
Abstract
Despite U.S. child protective services (CPS) agencies relying on mandated reporters to refer concerns of child maltreatment to them, there is little data regarding which children mandated reporters decide to report and not to report. This study addresses this gap by utilizing a population-based linked administrative dataset to identify which children who are hospitalized for maltreatment-related reasons are reported to CPS and which are removed by CPS. The dataset was comprised of all children born in Washington State between 1999 and 2013 (N = 1,271,416), all hospitalizations for children under the age of three, and all CPS records. We identified maltreatment-related hospitalizations using standardized diagnostic codes. We examined the records for children with maltreatment-related hospitalizations to identify hospitalization-related CPS reports and if the child was removed from their parents. We tested for differences in these system responses using multinomial regression. About two-thirds of children identified as experiencing a child maltreatment-related hospitalization were not reported to CPS. We found differences in responses by maltreatment subtype and the type of diagnostic code. Children whose hospitalizations were related to abuse and associated with a specific maltreatment code had increased odds of being both reported to CPS and subsequently removed by CPS.
Child protective services (CPS) agencies in the United States rely on mandated reporters to refer and identify concerns of child maltreatment. In federal fiscal year 2017, the majority (65.7%) of reports to CPS that were screened in for investigation were made by professionals and estimated to total over 1.5 million across the country (US HHS, 2019). Further, the majority of current data sources only identify children who have been reported to CPS (Putnam-Hornstein et al., 2011), and therefore does not provide a complete picture of cases of suspected maltreatment. Thus, our knowledge about who mandated reporters decide to report and not to report to CPS is limited. This study addresses this gap by utilizing a population-based linked administrative dataset to identify which children who are hospitalized for maltreatment-related reasons are reported to CPS and, of those reported to CPS, which children are removed by CPS.
Mandated Reporting
Pediatrician C. Henry Kempe and colleagues published an influential article about “Battered Child Syndrome” in 1962 (Myers, 2008). In the article, the authors described both the presentations of child maltreatment that physicians may encounter and the importance of physicians reporting their concerns to the appropriate community agency, despite their reluctance to do so (Kempe et al., 1962). Policymakers followed Kempe’s lead and by the end of 1967, all 50 states and the District of Columbia had mandated reporting laws for all health care professionals (Waldfogel, 1998). The Child Abuse Prevention and Treatment Act (CAPTA) was passed federally in 1974 which tied the allocation of federal funds to a number of requirements by states, including state-level mandated reporting laws (Mathews & Kenny, 2008). Specifically, the passage of CAPTA led to the expansion of professions required to report concerns of maltreatment, the elimination of suspected harm being required to be characterized as serious harm, and the expansion of types of maltreatment required to be reported to include sexual abuse, neglect, and emotional abuse (Mathews & Kenny, 2008).
Despite the intention of keeping children safe, mandated reporting laws have been criticized. Melton (2005) referred to mandated reporting as “a policy without reason” arguing that the creators of the policy underestimated the size of the child maltreatment problem as CPS systems do not need help finding cases. Melton’s critique also contended that few of the cases brought to the attention of CPS result in serious physical harm to children, but rather typically have roots related to poverty. This, Melton (2005) asserts, leads to a mismatch between how CPS responds to concerns of maltreatment and the interventions needed by families.
In response to the criticisms of Melton (2005), Drake and Jonson-Reid (2007) examined the empirical evidence and found little support to sustain Melton’s concerns. In terms of identifying maltreatment cases, Drake and Jonson-Reid (2007) cited the National Incidence Study of Child Abuse and Neglect (NIS-3) which found that only about a quarter of seriously maltreated children were reported to CPS (Sedlak & Broadhurst, 1996). The NIS-4, the most recent version of the National Incidence Survey, found that the percentage of seriously maltreated children reported to CPS rose, but was still less than a third of all identified children (Sedlak et al., 2010). Other rebuttals to Melton (2005) have included moral and social justice arguments in order to protect children (Mathews & Bross, 2008).
Recent research highlights the distinctive risk that a CPS report is indicative of, beyond that of poverty. Putnam-Hornstein (2011) found a report to CPS, regardless of screening decisions by CPS, to be the strongest risk factor for injury mortality before the age of five in a population-based study of children in California. More recently, a longitudinal study in Wisconsin found that children alleged to have experienced neglect had poorer early adult outcomes than children exposed to poverty of similar length and depth and not reported to CPS (Font & Maguire-Jack, 2020). Taken together, these studies suggest that though poverty may be a common characteristic for children reported to CPS, the risk that results in a report to CPS goes beyond that of simple poverty.
Millions of reports concerning maltreatment are made to CPS annually in the U.S. (US HHS, 2019). However surveys of mandated reporters, including pediatricians, have indicated that they continue to be reluctant to report suspected maltreatment to CPS, just as Kempe and colleagues reported in 1962 (Flaherty et al., 2008; Sege et al., 2011). Reasons for not reporting include a lack of understanding of mandated reporting laws (Gunn et al., 2005), previous poor experiences with CPS (Flaherty et al., 2008; Gunn et al., 2005; Vulliamy & Sullivan, 2000), apprehensions about damaging the relationship with the child’s family (Gunn et al., 2005), previous experience testifying or being deposed in a maltreatment case (Gunn et al., 2005), and reservations regarding outcomes after reporting to CPS (Jones et al., 2008).
There is little data to quantify the magnitude of reluctance to report to CPS at a population level, but two population-based studies used linked administrative datasets to identify the CPS report rates of infants diagnosed with prenatal substance exposure. Both studies found that health professionals reported these children to CPS at relatively low rates. In California, 53.4% of infants diagnosed with prenatal substance exposure were reported to CPS (Putnam-Hornstein et al., 2016) while 42.4% of infants diagnosed with prenatal substance exposure were reported to CPS in Washington State (Rebbe et al., 2019a). These low report rates are despite directives set forth by the 2010 reauthorization of the federal law the Child Abuse Prevention and Treatment Act (CAPTA) that mandate notification of these infants to CPS (Lloyd et al., 2019). Thus, even though U.S. child protection systems are dependent on members of the public, and especially mandated reporters, to refer concerns of child maltreatment to CPS, the limited existing evidence on this subject suggests that these reports do not occur at the rate policies require that they should.
The underreported cases of child maltreatment by mandated reporters is an element in U.S. child welfare systems that has not been examined in as much detail, primarily due to a lack of data enabling such analyses to occur. The majority of current data only identifies children after they have been reported to CPS (Putnam-Hornstein et al., 2011). However, how professionals and agencies respond to identified maltreatment has been recognized as the most useful research for policy-makers because these professionals and agencies have great capacity to change (Jud et al., 2016). This study addresses this important component of U.S. child welfare systems by focusing on one context where mandated reporters interact with maltreated children, namely, hospitals.
Present Study
The aim of this study was to identify the initial responses of hospitals and CPS to children under the age of three hospitalized with child maltreatment-related diagnoses. Specifically, we were interested in which of these children were reported to CPS and which were removed by CPS during, or just after the hospitalization. In our models, we included factors from the child’s birth record and related to the hospitalization. This study utilized a unique population-based dataset of linked birth records, hospital discharges, and child protective services (CPS) administrative data. Datasets such as these have previously been identified an important source of evidence to inform policy and practice that provides a more comprehensive understanding of child maltreatment and its related systems (Jonson-Reid & Drake, 2008). We identified hospitalizations that were related to maltreatment through standardized diagnostic codes, the International Classification of Disease, Ninth Revision (ICD-9). More precisely, we used the codes identified by Schnitzer et al. (2011) to be suggestive of maltreatment and codes specifically indicative of maltreatment.
Method
Data
The data for this study are from a unique population-based dataset of linked birth records, hospital discharges, and child protective services (CPS) administrative data for all children born in Washington State from 1999 through 2013 (N = 1,271,416). A sequential deterministic linkage methodology was used to construct the dataset, as explained in Herman et al. (1997), using personal identifiable information, such as names and birthdates. After the linkages were complete, the dataset was de-identified for analysis. This is part of a larger parent study that has approval through the Washington State Institutional Review Board (IRB). The dataset includes information from the children’s birth records, any hospital admissions they have had within Washington State, and any involvement with the Washington State CPS agency. The dataset includes 332,676 unique hospitalizations from 1999 through 2013.
We examined the hospitalization records to identify if children had experienced a hospitalization related to maltreatment using the ICD-9 diagnostic codes. To identify maltreatment-related hospitalizations, we used ICD-9 codes that were specifically associated with maltreatment as well as codes suggestive of maltreatment. We restricted the analysis to hospitalizations that occurred before the child’s third birthday because the ages included for the suggestive codes identified by Schnitzer et al. (2011) were through 3 years of age (except one code). Further, our previous analysis of these data indicated that neglect-related hospitalizations occurred most frequently for children 1–2 years of age (Rebbe et al., 2021). Of the children identified with maltreatment-related hospitalizations, 4% (156) had multiple child maltreatment-related hospitalizations before their third birthday during the observation time period. Only the first child maltreatment-related hospitalization was included in the analysis so that we would not duplicate the sociodemographic variables through children with multiple hospitalizations and to homogenize the cohort. Some children (14) had multiple hospitalizations on the same date, indicating a likely transfer from one hospital to another for the same concerns. For these cases, the hospitalization that resulted in a transfer was removed from the dataset for analysis.
Measures
Initial responses
A three-outcome variable was created to indicate the initial response once the child was hospitalized for child maltreatment: 1) no CPS report or removal related to the hospitalization, 2) an intake made during the period of time the child was hospitalized (and no hospitalization-related removal), and 3) a hospital admission-related removal. The time period indicating a report related to the hospitalization started 4 days prior to the admission date through the discharge date, which allowed for the possibility of a child being in an emergency department prior to the hospital admission because emergency rooms were a typical entry point to the hospitalization for the children in this study. Further, the intakes were restricted to reporters who were categorized as medical professionals, mental health professionals, social service professionals, CPS workers, and law enforcement to ensure that the report was by a mandated reporter related to the hospitalization. A CPS removal was indicated when a removal occurred between 4 days prior to the admission date and 5 days after the discharge date from the hospitalization to allow for the court procedures necessary related to removals to occur.
Maltreatment category
A categorical variable was constructed based on the hospitalization ICD-9 diagnosis maltreatment subtype classification by Schnitzer et al. (2011). A table containing the codes is located in Appendix A. Each hospitalization had up to 25 diagnostic codes plus an external cause of injury code (E-code). Thus, for hospitalizations that had diagnoses from multiple categories of maltreatment, these were labeled as “poly-type.” The specific codes for maltreatment were also included in these categories. The ICD-9 specific codes that did not specify a type (995.5, 995.59, E967, and V71.81) were included in the “undesignated maltreatment” category, which included the “physical abuse or neglect” category from Schnitzer et al. (2011). The code for shaken baby syndrome (995.55) was included in the abuse category. The emotional/psychological abuse codes were included with the neglect category. The final categories included were: abuse, neglect, sexual abuse, undesignated maltreatment, and poly-type.
Specific maltreatment code
A binary variable constructed indicating the type of maltreatment ICD-9 code associated with the hospitalization. Codes were identified as specific if one of the explicit maltreatment-related codes (995.50-995.59, E967, V7181, V715) was associated with the hospitalization. If no specific maltreatment code was used, but the hospitalization was associated with a code identified as suggestive of maltreatment by Schnitzer et al. (2011), the maltreatment hospitalization was identified as suggestive.
Child sex
A binary variable was included based on the child’s birth record, with female treated as the referent category as previous research has indicated the male children are at higher risk for maltreatment-related hospitalizations (Mason et al., 2018).
Maternal race/ethnicity
This variable was constructed from two variables from the birth record, a race variable and an ethnicity variable. The categorical variable included White, Black, Hispanic, Native American, Asian/Pacific Islander, and other/unknown, with White as the reference category given it was the largest category in the cohort. A binary variable compared all race/ethnicity categories to non-Hispanic White.
Child age
A binary variable was constructed to indicate if the child was an infant (less than 1 year of age) on the hospitalization admission date or not.
Infant birth weight
The infant’s birth weight was converted to a binary variable as either low birth weight, as indicated below 2,500 grams, or normal birth weight, those of at least 2,500 grams, a typical construction for this variable (Mason et al., 2018; Putnam-Hornstein & Needell, 2011).
Parity
The number of live births the mother experienced prior to the current birth on the birth record was constructed as a binary variable as either the mother’s first-born child or a subsequent birth.
Birth payment category
A binary variable regarding the health insurance type used to pay for the birth, according to the birth records, as either private insurance or public insurance (like Medicaid). Private insurance was treated as the referent category as it was the largest category.
Prenatal care start trimester
A binary variable with first and second trimester prenatal care starts as the referent category and no or late (third trimester) prenatal care as the second category as the majority of births in this time period had prenatal care starts in the first or second trimester.
Maternal age
A binary variable was constructed based on the mother’s age at the time of birth, indicating whether the mother was a teenager (19 or younger) or older.
Analytic Approach
The distribution of initial responses was calculated for each of the measures. We then used multinomial logistic regression to test which factors were associated with the system responses. Multinomial logistic models extend logistic regression models where they include three or more outcome options and this approach is conceptualized as a series of logistic regressions (Gelman & Hill, 2007). In this case, the three-outcome initial response variable was the outcome variable. The possible outcomes were “No CPS Report,” “CPS Report” without a removal, and “Report & Removed” which also included a CPS report. Multinomial logistic regression was run with “No CPS Report” as the outcome reference using the multinom() function in the R “nnet” package (Venables & Ripley, 2003). Multinomial logistic regression was chosen over ordinal logistic multinomial models because these models require an order or ranking to the outcomes (Gelman & Hill, 2007). Without the additional information that clinicians use to make their determination of how to respond to maltreatment-related hospitalizations, we decided not to impose an order onto the outcomes. The equations for the multinomial model are as follows:


where βX is the vector of coefficients:
The binary maternal race category was used as it was found to be a better fit than a model with each of the maternal race categories as indicated by its lower BIC score (5,646.89 for categorical vs. 5,593.77 for binary). Results are presented as odds ratios.
In order to enhance interpretability beyond the coefficients (King et al., 2000), we used simulation to calculate the predicted probabilities of the system responses using the R package “simcf” (Adolph, 2013). Using the parameters from the predictive distributions of the model defined by the variance-covariance matrix, specifically allowing the maltreatment types and the specific maltreatment code status to vary while holding the covariates at the mean, we drew 1,000 simulations and plotted them by maltreatment type and specific maltreatment code status.
Results
Descriptive Statistics
A total of 3,907 children were identified as being hospitalized for a maltreatment-related reason. The flow of the initial system responses is presented in Figure 1 through the use of a Sankey diagram, moving from left to right. It displays in the first step the proportion of the hospitalizations by maltreatment type. The second step shows the proportion with either a specific or non-specific maltreatment code from the maltreatment types illustrated in the first step. The third and fourth steps are CPS reports and removals, respectively, moving from the previous steps.
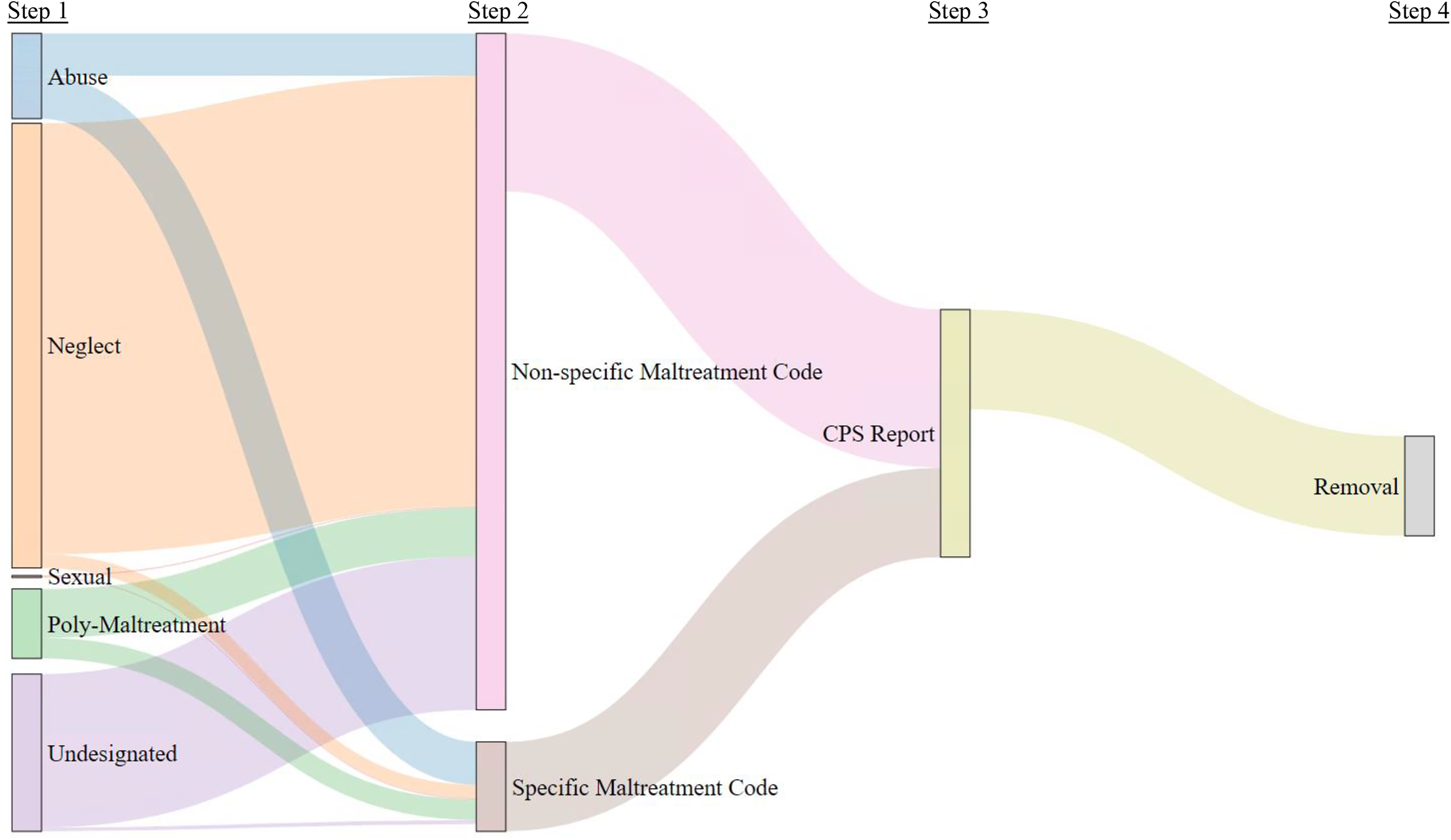
Flow of responses to child maltreatment-related hospitalizations.
Table 1 provides a description of the population of children in this study. Children under the age of one made up just under half (47.7%) of children with maltreatment-related hospitalizations in the study. Of the children identified as experiencing a maltreatment-related hospitalization, 56.6% were identified as male on their birth records. More than half of the hospitalizations (58.6%) were associated with neglect. Only 10 children had hospitalizations related to sexual maltreatment, therefore that category has been removed from the results presentation.
Distribution of Maltreatment Type and Sociodemographic Variables by System Respon.
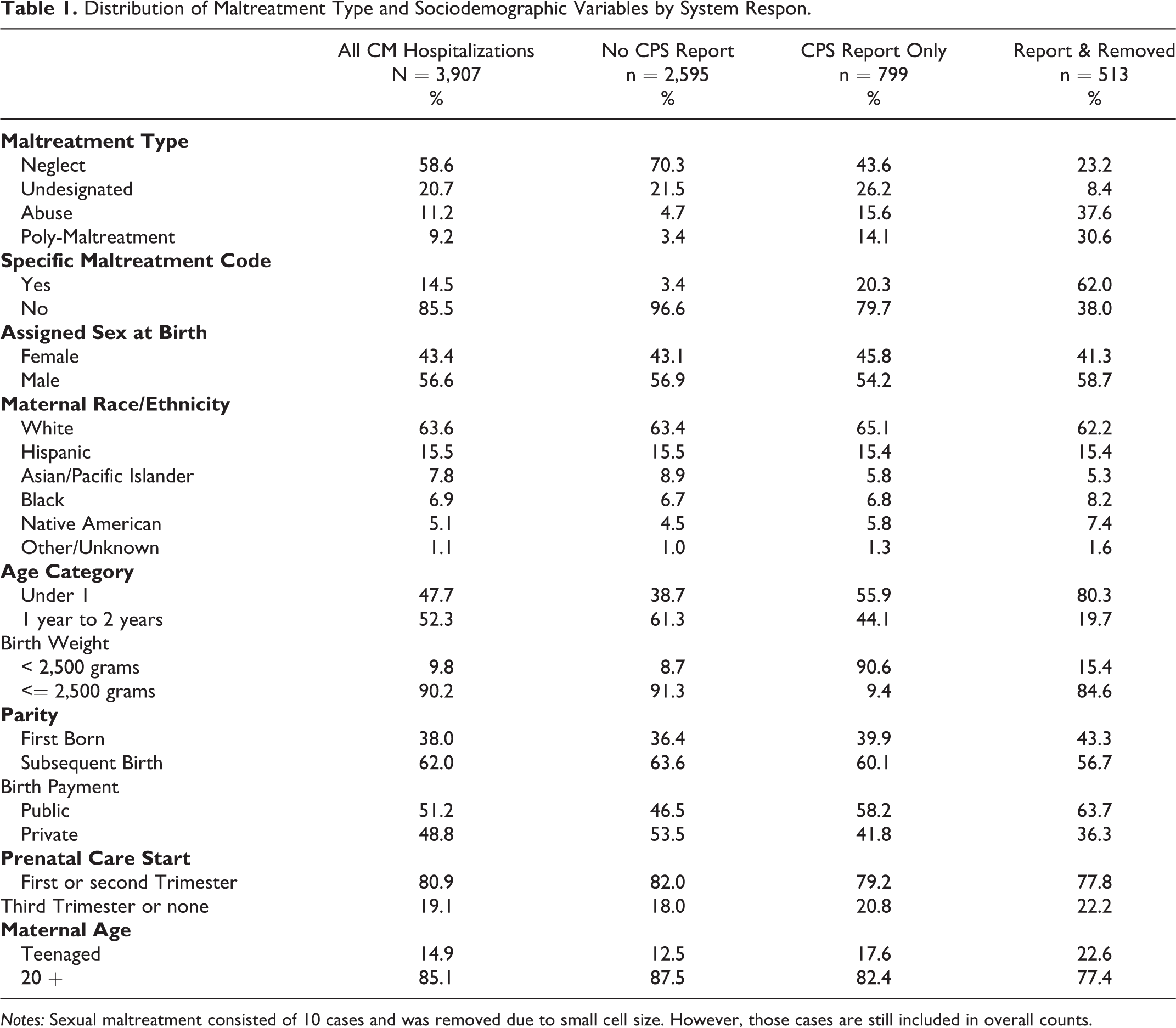
Notes: Sexual maltreatment consisted of 10 cases and was removed due to small cell size. However, those cases are still included in overall counts.
Table 1 also presents the distribution of the systems responses by each of the included factors from the birth and hospitalization records. About two-thirds (n = 2,595) of children identified as hospitalized for maltreatment-related reasons were not reported to CPS, while 20.5% were reported to CPS without a related removal, and 13.1% were removed. Differences were observed in the distribution of response category by the presence of a specific maltreatment code. The vast majority of all children not reported to CPS (96.6%) did not have a specific maltreatment code associated with their hospitalization, but 15.3% of children who did have specific maltreatment code were also not reported to CPS.
Figure 2 presents the system responses by diagnostic code type and maltreatment subtype. More than half of hospitalizations related to a specific maltreatment code resulted in a removal (56.1%) and 15.3% were not reported to CPS at all. Three quarters (75.1%) of hospitalizations associated with suggestive codes were not reported to CPS. The majority (79.6%) of neglect-related hospitalizations were not reported to CPS, and only 5.2% resulted in a removal. Removals were highest for abuse and poly-maltreatment hospitalizations at 44% and 43.9%, respectively. About a quarter of abuse-related (27.6%) and poly-maltreatment (24.6%) hospitalizations were not reported to CPS.
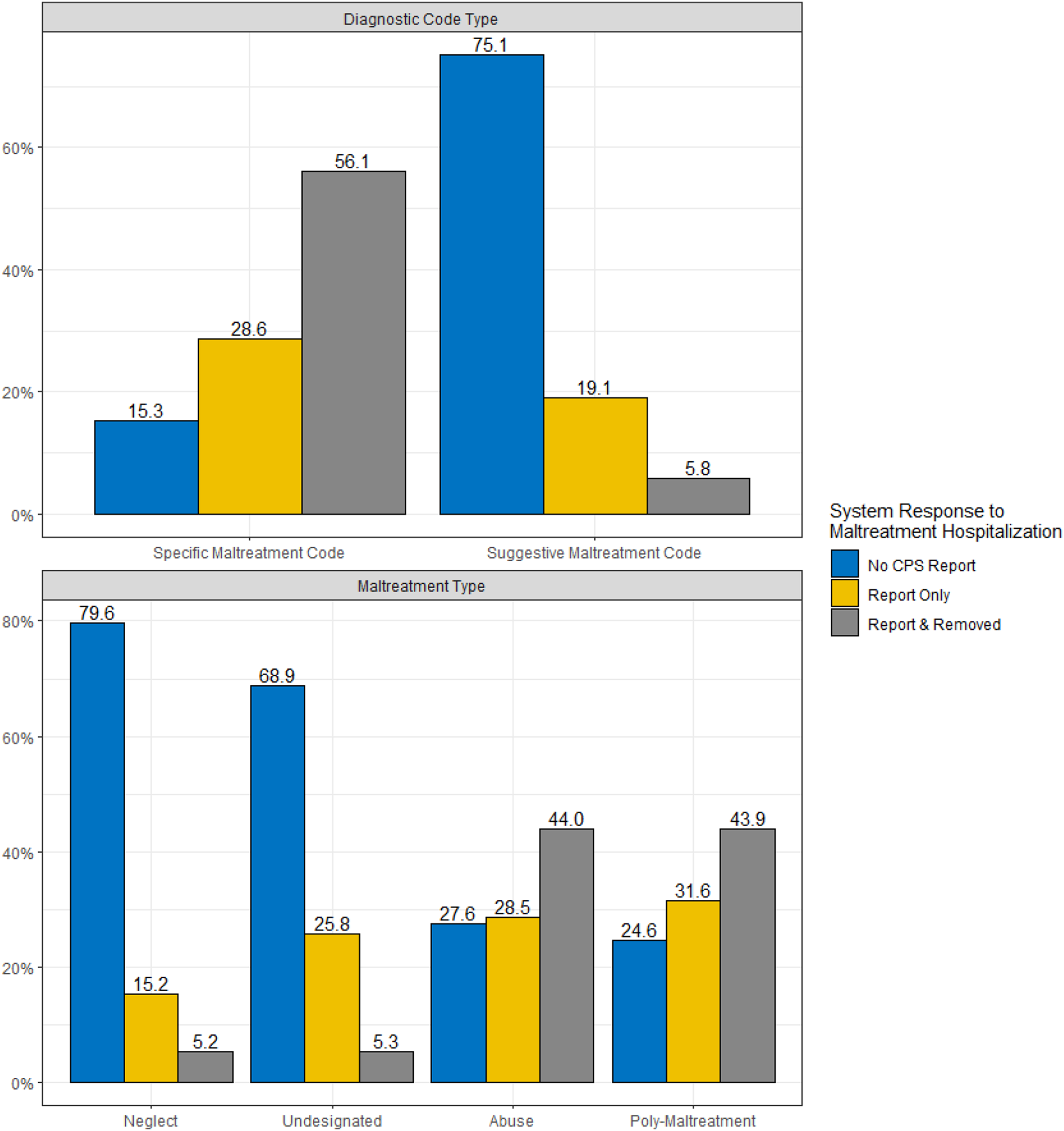
Distribution of system responses by code and maltreatment type.
Multinomial Logistic Regression
Figure 3 presents the odds ratios of the multinomial logistic regression. Compared to neglect, all of the other types of maltreatment had increased odds of both reports to CPS and removals by CPS. In terms of reports to CPS (without removal), the odds of being reported to CPS without an associated removal were 3.7 times higher for children with abuse-related diagnoses, 3.4 times higher for poly-maltreatment related diagnoses, and 1.9 times higher for undesignated maltreatment type diagnoses compared to children with neglect-related diagnoses. Just two of the maltreatment subcategory diagnoses had higher odds for being removed compared to children with neglect related diagnoses: abuse (OR: 6.89; 95% CI: 4.83, 9.83) and poly-maltreatment (OR: 4.65; CI: 3.09, 7.02).
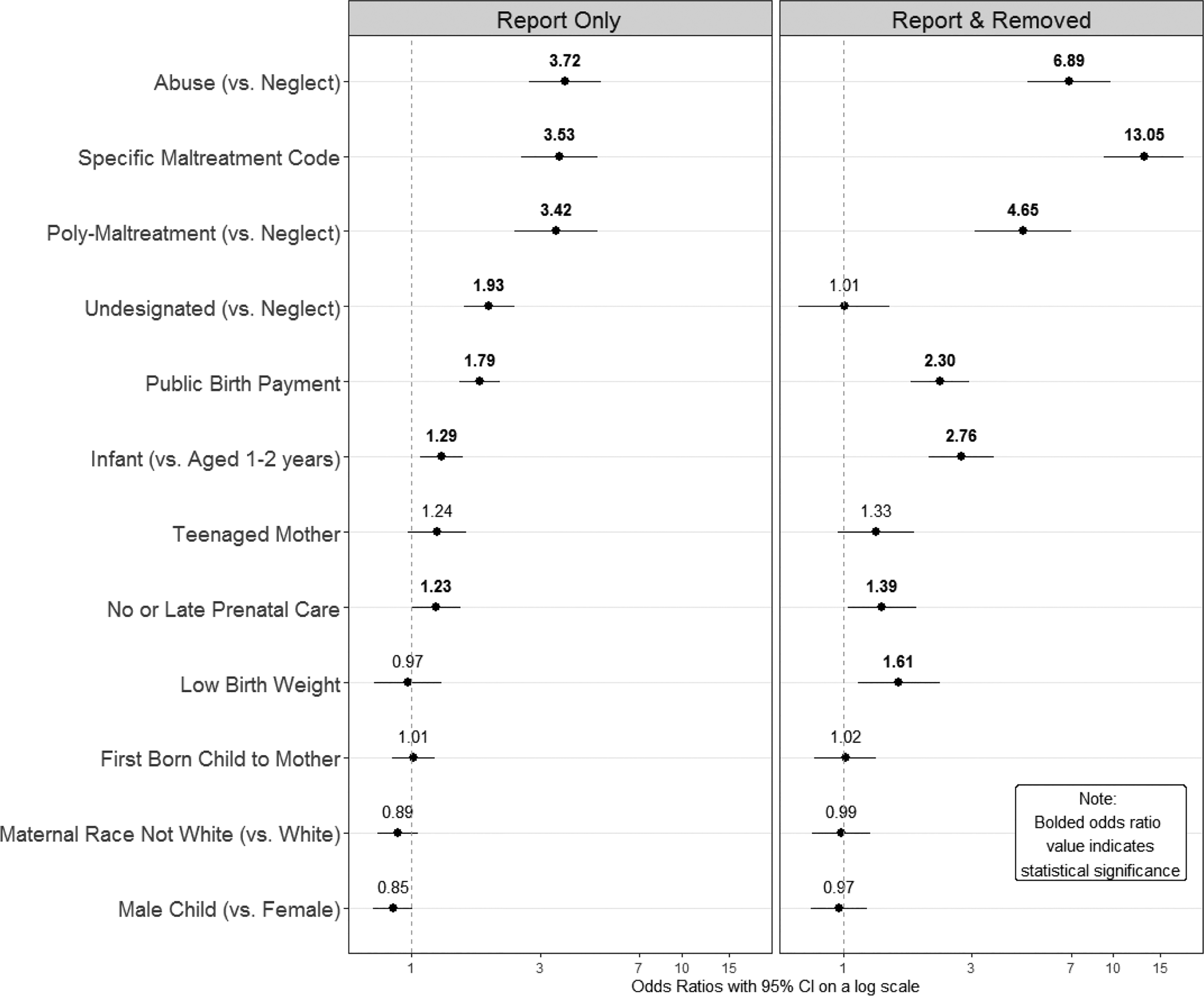
Odds ratios of system responses from multinomial regression.
The use of a specific maltreatment diagnosis increased the odds that a CPS report would be made and that the child would be removed by CPS. Specifically, children who had a specific maltreatment diagnosis had odds 3.5 times higher for being reported to CPS and odds 13.1 times higher of being removed by CPS than children whose diagnoses did not specifically indicate maltreatment.
Risk factors identifiable on the birth record also had increased odds of CPS interventions. Children whose births were paid for using public insurance, like Medicaid, had increased odds for CPS reports (OR: 1.79; 95% CI: 1.50, 2.12) and removals (OR: 2.30; CI: 1.79, 2.95) than children whose births were paid for using private insurance. Children born to mothers who started prenatal care late or did not receive any at all had prenatal care had increased odds for a CPS report (OR: 1.23; CI: 1.00, 1.52) and removals (OR: 1.39, CI: 1.04, 1.87). Infants were more likely to experience CPS reports (OR: 1.29, CI: 1.07, 1.55) and removals (OR: 2.76, CI: 2.09, 3.64) than children aged 1 or 2 years old. Maternal race, the child’s age in days at the time of hospitalization, the child’s sex, maternal age, and parity were not found to have statistically significant impacts on the odds of reports or removals.
Figure 4 presents the predicted probabilities of the system responses produced by simulating the multinomial logistic regression results. The first column presents the probability of not being reported to CPS, the second column the probability of a CPS report without removal and the third column contains the probability of being reported and removed. The rows are for the specific (top) and suggestive (bottom) maltreatment codes. Colors distinguish the different maltreatment types. Each circle represents the predicted probability for a single instance of the 1,000 simulations. The point estimates, or the mean of the simulations, is presented for each cell.
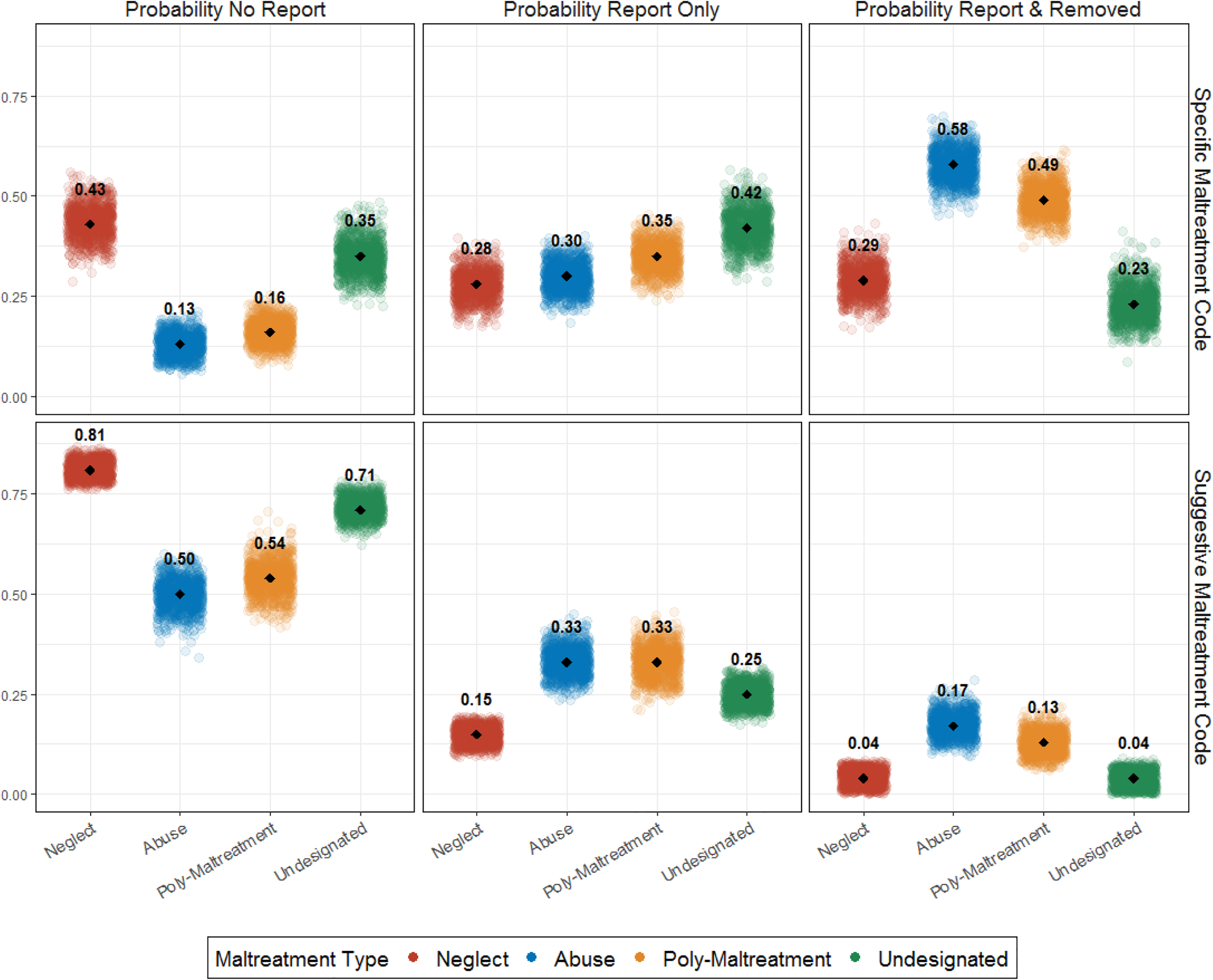
Probabilities of system responses by maltreatment subtype and diagnostic code type.
Children with neglect-related hospitalizations have higher predicted probabilities for not being reported to CPS for both maltreatment code statuses: suggestive (point estimate: 0.81) and specific (PE: 0.43). Put differently, 81% of children hospitalized with an accompanying suggestive neglect diagnosis were predicted not to be reported to CPS and 43% of those with a specific neglect-related diagnosis were predicted not to be reported to CPS. For all maltreatment types, the predicted probability of being unreported to CPS was higher for those without a specific maltreatment diagnosis. Conversely, those with specific maltreatment diagnoses had higher predicted probabilities of being removed by CPS across all maltreatment types.
Discussion
This study found that about two-thirds of children under the age of three hospitalized for child maltreatment-related reasons are not reported to CPS. While it is not clear from our data if all the identified cases should have been reported to CPS, CPS agencies in the U.S. are reliant on mandated reporters and members of the public to alert them to concerns of child maltreatment. Without these reports to CPS agencies, these agencies cannot intervene and offer families services, as only 0.4% of all screened-in reports came from the victims themselves in 2017 (US HHS, 2019). Health professionals, inclusive of a variety of professions, are particularly important in this structure of child protection systems, especially in light of recent research identifying that sentinel injuries are being missed by health professionals prior to more serious injuries (Berger & Lindberg, 2019). Indeed, these hospitalizations are critical opportunities for intervention, and health professionals, especially pediatricians, are integral to this (Jackson et al., 2015; Letson et al., 2016). The results of this study indicate that these opportunities for intervention are being missed by health professionals. Future research should examine if there are differences in CPS reporting by hospital type.
Multidisciplinary child protection teams have been formed in many hospitals in recognition of the important opportunity for child maltreatment intervention that exists when children are presented for medical treatment and the benefit of interdisciplinary collaboration (Kistin et al., 2010). Future research should examine if and how the presence of a child protection team at the hospital impacts the reporting of child maltreatment-related hospitalizations to CPS.
These results are similar to the results found in regard to prenatal substance exposure in California (Putnam-Hornstein et al., 2016) and Washington State (Rebbe et al., 2019a). Those results found that just over half of California infants and slightly less than half of Washington State infants diagnosed with prenatal substance exposure were reported to CPS and that there was great variation in reports and removals depending on the type of substance the infant was exposed to in utero. Likewise, the system responses to child maltreatment-related hospitalizations in this study depended on the diagnosis associated with the hospitalization.
We identified clear differences in the system responses by the maltreatment type. About 20% of neglect-related hospitalizations were reported to CPS (inclusive of both reports only and removals) while abuse and poly-maltreatment related hospitalizations had about three quarters resulting in at least a CPS report. Similarly, abuse-related hospitalizations had the highest rate of cases resulting in removals by CPS. But an important contextual factor here is the use of specific maltreatment codes. The use of a specific maltreatment code had a very different distribution than hospitalizations associated with suggestive codes, where about 85% of hospitalizations with a specific code resulted in at least a CPS report. In contrast, just about a quarter of hospitalizations with a suggestive code were reported to CPS.
Yet, the finding that there are still some hospitalizations associated with child maltreatment specific diagnoses that do not result in a CPS report supports previous research that health professionals do not always reports concerns of child maltreatment even when they suspect it has occurred (Flaherty et al., 2008; Sege et al., 2011). Further research is warranted to understand the patterns that may accompany this finding and to identify if improved policy or training is necessary.
One important aspect regarding the ICD-9 codes is that it has limited coding options in regard to neglect. This may be a reflection of the medical field not considering neglect to be an important aspect of child maltreatment requiring a diagnostic code. If that is accurate, this is further complicated because it is difficult to discern whether the dearth of neglect codes is the result of the ICD-9 code authors responding to the practices of health professionals or health professionals acting in accordance with the established ICD-9 codes. Nevertheless, this exemplifies the utility of the suggestive codes by Schnitzer et al. (2011) and that the ICD-10 codes include improved neglect codes, including one for inadequate supervision (McKenzie & Scott, 2011). Future research should examine the ICD-10 child maltreatment-related codes and the ICD-11 codes when they are implemented.
Another issue this elicits is how health professionals evaluate the suggestive diagnoses in regard to child maltreatment. One explanation is that health professionals in Washington State disagree with the Schnitzer et al. (2011) taxonomy of suggestive codes. This possibility indicates that further work is likely needed to authenticate this classification of suggestive codes, including the consideration of codes not contained in the Schnitzer et al. (2011) list that may be suggestive of maltreatment such as oral injuries (Dorfman et al., 2018) or extremity fractures (Leventhal et al., 2008). However, research has also indicated that health professionals often miss signs of child maltreatment (Berger & Lindberg, 2019) and are often reluctant to report child maltreatment to CPS (Flaherty et al., 2008; Sege et al., 2011). Thus, the source of the disagreement between the suggestive codes and the filing of CPS reports is unclear. This is an area for future research which should include an examination of variation at different levels, such as hospital or geographic discrepancies, which may indicate cultural, policy, coding, or training differences.
This study’s results of the system responses to child maltreatment-related hospitalizations address an important gap in our understanding regarding how health professionals report child maltreatment to CPS at a population-level. Further, the results provide crucial information regarding CPS removals of children from their caregivers upon receipt of these reports. This information is the result of using a novel population-based linked administrative database that enabled this study to track children longitudinally across the various systems they interact with, specifically, from birth to hospital to CPS. Databases, such as this, have previously been identified as an important source of evidence to inform policy and practice because they provide a more comprehensive understanding of child maltreatment and its related systems (Jonson-Reid & Drake, 2008). The results of this study realize this potential and provide new knowledge at the system level so that we can understand how these responses occur across the entire state of Washington, providing more information about how these systems interact than either a sample or a survey. Data linkages like the ones conducted for this study are a growing part of the child welfare field (Eastman & Putnam-Hornstein, 2019; Mason et al., 2018; Parrish et al., 2011; Rebbe et al., 2019b), but only exist in a limited number of jurisdictions and vary by which systems they are able to link. The only other U.S. study, to our knowledge, that utilized administrative data that linked hospital and CPS data, as done here for this study, did not examine this critical question regarding health professionals reporting hospitalizations related to child maltreatment to CPS and if CPS removes these children from their caregivers (Schnitzer et al., 2004). Instead, that study focused on the ascertainment of the number of children who experienced maltreatment, as measured by hospitalization or CPS maltreatment substantiation. This study extends the analysis of the administrative data to provide information on which children are reported to CPS and then, subsequently, which children are removed from their parents. Understanding these decision points is critically important regarding child protection and the safety of children.
Limitations
Despite the new knowledge generated by this study, there remain limitations. First, as with all administrative data studies, we cannot account for the complex nature of individual cases and the many pieces of information that health care professionals and CPS investigators consider when making their decisions, including consultations with a hospital child protection team. Second, it is possible that in the linkage process some matches were missed. Third, our analysis relied on ICD diagnostic codes, which despite having standardized definitions (Farst et al., 2013), may not be applied uniformally across hospitals (Hooft et al., 2015) or sociodemographic groups. Further research is needed to understand variability in coding practices. Relatedly, it is possible that for children with the diagnosis code V71.81 (observation for abuse and neglect) that maltreatment was ruled out after treatment and therefore not reported to CPS. Additionally, these are the results from a single U.S. state and it is unclear if similar results would be found in different states. Similar research should be conducted in other jurisdictions to see if similar patterns are found. Finally, our data is limited to hospital admissions and do not capture other medical encounters, such as emergency department visits, where presumably many more children are seen. Future research should include medical encounters that do not result in hospital admissions to examine if similar patterns exist in response to child maltreatment.
Conclusion
This study provides new knowledge that ascertains which maltreatment-related hospitalized children are reported to CPS by health professionals and, of those children, which are removed immediately by CPS. Two important findings came from this analysis. Firstly, the responses were dependent on the subtype of maltreatment and type of diagnostic code used. Specifically, physical abuse and codes specifically related to maltreatment had higher rates of CPS reports and removals. Secondly, about two-third of children who experienced a maltreatment-related hospitalization were not reported to CPS, despite mandated reporting laws. These results provide the broadest and most rigorous understanding of how children move from the health system of hospitals to CPS agencies to date. The new knowledge identified through this study has important implications for our understanding how current systems are responding to child maltreatment.
Supplemental Material
Supplemental Material, sj-pdf-1-cmx-10.1177_1077559520984549 - Reports and Removals of Child Maltreatment-Related Hospitalizations: A Population-Based Study
Supplemental Material, sj-pdf-1-cmx-10.1177_1077559520984549 for Reports and Removals of Child Maltreatment-Related Hospitalizations: A Population-Based Study by Rebecca Rebbe, Joseph A. Mienko and Melissa L. Martinson in Child Maltreatment
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Steve and Connie Ballmer Family Giving, Casey Family Programs, Stuart Foundation, and partial support for this research came from a Eunice Kennedy Shriver National Institute of Child Health and Human Development research infrastructure grant, P2C HD042828, to the Center for Studies in Demography & Ecology at the University of Washington.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.