
Abstract
Emerging adults demonstrate the highest rates of deliberate self-harm (DSH) and thus represent a population in need of further study. While child maltreatment (CM) history is a risk factor for DSH, the mechanisms behind this relationship are not fully understood. This study tested a model of mechanisms linking CM with DSH (likelihood of engaging in the behavior and frequency among those who self-harm) via negative urgency (tendency to engage in impulsive behaviors under conditions of negative affect), distress tolerance, sense of control, and desire for control in a sample of college students. As hypothesized, CM had a strong positive direct association with both the likelihood and frequency of DSH. CM was positively associated with negative urgency and inversely associated with distress tolerance and sense of control. Negative urgency was positively associated with DSH likelihood and frequency. Distress tolerance was not directly associated with DSH but was indirectly associated with DSH likelihood and frequency via negative urgency. Sense of control was not associated with the likelihood of engaging in DSH; however, among those who endorsed a history of DSH, sense of control was positively associated with DSH frequency. Desire for control was not associated with either CM or DSH.
Emerging adulthood can be an exciting time filled with new opportunities and challenges, but for some, this developmental period is marked by increased risk of engaging in potentially harmful behaviors. One such risky behavior is deliberate self-harm (DSH), which refers to the deliberate, direct destruction or alteration of body tissue without conscious suicidal intent, but resulting in injury severe enough for tissue damage to occur (Gratz, 2001). DSH (also referred to as nonsuicidal self-injury) is a relatively common behavior, with a recent population-based epidemiologic research study on U.S. adults finding lifetime prevalence rates of 5.9% (Klonsky, 2011). Rates among emerging adults have typically been higher with studies finding 12% to 38% of college students endorsing at least one lifetime act of DSH (Borrill, Fox, Flynn, & Roger, 2009; Brown, Williams, & Collins, 2007; Gratz & Roemer, 2008; Whitlock, Eckenrode, & Silverman, 2006). Following a review of prevalence rates among existing studies, Rodham and Hawton (2009) reported that young adults between ages 18 and 25 are at highest risk of engaging in DSH, thus signifying additional research targeting this at-risk population is needed.
Many studies have found positive associations between the various forms of child maltreatment (CM; including sexual abuse, physical abuse, emotional abuse, and neglect) and DSH (Boudewyn & Liem, 1995; Briere & Gil, 1998; Gratz, 2006; Gratz & Chapman, 2007; Rodriguez-Srednicki, 2001; Sansone, Sinclair, & Wiederman, 2009; Zoroglu et al., 2003). Although it is established that CM history increases risk of numerous risky behaviors, including DSH, further research identifying mechanisms linking CM and DSH is needed. Individuals who engage in DSH often do so years after their maltreatment experiences; thus, CM appears to affect the development of individual characteristics that are more proximal risk factors for DSH. Identification of these factors can assist in the development of prevention and treatment strategies.
Recent research has shown that a specific type of impulsivity, negative urgency, mediates the relationship between CM and DSH (Arens, Gaher, & Simons, 2012). Negative urgency refers to the tendency to engage in impulsive behaviors under conditions of negative affect despite possible harmful long-term consequences (Whiteside & Lynam, 2001), and it has been shown to be related to various maladaptive behaviors, including DSH (Ogle & Clements, 2008), substance use (Anestis, Selby, & Joiner, 2007), and disordered eating (Anestis et al., 2009). However, the relationship between CM and DSH is likely more complex with additional individual characteristics contributing to this relationship.
A separate but related construct to negative urgency, distress tolerance, appears to play a role in the relationship between CM and DSH. For instance, Linehan’s (1993) biosocial model suggests that invalidating environments during childhood fail to teach children how to tolerate emotional distress, and invalidating environments during childhood predict poor distress tolerance in adults (Mountford, Corstorphine, Tomlinson, & Waller, 2007). Individuals with low distress tolerance perceive distress as unbearable, as they believe they are unable to handle being upset. Consequently, the emotional regulation of those with low distress tolerance is characterized by great efforts to avoid the overwhelming negative emotions (Simons & Gaher, 2005), and distress tolerance has been shown to be inversely associated with negative urgency (Gaher, Hofman, Simons, & Hunsaker, 2013; Wray, Simons, Dvorak, & Gaher, 2012). Moreover, the affect regulation model of DSH asserts that DSH is a way of escaping from the experience of intense distress for those with limited ability to tolerate such emotions (Nock & Mendes, 2008; Suyemoto, 1998), and poor distress tolerance has been found to be an important explanatory factor in the development and maintenance of DSH (Chapman, Gratz, & Brown, 2006; Klonsky, 2007; Nock & Mendes, 2008; Slee, Garnefski, Spinhoven, & Arensman, 2008). Although extant studies emphasize the role of distress tolerance in DSH, no known studies have examined a single model incorporating CM, distress tolerance, negative urgency, and DSH.
Sense of control (one’s view of having control as well as belief in ability to gain control; Shapiro, Potkin, Jin, & Brown, 1993) and desire for control are two additional variables that may play a role in the relationship between CM and DSH. Theoretical and preliminary evidence suggests that low sense of control and high desire for control may result from CM, and individuals who are maltreated as children place important value on control as adults (Cole, Woolger, Power, & Smith, 1992; Finkelhor & Browne, 1985; Lehavot, Walters, & Simoni, 2009; Perkins & Allen, 2006). Thus far, limited research has been conducted to test this theory. In one study, female adult survivors of incest reported less sense of control over their feelings related to parenting as compared to those without histories of incest (Cole et al., 1992). Within mothers enrolled in a community-based home visitation program, lifetime history of violent trauma (including childhood physical and sexual abuse) was related to decreased sense of control over current and future circumstances (Stevens, Ammerman, Putnam, & Van Ginkel, 2002).
Those raised in chaotic and unpredictable environments may come to believe they do not have control over their environments. For instance, Finkelhor and Browne (1985) discussed how the dynamic of powerlessness that is often associated with sexual abuse distorts children’s sense of their ability to control their lives, and they theorized that some abuse survivors may acquire dysfunctional needs to control as a way to compensate for their sense of powerlessness. If this theory is supported, victims of CM may engage in maladaptive behaviors, such as DSH, in an effort to gain a sense of control over some aspect of their lives. Indeed, low sense of control and high desire for control has been hypothesized to increase risk of DSH (Aizenman & Jensen, 2007; Briere & Gil, 1998; Haines & Williams, 1997).
Although independent associations have been found between CM and issues of control and between issues of control and DSH, no known studies to date have examined the mediating role of sense of control and desire for control in the relationship between CM and DSH. It is likely that low sense of control and high desire for control are consequences of an aversive childhood environment, and DSH may provide an individual with a sense of control over negative emotions as well as physical evidence of control over one’s body. Independent associations have been found among the constructs of CM, distress tolerance, sense of control, desire for control, and DSH, but these constructs have not been investigated in a comprehensive model.
Through the use of structural equation modeling, this study examines the relationships between CM, distress tolerance, negative urgency, sense of control, desire for control, and DSH. We expected that CM would be positively and directly associated with the likelihood of DSH engagement and frequency of DSH among those young adults who engaged in the behavior. We also hypothesized that CM would be positively associated with negative urgency and desire for control and inversely associated with distress tolerance and sense of control. Moreover, we hypothesized negative associations between distress tolerance and DSH (likelihood and frequency) and between sense of control and DSH (likelihood and frequency), as well as positive associations between negative urgency and DSH (likelihood and frequency) and desire for control and DSH (likelihood and frequency). Finally, we presumed there would be significant indirect associations between CM and DSH (likelihood and frequency) via negative urgency, distress tolerance, sense of control, and desire for control.
Method
Participants
The initial sample included 641 undergraduate college students attending a mid-size Midwest state university. Age ranged from 18 to 25 (M = 19.68, SD = 1.59). Consistent with the overall student population distribution, the sample had a higher percentage of women (73%). With regard to the self-identified racial background of participants, 91.9% were Euro-American/White, 2.5% were African American/Black, 1.4% were Native American/Alaska Native, 1.4% were Asian, 1.9% Multiracial, and 1.0% were other or did not wish to respond. In addition, 1.6% identified as Hispanic or Latino. The range of years of school completed was 12 to 18 (M = 13.30, SD = 1.46).
Measures
DSH
The Deliberate Self-Harm Inventory (DSHI; Gratz, 2001) is a 17-item, behaviorally based, self-report questionnaire used to assess self-harming behaviors. This measure assesses onset, frequency, severity, duration, and type of self-harming behavior via 17 questions (e.g., Have you ever intentionally cut your wrist, arms, or other area(s) of your body?), each followed by five follow-up questions (e.g., How old were you when you first did this? How many times have you done this?). Responses for Item 17 (Have you ever intentionally done anything else to hurt yourself that was not asked about in this questionnaire?) were independently examined by two raters to determine whether it met the definition of DSH (κ = 0.89, p < .001). In the current sample, the DSHI was found to have adequate internal consistency of the dichotomous DSHI items (α = .69). For negative binomial hurdle (NBH) model analysis, total frequency was calculated by summing the frequency of acts for each item (Gratz, 2001).
CM
The Child Abuse and Trauma Scale (CATS; Sanders & Becker-Lausen, 1995) consists of 38 items (e.g., Did you feel safe living at home? Did your parents ever hit or beat you when you did not expect it?) rated on a 5-point scale ranging from never (0) to always (4). The measure was designed to provide a quantitative index of the frequency and extent of various types of maltreatment in childhood and adolescence. Five of the items are reverse scored. Internal consistency in the current sample was good for the total score (α = .90). Internal consistency for the subscales of negative home environment/neglect (α = .91), punishment (α = .59), and sexual abuse (α = .82) was comparable to properties previously examined in a college population (Sanders & Becker-Lausen, 1995). In this study, subscale scores were used as indicators for the CM latent variable.
Sense of control and desire for control
The Shapiro Control Inventory (Shapiro, 1992) includes 187 items. The domains of sense of control and desire for control were used in this study. For these domains, participants rate the extent to which statements apply to them on a 7-point Likert-type scale ranging from never (1) to always (7). Positive sense of control consists of 11 items measuring perceived self-efficacy, ability to set meaningful goals, skills to carry out the goals, and appropriate level of self-control. Negative sense of control consists of 5 items measuring loss of control, lack of control, and control from others. Internal consistency in the current sample was good for positive sense of control (α = .93), negative sense of control (α = .80), and overall sense of control (α = .92). The domains of positive and negative sense of control were used as indicators for the latent variable overall sense of control. The desire for control scale contains 11 items including desire to control self, desire to control others, the importance of the appearance of being in control, and the fear of losing control. It had an internal consistency of α = .76. For this study, item parcels were formed for desire for control using the item-to-construct method (Little, Cunningham, Shahar, & Widaman, 2002). The item parcels were then used as indicators for the desire for control latent variable.
Distress tolerance
The Distress Tolerance Scale (DTS; Simons & Gaher, 2005) is a 15-item self-report measure in which participants indicate the extent to which they can experience and withstand distressing psychological states on a 5-point scale ranging from strongly agree (1) to strongly disagree (5). The DTS encompasses four types of emotional distress items, including perceived ability to tolerate emotional distress, subjective appraisal of distress, attention being absorbed by negative emotions, and regulation efforts to alleviate distress. Higher scores indicate greater levels of distress tolerance. The DTS has demonstrated appropriate convergence with other self-report ratings of affective distress and regulation (Simons & Gaher, 2005). Internal consistency in the current sample was adequate for the total score (α = .88) and subscales of tolerance (α = .76), absorption (α = .80), appraisal (α = .82), and regulation (α = .70). For this study, subscale scores were used as indicators for the latent variable distress tolerance.
Negative urgency
The UPPS Impulsive Behavior Scale (Whiteside & Lynam, 2001) is a 45-item inventory created to measure four distinct personality pathways to impulsive behavior, including negative urgency, premeditation (lack of), perseverance (lack of), and sensation seeking. Each subscale uses a rating scale ranging from not true of me (1) to very true of me (5). The current analysis focused on negative urgency, which specifically addresses the role of negative emotion in impulsive behaviors. The urgency subscale consists of 12 items (e.g., When I feel bad, I will often do things I later regret in order to make myself feel better now; When I am upset I often act without thinking). Internal consistency in the current sample was high (α = .88). Item parcels for urgency were formed using the item-to-construct method (Littleet al., 2002) and were used as indicators for the negative urgency latent variable.
Procedure
Following approval from the institutional review board, recruitment was conducted via announcements through the university’s online research recruitment program. Participants were informed that their responses were completely confidential, anonymous, and voluntary. Participants completed questionnaires online and received course credit as compensation for their time.
Data Preparation and Analysis Overview
Preliminary analyses were conducted using Statistical Package for the Social Sciences 19. The hypothesized structural equation model was estimated using Mplus Version 6.1 (Muthén & Muthén, 2010). Based on the recommendations of Kline (2011), preliminary analyses evaluated assumptions of structural equation modeling, including the absence of multicollinearity and singularity, multivariate normal distribution, and linear relationships. Identified outliers within CM subtypes, positive sense of control, negative sense of control, the three desire for control parcels, and DSH frequency were reduced in value to one unit greater (or lesser) than the nearest nonoutlying value (Tabachnik & Fidell, 2001). Univariate normality among all observed variables, with the exception of DSH, was assessed using histograms with normal curves and z-scores. Skewness for all variables except sexual abuse was found to be within acceptable ranges. Given that maximum likelihood estimation (MLR) is robust to nonnormality (Kline, 2011), and only one variable (sexual abuse) was found to have a nonnormal distribution (i.e., positively skewed), no transformations were performed. No problems related to multicollinearity or singularity were identified.
Given the high positive skew of DSH and excess zeros (i.e., no history of DSH), traditional methods of analysis are untenable. Previous research has indicated overdispersed count distributions that allow for the modeling of excess zeros are appropriate for this type of data (Bethell, Rhodes, Bondy, Lou, & Guttmann, 2010). Thus, we examined both a zero-inflated negative binomial (ZINB) model and a NBH model as appropriate distributions for modeling the current data. For this study, a NBH model was selected. The model was estimated using full-information MLR with robust standard errors. Data were assumed to be missing at random, but not completely at random (Enders & Bandalos, 2001). To better control the temporal ordering of constructs assessed cross-sectionally, data from individuals with last incident of self-harm greater than five years (n = 40) were removed from the analytic sample prior to further analyses.
Results
Descriptive and Bivariate Statistics
With regard to DSH prevalence, 32% of participants (n = 203) endorsed at least one incident of DSH in their lifetime. Nine percent of participants (n = 59) deliberately harmed themselves 10 or more times. Of those endorsing DSH history, the mean number of incidents was 26.50 (SD = 115.21, Mdn = 4, Skew = 8.77). Seventy-eight percent of participants endorsed harming within the past 5 years (M = 3.19 years since last incident, SD = 3.10). Among self-harming participants, the most frequently endorsed methods were skin cutting (44%), severe scratching (31%), sticking self with sharp objects (20%), and carving words into skin (17%). Men (39%) were more likely than women (29%) to endorse a history of DSH, χ 2 (1) = 5.98, p = .014. However, among those who endorsed a history of DSH, women reported higher DSH frequency, χ 2 (1) = 4.78, p = .029. Bivariate correlations are presented in Table 1. All hypothesized relationships were significant, except for desire for control, which was not significantly associated with CM or DSH and thus excluded from the analysis.
Correlation Matrix.
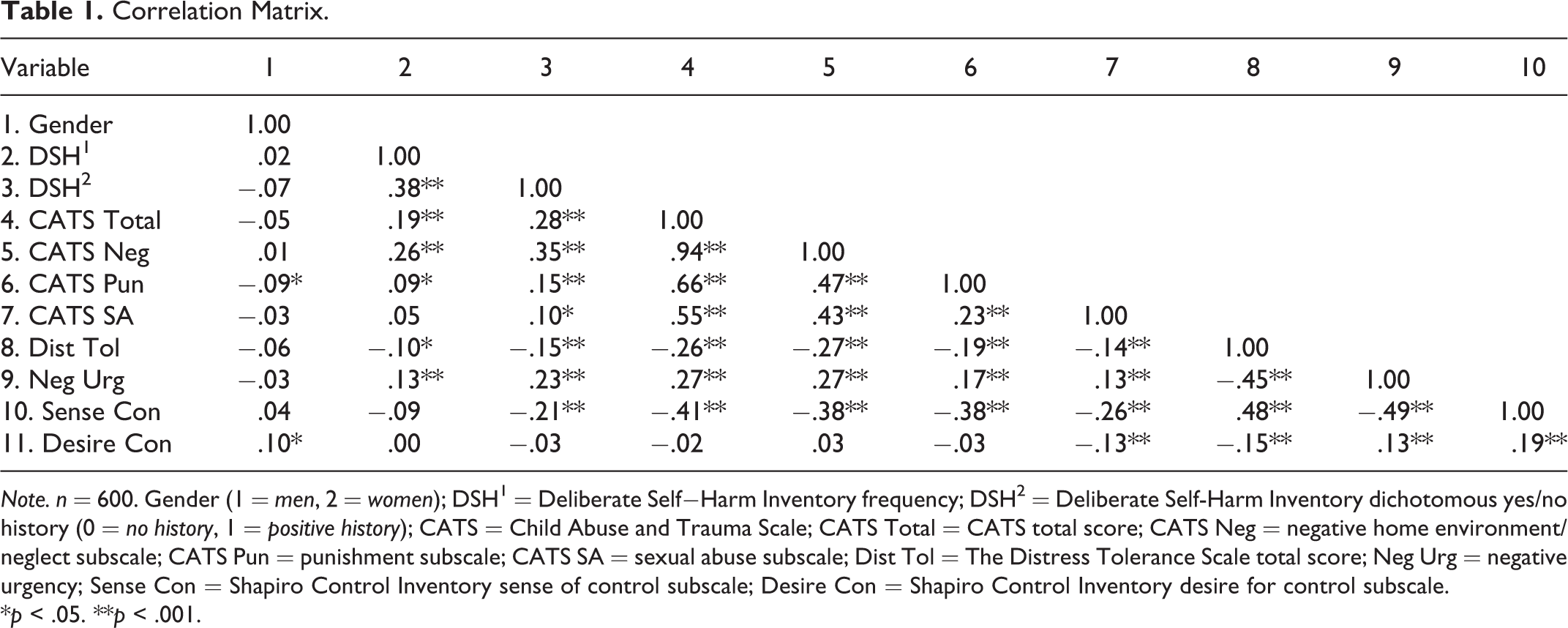
Note. n = 600. Gender (1 = men, 2 = women); DSH 1 = Deliberate Self−Harm Inventory frequency; DSH 2 = Deliberate Self-Harm Inventory dichotomous yes/no history (0 = no history, 1 = positive history); CATS = Child Abuse and Trauma Scale; CATS Total = CATS total score; CATS Neg = negative home environment/neglect subscale; CATS Pun = punishment subscale; CATS SA = sexual abuse subscale; Dist Tol = The Distress Tolerance Scale total score; Neg Urg = negative urgency; Sense Con = Shapiro Control Inventory sense of control subscale; Desire Con = Shapiro Control Inventory desire for control subscale.
*p < .05. **p < .001.
Measurement Model
The current analysis first evaluated the measurement model’s fit according to guidelines proposed by Hu and Bentler (1999). For fit indices, a cutoff value of .95 is considered acceptable for the comparative fit index (CFI) and Tucker–Lewis index (TLI), a cutoff value close to .06 for the root mean square error of approximation (RMSEA; with 90% confidence intervals [CIs] [0, .10]) is acceptable, and a cutoff value of the standardized root mean square residual (SRMR)
Model Selection
After identifying the measurement model, we tested two distributional outcomes associated with overdispersed counts and excess zeros: zero-inflated negative binomial (ZINB) and negative binomial hurdle (NBH). A ZINB model allows for the modeling of two processes. First, it estimates a two-class latent variable, with the assumption that zeros are generated via two distinct processes (“always zero” vs. “sometimes zero”). The likelihood of a zero outcome via one of these processes is then tested. Second, it models a negative binomial distribution among non-zero observations (Muthén & Muthén, 1998–2010). An NBH model has the advantage of relying on the observed data, rather than an unobserved latent process of zero generation. The hurdle model estimates a conditional logistic outcome for the likelihood of engaging in self-harm, as well as a zero-truncated negative binomial outcome for the non-zero observations (Muthén & Muthén, 1998-2010). Previous research has suggested that the NBH performs better than other count models with self-harm data (Bethell et al., 2010). For our data, the NBH model (Akaike Information Criterion [AIC] = 13,915.42, Bayesian Information Criterion [BIC] = 14174.85, sample-size adjusted BIC [SSBIC] = 13,987.53) showed a better fit to the data than a ZINB model (AIC = 13,937.16, BIC = 14,196.58, SSBIC = 14,009.27). In addition, a Vuong test of model log likelihoods supported the NBH model over the ZINB model, V = 2.28, p = .023. Thus, the NBH model was selected. This two-part model allows for the simultaneous modeling of both the likelihood of engaging in any self-injurious acts (self-harmers vs. non self-harmers) via a logistic function, as well as the frequency of engaging in self-injurious acts (among those who clear the hurdle) via a truncated negative binomial count distribution.
Negative Binomial Hurdle Model
For the NBH model, CM and gender served as exogenous variables. Effects from CM to DSH were expected to be indirect through negative urgency, distress tolerance, and sense of control. Direct paths were specified between CM to negative urgency, distress tolerance, and sense of control. A direct path from distress tolerance to negative urgency was specified. In turn, direct paths were specified from negative urgency, distress tolerance, and sense of control to DSH (count and hurdle). Gender was a covariate for all variables. Sense of control was allowed to covary with negative urgency and distress tolerance. Traditional statistics to assess model fit, such as RMSEA and CFI, are not available for this type of model; however, the AIC (13,915.42) and BIC (14,174.84) are provided.
In the final model (see Figure 1), CM was positively associated with negative urgency and was inversely associated with distress tolerance and sense of control. Negative urgency was positively associated with both the likelihood of engaging in DSH and the frequency of DSH among those who endorsed a history of DSH. As hypothesized, we found significant indirect effects of CM on the count portions of DSH via negative urgency while indirect effects of CM on the hurdle portion of DSH via negative urgency approached significance. Directionally, distress tolerance was inversely associated with both the likelihood and frequency of DSH, but these associations did not reach statistical significance. While specific indirect effects of CM on DSH via distress tolerance were not significant, the effects of CM on both the count and hurdle portions of DSH were indirect through distress tolerance when negative urgency mediated the relationship between distress tolerance and DSH. Contrary to hypothesis, sense of control was not associated with the likelihood of engaging in DSH but was positively associated with frequency among those who endorsed DSH history. Moreover, the indirect effect of CM on the count portion of DSH via sense of control was significant. Specific indirect effects are listed in Table 2. The total indirect effect between CM and the likelihood of DSH was nonsignificant. However, CM had a strong positive direct association with both the likelihood and frequency of DSH, resulting in a positive total effect between CM and DSH likelihood. The total indirect effect between CM and DSH frequency among those who endorsed a history of DSH was negative, possibly due to the robust inverse association between CM and sense of control. Moreover, two or more indirect effects of opposing directions may cancel each other out, potentially leading to a nonsignificant total indirect effect despite the presence of significant specific indirect effects (Hayes, 2009). Consistent with the likelihood model, however, the total effect (direct and indirect) between CM and frequency of DSH was positive and statistically significant. Thus, CM is robustly associated with the likelihood and frequency of DSH.
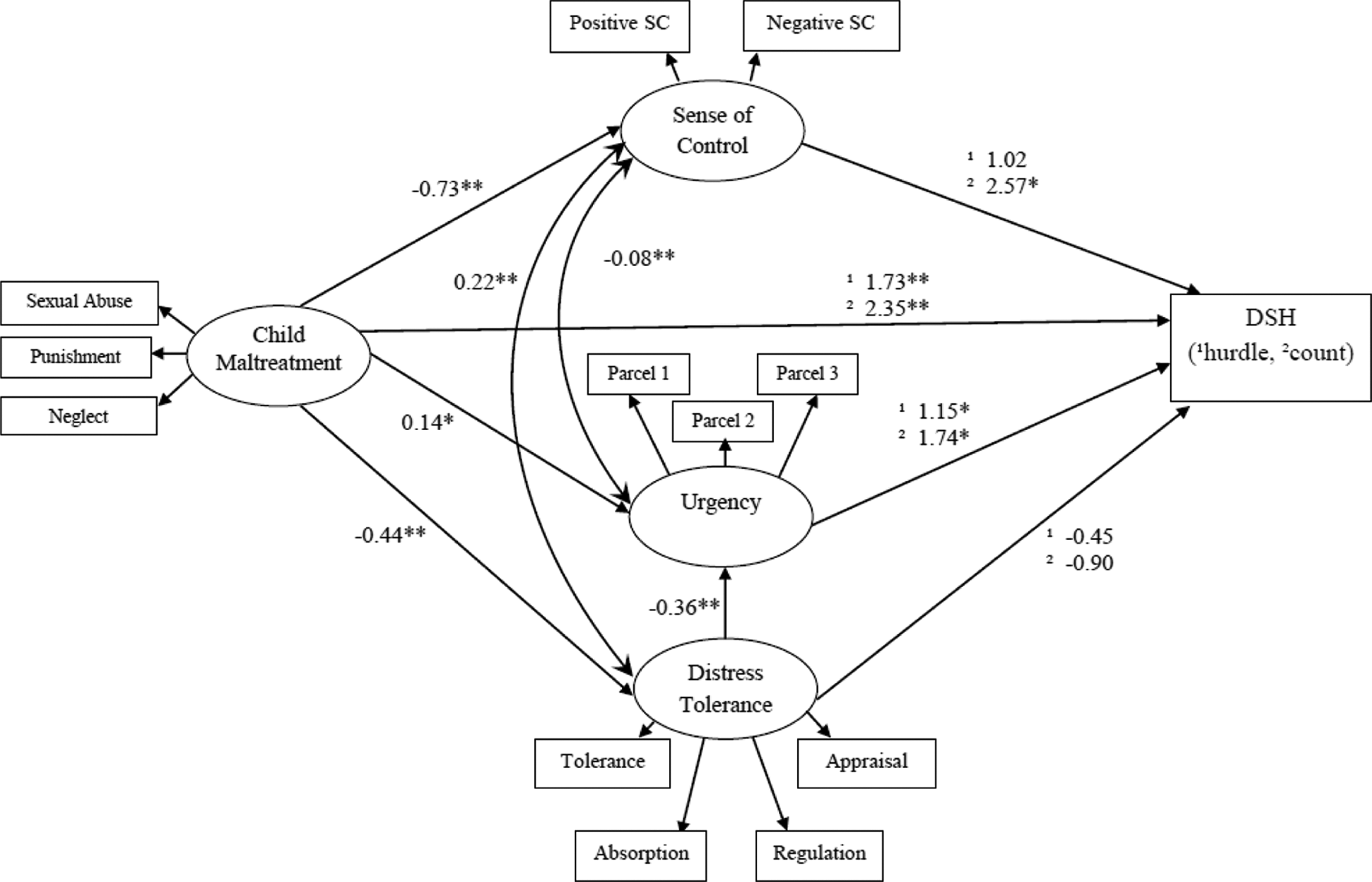
Final structural model with unstandardized path coefficients. All coefficients presented are linear estimates (i.e., not rates), so that indirect effects in Table 2 are interpretable. Coefficient above (superscript 1) is likelihood of any DSH among full sample. Coefficient below (superscript 2) is frequency of DSH among those who report self-harm. Gender is included in the statistical model as a covariate but not included in the figure for visual clarity. DSH = deliberate self-harm. *p < .05. **p < .001.
Direct and Indirect Effects From Childhood Maltreatment to Deliberate Self-Harm.
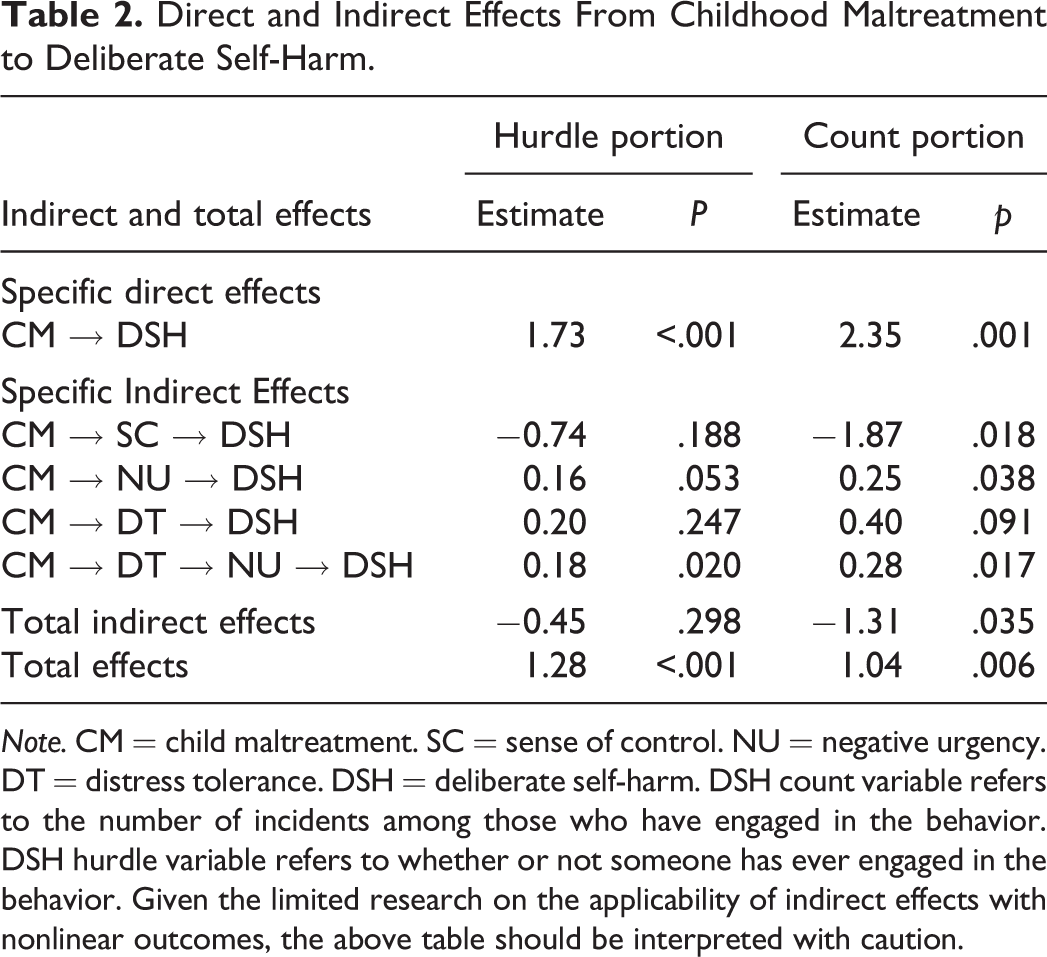
Note. CM = child maltreatment. SC = sense of control. NU = negative urgency. DT = distress tolerance. DSH = deliberate self-harm. DSH count variable refers to the number of incidents among those who have engaged in the behavior. DSH hurdle variable refers to whether or not someone has ever engaged in the behavior. Given the limited research on the applicability of indirect effects with nonlinear outcomes, the above table should be interpreted with caution.
Discussion
The purpose of this study was to examine potential mechanisms by which CM relates to DSH by testing a structural equation model incorporating the hypothesized explanatory variables of distress tolerance, negative urgency, sense of control, and desire for control. The overall model fit the data well; however, not all hypothesized paths were found to be significant. We discuss the findings in turn, beginning with general findings related to DSH and then transitioning to the NBH model.
DSH
Consistent with previous studies of undergraduate students, 32% of participants endorsed at least one lifetime incident of DSH. While 9% of participants endorsed deliberately harming themselves 10 or more times, previous studies using the DSHI have found frequency rates of 10 or greater to range from 14% to 18% (Gratz, 2001, 2006; Gratz & Chapman, 2007; Gratz, Conrad, & Roemer, 2002). The finding that men were more likely to endorse at least one incident of DSH was surprising considering previous studies have found either higher rates among women (Boudewyn & Liem, 1995) or no gender difference (Briere & Gil, 1998; Brown et al., 2007; Gratz et al., 2002). However, among those who endorsed a history of DSH, women endorsed higher frequencies, suggesting they are more likely to engage in repetitive self-harm.
Structural Equation Model
The structural equation model provides a framework for an integrated conceptualization of the mechanisms by which CM is associated with DSH. Because the negative binomial hurdle model for DSH separates the decision to engage or not engage in DSH from the frequency of those who have engaged in at least one instance of the behavior, paths were tested for both the count and the hurdle portions of the model. As hypothesized, CM was directly associated with DSH (decision to engage in the behavior as well as frequency of those who harm). In addition, CM was indirectly related to DSH likelihood and frequency via distress tolerance and negative urgency. Results suggest negative urgency accounts, at least partially, for the association between CM and whether one decides to engage in DSH, as well as the association between CM and repeat incidents of DSH. The significant role of negative urgency in both the count and hurdle portions of the model indicates the tendency to act impulsively under conditions of negative affect plays a role in the decision to engage in DSH as well as recurrent DSH for those who engage in at least one incident. Contrary to hypothesis, no direct relationship was found between poor distress tolerance and DSH likelihood or frequency; however, distress tolerance was associated with negative urgency, which was then related to DSH likelihood and frequency. According to the theoretical model, CM directly increases risk of poor distress tolerance and negative urgency. In addition, poor tolerance for distress increases risk of acting impulsively under conditions of negative affect, which in turn increases risk of DSH. These results are consistent with prior studies demonstrating individuals with histories of CM or harsh discipline practices are more likely to be impulsive than individuals without histories of CM (Brodsky et al., 2001; Corstorphine, Waller, Lawson, & Ganis, 2007; Straus & Mouradian, 1998). Results are also concordant with theories within the biosocial (Linehan, 1993), emotional dysregulation (Gratz & Roemer, 2008; Yates, 2009), and psychological (Nock & Cha, 2009) models of DSH in which individuals are more likely to engage in recurrent DSH, given the propensity to react impulsively under conditions of intense negative affect.
One plausible explanation for the relationship between CM, distress tolerance, and negative urgency is that parents who use harsh discipline practices may communicate that negative affect is intolerable, and it is acceptable and appropriate to react impulsively. For instance, prior research has shown that physical punishment carried out impulsively by the parents is related to impulsiveness in the child (Straus & Mouradian, 1998). Moreover, CM can affect cortisol regulation and hypothalamic–pituitary–adrenal axis functioning (Cicchetti & Rogosch, 2001a, 2001b; De Bellis et al., 1999; Hart, Gunnar, & Cicchetti, 1995; Kaufman, 1991), which are important components of emotion regulation (Maughan & Cicchetti, 2002). As such, individuals whose biological systems have been altered by CM may be less likely to tolerate distress and more prone to engage in self-destructive behaviors in an effort to reduce negative affect. Conversely, some individuals may have a genetic predisposition to poor distress tolerance and negative urgency. (Beauchaine & Neuhaus, 2008; Paaver, Kurrikoff, Nordquist, Oreland, & Harro, 2008), which may then increase problematic behavior engagement (Eisenberg et al., 2009). In turn, parents of impulsive children may experience greater stress and frustration (Baker, 1994) and resort to using harsh discipline tactics in an effort to control their children (Crouch & Behl, 2001).
As hypothesized, CM history was associated with poor sense of control. Sense of control was hypothesized to be related to both DSH outcomes; however, results were somewhat inconsistent. At the bivariate level, sense of control was associated with a history of DSH but was not significantly associated with the frequency of DSH. Conversely, in the NBH model, sense of control was not associated with DSH history but was significantly positively associated with frequency among those who have injured. Although sense of control was negatively correlated with DSH in the preliminary analysis, the signs were opposite from both the correlation matrix and what was hypothesized within the structural equation model (i.e., rather than being negatively associated with DSH history, sense of control was actually positively associated with DSH history in the NBH analysis). This is similar to an issue elaborated by Hayes (2009). Specifically, it is possible to have opposing indirect and direct effects, resulting in a nonsignificant total effect (see Hayes, 2009, pp. 413–414). This suggests the possibility of a complicated situation in which a single variable has competing associations (both positive and negative) resulting in paradoxical associations. While this may be the result of a statistical anomaly, it may also be an interesting aspect of the underlying psychological processes involved in the larger mediation model. Thus, our results may be indicative of a suppression effect that occurs when the relationship between a predictor and criterion, while controlling for other predictors, is opposite from what is expected given the bivariate correlations (Shieh, 2006). In other words, the reverse findings may be a statistical result of including other predictors of DSH in the model. Conversely, if model results are a true representation of directional effects (similar to the case in the Hayes, 2009, example), an alternative explanation is warranted. It seems that (at least at the strictly bivariate level) sense of control reduces the likelihood of engaging in self-harm; thus, individuals who do engage in self-harm have lower global levels of sense of control. When we then look only at the group of self-harmers, we see that sense of control is associated with increased self-harm. For individuals who engage in self-harm, this behavior may actually serve as a method of increasing one’s sense of control, thus resulting in the observed positive association between sense of control and DHS frequency. This may help explain why self-harming behaviors are so difficult to extinguish and may be a potentially important finding for the development of future interventions. These seemingly contradictory findings suggest additional research on the relationship between sense of control and DSH is warranted.
Contrary to hypothesis, desire for control was not associated with CM or DSH. This finding was somewhat surprising considering that desire for control has been previously thought to be associated with CM (Finkelhor & Browne, 1985; Svirko & Hawton, 2007) and DSH (Briere & Gil, 1998; Svirko & Hawton, 2007). However, this study does not support the notion that CM history has a significant impact on one’s desire to control self and others, one’s value on maintaining the appearance of being in control, or one’s fear of losing control. In addition, no significant association was found between desire for control and DSH, indicating the presence of other factors better account for the behavior.
Limitations
Several limitations should be noted. First, because the study was conducted on primarily female college students with limited ethnic diversity, the generalizability of results is limited. Our sample may not adequately capture the experiences of individuals with severe abuse histories, whom may be less likely to enroll in postsecondary education. Second, the data in this study may have been vulnerable to reporter bias and method variance. Although, the use of self-report measures of CM and DSH make it difficult to verify the actual occurrence of any of these phenomena, the measures used have shown good validity and reliability.
With regard to statistical limitations, the CATS is a continuous scale that does not provide categorical estimates of the presence versus the absence of maltreatment (Sanders & Becker-Lausen, 1995). Hence, no descriptive data for the prevalence of CM are provided for this sample. While internal consistency for the CM total score was good, internal consistency for the punishment subscale was lower, which may affect model fit. Moreover, any overlap in mediator constructs may contribute to multicollinearity. Additional statistical dilemmas relate to conducting analysis on a sample with relatively low rates of DSH and CM. The negative binomial hurdle model accounts for overdispersion and zero observations; however, this type of model does not allow for traditional fit statistics. In addition, there is currently little research on the measurement of indirect effects with nonlinear outcomes. Given these limitations, the current analysis used a pseudo measure of indirect effects and these effects should be interpreted with caution. Although this study tested potential mechanisms for DSH to occur, causal inferences cannot be made with this nonexperimental design.
Finally, although this study focuses on variables that mediate the relationship between CM and DSH, it should be noted that CM history is neither a sufficient nor determining risk factor for DSH. Many individuals who have been maltreated as children do not go on to engage DSH, and many who engage in DSH have no CM history. As such, future research would benefit from including additional life experiences beyond CM and invalidating environments that may be risk factors for DSH.
Clinical Implications and Future Directions
These findings contribute to our understanding of the mechanisms underlying DSH, which is important in developing prevention strategies and clinical interventions. Although many who engage in DSH retrospectively report histories of child abuse or neglect, it may be in the patient’s best interest to address self-destructive and therapy-interfering behaviors such as DSH prior to beginning evidenced-based trauma-focused treatment (Gratz & Chapman, 2009; Linehan, 1993). Many recent theories emphasize the role of emotional dysregulation in DSH (Gratz, 2007; Nock & Cha, 2009); therefore, increasing one’s emotional regulation is often the long-term goal in reducing DSH. Specific constructs that clinicians may wish to target include negative urgency, distress tolerance, and sense of control. Additional clinical research on specific therapy techniques that effectively address these constructs is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.