
Abstract
It is not uncommon for caregivers and adolescents to provide different perspectives of adolescents’ mental health symptoms; however, few studies have examined these discrepancies, especially between foster parents and adolescents in the child welfare system. The goal of this study was to investigate the levels of disagreement on adolescent mental health symptoms among caregivers and adolescents in foster care, to examine factors associated with caregiver–adolescent discrepancies, and the potential moderating role of caregiver–child closeness on the link between the length of time the youth lived with caregivers and discrepancies regarding adolescent mental health symptoms. These research questions were examined using two measures of adolescent–caregiver disagreement, intraclass correlations and discrepancy scores, using data from a nationally representative study of youth involved with the child welfare system. Analyses of 183 adolescent–caregiver dyads revealed caregiver–adolescent disagreement on adolescents’ internalizing and externalizing symptoms, with caregivers reporting higher levels of adolescents’ problems on average. Adolescent gender, type of maltreatment experienced, and placement type were associated with caregiver–adolescent discrepancies. Results also indicated that closeness with caregivers significantly moderated the relationship between the length of time adolescents lived with their caregivers and discrepancies on adolescent externalizing symptoms.
Adolescents involved with the child welfare system have a high prevalence of mental health concerns (Landsverk, Burns, Stambaugh, & Rolls Reutz, 2006); however, the level of reported mental health symptoms may differ depending upon who is asked. Indeed, research demonstrates discrepancies between caregiver and youth reports of adolescent mental health (De Los Reyes & Kazdin, 2005), and these differences may be clinically meaningful (Lyons, Rawal, Yeh, & Tracy, 2002). Because appraisals of mental health problems can inform important issues ranging from access to services to adolescent mental health outcomes, it is important to gain a better understanding of factors associated with discrepancies, particularly for adolescents in foster care. The purpose of this study, therefore, was to examine the levels of disagreement on adolescent mental health symptoms among caregivers and adolescents in foster care and investigate factors associated with discrepancies.
Research suggests that caregivers can serve as key corroborators of youths’ well-being (e.g., Fisher, Bunn, Jacobs, Moran, & Bifulco, 2011). However, it is common for caregivers and adolescents to disagree about the levels of adolescent internalizing and externalizing symptoms (De Los Reyes & Kazdin, 2005), and there are consequences of such disagreement. Specifically, significant caregiver–adolescent disagreement about adolescent mental health is a risk factor associated with adverse adolescent outcomes such as drug use, school expulsion, early pregnancy, self-harm, need for mental health services, and longer term emotional and behavioral problems (Ferdinand, van der Ende, & Verhulst, 2004). Although research specific to youth in foster care is very limited, findings suggest that discrepancies between caregivers and the adolescents in their care are associated with increased adolescent mental health symptoms over time (McWey, Cui, & Holtrop, 2015) and ultimately the breakdown of foster care placements (Strijker, Oijen, & Knot-Dickscheit, 2011). Given the potential for these negative outcomes, more research is needed on caregiver–adolescent disagreement about adolescent mental health symptoms (Zimmerman & Pogarsky, 2011), particularly for adolescents in foster care.
Studies conducted with samples of caregivers and adolescents among the general population demonstrate that adolescents’ self-reports of their mental health symptoms tend to be higher than their caregivers’ reports of the adolescents’ symptoms (Burk & Laursen, 2010; Petot, Rescorla, & Petot, 2011; Youngstrom, Loeber, & Stouthamer-Loeber, 2000), and findings generally indicate modest agreement (e.g., r = .26–.41) between caregivers and adolescents across studies (Burk & Laursen, 2010; De Los Reyes & Kazdin, 2005). Contrary to findings among caregiver–adolescent dyads in the general population, the limited research specific to child welfare samples demonstrates that caregivers tend to report higher levels of mental health concerns compared to adolescents themselves (McWey et al., 2015; Srtijker et al., 2011). More specifically, in one of only few known studies of caregiver–adolescent disagreement specific to youth in foster care, researchers found significant dissimilarities between caregivers’ and adolescents’ reports of adolescent mental health symptoms using the Child Behavior Checklist (CBCL) and Youth Self-Report (YSR; Achenbach, 1991). Further, higher levels of caregiver–adolescent disagreement on adolescents’ internalizing symptoms predicted increases in the levels of adolescent externalizing symptoms 36 months later (McWey et al., 2015). Similarly, in a study of caregiver–adolescent discrepancies involving a sample of adolescents in foster care in the Netherlands, researchers reported large differences on the Internalizing and Externalizing subscales of the CBCL and YSR among caregiver–adolescent dyads (Srtijker et al., 2011). There was an inverse relationship between agreement and severity of problems, where higher levels of disagreement were associated with more severe problems according to the adolescents (Srtijker et al., 2011). Finally, a study of children ages 4–11 in a foster care in Australia found a low correlation between caregiver and youth agreement on youth internalizing symptoms (Tarren-Sweeney, Hazell, & Carr, 2004). Taken together, extant research specific to families involved with the child welfare system, albeit limited, demonstrates patterns of agreement that differs from what is observed with parent–adolescent dyads among the general population. Because of the clinical significance of discrepancies, it is important to understand factors associated with caregiver–adolescent disagreement (De Los Reyes, 2011; Zimmerman & Pogarsky, 2011).
Research suggests that specific adolescent demographic characteristics may be linked with differences between caregivers’ and adolescents’ perceptions of adolescent mental health symptoms. Specifically, caregivers tend to demonstrate better agreement with younger children (ages 6–11 years) versus older youth (ages 12–19 years; De Los Reyas & Kazdin, 2005). With regard to gender, some findings indicate that caregivers are more likely to report higher levels of internalizing symptoms of females and higher levels of externalizing symptoms of males (Tarren-Sweeney, Hazell, & Carr, 2004), but research specific to dyadic differences specifically is inconclusive (De Los Reyas & Kazdin, 2005). Moreover, the type of maltreatment experienced by the adolescent may also be associated with the perceptions of adolescent mental health. For instance, Tarren-Sweeny (2008) found that caregivers reported higher CBCL scores for children in foster care who were physically or sexually abused compared to other forms of maltreatment. Another study involving adolescents exiting foster care, however, found that although the occurrence of physical abuse, sexual abuse, and physical neglect were associated with reports of internalizing symptoms, only physical abuse was associated with externalizing and internalizing behaviors when controlling for other types of abuse experienced (McMillen et al., 2005). Finally, placement type may also be linked to dyadic differences. Specifically, because youth placed in kinship care may have similar backgrounds, experiences, and a shared family history as their kinship provider, one might expect lower differences in caregiver and youth reports of mental health symptoms compared to youth in other placement types. In light of these mixed findings, and coupled with the limited research examining the extent to which these factors predict discrepancies specifically, we explored the extent to which adolescent age, gender, type of maltreatment experienced by the adolescent, and placement type were related to caregiver–adolescent discrepancies on adolescent internalizing and externalizing symptoms.
While research on determinants of informant discrepancies is limited (De Los Reyes & Kazdin, 2005), the quality of the caregiver–adolescent relationship may be a key factor. Specifically, disagreement about mental health symptoms may be a reflection of low levels of caregiver–adolescent closeness (De Los Reyes & Kazdin, 2005). For instance, using dyadic correlations, researchers found that relationship support was inversely associated with mothers’ and adolescents’ shared view of adolescent internalizing and externalizing symptoms (Burk & Laursen, 2010). Similarly, Burk and Laursen (2010) found that caregiver and youth between-reporter correlations of adolescent behavior problems were significantly and inversely associated with relationship quality. While these findings are specific to caregiver–adolescent dyads in a community sample, the role of the caregiver–adolescent relationship may be particularly germane to youth in foster care. Although not empirically tested, it is presumed that there may be linkages between the length of time an adolescent has resided with their caregiver, relationship closeness, and dyadic agreement; the longer the caregiver and adolescent have lived together, the more time they have had to form a relationship and become attuned to one another, particularly with regard to the more visible types of mental health symptoms (e.g., externalizing problems). Because the caregiver–adolescent relationship may help buffer against the known risks associated with placement in foster care (Oosterman, Schuengle, Wim Slot, Bullens, & Doreleijers, 2007; Withington, Duplock, Burton, Eivers, & Lonne, 2017), it is particularly important to investigate the extent to which relationship closeness moderates the discrepancies between caregivers and adolescents in foster care.
The Present Study
The goal of this study was to investigate the levels of disagreement between caregivers and adolescents on adolescent mental health symptoms and the factors associated with discrepancies within a sample of adolescents in out-of-home (OOH) care. This study involved caregiver–adolescent dyads and both mixed and between-dyad data, necessitating that we employ a standard dyadic design using an idiographic approach (Kenny, Kashy, & Cook, 2006). Specifically, intraclass correlations (ICCs) were calculated to examine aspects of caregiver–adolescent agreement (Youngstrom et al., 2000). Because the ICC could yield negative values, following other researchers, we also computed dyadic discrepancy scores (e.g., Petot et al., 2011; Youngstrom et al., 2000). We hypothesized that there would be discrepancies between caregiver and adolescent reports of both internalizing and externalizing symptoms. Further, we explored whether specific characteristics including adolescent age, gender, the type of maltreatment experienced, and placement type would be associated with the discrepancies between caregiver and adolescent reports of internalizing and externalizing symptoms. Finally, we hypothesized that closeness with caregivers would moderate the relationship between the length of time the adolescent lived with the caregiver and caregiver–adolescent discrepancies on externalizing and internalizing symptoms.
Method
Sample and Procedures
This study utilized data from the National Survey of Child and Adolescent Well-Being (NSCAW). The NSCAW project examined the well-being of a nationally representative sample children and adolescents involved with the child welfare system (National Data Archive on Child Abuse and Neglect [NDACAN], 2002). The target population of the NSCAW study was U.S. children who were subjects of child maltreatment investigations. The project involved a two-step stratified sampling design where the United States was divided into sampling strata from which primary sampling units were created. A random selection scheme was applied, so that the same number of children were selected from each unit (NDACAN, 2002). Then, the data were divided into two mutually exclusive samples of children: Those who were subjects of investigations of abuse or neglect (N = 5,501) but may or may not have been removed from the home and children in “long-term foster care” who were removed from their homes and placed in OOH care for approximately 1 year at the time of data collection (N = 727). Because of the focus of this study, the long-term foster care sample was used and the sample was further restricted to adolescents (N = 183).
The average age of the adolescents in the sample was 13 years (SD = 1.4, range: 11–16) and 52% (n = 95) were males and 48% (n = 88) were females. The racial and ethnic composition of the adolescents included 40% (n = 73) who self-identified as Black, 35% (n = 64) as White, 14% (n = 25) as Hispanic, and 11% (n = 21) as Asian, multiracial, or “Other.” The racial and ethnic composition of the caregivers included 45% (n = 81) White, 40% (n = 74) Black, 9% (n = 17) Hispanic, and 6% (n = 11) Asian, multiracial, or Other. Regarding the relationships of the caregiver to the adolescent, 46% (n = 84) were foster parents, 37% were kin (n = 68), and 16% (n = 31) were “other nonrelatives.” The average length of time adolescents lived with their caregivers was 26.27 months (range of 1–122).
Measures
Caregiver report of internalizing and externalizing symptoms
Caregivers were asked to complete the CBCL (Achenbach, 1991). The Internalizing and Externalizing subscales were used to assess caregivers’ perceptions of adolescents’ mental health symptoms. The Internalizing Symptoms Scale includes 32 items from the Withdrawn (9 items), Anxious/Depressed (14 items), and Somatic Complaints (9 items) Syndrome subscales. The Externalizing scale encompasses 27 items from the Delinquent Behavior (8 items) and Aggressive Behavior (19 items) subscales. Response options range from 0 (not true) to 2 (very true). Higher scores signify higher levels of internalizing and externalizing symptoms. The CBCL is a widely used, psychometrically sound assessment of mental health symptoms (Tarren-Sweeney et al., 2004). Among the NSCAW sample, the internal consistency of the CBCL Internalizing subscale was .80, and the test–retest reliability of the Externalizing subscale was .81 (NDACAN, 2002).
Adolescent report of internalizing and externalizing symptoms
Adolescents were asked to complete the YSR form (Achenbach, 1991). The YSR captures adolescent self-report data that parallel the caregiver report on the CBCL (Achenbach, 1991). As with the CBCL, the Internalizing Scale of the YSR is computed by adding the 32 items comprising the Withdrawn, Anxious/Depressed, and Somatic Complaints Syndrome subscales, and the Externalizing Scale is the sum of 27 items from the Delinquent and Aggressive Behavior subscales. Response options are the same as the CBCL and higher scores indicate greater levels of symptoms. The reported test–retest reliability coefficients of YSR generally range from .72 to .96 (Achenbach, 1991). For the NSCAW sample, the test–retest reliability of the Externalizing subscale was .90 for the Internalizing Symptoms Scale and .81 for the Externalizing Symptoms Scale (NDACAN, 2002).
Closeness with caregiver
Adolescents completed an abbreviated version of the Rochester Assessment Package for Schools–Student. The Emotional Security subscale was used to assess adolescents’ reports of levels of closeness with their current caregiver. The assessment includes 3 items including “When I am with my [caregiver], I feel good” and “When I am with my [caregiver], I feel mad,” with options ranging from 1 (not true at all), 2 (not very true), 3 (sort of true), and 4 (very true). Higher scores indicate higher caregiver relationship quality. For youth in the NSCAW sample, the reported reliability for the Emotional Security subscale ranged from .65 to .76 (Dowd et al., 2006). In this study, the α coefficient was .69.
Other variables
Youth reported their age (in years) and gender (0 = female, 1 = male). Regarding type of maltreatment, in keeping with other longitudinal studies of child abuse and neglect (see English & LONGSCAN Investigators, 1997), NSCAW used a modified form of the Maltreatment Classification Scale (Manly, Cicchetti, & Barnett, 1994), where caseworkers reported the types of maltreatment experienced by the adolescent and, of those, which type was “the most serious” (Rosenthal & Curiel, 2006). Maltreatment categories included neglect, physical abuse, sexual abuse, and “other maltreatment” (e.g., educational maltreatment, emotional maltreatment, or exploitation). The maltreatment experienced by adolescents included neglect (48%, n = 87), followed by other maltreatment (19%, n = 36), physical abuse (17%, n = 31), and sexual abuse (16%, n = 29). Placement type was categorized as foster home, kinship care, and other type. Caseworkers reported the length of time (in months) adolescents lived with their current caregiver. These variables were included in the analytic models.
Plan of Analysis
As a preliminary step, paired t tests were conducted to compare the mean levels of adolescent and caregiver reports on adolescents’ internalizing and externalizing symptoms. To test the hypothesis that there would be disagreement between adolescent and caregiver reports, double entry ICCs were calculated for each dyad. The ICC calculated this way captures scatter, shape, and slope similarity of the profiles and therefore is a preferred approach to examining similarity (Furr, 2010; Petot et al., 2011; Youngstrom et al., 2000). In addition to ICCs, which focus more on agreement, discrepancy scores were calculated for each dyad in order to predict cross-informant discrepancies (Petot et al., 2011; Youngstrom et al., 2000). Standardized discrepancies scores were used rather than raw difference scores because they have the advantage of placing scores on the same metric for comparison (Laird & Weems, 2011).
To examine the role of demographic characteristics in explaining the caregiver–adolescent discrepancies, covariates (i.e., age, gender, type of maltreatment, placement type) were used to predict discrepancies in regression analyses. Finally, the interaction between closeness with caregivers and the length of time adolescents lived with their caregivers was modeled to examine the hypothesized moderating effect of adolescent–caregiver closeness on externalizing and internalizing symptom discrepancy scores. Following Aiken and West (1991), the variables length of time and closeness to caregiver were both centered and the interaction terms were calculated using the centered values.
Results
Preliminary Analyses
Means, standard deviations, and correlations of the variables are provided in Table 1. The correlations between adolescent report and caregiver report on adolescent internalizing symptoms (.26, p < .01) and externalizing symptoms (.37, p < .01) were positive and significant. The moderate sizes of the correlations suggested certain degrees of differences between caregiver and adolescent reports. Results from paired t tests indicated that the average score of internalizing symptoms reported by adolescents (M = 10.5, SD
Descriptive Statistics of and Correlations Among Study Variables.
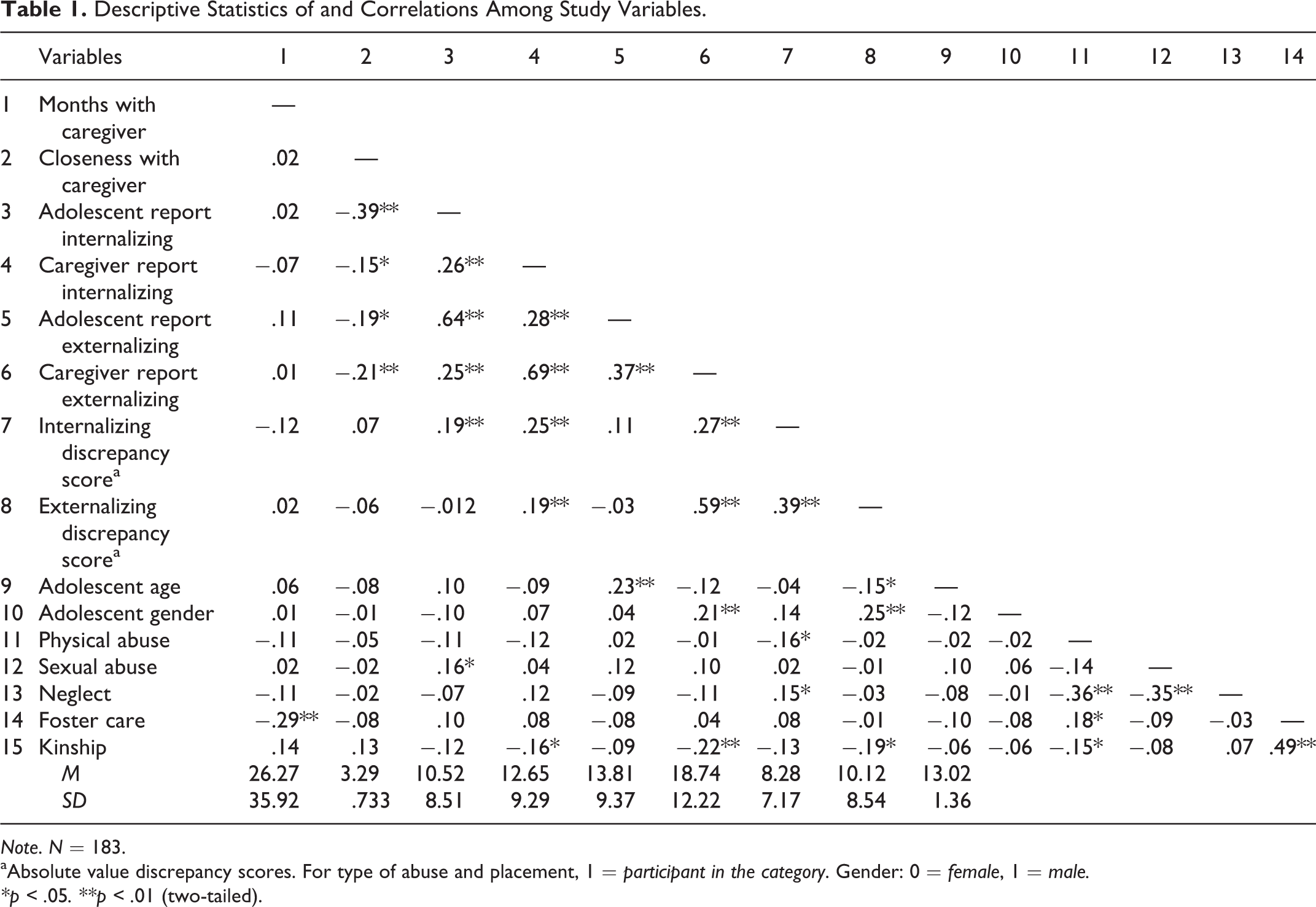
Note. N = 183.
aAbsolute value discrepancy scores. For type of abuse and placement, 1 = participant in the category. Gender: 0 = female, 1 = male.
*p < .05. **p < .01 (two-tailed).
Bivariate correlations with gender also indicated that caregivers reported higher levels of externalizing symptoms for males, and externalizing discrepancy scores were higher for males compared to females. Compared with those who experienced other types of maltreatment, youth who experienced physical abuse had lower internalizing discrepancy scores and youth who experienced neglect tended to have higher internalizing discrepancy scores. Regarding type of placement, youth in kinship placements had lower caregivers’ reports of internalizing symptoms, externalizing symptoms, and externalizing discrepancy scores. Moreover, closeness with caregivers was inversely associated with adolescent report of internalizing and externalizing symptoms and caregiver report of internalizing and externalizing symptoms.
Tests of Disagreement: ICCs and Standardized Discrepancy Scores
To test the hypothesis regarding disagreement between caregivers and adolescents on reports of adolescents internalizing and externalizing symptoms, we first calculated a double entry ICC for each dyad. The average ICC was −.35 (SD = .49) for the Internalizing Scale and −.43 (SD = .59) for the Externalizing Scale. The negative ICC values indicated that adolescents and caregivers differed in their profiles.
Negative ICC values can be confusing, as they may suggest dissimilarity despite similar profile shapes (Furr, 2010). In other words, a negative double entry ICC could be observed even if two profiles are similar in shape. Thus, standardized discrepancies scores were calculated and used in subsequent analyses (Laird & Weems, 2011; Petot et al., 2011; Youngstrom et al., 2000). Specifically, we standardized the caregiver scores and the adolescent scores across the whole sample, then subtracted adolescent standardized scores from caregiver standardized scores (because caregiver scores were higher, on average, than adolescent scores). After obtaining the standardized discrepancy scores, we took the absolute values of the standardized discrepancy scores and conducted a series of analyses to investigate the extent to which demographic characteristics were associated with caregiver–adolescent discrepancies.
Factors Associated With Caregiver–Adolescent Discrepancies
Specifically, adolescent age, gender, type of maltreatment (with “other” as the reference group) and placement type (with “other” as the reference group) were entered in regression models as predictors with absolute values of the standardized discrepancy scores as outcomes. Internalizing and externalizing outcomes were tested in separate models. The results from the two models are presented in Table 2. For the internalizing discrepancy score model, adolescent gender was positively and significantly associated with caregiver–adolescent discrepancies (b = .12, p < .05), suggesting male youth had higher disagreement with caregivers. Adolescents who experienced physical maltreatment reported more agreement with caregivers as compared to those who experienced other maltreatment (b = −.17, p < .05). Finally, youth in kinship care reported more agreement with their kin caregivers as compared to those in other placements (b = −.14, p < .05). For the externalizing discrepancy score model, adolescent gender (b = .19, p < .05) and kinship care (b = −.22, p < .01) suggested a similar pattern of findings.
Standardized Regression Coefficients of Demographic Characteristics on Standardized Difference Scores in Internalizing and Externalizing Symptoms.
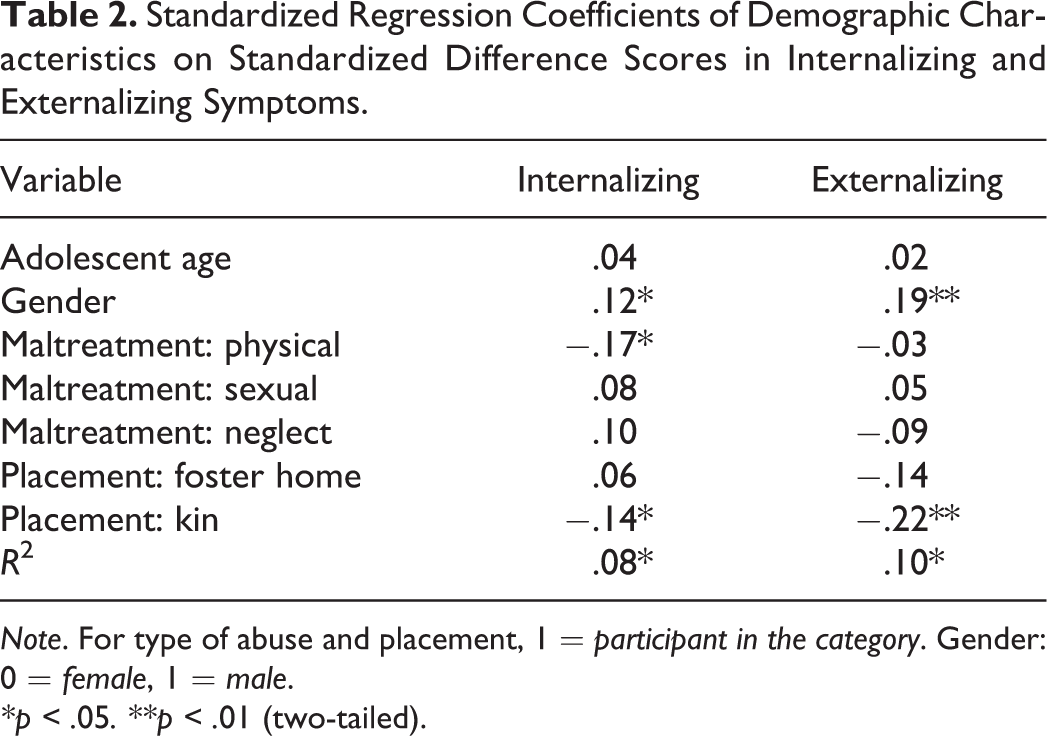
Note. For type of abuse and placement, 1 = participant in the category. Gender: 0 = female, 1 = male.
*p < .05. **p < .01 (two-tailed).
Because the direction of the discrepancy scores may indicate different patterns of disagreement (e.g., a positive discrepancy score indicating a caregiver’s score as higher than the adolescent’s score vs. a negative discrepancy score indicating a higher adolescent score than caregiver score), the discrepancy scores were further split into two groups: those with negative discrepancy scores (adolescent reported higher than caregiver) and those with positive discrepancy scores (caregiver reported higher than adolescent) in order to examine the direction of the relationships for each group. Results from regressions suggested that they did not differ significantly. Thus, we proceed the subsequent analysis with the absolute standardized discrepancy scores.
Moderation Analyses: Closeness With Caregivers
Moderating effects between the length of time the adolescent lived with the caregiver and adolescent reported level of closeness with their caregiver were tested on the absolute value discrepancy scores of internalizing and externalizing symptoms. Length of time, closeness to caregiver, their interaction term, and the covariates adolescent age, gender, type of maltreatment, placement type were included in the models. For externalizing symptoms, results indicated that closeness with caregivers significantly moderated the relationship between length of time with caregivers and discrepancy on externalizing symptoms (b = −.24, p < .01). Figure 1 illustrates the interaction effects. As expected, the longer the time the adolescent had lived with their caregiver, the less disagreement on externalizing symptoms, with this association being significantly stronger for adolescents who reported closer relationships with their caregivers as compared to those with less close relationships with their caregivers. Conversely, when caregivers and adolescents did not have a close relationship, the longer they lived together, the higher the discrepancy on externalizing symptoms. The moderating effect of caregiver–adolescent closeness on discrepancy in internalizing symptoms was not significant (b = −.08, ns).
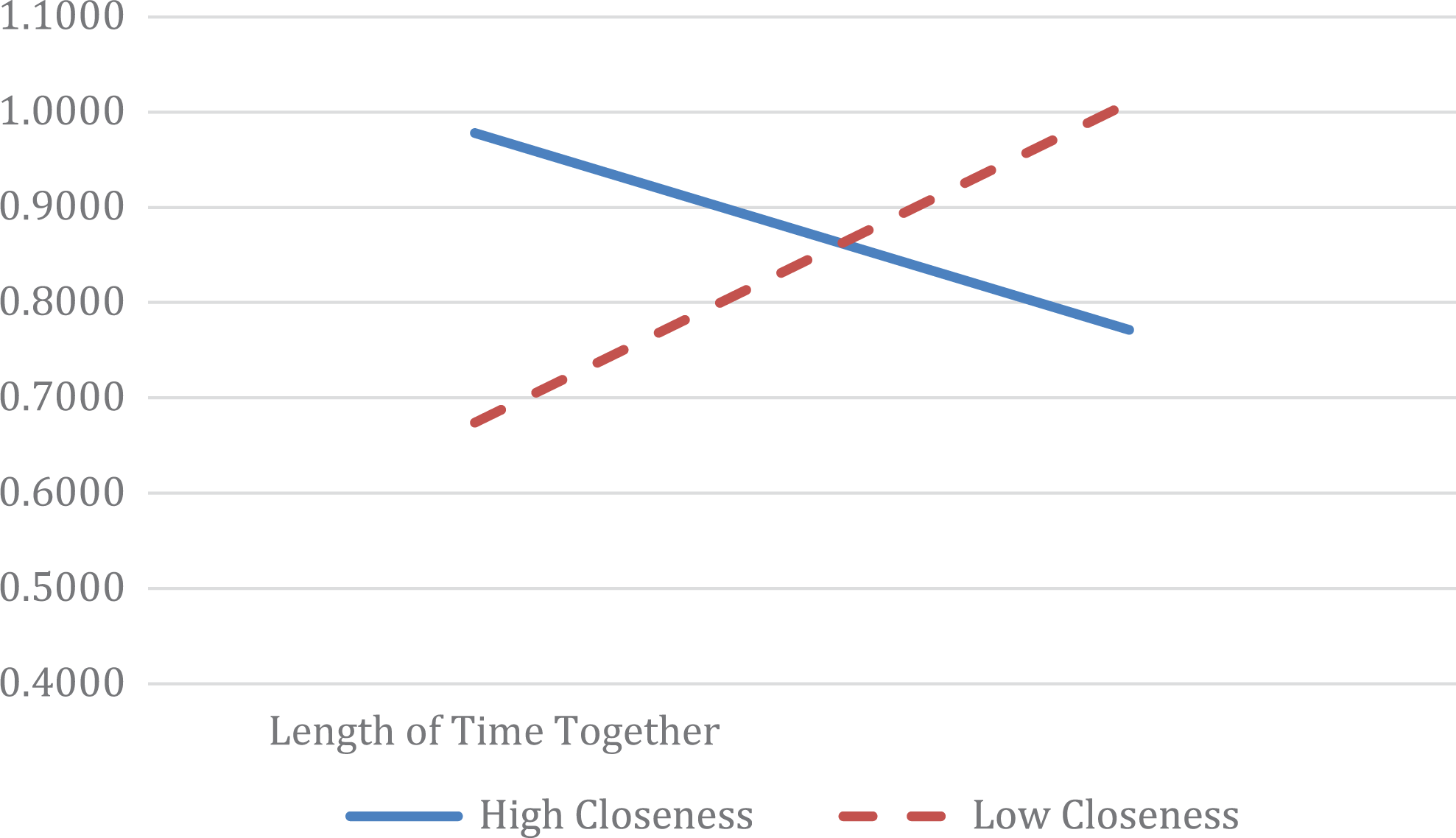
Interaction between length of time together and closeness on externalizing symptoms discrepancy scores.
Discussion
Differences between caregiver and adolescent accounts of adolescent mental health symptoms may be clinically meaningful, especially among caregivers and adolescents in foster care (Burk & Laursen, 2010; Striker, van Oijen, & Knot-Dickscheit, 2011); however, most research does not conduct dyadic analyses of caregivers’ and youths’ reports (Youngstrom et al., 2000). This study involved dyadic analytic techniques to investigate levels of disagreement between caregivers’ and adolescents’ perceptions of adolescents’ internalizing and externalizing symptoms and examined factors associated with discrepancies. Findings from this study extend current knowledge in several key ways.
First, this study adds to the small body of research on caregiver–adolescent disagreement using dyadic data by focusing on a sample of adolescents in foster care. Although studies have found modest agreement between caregivers and adolescents in the general population (Burk & Laursen, 2010; Petot et al., 2011; Youngstrom et al., 2000), few studies have involved higher risk samples. Adolescents in foster care are a distinctive group because they are more likely to be at risk of mental health concerns (Landsverk et al., 2006). As such, disagreement between caregivers and adolescents could be especially important. Studies of caregiver–adolescent disagreement in the general population suggest that caregivers tend to report lower levels of adolescents’ problems than adolescents report themselves (Petot et al., 2011; Youngstrom et al., 2000). Findings from the present study offered a different perspective, perhaps unique to the foster caregiver–adolescent relationship. Specifically, adolescents in foster care in the present study reported significantly lower levels of internalizing and externalizing symptoms compared to their caregivers’ reports.
There are several potential explanations for such differences. For example, it is possible that a caregiver might be aware of the negative mental health outcomes frequently associated with youth in foster care (e.g., McMillen et al., 2005; White, Havalchak, Jackson, O’Brien, & Pecora, 2007) and be highly sensitive to the potential for mental health symptoms to be exhibited by the adolescent. It may also be that caregivers are inadvertently affected by stereotyped beliefs about youth in foster care and expect mental health concerns. These perceptions and expectations, in turn, may result in caregivers systematically overestimating levels of adolescent internalizing and externalizing symptoms. On the other hand, given the link between adolescent behavior problems and the number of foster care placements adolescents experience (Landsverk et al., 2006), adolescents in foster care may underreport symptoms for fear of disrupting their placement stability (Kools, 1997). In fact, past research with a sample of dyads involved in the foster care system has demonstrated that caregiver–adolescent disagreement was inversely associated with adolescent placement stability (Strijker et al., 2011) that may help explain instances when adolescents might underreport symptoms.
Indeed, because such discrepancies are clinically meaningful, some suggest that it is important to move beyond trying to determine which informant is more accurate and to isolate factors associated with such discrepancies (De Los Reyes, 2011; Zimmerman & Pogarsky, 2011). Results of this study also contribute to the literature by indicating that adolescent gender, type of maltreatment, and type of placement were linked with discrepancies in ratings of mental health. Specific to gender, findings demonstrated that discrepancies were higher among dyads with a male adolescent compared with dyads with a female adolescent. These findings differ, somewhat, from the mostly inconclusive results found in other studies (e.g., De Los Reyas & Kazdin, 2005), and these differences may be due to the fact that extant research on predictors of discrepancies is generally not specific to youth in foster care. More research is needed on gender effects; however, findings suggest that it may be important to assess for differences in caregiver–adolescent male reports of mental health symptoms. Although most research on caregiver–adolescent discrepancies has been conducted with community-based samples, we also tested variables specific to the foster care context that are known correlates of mental health symptoms (i.e., type of maltreatment experienced and type of placement). Higher agreement was demonstrated between caregivers and adolescents who experienced physical abuse and between caregivers and youth in kinship care compared to other types of placement. Taken together, findings from the present study indicate that when adolescents in OOH placements present for mental health services, it may be worthwhile to consider the degree to which adolescent gender, type of maltreatment, and placement type are linked with caregivers’ perceptions about the adolescent’s mental health symptoms. Working with caregivers to provide psychoeducation and facilitating caregiver–adolescent dialogues about mental health symptoms may support treatment efforts.
Researchers have suggested that discrepancies may be indicative of caregiver–adolescent relationship closeness (De Los Reyes & Kazdin, 2005), and caregiver–adolescent closeness for youth in foster care arguably has greater potential for relationship quality variability (Dozier & Lindhiem, 2006). Given that positive caregiver–adolescent relationships may help buffer the known risks associated with involvement in the foster care system (Oosterman et al., 2007), it was central to examine the extent to which closeness was linked with discrepancies. It is noteworthy that closeness to caregivers moderated the association between discrepancies on adolescent externalizing but not internalizing symptoms. Indeed, compared to externalizing symptoms, internalizing symptoms are harder for others to observe and adolescents may be less inclined to share feelings of sadness and anxiety with caregivers (Strijker et al., 2011). Although additional research is needed, if discrepancies are indeed reflective of the caregiver–adolescent relationship, systemic interventions may be warranted for adolescents experiencing mental health concerns.
Research has demonstrated that for youth in foster care, mental health may be best supported through interventions that include the caregiver (Landsverk et al., 2006), and various empirically supported intervention options exist. For example, both multisystemic therapy (Henggeler, Schoenwald, Borduin, Rowland, & Cunningham, 2009) and multidimensional treatment foster care (Chamberlain, 2003) extensively involve foster parents in treatment and are effective interventions for adolescents exhibiting mental health symptoms (Henggeler & Sheidow, 2012). Unfortunately, evidence-based interventions are underused in the foster care system (Spielfogel, Leathers, Christian, & McMeel, 2011). Alternatively, standard treatment approaches could incorporate a focus on the foster caregiver–youth relationship.
Moreover, some suggest that caregiver–youth disagreement also has important implications for engagement in treatment itself (De Los Reyes & Kazdin, 2005; Israel, Thomsen, Langeveld, & Stormark, 2007). In fact, greater caregiver–youth discrepancies predicted lower levels of parent involvement in treatment (Israel et al., 2007), which can undermine treatment effectiveness. Perhaps when the adolescent and caregiver are in greater agreement, services are more effectively utilized, which may curtail the development of mental health problems over time.
Finally, the methodological approaches employed in this study also contribute to the literature. Specifically, this study involved dyadic data analyses with two measures of adolescent–caregiver disagreement, the ICC and discrepancy scores. Doing so provides a more comprehensive approach to understanding differences. Indeed, scholars have called attention to the importance of using multiple indices when investigating interrater agreement (Youngstrom et al., 2000). In addition, this study drew from a large, nationally representative sample of adolescents in the U.S. child welfare system. Previous work in this area provided an important foundation by involving convenience samples of foster families in Australia and the Netherlands (e.g., Strijker et al., 2011; Tarren-Sweeney et al., 2004). This study built upon these findings by testing hypotheses with a generalizable sample of U.S. adolescents in foster care.
The present study has several strengths, especially the use of dyadic analyses and the nationally representative sample of adolescents in foster care across the country. There were also some limitations. First, there are many additional factors that may be associated with adolescent mental health symptoms. Broadening the scope of determinants to include the frequency of contact with the biological family, number of foster home placements, academic successes and/or failures, and other potential protective factors and stressors may help provide a more comprehensive view of discrepancies and adolescent mental health outcomes. Further, we used two indicators of disagreement, the ICC and discrepancy scores, both of which have limitations (Furr, 2010). To address the shortcomings of each indicator, scholars have supported using multiple indicators of disagreement (e.g., Youngstrom et al., 2000), as was done in the present study. Still, future research should continue to explore factors associated with discrepancies and work toward determining reliable and valid ways to assess discrepancies in perspectives and the implications for mental health.
Furthermore, although there are excellent measures of child behavior problems (such as the CBCL), due to informant discrepancies, there is no one “gold standard” for accurately assessing clinical problems, particularly for youth (De Los Reys & Kazdin, 2005, p. 483). As documented in past research, assessments may result in either an over- or underestimation of problems depending on who is asked (Youngstrom et al., 2000). Given the costs associated with mental health services for youth in foster care (Fang, Brown, Florence, & Mercy, 2012) and the number of youth estimated to have clinically significant problems (Landsverk et al., 2006), accurate assessments of these mental health concerns are essential. Thus, as scholars have been urging for some time (e.g., Buehler, 2006; Maguire, 1999; Zimmerman & Pogarsky, 2011), systematically incorporating data from multiple family members may provide a more comprehensive perspective of adolescent functioning.
Regarding the type of maltreatment adolescents experienced, although the NSCAW study followed protocol similar to other longitudinal studies of child maltreatment (see English & LONGSCAN Investigators, 1997), the interrater reliability among caseworkers is unknown. This represents a study limitation and opportunity for future researchers. In addition, the sample was restricted to adolescents because only youth ages 11 and older completed measures of interest for this study. Future research can test the replicability of these findings with youth of younger ages. Moreover, the design of this study does not allow for determinations related to cause and effect. Although relationship closeness was tested as a moderating variable in the association between the length of time adolescents lived with the caregivers and caregiver–adolescent discrepancies, it is possible that caregiver–adolescent disagreement on adolescent mental health may cause low relationship closeness. Finally, because of concerns of limited power, only the results of moderation analyses using absolute difference scores were reported. It may be meaningful to test directional discrepancy scores in future analyses.
In sum, understanding caregiver–youth disagreement is important because discrepancies have been linked with negative adolescent outcomes including drug use, school expulsion, early pregnancy, self-harm, need for mental health services (Ferdinand et al., 2004), and specific to youth in foster care, increased adolescent mental health symptoms over time (McWey et al., 2015) and the breakdown of foster care placements (Strijker et al., 2011). Results of the present study suggest that caregiver and adolescents provide significantly different ratings of youth mental health symptoms, and that gender, type of maltreatment experienced by the adolescent, and placement type may be associated with levels of discrepancy. Results also importantly indicate that higher quality relationships with caregivers moderate such discrepancies. Because the caregiver–adolescent relationship can mitigate discrepancies and help buffer against the known risks associated with placement in foster care (Oosterman et al., 2007; Withington et al., 2017), findings highlight the importance of promoting high-quality caregiver–adolescent relationships for youth. Doing so may have clinically significant implications for long-term outcomes of adolescents in foster care.
Footnotes
Authors’ Note
This article includes data from the National Survey on Child and Adolescent Well-Being, which was developed under contract with the Administration on Children, Youth, and Families, U.S. Department of Health and Human Services (ACYF/DHHS). The data have been provided by the National Data Archive on Child Abuse and Neglect. The information and opinions expressed herein reflect solely the position of the authors. Nothing herein should be construed to indicate the support or endorsement of its content by ACYF/DHHS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.