
Abstract
The study compared life course models (LCM; accumulation, recency, and sensitive period) of child maltreatment and general psychopathology in a large, national longitudinal data set of 1354 youth ages birth-16 years (657 boys, 53.2% Black, 59.7% <$40K caregiver income). Previous research has supported the accumulation and recency models, albeit with shorter or fewer time periods of outcome measurement. We extend this work by modeling the impact of combined abuse and neglect allegations on a general psychopathology factor (dysregulation profile). Cross-sectional structural equation models were constructed using LCMs and tested across two-year periods from 4–16 years old and compared using Akaike Information Criterion weights. The recency variable generally explained the greatest proportion of variance in psychopathology. Notably, maltreatment more proximal to the time of outcome measurement had the strongest effect, suggesting that more recent maltreatment may have stronger effects on general psychopathology. These results lend support to a recency effect of maltreatment on psychopathology outcomes, although substantive overlaps with the accumulation model are noted.
Child maltreatment (CM) is a widespread problem, with nearly 300 million children aged 2–4 years old having been physically or emotionally abused (WHO, 2020). The National Incidence Study of Child Abuse and Neglect tracks incidents of abuse and neglect via reports by mandatory reporters; its fourth iteration (NIS- 4) recorded a rate of 3.95% of children in the United States being subject to any kind of CM. CM is associated with severe deleterious consequences across time. Aside from the physical injuries incurred by physically and/or sexually abused children, many of these children go on to suffer social and behavioral problems, cognitive and school problems, poor mental health outcomes, and poor overall medical health (Widom, 2014). The mainstream ecological-transactional model of CM suggests that CM brings about deviations from the average expectable environment of the child, leading to failures to resolve salient developmental issues at each developmental stage with the consequent poor outcomes (Cicchetti & Valentino, 2015).
Incorporated at the microsystem level of the ecological-transactional model are the dimensions of CM. Occurrences of CM have a multifaceted temporal dimension, encompassing when CM occurs (developmental timing/sensitive periods), how proximal the CM occurrences are to the time of measurement (recency), and accumulation. Accumulation is a broad construct that can refer to any of the following: how many distinct CM exposures occur (total frequency), the number of developmental periods the CM occurrences span (periodic frequency), and the duration between the time of first CM event and last CM event (duration; Jonson-Reid et al., 2012). It can also refer to the degree to which CM occurrences are closely clustered in time (conglomeration). These temporal dimensions, also termed life course models (LCM; Dunn et al., 2018), are key features of the etiological models of CM, since a wide array of evidence suggests that these subdivisions of the temporal dimension are influential over CM outcomes.
While the temporal dimension seemingly affects outcomes, it remains unclear which facets are the most explanatory. Sensitive periods posit that maltreatment occurring in certain periods are more explanatory of outcomes than maltreatment occurring in other periods. A review of CM studies found that while sensitive periods had effects on a variety of child outcomes (such as mental disorders, correlated neuroanatomical changes, and other psychological functions), no consistent sensitive periods could be identified (Schaefer et al., 2022). Effects indicating a dose-dependent relationship between CM and mental health outcomes/mental functioning have been found in a variety of studies (Harpur et al., 2015; Jaffee & Maikovich-Fong, 2011; Jonson-Reid et al., 2012; Russotti et al., 2021; Young-Southward et al., 2020), supporting the role of accumulation. Several studies have also found recency effects. For instance, Shanahan et al. (2011) found that CM occurring in the same period as outcome measurement was predictive of child-onset and adolescent onset depression, while antecedent CM was not. Other studies examining diverse outcomes like delinquency, substance use, and mental health have found that CM in adolescence was more explanatory of negative late adolescent outcomes than CM in childhood (Ireland et al., 2002; Thornberry et al., 2001; Tracy et al., 2019). These studies indicate the need to examine CM effects on broader outcomes, as well as the need to test multiple facets of these temporal dimensions in the same study.
Theoretical shifts in developmental psychopathology suggest traditional disorder-based models may be less explanatory than factors accounting for general risk for psychopathology. Just as a general intelligence, or g, appears to account for associations between test scores across cognitive tests for the same individual, Caspi et al. (2014) suggested that p might serve a similar function, reflecting various dimensions of psychopathology. p is thought to be clinically useful as an index of overall impairment, which can support treatment planning and goal setting (Martel et al., 2017; Patalay et al., 2015; Smith et al., 2020). The dysregulation profile (DP) is a similar construct found exclusively in children, typically comprising one general DP factor superordinate to three specific factors of anxiety/depression, aggressive behavior, and attention problems (Deutz et al., 2018). Deutz et al. (2020) noted that while p and DP have different operationalizations and factors (such as attentional problems and thought-problems for g), they concluded that qualitative differences in their operationalizations negligibly impact the association with antecedent characteristics and outcomes, suggesting that DP may similarly be useful as a general factor of psychopathology. Further, Deutz et al. (2016) found that a bifactor DP model was the best fitting model for modeling CBCL factors in adolescence, suggesting the validity of the measure in both adolescence and childhood. Given our focus on the development of psychopathology across childhood into adolescence and the broad risks for psychopathology conferred from multiple forms of CM, we focus on the general DP factor in this investigation.
Current Study
To our knowledge, two direct comparisons have been made in the literature between different temporal models of childhood adversity. Dunn et al. (2018) investigated relations between LCMs of childhood adversity exposure and later mental health outcomes in a prospective longitudinal sample of children from birth to eight years old. They compared the extent to which each of the three LCMs — recency, accumulation, and sensitive period — were predictive of psychopathology symptoms at eight years old. Childhood adversities were defined as caregiver emotional or physical abuse, sexual or physical abuse (by anyone), financial stress, and parental legal problems. The accumulation model was defined as the sum of the number of 12-month periods in which exposure to maltreatment occurred. The recency model was defined using the accumulation model but weighted the sum, such that periods closer to the final measurement point had higher weights. Finally, the sensitive period model was defined as an indicator variable (exposed/not exposed) for each period. They analyzed the results using a least angle regression procedure for the models among each type of adversity. Overall, they found that across adversities, child psychopathology symptoms were better explained by accumulation and recency of exposure than sensitive periods. With both caregiver abuse and abuse by anyone, more recent exposures, followed by accumulation, had the most influence. Only two sensitive periods emerged: during very early childhood for financial stress in girls and very early childhood for parental legal problems (Dunn et al., 2018).
Russotti et al. (2021) operationalized the temporal dimension of CM in terms of chronicity (operationalized similarly to accumulation as defined by Dunn and colleagues), developmental timing (recent and/or early-onset), and as a binary variable (any maltreatment vs. no maltreatment), examining these effects on the internalizing and externalizing factors of the CBCL from 10–12 years old and subsequent psychopathology presentations around 20 years old. Maltreatment types used included physical, sexual, emotional abuse and neglect. They then tested the three dimensional models separately: the binary variable, chronicity/accumulation (as a number of developmental periods), and the four categories of early-onset recent maltreated, early-onset nonrecent maltreated, late-onset maltreated, and non-maltreated. After conducting confirmatory factor analysis on the factor structure of the latent CBCL factors being examined, they estimated three structural equation models using the three dimensional models separately as regression predictors. Results found that the chronicity/accumulation model better captured the developmental pathways across time as compared to the binary variable. The late onset-only group predicted externalizing symptoms, while the early-onset recent group had greater risk of internalizing and externalizing symptoms. These results lend support to the accumulation model, the school-age sensitive period model, and provide evidence against an early sensitive period.
Integrating and expanding upon previous efforts, we explored the degree to which LCMs (recency, accumulation, and sensitive period; Dunn et al., 2018) of combined maltreatment (physical, sexual, emotional abuse, and neglect; Russotti et al., 2021), explained general psychopathology outcomes using the DP framework. As psychopathological symptoms commonly manifest in childhood and express more fully as disorders in adolescence and emerging adulthood (Zeman et al., 2020), more nuanced examinations of timing of CM across childhood, using developmentally appropriate conceptual frameworks, like DP, are needed. The use of a large, national prospective longitudinal sample of children (LONGSCAN; Runyan et al., 2020) afforded the opportunity to extend the time periods of assessment and increase the number of observation periods from both Dunn’s and Russotti’s work, as well as provide a more comprehensive view of psychopathology.
Methods
Data Source
LONGSCAN is a multi-site consortium of research studies on CM with coordinated data collection procedures, assessment measures, and schedules (Runyan et al., 2020). The comprehensive and longitudinal nature of LONGSCAN makes it ideal for secondary analysis of this type, with measures collected at ages 0, 2, 4, 6, 8, 10, 12, 14, and 16 years and a total sample size of 1354 children. The attrition rate across sites from baseline to age 16 was 33.9% (Runyan et al., 2020). The overall sample was geographically representative, with the studies conducted in the East (EA), Midwest (MW), Northwest (NW), Southwest (SW), and South (SO) regions of the United States. The EA cohort (n = 282) consisted of children from low-income families served at three pediatric clinics, with groups within this sample having either had inadequate growth in the first two years of life, parents who had a HIV infection or used drugs, or no other identified risk factors. The MW cohort (n = 245) contained children from families reported to child protective services (CPS), comprising two-thirds of the sample; half of these were provided access to comprehensive services (including mental health services), while the other half only received an intervention from CPS. The remaining third were controls from the neighborhood. The NW cohort (n = 254) comprised children aged 0 to 4 judged to be at moderate risk of CM by CPS after their families were reported to CPS, with 60% of the reports being substantiated. The SW cohort (n = 330) included children who were put in out-of-home placement with a relative or foster family, while the SO cohort (n = 254) was drawn from children identified as high risk of CM by a state-level public health tracker, with a ratio of 2:1 between non-reported children to reported children.
Demographic characteristics of the analytic sample are outlined in supplemental materials (Supplemental Table 1). Overall, the sample contained an approximately even mix of girls and boys, with over half of the sample identifying as African American. The majority of the sample’s caregiver income was below $40K. Proportions of children exposed to any kind of maltreatment (physical, sexual, emotional, neglect) prior to the point of measurement ranged from 55.8% (at Wave 4) to 67.1% (at Wave 10). Proportions stabilized from Wave 10 onwards.
Measures and Procedures
Measures include the temporal dimensions of CM from the Derived Maltreatment Dataset as coded by trained LONGSCAN investigators from CPS records and general psychopathology as captured by the Achenbach Child Behavior Checklist (CBCL) 2–3 and CBCL 4–18 Caregiver Report. Details regarding the measures used are drawn from the LONGSCAN Measures Manuals - Volume I (Hunter et al., 2001), Volume II (Hunter et al., 2002), III (Knight et al., 2010), IV (Knight et al., 2014a), and V (Knight et al., 2014b). Analyzed scales were administered during face-to-face interviews (before age 8), computer-assisted face-to-face interviews (age 8) and through the Audio-Computer Assisted Self Interview delivery system from age 12 onward. Full data collection procedures are outlined in Runyan et al. (2020).
Achenbach CBCL
The Achenbach Child Behavior Checklist 4 to 18 (CBCL; Achenbach & Ruffle, 2001) caregiver report form assesses eight areas of problems in 4 to 18 year olds: Social Withdrawal, Somatic Complaints, Anxiety/Depression, Social Problems, Thought Problems, Attention Problems, Delinquent Behavior, and Aggressive Behavior. In LONGSCAN, the scale was generally reliable, with a Cronbach’s alpha of 0.62–0.92 for boys aged 4–11 and 0.66–0.92 for girls aged 4–11. The CBCL Dysregulation Profile (DP), developed by Biederman et al. (1995), is comprised by the Anxiety/Depression Problems, Attention Problems, and Aggressive Behavior scales. The latent factor CBCL-DP was constructed from a bifactor model and used in analysis at wave 4 (M = 21.58, SD = 14.34), wave 6 (M = 23.13, SD = 15.41), wave 8 (M = 23.19, SD = 16.58), wave 10 (M = 21.65, SD = 17.43), wave 12 (M = 23.39, SD = 17.84), wave 14 (M = 23.09, SD = 18.96), and wave 16 (M = 21.09, SD = 18.90). Means and standard deviations provided here are of the raw summed scores, as opposed to the latent factor.
Derived Maltreatment Dataset
The LONGSCAN researchers consolidated CM data regarding time of referral, number of CM allegations, and substantiated allegations within time periods, type of CM for each, and whether the type of CM experienced was singular or multiple. CM data was drawn from multiple sources. Maltreatment data was extracted and coded by trained coders from Child Protective Services Agency narratives using the Modified Maltreatment Classification System (English & The LONGSCAN Investigators, 1997). Additionally, self-report measures for physical and sexual abuse and emotional maltreatment were administered at age 12 (Measure Manual of Functioning and Outcomes in LONGSCAN: Middle Adolescence [Age 16]; LONGSCAN Coordinating Center, 2014). These sources were combined by LONGSCAN investigators into a single combined maltreatment variable for analysis. Types of maltreatment included in the current study include physical and sexual abuse, emotional maltreatment, and neglect. Definitions of maltreatment types were defined in the Modified Maltreatment Classification System (English and The LONGSCAN Investigators, 1997). Here, physical abuse is defined as the intentional infliction of an injury upon a child by a caregiver or responsible adult. Sexual abuse is any attempted or actual sexual contact between a caregiver of other responsible adult and a child for the purposes of the caregiver’s or responsible adult’s sexual gratification or financial benefit. Emotional maltreatment is defined as a parent’s relentless or extreme thwarting of a child’s basic emotional needs and/or acts by parents that are insensitive to a child’s developmental level, causing harm. Basic emotional needs include psychological safety and security, acceptance and self-esteem, and age-appropriate autonomy. Neglect is defined as physical neglect that either involves a failure to provide a minimum degree of care to meet the child’s physical needs or a lack of supervision involving inadequate precautions for a child’s safety relative to their developmental level. CM is recorded at intervals of two years, from birth to 16 years of age. No clear age cut-off dates were apparent for the intervals since the LONGSCAN researchers collected data from each person at a different date; however, because the data is recorded as counts of CM occurring within a particular age interval, there should be no overlaps in the intervals.
Data Analytic Plan
Description of Life Course Models Operationalized as Manifest Variables in the SEM.
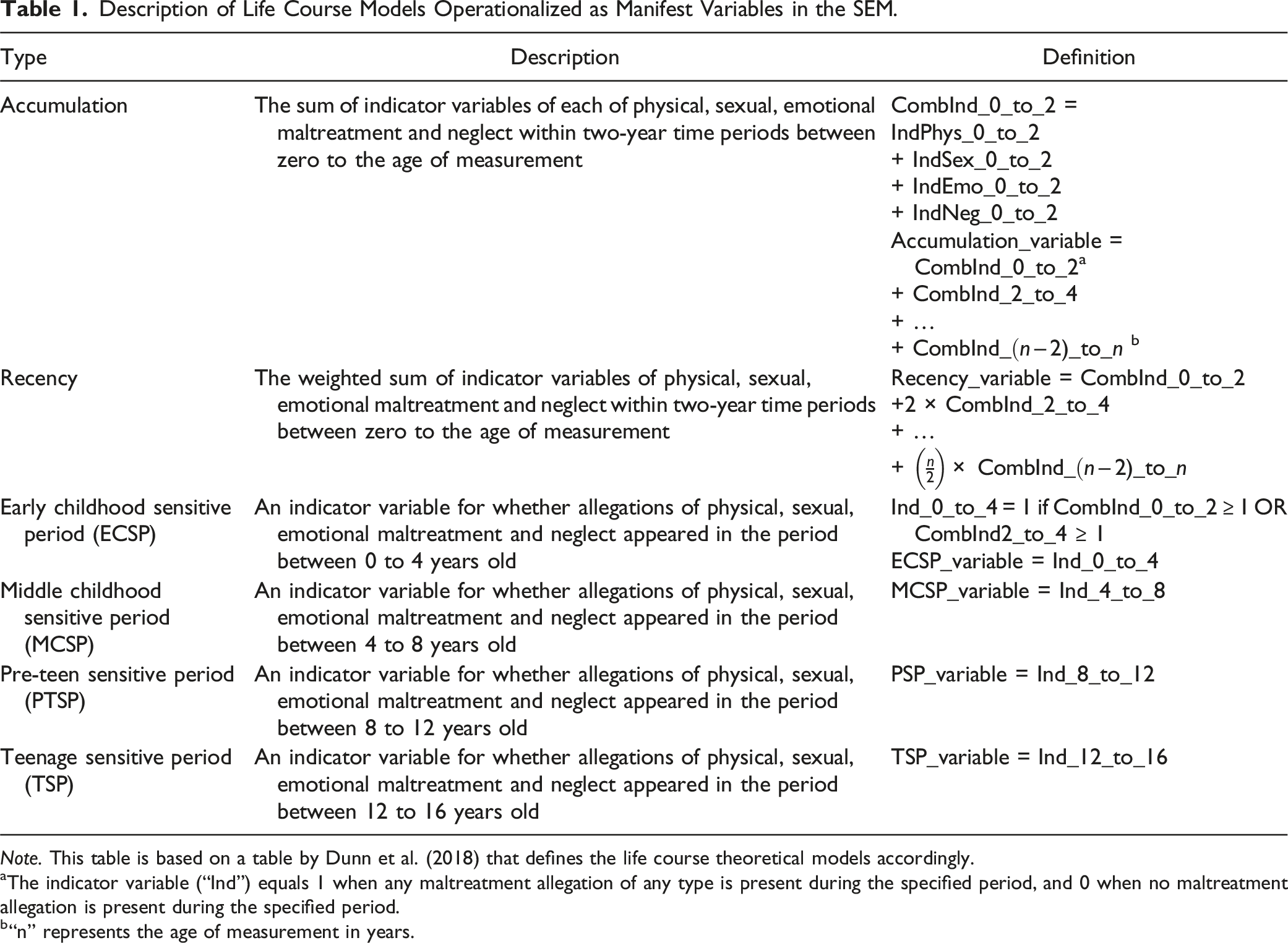
Note. This table is based on a table by Dunn et al. (2018) that defines the life course theoretical models accordingly.
aThe indicator variable (“Ind”) equals 1 when any maltreatment allegation of any type is present during the specified period, and 0 when no maltreatment allegation is present during the specified period.
b“n” represents the age of measurement in years.
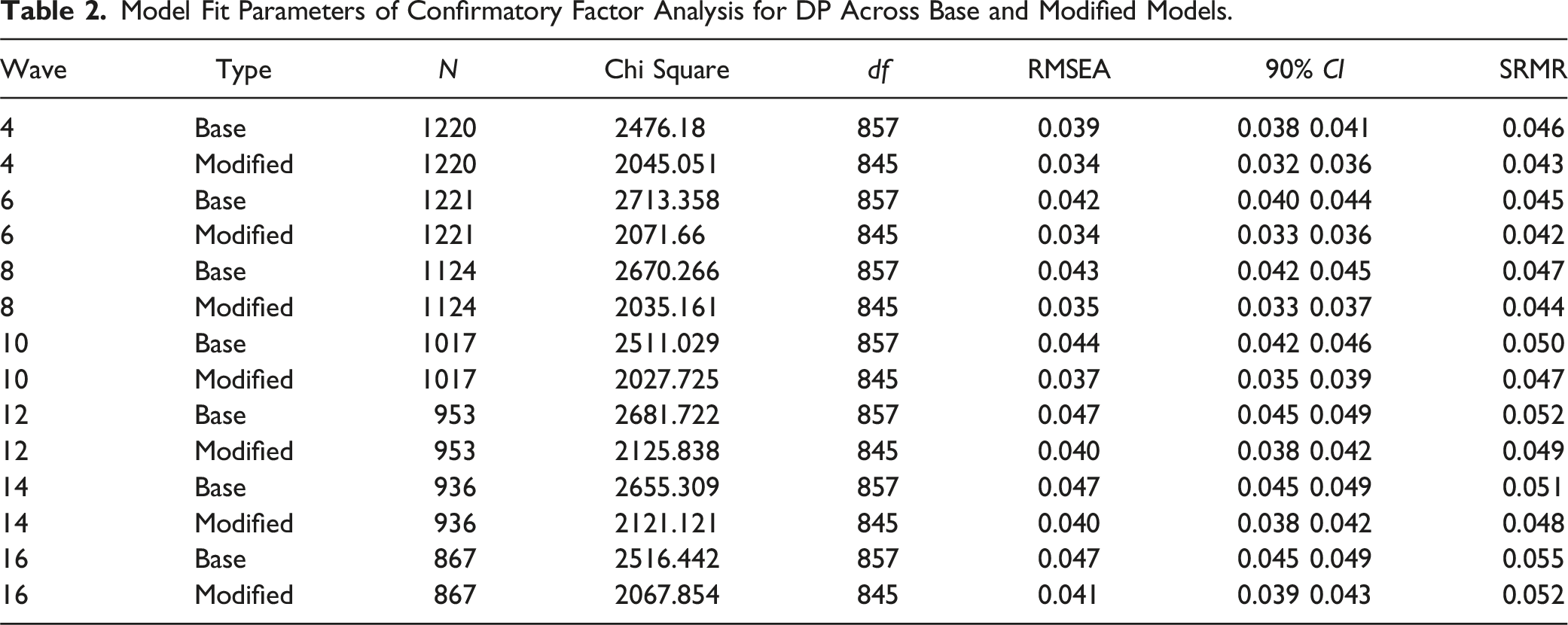
Confirmatory factor analysis (CFA) using maximum likelihood parameter estimation with robust standard errors was applied as the data was distributed normally. The root mean square of approximation (RMSEA) and the standardized root mean square residual (SRMR) indexed fit. RMSEA <0.05 indicated close fit, RMSEA <0.08 reasonable fit (Browne & Cudeck, 1993), and SRMR <0.08 good fit (Hu & Bentler, 1999). Comparison of structural models at each wave was determined using Akaike Information Criteria (AIC), with the lowest AIC being selected. AIC weights were calculated from the AICs to demonstrate the probabilistic difference between the models. AIC weights are calculated using the difference between the model’s AIC and the smallest AIC among the models, then calculated as a proportion of the sum of each of these differences (Wagenmakers & Farrell, 2004). They can be understood as the “probability that [the model] is the best model, given the data and the set of candidate models” (Wagenmakers & Farrell, 2004, p. 194). AIC and related information criteria provide estimates of out-of-sample prediction error; that is, they anticipate how well a model can predict future data. They accomplish this by including penalty terms for the number of free parameters, which corrects for the ability of more complex models to more easily overfit the current data. A model with more parameters (and thus more flexibility) must not only outperform simpler models, but do by enough to also overcome this overfitting penalty. However, AIC only estimates out-of-sample prediction error up to a constant for a given sample of outcome values. As such, the absolute scale of AIC scores is meaningless; only the relative values matter among a collection of models that have been applied to the same sample, with the lowest AIC (i.e., lowest estimated error) being favored (for details, see McElreath, 2018).
To examine potential covariates, relations between demographics and the manifest DP variable (summed CBCL Aggressive Behavior, Attention Problems, Anxious/Depression subscales) indicated that gender had a minor effect on the manifest DP variable, while both race and site had a major effect at each wave. As site closely captured the racial patterns, χ2 (12, Ns = 868–1221) = 310.48–431.14, ps < .001), only site was subsequently included as a covariate in the cross-sectional models. Given the variability in items assessing treatment exposure across sites and substantive differences in access, models including both covariates failed to converge. As such, we use site as a proxy for treatment as well. The latent DP factor was regressed upon the LCMs and covariates in structural models at each wave. If the R2 estimate was statistically significant using a Bonferroni-corrected critical p-value (p < .05/𝑛 comparisons), the model result estimates, standard errors, standardized model result estimates, and model result p-values for that LCM are reported.
Results
Measurement Models
Model Fit Parameters of Confirmatory Factor Analysis for DP Across Base and Modified Models.
Structural Models
Prediction of DP by Each LCM Sorted by Wave.
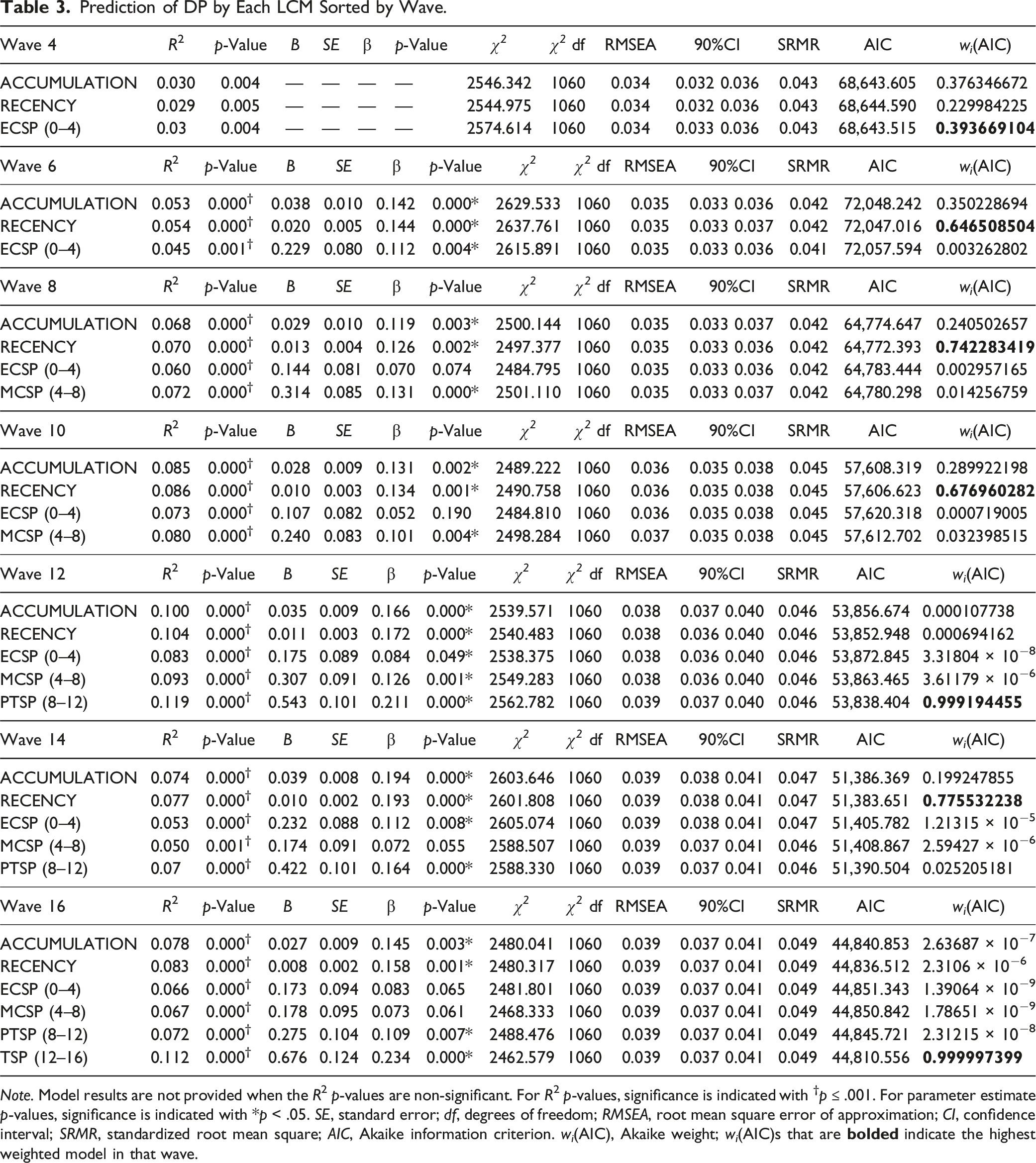
Note. Model results are not provided when the R2 p-values are non-significant. For R2 p-values, significance is indicated with †p ≤ .001. For parameter estimate p-values, significance is indicated with *p < .05. SE, standard error; df, degrees of freedom; RMSEA, root mean square error of approximation; CI, confidence interval; SRMR, standardized root mean square; AIC, Akaike information criterion. w
i
(AIC), Akaike weight; w
i
(AIC)s that are
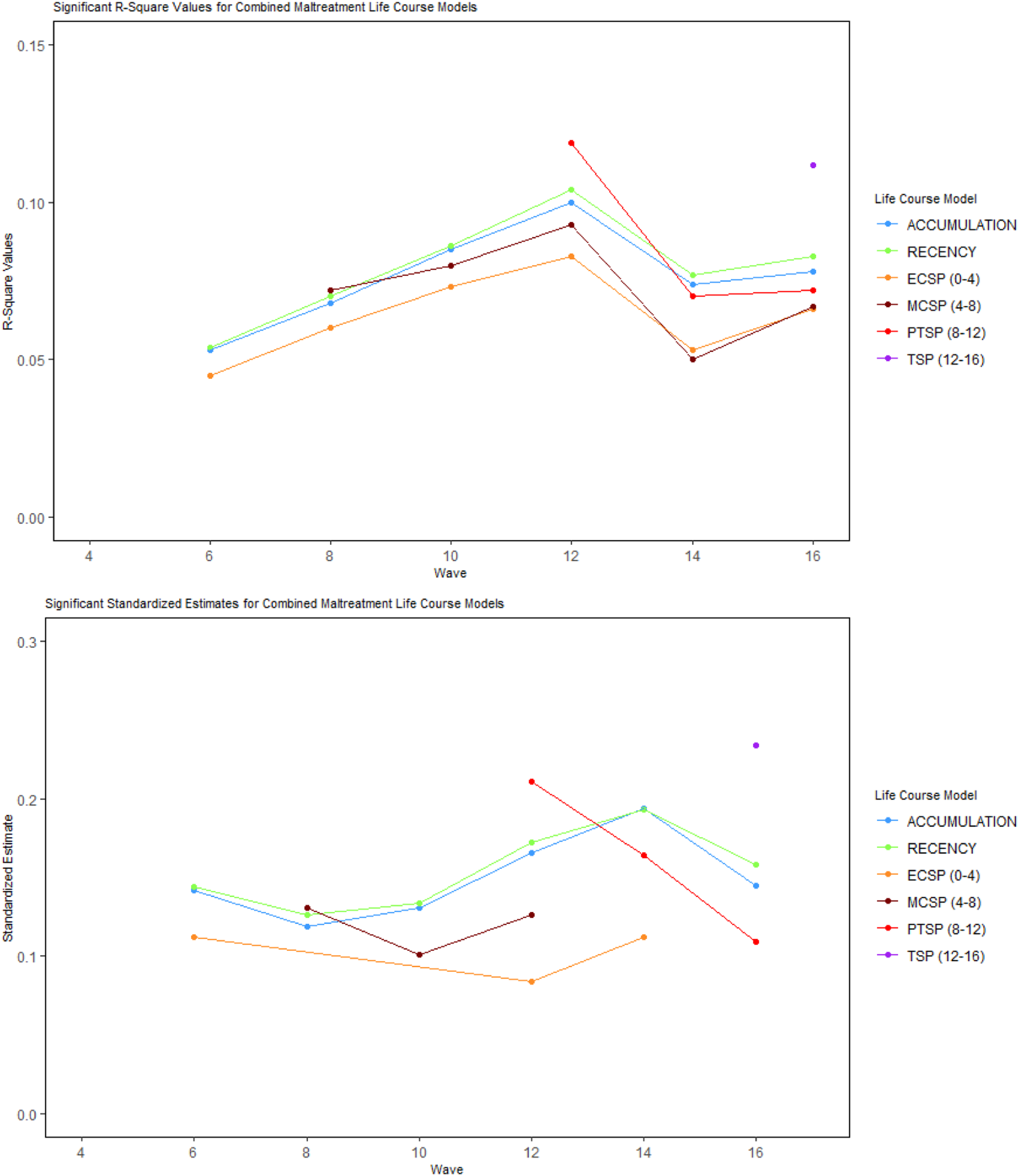
Model R2 (top; p < .001) and standardized parameter estimates for statistically significant LCMs (bottom; p < .05).
Standardized Model Estimates for Each LCM Across Each Wave.
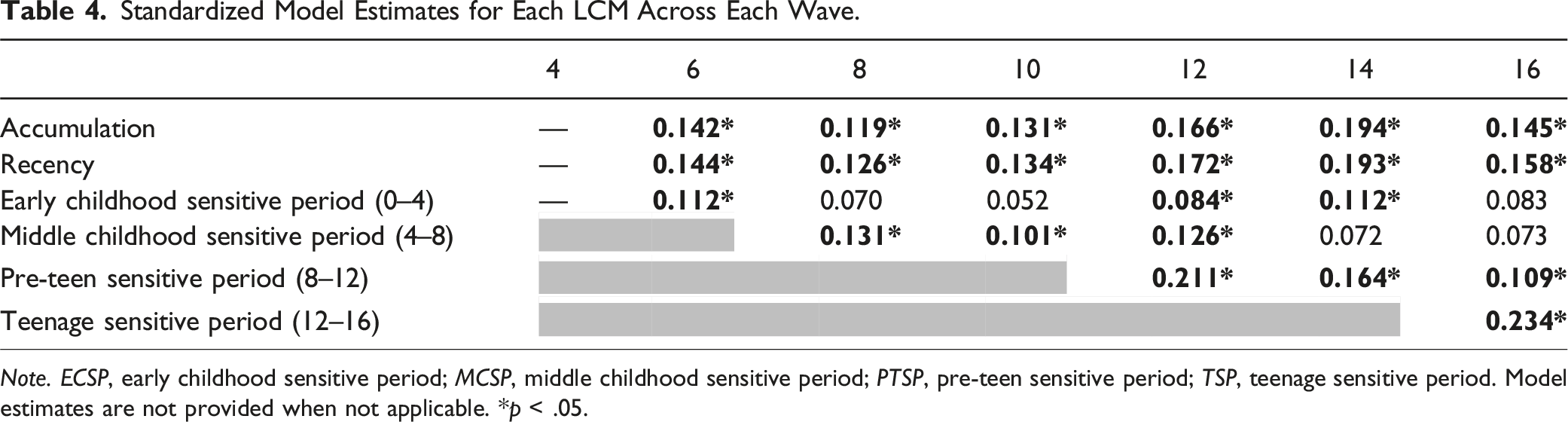
Note. ECSP, early childhood sensitive period; MCSP, middle childhood sensitive period; PTSP, pre-teen sensitive period; TSP, teenage sensitive period. Model estimates are not provided when not applicable. *p < .05.
Discussion
We examined relations between LCMs and general psychopathology, using the DP framework. Three LCMs with strong empirical and theoretical support were tested: the accumulation, recency, and sensitive period LCMs. We estimated the degree to which each CM LCMs explained general psychopathology outcomes from birth to 16 years of age. All three models related to psychopathology and explained larger proportions of the variance than found previously. Overall, the recency LCM best explained general psychopathology with slightly larger effect sizes than the accumulation LCM across age. Furthermore, the model with the recency variable had the best model fit across the most waves. The sensitive periods most proximal to the DP assessment were the most robust, consistent with Russotti et al. (2021) where recent CM was most predictive of future psychopathology. Unique to this study, the ECSP and MCSP LCMs influenced psychopathology in adolescence as well as in earlier childhood, suggesting a delayed effect. Our findings are consistent with previous findings that CM has small direct causal effects on mental health, whether assessed cross-sectionally or longitudinally, for different mental health outcomes, and across sex and age (Baldwin et al., 2023).
These results provide support for both the recency and accumulation theories. The recency model was generally the best performing, and proximal sensitive periods served as the most explanatory LCM for those periods. Taken in combination, this appears to provide support for the recency theory - namely, that CM proximal is more influential in explaining psychopathology contemporaneously than CM occurring earlier. The mechanism underlying this pattern is unclear. However, resilience theory suggests that people exposed to traumatic events may initially experience symptomatology, then after some time evidence a trajectory of gradual recovery to reach normal functioning (Bonanno et al., 2011).
It is unclear whether the recency model’s effects were a product of recency itself or its overlap with the accumulation model. Recency and accumulation models were very highly correlated, with values greater than 0.90 across all waves, limiting our ability to interpret these models separately. The recency model effect sizes were equal or slightly better than the accumulation model effects, but these differences were not substantial. As these models generally outperformed the sensitive period models, this lends support to the cumulative (summative frequency) model of CM (Appleyard et al., 2005). This aligns with previous research finding stronger associations between the dose-response/periodic frequency models of CM and psychopathology than sensitive period models (Jaffee & Maikovich-Fong, 2011; Jonson-Reid et al., 2012; Mackenzie et al., 2011; Russotti et al., 2021). Recent evidence suggests emotional regulation may mediate relations between childhood adversity and psychopathology (Miu et al., 2022). Emotional dysregulation plays a central role in DP (Masi et al., 2015), forming part of the persistent vulnerability profile for psychopathology. As emotion regulation changes across the lifespan (Ruba & Pollak, 2020), this may explain why the accumulation model generally outperformed other LCMs; patterns of pervasive CM may lead to consistent disruptions in the healthy development of emotional regulation, leading to worse psychopathology outcomes over time.
These results provide only limited support the sensitive period model. This model predicts that CM experienced in a specific period are more influential in terms of future functioning than CM experienced in any other period; our results do not align with this prediction. All four sensitive period LCMs had their strongest effects when first introduced, with reduced influence on psychopathology as time passed (excluding TSP assessed at a single timepoint). This finding is consistent with previous findings showing a lack of consistent sensitive periods across a variety of child outcomes (Schaefer et al., 2022). Since there was no consistent sensitive period found to be influential at multiple timepoints, but rather only when the sensitive period was proximal to the outcome measurement timepoint, this finding was interpreted as supporting the recency model rather than the sensitive period model. One explanation for this inconsistency could be that different child outcomes may have different sensitive periods. For instance, a systematic review of the link between CM and depression found that exposure to CM in middle childhood led to the highest risk of developing depression at any age (Li et al., 2023), while exposure to violence between birth and three years old was associated with greater externalizing symptoms than exposure to violence at older ages (Dunn et al., 2020). Sensitive periods may also be less detectable in models incorporating composite measures of maltreatment rather than individual types (Schaefer et al., 2022). In any case, our study examined which temporal pattern of CM best explained general psychopathology, and the sensitive period model provided the worst account for these changes.
An important theoretical point is that none of these temporal models of CM are mutually exclusive. Temporal patterns of psychopathology may be the result of a combination of the effects of accumulation, recency, and sensitive periods. Our study indicates that both accumulation and recency effects may be present, each potentially explained by different mechanisms. Advancing our theory in this regard will require further longitudinal work testing potential mechanisms involved in accumulation and recency, such as disruptions to emotional regulation development. Trajectory approaches are particularly informative when considering such time-varying predictors.
This study demonstrates several strengths. This is the first study to utilize a measure of general psychopathology in testing the effects of the temporal dimension of CM. Given the value of general psychopathology factors as indicators of clinical impairment, this study demonstrates developmental associations between combined maltreatment and impairment broadly construed. The use of a large, national prospective longitudinal sample of children afforded the opportunity to extend the time period of assessment from previous work (Li & Godinet, 2014) and provide a more holistic view of psychopathology. The two-year assessment periods also afford a greater number of observational periods than Russotti et al. (2021) work. As the data was captured prospectively from case files, we avoid the self-presentation bias and memory-related issues associated with retrospective self-report (Greenhoot, 2011; MacMillan et al., 2003) and rule out the possibility that recency effects can be explained solely by recall bias. The LONGSCAN sample was intentionally selected to maximize the degree of CM measured, thus increasing the number of incidents available and the capacity for the LCM model to predict psychopathology outcomes. We specifically accounted for site differences in the models, given the variability between sites in study conditions, sample characteristics, data collection, and access to treatment (Runyan et al., 2020).
This work also has limitations. Since the LONGSCAN sample is comprised of children at high-risk of CM, the generalizability of findings to lower-risk populations is limited. Furthermore, we were unable to assess the effects of mental health treatment on the sample. Given that access to treatment was conflated with study location, and that operationalization of treatment varied greatly across years and locations, model convergence was negatively impacted as a result. Location was the covariate used in analysis to address this limitation but is not optimal. Additionally, we had the choice of allegations, validated reports, and substantiated reports to operationalize CM. Empirical work has shown that the risk experienced by children who are the subject of unsubstantiated reports is often equally high as substantiated reports, reflected in rates of entry into special education (Jonson-Reid et al., 2004), subsequent placement into foster care (Kohl et al., 2009), and a wide range of developmental, cognitive, emotional, and substance use outcomes (Casanueva et al., 2012). Moreover, we largely adhered to the operationalization of the LCMs by Dunn et al. (2018) which had substantial overlap between accumulation and recency models, leading to very high correlations between the models in our sample. Other operationalizations of accumulation and recency should be explored in future work. This issue contributed to collinearity of the LCMs, requiring us to run these models separately. Another issue concerning the operationalization of the LCMs was that the accumulation and recency models had greater variability in their scores compared to the sensitive period operationalization, which may have advantaged the former LCMs over the latter in the model comparisons. A potential future direction would be to examine the LCMs under different operationalizations so that the models can be tested simultaneously, as this would allow stronger claims to be made for favoring one model over another. Finally, the nature of this study aimed to capture the general effects of a broadly defined CM on a general factor of psychopathology, DP. The accumulation and recency variables captured the quantities of different types of maltreatment in their operationalizations, while the sensitivity period was operationalized as an indicator of whether any of the different types of maltreatment occurred. Given that these operationalizations aggregated multiple types of maltreatment and types of outcomes in different ways, a new approach may be necessary to determine causal risk mechanisms of specific types of maltreatment for specific outcomes.
Our findings have important clinical implications. Clinicians should seek to capture timing information in their CM screening to improve prediction of general psychopathology (English et al., 2005). This information may help clinicians tailor their therapeutic strategies in accordance with the expected trajectory of psychopathology symptoms. While prevention efforts should ideally target children of all ages at risk of CM, these results imply that we should prioritize efforts targeting children who are likely to experience abuse across multiple developmental periods (Hindley et al., 2006). Risk factors for a high periodic frequency of CM should be investigated and identified to fine-tune effective prevention efforts. Furthermore, the acute effects of proximal CM on psychopathology suggests that additional clinical attention should be paid to children who have recently experienced CM, regardless of age. Our results underline the need for a stronger theoretical base for the chronic and recency models of CM and reinforce the explanatory value of the temporal dimension of CM for general psychopathology.
Supplemental Material
Supplemental Material - Life Course Models of Child Maltreatment: Effects on General Psychopathology Outcomes in a Longitudinal Sample
Supplemental Material for Life Course Models of Child Maltreatment: Effects on General Psychopathology Outcomes in a Longitudinal Sample by Dylan Wong, and Kristen G. Anderson in Child Maltreatment.
Footnotes
Acknowledgments
The authors would like to thank Gregory Jensen, PhD for his feedback on statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.