
Abstract
Persistent substance use during the transition into adulthood increases risk for long-term mental and physical health problems. Participants (N = 483) and their caregivers were recruited at age 4 years due to exposure to (or high risk for) child abuse and/or neglect. Data on adverse childhood experiences (ACEs) were collected prospectively during participant ages 0–18 years between the 1990s and early 2000s. In 2012, participants reported past 12-month substance use at a follow-up online survey in young adulthood (Mage = 23.8). A latent class analysis using nine dichotomous substance use indicators was fit to the data. Comparative fit indices favored a 4-class solution characterized by (1) high rates of tobacco and cannabis use (n = 66), (2) high rates of heroin/non-prescription opioid and non-prescription tranquilizer/sedative use (n = 21), (3) high rates of poly-substance use (n = 21), and (4) low rates of substance use (n = 375). Abstainers generally experienced fewer childhood adversities and adult IPV exposure relative to other classes and tended to report less substance use as adolescents. This work reinforces the prospective association between childhood adversity and problematic patterns of substance use observed in young adulthood, and offers key implications for providers, researchers, and policymakers.
Experimentation with drugs and alcohol is a normative practice among adolescents, but continued use into early adulthood increases risk for long-term mental, physical, and socioeconomic challenges (Kertesz et al., 2012; Lovell et al., 2018). Person-centered analytic techniques have proven useful for identifying discrete groups of youth whose substance use diverges from normative adolescent experimentation (Dierker et al., 2007; Hyucksun Shin et al., 2010). While many socioecological factors can increase risk for adolescent substance use, adverse childhood experiences (ACEs) have emerged as a particularly salient risk factor. At present, the extant research in this area is based largely on cross-sectional samples and retrospective reporting of ACEs. Currently, there remains a dearth of scientific evidence surrounding patterns of substance use in young adulthood among individuals exposed to severe ACEs. To address this gap, the present study used latent class analysis to identify discrete patterns of substance use in young adults with significant ACEs exposure.
Substance Use and Associated Outcomes
Substance use among adolescents and young adults represents one of the largest and most preventable public health problems in the United States, with staggering consequences in both the short and long term. Drug and alcohol overdoses account for thousands of adolescent deaths each year (Ali et al., 2019), with an alarming spike observed during the COVID-19 pandemic (Lee & Singh, 2023). More indirectly, intoxication by substances is thought to play a crucial role in each of the top three leading causes of death for 12-19-year-olds – accidents, homicides, and suicides (Hall et al., 2016). When heavy substance use continues into adulthood, it is typically associated with a wide range of negative long-term outcomes, including psychiatric problems, physical health issues, neurocognitive deficits, and mortality (Kertesz et al., 2012; Lovell et al., 2018). Fortunately, most adolescents who experiment with drugs and alcohol do not develop long-term maladaptive substance use habits (Khurana et al., 2015). Of greater concern is the smaller proportion of youth whose alcohol and substance use becomes more entrenched, habitual, and impairing during the transition into adulthood.
Substance Use and Childhood Adversity
Substance use is prevalent in individuals who have experienced adverse childhood experiences (ACEs), such as poverty, abuse, neglect, family dysfunction or separation, and parental mental illness (Huang et al., 2011; Kristman-Valente & Wells, 2013). The mechanisms underlying the association between ACEs and substance use are complex. At the individual level, ACEs can disrupt core biological self-regulatory and reward-related processes that underlie impulse control and sensation-seeking (Novick et al., 2018). ACEs can also cause traumatic stress and other painful affective states, which individuals may seek to alleviate or numb through the use of substances (Hawn et al., 2020). At the interpersonal level, exposure to ACEs can steer individuals toward riskier peer groups where substance use is more socially accepted (Trinidad, 2021), increasing risk for further ACEs (e.g., via exposure to community violence; Evans et al., 2023). More broadly, various macro-level factors in the United States contribute to the conditions that predispose families to ACEs and substance use to begin with, including structural racism, economic inequality, limited educational opportunities, selective enforcement of drug policy, and insufficient public funding for social support services (Amaro et al., 2021; Settipani et al., 2018).
Heterogeneity in Substance Use Patterns
Person-centered analytic approaches have provided insight into the heterogeneity of substance use patterns among adolescents and early adults. This work confirms that substance use tendencies are not distributed normally. Rather, individuals tend to fall into discrete groups according to their preferred substance types and their frequency of use. Nationally-representative and community-based samples typically identify a large proportion of individuals who report little-to-no substance use, followed by 2-4 additional smaller “moderate” and “high-use” groups characterized by alcohol, tobacco, or polysubstance use (Gilreath et al., 2014; Lee et al., 2020; Patrick et al., 2020; Wu et al., 2020).
Given the strong link between childhood adversity and substance use, substance use patterns in populations with high ACEs exposure are likely to differ from those in general population samples. Yet, only a handful of studies have employed person-centered analyses to explore this possibility. Three studies reporting on samples of low-income adolescents involved in child welfare or enriched for maltreatment experiences identified 3-6 classes, including relatively high proportions of “heavy” or “poly” users (17-30%) and “moderate” alcohol and cannabis users (30-50%), and relatively low proportions of “low” or “abstinent” users (Hyucksun Shin, 2012; Hyucksun Shin et al., 2010; Rivera et al., 2018; S. M. Snyder & Smith, 2015). Other studies have characterized latent substance use patterns in young adult and adult samples that included maltreatment-exposed individuals (Armour et al., 2014; Snyder & Merritt, 2015; Snyder & Rubenstein, 2014). These studies, which relied on retrospective reports of childhood adversity and cross-sectional analyses, consistently found that maltreatment histories were associated with membership in higher-risk substance use classes. While informative, the practical application of this work remains limited. Most apparent is the consistent use of cross-sectional, retrospective reporting of ACEs. This is problematic in light of meta-analytic investigations confirming that retrospective reporting of adversity does not accurately capture the experiences of children as measured in longitudinal studies (Baldwin et al., 2019). Moreover, few studies have attempted to characterize substance use patterns in maltreated samples beyond adolescence. This work is critical because substance use that continues into adulthood is often indicative of more entrenched and enduring habits, whereas most adolescent substance users never develop long-term substance-related problems (Khurana et al., 2015). Characterizing substance use patterns among young adults is crucial, particularly among those whose childhood experiences have already increased their risk for maladaptive outcomes. Doing so can inform research on risk stratification, guide trauma-informed prevention and treatment practices, and support policies aimed at early intervention.
Present Study
The present study sought to address these crucial literature gaps by (1) identifying distinct patterns of substance use among young adults with histories of childhood adversity using LCA; (2) examining whether adversity – both in childhood (ACEs) and in adulthood (e.g., interpersonal violence [IPV], assault, traumatic loss) – were differentially associated with membership in these empirically derived classes; and (3) investigating how class membership related to key sociodemographic variables and functional outcomes, with the goal of clarifying which subgroups may be at greatest risk and thereby informing prevention, intervention, and policy efforts. Based on previous work, it was anticipated that 3–5 discrete classes would emerge from the data, comprising 1–2 “moderate use” classes (likely characterized by high rates of alcohol and/or tobacco use), a single “low-use/abstinent” class, and 1–2 smaller “high-use/poly-use” classes. Given the severity of adversity experienced by the current sample (e.g., child physical and sexual abuse, neglect), it was anticipated that a larger proportion of participants would fall in moderate and high-use classes compared to previous general population and community-based samples. Next, using longitudinal data, associations between key psychosocial/sociodemographic variables and class membership were examined, with a particular focus on the impact of prospectively-measured adversity across childhood and adolescence. We expected that these childhood stressors, as well as more contemporaneous stressors (e.g., intimate partner violence), would be associated with higher-use classes.
Methods
Sample and Procedures
Participants in the current study were a subset of individuals (N = 483) who participated in the Longitudinal Studies of Child Abuse and Neglect (LONGSCAN), a 30-year, prospective consortium of studies investigating the causes and consequences of child maltreatment (Runyan et al., 1998). The original LONGSCAN study identified and recruited 1354 children prior to age four, across five sites nationwide, due to their risk for Child Protective Services (CPS) involvement. Participants and their caregivers were then interviewed biannually from age four through 18 throughout the 1990s and early 2000s about the child’s development, family and neighborhood environment, and possible physical, sexual, and psychological abuse. CPS records were systematically and regularly coded to identify reports of alleged maltreatment for each child (English & LONGSCAN Investigators, 1997). Each LONGSCAN site obtained approval from their respective institutional review boards and written, informed consent/assent was acquired from all participating caregivers and children.
The current study combined prospective LONGSCAN data with additional data from a follow-up online survey in 2012 examining participants’ substance use as young adults (Mage = 23.78, SD = 1.95). Eligibility for the follow-up survey included the presence of at least one interview at age 14, 16, or 18, and at least four interviews between ages 4 and 18. 1,053 young adults met eligibility criteria, 483 (45.9%) of which completed the follow-up survey over a 3-4 year period beginning in 2012. Eligible participants who did vs. did not complete the follow-up survey differed on only a few variables. The Northwest site had a higher percentage of survey-completers than the other sites, while the Southern site had fewer respondents (χ24 = 50.60, p < .001). More females than males completed the survey (61.5% vs. 46.1%, χ21 = 29.37, p < .001). Other variables of interest were not associated with completion status (Dubowitz et al., 2019).
Measures
Sociodemographic Information and Recent Life Experiences
Participants self-reported their age, gender, race, high school graduation status, employment status, past-year status as a student, parental status, perceived physical health, and incarceration since age 18. Aside from age (continuous), race/ethnicity (four categories: White, Black, Hispanic, Multiracial/Other) and physical health (single, Likert-type item rated from 1 to 5), all sociodemographic variables were dichotomous (0 = no, 1 = yes).
Adult Substance Use
Participants self-reported their adult substance use via an adapted version of the National Survey on Drug Use and Health (Substance Abuse and Mental Health Services Administration, 2014). Specifically, participants reported on their past-12-month and past-30-day use of alcohol, cannabis, tobacco, cocaine, heroin, amphetamines, hallucinogens/ecstasy, non-prescription stimulants, and non-prescription sedatives/tranquilizers. Example items include: “During the past 30 days, on how many days did you have at least one drink of an alcoholic beverage”; “Have you used cocaine, in any form, during the past 12 months?” When participants endorsed using a particular substance, they were then prompted to answer questions assessing DSM-5 use disorder symptoms. The substance use-related items in the National Survey on Drug Use and Health have demonstrated excellent validity and reliability (Substance Abuse and Mental Health Services Administration, 2010).
Age 18 Substance Use
Participants self-reported their substance use when they were 18 years old via two measures: (1) a LONGSCAN-developed measure of tobacco, alcohol, drugs, and involvement in drug-related activities, derived from the Youth Risk Behavior Survey, Monitoring the Future Study, and the CHAMPS Study (W. Hunter et al., 2003); and (2) the substance use disorder scales of the National Institute of Mental Health Diagnostic Interview Schedule for Children—Youth IV (DISC-IV) (Shaffer et al., 1996). Both measures have good validity and reliability (Crowley et al., 2001; Dugré et al., 2020; Roberts et al., 1996).
Adverse Childhood Experiences (ACEs)
A summed index of the number of ACEs youth experienced between birth and the age 18 interview was created post-hoc based on eight dichotomous indicators (caregivers’ mental health problem, family member substance use or incarceration, witnessed family violence, and alleged child neglect, and physical, sexual, and emotional abuse), as is consistent with the ACEs survey developed by the Adverse Childhood Experiences Studies (Bynum et al., 2010; Dube et al., 2002). The specific measures used to create each of the eight indicators are described in supplemental materials.
Adult Traumatic Experiences and IPV
As part of the young adult survey, participants completed the LONGSCAN-developed Life Events checklist (Runyan et al., 1998) and the Revised Conflict Tactics Scales: Partner-to-Partner (CTS-2; Straus et al., 1996). The present study used two items from the Life Events checklist to determine whether participants experienced the death of a close family member and/or were the victim of an assault within the past year, as well as four subscales from the CTS-2 to assess experiences of IPV: Psychological Aggression, Physical Assault, Sexual Coercion, and Injury (e.g., had sprain/bruise, broken bone). Items were dichotomized before being summed into their respective subscales, as has been recommended by the measure’s authors (Morrison et al., 2023; Straus, 2008).
Data Analysis
The present investigation used latent class analysis (LCA) to identify discrete groups of youth based on their patterns of substance use. All analyses were conducted with Mplus version 8.1.5 (Muthén & Muthén, 2017). Nine dichotomous indicators of substance use (0 = no, 1 = yes) were included in the LCA: presence of two or more (1) alcohol and (2) cannabis use disorder symptoms; (3) any past-30-day tobacco use; and any past 12-month use of (4) cocaine, (5) opioids, (6) amphetamines, (7) hallucinogens/ecstasy, (8) non-prescription stimulants, and (9) non-prescription sedatives/tranquilizers. The dichotomous indicators for alcohol, cannabis, and tobacco use were defined using different severity/frequency criteria than the other substance use indicators for several reasons. Chiefly, alcohol, cannabis, and tobacco are more culturally accepted in the U.S. relative to the other included substances (Hathaway et al., 2011). They are also used more prevalently. This is reflected in the large proportion of the current sample who reported any past-12-month alcohol use (74%), cannabis use (43.6%), and tobacco use (43.2%), compared to past-12-month use of cocaine (4.6%), opioids (9.9%), amphetamines (4%), hallucinogens/ecstasy (8%), non-prescription stimulants (4.6%) and non-prescription sedatives/tranquilizers (4.8%). Any past-12-month use of alcohol, cannabis, and tobacco – alcohol in particular – is not likely to be a meaningful or clinically useful indicator. Finally, alcohol, cannabis, and tobacco use is associated with less functional impairment than use other substances, such as opioids, amphetamines, and cocaine (Center for Behavioral Health Statistics and Quality, 2021). For these reasons, the alcohol and cannabis use indicators were defined not as past-12-month use, but as “presence of two or more use disorder symptoms,” which represents the minimum number of symptoms required to meet criteria for an alcohol or cannabis use disorder. Tobacco use disorder symptoms were not assessed during data collection, so the tobacco use indicator was defined as “any past-30-day use.” When defined in this way, endorsement rates for the alcohol (19%), cannabis (20.1%), and tobacco (35.8%) use indicators more closely matched the endorsement rates for the other substance use indicators, which typically enhances class differentiation and improves interpretability of the final class solution (Weller et al., 2020).
To minimize the risk of local maxima, all models were estimated with multiple random sets of starting values. Model identification was confirmed by replication of the maximum loglikelihood across random starts and convergence with no optimization warnings, and only well-identified solutions were retained for interpretation. Missing data on the substance-use indicators were handled using full-information maximum likelihood (FIML) estimation with robust standard errors in Mplus, such that all available data contributed to parameter estimation under the assumption of missing at random. To account for potential non-independence of participants within recruitment sites, all latent class models were re-estimated using a complex mixture framework in Mplus with site specified as a clustering variable. This adjustment, which applies robust (sandwich) corrections to standard errors and fit statistics, yielded an identical class structure and comparable model fit, indicating that within-site dependence did not bias the results. Multiple fit indices were used to select the best-fitting class solution. Lower values on the Akaike Information Criterion (AIC; Akaike, 1987) Bayesian Information Criterion (BIC; Schwarz, 1978) and sample size-adjusted Bayesian Information Criterion (SSA-BIC; Sclove, 1987) indicate comparatively better fitting class solutions. Higher entropy values indicate greater distinction between classes within a solution. Significant Lo-Mendell-Rubin (LMR) and Bootstrapped likelihood ratio tests (LRT) indicate that a class solution is a significantly better fit than the model with one fewer class (Lo et al., 2001). A non-significant p-value for the G2 statistic indicates adequate model fit. Interpretability of the classes of a solution (e.g., class size, item thresholds) was also considered, with preference given to class solutions with classes of 20 individuals or more (4% of the sample).
Given that an interpretable class-solution was established, a secondary aim of this study was to explore how class membership varied on several different variables. A particular focus was on participants’ exposure to ACEs between 0-18 years old and their prior substance use in adolescence (i.e., age 18), both measured prospectively. We also examined class differences across several young adult psychosocial variables known to be associated with substance use (trauma and IPV exposure, incarceration, physical health), as well as several sociodemographic variables for exploratory purposes (gender, race/ethnicity, high school graduation status, parenthood, current employment status, past-year status as a student). Class differences were assessed using the automatic Bolck, Croon, and Hagenaars (auto-BCH) method (Asparouhov & Muthén, 2014; Bakk & Vermunt, 2016). The BCH framework provides Wald chi-square tests that adjust for classification error and unequal variances, offering a more rigorous alternative to traditional cross-tabulation. The goal in these analyses was descriptive, characterizing how classes differed on key outcomes rather than predictive modeling of class membership. The false discovery rate procedure by Benjamini-Hochberg was used for multiple comparisons (Benjamini & Hochberg, 2000).
Results
Missing Data, Bivariate Associations, and Descriptive Statistics
Sociodemographic Characteristics of Study Participants
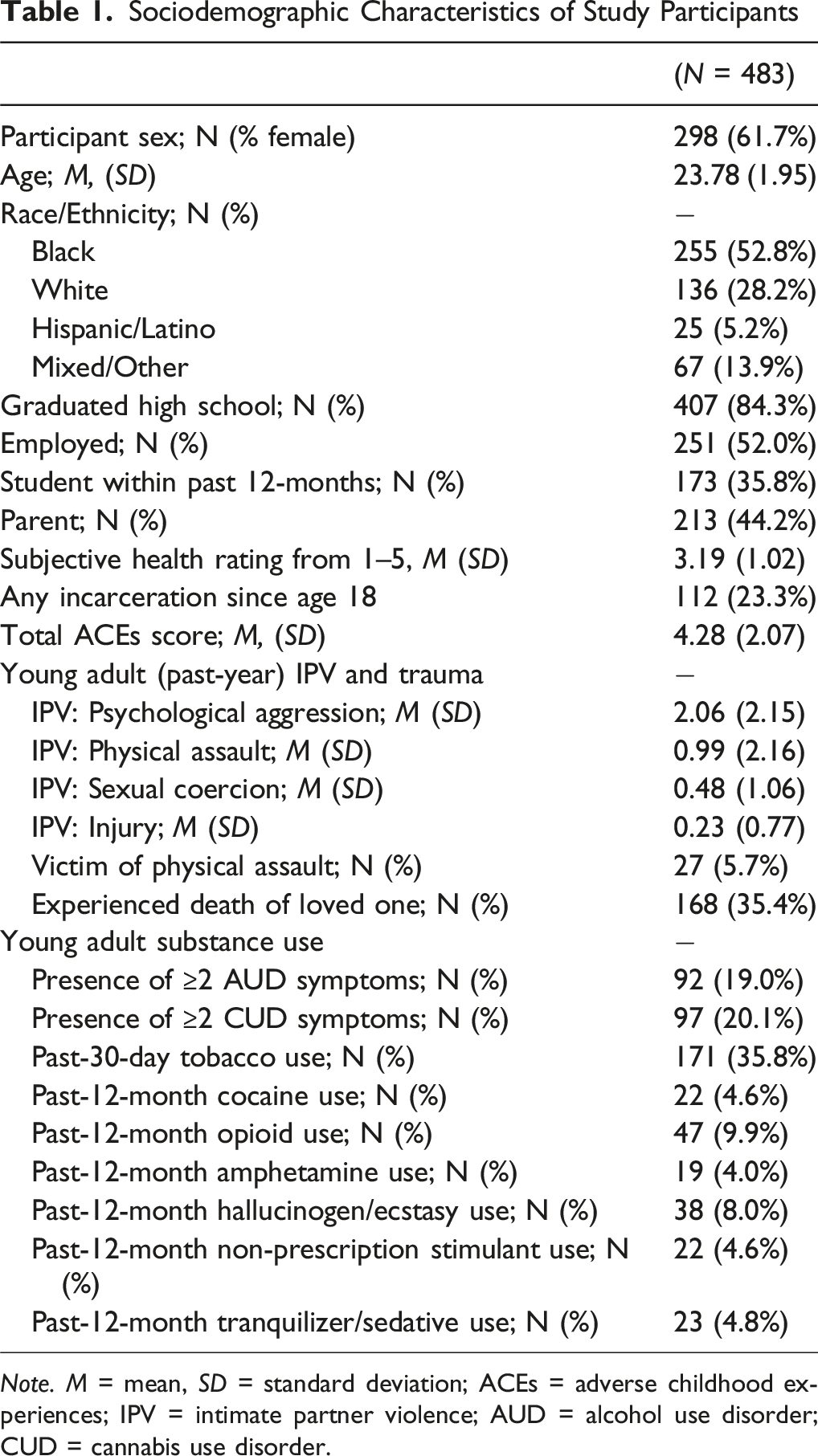
Note. M = mean, SD = standard deviation; ACEs = adverse childhood experiences; IPV = intimate partner violence; AUD = alcohol use disorder; CUD = cannabis use disorder.
LCA
Determining the Best-Fitting Class Solution
One-through five-class solutions were estimated and their fit was compared (supplemental materials Table S2). The four-class solution was identified as the best-fitting solution based on (1) a decrease in the AIC and SSA BIC, (2) a high level of entropy relative to the three- and five-class solutions, which was reflected in distinct item probabilities across the classes, (3) a significant LMR LRT and bootstrapped LRT, (4) a non-significant G2 statistic, and (5) class sizes that were considered interpretable. In evaluating class size, we considered not only statistical guidelines but also interpretability and clinical relevance. While some authors recommend a 5% minimum threshold for class size (Lanza et al., 2007), more recent work emphasizes that smaller classes may be appropriate when they represent theoretically anticipated or substantively meaningful subgroups and are well distinguished from other classes (Masyn, 2013; Nylund-Gibson & Choi, 2018). Simulation studies have further shown that small classes can be reliably recovered under adequate sample sizes and strong separation between latent groups (Tein et al., 2013). In the present study, the two smallest classes represented 21 participants each (4.3% of the sample). Despite their size, these classes were highly distinct and captured participants endorsing elevated rates of “hard” and illicit substance use – a subgroup we expected to comprise a minority of the sample but whose clinical importance warranted retention. Thus, we considered these classes interpretable, replicable, and substantively important.
Interpretation of the Four-Class Solution
Item probabilities for the four classes are depicted in Figure 1 and in Table S3. Based on these probabilities, the four classes were given the subjective labels of “Smokers,” “Depressant Users,” “Poly-users,” and “Abstainers.” Latent class probabilities for each substance.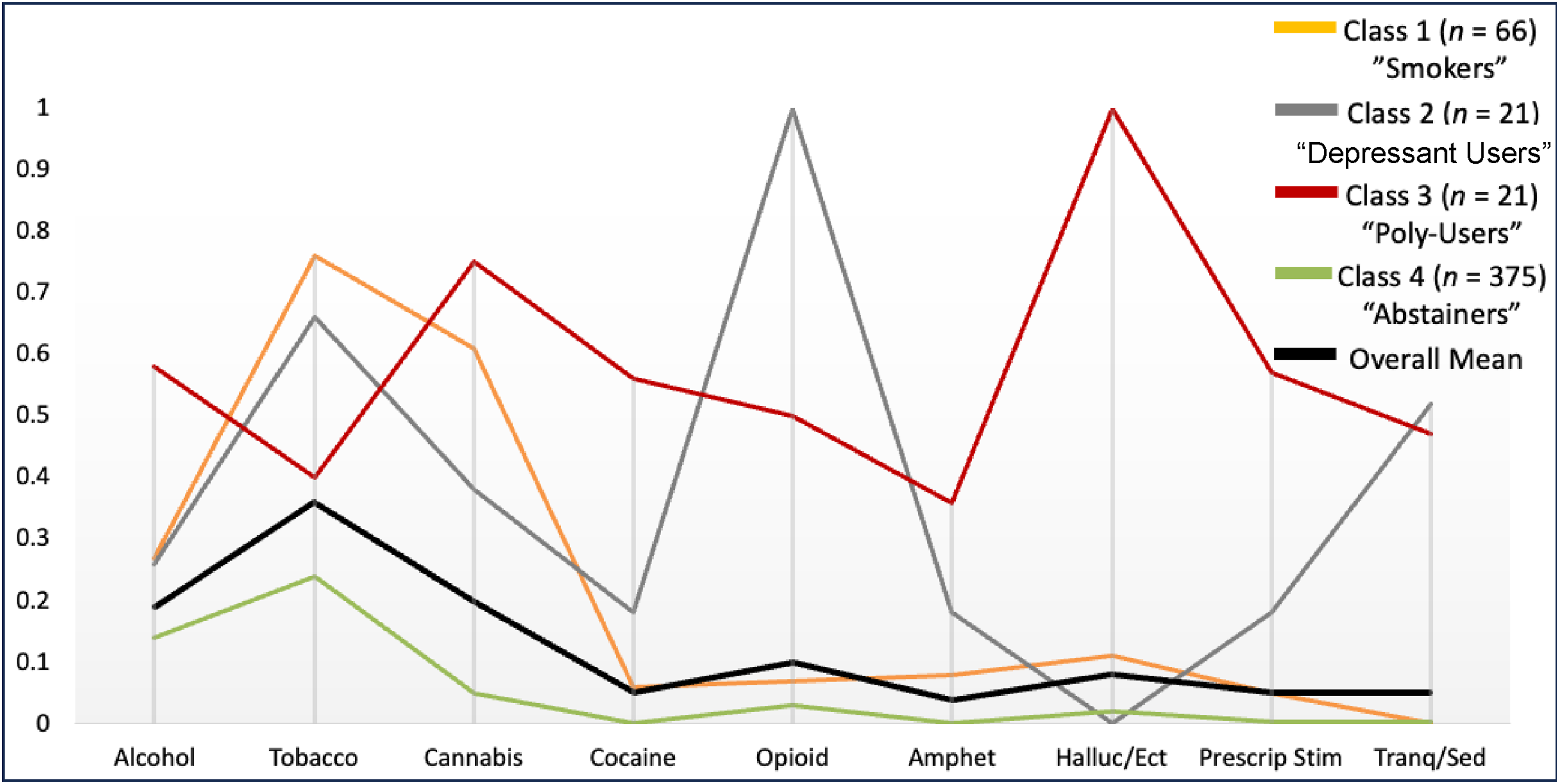
“Smokers” (n = 66, 13.7% of the sample) were characterized by a high probability of past-30-day tobacco use (.76) and presence of ≥2 cannabis use disorder symptoms (0.61) relative to the sample means of 0.36 and 0.21, respectively. “Depressant Users” (n = 21, 4.3%) were characterized by 100% endorsement of past-12-month opioid use, as well as a high probability of non-prescription tranquilizer/sedative use (0.52) relative to the sample mean (.01). “Poly-users” (n = 21, 4.3% of the sample) showed high probabilities of endorsing all substances compared to the sample means. Finally, “Abstainers” (n = 375, 77.6% of the sample) had little-to-no probability of endorsing illicit or non-prescription substances.
Predictors of Class Membership
χ2 Values for Equality of Means Test: Class Comparisons by ACEs, Past-Year Trauma, and IPV
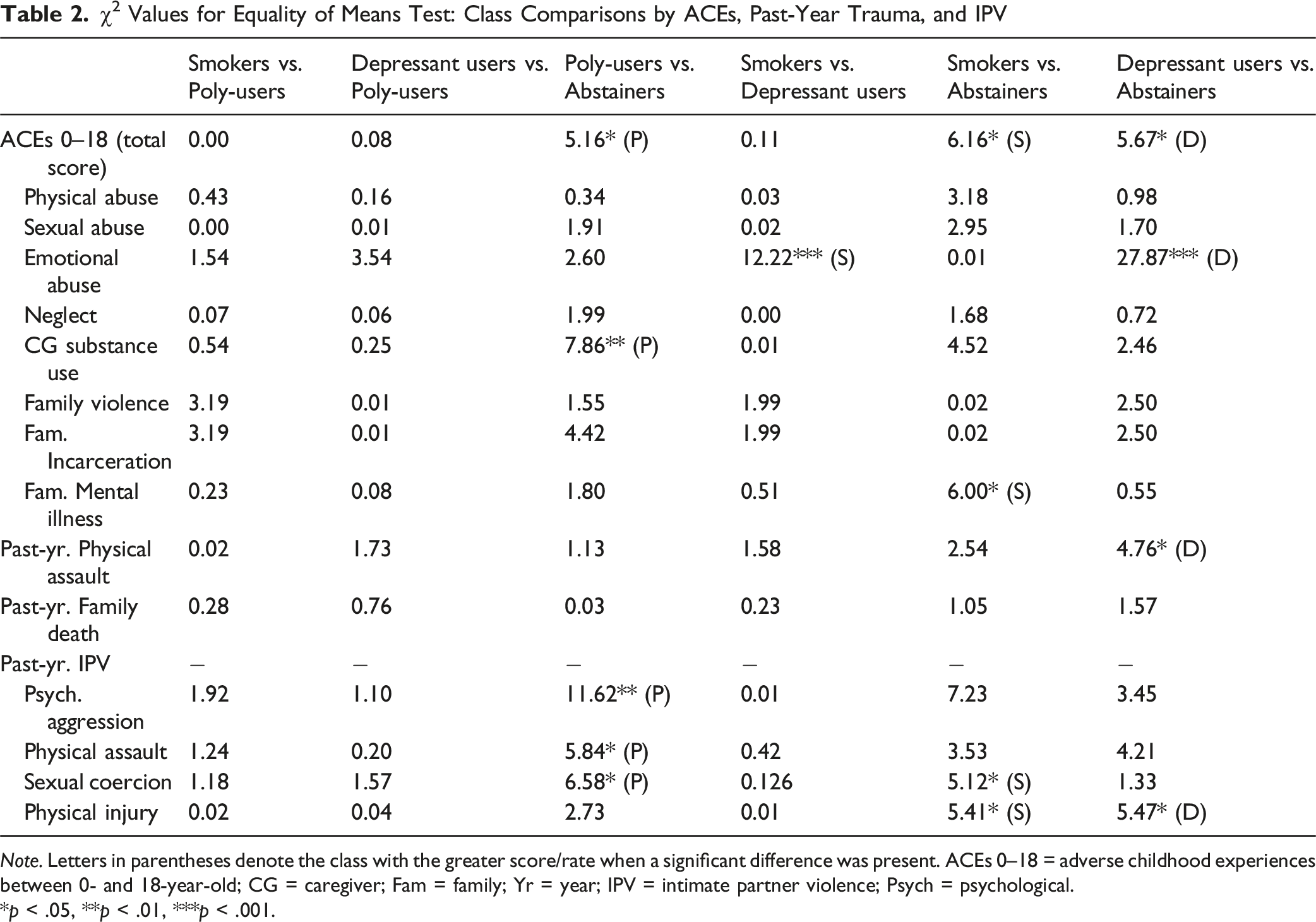
Note. Letters in parentheses denote the class with the greater score/rate when a significant difference was present. ACEs 0–18 = adverse childhood experiences between 0- and 18-year-old; CG = caregiver; Fam = family; Yr = year; IPV = intimate partner violence; Psych = psychological.
*p < .05, **p < .01, ***p < .001.
χ2 Values for Equality of Means Test: Class Comparisons by Sociodemographic Variables
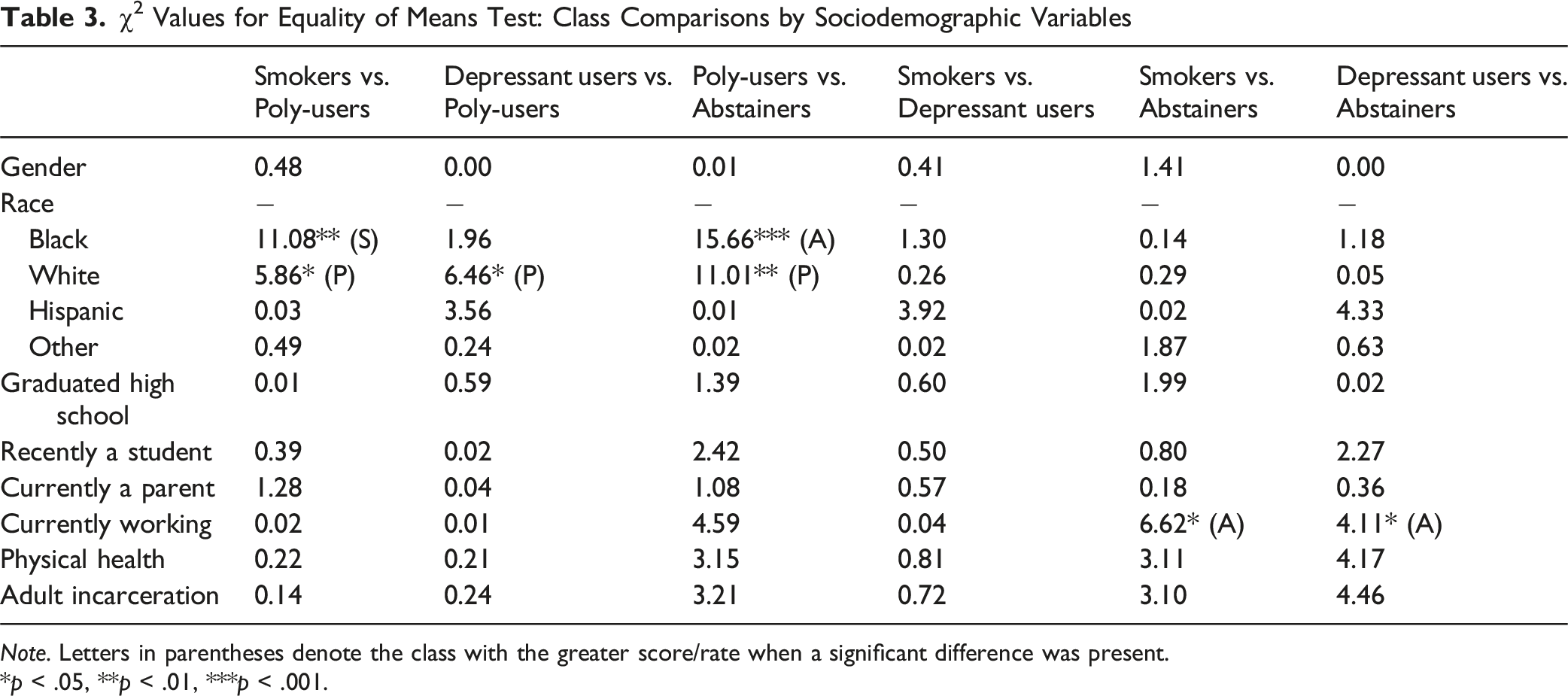
Note. Letters in parentheses denote the class with the greater score/rate when a significant difference was present.
*p < .05, **p < .01, ***p < .001.
χ2 Values for Equality of Means Test: Class Comparisons by Age 18 Substance Use
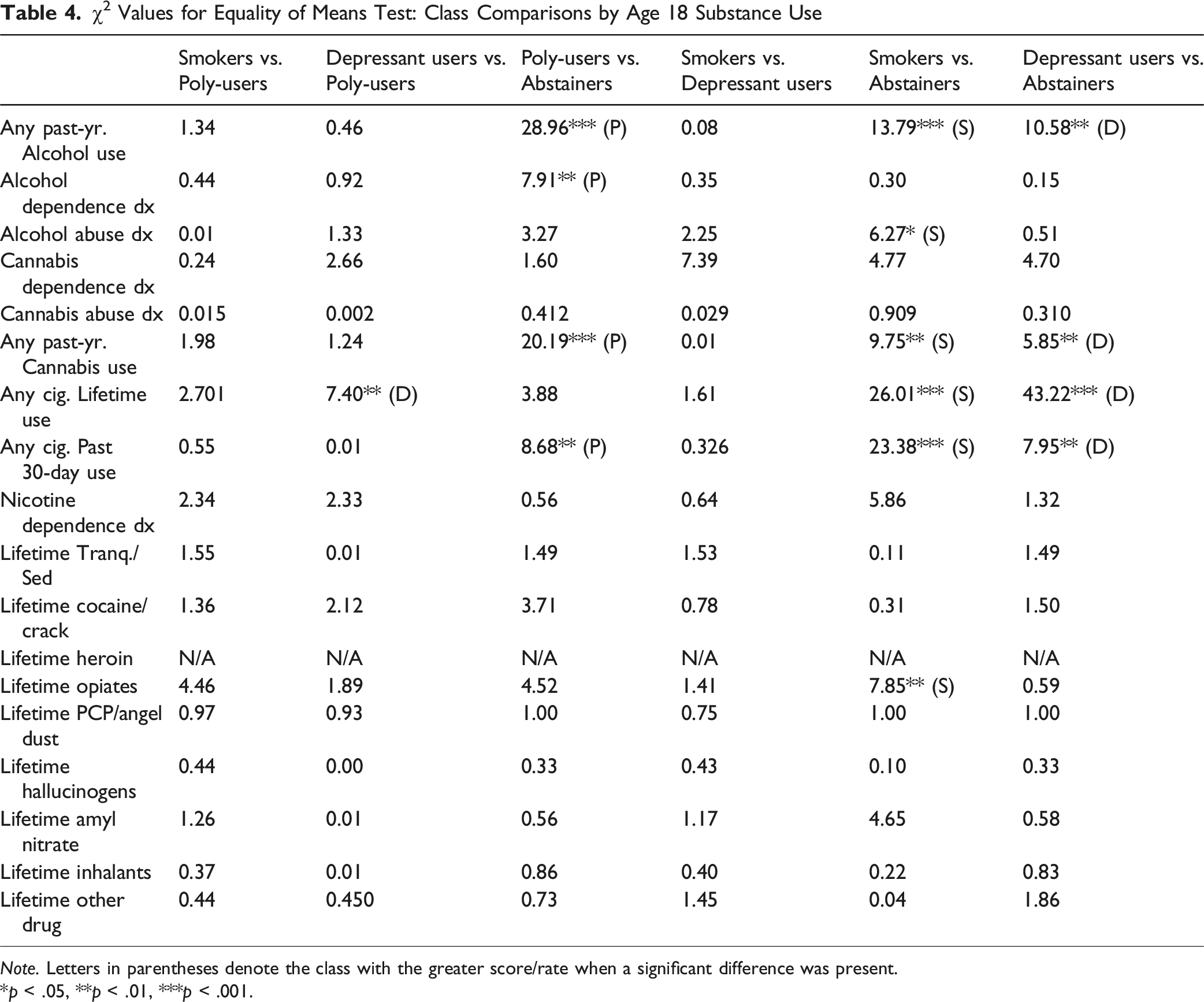
Note. Letters in parentheses denote the class with the greater score/rate when a significant difference was present.
*p < .05, **p < .01, ***p < .001.
Black participants tended to be underrepresented among Poly-users; they were more likely to classify as Smokers and Abstainers. Conversely, White participants comprised a higher proportion of Poly-users compared to all other classes. Abstainers were more likely than Smokers and Depressant Users to be working for pay. Classes did not differ by participants’ age, gender, high school graduation status, status as a past-year student or parent, incarceration in adulthood, or perceived physical health.
Sensitivity Analyses
Because a substantial proportion of the sample reported no or little past-year substance use (76%), we recognized that class enumeration might be heavily influenced by the presence of this large abstinent group. Indeed, based on the fit values presented in Supplemental Table S2, a 2-class model representing “users” and “non-users” emerged as a possible alternative to the 4-class model. To evaluate this possibility, we conducted a sensitivity analysis in which all abstainers were excluded (remaining n = 108), allowing us to determine whether the three higher-risk subgroups identified in the main analysis (“Smokers,” “Depressant Users,” and “Poly-users”) would still emerge when class estimation was restricted to participants reporting any past-year use.
Across 1- through 5-class models estimated in this restricted sample (fit indices presented in Table S4), the three-class solution demonstrated strong statistical support and offered the most interpretable and stable grouping structure. Notably, this model reproduced the same three high-risk subgroups identified in the full-sample analysis, with even clearer separation in their item-response probabilities. Although the four-class solution exhibited slightly lower AIC and SSA-BIC values, its smallest class contained only seven individuals (6.5% of the reduced sample; 1.4% of the total sample), which we considered too small to represent a reliable or clinically meaningful subgroup. Thus, we retained the three-class solution as the best-fitting model for the sensitivity analysis. The convergence of findings across the full and restricted analyses strengthens confidence in the robustness of the identified class structure and supports the decision to retain abstainers in the primary model.
Discussion
Adolescent substance use represents a significant public health concern. The present study identified and characterized latent classes of substance use patterns among a sample of young adults with significant childhood adversity. Findings revealed four unique, well-defined classes characterized by (1) high rates of tobacco and cannabis use (“Smokers”), (2) high rates of heroin/non-prescription opioid and non-prescription tranquilizer/sedative use (“Depressant Users”), (3) high rates of poly-substance use (“Poly-users”), and (4) low rates of substance use (“Abstainers”). Abstainers generally experienced fewer childhood adversities and past-year IPV relative to other classes. They were also less likely to have reported alcohol, cigarette, and cannabis use at age 18. This work represents one of the first attempts to characterize patterns of substance use among young adults with significant histories of adversity and maltreatment and offers important insights for clinicians working with maltreated youth. Implications for future research and public policy are also discussed in greater detail below.
Findings in the Context of Previous Latent Class Analyses
In many ways, the four-class solution identified here mirrors findings from previous general-population and community-based young-adult samples, which have generally found between three and six discrete classes with a single large “low-use” group and one to two “high-use” or “poly-use” classes; (Gilreath et al., 2014; Lee & Singh, 2023; Patrick et al., 2020; Wu et al., 2020). Similar class solutions have been identified among adolescents with histories of maltreatment as well, though with a larger proportion falling into moderate- and high-use classes (Hyucksun Shin, 2012; Hyucksun Shin et al., 2010; Rivera et al., 2018). Contrary to expectations, Abstainers comprised a large proportion (78%) of the present sample. This is similar to – if not larger than – the low-use classes found in previous general-population studies.
The relatively large proportion of individuals reporting minimal-to-no substance use may constitute evidence of substance-related resilience among LONGSCAN participants. Although much of the published LONGSCAN literature is deficit-focused, previous work has highlighted resilience across social, behavioral, and developmental domains (Dubowitz et al., 2016). Regarding substance-related resilience in LONGSCAN, the evidence is mixed. Participants at the age 16 interview generally reported higher rates of past-year alcohol (45%), cannabis (39%), and cigarette (48%) than similarly-aged peers in national surveys (Benedini & Fagan, 2020). However, by young adulthood, these rates began to mirror what is observed in the general population (Schulenberg et al., 2018). One exception is cannabis use, which has remained relatively high throughout the LONGSCAN study. Alternatively, the large “Abstainer” class found in the present sample may reflect attrition bias. LONGSCAN participants represent a uniquely hard-to-reach population, as evidenced by 54% attrition from study baseline to the young-adult follow-up survey. It is plausible that the 483 young adults who participated in the present study engaged in less substance use compared to the 871 lost to follow-up. Attrition bias, and its impact on the validity, reliability, and generalizability of substance use research, has been described extensively (Crisanti et al., 2014; Gray, 2016; Stewart et al., 2021), and is not unique to this study. Given the high-risk nature of this sample, as well as the unprecedented length of follow-up (i.e., 25+ years), the attrition rate in the present study was similar – if not lower – than comparable longitudinal studies (Gustavson et al., 2012).
The present findings diverged from prior LCA studies in a handful of notable ways. Firstly, a class characterized primarily by high alcohol use (and low illicit substance use) did not emerge here, despite similar classes appearing in several previous adolescent and young adult latent class analyses, both in general population samples (Patrick et al., 2020) and in high-adversity samples (Hyucksun Shin, 2012; Hyucksun Shin et al., 2010; Rivera et al., 2018; S. M. Snyder & Smith, 2015). It is possible that a “high alcohol use” class would have emerged if the indicator used in the LCA measured any past-year alcohol use rather than “use disorder symptoms,” as previous work has often done. Past-year alcohol use is typically greater than 75% of any given young adult sample, making the emergence of a “high alcohol use” class likely – though not particularly meaningful – when employing past-year indicators. In contrast, our approach prioritized problematic alcohol use, defined by the presence of multiple DSM-5 use disorder symptoms rather than any use. This operationalization was chosen to enhance the clinical specificity and construct validity of the indicator, distinguishing normative drinking, common in this developmental period, from alcohol-related impairment. Notably, even with this more stringent definition, problematic alcohol use still differentiated several high-risk classes (e.g., Smokers and Poly-users), underscoring its salience within broader patterns of substance involvement.
Another unique finding in the present study was the emergence of a class characterized by high rates of heroin or non-prescription opioid use (latent class probability = 1.0) and tranquilizer/sedative use (latent class probability = 0.52) – i.e., the “Depressant Users” class. Data for the present study were collected in 2012, a year when opioid prescribing in the U.S. was at its peak and overdose deaths were beginning to surge nationwide (Jones et al., 2018). It is possible that the “Depressant Users” class captures individuals who were particularly vulnerable to the irresponsible prescribing of opioids that was normal practice during that period. Also unique to the present investigation were the “Poly-users.” Though some form of “poly-use” class often emerges in substance use LCAs, the present Poly-user class was characterized by a 100% latent class probability of past-year hallucinogens/ecstasy use, in addition to high latent class probabilities of other substance use and use disorder symptoms. This specific pattern has not emerged in previous LCA studies to our knowledge.
Limitations
The present findings should be viewed within the context of certain limitations. First, the focus of this investigation was to identify and characterize patterns of substance use in a highly unique and adversity-exposed sample. While this represents a necessary first step given the dearth of available research, it will be crucial for future work to explore how membership in high-substance-use classes is associated with longer-term, downstream psychosocial outcomes domains, such as life satisfaction, relationship quality, and global functioning (Fairbairn et al., 2018; Zubaran & Foresti, 2009). Related, our focus on “any past-year” substance use precluded any conclusions about the severity of use in the LONGSCAN sample. These data are available but were considered beyond the scope of this study. Secondly, as noted earlier, inherent in longitudinal substance use research is the problem of response and attrition bias (Crisanti et al., 2014; Gray, 2016; Stewart et al., 2021). This problem is exacerbated when working with maltreatment-exposed individuals impacted by frequent placement changes and housing instability (A. A. Hunter & Flores, 2021). Finally, the present findings may not be broadly generalizable, both because of the high-risk nature of the sample and because of the relatively small proportion of Latinx participants, who represent one of the fastest-growing racial/ethnic groups in the U.S. (U.S. Census Bureau, 2023).
Treatment, Research, and Public Policy Implications
A crucial objective in improving our understanding of young adults’ substance use involves the translation of this knowledge into treatment, research, and policy strategies. First and foremost, our findings underscore the need for a trauma-informed approach to treating substance use problems (Bartholow & Huffman, 2021). Prior research has identified inconsistent implementation of trauma-informed clinical work in substance abuse treatment centers (Giordano et al., 2016). When substance use counselors are knowledgeable in trauma-informed care, they are typically better able to leverage patients’ maltreatment experiences to increase perceived severity of the problem and encourage attendance and motivation (Rosenkranz et al., 2012; Slesnick et al., 2008). Related, it is important that young people presenting for trauma symptoms be regularly screened and monitored for substance use and related impairment, given (a) higher rates of substance use problems in these populations (Huang et al., 2011; Kristman-Valente & Wells, 2013) and (b) the tendency for young adults to underreport their substance use (Steinhoff et al., 2023). In light of the present findings, it may benefit providers to inquire specifically about use of ecstasy and hallucinogens, which were associated with broader patterns of poly-substance use. These substances are less often the focus of treatment but are nevertheless associated with neurocognitive deficits and functional impairment when abused (Doyle et al., 2022; Montgomery & Roberts, 2022).
In addition to these clinical considerations, our findings highlight several avenues for future research. Most immediately, the present four-class solution will require replication in other diverse and high-risk young adult samples. Second, future work would benefit from investigating substances and routes of administration not captured in the present data. Examples include nicotine and cannabis vaping, as well as use of synthetic cannabis and hallucinogen products (Shafi et al., 2020). Additional research is needed to capture and characterize the changing patterns of use as cannabis and other substances are legalized, developed, and integrated into popular young adult culture. Third, in addition to its use toward characterizing patterns of substance use, latent class approaches may also be applied to typologies of adversity, as prior work has demonstrated (Aizpurua et al., 2023; Henry, 2020). Using LCA to examine heterogeneity in ACE exposure could clarify whether specific adversity profiles are differentially associated with the substance use classes identified here, and future research may benefit from integrating both approaches to better understand how distinct adversity and use patterns jointly contribute to risk.
From a policy perspective, the finding that most young adults – including those with adversity histories – fell into Abstainer or Low-use classes underscores the importance of prevention strategies that avoid over-pathologizing normative use while still targeting the small but high-risk groups identified here. More contemporary perspectives maintain that most substances, when used by adults in moderation, can be used recreationally without lasting neurocognitive or functional impairment (Frazer et al., 2018; Hart et al., 2012). Policy makers should consider a “harm reduction” approach to substance use legislation. This public health alternative to moral and disease models of substance abuse reduces the negative consequences of substance use, creates space for moderate use or use in safer conditions, and de-emphasizes the “abstinence-at-all-cost” perspective (H. S. Lee et al., 2011). Harm reduction approaches are also generally more cost-effective (Wodak & Cooney, 2006) and socially responsible than traditional anti-drug laws, which target minoritized communities and create racial disparities in incarceration (Earp, Lewis, & Hart, 2021; Pierson et al., 2020).
Conclusions
The present investigation sought to identify and characterize latent classes of individuals based on their past-year substance use in a sample with high rates of childhood maltreatment and adversity. Four discrete classes emerged from the data characterized by (1) abstinence from illicit substances, (2) high rates of tobacco and marijuana use, (3) high rates of opioid and tranquilizer/sedative use, and (4) poly-substance use. The four-class solution aligns with previous studies, which have typically documented 3-6 discrete groups, with 1-2 characterized by high- or poly-use. Novel findings identified here include the presence of an “opioid” class as well as a relatively large proportion of substance abstainers. This work reinforces the prospective association between ACEs and potentially problematic patterns of substance use in adulthood, and offers key implications for providers, researchers, and policy makers.
Supplemental Material
Supplemental material - Latent Classes of Substance Use in Young Adult Survivors of Child Maltreatment and Adversity: a 20-Year Prospective Investigation
Supplemental material for Latent Classes of Substance Use in Young Adult Survivors of Child Maltreatment and Adversity: A 20-Year Prospective Investigation by Nicholas M. Morelli, Benjamín Aceves, Emily A. Schmied, Kajung Hong, Michaela Gusman, Theresa Ngan Nguyen, Howard Dubowitz and Miguel T. Villodas in Child Maltreatment.
Footnotes
ORCID iDs
Ethical Considerations
Each study site obtained approval from their respective institutional review boards and written, informed consent/assent was acquired from all participating caregivers and children.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by grants from the Office of Child Abuse and Neglect, Administration on Children and Families, US DHHS (Grants Nos. 90CA1401, 90CA156901, 90CA1681, and 90CA1749), and the National Institute on Drug Abuse (Grant no. 5R01DA031189-04). Dr. Schmied and Dr. Aceves acknowledge the funding support of S21MD010690 (SDSU HealthLINK Endowment).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.