
Abstract
U.S. children suffer higher rates of death resulting from violence than children in economically comparable countries. Prevention of violent injury relies on robust data regarding demographic and contributing factors. This retrospective study of records from the New Mexico Office of the Medical Investigator (OMI), the University of New Mexico Children’s Hospital (UNMH), and the UNMH child protection team examined demographic and risk factors for child deaths and near-deaths resulting from violence or maltreatment (abuse or neglect) during the period August 1, 2019 - September 30, 2022. The OMI is the only forensic laboratory in the state, and UNMH is the state’s only pediatric trauma hospital. 76 children met inclusion criteria; 60 of these died. Most victims were male. Firearm injuries were most common among adolescents, and other injury mechanisms predominated among younger victims. Parent intimate partner violence (IPV) was more common among children who suffered non-fatal injuries than fatal; and parent IPV, current or prior child protective services involvement, and parent substance use were identified more often in children with non-firearm injuries versus firearm. Other risk factors did not discriminate between groups. Pooling data for serious non-accidental child injury would increase the data available for epidemiologic studies and prevention efforts.
Background
Children in the U.S. die at higher rates than children in economically comparable nations. The gap has widened significantly since 2015 for children ages 1-19 years, principally due to deaths resulting from inflicted violence. U.S. children beyond the neonatal period are more than 5 times as likely to be murdered and more than 15 times as likely to die by firearm compared to their counterparts, while youth suicide rates are similar in the U.S. versus other countries (Forrest et al., 2025).
Studies of risk factors associated with violent child deaths generally focus on a causal category, like child maltreatment or firearm possession, though there may be substantial overlap in identified factors. Exposure to substance use (Kelleher et al., 1994; Walsh et al., 2003; Mattson et al., 2022; Luo et al., 2025; Younas & Gutman, 2023; Roscoe et al., 2018; Negriff et al., 2023), intimate partner violence (IPV) (DiLauro, 2004; Edleson, 1999; Herrenkohl et al., 2008; Lamers-Winkelman et al., 2012; Mattson et al., 2022; Younas & Gutman), mental illness (Ayers et al., 2019; Roscoe et al., 2018; Sigel et al., 2019; Traynor et al., 2022), low socio-economic status (Luo et al., 2025; Trinidad & Kotagal, 2023), and to community violence (Austin et al., 2020; Faus et al., 2019; Mattson et al., 2020; Valentino et al., 2012) are associated with both maltreatment (abuse and neglect) against children overall and with childhood firearm injuries specifically. Additional risk factors for child maltreatment include caregiver history of maltreatment as a child (Assink et al., 2018; Martoccio et al., 2022), child disability (Legano et al., 2021), and reported use of corporal punishment (Heilmann et al., 2021; Ma et al., 2022; Zolotor et al., 2008) while gang involvement predicts greater likelihood that youth will carry a firearm (Lizotte et al., 2000; Tigri et al., 2016). For multiple types of violence against children the underlying risk factors are the same, and some forms of interpersonal violence can be risk factors for other harms. For example, both substance use and child maltreatment history increase the risk of IPV (Fazel et al., 2018). The pervasiveness of violence and recognition of interplay between risk factors has led to calls to broaden public health approaches to risk factor data (Mercy et al., 2017; Reza et al., 2001; Mercy & Tharp).
Robust data regarding risk factors is foundational to prevention efforts to reduce child deaths resulting from violence or neglect. Examination of factors associated with near-fatalities may also support prevention. In 2016, the Presidential Commission to Eliminate Child Abuse and Neglect Fatalities (CECANF, 2016) recommended including data from near-fatal child maltreatment cases, since the difference between dying and surviving may merely reflect a child’s access to timely medical care (Berger et al., 2015; CECANF, 2016). Studies of child maltreatment fatalities and near fatalities to date have identified similar risk factors (Pierce et al., 2017; CECANF, 2016; Berger), and prior referral to child protective services for abuse is associated with a greater risk of future abuse mortality (Putnam-Hornstein et al., 2013). In addition to enlarging the dataset on risk factors, examination of near fatality risk factors in individual cases may improve practitioners’ ability to prevent child deaths.
U.S. states report child abuse fatalities systematically to the National Child Abuse and Neglect Data System (NCANDS), but like child protective services data generally, reports are typically limited to cases occurring on state lands, and to cases occurring within family units. In addition, many jurisdictions have teams that review child deaths due to violence and other causes with the aim of informing prevention efforts. In contrast, reports on near-fatal child cases is limited. A principal reason for this is the lack of a standard accepted definition for what constitutes a near-fatality. Using a modified Delphi process involving professionals with relevant expertise, Campbell et al. proposed defining near-fatal child maltreatment as “life-threatening cardiopulmonary dysfunction directly attributable to suspected abuse or neglect as evidenced by (a) respiratory insufficiency/failure requiring intubation and mechanical ventilation, (b) respiratory insufficiency/failure requiring medications to reverse effects of toxic ingestion, or (c) cardiac arrhythmia with/without cardiopulmonary resuscitation (CPR)” (Campbell et al., 2021). In the 2023 Child Maltreatment report published by the U.S. Children’s Bureau, just 6 states (Colorado, Indiana, Georgia, Kentucky, Nevada, and Washington) described processes for analyzing data on near-fatal cases (US HHS, 2025). The goal of the current study was to examine demographic characteristics and risk factors for children who died or nearly died as a result of abusive, violent, or neglect injuries, in order to inform prospective data collection efforts that may improve prevention efforts.
Methods
This was a retrospective study of serious trauma and neglect cases presenting to the University of New Mexico Children’s Hospital (UNMH) and/or the New Mexico Office of the Medical Investigator (OMI) from August 1, 2019, through September 30, 2022. UNMH is the state’s only pediatric trauma hospital, and the only center in New Mexico that includes board-certified child abuse pediatricians. OMI conducts all child death medical investigations for New Mexico. Study patients were identified separately from three data sources: UNMH electronic health records, OMI records, and in child protection team records. The lists of patients from OMI and electronic hospital data were aggregated, and duplicate records were reconciled and then compared with child protection team records to yield a final set of unique patients.
For the purposes of this study, we adopted a definition of “near-fatality” that is similar to that derived by Campbell et al., and that has been utilized previously by one of the study authors for a network of child abuse pediatricians. Our definition of near-fatality is an injury or condition that would likely have resulted in death without medical intervention, where medical intervention necessary to prevent death is defined as one or more of the following: cardiopulmonary resuscitation (CPR); rescue breathing; removal of airway obstruction; intubation; administration of medications to stabilize cardiac or respiratory status, or blood pressure; intravenous correction of critical electrolytes or blood sugar; any surgical intervention to preserve brain function or prevent blood loss or infection; and any invasive monitoring to gauge neurologic status.
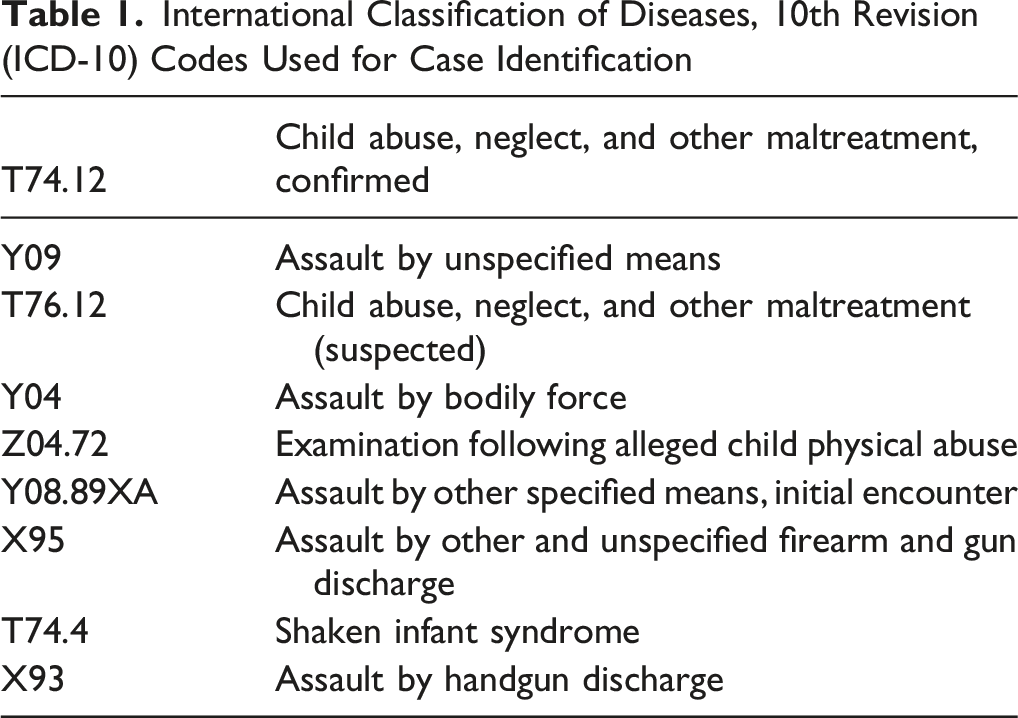
International Classification of Diseases, 10th Revision (ICD-10) Codes Used for Case Identification
Results
We identified 58 children in OMI records and 332 children in hospital records as possible study cases. All OMI children and 21 hospital children met study criteria. The most common reasons causing hospital cases to be excluded was that they were not fatal or near-fatal, or the initial suspicion of maltreatment was not confirmed. All included hospital children were identified by one or more of 3 codes: Z04.74 (“Examination following alleged child physical abuse”), T74.12 (“Child abuse, neglect, and other maltreatment, confirmed”) and Y09 (“Assault by unspecified means “). An additional 2 hospital children (one fatal, one near-fatal) were identified in the data maintained by the child protection team; in both cases, abuse was diagnosed as the cause of their injuries. The final cohort consisted of 76 children, recording 60 fatal and 16 near-fatal incidents (Figure 1). Flow diagram of study participants identified through Office of the Medical Examiner (OMI) and children’s trauma hospital data, State of New Mexico, August 1, 2019 – September 30, 2022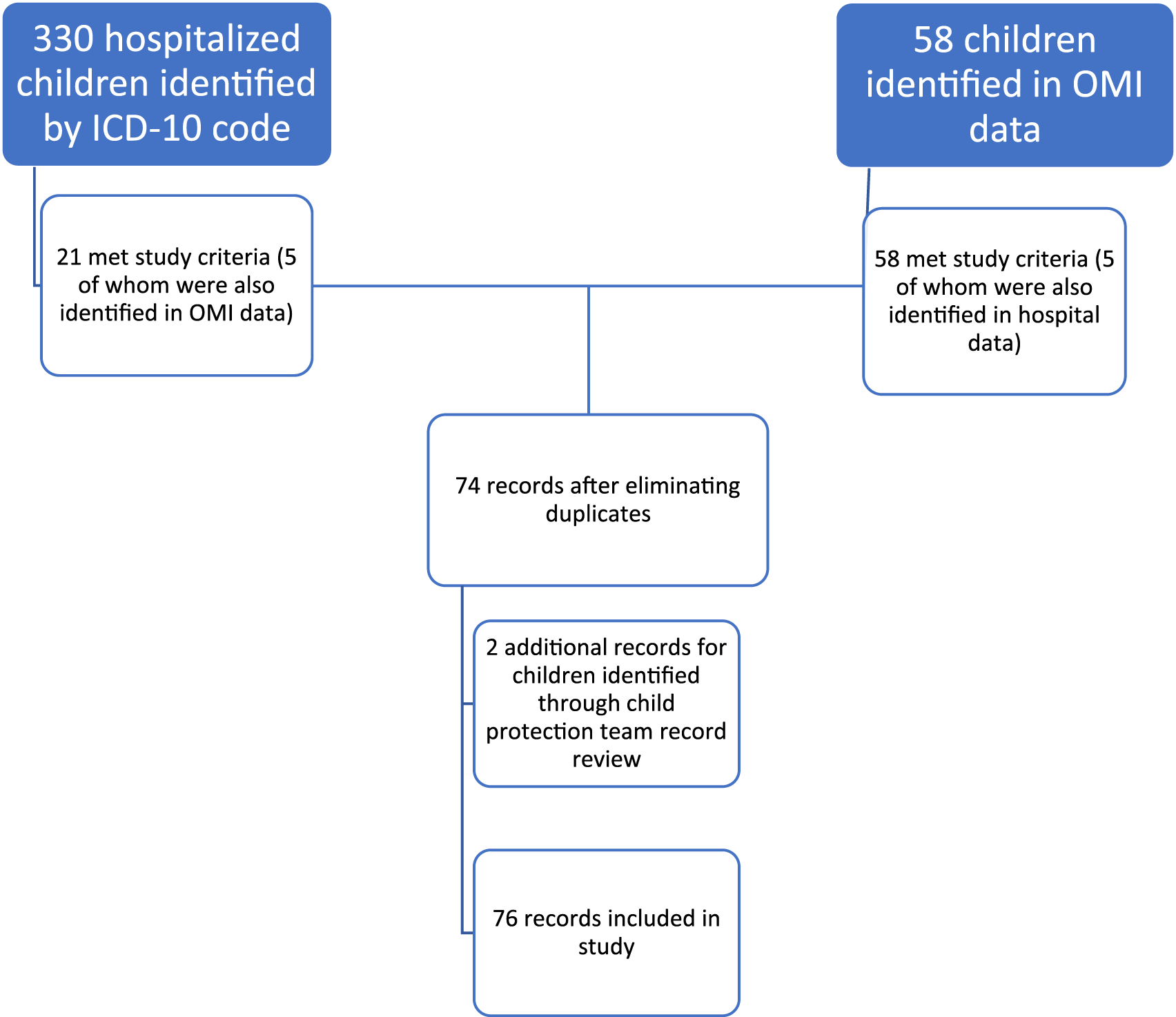
Demographic Characteristics of Fatal and Near-Fatal Child Maltreatment Cases in New Mexico, August 1, 2019 – September 30, 2022
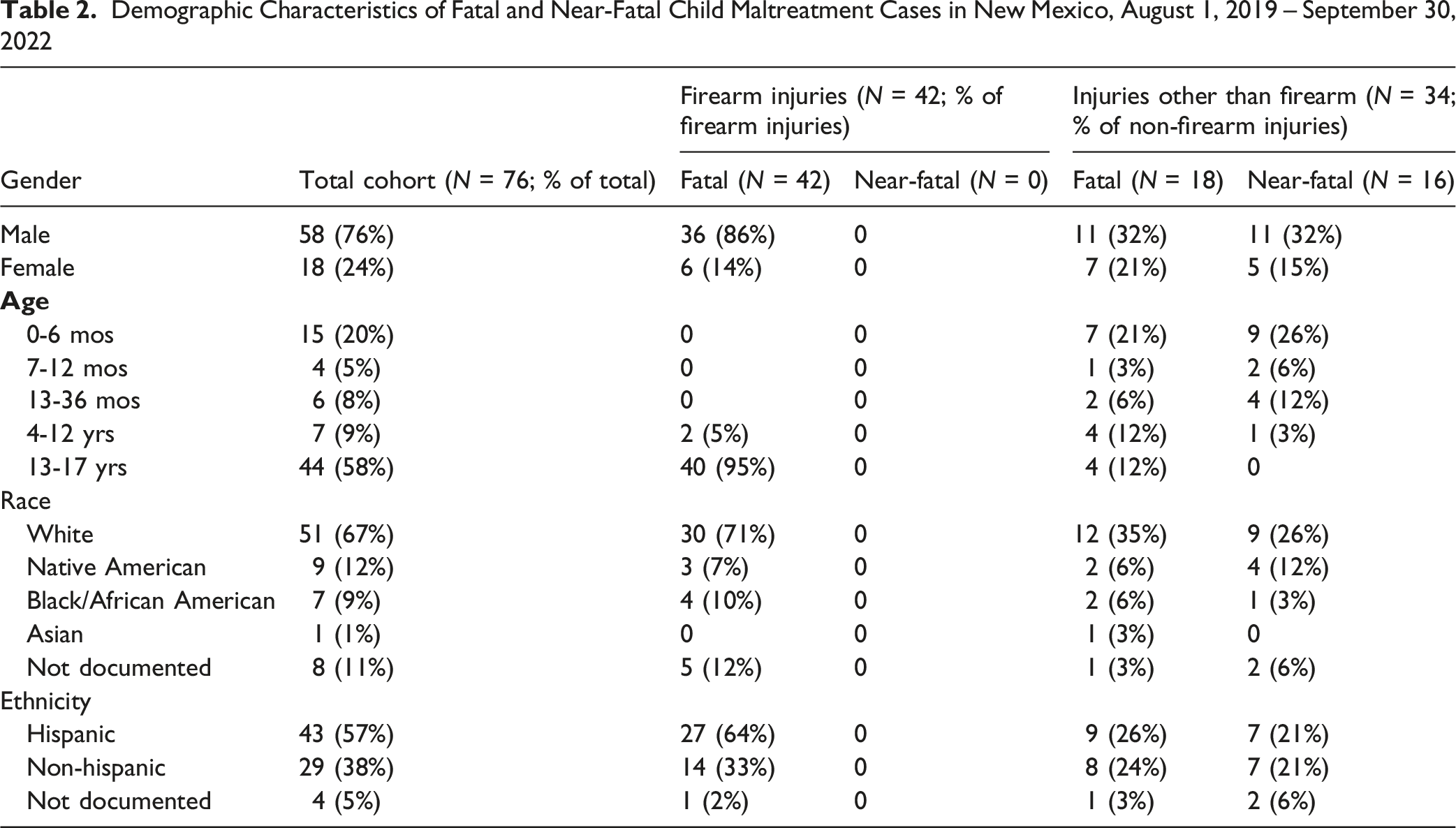
All children with firearm injuries died, whereas nearly half of children with other mechanisms of injury (16 children) survived. Most firearm injury victims were adolescents, causing the total cohort of children with fatal injury to be significantly older than those who suffered near-fatal injuries (average age 10.1 versus 1.0 years, p < .001). The most common cause of injury was firearm (42 children; 55.3%), followed by blunt trauma (25 children; 32.9%). Mechanisms of injury for the remaining incidents included poisoning (4 children), starvation (2 children), and 1 each: asphyxia, smothering, and penetrating neck wound. The average age of children with non-firearm-related injuries was 3.5 years; a significantly greater proportion of older children (8 of 9 children age >3 years) in this group died than younger children (10 of 25, p = .008). The maltreatment diagnosis was likely or definite neglect for 7 children, and likely or definite physical abuse/inflicted trauma for the remainder.
Risk Factors by Case Type, and % of Each Type, Among Fatal and Near-Fatal, and Among Firearm and Non-firearm Child Maltreatment Cases in New Mexico, August 1, 2019 – September 30, 2022
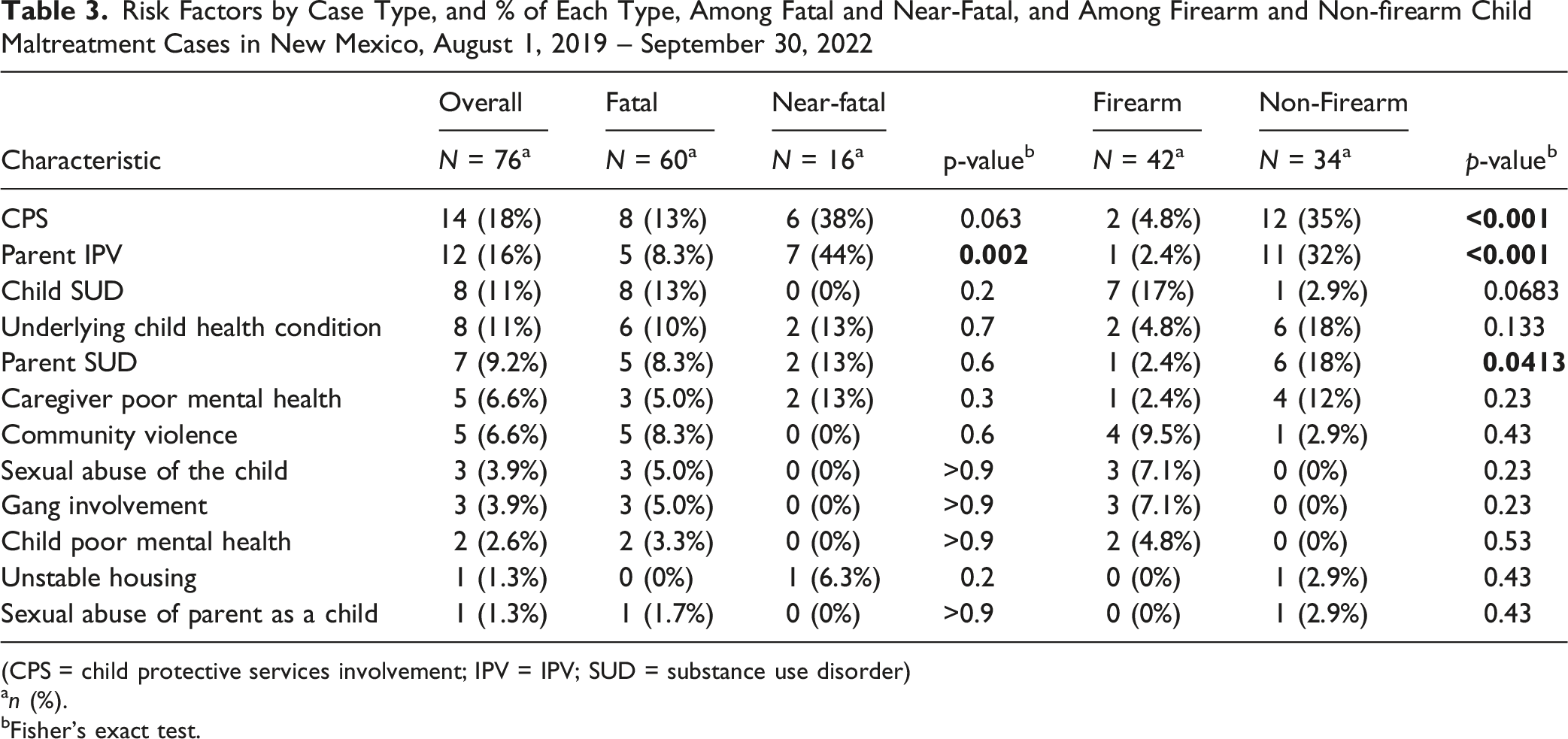
(CPS = child protective services involvement; IPV = IPV; SUD = substance use disorder)
an (%).
bFisher's exact test.
Discussion
The majority of children (∼80%) in our study died, and more than two-thirds of deaths were caused by a firearm. Firearm deaths in New Mexico have risen at alarming rates in recent years, moving the state from 7th to 3rd nationally for firearm deaths involving people of all ages between 1999 and 2021 (NM DOH, 2023). Among New Mexican youths (ages 14 – 17), the number seeking emergency department care for gunshot wounds rose 42% in July 2022 – June 2023 compared to the prior 12-month period (149 vs. 105, NM DOH, 2023). Alcohol and drug dependence have been increasingly associated with firearm homicides in New Mexico (NM DOH, 2023), and this was the most common risk factor for firearm injury in our study cohort.
Blunt trauma to the head, neck and/or torso was the second most common cause of fatal or near-fatal injury during the study period. Unsurprisingly, the children in this group were primarily very young (76% were <3 years old), consistent with a strong body of evidence indicating that caregiver frustration due to stressors such as infant crying and toddler toileting accidents are common triggers of violence in this age group (Brewster et al., 1998; Flaherty et al., 2006; Maguire et al., 2008; Peck et al., 2002).
Only parent IPV discriminated risk between fatal and non-fatal injuries, and firearm versus non-firearm; current or prior CPS involvement and parent substance use were additional significant factors for firearm versus non-firearm cases. The children affected by these three factors were younger, on average, than the full cohort (3.7 years versus 9.5). Our finding that no other risk factors were significantly different between groups suggests that it may be reasonable to pool data, thus providing larger datasets to support prevention efforts.
The primary limitations of our study included the retrospective design, and the fact that risk factors are not documented systematically in our hospital or medical examiner records. Given that inflicted trauma is a leading cause of serious injury and death among U.S. children (Leventhal et al., 2012; Michaels & Letson, 2021; US HHS, 2025), our data highlight a need for improved documentation of factors that may be leveraged for prevention. Alcohol and drug dependence, child protective services involvement, IPV, poor mental health, and chronic medical conditions are commonly recorded data elements in both hospital and medical examiner documentation; information about these risk factors was likely limited only by whether or not patients and families were willing to discuss them. The prominence of these risk factors in our study cohort was consistent with prior literature on risk factors for both child maltreatment and child firearm injuries (Younas et al., 2023; White et al., 2015; Negriff et al., 2023; Luo et al.; Pierce et al., 2017; Austin et al.). Conversely, we can draw only limited conclusions regarding the impacts of community violence, gang involvement, or housing instability in our cohort, since these require community-level data and shared definitions. Victims of child sexual abuse frequently do not report the crime (Manay & Collin-Vézina, 2021; Landberg et al., 2022; Hébert et al., 2009; Rennison); it was therefore surprising to find this recorded as a possible risk factor in 4 of our cases.
Our purposeful use of a broad selection of ICD-10 codes identified multiple children who were not victims of violence or neglect. However, only 3 of the codes were necessary to identify children who met our inclusion criteria. In addition, we found 2 hospital patients in data maintained by the child protection team who would have been missed using the codes alone. These 2 children were assigned codes indicating trauma, but erroneously, were not coded for inflicted injury (e.g. S06.5XOA for “traumatic SDH”), even though their abuse diagnoses are clearly documented in the electronic health record. Prior studies have found ICD-10 codes to have low sensitivity and only moderate specificity for identifying child physical abuse (Garza et al., 2021), and one study of the use of ICD-9 and ICD-10 codes for child maltreatment in 2 large national datasets revealed multiple inconsistencies (Noorbakhsh et al., 2002). ICD-10 codes have even lower sensitivity for detecting child neglect than for physical abuse (McKenzie et al., 2011), but one center found high positive predictive values (Calhoun et al., 2024). The fact that child neglect is challenging to capture in hospital coding is unfortunate given that it is more prevalent and is a factor in more child maltreatment deaths than abuse (Kobulsky et al., 2020; US HHS, 2025). The discrepancy in ICD counts of neglect compared to its high incidence in agency-reported data suggests that neglect cases are particularly prone to missed coding opportunities. Our research exposed data gaps including the need for quality improvement of ICD-10 coding to identify inflicted injury and neglect, and the lack of standardized collection of risk factor data. It also points to the potential utility of child protection team data for case ascertainment. Further research is needed to determine if other child, family and community risk factors may be similar between groups and to study child sexual abuse as a predictor of serious inflicted physical injury.
Conclusions
Parent IPV, current or prior CPS involvement, and parent substance use may be more predictive of non-fatal and non-firearm injuries than fatal and firearm injuries. Pooling of risk factor findings for serious non-accidental child injury would increase the data available for epidemiologic studies and prevention efforts.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr. Li Luo of the University of New Mexico School of Medicine, who provided statistical support for this project.
Ethical Considerations
The study conducted in accordance with the Declaration of Helsinki and was approved by the UNM Health Sciences Human Research Protections Office (study number 23–356) on 10/27/2024, with the need for informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the highly sensitive nature of the study topic, the authors are not permitted to share additional data details publicly.