
Abstract
The impact of safety-net hospital (SNH) acquisition by health systems on specialty care delivery remains unclear, with important implications for access and equity. We examined how SNH acquisitions affect oncology service availability, volumes, and patient characteristics among Medicare fee-for-service beneficiaries using claims data from 2008 to 2019. We identified 75 SNH acquisitions from 2011 to 2015 and 151 independently operated SNHs as controls, estimating changes using a weighted stacked event study design. Following acquisition, chemotherapy volumes increased significantly by 99.6 annual claims (95% CI: [21.9, 177.3]), representing an 84% increase from baseline, while advanced imaging, radiation therapy, and cancer-directed surgical volumes showed no significant changes. We observed no changes in service line availability or patient demographics including race and ethnicity, dual eligibility, or age. These findings suggest system integration may lead to selective expansion of scalable or financially favorable oncology services without markedly altering overall service offerings or Medicare populations served by SNHs.
Introduction
Safety-net hospitals (SNHs) are essential components of the U.S. health care system, serving as key access points for low-income, uninsured, immigrant, rural, and racially marginalized populations (America’s Health Care Safety Net: Intact but Endangered, 2000; Characteristics of Safety-Net Hospitals, 2014 #213, n.d.). Despite their central role in advancing health equity, many SNHs operate under persistent financial strain, with constrained resources, limited access to capital, high rates of uncompensated care, and workforce shortages (America’s Health Care Safety Net: Intact but Endangered, 2000; Bazzoli et al., 2012). These challenges undermine their ability to consistently deliver high-quality care—particularly specialty care, for which SNHs often have informal and fragmented referral networks (RAND Policy Insights, n.d.).
In recent decades, the structure of the U.S. health care system has also been fundamentally reshaped by the growing dominance of large health systems, which are increasingly acquiring hospitals and physician groups (Andreyeva et al., 2023). While such acquisitions are frequently justified as mechanisms to enhance coordination and preserve patients’ access to financially distressed providers, empirical evidence on their outcomes is mixed. Studies show that such vertical integration often leads to higher prices without commensurate improvements in care quality (Beaulieu Nancy et al., 2020; Cutler & Scott Morton, 2013; Mariani et al., 2022; Satiani et al., 2025). For SNHs, the implications of acquisition may be especially consequential. Prior work has raised concerns that SNH acquisitions may reduce the availability of core safety-net functions—particularly if system-level priorities do not align with local community needs (Henke et al., 2021; Oyeka et al., n.d.; Wood et al., 2024). Recent work has shown that following acquisition, some SNHs reduce important service lines such as obstetrics, inpatient psychiatry, and substance use disorder (SUD) treatment, potentially harming the care of underserved populations (Henke et al., 2021; Wood et al., 2024). However, evidence has also shown potential benefits. Integration of an SNH into a larger health system, however, may also offer financial stabilization and in some cases improved access to primary and specialty services (Bazzoli et al., 2003; Fact Sheet: Hospital Mergers and Acquisitions Can Expand and Preserve Access to Care, 2025 ; Oyeka et al., n.d.). A recent study of an acquisition and system integration of a large SNH reported improved quality outcomes, reductions in mortality, and improved patient experiences (Wang et al., 2022). Other work has found that acquisitions of rural hospitals, which are disproportionately located in low-income areas, were associated with reductions in in-hospital mortality for certain cardiovascular conditions (Jiang et al., 2021). Together, these findings highlight the mixed potential effects of acquisition on the financial viability, quality outcomes, and service line offerings at SNHs, which heavily impact the type of safety-net role these hospitals play in their communities.
The effect of SNH acquisitions on specialty care delivery is unclear, with potential for both service line expansion and reduction. Health systems often acquire SNHs when these hospitals have experienced periods of financial turbulence and publicly emphasize the value of acquisition in preserving and expanding access to specialty services. From this perspective, system affiliation could enhance specialty care through several pathways: providing capital for infrastructure investments in treatment facilities and equipment; facilitating clinical integration through access to specialist networks, multidisciplinary tumor boards, and evidence-based treatment protocols; achieving operational efficiencies through economies of scale in drug and equipment procurement, specialized staffing, and utilization management; and positioning specialty services as strategic priorities for investment. These potential benefits are especially salient for resource-constrained SNHs that may lack the capital or clinical infrastructure to independently expand complex specialty services.
However, acquisition could also lead to changes that reduce local service availability or negatively alter patterns of care delivery. Systems may consolidate high-complexity specialty care at flagship facilities to achieve quality improvements, operational efficiency, or volume-based advantages, potentially reducing service availability at lower-volume, peripheral hospitals. They may also redirect patients to higher-volume centers within the system to maximize reimbursement or clinical outcomes, or reallocate resources toward other service priorities that better align with system-level strategic goals. This would be particularly concerning for SNHs, given that the geographic proximity of specialty services has important implications for access among vulnerable populations who may face transportation barriers or challenges navigating referrals across multiple facilities. Whether system acquisition of SNHs leads to expanded local specialty services, the consolidation of care at larger health system hospitals, or other changes in patient care remains an empirical question with significant implications for health equity.
Existing research has largely focused on the effects of SNH acquisitions on core hospital services, but less is understood about their impact on access to specialty care service lines when these hospitals are absorbed into larger systems. Oncology offers a particularly informative case study through which to study these dynamics. Cancer is a leading cause of death in the United States. Cancer care is financially burdensome, inherently multidisciplinary, and often requires substantial upfront investments to provide treatments such as infused systemic therapy, radiation therapy, or complex surgeries (Common Cancer Sites—Cancer Stat Facts, n.d.). Stark inequities in cancer-related care access, diagnosis, and treatment remain widespread, underscoring the importance of cancer care for patients treated in safety-net settings (Chan et al., 2017; Crown et al., 2022; Goding Sauer et al., 2019; Perlow et al., 2018). In this study, we examined how the acquisition of SNHs by health systems affected oncology service availability, service volumes, and the characteristics of the patients served at acquired SNHs.
New Contribution
This study addressed several important gaps in understanding how health care consolidation affects specialty care delivery in safety-net settings. First, while prior research has examined how SNH acquisitions affect certain core hospital services such as obstetrics, psychiatry, and SUD treatment, we focused specifically on oncology service lines—an area where evidence has been limited. Second, to our knowledge, this is the first analysis to use health care claims data to assess oncology service availability and volumes at SNHs following acquisition, rather than relying on survey responses about service line provision. Using 100% Medicare fee-for-service claims from 2008 to 2019, we directly examined changes in service availability, volumes, and patient characteristics following acquisition across four distinct oncology service lines: chemotherapy, radiation therapy, advanced imaging, and cancer-directed surgery. Our findings revealed that system integration led to selective expansion of certain oncology services, such as chemotherapy, without broader changes in service line availability or the characteristics of the Medicare fee-for-service populations served by SNHs, suggesting that this type of consolidation may favor scalable or financially favorable services. These results contribute to a broader understanding of how health system acquisitions of SNHs may shape specialty care in the health care safety net.
Method
Data Sources and Hospital Sample
We constructed a longitudinal dataset of general acute care SNHs and their system affiliations using data from the Health System and Provider Database (HSPD) and the Centers for Medicare & Medicaid Services Healthcare Provider Cost Reporting Information System (HCRIS) from 2010 through 2018. The HSPD is a relational database containing information on health system ownership of hospitals, clinics, and physician groups (Health Systems and Provider Database (HSPD) Methodology—Data Resources, n.d.). Using publicly available HCRIS data, we classified hospitals as SNHs if they fell within the top quartile in their state on either of two measures during the first 2 years of observation in the study period: the Disproportionate Share Hospital (DSH) index or uncompensated care as a share of operating expenses (Hefner et al., 2021; Popescu et al., 2019; Winkelman & Vickery, 2019). This composite definition was used to capture the heterogeneity of the safety net, as DSH-based classifications typically identify larger, urban academic hospitals, whereas uncompensated care measures are more likely to capture smaller, often rural providers (Chatterjee et al., 2020; Hefner et al., 2021; Popescu et al., 2019). This composite approach reduces over-reliance on a single metric and better reflects the heterogeneity of SNHs. DSH-based classifications typically identify larger, urban academic hospitals, whereas uncompensated care measures are more likely to capture smaller, often rural providers (Chatterjee et al., 2020; Hefner et al., 2021; Popescu et al., 2019). By combining both measures, we capture the breadth of hospitals serving safety-net functions, both larger urban teaching hospitals and smaller rural facilities at financial risk, allowing our findings to be relevant across diverse safety-net settings. Baseline hospital characteristics included size (bed count), rurality (based on Metropolitan Statistical Area designation as in the Medicare Cost Reports), ownership type (public, for-profit, or nonprofit), and receipt of Graduate Medical Education (GME) payments.
Identifying Acquisition Events
We used the HSPD to identify SNH acquisitions, defined by any event in which an SNH changed from independent to system-affiliated status in the HSPD between 2011 and 2015. Within the HSPD, a health system is defined as a set of jointly owned or managed provider organizations that includes at least one general acute care hospital, 10 primary care physicians, and 50 total physicians operating within a single hospital referral region. Treatment group hospitals were required to have independent ownership for at least 3 continuous years preacquisition and system-ownership for at least 4 years postacquisition to ensure sufficient pre- and postperiods for establishing trends and evaluating changes in outcomes, particularly those requiring major investments such as the establishment of new service lines. SNHs acquired after 2015 were not included in the treatment group but were retained as controls up until their acquisition year. All identified transactions were manually validated via public records. Hospital ownership type and status were also manually verified across the study period.
Patient Population and Outcomes
We used 100% Medicare Inpatient and Hospital Outpatient files from 2008 through 2019 to identify fee-for-service beneficiaries who had any inpatient or outpatient claim (within the cancer-related service lines described below) with a cancer diagnosis code from an SNH in our sample (Supplemental Appendix 1). For analyses requiring patient attribution to hospitals, attribution was done based on where patients received the plurality of their hospital-based oncology services within a given calendar year.
Oncology Service Lines
We assessed oncology service lines across four domains: (a) physician-administered chemotherapy services, including cytotoxic chemotherapy, targeted therapies, and immunotherapy; (b) radiation therapy procedures, encompassing both planning and treatment delivery codes for basic and advanced radiation modalities; (c) advanced imaging services, including positron emission tomography (PET), computed tomography (CT), and magnetic resonance imaging (MRI) scans; and (d) breast and colorectal surgical resections, including lumpectomies, mastectomies, and colonic or rectal resections. We focused on breast and colorectal surgical resections—including lumpectomies, mastectomies, and colon or rectal resections—because these are among the most common cancer-related procedures and are procedures that could plausibly be performed by general surgeons, including those practicing in resource-limited or more remote hospital settings. Procedures were identified using International Classification of Diseases, Ninth Revision (ICD-9), International Classification of Diseases, 10th Revision (ICD-10), and Current Procedural Terminology (CPT) codes (Supplemental Appendix 2).
Dependent Variables
We evaluated two primary hospital-level oncology measures for each treatment modality: service availability and service volume. Service availability was defined using binary indicators for whether a hospital billed at least five unique claims with a relevant cancer diagnosis code in each year for physician-administered chemotherapy (including cytotoxic chemotherapy, targeted therapy, and immunotherapy), radiation therapy, cancer-directed surgery for breast or colorectal cancer, or cancer-related advanced imaging. Service volume was the total number of unique cancer-related claims for each type of service. In addition, we assessed changes in the characteristics of patients with cancer treated at the SNH, examining the proportion of fee-for-service Medicare beneficiaries receiving each service who were dually eligible for Medicare and Medicaid and whose race and ethnicity were non-Hispanic Black or Hispanic (based on the Medicare RTI race variable), and we described the average beneficiary age of patients treated (Supplemental Appendix 3).
Study Design and Statistical Analysis
We first conducted descriptive analyses characterizing SNH ownership trends and comparing baseline characteristics between acquired and nonacquired SNHs. We then employed a weighted stacked event study design to estimate the association between acquisition and cancer-related service delivery. Our primary model compares each dependent variable at acquired SNHs to a control group of SNHs that remained independent throughout the study period. Models adjusted for hospital size, urban versus rural location, ownership type, and graduate medical education payment status. We present results using a weighted estimator of the trimmed aggregate average treatment effect on the treated (Wing et al., 2024). This estimator addresses biases common in staggered adoption difference-in-differences designs by producing event-time-specific treatment effects while minimizing bias from compositional changes in treated groups over time. It also applies corrective weights to resolve the inconsistent weighting of treated and control units that can bias estimates in unweighted stacked event study designs. To avoid conflating pre- and postacquisition effects due to variable acquisition timing during the calendar year, we excluded the year of acquisition from the analysis and used the year prior to acquisition (event year t = −1) as the reference year.
We conducted several sensitivity analyses including (a) models using a restricted control group that included only continuously independent hospitals that were later acquired, (b) models without covariate adjustment, and (c) models among SNHs that already offered cancer-related services at baseline to assess whether utilization patterns differed in hospitals with preexisting infrastructure, where additional investment in new service capacity was less likely to be required. To identify control hospitals that were acquired after our study period (i.e., “later-acquired” SNHs), we used publicly available data from the CMS Change of Hospital Ownership database for 2019 through 2024 in combination with a public record search. We assessed the robustness of our findings using a nonstacked event study approach based on the estimator developed by Sun and Abraham, which accounts for potential treatment effect heterogeneity in settings with staggered treatment adoption (Sun & Abraham, 2021). Finally, we stratified results by SNH definition (DSH vs. uncompensated care) to examine heterogeneity in effects and conducted placebo tests using randomly assigned acquisition dates.
All models included hospital and year fixed effects, and standard errors were clustered at the hospital level. We tested for differential pretrends using an omnibus F-test of whether all preacquisition period coefficients jointly equal zero. Two-sided p-values <.05 were considered statistically significant. Analyses were conducted using StataMP (StataCorp, College Station, TX). The study was deemed not human subjects research by the Harvard Longwood Campus Institutional Review Board.
Results
Hospital Characteristics and Acquisitions
Among 226 SNHs, 75 (33.2%) were acquired by a health system during the study period, and 151 (66.8%) were continuously independent (control hospitals) during the study period (Table 1). Among the control SNH group, 58 (38.4%) were acquired after 2015 (only years preceding acquisition were used for these controls). Compared with independent SNHs, acquired SNHs were statistically more likely to be not-for-profit (64.0% vs. 40.4%) and less likely to be publicly owned (21.3% vs. 52.3%). Acquired SNHs were also more likely to be in urban areas (72.0% vs. 41.1%), receive any GME payment (26.7% vs. 6.6%), and have more than 200 beds (34.7% vs. 12.6%) (Table 1). Most SNHs (82.3%) met inclusion criteria based on the uncompensated care cost definition, and 35.0% met the criteria under the DSH index definition. A minority of hospitals (17.3%) met both criteria. There were no statistically significant differences in the composition of SNH types—uncompensated care-only, DSH-only, or both—between acquired and independent SNHs (Table 1).
Acquired and Control Hospital Cohort Characteristics, 2008–2019.
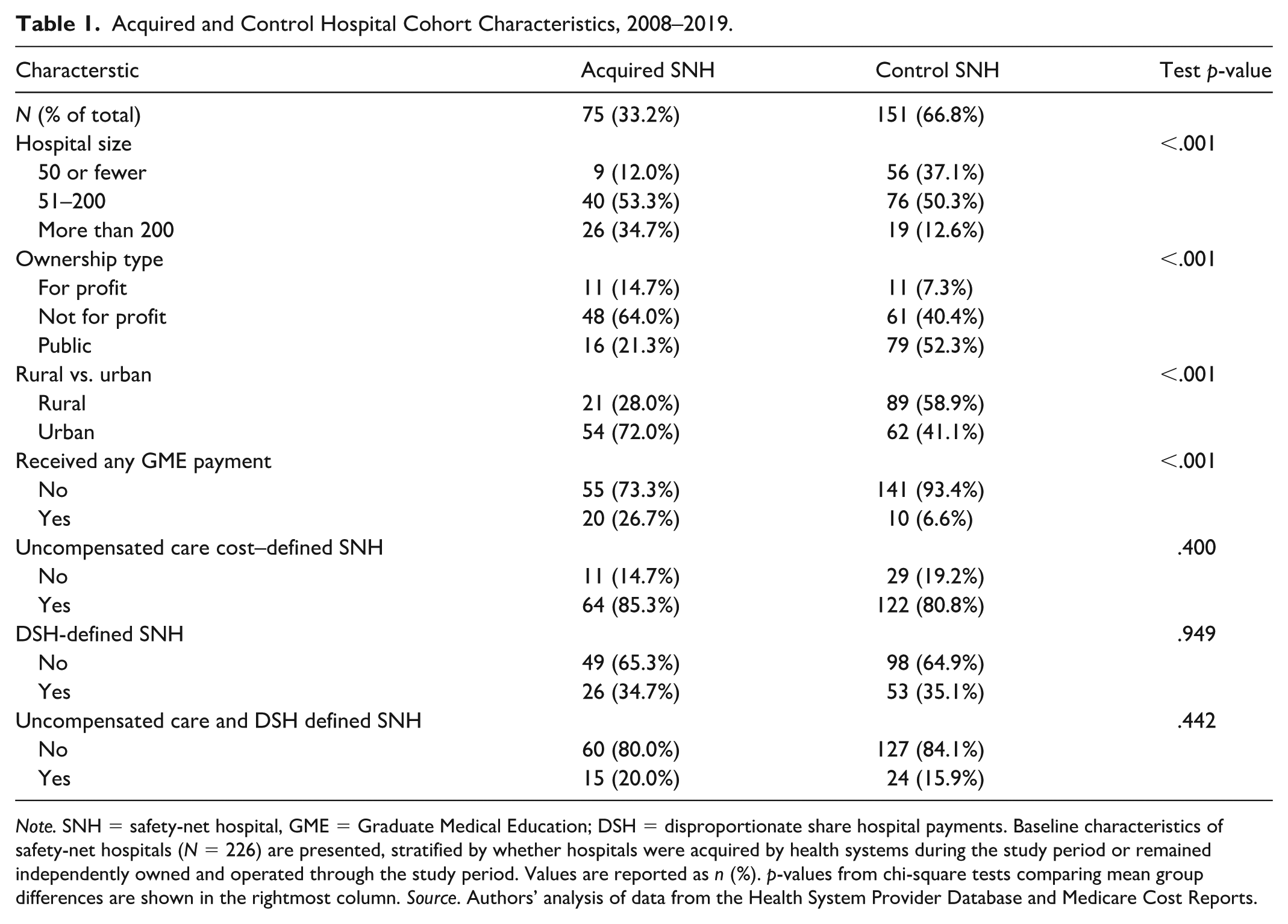
Note. SNH = safety-net hospital, GME = Graduate Medical Education; DSH = disproportionate share hospital payments. Baseline characteristics of safety-net hospitals (N = 226) are presented, stratified by whether hospitals were acquired by health systems during the study period or remained independently owned and operated through the study period. Values are reported as n (%). p-values from chi-square tests comparing mean group differences are shown in the rightmost column. Source. Authors’ analysis of data from the Health System Provider Database and Medicare Cost Reports.
Cancer-Related Service Line Offerings
Acquisition and system integration was not associated with any change in the likelihood of offering individual service lines, including physician-administered chemotherapy services (difference-in-differences estimate = 0.09 pp; 95% CI [−7.1, 7.3]; baseline: 35.6%), radiation oncology treatments (–2.15 pp; 95% CI [–6.56, 2.25]; baseline: 27.3%), advanced PET/CT/MRI imaging services (1.65 pp; 95% CI –[2.81, 6.12]; baseline: 91.1%), or breast and colorectal surgical service lines (–0.01 pp; 95% CI [–6.00, 5.97]; baseline: 33.6%) at acquired SNHs relative to the control group. Event study plots showing adjusted differences by year relative to the year before acquisition are shown in Figure 1. Regression outputs for all main model estimates are presented in Supplemental Table 1; across all models, we did not find evidence of differential pretrends.
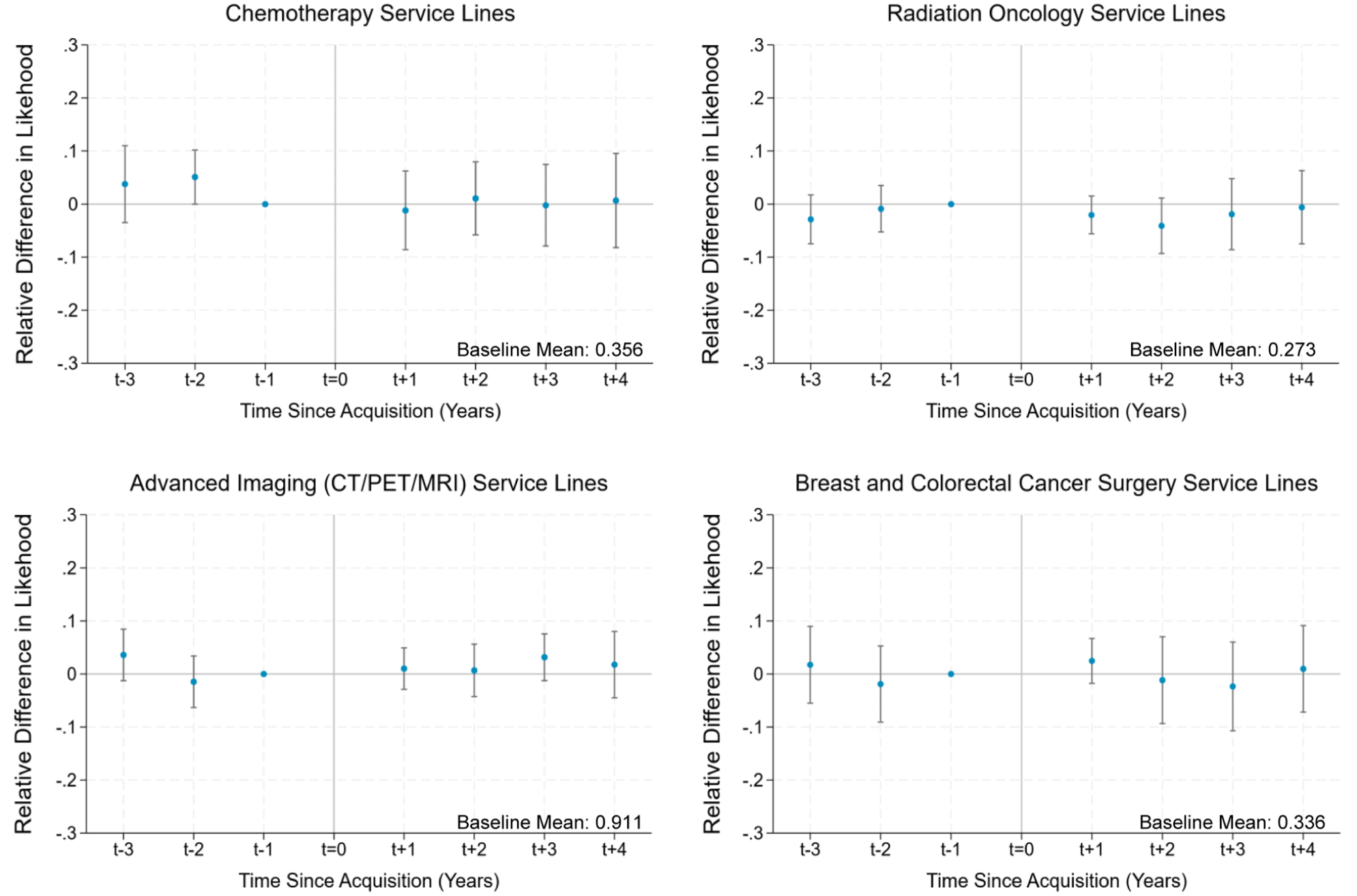
Cancer-related service line offering following safety-net hospital acquisition, 2008–2019.
Cancer-Related Service Volumes
Following integration, acquired SNHs demonstrated an average increase in annual chemotherapy administration volume (99.6 claims; 95% CI [21.9, 177.3]), representing an 84% increase from the baseline mean of 119.4 claims, relative to control hospitals. There was no detectable change in average annual imaging volume (−26.0 claims; 95% CI [−77.8, 25.7]; baseline M: 130.3 claims), radiation oncology volume (47.9 claims; 95% CI [−40.8, 136.6]; baseline: 176.9 claims) or breast and colorectal cancer resection surgery volumes (−0.6 claims; 95% CI [−2.0, 0.8]; baseline: 8.7 claims). Overall average cancer-related service volume increased over time following SNH acquisition (Figure 2), although the average change in the post period was not statistically significant (120.9 claims; 95% CI [−18.2, 260.1]; baseline: 435.4 claims).
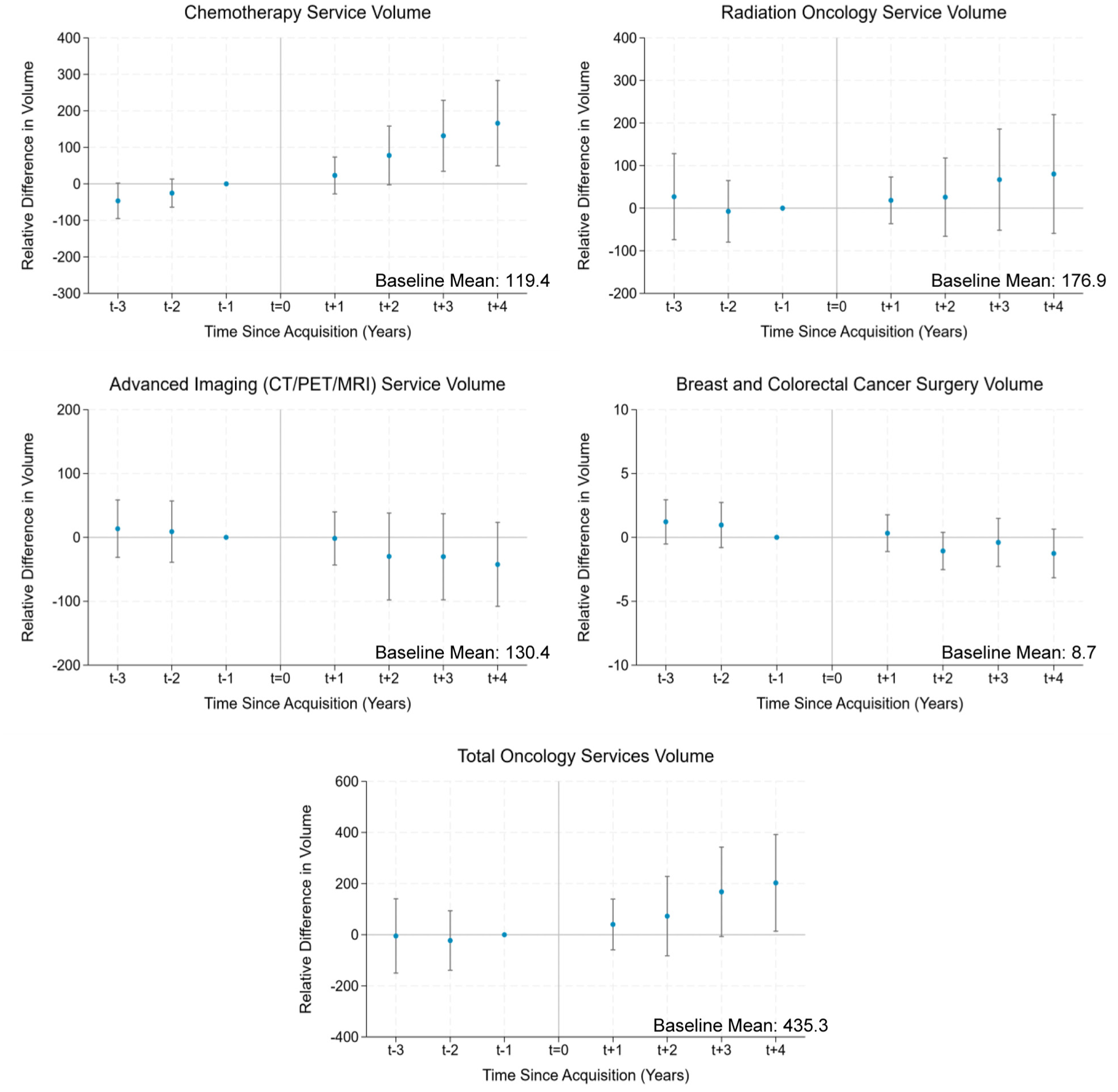
Cancer-related service line volumes following safety-net hospital acquisition, 2008–2019.
Characteristics of Patients with Cancer Treated at SNHs
We found no statistically significant changes in the demographic characteristics of cancer patients served in terms of race and ethnicity, dual eligibility status, and average age, following hospital acquisition. Acquired SNHs demonstrated no change in the percentage of patients identified as Non-Hispanic Black (1.3 pp; 95% CI [–0.6, 3.2]; baseline M: 19.7%), Hispanic (–1.1 pp; 95% CI [–2.4, 0.0]; baseline: 8.4%), or Non-Hispanic White (0.5 pp; 95% CI [–1.8, 2.7]; baseline: 69.3%). There was also no associated difference in the percentage of dual eligible beneficiaries (0.5 pp; 95% CI [–2.1, 3.1]; baseline: 36.2%) or average beneficiary age (–0.0 years; 95% CI [–0.6, 0.5]; baseline M: 73.1 years) compared with control hospitals after acquisition (Figure 3).
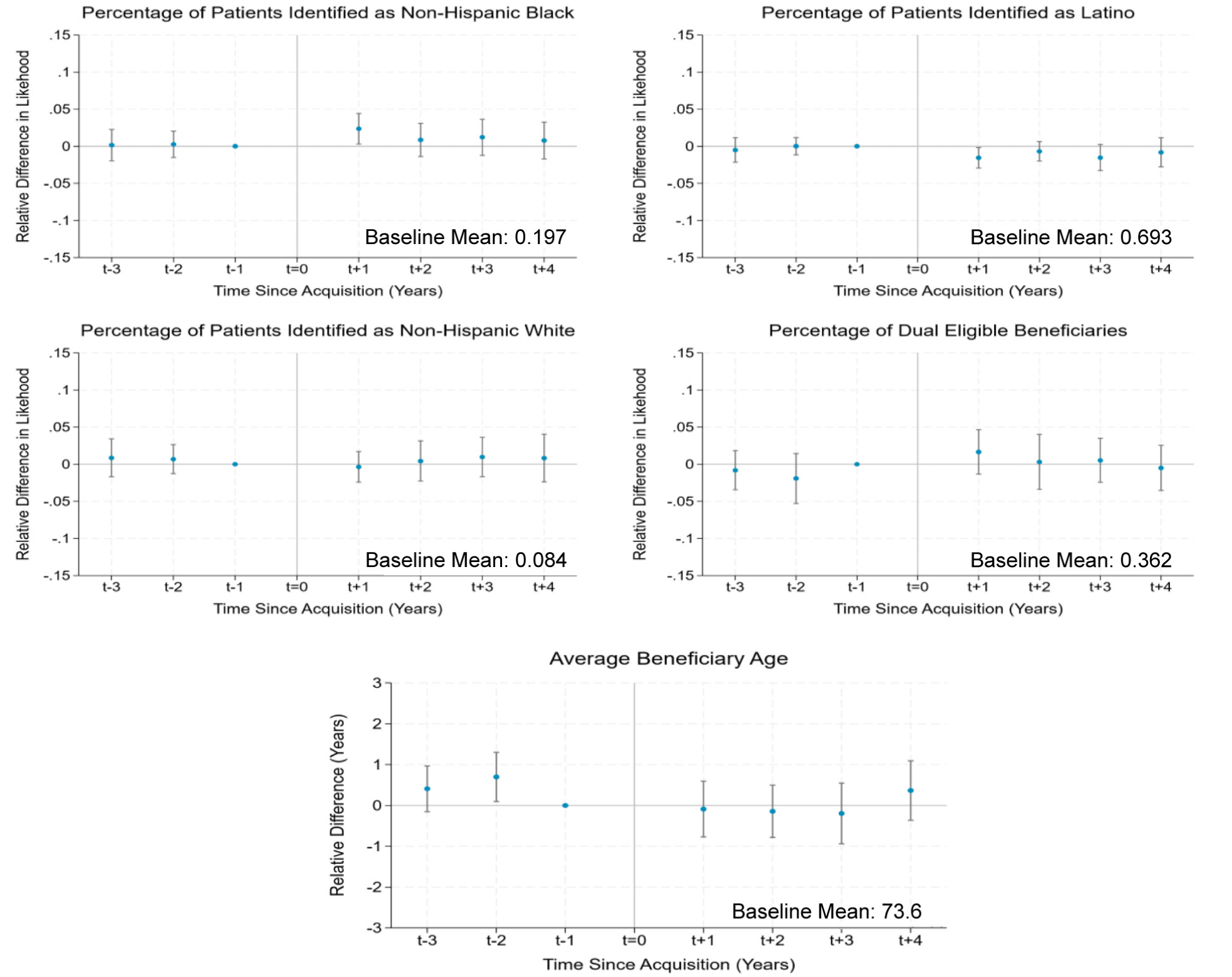
Hospital-level characteristics of fee-for-service Medicare beneficiaries served, 2008–2019.
Secondary Analyses
Sensitivity analyses restricting control hospitals only to only later-acquired hospitals, and models with covariate adjustments yielded similar results to the main findings (Supplemental Figures 1 and 2). Chemotherapy and total service volume changes following acquisition were larger among hospitals that already offered cancer-related services at baseline (Supplemental Figure 3). Findings were also robust to the event study estimation strategy using the event study design developed by Abraham and Sun, which accounts for any possible heterogeneity in treatment effects over time in settings of staggered treatment adoption (Supplemental Figure 4). Heterogeneity analyses did not suggest major differences in effects between hospitals identified by differing SNH definitions (DSH index vs. uncompensated care cost criteria) following acquisition (Supplemental Figure 5). Placebo tests which randomize treatment timing (i.e., year of acquisition) were not statistically significant (Supplemental Figure 6).
Discussion
This study provided new evidence on how acquisitions of SNHs by health care systems were not associated with changes in service line availability but did lead to changes in cancer-related service delivery. Specifically, system integration was associated with increased chemotherapy service volumes, but not with detectable changes in radiation, imaging, or surgical volumes. Moreover, there were no changes in the demographic characteristics of the fee-for-service Medicare population served.
These findings have several potential implications. First, the increase in chemotherapy volume may reflect expanded capacity for delivering certain cancer-related services following acquisition. However, the absence of similar trends for other cancer-related services suggests that system integration may lead to selective expansion—favoring services that are more straightforward to scale and/or more profitable within hospital reimbursement structures (Zaorsky et al., 2021). This shift may have also been favorable for this hospital cohort, as many of these hospitals were 340B-qualifying and therefore likely eligible for drug discounts, allowing them to generate even greater profits from delivering chemotherapy (Conti et al., 2019). This finding is also supported by the larger increases in volumes among hospitals that were already offering these services prior to acquisition. Whether these trends reflect strategic reallocation of resources or broader system-level shifts in care delivery requires further investigation. Second, the stability of service line offerings at acquired hospitals suggests that integration alone may not lead to substantial investment in expanding the availability of specialty oncology services on site, despite systems’ public commitments to preserve and expand access. It is possible that health systems are redistributing service provision across their network, directing patients to other hospitals within the system. If so, this could reflect improved access, but it may also pose new burdens for patients, particularly in terms of travel and continuity. Third, the stability in the characteristics of patients served by SNHs postacquisition suggests that system integration does not appear to substantially displace fee-for-service Medicare patients who were historically served by these SNHs. While this finding may be reassuring, it does not capture potential changes in access among under-65 Medicaid or uninsured populations, for whom concerns about restrictions to care access following acquisition may be greater.
This study has several limitations. First, we relied on Medicare fee-for-service claims, which limits the generalizability of our findings for younger, commercially insured, under-65 Medicaid-enrolled, and uninsured populations. Nevertheless, Medicare is a critical payer for cancer care in the United States, particularly among older adults. Second, while we captured the presence and volume of cancer-related services, we were unable to observe quality of care, or patient-level spending and clinical outcomes. Third, our treatment group required hospitals to be observable within an 8-year transaction window, which excluded hospitals that were acquired and subsequently closed. Fourth, we did not include geographic controls; treatment and control hospitals are in different markets, and service line offerings and volumes likely depend on local demand. Fifth, changes in the characteristics of patients served were assessed at the hospital-year level, which may obscure more granular variation at the individual level. In addition, while we examined service availability at acquired hospitals, we did not track whether patients living near these facilities experienced changes in site of hospital care or outpatient care. Future research examining community-level outcomes will be important for understanding the full impact of SNH acquisitions on access to specialty care. Sixth, SNHs that were never acquired may differ systematically from those that were acquired, a distinction supported by our descriptive comparisons of treatment and control hospitals. To address this concern, we estimated models both with and without covariate adjustment and also assessed for differential pretrends to test the plausibility of the parallel trends assumption and provide evidence that treatment and control hospitals were on similar trajectories prior to acquisition. Across all models, we did not find evidence of differential pretrends (Supplemental Table 1). Although endogeneity of the acquisition decision is a potential concern, it poses limited threat to our findings as SNHs are typically acquired during financial distress rather than because of preexisting operational strengths, and sensitivity analyses among hospitals with preexisting oncology capacity show larger volume increases among acquired hospitals than similarly equipped controls. Our quasi-experimental design included hospital and time fixed effects and adjusted for observable characteristics, though residual confounding from unmeasured time-varying factors may remain. Notably, differential state Medicaid expansion could have affected the attractiveness of SNHs as acquisition targets; however, our sample includes hospitals from both expansion and nonexpansion states in both the acquired and control groups, and the timing of the observed volume increases varies in its relationship to state Medicaid expansion decisions. More broadly, our results were consistent across multiple estimation strategies, sensitivity analyses, and placebo tests for treatment timing. Finally, we may have had limited power to detect changes in certain outcomes due to relatively small service volumes for oncology patients at some SNHs within the 100% Medicare fee-for-service data.
Our findings contribute to the growing literature on health care consolidation by focusing on changes in cancer-related services provision in safety net settings, where there has been less empirical investigation to date. To our knowledge, this was the first analysis to use health care claims data to understand service availability and volumes rather than survey responses about service line provision. Nevertheless, our analysis assessed delivery at the hospital level and did not capture patient outcomes or network-wide shifts in care delivery. Future research should examine whether observed changes in service volume translate into differences in care quality or clinical outcomes. Investigating how integration influences access to oncology care across a system—including outpatient networks, referral pathways, and patient travel time and continuity—would also be important. Future work should also examine the relationship between service provision at acquired hospitals and co-located oncology physician groups, and whether concurrent physician group acquisition may be a mechanism driving the observed chemotherapy volume increases. Finally, deeper examination of the financial and operational drivers of selective service expansion (including how acquisition may affect the cost or intensity of oncology services delivered) could inform more equitable reimbursement models to support the mission of SNHs within consolidated systems.
Conclusion
We investigated how SNH acquisitions by large health care systems affect cancer-related service delivery. We found that that acquisitions may selectively influence certain oncology services, such as volume of chemotherapy delivered, without fundamentally altering the fee-for-service Medicare patient populations served. Our study contributes to a broader understanding of how consolidation shapes service line dynamics within the safety net. Further work is needed to assess whether these changes translate into improved care quality and equitable access for structurally marginalized populations.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587261453480 – Supplemental material for Changes in Oncology Care Provision Following Safety-Net Hospital Acquisition by Health Systems
Supplemental material, sj-docx-1-mcr-10.1177_10775587261453480 for Changes in Oncology Care Provision Following Safety-Net Hospital Acquisition by Health Systems by Rebecca A. Bromley-Dulfano, Nancy D. Beaulieu, Mary Beth Landrum and Nancy L. Keating in Medical Care Research and Review
Footnotes
Acknowledgements
The authors thank Robert Wolf, Lauren Riedel, and Jen Cabrera Rodriguez for their technical support; and to Paula Chatterjee for the valuable discussion and feedback on an earlier version of the paper.
Ethical Approval and Informed Consent Statements
The study was deemed not human subjects research by the Harvard Longwood Campus Institutional Review Board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIH and AHRQ. This project was supported by grants R01CA255035 from the National Cancer Institute (NCI), U19HS024072 from the Agency for Healthcare Research and Quality, and T32HS000055 (Ms. Bromley-Dulfano) from the Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services. This work does not necessarily reflect the views of the funders. Ethical approval and informed consent statements.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: None of the authors has any affiliation or financial involvement that conflicts with the material presented in this report. The authors report additional funding from the National Institutes of Health, Arnold Ventures, and the Commonwealth Fund not related to the current work.
Data Availability Statement
The data are confidential administrative claims data and as such cannot be made available
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.