions diminished social cues (Hayirli et al., 2021; Hollingshead, 1996) and lowered professional and status distinctions among members, which are more salient in in-person interactions (Martins et al., 2004). It is possible that these changes were more salient in our context because most participating clinicians and staff in our setting had a limited experience with virtual care prior to the CVOU. More research is needed to understand how virtual care delivery technology and practices affect interpersonal processes, such as interaction patterns, psychological safety, trust, and cohesion, among frontline clinicians and staff.
This study highlights the opportunity and ability to attend to social determinants of health when patients are receiving care at home. Although the CVOU protocols directed nurses and paramedics to focus on assessing patients’ COVID-19 symptoms, our findings suggest that patients were keen to express nonmedical issues, such as food insecurity, transportation, and family support, that were affecting their health and treatment. In the ED, a team of social workers and case managers exists to address nonmedical issues that patients raise. However, it is possible that that such issues were more present and relevant to the care that patients were receiving at home versus in the ED. It is also likely that patients felt more comfortable discussing them in their home environment, especially after having had the chance to build a rapport over several days with the same clinicians. Moreover, telehealth and home visits may help paramedics and other clinicians to recognize aspects of a home environment that could affect patients’ health and ability to follow on care plans that may not have been evident in the ED.
Thus, the growing shift from hospital care to hospital-at-home care (Leff et al., 2005) may aid health care organizations to better address social determinants of health and manage their effects for at-risk populations. Programs in the future should be prepared to address patient needs related to social determinants of health that are uncovered by virtual care delivery models. Including social workers and case managers could be helpful in assessing needs and providing resources. In the current iteration of the virtual observation unit being implemented in the MGH ED following the CVOU, patients must be referred by a primary care physician to enroll. If needs related to social determinants of health arise, then the ED clinicians and staff consult with the primary care team for assistance with addressing those needs.
The ongoing pandemic propelled patients and providers to adopt virtual care across conditions and settings, including the combination of RPM and MIH to build virtual observation units. These units could be safely adopted for other chronic and acute conditions (e.g., Sitammagari et al., 2020). As insurers and policymakers decide on how to cover this type of care moving forward past the pandemic health emergency, more evidence is needed on how these units affect patient outcomes. Virtual observational units could result in more timely, cost-efficient, and patient-centered care (Levine et al., 2021). Our results add to the growing literature on the benefits of remote monitoring programs and virtual care as the future of these programs continues to be debated. By allowing nonphysician providers to play a larger role in patient care, these virtual units could result in more efficient use of resources, including physician’s time. Our findings add that it may also lead to positive experiences for other frontline staff, including feeling heard by team members and experience of meaningfulness in work.
This study has several limitations. First, interviews took place 3 to 4 months following the CVOU implementation. An arguably considerable lapse of time could risk memory gaps and errors. However, many of the interviewees described the CVOU as a distinct program implemented during a unique time and were able to vividly recall experiences and specific memories during our conversations. Second, this study was conducted in a single institution and findings may not be generalizable outside the ED and academic hospital settings. To our knowledge, there have been no other empirical studies examining frontline clinician and staff experiences of implementing RPM and MIH. More research is needed to explore the frontline perspectives on implementing virtual care delivery processes across different contexts. Third, most of the interviewees’ experience with the CVOU implementation was positive. It is possible that people who did not have a positive experience chose not to volunteer their time in an interview. However, it is also possible that the CVOU had a sweeping buy-in because it allowed safe care delivery during the pandemic and also because program leadership consulted many frontline clinicians and staff during its design, taking a bottom-up approach. Fourth, while the adoption of the CVOU affected both patients and providers, in this study we only examined what the adoption looked like from the providers’ perspective. Future research should explore patient experiences with programs like the CVOU that entail RPM and virtual patient interactions with clinicians and staff.
Conclusion
Health care delivery is likely to continue to advance with programs like the CVOU that leverage RPM, MIH, and other technologies that facilitate virtual care. Findings from this study suggest that in addition to access, care quality, and patient experiences (Aashima & Sharma, 2021; Ashwood et al., 2017; Snoswell et al., 2021), uses of virtual care can have spillover effects on care team dynamics and morale. Understanding the impact of implementing virtual care on users, namely, the frontline clinicians and staff, will be key to successfully sustaining and scaling its use.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587221108750 – Supplemental material for Implementing a COVID-19 Virtual Observation Unit in Emergency Medicine: Frontline Clinician and Staff Experiences
Supplemental material, sj-docx-1-mcr-10.1177_10775587221108750 for Implementing a COVID-19 Virtual Observation Unit in Emergency Medicine: Frontline Clinician and Staff Experiences by Olivia S. Jung, Ilana Graetz, Stephen C. Dorner and Emily M. Hayden in Medical Care Research and Review
Footnotes
Acknowledgements
We are grateful to the Massachusetts General Hospital Emergency Department clinicians and staff who generously shared their time and thoughts in interviews. We thank Ariel Avgar and Beth Goodrick for insightful feedback in developing this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.