
Abstract
Although a cycle of harsh and abusive parenting has been recognized for decades, this cycle is not inevitable. Indeed, the mechanisms underlying such patterns, and the resources parents may access to disrupt this cycle, require further study. Research investigating those processes has either relied on cross-sectional designs or largely assessed mediators or moderators at one time point. The current investigation of parent–child aggression (PCA) risk utilized a longitudinal design to consider possible mediators and moderators across three time points. Mothers and fathers reported on their personal history of physical and psychological abuse during the last trimester of the mother’s pregnancy; their PCA risk was assessed concurrently when their child was 6 months and when their child was 18 months. Current findings support several mediators for mothers, although fewer for fathers, prenatally, but mediation was not observed across time. Similarly, several moderators of the effect of personal history of physical and psychological aggression on PCA risk were identified prenatally but not across time. Thus, several qualities believed to account for, or mitigate, the intergenerational transmission of PCA may not be consistent—underscoring the continued need to identify factors that account for the cyclical process versus what may interrupt intergenerational transmission.
Keywords
Since 2011, child protective services has witnessed an increase in maltreatment referrals, investigations, and substantiated cases (U.S. Department of Health and Human Services [DHHS], 2017). Although over 4 million children were referred in 2015 (DHHS, 2017), such official statistics are routinely judged to underestimate the true incidence of maltreatment, particularly physical abuse that constitutes 26% of all maltreatment (Sedlak et al., 2010). Physical discipline use is also pervasive in the United States, with almost two thirds of parents reporting recently spanking their 3-year-old (Taylor, Lee, Guterman, & Rice, 2010). Use of physical discipline strongly predicts physical abuse (Gershoff & Grogan-Kaylor, 2016), with spanking of children as young as one predicting later involvement in child protective services (Lee, Grogan-Kaylor, & Berger, 2014). Because physical abuse often arises during escalating episodes of physical discipline (Benjet & Kazdin, 2003; Durrant, Trocmé, Fallon, Milne, & Black, 2009), many have argued that physical abuse and physical discipline are both end points on a parent–child aggression (PCA) continuum (Gershoff, 2010; Greenwald, Bank, Reid, & Knutson, 1997; Rodriguez, 2010a; Straus, 2001; Whipple & Richey, 1997). Physical abuse can thereby be construed as a consequence of intensified, escalating physical discipline.
Professionals seeking to prevent child abuse strive to predict the likelihood a parent will escalate along such a continuum to become abusive—termed child abuse potential (Milner, 1994). Child abuse potential involves qualities observed in those who physically abuse their children, which relates to both physically and psychologically abusive discipline tactics (Rodriguez, 2010a; Rodriguez & Richardson, 2007) as well as coercive discipline practices (Haskett, Scott, & Fann, 1995; Margolin, Gordis, Medina, & Oliver, 2003). Therefore, consistent with a continuum approach, PCA risk can be conceptualized inclusively to encompass greater child abuse potential and likelihood of applying harsh and abusive discipline practices. The current investigation will evaluate how parents’ personal history of physical and psychological aggression as children predicts their own PCA risk by considering potential mediators and moderators.
Role of History
One of the most classic theories proposed to characterize parents’ use of harsh and abusive parenting is the intergenerational transmission hypothesis—also known as the cycle of violence—in which those who experienced harsh and abusive parenting as children grow up to become harsh or abusive parents (Curtis, 1963; Straus, 1983). Indeed, several studies support such intergenerational persistence for child maltreatment (e.g., Bartlett, Kotake, Fauth, & Easterbrooks, 2017; Berlin, Appleyard, & Dodge, 2011; Thornberry & Henry, 2013) as well as harsh parenting (e.g., Bailey, Hill, Oesterle, & Hawkins, 2009; Simons, Whitbeck, Conger, & Wu, 1991). Those who retrospectively report experiencing more physical abuse also report receiving more psychological abuse (Bifulco, Moran, Baines, Bunn, & Stanford, 2002; Miller-Perrin, Perrin, & Kocur, 2009), and mothers who received more childhood physical and emotional abuse obtain higher child abuse potential scores and report administering more physical and psychological aggression (Bert, Guner, & Lanzi, 2009; Cohen, Hien, & Batchelder, 2008).
Although this cyclical process is widely recognized in lay and professional circles alike, early work revealed the cycle was not immutable because the majority of those with harsh and abusive discipline histories did not perpetuate this cycle (Kaufman & Zigler, 1987; Widom, 1989). Indeed, some studies suggest equivocal support for intergenerational transmission, particularly for physical abuse (Sidebotham, Golding, & the ALSPAC Study Team, 2001; Widom, Czaja, & DuMont, 2015). Such findings are consistent with the premise that some parents maintain the cycle, whereas others disrupt this intergenerational process (Dixon, Browne, & Hamilton-Giachritsis, 2009). Moreover, the effects of personal history of harsh and abusive parenting on PCA risk may diminish if current functioning is considered; one study found that the effect of personal history of abuse on perpetration of abuse decreased when controlling for current levels of adult difficulties (e.g., mental health, poverty; Ben-David, Jonson-Reid, & Kohl, 2015). Thus, continued work is needed to clarify what may be the mechanisms that account for the intergenerational transmission of PCA as well as what resources parents may access to break this cycle.
Mediating Factors
Apart from the intergenerational transmission hypothesis to predict PCA, social information processing (SIP) theory has been applied to predict PCA risk (Milner, 2000). SIP theory proposes cognitive–behavioral individual-level factors that may culminate in PCA, including parenting beliefs like physical discipline approval, expectations and evaluations, and awareness of discipline options (Milner, 2000; Rodriguez, Silvia, & Gaskin, 2017). A personal history of harsh and abusive parenting may confer increased risk of parents’ use of harsh and abusive PCA via a number of possible mechanisms, not only individual-level factors but community factors as well (cf. Valentino, Nuttall, Comas, Borkowski, & Akai, 2012). The current study concentrates on potential individual-level mediators consistent with SIP theory, particularly given that these cognitive processes are conceivably therapeutically modifiable.
Of the parenting beliefs considered in SIP theory, approval of physical discipline is one potential mechanism that may arise from a personal history of harsh and abusive parenting. For example, PCA risk was elevated for adolescent mothers who value corporal punishment (Haskett, Johnson, & Miller, 1994), and favorable disciplinary attitudes mediate the concurrent association between disciplinary history and disciplinary responses (Bower-Russa, 2005). Mothers with greater personal experience of physical punishment and violence were more likely to report spanking their infants as well as holding attitudes approving of corporal punishment—yet such PCA approval attitudes did not mediate the association between adverse childhood experiences and infant spanking (Chung et al., 2009). Others have found that grandparents’ effect on their children’s harsh parenting was not consistently—and possibly only weakly—attributable to those parents’ beliefs in the value of physical discipline (Simons et al., 1991). Notwithstanding these mixed results, attitudes endorsing PCA could be one mechanism whereby a personal history of harsh and abusive parenting is transmitted intergenerationally.
Alternatively, a personal experience of harsh and abusive parenting may affect a parent’s perceptions of children’s intent, cultivating negative attribution biases. Prior research has identified negative child attributions relate to child abuse potential (e.g., Rodriguez & Tucker, 2015) and has identified parents’ negative attributions and unrealistic expectations partially mediated intergenerational abuse transmission (Dixon, Hamilton-Giachritsis, & Browne, 2005a). But another study observed that mothers’ personal physical abuse history, but not overall hostile attributions, predicted their children’s victimization (Berlin et al., 2011), although this study did not operationalize negative attributions relevant to children. Related to negative attributions, higher PCA risk parents appear to expect more compliance from children (Rodriguez, Smith, & Silvia, 2016b). Perhaps a personal experience of harsh and abusive parenting transmits an expectation of greater compliance from their own children. Parents with more harsh and abusive parenting histories may also have less exposure to nonphysical discipline approaches. Given greater familiarity with harsh techniques predicts their use by parents (Rodriguez & Sutherland, 1999), not surprisingly, many parenting programs strive to educate parents on nonphysical discipline alternatives (e.g., Knox & Burkhart, 2014; Prinz, Sanders, Shapiro, Whitaker, & Lutzker, 2009). Potentially, the cycle is thus perpetuated because of limited personal exposure to nonphysical discipline options.
Apart from the potential impact of personal history on the development of SIP parenting beliefs, the experience of harsh and abusive PCA contributes to negative mental health consequences such as psychological and substance use difficulties (e.g., Herrenkohl, Hong, Klika, Herrenkohl, & Russo, 2013). A robust relationship has also been identified between perpetration of harsh and abusive parenting and parents’ co-occurring mental health and substance use problems (Doidge, Higgins, Delfabbro, & Segal, 2017; Stith et al., 2009) as well as intimate partner violence (Bourassa, 2007; Capaldi, Kim, & Pears, 2009). Thus, a parent’s personal history of harsh and abusive parenting may indirectly increase their own risk of later PCA perpetration because of the influence of that history on personal vulnerabilities like compromised mental health, which would be more proximal to PCA perpetration (e.g., Milner et al., 2010). As noted earlier, the effects of personal history on perpetuation of PCA are diminished when considering proximal adult functioning such as mental health difficulties (Ben-David et al., 2015). Others have reported mental health problems as well as living with a violent adult accounted for parents’ risk of intergenerational abuse transmission (Dixon, Hamilton-Giachritsis, & Browne, 2005b). In contrast, mediation in the intergenerational transmission of mothers’ abusive parenting was not observed for maternal mental health problems in another study (Berlin et al., 2011), although substance use problems have been proposed as a mediator (Appleyard, Berlin, Rosanbalm, & Dodge, 2011). Collectively, these proximal indices of personal vulnerabilities which may arise from a history of harsh and abusive parenting—mental health problems, substance use, and intimate partner violence—may serve to compromise, or “tax,” a parent’s discipline decision-making abilities, thereby increasing their risk to escalate PCA. Such taxes are also implicated as risks in the SIP model of PCA risk (Milner, 2000; Rodriguez et al., 2016b) and may represent an alternative pathway, apart from parenting beliefs, whereby a personal history of harsh and abusive parenting increases a parent’s risk to perpetuate the cycle.
Moderating Factors
Yet as noted earlier, many parents break the cycle of violence. Identifying intrapersonal and interpersonal factors that may mitigate a personal history of harsh and abusive parenting would represent critical targets for prevention and intervention. Consistent with a burgeoning interest in resilience (Masten, 2014), we focus on positive, protective mechanisms that may buffer a personal history of harsh and abusive parenting rather than risks that could worsen the effects of history. For example, having a supportive partner may mitigate intergenerational transmission (Schofield, Conger, & Conger, 2016), although others have not identified supportiveness of a partner as a significant moderator (Herrenkohl, Klika, Brown, Herrenkohl, & Leeb, 2013). Greater social support was identified as a quality that distinguishes between those who break the cycle versus those who maintain (Dixon et al., 2009). Other than interpersonal resources, comparatively less research has considered the role of intrapersonal resources as buffers in the intergenerational transmission of PCA. Emotion dysregulation is associated with personal experience of harsh and abusive parenting (Kim & Cicchetti, 2010) as well as increased child abuse risk (Lowell & Renk, 2017), with better maternal emotion regulation linked to less overreactive discipline approaches (Lorber, 2012). Potentially, emotion dysregulation may not only represent a result of such a personal history; stronger emotion regulation abilities as an adult could serve to buffer the likelihood of parents overreacting and engaging in harsh and abusive parenting, thereby decreasing parents’ PCA risk. Additionally, some research suggests more problem-focused coping skills relate to lower parental PCA risk (Cantos, Neale, O’Leary, & Gaines, 1997; Rodriguez, 2010b), although others have suggested coping skills are more equivocal in increasing PCA risk (Black, Heyman, & Smith Slep, 2001). Yet women’s poorer coping skills also appear to be a consequence of personal history of physical or psychological abuse (Hager & Runtz, 2012). Some initial evidence suggests active coping skills may represent a positive resource to mitigate poor parenting history (Schofield, Conger, & Neppl, 2014). The potential ability of interpersonal resources, such as greater partner satisfaction and social support satisfaction, as well as intrapersonal resources, such as stronger emotion regulation and coping abilities, warrants further inquiry as potential moderators of the intergenerational transmission of harsh and abusive parenting.
Methodological Issues
An important consideration in reflecting on the extant research in this area involves both sampling and design issues. In terms of sampling, prior research has investigated PCA risk in expectant parents (Florsheim et al., 2012) as these populations represent ideal prevention targets. Because maltreatment is more prevalent in children under age 1 (DHHS, 2017), many prevention programs intentionally identify at-risk pregnant (e.g., Bugental et al., 2010; Pajer et al., 2014) and perinatal mothers (Duggan et al., 2004; Peacock, Konrad, Watson, Nickel, & Muhajarine, 2013). Moreover, we continue to need to investigate how fathers’ intergenerational PCA transmission unfolds given the traditional research attention on mothers, although fathers may demonstrate similar PCA risk profiles (Rodriguez, Smith, & Silvia, 2016a, 2016b; Slep & O’Leary, 2007). Overlooking fathers is particularly unfortunate given that fathers and father figures represent nearly half of the physical abuse cases (DHHS, 2017; Sedlak et al., 2010).
In terms of design issues, although researchers often approximate variables of interest with single measures that may only modestly represent a construct of interest, theoretically based multiple-indicator approaches demonstrate advantages (Little, Lindenberger, & Nesselroade, 1999). One measure of an independent variable may evidence psychometric weaknesses as well as conceptual or item overlap with the measure of the dependent variable, but such limitations can be offset by including multiple measures that balance each other and minimize overlap. In addition, researchers often rely on child abuse reporting systems—which are subject to high false negatives—or on self-reports alone to measure constructs, which are subject to reporting biases. Constructs like PCA risk and its predictors are vulnerable to such response distortions, which can be addressed by including more covert measures such as analog tasks that are more resistant to participant response manipulation (DeGarmo, Reid, & Knutson, 2006).
Finally, methodological questions have been posed regarding research on the intergenerational transmission of harsh and abusive parenting. One review of 200 studies of the physical abuse cycle observed a number of methodological study limitations (Ertem, Leventhal, & Dobbs, 2000). As reviewed above, research findings on mediators and moderators have been conflicting. Further, whether the effects of a mediator or moderator between reported history of harsh and abusive parenting and PCA risk can be demonstrated across time remains unclear. Prior research investigating potential mediation or moderation has adopted cross-sectional designs (e.g., Bower-Russa, 2005; Milner et al., 2010; Smith, Cross, Winkler, Jovanovic, & Bradley, 2014) or longitudinal designs that either assess the proposed mediator/moderator at a single time point (e.g., Appleyard et al., 2011; Berlin et al., 2011; Chung et al., 2009; Herrenkohl, Klika et al., 2013; Schofield et al., 2016) or collapsed across time points (e.g., Dixon et al., 2005a, 2005b, 2009; Pears & Capaldi, 2001). Consequently, the current research does not clarify whether a given mediator or moderator operates consistently at multiple time points.
Current Investigation
The current study thus examined potential mediators and moderators between personal history of physical and psychological aggression and mothers’ and fathers’ own PCA risk across time. Using a longitudinal multimethod design, mothers and fathers reported on their personal experience of physical and psychological aggression at the first time point and their PCA risk across three time points. For the first research question, a multiple-mediational model (see Figure 1) was considered: Greater maladaptive current functioning (mental health, substance use problems, and intimate partner violence—”taxes”), attitudes approving of PCA, more negative child attributions, less knowledge of nonphysical discipline alternatives, and greater child compliance expectations may mediate the relationship between parents’ personal history and their PCA risk, operating in parallel across time. For the second research question, we considered moderator models for four possible resources parents may draw upon to reduce the effects of personal history of harsh and abusive parenting on their own PCA risk: coping skills, couple satisfaction, emotion regulation, and social support satisfaction. Each resource was considered individually for mothers and fathers to identify specific potential targets for prevention/intervention.
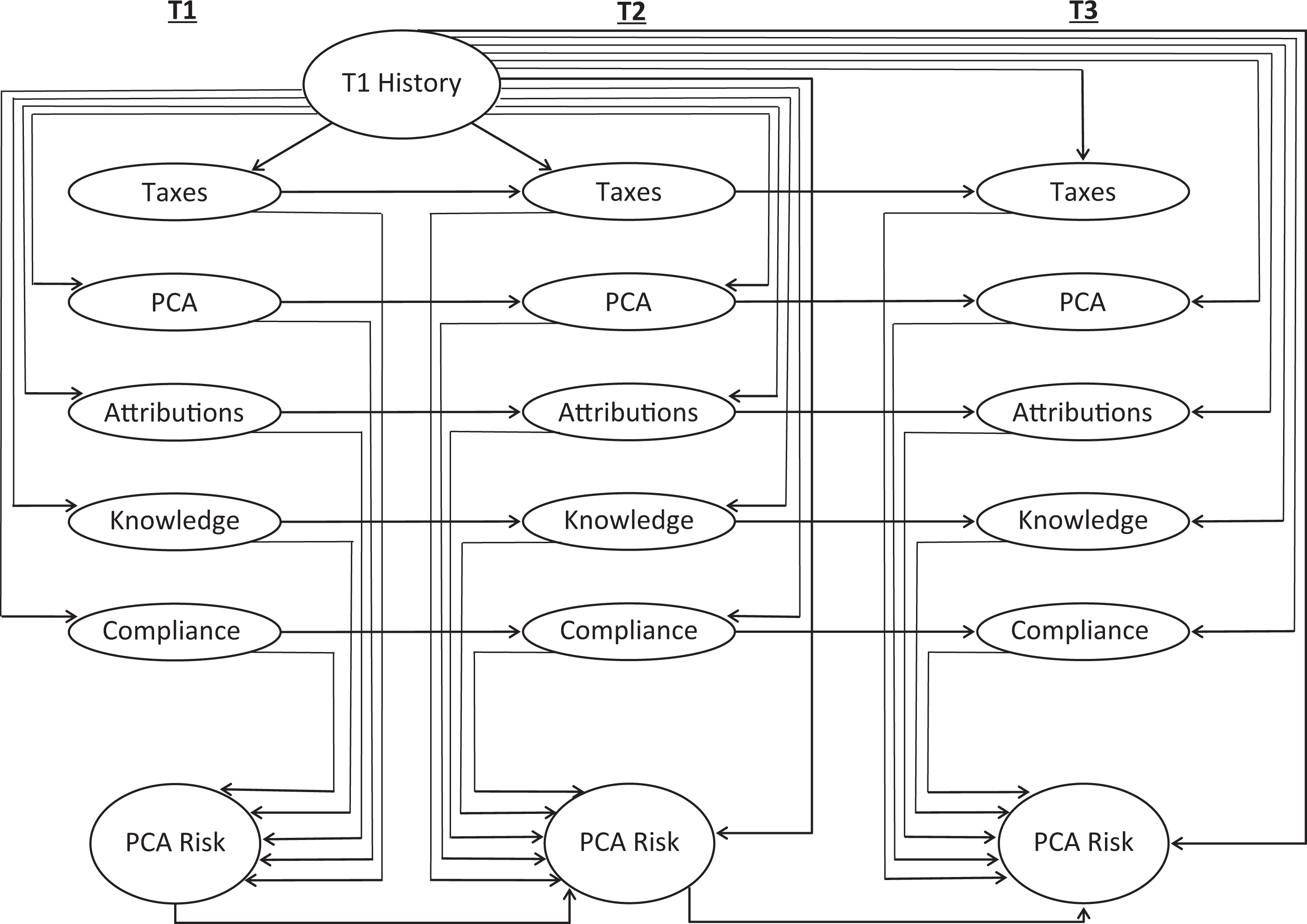
Proposed multiple mediation model.
Method
Participants
The sample included families enrolled in a prospective longitudinal study, the “Following First Families” (Triple-F) Study, which tracked the emergence of PCA risk in first-time families. Triple-F oversampled for sociodemographic risk in a large urban city in the Southeast. At Time 1, 203 primiparous women and 151 of their male partners (86% of fathers who were available to participate) were enrolled in the last trimester of the mother’s pregnancy. For Time 2, families were reassessed when the child was 6 months old (±2 weeks), and at Time 3, families were reassessed when the child was 18 months old (±3 weeks).
In two families, the baby died shortly after birth; thus, the family was not eligible to continue in Triple-F. Of the remaining 201 mothers, 186 participated in Time 2 and 180 at Time 3. Triple-F also permits “fathers” to change during the course of the study because mothers change partners, and thus, the child would have a new father figure (this allows for a more realistic assessment of the family for the larger study). Although we involved 146 fathers at both Time 2 and Time 3, only the same father from Time 1 was eligible for the current analysis, resulting in 140 fathers at Time 2 and 141 fathers at Time 3. Data missing at a given time point for either mothers or fathers were estimated (see Analytic Plan section).
Mothers were on average 26.04 years old at Time 1 (SD = 5.87) and fathers were on average 28.87 years old (SD = 6.10). Mothers reported racial and ethnic identity as 50.7% Caucasian, 46.8% African American, 1% Asian, and 1.5% Native American; of these, 3% also identified as Hispanic/Latina and 5.5% identified as biracial. For fathers, racial and ethnic identity was reported as follows: 54% Caucasian, 45.3% African American, 0.7% Asian; additionally, of these, 4% identified as Hispanic/Latino and 4.7% identified as biracial. Mothers reported on their highest educational level as 30.3% high school or less, 20.9% some college or vocational training, 21.4% college degree, and 27.4% beyond college degree. For father’s highest educational level: 25.3% high school or less, 24.7% some college or vocational training, 27.3% college degree, and 22.7% beyond college degree. Of the sample, 74% of mothers were living with the father of the child. Over 42% of mothers were receiving public assistance, with 49.3% within 150% of the federal poverty line; over half reported an annual household income under US$40,000. At Time 1, 53.2% of mothers evidenced sociodemographic risk, meeting at least one of the following criteria: (a) receipt of public assistance, (b) 150% below the poverty line, (c) high school education or less, and (4) age 18 or younger.
Measures
See Table 1 for measures for each construct (see Rodriguez Silvia & Gaskin, 2017 for further details). Internal consistencies' ranges for measures across time, for mothers and fathers separately, appear in Table 2.
Measures by Construct.
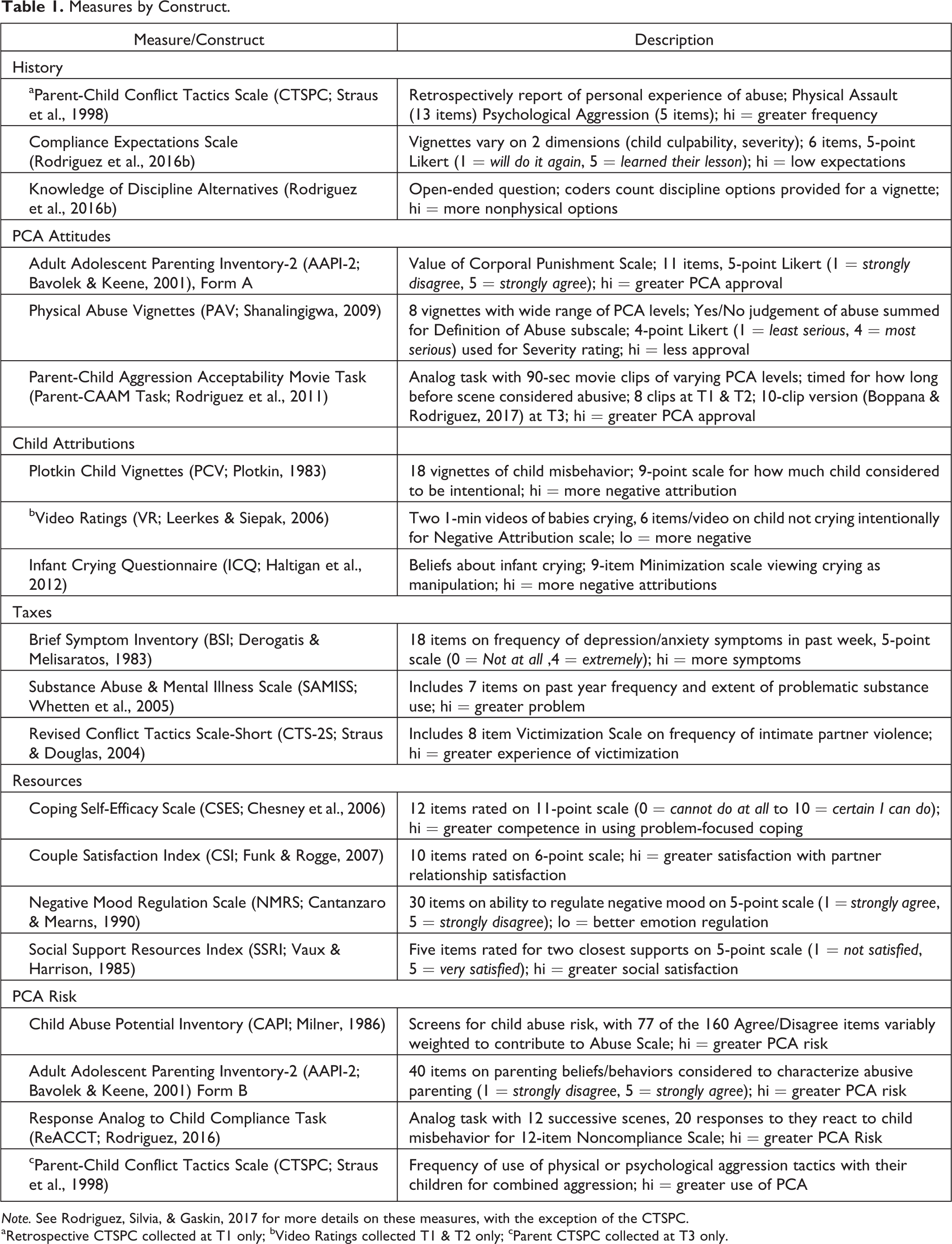
Note. See Rodriguez, Silvia, & Gaskin, 2017 for more details on these measures, with the exception of the CTSPC.
aRetrospective CTSPC collected at T1 only; bVideo Ratings collected T1 & T2 only; cParent CTSPC collected at T3 only.
Means, Standard Deviations, and Internal Consistencies for Mothers and Fathers by Time Point.
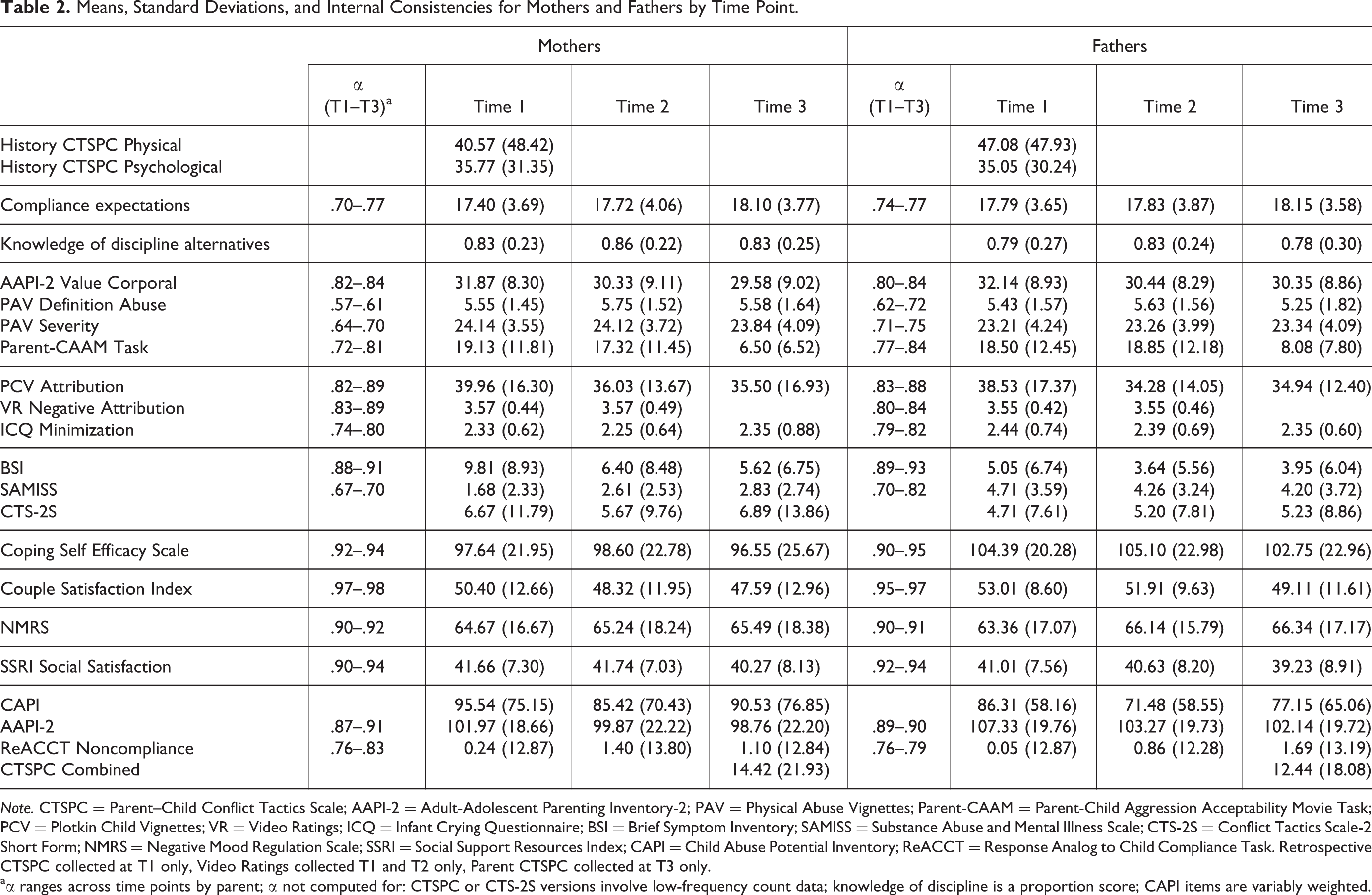
Note. CTSPC = Parent–Child Conflict Tactics Scale; AAPI-2 = Adult-Adolescent Parenting Inventory-2; PAV = Physical Abuse Vignettes; Parent-CAAM = Parent-Child Aggression Acceptability Movie Task; PCV = Plotkin Child Vignettes; VR = Video Ratings; ICQ = Infant Crying Questionnaire; BSI = Brief Symptom Inventory; SAMISS = Substance Abuse and Mental Illness Scale; CTS-2S = Conflict Tactics Scale-2 Short Form; NMRS = Negative Mood Regulation Scale; SSRI = Social Support Resources Index; CAPI = Child Abuse Potential Inventory; ReACCT = Response Analog to Child Compliance Task. Retrospective CTSPC collected at T1 only, Video Ratings collected T1 and T2 only, Parent CTSPC collected at T3 only.
aα ranges across time points by parent; α not computed for: CTSPC or CTS-2S versions involve low-frequency count data; knowledge of discipline is a proportion score; CAPI items are variably weighted.
Procedures
Families were recruited with flyers distributed at local hospitals’ obstetric/gynecological clinics and affiliated childbirth courses. To enroll in the study, at Time 1, primiparous expectant mothers in the final trimester of their pregnancy who were interested in participating contacted the lab to arrange a 2- to 2½-hr session; whenever available, their partners were also scheduled. At Time 2 and Time 3, 3-hr sessions were scheduled. Mothers completed their protocol in a separate, private area independently of their partner. Participants entered all responses on laptop computers while wearing headphones. The full longitudinal study was approved by the university’s institutional review board.
Results
Analytic Plan
All models were estimated with Mplus 8, using full information maximum likelihood estimation with robust standard errors to accommodate missing values for a given time point. The multiple-mediation model depicted in Figure 1 was evaluated for mothers and fathers separately; the moderator models considered each proposed moderator (coping efficacy, couple satisfaction, emotion regulation, and social satisfaction) individually, separately for mothers and fathers. For Figure 1, consistent with prior work with these data (Rodriguez et al., 2016a, 2016b, 2017), composite scores were created by standardizing each variable and averaging the standardized scores. Composite scores were based on the following measures: PCA risk (Child Abuse Potential Inventory [CAPI] Abuse Scale, Adult Adolescent Parenting Inventory-2 [AAPI-2] Total, Response Analog to Child Compliance Task Noncompliance, and Parent–Child Conflict Tactics Scale [CTSPC] Combined Aggression), personal history (Retrospective CTSPC Physical Assault and Psychological Aggression), PCA approval attitudes (AAPI-2 Corporal Punishment Scale, Physical Abuse Vignettes [PAV] Definition of Abuse, PAV Severity Rating, and Parent Child Aggression Acceptability Movie Task), negative attributions (Plotkin Child Vignettes Attribution, Video Ratings Negative Attribution Total, and Infant Crying Questionnaire Minimize Total), and taxes (Brief Symptom Inventory Total, Revised Conflict Tactics Scale-Short Victimization Total, and Substance Abuse and Mental Illness Scale Total). Knowledge of Nonphysical Discipline Alternatives and Compliance Expectations were single scores. Indirect effects in the mediation path models were tested using bias-corrected bootstrapping (with 2,000 samples) to estimate 95% confidence intervals (CIs). CIs are not necessarily symmetric, and indirect effects are considered significant if the CI excludes zero. For tests of moderation, multiplicative interaction terms for each proposed moderator were entered into the models.
Preliminary Analyses
Table 2 presents sample means and standard deviations, separately for mothers and fathers, by time point. The observed sample mean CAPI Abuse Scale scores and AAPI-2 Total scores were within normal limits. Given the complexity of the models, path models were not estimated with demographic covariates; prior work with these data has also demonstrated no differences in path models predicting PCA risk when including demographic characteristics (Rodriguez et al., 2016a, 2016b, 2017).
Research Question 1: Mediation
Results for the multiple mediation model (Figure 1) for mothers are presented in Table 3. In Block 1 of Table 3, for the path coefficients directly to PCA risk: whereas personal history and all proposed mediators had significant coefficients at Time 1, by Time 2, only knowledge of nonphysical discipline alternatives and negative attributions were significant; by Time 3, PCA approval attitudes and personal taxes return to significantly predicting PCA risk. Note that personal history predicted PCA risk at Time 1 but appears to disappear when their child is an infant, returning to only a trend level by Time 3. Block 2 displays the paths from personal history to the proposed mediators, indicating that, although personal history is significantly related with all but negative child attributions at Time 1, these effects disappear at Time 2, although personal taxes reemerges as significant by Time 3. Block 3 conveys stability in the lagged constructs across time. Most importantly, Block 4 presents the indirect effects from personal history to PCA risk through each proposed mediator. In Time 1, greater knowledge of nonphysical discipline alternatives, favorable PCA attitudes, and heightened personal taxes were significant indirect effects accounting for the relationship between expectant mothers’ personal history of PCA and their PCA risk; but by Time 2, these effects have faded, and by Time 3, only the indirect effect through personal taxes even approaches significance. Thus, although some of the proposed mediators demonstrated significant indirect effects initially, the indirect effects were not observed across time.
Standardized Coefficients With Confidence Intervals for Mothers’ Mediation Model.
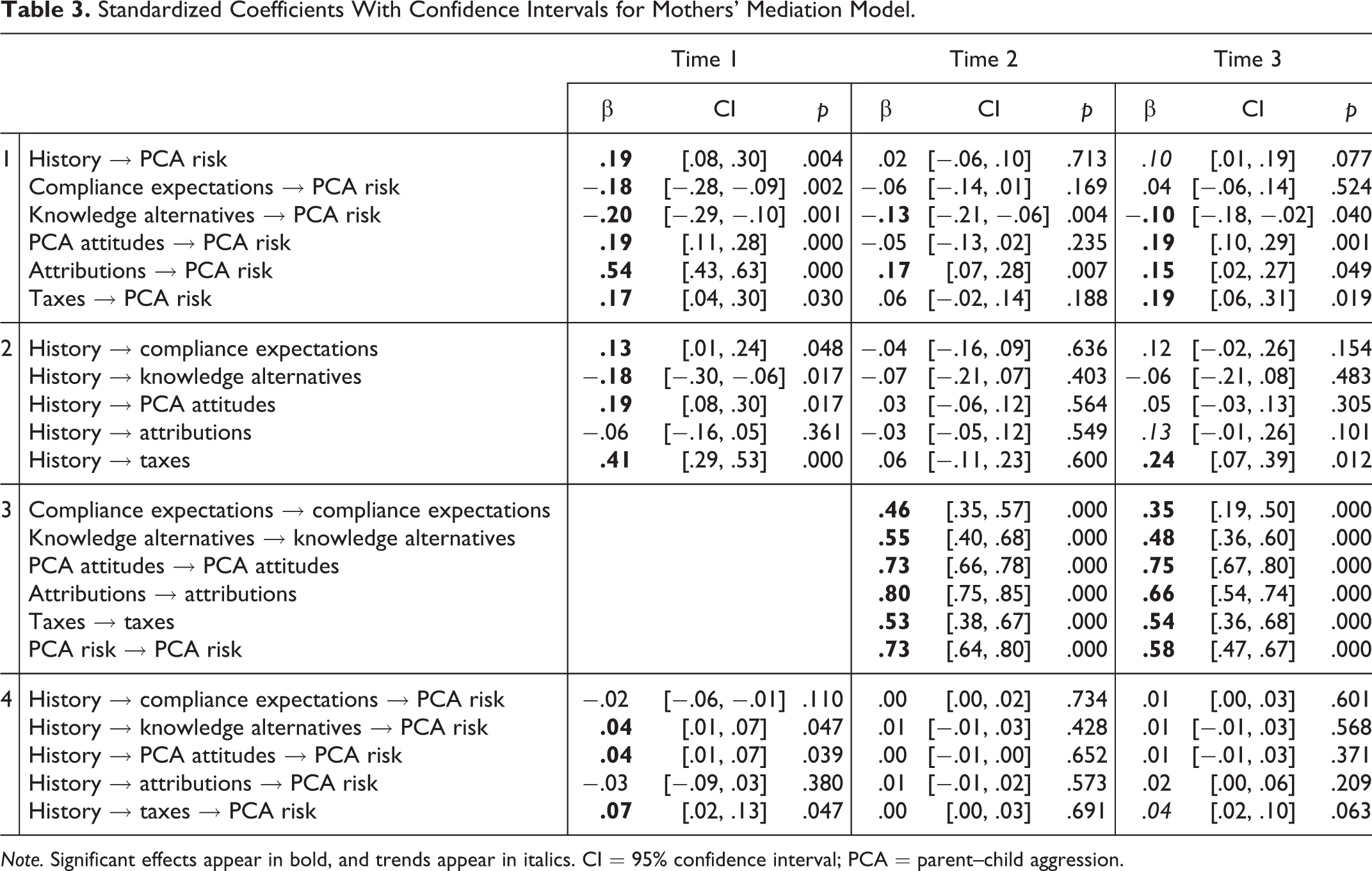
Note. Significant effects appear in bold, and trends appear in italics. CI = 95% confidence interval; PCA = parent–child aggression.
The multiple mediation model for fathers appears in Table 4. In Block 1, note fathers’ personal history, when including all the potential mediators, does not significantly directly predict PCA risk until Time 3; compliance expectations predict expectant fathers’ PCA risk at Time 1, but PCA approval attitudes and negative child attributions predict PCA risk at both Time 1 and Time 3. The effects in Block 2 suggest personal history is related to knowledge of nonphysical discipline alternatives, approval of PCA, and greater personal taxes at Time 1, but these effects disappear by Time 2. Thus, although personal history begins to predict PCA risk by Time 3, no indirect effects through the proposed mediators are observed in the Block 4 section with the exception that PCA approval attitudes at Time 1 indirectly links personal history with PCA risk.
Standardized Coefficients With Confidence Intervals for Fathers’ Mediation Model.
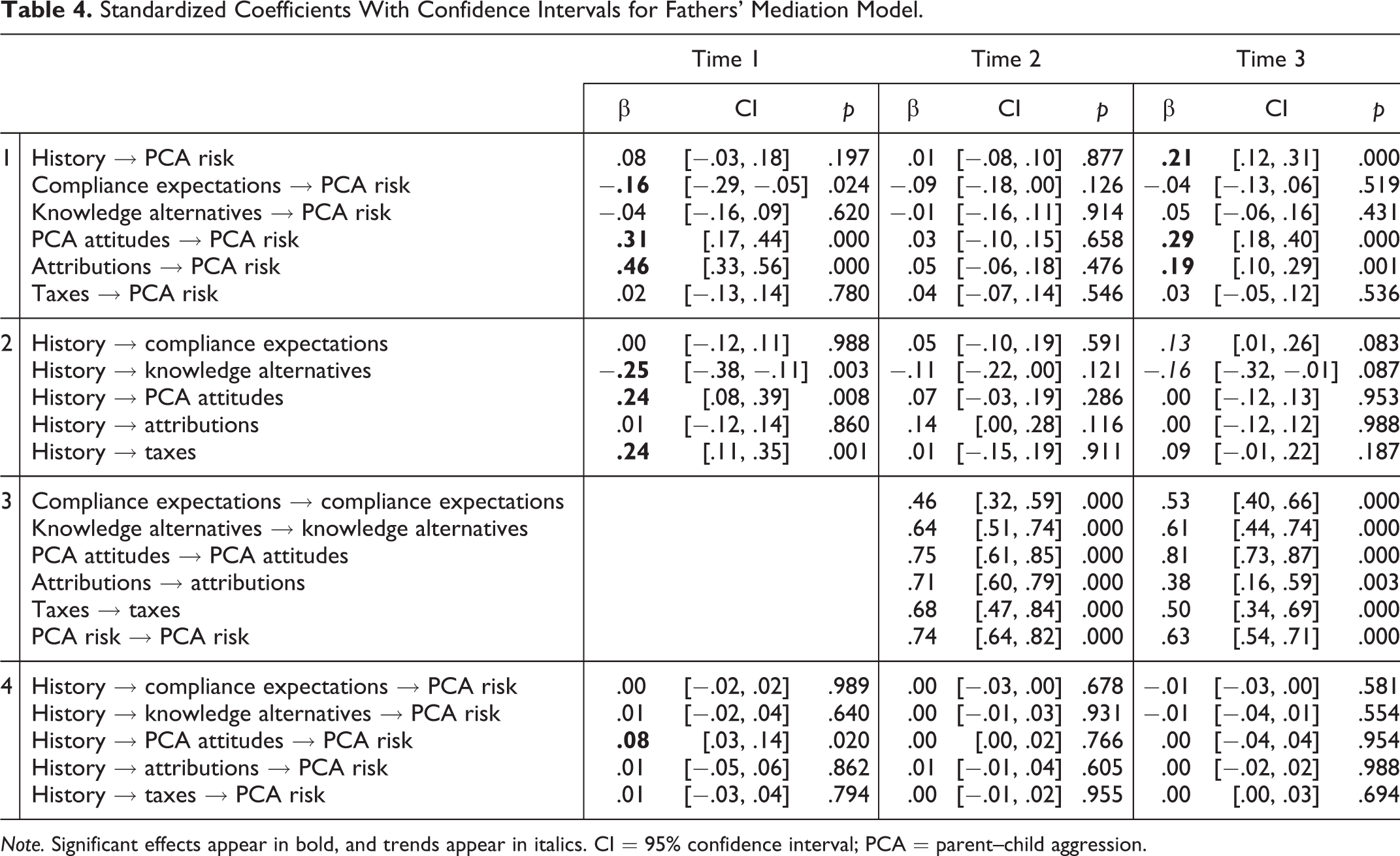
Note. Significant effects appear in bold, and trends appear in italics. CI = 95% confidence interval; PCA = parent–child aggression.
Research Question 2: Moderation
Table 5 displays the results from the proposed four moderators for both mothers (top) and fathers (bottom). First, note that history significantly predicted PCA risk at Time 1 and Time 3. For mothers, increased sense of effective problem-solving coping skills reduced the effect of personal history on PCA risk at Time 1; however, although coping skills were still predictive of PCA risk at Time 2, coping skills did not moderate personal history past Time 1. Greater partner satisfaction in mothers predicted lower Time 1 PCA risk and Time 3 PCA risk; in addition, couple satisfaction buffered the effect of personal history at Time 1 and Time 2 but not at Time 3. Mothers with better emotion regulation demonstrated lower PCA risk, but only a trend-level moderation was observed at Time 1. Finally, although mothers’ greater social satisfaction predicted lower PCA risk at Time 1 and Time 3, social support was only a marginal moderator at Time 1. Therefore, couple satisfaction appeared to be the best moderator for mothers.
History Effects on PCA Risk by Resources for Mothers (Top) and Fathers (Bottom).
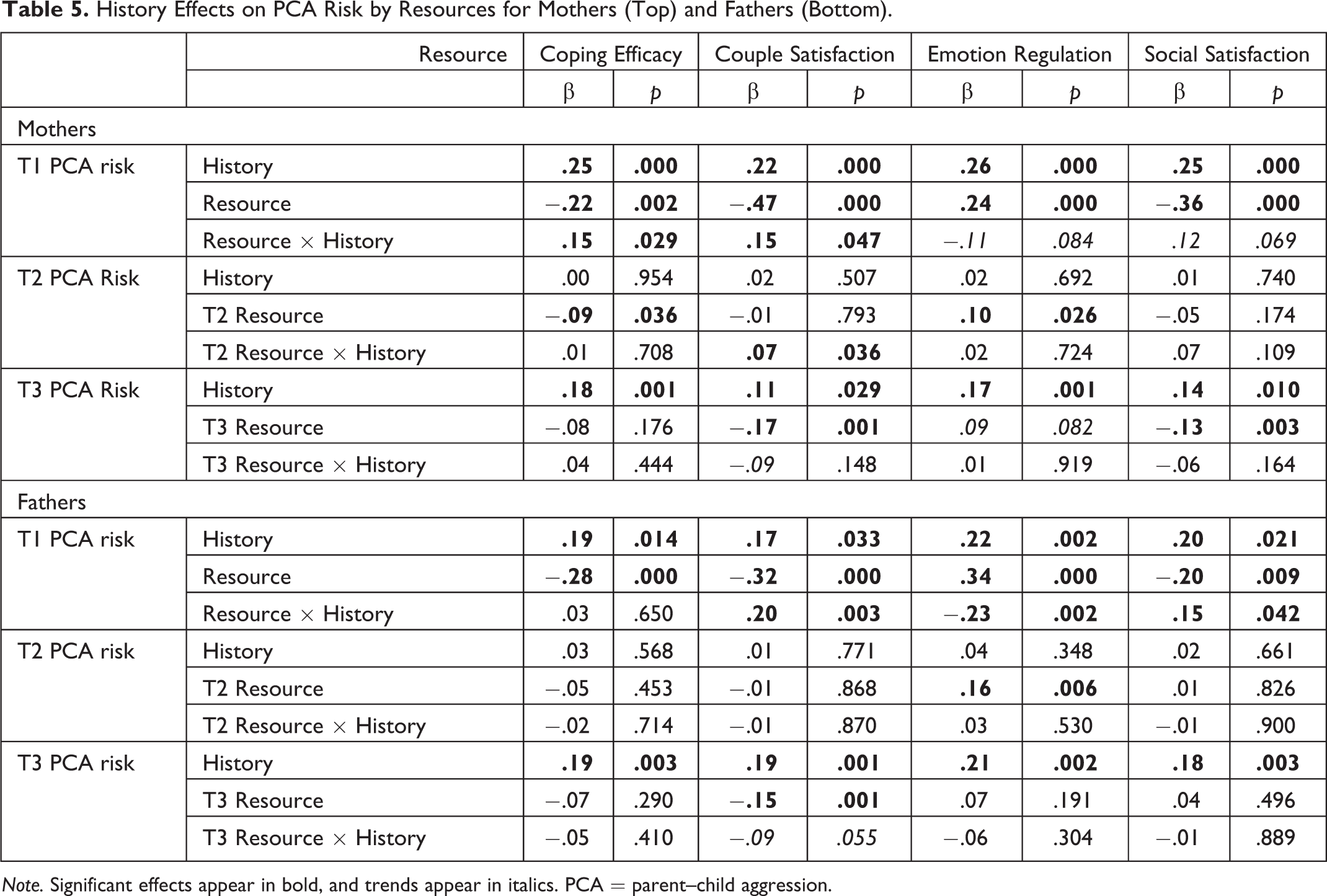
Note. Significant effects appear in bold, and trends appear in italics. PCA = parent–child aggression.
For fathers’ moderation models (bottom of Table 5), note that personal history of harsh and abusive parenting predicted paternal PCA risk only at Time 1 and Time 3. Greater problem-focused coping skills predicted lower Time 1 PCA risk, but moderation of the effect of personal history on PCA risk was not observed at any time point. However, fathers’ greater couple satisfaction predicted Time 1 and Time 3 PCA risk and buffered the effects of personal history on PCA risk at Time 1, but these moderation effects were not apparent at Time 2 and became marginal at Time 3. Better emotion regulation abilities also predicted PCA risk at Time 1 and Time 2 and buffered the effect of personal history on PCA risk at Time 1, but moderation had faded by Time 2. Social support was a significant predictor of and moderator for PCA risk only at Time 1. Consequently, couple satisfaction, emotion regulation, and social support were initial moderators of personal history on PCA risk, but such moderation was not sustained.
Discussion
The current study investigated mechanisms that may account for, or buffer, the connection between parents’ personal history of harsh and abusive parenting and their PCA risk. Present findings indicate that, for both mothers and fathers, a history of physical and psychological aggression predicted PCA risk prenatally as well as when their children were toddlers. With regard to the first research question using the multiple-mediation model, mothers’ knowledge of nonphysical discipline alternatives, PCA approval attitudes, and maladaptive current functioning (mental health and substance use problems, and intimate partner violence—“taxes”) mediated the relationship between personal history and PCA risk only prenatally. In contrast, for fathers, mediation was only observed for PCA approval attitudes prenatally. For the second research question, mothers’ problem-focused coping and couple satisfaction significantly buffered the effect of personal history only on prenatal PCA risk. For fathers, couple satisfaction, emotion regulation, and social satisfaction moderated the effect of personal history only on prenatal PCA risk.
Current findings on the relationship between personal history of physical and psychological aggression and PCA risk partly mirror past research documenting a cycle of intergenerational abusive or harsh parenting (Bailey et al., 2009; Bartlett et al., 2017; Bert et al., 2009). But as seen in Table 2, the effects of such personal history were only observed prenatally and at toddlerhood, for both mothers and fathers, not when their infants were 6 months—namely, immediately after the transition to parenthood. Such a pattern indicates one’s personal history of harsh and abusive parenting may exert more influence on PCA risk at different stages, perhaps reflecting developmental shifts in parenting demands (Bornstein, 2005). Future research could consider whether a parent’s personal history is more salient in certain developmental periods by tracking PCA risk as children get older. Potentially, parents may draw more upon their own history when expecting their baby (given no other reference point other than their own upbringing) and then again when confronted with the more demanding behavior of mobile, more defiant toddlers—demands less evident in infancy. Alternatively, in the current study, personal history was only assessed prenatally, given that history was deemed to be a time-invariant variable. Perhaps the findings would differ with repeated assessments of history—which would likely reflect changing perceptions about one’s past experience of physical and psychological aggression. Although repeated assessments of personal history might have altered our results, prior research suggests only moderate stability in reports of physical abuse (r = .51) across 3 years (Fergusson, Horwood, & Boden, 2011). Further, discrepancies in the source of reports regarding history of physical abuse in particular have raised doubts regarding its intergenerational transmission (Widom et al., 2015 that). Fundamentally, researchers must evaluate whether the perception of one’s history is the process that gets activated when a parent is engaging in a physical discipline encounter that could escalate to abuse or whether it is consistent, and confirmed, experiences of past abuse and PCA that are more critical for intergenerational transmission.
With regard to mediation, greater compliance expectations, less knowledge of nonphysical discipline alternatives, stronger PCA approval attitudes, and worse “taxes” were related to mothers’ personal history of physical and psychological aggression, and all but compliance expectations were significant mediators prenatally. However, mothers’ negative child attributions were unrelated and did not mediate personal history, which is inconsistent with past research that collapsed attributions across two time points (e.g., Dixon et al., 2005a). In contrast, personal vulnerabilities that might tax mothers’ abilities may reappear as a mediator, as suggested by trends at the last time point, but these effects would be weak—consistent with the mixed findings supporting the role of such taxes as a mediator in mothers’ intergenerational transmission (Appleyard et al., 2011; Dixon et al., 2005b). Relative to mothers, fathers’ personal history was only related to less knowledge of nonphysical discipline alternatives and greater PCA approval attitudes prenatally, with only PCA approval attitudes serving as a significant mediator between personal history and PCA risk. Past research has also identified approval attitudes as weak mediators of personal history and harsh parenting (Simons et al., 1991), which was observed in the current study for both mothers and fathers prenatally. The proposed mediators appear to have more of a role in accounting for the relationship between mothers’ history and PCA risk than for fathers. Future research should contemplate alternative mediators that may account for fathers’ intergenerational transmission of PCA. However, no mediation was observed consistently for either mothers or fathers after their initial assessment. Compared to prior work, we assessed mediators at each time point because such variables are not viewed as time-invariant. This pattern again raises questions about the frequency with which parents’ history must be assessed to detect mediation coupled with questions regarding prior studies’ use of single assessments of potential mediators.
For moderation, mothers’ problem-focused coping skills and higher couple satisfaction prenatally buffered the negative effects of personal history on PCA risk. Better emotion regulation and greater social satisfaction were marginal, not significant, moderators of mothers’ history on prenatal PCA risk, contrary to expectations. By contrast, fathers’ higher couple satisfaction, stronger negative emotion regulation, and greater social satisfaction significantly mitigated the effects of history on prenatal PCA risk. Interestingly, higher couple satisfaction was a significant moderator for both mothers’ and fathers’ prenatal PCA risk but only a marginal moderator of their later PCA risk (Time 2 for mothers and Time 3 for fathers), which would suggest weaker effects than past research implicating the protective role of a supportive partner (Schofield et al., 2016). Given potential differences between mothers and fathers, more research is needed to identify which resources mothers and fathers may access to interrupt the intergenerational transmission of harsh and abuse parenting rather than assume that the same resources apply equally. Further, moderation was largely not observed past Time 1. Each moderator was assessed at all three time points because these resources are also not time-invariant in contrast to how they have been studied in prior work. Thus, future research should consider parents’ access to resources across multiple time points to observe how changes in resource levels affect differential trajectories in PCA risk.
Limitations
Despite the current longitudinal design, history of harsh and abusive parenting was assessed once, as previously stated; future work should carefully consider the implications of repeated assessments of personal history. Our findings are also based on both retrospective reports of physical and psychological aggression as well as estimates for their PCA risk and counts of how frequently PCA occurred (CTSPC) rather than substantiated reports of physical or psychological abuse either for parental history or toward their children. Due to disparities in abuse reporting (Widom et al., 2015), research should consider whether the effects of personal history on intergenerational transmission are differentially influenced by confirmed reports of abuse versus self-reports. Additionally, although the design involved three time points, if parenting is influenced by children’s developmental level, following parents into more challenging developmental stages (e.g., preschool) could clarify whether personal history becomes more critical in affecting PCA risk with increasing demands. Moreover, selected mediators reflected individual-level factors consistent with SIP theory, and moderators were identified from current resilience literature. However, other unidentified mediators (e.g., community and social norms and other individual-level factors) may also be relevant to mothers’ and fathers’ intergenerational transmission. Also note that the protective factors we considered “taxes,” such as intimate partner violence, psychopathology, and substance use, could also represent moderators that exacerbate personal history and that some moderators (e.g., coping skills, emotion regulation) could act as mediators—an alternative direction for future studies. Further, the present study utilized multiple measures to assess most mediators, but moderators were each assessed with one measure; future research could adopt more comprehensive assessments of both mediators and moderators. Physical and psychological aggression were also collapsed for both history and PCA risk because of high concordance, as has been previously observed (Bifulco et al., 2002; Miller-Perrin et al., 2009); however, future research could consider differential intergenerational processes between physical and psychological abuse as well as considering the potential role of history of sexual abuse and neglect on intergenerational transmission. Finally, although a socioeconomically and racially diverse sample was recruited, a notably smaller proportion were Hispanic.
Implications
In general, our findings echo past research suggesting a connection between personal history of harsh and abusive parenting and use of PCA (Bartlett et al., 2017; Berlin et al., 2011; Thornberry & Henry, 2013). Given that coping strategies and types of supports often differ by gender as parents transition into parenthood (Alexander, Feeney, Hohaus, & Noller, 2001), understanding which resources are most important for mothers versus fathers remains an important area for future inquiry. Further, although fathers account for a high proportion of the harshest PCA (DHHS, 2017; Sedlak et al., 2010), they are often ignored in PCA research and prevention efforts (Lee, Bellamy, & Guterman, 2009). Additional research is needed on how both mothers and fathers initiate active coping strategies to deal with parenting challenges along adaptive, nonaggressive avenues.
Yet our findings raise questions about our current knowledge of the potential mediators and moderators given some methodological differences from the extant literature. Given the scope of PCA in the United States, more rigorous research is needed to further clarify what contributes to and disrupts the cycle of PCA—including whether different factors emerge as more salient at varying developmental stages. Although current findings support some potential mediators and moderators, the need to identify more sustained risk factors and resiliencies in the intergenerational transmission of harsh and abusive parenting—implementing robust research designs—remains critical.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development or the National Institutes of Health.
Acknowledgment
The authors would like to thank their participating families and participating obstetrics/gynecology clinics that facilitated recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by award number R15HD071431 from the National Institute of Child Health and Human Development.