
Abstract
Trauma-focused cognitive–behavioral therapy (TF-CBT), a well-established, evidence-based treatment for children who have experienced trauma, has been increasingly utilized in a group format. Group therapy formats are appealing because they can be highly effective and have the potential to reach larger numbers of clients. Moreover, TF-CBT group delivery may be particularly valuable in reducing the feelings of shame, isolation, and stigma experienced by youth and their caregivers in the aftermath of traumatic experiences. This article reviews the group TF-CBT research, discusses the therapeutic benefits of TF-CBT therapy groups, and provides clinical and logistical guidance for implementing TF-CBT in group format, including a session-by-session protocol. Future directions for research and clinical work in this area are also discussed.
Trauma-focused cognitive–behavioral therapy (TF-CBT) was designed to help children, adolescents, and their families recover from the negative effects of traumatic experiences. Among treatments designed for this purpose, several reviews of the literature suggest that TF-CBT has the strongest empirical support for treating this population with 16 randomized controlled trials (RCTs) completed to date (de Arellano et al., 2014; Dorsey, Briggs, & Woods, 2011; Saunders, Berliner, & Hanson, 2004; Silverman et al., 2008). The efficacy of TF-CBT was originally evaluated by testing an individually delivered treatment for children with a history of sexual abuse (Cohen, Deblinger, Mannarino, & Steer, 2004; Cohen & Mannarino, 1996, 1998; Cohen, Mannarino, Perel, & Staron, 2007; Deblinger, Lippmann, & Steer, 1996; Deblinger, Mannarino, Cohen, Runyon, & Steer, 2011; King et al., 2000). More recent studies replicated the effectiveness of individual TF-CBT with children exposed to domestic violence, children impacted by natural disasters, and children placed in foster care as well as youngsters impacted by multiple, diverse traumas in the United States (U.S.) and internationally (Cohen, Mannarino, & Iyengar, 2011; Diehl, Opmeer, Boer, Mannarino, & Lindauer, 2015; Dorsey et al., 2014; Jaycox et al., 2010; Jensen et al., 2014; Murray et al., 2015). Three randomized trials also have examined the efficacy of TF-CBT delivered in group format (Deblinger, Stauffer, & Steer, 2001; McMullen, O’Callaghan, Shannon, Black, & Eakin, 2013; O’Callaghan, McMullen, Shannon, Rafferty, & Black, 2013). The purpose of this article is to review the research on group TF-CBT, discuss the therapeutic and cost benefits of TF-CBT delivered in groups, and provide clinical and logistical guidance for implementing TF-CBT in group format, including a sample session-by-session protocol. An additional session-by-session protocol is available in the Online Supplemental Table 2. This is the first article to date to include this focus on clinical guidance for group delivery, which supplements the already available individual TF-CBT training manuals and free of charge website training (Cohen, Mannarino, & Deblinger, 2006, 2012; Deblinger, Mannarino, Cohen, Runyon, & Heflin, 2015; http://tfcbt.musc.edu). Directions for future clinical research with regard to group TF-CBT are also discussed.
In recent years, there has been growing interest in the efficacy and implementation of TF-CBT groups. This may be due to the increasing demand for TF mental health services and the potentially greater cost-effectiveness of group therapy approaches in general. To date, research has not specifically examined differences in clinical outcomes or cost-effectiveness for group versus individual TF-CBT. However, one study examining a similar CBT for child trauma (Salloum & Overstreet, 2008) and several studies comparing group versus individual CBT approaches for child anxiety have found no significant differences in clinical outcomes for delivery modality (Liber et al., 2008; Manassis et al., 2002). These findings suggest that group versus individual TF-CBT delivery modes may not differentially impact outcomes, with decisions about delivery mode potentially best determined by pragmatic issues (e.g., wait lists and cost) and/or client preferences. In the area of cost-effectiveness, findings from a recent quasi-experimental study found that TF-CBT delivered individually was considerably more cost-effective in the long term as compared to treatment as usual (Greer, Grasso, Cohen, & Webb, 2014), and that trauma-specific CBTs had high benefit-to-cost ratios (Washington State Institute for Public Policy, 2014). Although untested, we believe that group delivery of TF-CBT is similarly more cost-effective than treatment as usual and potentially a more cost-effective strategy than individual delivery of TF-CBT due to reduced total therapist hours per client.
Group TF-CBT Research
Evidence for TF-CBT group delivery comes from two studies in the United States with young children who experienced sexual abuse (one open trial and one RCT), two RCTs in the Democratic Republic of Congo (DRC) with war-affected adolescents, and an open trial in Tanzania with orphaned children (O’Donnell et al., 2014). The two U.S. studies focused on children aged 2.5–10 years with a history of sexual abuse and their nonoffending mothers and include an open trial (Stauffer & Deblinger, 1996) and an RCT (Deblinger et al., 2001). The RCT documented the superior efficacy of TF-CBT groups as compared to support groups in helping mothers overcome abuse-related distress and intrusive thoughts, while also documenting that young children assigned to the TF-CBT groups showed significantly greater improvement with respect to body safety knowledge and skills than those children assigned to educational support groups. These improvements were maintained at a 3-month follow-up. This study, however, did not demonstrate significant differences across conditions on post-traumatic stress disorder (PTSD) symptoms, most likely because trauma narration in the TF-CBT groups was minimized due to the group format and the very young age of the children. Thus, as described below, TF-CBT groups currently incorporate trauma narrative individual sessions midway through the group program.
A substantial proportion of the evidence for TF-CBT group effectiveness comes from two small RCTs in the DRC and an open trial in Tanzania. The decision to use the group format for these trials in low-income African countries reflects both the possibility for greater reach and a potentially more culturally syntonic option for treatment delivery, given the collectivist cultures. There are some differences in implementation of TF-CBT in low-income countries, primarily that treatment is delivered by lay counselors—individuals with little to no prior mental health training—due to the shortage of mental health professionals. Lay counselors receive more intensive training (e.g., 2 weeks), close supervision, and are connected to local mental health professionals and organizations that can provide clinical support. Additionally, TF-CBT is provided with fidelity, but local stories, idioms, and cultural norms are acknowledged while teaching new skills. The first RCT in DRC, which focused on girls aged 13–17 years who had been exposed to multiple traumas including war-related trauma and sexual exploitation (O’Callaghan et al., 2013), compared a 15-session group-based, culturally modified version of TF-CBT to a wait-list control condition. Trauma narrative work was conducted in two to four individual sessions. The TF-CBT group led to significantly greater reductions in posttraumatic stress symptoms (PTS) as well as other psychosocial difficulties among the girls. The second RCT, by the same research group and using a similar TF-CBT group structure (i.e., 15 group sessions and two to four individual trauma narrative sessions), focused on former child soldiers and other war-affected boys, also aged 13–17 years, with very similar results (McMullen et al., 2013). Boys in the TF-CBT group had significant decreases in PTS and other psychosocial difficulties when compared with the wait list. Treatment gains were maintained or improved at the 3-month follow-up in both studies.
Another study that examined the potential value of group TF-CBT for multiply traumatized children was conducted in Tanzania with children aged 7–13 years who experienced the death of one or both parents and were having symptoms of PTS and/or maladaptive grief (O’Donnell et al., 2014). The pre–post findings of this open trial demonstrated significant reductions in PTS, grief, depressive symptoms, and behavioral problems at the end of treatment, with gains maintained at a 3- and 12-month follow-up. The approach included 12 group sessions (concurrent child and caregiver groups), the first eight of which were focused on the PRACTICE components of TF-CBT, with the final four groups focused on grief-specific components (see Cohen et al., 2006; online, free of charge TF-CBT Child Traumatic Grief training: http://ctg.musc.edu/). Individual trauma narrative sessions were conducted either at the child’s home or in a community setting (e.g., school) between-group sessions starting after Group Session 4 with children receiving two to four trauma narrative sessions. A portion of the group sessions (e.g., 20–30 min) during the final phase of treatment (i.e., Sessions 7–12) was dedicated to conjoint activities. Currently, a large-scale RCT (R01 MH095749; Dorsey & Whetten, MPIs) is underway in both Tanzania and Kenya to provide a more rigorous test of the group intervention.
It should be noted that participants in the groups described above have ranged from 2.5 to 17 years of age, but for purposes of this article, both children and teens will generally be referred to as children. In addition, it should be noted that “parents” involved in TF-CBT groups have included biological, adoptive, and foster parents, grandparents, other adult custodial relatives (e.g., aunts, uncles, and adult siblings), and nonrelative caregivers. Given the diversity of the child–parent relationships, for purposes of this article, adults participating in groups will be referred to as caregivers.
Potential Benefits of Group TF-CBT
Providing TF-CBT in a group format has many practical and therapeutic benefits. Groups allow for the provision of services to more clients at one time, which may also decrease waiting lists in clinics that serve large numbers of clients. In addition, groups conducted in the evenings increase the availability of these popular after school, after work therapy appointment times for more families. Group therapy can be conducted in a cost-effective manner with fewer therapists providing services to more families. With rising costs for mental health services and increasing reliance on managed behavioral health care systems, group therapy programs represent a generally acceptable approach to adapting evidence-based services to meet cost and service limits imposed by most managed care plans. Moreover, the required TF-CBT practice of administering standardized measures to assess group participants’ traumatic stress symptoms pre- and postgroup participation can provide the needed data to make the case for more intensive individual therapy, which may be necessary for the small group of less responsive group participants to obtain the needed managed care authorization for individual services. The group format also has the added benefit of being an excellent training vehicle for graduate students/postdoctoral fellows or new clinical staff as trainees and less experienced staff can serve as cotherapists. Such a format allows recently trained TF-CBT therapists to observe and be observed by more experienced staff members/supervisors. This approach, which allows for on the job coaching, is particularly helpful in low-resource settings (e.g., rural areas and low-income countries), where access to highly trained providers is limited.
For children, the group format often promotes a sense of shared experience that is, in and of itself, destigmatizing and may be particularly powerful in relieving the feelings of shame that many children impacted by interpersonal violence experience. This is very important given the research suggesting that feelings of shame are powerful predictors of long-term maladjustment in the aftermath of abuse (Feiring & Taska, 2005). Groups also allow for combining therapeutic work with fun and joy that can be infectious among participants and therapists, which may be an important benefit given the evidence that the use of humor supports healing in the aftermath of traumatic experiences (Davidson et al., 2005). In addition, groups provide an excellent format when teaching children skills, in that they can practice together and support each other in skill use.
The group modality also can be an excellent format for psychoeducation and skill building for caregivers (Webster-Stratton, Reid, & Hammond, 2004). More specifically in relation to TF-CBT, Deblinger, Stauffer, and Steer (2001) noted that caregivers assigned to TF-CBT groups exhibited decreased abuse-related distress and intrusive thoughts as well as decreased venting and rumination about frustrations with the justice and child protection systems as compared to caregivers assigned to support groups. This seemed to be a reflection of the TF-CBT structure which, when implemented in group format, encouraged the sharing of constructive coping efforts by providing a forum for caregivers to report each week on their successful skill implementation outside of sessions. Through this sharing, caregivers inspired each other to practice effective parenting and coping skills at home. Finally, TF-CBT provided in a group format may be particularly effective in demonstrating the prevalence of certain types of stigmatized traumatic events, such as child sexual abuse and related trauma(s), while also reducing the shame and stigma associated with such trauma(s) in the context of a supportive environment.
Protocol of Group TF-CBT
In high-income countries in which mental health professionals are more widely available, it is recommended that lead therapists considering implementing TF-CBT in group format be licensed in general mental health practices and have prior training and experience in individual TF-CBT implementation. Recommended training includes the free of charge TF-CBT training available online (https://tfcbt.musc.edu/), face-to-face introductory training, as well as at least 6 months of expert case consultation during initial implementation efforts. Although group TF-CBT follows the same structure and principles of individual TF-CBT, it does require additional skills in the management and dynamics of groups and collaboration with other therapists. Thus, it is advisable to begin offering small TF-CBT groups with optimally four to five children (with potential future groups including as many as six to eight children depending on demand), while also establishing weekly group supervision/consultation sessions during which group progress and dynamics are reviewed with the other group therapists. These group supervision/consultation sessions are designed to support fidelity to the TF-CBT model.
Group TF-CBT is provided to caregivers and children in separate groups that run concurrently for between 10 and 14 group sessions. Child participants should preferably be at about the same developmental level. Both same-gender and mixed-gender groups have been successful, although the studies in Africa included single-gender groups, as that was perceived to be more culturally appropriate. Groups are sometimes made up of children who have been through the same type of trauma (e.g., sexual abuse) or experience (e.g., death of loved ones), while other groups have included youth with diverse trauma histories with at least one type of trauma or unifying circumstance (e.g., foster care) in common. The caregiver group is led by one or more therapists and the child group is ideally led by at least two therapists, allowing for individual child work when needed. The groups move through the PRACTICE components in parallel. The PRACTICE components include Psychoeducation and Parenting, Relaxation, Affect expression and modulation, Cognitive coping, Trauma narrative and processing, In vivo mastery, Conjoint sessions, and Enhancing safety and future development. The caregiver and child groups may come together at the end of each session for conjoint session time or conjoint activities may be reserved for later therapy sessions. Brief conjoint activities are valuable early in treatment as they reinforce the skills learned in the separate groups (e.g., relaxation skills, emotional expression skills, praise, etc.). PRACTICE assignments are often given to encourage caregivers as well as children to try out the skills being learned between sessions (some examples of such are provided below). Based on prior experience, group sessions are ideally at least one to a maximum of 2 hours (Deblinger et al., 2001; O’Donnell et al., 2014). Confidentiality issues are handled in a similar manner as individual therapy; however, although group members are encouraged to maintain confidentiality, it is important to note that strict confidentiality by others in the group cannot be guaranteed.
The children work on the various components together as a group throughout the treatment except when engaged in the trauma narrative development. Trauma narrative details are not shared in group sessions so that group members are not exposed to details of another child’s traumatic experiences. These procedures are similar to those for other group interventions that include a trauma focus. Children can create a title and general introduction to the narrative together during group sessions, as these are not details about the trauma itself. The timing for initiation of the trauma narrative development sessions may vary somewhat based on several factors including the possible incorporation of traumatic grief components (i.e., Tanzania groups) as well as the children’s demonstrated needs for additional skill-building work. Generally, the first trauma narrative development session occurs after Session 4 or 5 but typically before Session 7 depending on the group’s therapeutic needs. During the trauma narrative component, children can either be pulled out of the group to work on their trauma narratives individually or individual sessions with each child can be scheduled in between-group sessions. For the pull-out option, one therapist takes a child out of group one at a time (for 15–20 min), while another therapist engages the rest of the group in an activity. These individual meetings allow for time with the child to create and process the trauma narrative. During this phase of treatment, caregivers are also prepared individually for the sharing of the narrative by the therapist who has worked with the child; this too can occur in a range of settings. These individual trauma narrative sessions may vary in number from two to five sessions and may be conducted at the clinic, at homes, and in community centers as in the Tanzania study. Regardless of which option is selected, the same therapist should work with the child on the narrative, prepare the caregiver for hearing the narrative, and facilitate the sharing of the narrative during the conjoint session when clinically appropriate.
These individual meetings also alleviate the caregivers’ often expressed concerns about children sharing their traumatic experiences with the group and/or children being exposed to the details of others’ traumatic experiences. When meeting with the child individually (utilizing either option), the completion of the narrative, including processing and preparation for the conjoint session in which the narrative is shared, is conducted in a similar manner as in individual therapy (Cohen et al., 2006). There may not be an opportunity to complete as many total trauma narrative chapters with children participating in group as compared to individual therapy, but the number completed is typically sufficient to assist with PTS reduction, as it is neither necessary nor helpful to have a chapter about every incident of a trauma if multiple incidents occurred. More information about encouraging the inclusion of particular chapters is highlighted in the session-by-session outline later in this article. It is important to provide similar individual session time for caregivers to not only prepare them for possibly reading the narrative (if clinically appropriate) but also to provide an opportunity for the disclosure of information they may not have felt comfortable sharing in the group setting. Although caregivers are typically willing to share most concerns in the group, they may prefer to address some issues in private.
Overall TF-CBT group structure
Group sessions need to be carefully structured for both the caregivers and children. A potential challenge in the caregiver group is the leader allotting roughly equal time to all participants. In addition, the careful selection of activities is important, particularly for groups with young children or children with behavioral difficulties. Activities should teach and reinforce the various skills in an engaging, fun, and interactive manner. Some activities that work well in individual therapy are not as effective in a group. For example, activities that can get a child overly excited often lead to the group losing focus. Activities that allow for some physical movement in a controlled manner often work well in a group, particularly with young children who may have a limited attention span and excess energy. Behavior management is also important in the child group, again particularly with young children or children with behavioral difficulties. Praise should be used liberally in all groups. The necessity of using more formal point systems and rewards should be determined on a group-by-group basis, as some groups may require frequent, concrete reinforcements throughout the session. Time-out can be utilized in a group with younger children. An explanation of time-out, when it is used (e.g., a child gives another child a not OK touch), and the procedure (e.g., which corner the child sits in) should be explained to both children and caregivers. The use of praise, reflective listening, selective attention, positive reinforcement, and negative consequences such as time-out is consistent with the principles and skills taught in the caregiver group.
When implementing TF-CBT individually, the treatment model is often tailored to the child and caregiver’s particular needs. Group TF-CBT, however, typically requires therapists to maintain a commitment to the planned weekly agendas in order to best accommodate all participants. Outlined below are the general objectives of group treatment sessions. It should be noted that there is considerable flexibility in the order of the proposed session activities and there are a wide array of creative activities that can achieve the described session goals. Thus, the outline offers general concepts that are important to cover across the three phases of treatment: the stabilization and skill building phase (PRAC), the trauma narrative and processing phase (T), and the integration and consolidation phase (ICE). Although fidelity to the overall flow of TF-CBT sessions is important, TF-CBT therapists are encouraged to address the specific needs and concerns presented by clients with compassion, creativity, and some flexibility while remaining aware of the importance of forward movement for the benefit of all group participants. For example, for groups in which there is a concern about ongoing risk for multiple children, the safety skills component can be moved to earlier in treatment, as would be done in individual therapy (Cohen et al., 2006). Given the time-limited nature of group, it is important to have a general outline and at least tentative agendas that can be modified depending on the needs of the families. The protocol given subsequently, Table 1, and online supplemental Table 2 provide general topics and activities covered and can also serve as a fidelity checklist designed for implementing TF-CBT in group format similar to the way that another TF-CBT fidelity checklist has been used to guide individual TF-CBT (Deblinger et al., 2015). The session-by-session guide for the group intervention for children who experienced the death of a parent (and includes coverage of the grief elements) is available here: http://cmx.sagepub.com.
Group TF-CBT Session-by-Session Outline.
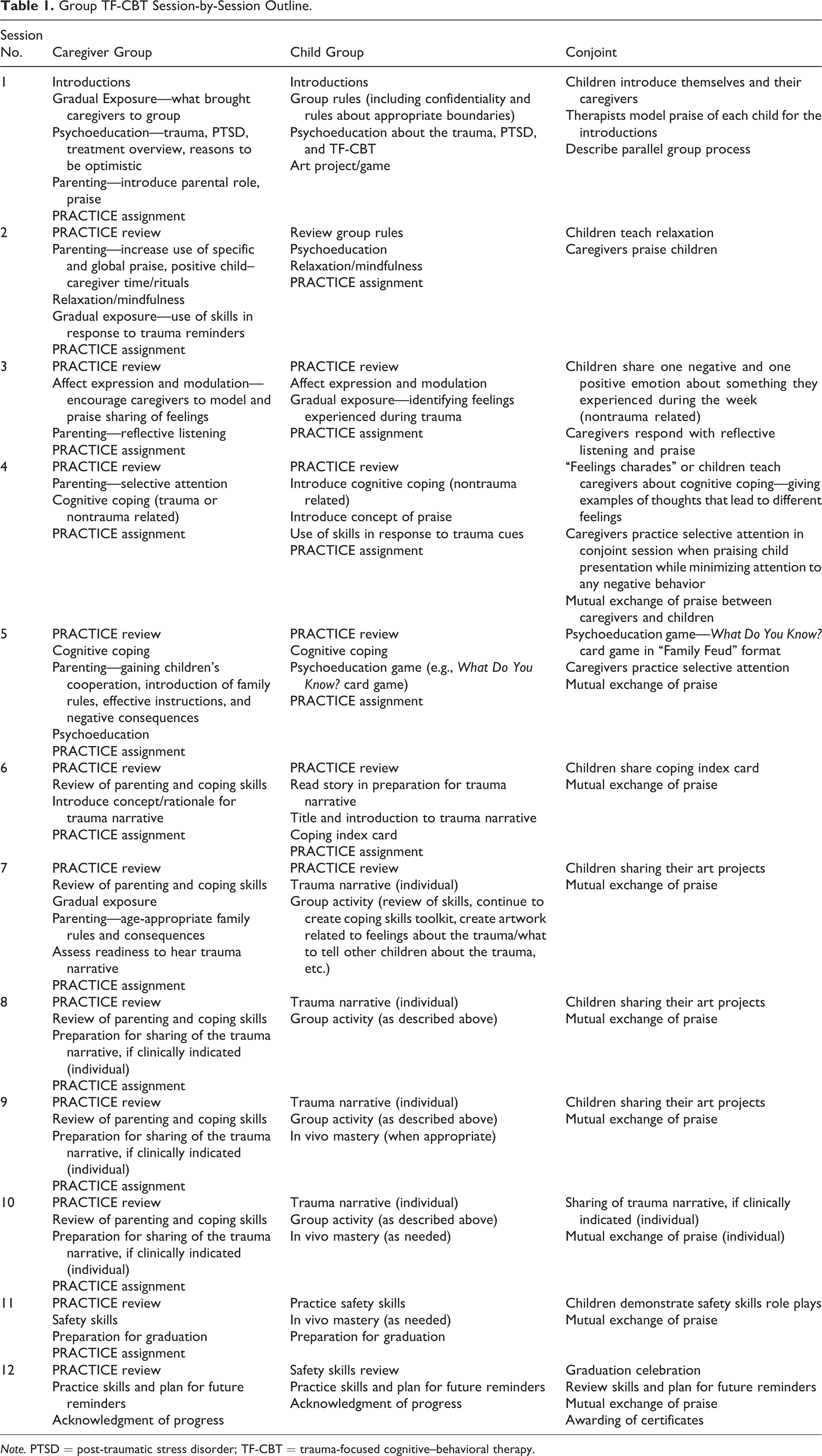
Note. PTSD = post-traumatic stress disorder; TF-CBT = trauma-focused cognitive–behavioral therapy.
Group TF-CBT Session-by-Session
The overall goals of the stabilization and skill building phase of group sessions are to create a therapy-conducive, safe group environment (e.g., group member introductions and set group expectations), introduce TF-CBT in terms of its theoretical basis and structure, begin gradual exposure with a general discussion about the identified childhood trauma(s), engage in skills development, and build group member engagement.
Session 1
Conjoint Session 1
The group program may begin with a brief conjoint child–caregiver session, particularly for young children, during which therapists introduce themselves and briefly but enthusiastically describe the parallel groups for children and their caregivers. Therapists should describe the separate but parallel caregiver and child groups emphasizing the fun and creative therapy activities for children and the important opportunities for learning and support for the caregivers. While the trauma focus may be briefly acknowledged, it is important that the written trauma narrative is not highlighted, as this can be anxiety provoking particularly for children. Therapists may encourage children to briefly introduce themselves and their caregivers by name. This provides an opportunity for therapists to model specific praise of each child’s introduction, while also assessing each child’s comfort level with the group format before separating the caregiver and child groups.
Caregiver Session 1
Evidence
Child Session 1
Following introductions, group rules are typically established by asking the children for rules that may be reviewed at the start of sessions when necessary. Children often spontaneously suggest listening and following directions. A rule about appropriate boundaries is typically included. With younger children, this rule may be described using the terms OK and not OK touches; for example, “Only use OK touches and OK words.” A brief discussion about OK and not OK touches follows, so the children are clear on what these rules mean. A rule about confidentiality is also included, such as “What is shared in group stays in group.” However, given that many traumas, such as sexual abuse, are generally surrounded by secrecy, a caveat is made that children may share what they are discussing in group with their caregivers to encourage open child–caregiver communication. At some point in this first session, it is important to note that all of the children in the group have experienced some type of trauma. The trauma(s) to be discussed may then be listed (e.g., sexual abuse, domestic violence exposure, traumatic loss, etc.) depending on the group makeup. As noted above, this shows children they are not alone in their experience and begins the gradual exposure process. Psychoeducation about the trauma(s) experienced, PTSD, and TF-CBT also begins in Session 1. Ideally, the group should end with a fun activity to facilitate group members getting to know one another, such as an art activity and/or a charades game in which participants share favorite hobbies. Time permitting, children may also be taught and engaged in a relaxation activity or exercise.
Session 2
Caregiver Session 2
Session 2 may begin with a review of caregivers’ reactions and questions regarding the information and the educational handout provided in the last session. This allows the therapist an opportunity to validate reactions and continue gradual exposure highlighting information that is destigmatizing and hopeful (e.g., prevalence of the trauma(s) experienced and reasons to be optimistic about child’s recovery), while also checking in on caregivers’ efforts toward the identification of resilient child behaviors exhibited between sessions.
The parenting component may begin, or continue, in this session with a focus on helping caregivers understand the development of PTSD symptoms, while learning to encourage adaptive child behaviors with positive family rituals and specific praise. The therapist may focus on encouraging caregivers to initiate and/or reinstate positive family rituals (e.g., child–caregiver walks, bedtime stories, family dinners, etc.) or one-on-one time that will create natural opportunities for caregivers to use praise with their children. During caregiver group sessions, it is important to repeatedly emphasize the power of positive caregiver attention, while also reviewing factors that enhance the effectiveness of praise for positive behaviors (e.g., specificity, enthusiasm, and avoidance of negative tags). Each week, caregivers’ feedback on their experience using praise during the past week should be elicited, providing an opportunity for the therapist to acknowledge that children who are not accustomed to receiving praise do not always respond favorably to praise initially but with time they will not only appreciate it but will often begin to return expressions of praise. As the group progresses, therapists’ predictions are often reinforced by various caregivers’ reports of their experiences with praise. Caregiver behavior rehearsals often begin with the sharing of the specific praise each caregiver plans to express to the child during a brief conjoint session. This provides an opportunity for caregivers to receive positive and constructive feedback from the group therapist as well as other group members before they actually share the planned praise with their child during a brief conjoint group activity. Caregivers’ initial praise examples often inadvertently include negative tags (e.g., Nice job, if you would only do that every day). Thus, caregiver behavior rehearsal and feedback from other caregivers, who are similarly attempting to master the use of specific and purely positive praise have been found to be particularly valuable during group.
The caregiver and child groups move in parallel and therefore relaxation is also typically taught in the caregiver group with an activity that engages caregivers in focused breathing or a mindfulness exercise. As a PRACTICE assignment this session, caregivers may be encouraged to practice and model for their children the use of relaxation skills (e.g., focused breathing) and continue to specifically praise adaptive child behaviors. The caregivers are each encouraged to select specific adaptive child behaviors that can replace problem child behaviors, so the therapist can follow-up on progress with praising those particular behaviors. Caregivers also should be apprised of the rationale for gradual exposure and the plan for the child group sessions to ensure they are comfortable with the activities, including, for example, teaching children the names of private parts (in the case of a group focused on child sexual abuse). Therapists generally utilize a combination of didactics, modeling, and behavioral rehearsal throughout the group program.
Child Session 2
During this early session, it is important to engage in gradual exposure by modeling and reviewing language that will help the children speak clearly and comfortably about the trauma(s) endured (e.g., sexual abuse, physical abuse, domestic violence, death, etc.). With younger children who have experienced sexual abuse, for example, body parts identification may be taught using cutouts of a boy and a girl in bathing suits. Children identify all body parts including “nonprivate” and private parts (i.e., vagina, breasts, penis, and buttocks; as noted above, caregiver permission is obtained in advance). For adolescents, following a playful competition during which the teens compete on the number of terms they know for the private parts (including slang terms), the group then may be encouraged to use the doctors’ terms when discussing sexual abuse and/or other sex education. Basic information about the prevalence, impact, and dynamics of types of traumas experienced by group participants may be reviewed in a manner appropriate to the developmental stage of the children.
As in individual TF-CBT, relaxation is taught in an age-appropriate manner relatively early in treatment often starting with deep breathing. Other relaxation skills such as progressive muscle relaxation, imagery, and/or mindfulness techniques can be taught. The use of these relaxation skills between sessions may be discussed and encouraged as a PRACTICE assignment particularly when coping with trauma reminders. The children may then be prepared to teach at least one relaxation skill to their caregivers in the conjoint portion of Session 2.
Conjoint Session 2
The conjoint activity typically involves the children as a group teaching their caregivers a relaxation skill. This activity is often followed by caregivers one at a time offering their children praise (as prepared) for a previously identified positive child behavior. This conjoint activity is often repeated across group sessions, so that caregivers can practice and hone their praise skills over the course of the group program.
Session 3
From this point on, the child sessions are described first as the caregiver session content typically follows in parallel.
Child Session 3
This child group may continue psychoeducation with a review of the use of relaxation skills to cope with daily stressors and trauma reminders. Next, affect expression is typically introduced by asking the children to generate a list of as many feelings as they can (e.g., within 45 seconds) and later engaging in an activity in which children explain what a particular feeling word means or giving an example of a time they felt that way. Teens may enjoy identifying situations that have a range of different emotions (e.g., starting a new school and going on a date) and listing all of the related emotions. Once a long list of feelings has been generated with hints by the therapists, if necessary, the various feelings listed may be combined and utilized throughout the group program. As part of ongoing gradual exposure, children may be asked to share feelings from the list, either verbally or by circling those that they experienced at the time of the trauma(s). “Feeling charades” (acting out a feeling without words while others guess the feeling) is another fun activity that can be played. After the game, the therapist emphasizes how much more effective it is in the long run to share feelings in words so others do not have to guess what they are feeling since sometimes people guess wrong. Next, children may begin a list of tools/skills they can utilize to help manage distressing emotions (e.g., talking to others, deep breathing, listening to music, etc.), creating a coping toolkit that can be added to throughout the group. Therapists may need to gently steer children away from problematic affect regulation activities such as punching walls or yelling and screaming by having them examine the consequences of such methods. As a PRACTICE assignment, children may be encouraged to share their feelings in words with their caregivers between sessions and take note of the skills and activities they naturally use to manage their emotions with an emphasis on incorporating the use of skills discussed in group.
In preparation for the conjoint session, children may be encouraged to share how they felt in nontrauma-related situations (“I felt…when…”). In fact, children may prepare to share with caregivers in the conjoint session a negative feeling and a positive feeling they experienced during the week by practicing specific I felt…when…statements. For this exercise, therapists should steer children away from sharing trauma-related feelings with caregivers this early in treatment instead focusing them on sharing mildly negative feelings they may have had about school, friends, or other recent experiences. It is also helpful to encourage children to share a positive feeling about something their caregiver did that they liked (e.g., “I felt happy when you helped me with my homework”). Therapists are encouraged to prepare notes about the feeling statements children plan to share to prompt them during the conjoint group sessions when nerves cause some children to forget their plan.
Caregiver Session 3
The caregiver group therapist may initiate group with a review of the caregivers’ PRACTICE assignment, which involves eliciting detailed descriptions of caregivers’ efforts to praise the adaptive child behaviors identified in the previous session as well as children’s reactions to those efforts. Caregivers often report surprise at the effectiveness of praise for specific behaviors. Once again, the therapist provides positive as well as constructive feedback regarding the caregivers’ PRACTICE assignment efforts with respect to praise.
The children’s group agenda may then be described to caregivers, including the activities planned to help the children expand their emotional vocabulary and verbally express their feelings, while also learning to more effectively manage their feelings. The rationale for such activities should emphasize research that children who express feelings in words rather than behaviors exhibit more positive adjustment (Eisenberg, Cumberland, & Spinrad, 1998).
The parenting topic that may be introduced in this session is reflective listening, which is designed to encourage adaptive behaviors and the effective expression of feelings by the children. It is important to encourage caregivers to role-play reflective listening skills in the group, as caregivers tend to be highly directive and jump quickly to problem solving when children share problems or express negative feelings. Rather, caregivers are reminded that there are many problems for which there are no real solutions, and children often simply want to feel heard. Thus, it is very helpful to have caregivers practice reflective listening via role plays with the therapist playing their child, while other caregivers observe and signal with a raised hand when the role-playing caregiver inadvertently moves into problem-solving mode as opposed to purely listening and validating the expressed feelings. During these role-play exercises, caregivers should be encouraged to minimize their attention to negative behaviors and focus on listening and specifically praising the child’s efforts to share feelings. Caregivers may be prepared for the conjoint activity by briefly practicing reflective listening via role plays that utilize the positive and negative feelings the child is planning to share (i.e., one of the child group therapists can provide that information in advance of the conjoint session).
For their PRACTICE assignment, caregivers are encouraged to model the appropriate sharing of feelings (e.g., frustration with work or disappointment) and catch and praise not only the adaptive child behaviors identified previously but also children’s efforts to appropriately share positive and/or negative feelings with words during the week. In terms of self-care, caregivers may also be asked to identify individuals in their lives with whom they can share their feelings and receive positive support particularly with regard to the crisis they are facing.
Conjoint Session 3
The conjoint activity may involve each child first sharing his or her prepared negative and then positive feeling statements with his or her caregiver(s), who practices responding simply with reflective listening and specific praise (e.g., “You felt sad and frustrated when you did poorly on the math test. I am really glad you shared your feelings with me about that test.”). In addition, the caregiver may share another specific praise regarding a positive adaptive behavior the child exhibited during the week. Global praise (e.g., “I’m so proud to be your parent”) or other means of expressing unconditional love for the child (e.g., hugs, high fives, and “I love you”) may be encouraged as well during these conjoint PRACTICE activities.
Session 4
Child Session 4
The child group typically starts with a review of coping skills learned thus far and children’s successful efforts sharing and managing their feelings between sessions. Next, the therapist may offer an introduction to cognitive coping in relation to nontrauma-related thoughts and feelings. Even very young children can master cognitive coping skills, but it is preferable to explain and offer examples of the simple relationship between thoughts and feelings to them, while the interrelationships between thoughts, feelings, and behaviors may be explained to older children and teens using the cognitive triangle. The group format allows children to share everyday examples of common social stressors (e.g., fight with a friend) that often highlight the fact that all children talk to themselves about their troubles and often have very similar thoughts and feelings. Children are then introduced to the concept of helpful and unhelpful thoughts and are given nontrauma-related example thoughts to decide if they are helpful or unhelpful as well as accurate or inaccurate. Again, working together, children determine the helpfulness of the thoughts by imagining how such thoughts might impact children’s feelings and behaviors. Older children and adolescents may be encouraged to begin trying to take note of their thoughts outside of session as a PRACTICE assignment using an automatic thought record. This important skill may then be added to each child’s individualized coping skills toolkit, which they may be encouraged to continue to draw on between sessions.
In preparation for the conjoint session, the therapists typically also introduce the concept of praise to the child group members and ask the children to identify a statement of praise they can say to their caregivers in the conjoint portion of the session. Over time, the children are steered away from praising their caregivers for things that cost money, as these things often need to be limited and it is preferable to encourage praise of the caregiver’s assistance, kind words, time spent together, and so on. Children’s statements of praise may be written down in order to prompt them during the conjoint session if they forget what they had planned to say. Other choices to offer children for conjoint activities include engaging their caregivers in a group feelings activity such as “feelings charades” or presenting their knowledge of cognitive coping to the caregiver group with each child, for example, presenting a thought and the resulting emotion. These examples can include both helpful and unhelpful thoughts as well as positive and negative emotions. The therapist might prompt the children in the conjoint session by asking them to describe the emotions generated by particular thoughts (e.g., “I am no good at anything”; “If I work hard, I can succeed”).
Caregiver Session 4
The caregiver group begins as usual by reviewing parenting PRACTICE assignment efforts and providing feedback. After eliciting caregivers’ accounts of their experiences with PRACTICE assignments at home, the parenting topic of selective or differential attention may be introduced. Caregivers are asked to identify a mild negative behavior the child has repeatedly exhibited that they may begin to actively ignore while they simultaneously identify and praise a positive replacement behavior. Caregivers, however, must be forewarned that when initiating active ignoring, the ignored behavior will sometimes get worse before it gets better (i.e., extinction burst) requiring a commitment to continue ignoring the behavior (assuming it is not dangerous in any way) until it diminishes. Caregivers may also be prepared to use praise and active ignoring skills during the conjoint session when children’s anxieties lead them to misbehave a bit in conjoint session. The parenting PRACTICE assignment then typically encourages a focus on utilizing selective attention, which combines active ignoring of a mild problem behavior with praising an identified positive replacement behavior.
Next, the planned agenda for the child group may be shared. Typically, cognitive coping skills are then introduced using the cognitive triangle with caregivers as well. Unlike the children who learn to apply these skills to nontrauma-related experiences only (at this stage of therapy before the narrative is completed), caregivers are encouraged to identify times they have found themselves feeling distressed about the trauma(s) endured by the child. The therapist can then elicit from caregivers the types of feelings experienced as well as underlying thoughts. The therapist may continue to elicit thoughts, recording them on a white board, until there are both functional and dysfunctional thoughts shared by caregivers, which then allows the group to begin to identify thoughts that are accurate and helpful as well as thoughts that are unhelpful and/or inaccurate. Once problematic thoughts are identified by the group, the therapist may challenge unhealthy thoughts through the use of Socratic questioning and the review of contradictory evidence. The group format also allows the therapist to encourage caregivers to help one another with problematic thoughts using the information they have learned thus far, which can be particularly therapeutic for participants.
Caregivers’ PRACTICE assignment is typically to continue to implement parenting skills including praise and active ignoring and to record in a journal or automatic thought record (provided by the therapist) their feelings and thoughts during the week when they find themselves dwelling on the trauma(s) or other distressing situations. After identifying problematic thoughts that seem to underlie their distressing feelings, caregivers are asked to practice replacing those problematic thoughts with more accurate, helpful thoughts while also recording how those new thoughts impact their feelings. One caregiver, for example, who had been blamed for the death of his or her spouse used the cognitive restructuring technique to combat feelings of shame and depression. Caregivers should also be prepared for the conjoint activity by being asked about the praise for their child. Even at this point in treatment, caregivers often need some coaching to remain purely positive and avoid negative tags when they praise. Thus, it is important to continue to have caregivers share the praise they will offer their child before the conjoint session, so they can receive constructive feedback if needed.
Conjoint Session 4
As noted above, this conjoint session may involve the children presenting or teaching cognitive coping skills to caregivers or the children engaging the caregivers in an affect expression or regulation activity, such as feelings charades. The children act out feelings without using words and the caregivers attempt to guess the feelings. Caregivers are encouraged to practice their selective attention skills. Following the conjoint activity, there may be a mutual exchange of praise, which can become an ongoing ritual to end sessions throughout the program. Children and caregivers may need some encouragement to make eye contact while delivering and receiving praise. Some teens balk at this activity at first but come to look forward to exchanging praise by the end of the group program.
Session 5
Depending on group progress, this session may focus on continued development of cognitive coping as well as integration of all the skills reviewed thus far.
Child Session 5
The child group may start with additional activities related to cognitive coping such as reading a story that demonstrates the concept, drawing people with thought bubbles on a white board, and so on, and following up on the PRACTICE assignment if one was encouraged. During this session, an emphasis is placed on the children identifying different types of (nontrauma related) problematic thoughts as well as helpful replacement thoughts. Older children and adolescents may be given a PRACTICE assignment of catching everyday dysfunctional thoughts and replacing them with healthier replacement thoughts using automatic thought records and/or a journal. It is then critical to review the children’s experience with this assignment in the session that follows.
In preparation for the conjoint session activity, psychoeducation may be reviewed, often using the What Do You Know? card game when the groups are in English or Spanish (Deblinger, Neubauer, Runyon, & Baker, 2006). Group format is quite conducive to engaging in a question and answer game using a game show-type format in which the question is read and children compete for points. It is important to carefully select the game questions to include those that cover the trauma(s) experienced by the group participants as well as those that are age appropriate. Children are often surprisingly excited about the possibility of showing off their newfound knowledge to their caregivers in the context of a conjoint session game. As in prior sessions, the children may also prepare praise statements for their caregivers.
Caregiver Session 5
In the caregiver group, the cognitive coping PRACTICE assignments may be reviewed as it is likely to take some time for caregivers to overcome the dysfunctional thoughts with which they may be struggling. The therapist, with the help of the other caregivers, may continue to utilize Socratic questioning to challenge dysfunctional thoughts that caregivers share in group. This session’s parenting topic is typically related to caregivers gaining their children’s cooperation with effective instructions and the introduction of family rules and negative consequences.
Psychoeducation is reviewed in preparation for the conjoint activity that is designed to begin the process of helping caregivers and children discuss the trauma(s) experienced in general terms. Depending on group progress, therapists may suggest to caregivers that children may begin to have individual time with their therapists in order to focus more on their personal experiences. The trauma narrative, however, is not typically highlighted until it becomes clear that most children will be responsive to creating some type of trauma narrative or other trauma exposure product (e.g., drawing, poem, rap, etc.). Praise statements for the children are also prepared and reviewed by therapists. Caregivers are encouraged to implement parenting and individualized coping skills PRACTICE assignments during the week. Therapists are often more successful in encouraging caregivers’ commitment to engaging in healthy coping practices between sessions by frequently emphasizing their important influence as coping role models for their children.
Conjoint Session 5
For this session’s conjoint activity, the families often review psychoeducation through the game show format referred to as “Family Feud.” The format of this game requires each family to agree on a team name, which is written on the dry erase board where points will be tracked. Questions are read and children and their caregivers raise their hands to answer the question; team members can help each other out with their responses. Points are earned for effort (i.e., volunteering to answer a question) and correct answers as well as for team members praising each other for correct responses. Although specific details of children’s traumatic experiences are not discussed, the game likely triggers traumatic memories that are essentially paired with neutral, and in many cases, positive emotions as the competitive game format often elicits laughter and feelings of pride. These emotions may then replace the overwhelming negative emotions that have been associated with the traumas being discussed. Again, this activity might lead to some mild negative child behaviors due to discomfort or overly enthusiastic competitive child behaviors. Caregivers thus have another opportunity to use praise and selective attention. The conjoint session may again end with a positive end-of-session ritual such as the mutual exchange of praise that each caregiver–child dyad engages in one at a time.
Session 6
Child Session 6
This child group typically starts by introducing the concept of a trauma narrative through the reading of a story, handout, or published narrative about the type of trauma(s) experienced by group participants (e.g., Please Tell, Jessie, 1991, Something is Wrong at My House, Davis, 2010). The children are then prompted to share a title and introduction similar to the character in the book as if they were going to write their own book. If chapters more directly related to the trauma will not begin until the next session, the trauma narrative is not explicitly introduced to avoid raising anxiety about the narrative over the course of the week. A fill-in-the-blank introduction can be utilized with younger children to facilitate completion in the group setting. After completing a title and introduction, depending on the progress and makeup of the group, therapists may turn the focus of the group to continuing to integrate coping skills by encouraging the creation of coping skills index cards in which children list their top three coping skills they can use at home when they become upset. Groups that are progressing well may be ready to begin the development of the outline for their trauma narrative and the second more detailed chapter of their trauma narrative in individual pull-out sessions. See Session 7 below for more details regarding the process for beginning the trauma narrative. Children may also be introduced to the concept of self-praise by learning to make self-statements such as “I’m proud of …” or “I’m good at …” while also generating praise statements for their caregivers in preparation for the conjoint session.
Caregiver Session 6
The caregiver group begins as usual with a discussion about the previous week’s PRACTICE assignment. The concept and rationale for the increased focus on trauma narration and processing in the children’s group is shared with caregivers when appropriate. The therapist may emphasize the focus on helping children discuss, express verbally, and/or write about their thoughts and feelings about the traumatic experiences through individualized activities. It is important not to overly focus on a written narrative as the children in the group may vary in the way they are engaged in the trauma narrative and processing. However, it is important to emphasize the overall goals of reducing children’s trauma-related avoidance and/or shame while supporting their efforts to make sense of their experiences. The caregiver group also continues to focus on the implementation and review of effective parenting and coping skills. Thus, caregivers may continue to be given individually tailored parenting and coping PRACTICE assignments.
Conjoint Session 6
For the conjoint activity, children typically share their coping skills index cards with their caregivers, so the caregivers can prompt them to use these skills throughout the week. Children and caregivers then may exchange praise.
Sessions 7 Through 10
By this stage of the group therapy program, the focus of treatment with the children turns to the trauma narrative and processing, while caregivers continue to integrate the coping and parenting skills they have been learning. This process is followed by preparing the child and the caregiver individually, as clinically indicated, for a conjoint session in which the trauma narrative is shared. As noted above, the concept of a narrative in written form is not introduced in group as all children may not complete the narrative in the same manner. Similarly, given that it may not be appropriate to share the trauma narrative with caregivers in all cases, careful clinical judgment should be used regarding any group discussions of sharing the narratives with caregivers. Moreover, if there is no expectation of a written narrative that will be shared, therapists can use their discretion to help children create narratives in the manner best for them and can determine that the narrative will be shared in part, in its entirety, or not at all without caregivers or children in the group thinking they have not met certain group expectations.
As noted above, the trauma narrative is completed individually with the children either by pulling out the children from group one at a time or scheduling individual sessions in between-group sessions. The process of completing the trauma narrative, processing, and preparing for the conjoint session in which the trauma narrative is shared continues in a manner similar to individual therapy (Cohen et al., 2006). The number of sessions children have to complete the narrative, however, is limited by the group time frame. Thus, chapters may be more limited and, for example, might only include the first, middle, and/or last times the trauma occurred (if there were multiple incidents). At least one middle episode is important to include in cases involving chronic abuse, as middle episodes are often associated with greater shame for children who may have begun to anticipate these episodes but were not yet able to disclose. Also, for those who have experienced multiple or complex trauma, it is important to identify chapters that reflect the overarching trauma themes that may underlie a child’s symptoms (e.g., self-blame, betrayal, distrust, etc.). In addition, it is helpful for children to include a situation related to the trauma that the child thought he or she would never tell anyone about (e.g., the saddest, scariest, or most shameful time/situation) and it can be helpful to have children include positive memories about the deceased loved one (if relevant), personal strengths demonstrated, and/or kindnesses or support received from others. Children individually process their chapters and complete a final chapter that demonstrates the culmination of what they have learned about the trauma and about themselves, others, and the world, and/or what they might want other children to know. As in individual therapy, the appropriateness of sharing some or all of the narrative with the caregiver should be carefully assessed and only when appropriate children share their narratives in a private conjoint session.
When children are being pulled out individually by one therapist for narrative work, the other child group therapist engages the remaining children in activities such as a review of coping skills through discussing or continuing to design and/or create their coping skills toolkits. In addition, at this stage of treatment, children often enjoy creating individual- or group-art projects that might depict how children feel when they have experienced trauma, how they feel after participating in counseling, what they have learned, and/or what they would like other children to know about the type of trauma experienced. These activities may be ongoing during the group sessions when some children are still completing their trauma narratives in separate individual sessions. Many trauma-related avoidant behaviors (e.g., refusing to sleep alone) naturally decrease through the process of the trauma narrative and processing. However, if trauma-related avoidant behaviors remain following the processing of the narrative, an in vivo plan can be created at this time to decrease the avoidance. This would be conducted in a manner similar to individual therapy (Cohen et al., 2006).
The caregiver groups during this phase may continue to begin with a review of the PRACTICE assignments, followed by discussion and practice of parenting skills and cognitive coping. At this point in treatment, there is an increasing focus on gradual exposure to discussing their children’s traumatic experiences. If all the children are engaged in one type of narrative or another, the concept of and rationale for the trauma narrative may be reviewed and caregivers may be asked to share more details concerning their children’s traumatic experiences to allow therapists to assess caregivers’ emotional preparedness for potentially hearing their child’s narrative. Whenever possible, it is helpful to provide positive updates to caregivers on their children’s progress particularly with respect to their overall ability to acknowledge and/or discuss their traumatic experiences. Parenting skills training at this stage may continue to focus on encouraging adaptive behaviors, while consistently learning to highlight family rules and administer mild consequences (e.g., time-out) for breaking those rules. The PRACTICE assignments are tailored to address parenting and coping skills most relevant to group members.
Conjoint activities during the trauma narrative development phase may consist of, time permitting, the mutual exchange of praise and the children sharing their art projects, thus providing further gradual exposure to discussing the trauma(s) with caregivers. Again, this allows therapists opportunities to observe and assess group participants’ emotional reactions in terms of planning for possible individual trauma narrative sharing sessions (Cohen et al., 2006).
It is important for therapists to continue to carefully assess the caregivers’ readiness to hear the trauma narrative from the child in a manner similar to that of individual therapy (Cohen et al., 2006). Caregivers need to be prepared individually for the conjoint session either during individual sessions between-group sessions or through individual pull outs with each caregiver during the group. During these individual caregiver sessions, the narrative should be shared (when clinically indicated) with the caregiver without the child present. As in individual therapy, this is critically important in assessing whether it would be of therapeutic benefit to have the child share all, some, or none of the narrative with the caregiver himself or herself (Cohen et al., 2006). The therapist should elicit the caregiver’s reaction to the trauma narrative, so that questions and concerns can be addressed prior to meeting with the child and so the therapist can help the caregiver process his or her emotional reactions. This will help the caregiver to more effectively manage his or her own emotions and focus more on supporting the child around what has been shared if and when the narrative is shared in a private conjoint caregiver–child session. One caregiver, for example, was not aware until the group leader shared the child’s narrative with her in preparation for the conjoint session (in an individual meeting), that the child remembered the parent’s death, in great detail. She and the child had not discussed the death during the intervening 7 years. The caregiver was saddened to realize that the child had been thinking about the death for all of that time; she had assumed the child did not remember what happened.
The sharing of the trauma narrative, if clinically appropriate, typically occurs between Sessions 8 and 10 with each family separately reviewing with the therapist the child’s narrative as in the case of individual therapy (Cohen et al., 2006). In the traumatic grief groups, sharing occurs in Session 8 to allow for grief-focused group work subsequent to trauma narrative completion (see O’Donnell et al., 2014). Specific grief-focused work with the children includes addressing their ambivalent feelings and relationships with the deceased as well as preserving positive memories of the deceased. Another important focus for grieving children is developing and committing to ongoing positive relationships.
Session 11
By this session, caregivers and children have generally completed the development, processing, and sharing of the trauma narrative. Thus, the focus of Session 11 turns to personal safety, as well as the consolidation of skills and closure.
Child Session 11
During this session, safety skills are introduced or reviewed if previously discussed and role plays are typically taught and practiced by the children in an age-appropriate manner relevant to the primary trauma(s) endured (Deblinger et al., 2001). Safety plans and role plays that involve the practicing of calling 911 might be incorporated in groups with children exposed to domestic violence. For children who have been sexually abused, the safety skills component may start with psychoeducation about touches or age-appropriate sex education. Younger children may review OK, not OK, and confusing touches. For older children, age-appropriate sex education is provided (with caregiver permission) as well as a discussion of timelines for ideal “romantic” relationships (i.e., when one begins holding hands, kissing, hugging, engagement, marriage, sex, etc.). Safety skill scenarios (e.g., abuse threats, exposure to domestic or community violence, etc.) are created and roleplayed that are relevant to the children in the group. During this session, therapists may also elicit from the children ideas that might contribute to their final group celebration. Even older children often enjoy making and decorating graduation caps for the end of therapy celebration. Finally, they generate their praise statements for the caregivers.
Caregiver Session 11
The caregiver group may start as usual with the PRACTICE assignment review. The rationale and limitations (e.g., these skills are not a guarantee that the child will never experience victimization again) for teaching children personal safety skills are presented in an interactive manner, so that caregivers can ask questions and prepare for the conjoint activity. This may involve caregivers participating in brief preparatory role plays in which they act as themselves demonstrating how they would respond to the child disclosing a new threat or an experience of abuse or exposure to violence. Later during the conjoint session, caregivers will engage in very similar role plays with their children. Depending on the potential concerns for revictimization and/or acting out behaviors, more than one session may focus on safety skills. During this session, preparations may also be discussed for the graduation celebration. Caregivers may be encouraged to collaborate in planning the celebration party by contributing music, decorations, drinks, snacks, and/or desserts. The PRACTICE assignment is typically the continued use of the parenting and coping skills.
Conjoint Session 11
Children typically demonstrate the safety skills role plays for the caregivers during this conjoint session with each child participating in a role play with his or her caregiver playing the part of the adult the child tells. When appropriate, caregivers reflect back what the child has disclosed and specifically praise the child for his or her use of the safety skills. Children and caregivers then may engage in the mutual exchange of praise.
Session 12 (Final/Graduation Session)
Child Session 12
The final child group typically starts with a review of the safety skills role plays as well as a discussion of the various skills learned in group. Depending on the age of the children, a graduation activity may be planned. Young children may enjoy singing the “My Body” song (www.peteralsop.com) with or for their caregivers. In the final session, older children and teens may enjoy presenting to their caregivers a group art project, rap, or news show about what they learned about the trauma(s) experienced. The children may also be encouraged to prepare self-praise and praise for their caregivers related to the caregivers’ group participation or changes at home as a result of their group participation.
Caregiver Session 12
The caregiver group begins as usual with the PRACTICE assignment review. The various skills taught throughout therapy are reviewed with a focus on the continued use of skills after therapy ends to reduce the risk of relapse while also encouraging caregivers to feel free to contact the therapist for support if such needs arise. Caregivers may be encouraged to prepare praise for the final conjoint session that acknowledges their children’s behavioral progress and participation in group. This final praise also often includes global expressions of praise (e.g., I love you) and affection, including hugs and high fives.
Conjoint Session 12
For the conjoint activity, children often enjoy entering the caregiver group room wearing their graduation caps with “pomp and circumstance” playing. A planned group activity may then be introduced as previously described. Children sit next to their caregivers and graduation certificates are distributed to children and caregivers one by one. The final mutual exchange of praise may take a bit longer than usual, as caregivers are encouraged to be as effusive as possible with their praise. Finally, a relaxed, unstructured celebration begins with the sharing of food brought by the caregivers, music, and casual conversation. When the children leave, they may be encouraged to walk through the office suite or clinic setting wearing their graduation caps to share their accomplishment with office staff that may be on hand with congratulatory remarks, handshakes, and high fives.
Conclusions and Future Directions
In conclusion, TF-CBT in group format may provide an alternative to individual delivery in situations in which large numbers of children and their caregivers are in need of TF treatment such as in the aftermath of widespread disasters as well as in urban and/or international settings where specialized therapy resources may be limited. Initial research on group-delivered TF-CBT shows positive outcomes (Deblinger et al., 2001; McMullen et al., 2013; O’Callaghan et al., 2013), with the largest group TF-CBT randomized trial to date currently underway in Tanzania and Kenya. Future directions for research include comparative outcome and cost–benefit analyses on group versus individual TF-CBT approaches. Such research may help to identify distinct client profiles that may show greater responsiveness to group versus individual approaches (e.g., children with high levels of shame and caregivers with higher levels of depression and parenting deficits). Rural settings present challenges for group programs, as considerable delays are likely to occur waiting for a sufficient number of families to form a group. The use of telehealth methods to create groups in such settings may offer another fruitful area for research on the dissemination TF-CBT services. Research on evidence-based practices is increasingly focused on feasible methods of scaling up practice and achieving sustainability (Wiltsey Stirman et al., 2012). Including group delivery as a mechanism for providing TF-CBT to children and their families allows an additional option for reaching a greater number of children with need and, as previously mentioned, for using on-the-job coaching methods to build a skilled expansive workforce of TF-CBT providers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author is a developer of TF-CBT and receives royalties and honoraria for TF-CBT related activities. The second and third authors receive honoraria for TF-CBT related activities.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible in part by funding from grant numbers MH053241, MH081764, and MH096633 awarded from the National Institute of Mental Health (NIMH). The authors would like to acknowledge Beth Cooper, MS, for her review of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.