
Abstract
While cancer screening guidelines increasingly recommend incorporating life expectancy estimates to inform screening decisions for older adults, little is known about how this happens in practice. This review summarizes current knowledge about primary care clinician and older adult (65+) perspectives about use of life expectancy to guide cancer screening decisions. Clinicians report operational barriers, uncertainty, and hesitation around use of life expectancy in screening decisions. They recognize it may help them more accurately weigh benefits and harms but are unsure how to estimate life expectancy for individual patients. Older adults face conceptual barriers and are generally unconvinced of the benefits of considering their life expectancy when making screening decisions. Life expectancy will always be a difficult topic for clinicians and patients, but there are advantages to incorporating it in cancer screening decisions. We highlight key takeaways from both clinician and older adult perspectives to guide future research.
Introduction
Cancer screening decisions are complex for older adults. As people age and “age out” of guideline recommendations, it becomes more difficult to weigh whether the benefits of screening (e.g., early detection and treatment; survival and mortality benefit) outweigh the potential harms (e.g., overscreening, overdiagnosis, false positive results, follow-up testing complications, overtreatment) (S. J. Lee, Boscardin et al., 2013; S. J. Lee, Leipzig et al., 2013; R. A. Smith et al., 2019). Unfortunately, there is limited data to guide these decisions, as most randomized control trials of routine cancer screening tests, have not included adults over the age of 75.
There are a lot of reasons why life expectancy might be useful to consider in the context of cancer screening for older adults. Compared with chronological age, life expectancy (i.e., how long statistical models predict that a person will live based on their age, health, comorbidities, and functional status) is a more nuanced metric to assess whether the benefits outweigh the risks of cancer screening for older adults (Cho et al., 2013). From an evidence perspective, research suggests patients with life expectancies of less than 10 years are unlikely to live long enough to derive the distant survival benefits of cancer screening, though data differ by cancer type (S. J. Lee, Boscardin et al., 2013). U.S.-based national guidelines already recognize that life expectancy is an important metric to consider, and many recommend against routine cancer screening for older adults with a life expectancy of less than 10 years (Cho et al., 2013; Qaseem et al., 2013; Taksler et al., 2013).
However, national guidelines provide little guidance on how to implement the recommendation to consider and estimate a patient’s life expectancy and assess if the benefits of screening outweigh the harms. Furthermore, incorporation of life expectancy in cancer screening decisions in practice depends upon acceptance from both clinicians and patients (Chung, 2018; Salzman et al., 2016; Tazkarji et al., 2016; Walter & Covinsky, 2001). Little empirical work has documented perspectives and practices in this space. A recent study found that over 75% of older adults with limited life expectancy intend to continue cancer screening, and less than 25% recall discussing the need for continued screening tests with their clinician (Kotwal et al., 2019). These data and expert commentaries (Chung, 2018; Rochman, 2014) raise questions about how clinicians and older adults feel about life expectancy and if it is being considered in clinical practice to inform cancer screening decisions.
New Contributions
There is a need for a holistic understanding about what is known about clinician beliefs, challenges, and current practices related to the estimation and use of life expectancy in the context of cancer screening, and how well older adults understand and perceive the estimation of their life expectancy to inform these screening decisions. While studies have explored some of these questions and the literature on this topic is growing, no reviews have summarized and compared primary care clinician and older adult perspectives in this area. Importantly, this review makes a new contribution to the literature that explores how clinicians and older adults feel about the current push to frame when to discontinue screening based upon life expectancy estimations, as suggested in national guidelines (Cho et al., 2013; Qaseem et al., 2013; Taksler et al., 2013). Understanding these perspectives, preferences, and current practices is relevant to clinicians and practitioners who are responsible for implementing these guideline recommendations and participate in these care decisions in clinical practice, as well as policy makers who advocate for and design clinical practice guidelines to improve both individual- and population-level care decisions. Furthermore, this work is needed for health services researchers who investigate guideline implementation, reduction of low-value care, shared decision-making, and preventive care decision-making for older adults more broadly.
This narrative review aims to (a) provide a summary of existing literature and current knowledge about both primary care clinician and older adult perspectives about use of life expectancy to guide cancer screening decisions, (b) compare clinician and older adult perspectives, and (c) highlight key takeaways from the literature to guide future research.
Framework
A wealth of literature about cancer screening decisions for older adults recommends that decision-making about screening be an individualized and tailored to each patient to improve screening decisions and outcomes (Breslau et al., 2016; Kotwal & Walter, 2020; K. T. Lee et al., 2018; Taksler et al., 2013; Walter & Covinsky, 2001). To determine what this looks like in practice, Walter and Covinsky (2001) developed a framework to guide individualized cancer screening decisions in older patients and suggest it may be more useful to clinicians than age-based guidelines. The framework posits that three steps should be followed to make high-quality cancer screening decisions: (a) assess the patient’s overall health and estimated life expectancy, (b) consider the patient’s individual screening preferences and values, and (c) assess how the patient’s health, life expectancy, and individual screening preferences impact the potential benefits and harms of cancer screening (Walter & Covinsky, 2001). This narrative review focuses on the first step in this conceptual framework, anchoring screening decisions in estimates of an older adult’s life expectancy to facilitate weighing the risks/harms and benefits of screening for an individual older adult, as a critical, but under-implemented, first step for making individualized and informed cancer screening decisions.
Approach
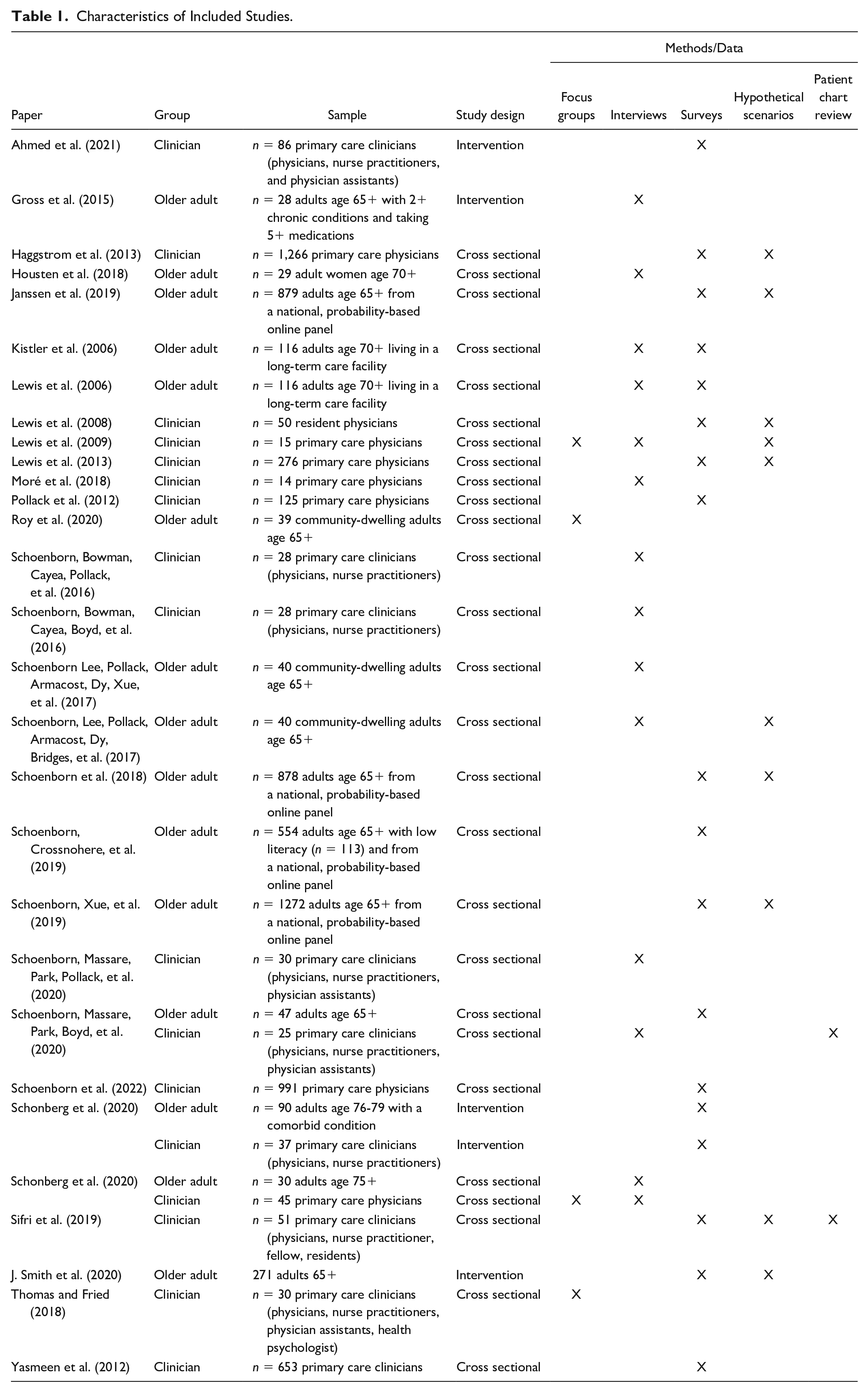
This review was guided by informational interviews with clinical and research experts on the topic of cancer screening in older adults to identify key questions and tensions in this decision-making context and generate a preliminary list of search terms. We searched PubMed to identify peer-reviewed studies reporting original data on clinician and older adult (aged 65 and older) perspectives and preferences on use of life expectancy in cancer screening decisions. following search strategy was used to identify clinician literature: (cancer screening) AND (clinician OR physician OR doctor) AND (older adult OR elderly OR older patient) AND (life expectancy OR prognosis). The following search strategy was used to identify older adult literature: (cancer screening) AND (older adult OR elderly OR older patient) AND (life expectancy OR prognosis). The database search identified nine articles meeting the inclusion criteria for clinician literature, 11 articles meeting the inclusion criteria for older adult literature, and three articles meeting the inclusion criteria for both clinician and older adult literature. References of the included articles were also reviewed to identify additional literature not found in the database search, resulting in one additional article meeting criteria for older adult literature, and five for clinician literature. Included articles were published between 2006 and 2021. Overall, most studies were observational (84%), report quantitative data (58%), and range in sample size from 14 to 1272 (median = 50). Details of included studies are presented in Table 1.
Characteristics of Included Studies.
First, we critically reviewed each article using a deductive analytic approach to identify findings related to pre-determined themes identified during the informational interviews with clinical and research experts. A deductive approach is useful when the structure of analysis can be operationalized and organized based on the basis of previous knowledge or pre-determined categories (Elo & Kyngäs, 2008). We focused on the following themes: beliefs and attitudes about life expectancy/prognosis, perspectives on cancer screening cessation and overscreening, life expectancy estimation, barriers and facilitators of life expectancy use for cancer screening decisions, and communication and discussion preferences regarding life expectancy. Next, we used an inductive data-driven approach to identify additional themes from the literature that emerged during the review and analysis process (Cavanagh, 1997; Elo & Kyngäs, 2008). We used a data extraction sheet to characterize findings and themes extracted from the articles during the analysis process by population (clinicians or older adults/patients) to allow for synthesis, comparison, and generation of key takeaways across studies (see Table 2).
Key Takeaways From Clinician and Older Adult Literature.
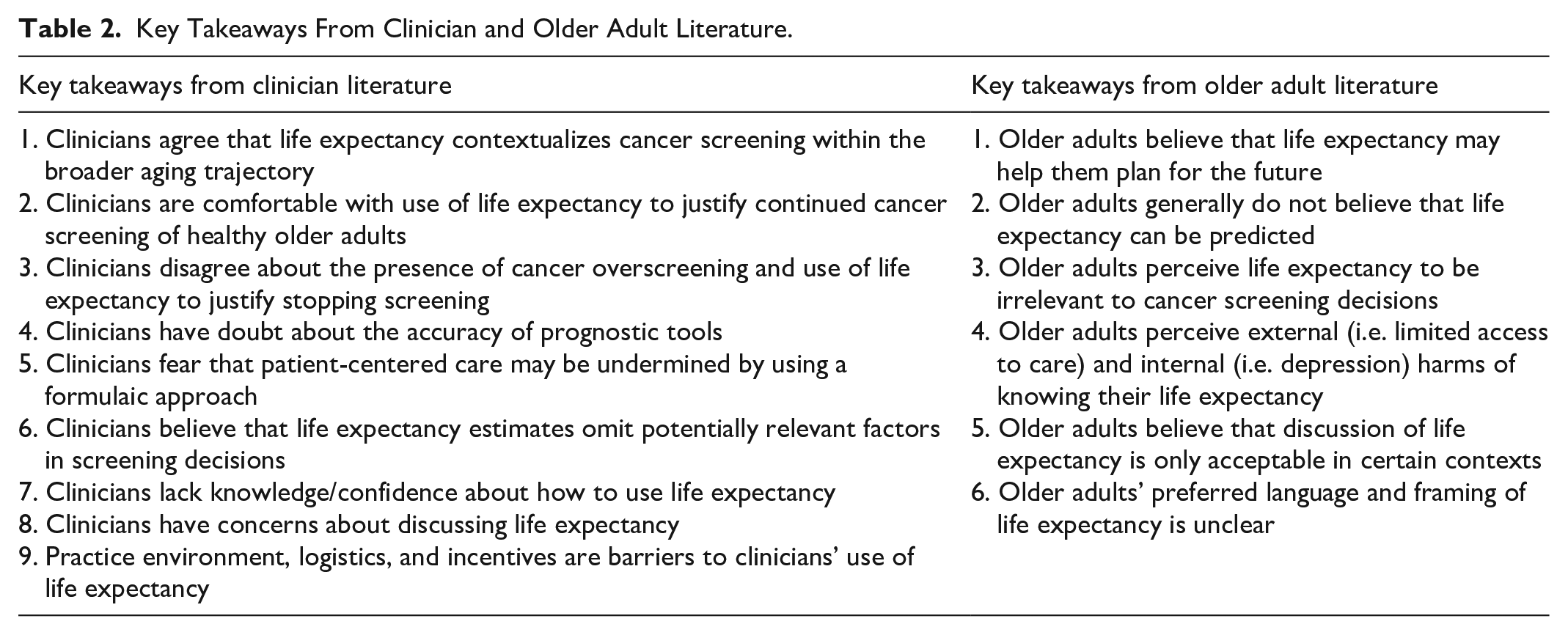
Below, we present nine key takeaways from the clinician literature that illuminate their perspectives and barriers to using life expectancy to guide cancer screening recommendations and discussions with older adults. Then, we present six key takeaways from the older adult literature that illuminate their perceptions and preferences about use of life expectancy in cancer screening discussions and decisions.
Findings
Clinician Perspectives on and Use of Life Expectancy Estimates
Clinicians Agree That Life Expectancy Contextualizes Cancer Screening Within the Broader Aging Trajectory
Clinicians reported broad perceived benefits of considering and discussing a patient’s life expectancy, including establishing realistic expectations for patients about medical care and health progression, encouraging conversations about future planning and advanced care, and promoting shared decision-making and collaborative decision-making through understanding of patient goals of care (Moré et al., 2018; Thomas & Fried, 2018). For example, Moré et al. (2018) interviewed a small sample of clinicians (n = 14; 78% geriatricians) who reported that discussions of long-term prognosis empower clinicians to more effectively collaborate with older patients and their family members in making appropriate care decisions by ensuring everyone involved understands the prognosis and goals of care (Moré et al., 2018).
Clinicians are Comfortable With Use of Life Expectancy to Justify Continued Cancer Screening for Healthy Older Adults
Clinicians perceive life expectancy estimates as a metric to optimize selection of healthy other adults to continue cancer screening by providing important context when considering lag-time benefit and potential harms of continued cancer screening (Lewis et al., 2009; Thomas & Fried, 2018). In particular, clinicians noted that life expectancy estimates provide clinicians with context for broader clinical considerations such as an older patient’s clinical decline, whether they are at an increased risk for adverse outcomes, and how different tests or procedures will impact the patient’s overall quality of life (Thomas & Fried, 2018). They also recognize that life expectancy may be a more helpful measure than age to determine who may benefit from screening, as life expectancy considers clinical and functional status of older adults (Moré et al., 2018; Schoenborn, Bowman, Cayea, Pollack et al., 2016). In addition, life expectancy is a particularly useful metric to help clinicians prioritize care decisions for older adults (Moré et al., 2018) and may facilitate more individualized cancer screening discussions and decisions (Lewis et al., 2013; Thomas & Fried, 2018). As such, clinicians believe it is appropriate to use life expectancy to justify continued cancer screening of healthy older adults, and report being comfortable recommending older adults continue cancer screening based on longer life expectancy estimates (e.g., >10 years) (Schoenborn, Bowman, Cayea, Pollack et al., 2016).
Clinicians Disagree About the Presence of Cancer Overscreening and Use of Life Expectancy to Justify Stopping Screening
While many clinicians believe life expectancy improves clinical assessment of older adults and optimizes selection for cancer screening, there is debate among clinicians about whether life expectancy should be used as a marker of overscreening or to justify the discontinuation or stopping of cancer screening. For example, Schoenborn et al. (2020) found that while most clinicians perceive overscreening for older patients with limited life expectancy to be harmful (60%), especially for those with multiple chronic conditions, others did not feel overscreening is a significant problem or think overscreening is acceptable (Schoenborn, Massare, Park, Pollack et al., 2020). Among clinicians who think overscreening is acceptable, some feel the benefits of screening and finding treatable cancers for individual patients outweighs the potential harms (Schoenborn, Massare, Park, Pollack et al., 2020), with some clinicians even stating that they believe that “it’s beneficial to screen for cancer at all ages” (Sifri et al., 2019). The same study also found controversy among clinicians around using limited life expectancy to define overscreening for cancer in older adults, with several clinicians expressing disagreement with the guideline framework of using limited life expectancy to guide discontinuation of cancer screening (Schoenborn, Massare, Park, Pollack et al., 2020). In a recent national survey of 991 primary care physicians, almost 25% did not agree that life expectancy of less than 10 years is a reasonable criterion for stopping cancer screening (Schoenborn et al., 2022). So, despite comfort recommending and justifying older adults continue cancer screening based on longer life expectancy estimates, clinicians report discomfort making judgments and recommendations about older adults stopping screening based on limited life expectancy (e.g., <10 years) (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Haggstrom et al., 2013; Yasmeen et al., 2012).
Clinicians Have Doubt About the Accuracy of Prognostic Tools
Despite recognition of the benefits of discussing life expectancy and long-term prognosis with older patients, clinicians doubt the accuracy and validity of prognostic tools citing unclear algorithms and concerns about missing variables. Several studies found that clinicians have concerns about the accuracy of life expectancy estimates and predication tools, and worry such estimates may not be able to accurately inform screening decisions (Lewis et al., 2009; Schoenborn et al., 2022; Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schoenborn, Massare, Park, Pollack et al., 2020; Thomas & Fried, 2018)., In addition to broader concerns about the accuracy of estimation tools, clinicians in several studies noted concerns about using life expectancy prediction tools or models based on population-level data to determine care for individual patients (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schoenborn, Massare, Park, Pollack et al., 2020; Thomas & Fried, 2018). Specifically, some clinicians feel it may be unfair when caring for an individual to base a care decision on population data (Thomas & Fried, 2018). Others questioned whether the predictive algorithms are accurate enough to apply to a single patient (Schoenborn, Massare, Park, Pollack et al., 2020). Thomas et al. (2018) found that clinicians who participated in focus groups about the scope of prognosis in the care of older adults also reported reservations about using mortality risk or life expectancy to make care management decisions (Thomas & Fried, 2018). A consistent finding across studies is that clinicians consider multiple clinical and individual factors to be important when evaluating whether an older patient is likely to benefit from continued cancer screening (Ahmed et al., 2021; Lewis et al., 2009, 2013; Moré et al., 2018; Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schoenborn, Massare, Park, Boyd et al., 2020; Schoenborn, Massare, Park, Pollack et al., 2020; Schonberg, Jacobson et al., 2020; Schonberg, Karamourtopoulos et al., 2020; Sifri et al., 2019; Thomas & Fried, 2018), and clinicians have further concerns that life expectancy estimation models may be missing important predictor variables or ability to account for changes in patient status over time (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schoenborn, Massare, Park, Pollack et al., 2020; Thomas & Fried, 2018).
Clinicians Fear That Patient-Centered Care may be Undermined by Using a Formulaic Approach
Clinicians also report several concerns that estimating life expectancy using a formulaic approach may negatively impact or undermine patient-centered care. For example, clinicians are concerned that implementing guidelines based on life expectancy and prognosis tools may introduce bias for the sake of reducing medical costs by denying screening for all older adults who have a calculated life expectancy of less than 10 years, or undermine patient-centered care by focusing more on numerical estimations and less on individual patient circumstances and preferences (Schoenborn, Massare, Park, Pollack et al., 2020).
Further, clinicians report concerns that life expectancy estimates may introduce bias and/or contribute the widening health disparities and inequities for racial and ethnic minorities as well as those with low socioeconomic status (Schoenborn et al., 2022; Schoenborn, Massare, Park, Pollack et al., 2020). Stemming from concerns about biased care, Schoenborn et al. (2020) found that clinicians interviewed about overscreening for cancer in older adults with limited life expectancy worry that use of life expectancy estimates may limit patient access to care, especially for racial minorities, as some clinicians perceive a link between using life expectancy to guide cancer screening and racism in the medical system (Schoenborn, Massare, Park, Pollack et al., 2020). Specifically, several of the 30 clinicians interviewed expressed concerns that prognostic tools use algorithms that consistently predict lower life expectancy for racial minorities. As a result, they are concerned that use of these tools will result in lower screening rates for those who may actually benefit from continued screening, and ultimately widen racial cancer health disparities (Schoenborn, Massare, Park, Pollack et al., 2020).
Clinicians Believe That Life Expectancy Estimates Omit Potentially Relevant Factors in Screening Decisions
Clinicians also note concerns that basing cancer screening decisions on life expectancy estimates may ignore or omit consideration of patient-perceived and non-mortality benefits of screening. For example, Schoenborn et al. (2020) found clinicians worry that use of life expectancy to inform screening decisions does not account for non-mortality-related benefits of cancer screening (Schoenborn, Massare, Park, Pollack et al., 2020). Specifically, they express concern that patient-perceived benefits of screening, such as the reassurance patients feel after screening negative for cancer, the potential to be able to use less invasive treatment if cancer is screened for and caught earlier, or the potential that cancer screening and diagnosis, may trigger positive changes and behaviors in older patients may not be accounted for in life expectancy estimates (Schoenborn, Massare, Park, Pollack et al., 2020). While older patients may overestimate the mortality and non-mortality benefits of cancer screening, clinicians appear to struggle to determine how best to balance patient-perceived benefits of screening with the potential harms of screening in those with limited life expectancy. This tension represents a notable challenge clinicians face in guiding appropriate screening decisions for older patients.
Clinicians Lack Knowledge/Confidence About How to Use Life Expectancy
Several studies suggest that clinician use and discussion of life expectancy may be dependent on the their perceived level of certainty regarding their clinical assessment of patient prognosis and potential to benefit from continued screening (Lewis et al., 2009, 2013; Moré et al., 2018; Schoenborn, Bowman, Cayea, Pollack et al., 2016). In a survey of 125 university-affiliated primary care clinicians, 66.4% reported difficulty assessing a patient’s life expectancy to guide screening recommendations (Pollack et al., 2012). In another study, Lewis et al. (2008) evaluated 50 resident physician’s life expectancy estimates and colon cancer screening recommendations for hypothetical 75-year-old and 85-year-old adults with good, fair, and poor health and found that resident life expectancy estimates were most accurate, and screening recommendations were most agreeable with guidelines, for the 75 year old and the 85 year old in good health (Lewis et al., 2008). Furthermore, resident-reported uncertainty about estimated life expectancy and benefits of screening were associated with letting a patient decide whether they want to screen or not rather than making a direct recommendation (Lewis et al., 2008). Findings from this and other studies suggest that clinicians may be more comfortable and accurate estimating life expectancy for older adults in good health and struggle with estimates when older adults have comorbidities or deteriorating health (Haggstrom et al., 2013; Yasmeen et al., 2012), and that both cancer screening recommendations for and discussions with older adults may be dependent on how confident they are in their ability to accurately estimate life expectancy (Lewis et al., 2008).
Furthermore, clinicians are generally unfamiliar with estimation tools, lack confidence in how to use them, and don’t know how to interpret estimates in a meaningful way. Many clinicians do not report consistently using validated prognostic tools to estimate the life expectancy of older patients. One reason is that some clinicians report being unfamiliar with validated tools and indices to estimate patient life expectancy (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Sifri et al., 2019). For example, a 2019 survey of 51 clinicians in an urban, academic setting, found that most (78%) do not use estimation tools to assist with decision-making about cancer screening in older adults, but many (60%) reported that they would find tools to estimate patient life expectancy helpful (Sifri et al., 2019). Despite interest in using life expectancy estimation tools, may clinicians have questions about how to interpret results and use them to make relevant clinical decisions for individual patients (Schoenborn, Bowman, Cayea, Pollack et al., 2016). However, even if clinicians are familiar with available tools, they may choose not to use them because of reservations about using prognostic indices to generate life expectancy estimates (Thomas & Fried, 2018).
Clinicians who generally do not use validated prognostic tools to assess life expectancy in older adults sometimes instead use a “gestalt” sense or estimate based on their clinical experience and relationship with the patient (Moré et al., 2018; Schoenborn, Bowman, Cayea, Pollack et al., 2016; Thomas & Fried, 2018). Some clinicians report not using prognostic or life expectancy estimation tools at all, relying entirely on their gestalt estimate (Schoenborn, Bowman, Cayea, Pollack et al., 2016). Others use a combination of prognostic tools and their gestalt estimate (e.g., using mortality risk indices for the purposes of confirming their gestalt estimates of long-term prognosis to inform their care decisions) and feel that prognostic tools are not a substitute for clinical acumen (Thomas & Fried, 2018).
Notably, clinicians do not feel they have had adequate training about how to use prognosis in medical school, residency, or as practicing physicians (Ahmed et al., 2021; Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020; Sifri et al., 2019). Although a web-based training intervention showed short-term improvements in clinician attitudes about the importance of life expectancy in cancer screening, their confidence estimating life expectancy, confidence in communicating a recommendation to stop cancer screening, and knowledge on preferred ways to discuss cancer screening, the effects of the intervention waned by 6 months (Ahmed et al., 2021).
Clinicians Have Concerns About Discussing Life Expectancy
Clinicians see prognosis as a difficult topic to talk about (Ahmed et al., 2021; Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020). Overall, they don’t know how best to communicate about life expectancy with older patients and are unsure how to navigate anticipated negative reactions. For example, Schonberg et al. (2020) found younger clinicians (under age 40) in particular expressed needing guidance and did not feel they had “good language” for conversations about life expectancy (Schonberg, Jacobson et al., 2020). Compounding these concerns, clinicians also fear patients will react negatively to their life expectancy being estimated or used to determine what kind of care is appropriate for them (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020; Sifri et al., 2019; Thomas & Fried, 2018). For example, clinicians are concerned that patients will perceive them as judgmental, as abandoning, giving up, and not doing everything they can for their patients, or as rationing care if prognosis is incorporated into clinical decisions (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020). These concerns are amplified when communicating with older patients who have low literacy or who are highly educated, who have decreased cognition, or who do not have a strong patient-clinician relationship (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020).
There is also uncertainty among clinicians about whether life expectancy should be discussed with patients when recommending patients stop cancer screening. Some clinicians report that they omit cancer screening from clinical discussions entirely or subtly hint patients no longer need to screen rather than explicitly making a recommendation to stop screening or discussing the patient’s life expectancy (Schoenborn, Bowman, Cayea, Boyd et al., 2016). For example, Schonberg et al. (2020) found clinicians approach this topic by informing patients over age 75 that guidelines recommend they are no longer screened because they would rather patients think the recommendation is coming from guidelines than the clinician themselves (Schonberg, Jacobson et al., 2020).
Practice Environment, Logistics, and Screening Incentives are Barriers to Clinicians’ Use of Life Expectancy
Other barriers clinicians face to incorporating life expectancy into clinical decisions are related to practice logistics or environment. These include time constraints during clinical visits with patients that limit time for potentially difficult and sensitive discussions about life expectancy, the lack of emphasis or value placed on prognosis in societal or health care culture, incentives in the practice environment that encourage screening without consideration of life expectancy, and even concern about litigation (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020; Thomas & Fried, 2018). For example, clinicians fear that using life expectancy to determine screening may reduce uptake in certain populations. In particular, they fear legal scrutiny if they recommend against screening due to a patient’s limited life expectancy but the patient ends up with cancer (Schoenborn, Bowman, Cayea, Pollack et al., 2016; Schonberg, Jacobson et al., 2020).
Older Adult perspectives on Use of Life Expectancy Estimates
While clinicians can approach life expectancy estimation as one part of providing appropriate care for their patients, estimating life expectancy may be a very personal experience for an individual patient. As such, life expectancy is a fundamentally different concept to clinicians and patients, and older adults have distinct beliefs, attitudes, and preferences on the use of their life expectancy to inform their care.
Older Adults Believe That Life Expectancy May Help Them Plan for the Future
Older adults do perceive that knowing their life expectancy may benefit their health or health outcomes, positively impact their relationship with their clinician, and help them plan for the future (Kistler et al., 2006; Schoenborn et al., 2018). For example, Kistler et al. (2006) found that participants who expressed interest in knowing and discussing life expectancy with their clinicians believed it would help them with their ability to plan for the future, help them maintain open communication with their clinician as they age, and provide them with important knowledge about their own health (Kistler et al., 2006). A national online panel survey of adults 65 and older conducted by Schoenborn et al. (2018) found that participants felt discussing life expectancy could be beneficial by helping them better plan for the rest of their life and felt it was important to be open and honest in a patient-clinician relationship (Schoenborn et al., 2018). Other benefits mentioned in open-ended responses include the potential to identify what could be changed to extend their life, to help family members plan, and to satisfy curiosity for those who “just want to know” (Schoenborn et al., 2018).
Older Adults Generally do not Believe That Life Expectancy can be Predicted
Like clinicians, however, older adults are skeptical that their life expectancy, or how much longer they are going to live, can be predicted. As such, older adults question the accuracy of calculated life expectancy estimates and their clinicians’ ability to accurately predict how much longer they will live (Janssen et al., 2019; Kistler et al., 2006; Roy et al., 2020; Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017; Schonberg, Jacobson et al., 2020; Schonberg, Karamourtopoulos et al., 2020). For example, Kistler et al. (2006) found that among 116 highly-educated older adults age 70 and older, interviewed regarding their beliefs about physician-estimated life expectancy in the context of cancer screening, 64% didn’t think their clinician could accurately estimate their life expectancy, citing personal experience with incorrect estimates, complexity of medicine/lack of physician knowledge, and uncertainty as reasons why (Kistler et al., 2006). Among the 36% of participants who agreed or strongly agreed with the statement “I feel my main doctor can correctly estimate how long I might live,” most also acknowledged the limitations and uncertainty of clinicians making such predictions (Kistler et al., 2006). In a more recent study of 879 adults ages 65 and older, Janssen et al. (2019) found that only 14% of participants surveyed believed doctors can accurately predict life expectancy, and 47% did not (Janssen et al., 2019). There is also some evidence to suggest that faith or religious beliefs impact beliefs about accurately predicting or estimating life expectancy, with older adults across several studies believing that “only God truly knows” how long somebody has left to live (Housten et al., 2018; Kistler et al., 2006; Roy et al., 2020; Schoenborn et al., 2018).
Older Adults Perceive Life Expectancy to be Irrelevant to Cancer Screening Decisions
In addition, many older adults perceive cancer screening to be beneficial no matter what, so most feel that life expectancy is irrelevant. Participants in several studies specifically reported that they intended to get screened for cancer as long as they live, even if it does not improve their life expectancy (Housten et al., 2018; Lewis et al., 2006; Schoenborn, Xue et al., 2019). Moreover, educational interventions explaining the importance of life expectancy and health status on the potential benefits of screening do not appear to influence older adults’ cancer screening decisions even if they had a limited life expectancy (Gross et al., 2015). Many older adults state that do not find life expectancy relevant to cancer screening decisions and do not want to discuss it with their clinician (Lewis et al., 2006; Roy et al., 2020). For example, Lewis et al. (2006) found that among 116 adults 70 and older interviewed about continuing cancer screening later in life, 62% believed their own life expectancy was not an important factor for decision-making, and 48% preferred not to discuss life expectancy at all (Lewis et al., 2006).
Many older adults express preferences to receive individualized information to inform their cancer screening decisions but do not understand the relevance or support discussion of their life expectancy (Janssen et al., 2019; Roy et al., 2020; Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017; Schonberg, Jacobson et al., 2020). A small intervention study did find that at least some adults over the age of 75 thought life expectancy information would be helpful when deciding on cancer screening (Schonberg, Karamourtopoulos et al., 2020). However, there is also evidence that younger adults assign more importance to life expectancy when considering screening decisions than older adults do (Janssen et al., 2019).
Older Adults Perceive External (ie., Limited Access to Care) and Internal (i.e., Depression) Harms of Knowing Their Life Expectancy
Older adults report negative perceptions of the concept of life expectancy, fears about knowing life expectancy, and concerns that discussing life expectancy with their clinician may limit their access to care. Specifically, one study reported that older adults may worry that discussions about life expectancy might limit their access important tests with the potential to keep them alive longer, expressing skepticism about the screening lag-time to benefit, or holding beliefs that cancer screening may still help them live longer lives (Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017). More generally, some older adults report being uncomfortable discussing predictions of how long they have left to live, perceiving a negative connotation of the term or the idea of life expectancy (Roy et al., 2020; Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017).
In addition, older adults report internal harms of knowing or discussing their life expectancy and fear it may negatively impact them or their outlook on life. For example, Kistler et al. (2006) found that participants who did not want to know or discuss their life expectancy with their clinicians feared it might “discombobulate” them, interfere with their will to live, or color all of their subsequent decisions in life (Kistler et al., 2006). Similarly, Schoenborn et al. (2018) found that participants feared discussing their life expectancy could negatively impact their quality of life, and may worry or depress them (Schoenborn et al., 2018).
Older Adults Believe That Discussion of Life Expectancy is Only Acceptable in Certain Contexts
Older adults perceive talking about life expectancy with a clinician to be acceptable only in specific contexts or for specific purposes. Many appear to believe that life expectancy should only be discussed when it becomes limited. For example, a third of participants in a qualitative study of 40 adults age 65 and older did not want to discuss life expectancy at any time, a third said they wanted to discuss life expectancy only toward the end of life, and a third said they wanted to discuss life expectancy if it were longer than one year (Schoenborn, Lee, Pollack, Armacost, Dy, Xue et al., 2017). In addition, a survey of 878 adults age 65 and older found that the longer a hypothetical patient was expected to live, the smaller the proportion of participants who wanted to discuss life expectancy (Schoenborn et al., 2018). The same study also found that over half of participants (56%) only wanted to discuss life expectancy if it were less than two years, and 35% did not think a clinician should even offer the discussion about life expectancy at all (Schoenborn et al., 2018). On a related note, having a past experience with either a life-threatening illness or having discussed the life expectancy of a loved one were independently associated with participants wanting to discuss life expectancy with a clinician (Schoenborn et al., 2018).
Several studies in this review also found that older adults are more open to discussing and stopping screening if they are in a trusting relationship with their clinician (Housten et al., 2018; Roy et al., 2020; Schoenborn et al., 2018; Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017), and that older adults report less trust in clinicians’ recommendation to stop screening than to continue screening (Housten et al., 2018; Roy et al., 2020; Schoenborn, Massare, Park, Boyd et al., 2020). For example, Housten et al. (2018) interviewed a racially/ethnically diverse group of women aged 70 and older and found that participants reported they would continue mammography screening even if a doctor specifically told them that it would not increase their life expectancy, and that the recommendation against screening might make them question their doctor’s advice (Housten et al., 2018).
However, some older adults appear open to hearing or discussing life expectancy to inform cancer screening decisions to explain a clinician recommendation against screening (Schoenborn et al., 2018; Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017). For example, Schoenborn et al. (2018) conducted a national, probability-based online panel survey of adults ages 65 and older and found that 78.7% of participants did not think life expectancy should be discussed in the context of stopping cancer screening unless it was to provide justification for why a clinician recommended a patient stop screening (Schoenborn et al., 2018). In an earlier study, Schoenborn et al. (2017) found that older adults preferred their clinician explain a recommendation to stop screening by incorporating individual health status but were divided on whether life expectancy should explicitly be mentioned (Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017).
Older Adults’ Preferred Language and Framing of Life Expectancy Information in Unclear
Overall, it is unclear how life expectancy information or estimates should be discussed and framed to make it understandable, useful, and relevant to older adults for cancer screening decisions. A consistent finding across studies is that language and strategic framing are important when clinicians communicate with older adults about life expectancy and cancer screening. Several studies highlight the importance of clinicians using language that resonates with their patients (Schoenborn, Crossnohere et al., 2019; Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017; J. Smith et al., 2020). For example, a qualitative study that tested communication strategies for discussing screening cessation found that participants prefer phrasing that emphasizing screening tests may harm more than benefit (due to life expectancy), rather than explicitly saying they would not live long enough to benefit from the screening tests; patients felt that explicit phrasing was too “harsh” (Schoenborn, Lee, Pollack, Armacost, Dy, Bridges et al., 2017). Schoenborn et al. (2019) assessed the preferences of older adults aged 65 and older (n = 113 low literacy participants, n = 441 participants from national sample) regarding how clinicians frame and discuss colorectal cancer screening cessation and found explanations that mention life expectancy ranked low in both samples (Schoenborn, Crossnohere et al., 2019). In both groups, the most preferred phrase to explain colonoscopy cessation was “your other health issues should take priority” (Schoenborn, Crossnohere et al., 2019).
However, one study raised questions as to whether this “preferred” phrasing regarding life expectancy is appropriate. A 2020 randomized control trial built upon Schoenborn et al.’s 2019 findings and used an experimental design and hypothetical scenarios to investigate how incorporating health status and life expectancy into clinical conversations impacts older adults’ (n = 271; age 65-90) decision-making about screening cessation (J. Smith et al., 2020). They found that among participants who read statements about screening and life expectancy that were framed “negatively” (e.g., they may not live long enough to benefit from screening), intention to screen was lower and participants were more clear about their values related to their screening decision than those who received statements about their health status and screening (“your other health issues should take priority”) (J. Smith et al., 2020). However, those who read ‘positively’-framed statements about life expectancy (e.g., screening would not help them live longer) had higher cancer anxiety, reported lower trust in their clinician, and were less clear about their values related to their screening decision that those who read the negative framing about life expectancy (J. Smith et al., 2020). As such, there is limited evidence as to which discussion framing or specific phrasing about life expectancy are most accepted and most effective for cancer screening decision-making.
Discussion
Overall, clinicians believe that while there are benefits of considering a patient’s life expectancy, they question the accuracy of life expectancy estimates, are uncomfortable discussing such estimates, and identify multiple barriers to understanding and using life expectancy in the context of cancer screening. Clinicians do not know how to practically estimate life expectancy of individual patients, use estimates to make screening recommendations when life expectancy is limited, or discuss such estimates with patients to guide appropriate screening decisions, especially when it comes to stopping screening. These estimation barriers are consistent with broader literature reporting that lack of prognostic confidence is a primary cause of clinician reluctance to communicate prognostic information to older adults at the end of life (Hallen et al., 2015), and that clinicians are inconsistent, inaccurate, and often underestimate patient life expectancy (Clarke et al., 2009). Furthermore, these findings bring attention to an important gap between cancer screening guidelines that recommend assessing older adults’ life expectancy and the lack of training, tools, and confidence clinicians have to implement such guidelines in practice.
Many older adults, by contrast, challenge the idea that life expectancy can be estimated and see its discussion or use by clinicians as either irrelevant or potentially harmful. As such, many older adults don’t want to talk about their life expectancy. Those that do believe it should be discussed only in certain contexts such as when it is limited or to explain a clinician’s recommendation against cancer screening, rather than as a routine or stand-alone discussion to inform care or screening decisions. Such limits on the use of life expectancy are congruent with the large extent of literature on patient discomfort with discontinuing care in a range of contexts, including deprescribing or discontinuing medications (Brokaar et al., 2022; Burghle et al., 2020; Vordenberg & Zikmund-Fisher, 2020) and stopping cancer screening (Brotzman et al., 2022; Lewis et al., 2010; Torke et al., 2013). Patient discomfort and resistance to discontinuing care may reflect broader societal enthusiasm for screening and beliefs that more care is better care (O’Keeffe et al., 2021; Schwartz et al., 2004), well-documented clinician discomfort and reluctance to recommending against screening (Hoffman et al., 2010; Schonberg, 2018; Zikmund-Fisher et al., 2017), and multi-level challenges and complexities of deimplementing low-value care (Austin et al., 2021; Norton & Chambers, 2020; J. Smith et al., 2021).
Moving forward, it is important to prioritize research that solves clinician-perceived barriers and problems with life expectancy. If guidelines expect clinicians to use life expectancy to inform cancer screening recommendations for older patients, then they must be able to confidently estimate life expectancy, believe it is a relevant metric, and be able to effectively convey that to patients. Work is needed to investigate specifically how clinicians estimate the life expectancy of older patients in practice (including which factors they consider in such estimates, and which, if any, tools they use), in which contexts they consider life expectancy to be relevant, and how they communicate life expectancy estimates (quantitatively/numerically, qualitatively/conceptually, or as a threshold consistent with screening guidelines).
An important clinician concern identified in this review is related to health equity and concerns of bias in both the tools/algorithms used to estimate life expectancy of individuals and the gestalt estimates of life expectancy clinicians make themselves. Specifically, clinicians are concerned about race being used as a variable in estimates of life expectancy. While validated tools may not use race as a variable, they sometimes include factors that are influenced and patterned by race and that embody other biases and inequities in health across the life course. Some of these concerns about bias and inequities embedded in predictive models have been explored (Lantz & Ubel, 2005; Paulus & Kent, 2017, 2020; Vasan & van den Heuvel, 2022). As such, clinician skepticism of tools and concerns about exacerbating health inequities or limiting access to care, to some degree, is appropriate. There is potential for the tools that estimate life expectancy to be biased which may interact with some of the themes and findings in this review. Validated tools (and included variables) to estimate life expectancy to guide cancer screening decisions can be found on the e-prognosis website (http://eprognosis.ucsf.edu/).
In addition, we find evidence that both clinicians and older adults are generally uncomfortable using life expectancy in cancer screening decisions, but it is unclear whether these attitudes reflect discomfort and uncertainty toward the practice of applying a numerical value or estimate to life expectancy or toward the broader concept of life expectancy and prognosis in determining appropriate care. Future work should investigate and clarify the root source of patient and clinician discomfort with life expectancy both broadly and in the context of cancer screening.
It is important to recognize that the perspectives and concerns reported in past research may be based on hypothetical scenarios (see Table 1) or reflect discussions that are inconsistent with discussions recommended in cancer screening guidelines. Even when patients have reported on actual clinician encounters, their interactions have likely been with clinicians who are generally uncomfortable and untrained in how to estimate, use, and discuss their life expectancy as a metric to guide preventive care decisions. As such, it is unclear from this review whether older adults’ skepticism and attitudes about life expectancy reflect the uncertainty of clinicians’ beliefs and communication. It is possible that patient concerns may lessen and/or change if they are presented with clearer and more consistent messages about the relevance of their life expectancy in cancer screening decisions as they get older. Prioritizing research and the development of interventions to reduce the operational barriers clinicians face (e.g., improve clinician knowledge, skill, and confidence using and discussing life expectancy) is a necessary precursor for more accurate and actionable investigations of both clinician and older patient perceptions on use of life expectancy, especially when older adults face conceptual barriers to understanding life expectancy.
We limited this review to literature reporting on older adults aged 65 and older. We acknowledge that other authors have explored adult perspectives on life expectancy in younger populations (e.g., starting at age 50 or 60) and in other contexts (Kobayashi et al., 2017; Shubella et al., 2022; von Wagner et al., 2013). However, it is highly unlikely that people in younger populations face limited life expectancy or decisions to stop cancer screening. While questions about how adults of all ages perceive life expectancy and consider their life expectancy when making medical decisions are interesting, they are hypothetical for cancer screening decisions in populations younger than 65 years of age. As such, we felt it important to narrow our scope to patient populations for whom life expectancy questions are more personally relevant and imminent.
It is also important to acknowledge that while there is a small but growing literature on the use of life expectancy to guide cancer screening decisions in older adults, the majority of literature on this topic and in this review is dominated by one US-based research team and their interlocking collaborators. As a result, the findings presented here may not reflect a broad spectrum of perspectives or capture important differences which may exist in other countries and health systems. Though this small group of researchers has generated much of the literature in this review, it is worth noting they have used a range of rigorous and well-designed methods and approaches to investigate this decisional context, including collecting data on both clinicians and older adults, using hypothetical scenarios and individual perspectives collected in nationwide surveys, EHR and patient chart review, and qualitative interviews and focus groups. We laud these researchers for pursing this important and understudied area using diverse methods and approaches, while still acknowledging that a broader range of questions, contexts, and researchers is needed to fully understand the role of life expectancy in cancer screening guidelines, recommendations, decisions, and behavior.
This review has looked at older adult and clinicians’ perspectives on life expectancy narrowly in the context of cancer screening decision-making. However, tensions with the use of life expectancy as a decision-making metric occur in broader initiatives and interventions as well. For example, there are many efforts to research and reduce low-value care (Colla et al., 2015; Wolfson et al., 2014; Zikmund-Fisher et al., 2017), including those to deprescribe medication for older adults with limited life expectancy (Brokaar et al., 2022; Burghle et al., 2020; Wu et al., 2021) and discontinue overscreening for cancer more broadly when older adults no longer derive mortality benefits (Dossett et al., 2022; Kotwal et al., 2019; Pollack et al., 2012; Schoenborn, Boyd, Lee, Cayea, & Pollack, 2019). As such, the findings from this review may have broader implications for investigating and informing how best to implement life expectancy discussions in preventive and other health care contexts to better assess the risks and benefits of care, and better individualize care and patient–clinician communication to ultimately reduce low-value care among older adults.
Life expectancy is a population-level construct that does not always neatly apply to or predict what will happen with any individual patient. As such, it is really a conceptual shift to move from age-based cutoffs that are chosen based on population-level expectations of life expectancy to individually-tailored screening decisions that, in principle, should be based on personalized estimates of life expectancy. This shift is even more challenging when insurance payment approvals remain driven by age-based cutoffs (Norton & Chambers, 2020). It is hardly surprising that both this review and prior literature on cancer screening decisions find that both clinicians and patients feel little incentive to limit or discontinue screening for patients with shorter life expectancy if insurance plans will still pay for these low-value tests (Austin et al., 2021; Norton & Chambers, 2020; J. Smith et al., 2021). Developers of screening guidelines need to anticipate that recommendations for decision rules that rely on calculation and discussion of life expectancy are likely to face significant implementation challenges.
Finally, it is worth noting that life expectancy will always be a difficult topic for clinicians and patients. There is a natural desire for hope in the face of uncertainty which conflicts with the need to avoid unnecessary and potentially harmful screening that is unlikely to benefit an older patient. There are clear advantages to incorporating life expectancy in cancer screening decisions (and clear costs both financial and medical of failing to do so). So, the question should not be whether to consider life expectancy in such care decisions, but how to overcome the barriers outlined in this review to make life expectancy an appropriate component of cancer screening decision-making.
Footnotes
Acknowledgements
The authors thank Dr. KD Valentine for her thoughtful review and feedback on an early version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L.E.B. received support from the National Institutes of Health (grant: T32 AG027708).