
Abstract
As people have become increasingly concerned about their health, programs about health have proliferated on South Korean television. This study’s purpose is to identify the factors associated with and processes through which Korean adults intend to view health TV programs. The comprehensive model of information seeking (CMIS) was tested using structural equation modeling that was fitted with survey data from a nationally representative sample of 1,020 South Korean adults. Results indicate that the demographic antecedents of being female and older adult and the psychological antecedents of being health conscious and health literate significantly predicted the degree to which people would perceive health TV programs to be useful. Among the information carrier factors of health TV programs, utility was directly related to intention to view, while trust in health information on TV was only indirectly related to intention to view. For theoretical implications, we suggest further conceptual and operational refinement of CMIS. For practical implications, we highlight the importance of motivational and utility factors in predicting people’s intention to view health TV programs. Finally, this study stresses the importance of TV as a viable health information provider that can reduce health information gaps and help people (particularly older adults, the poor, and the less educated) to improve their health knowledge and health behaviors.
The aging of the population has become a serious social problem worldwide in both developed and developing countries (Bloom, Boersch-Supan, McGee, & Seike, 2011). The United Nations (2011) has announced that “the era of homo hundred” has arrived: by 2020, about 31 countries are predicted to have an average life expectancy above 80, and the number of people older than 100 will increase tenfold compared with 2010. Personal maintenance of health has become more important than ever, and in many societies the media play a key role in providing information about how best to do it (M. Choi, Seo, Choi, & Paek, 2014).
For decades, mass media, and particularly TV, have been important providers of health information. Although TV is regarded as a “traditional” medium, many people still get health information from it in a variety of formats such as news, talk shows, documentaries, and dramas (Dutta, 2007). But because of the Internet’s growing importance, research in recent years has focused mainly on health information online (e.g., Chen, Yamada, & Smith, 2014; Cline & Haynes, 2001; Warner & Procaccino, 2007). One lingering problem with the Internet is that, despite its increasing availability and accessibility, health information gaps across ages, gender, and socioeconomic status still exist (Coverdell & Utley, 2005; Raj, Singh, Sharma, & Goel, 2014). By contrast, with the recent proliferation of mobile and multimedia technology, TV seems to have regained its popularity because people can view it on a variety of channels and platforms, and they are no longer limited to viewing it on large sets in their homes. Recently, in the United States, TV’s popularity has been growing (Drier, 2015), and a similar trend has been found in South Korea (S. Choi, Kim, & Kim, 2014). As South Koreans become more health conscious and make use of new means for viewing TV, health programming has flourished on South Korean broadcast and cable TV channels (S. J. Kim, Lee, & Kim, 2001; Kwon, Kim, & Baek, 2014; Park, Chang, & Kwon, 2003).
Health programming on TV is itself not a new development. For example, as early as 1978, Finland was undertaking nationwide efforts to develop TV formats intended to enhance public health (Pekka, Erkki, Tina, Pekka, & Meri, 2009; Puska et al., 1987). Among these were several series of risk reduction and health promotion programs, for example, the North Karelia Project’s “Keys to Health,” which provided a format for health educators to advise participants and viewers about preventive health behavior changes (Pekka et al., 2009). On U.S. commercial broadcast TV, an entertainment reality show titled “The Biggest Loser” has run for 18 seasons. Using the simple format of a weight-loss competition, it has achieved both health- and entertainment-related goals, and its format has been exported to 25 countries such as Australia, several Asian countries, and several Arab countries (Chalaby, 2015).
Although health TV programming has been a global phenomenon for several decades, little research has been done on the factors associated with how people use TV programs for health information and the processes through which they intend to do so. The current study’s purpose is to examine these factors and processes with respect to people’s intention to view health TV programs in South Korea. To pursue this purpose, we use the comprehensive model of information seeking (CMIS). The CMIS intersects with other accounts of the processes and beliefs that predict health-related behavior—for example, the uses and gratifications perspective (Rubin, 2010), the health belief model (HBM; Janz & Becker, 1984; Rosenstock, 1974), and the media exposure and appraisal model (Johnson & Meischke, 1993). Built upon these existing theoretical accounts, CMIS delineates the pathways through which people engage in information seeking. CMIS has been used to understand the following: cancer-related information seeking behavior using either traditional media (Johnson & Meischke, 1993) or the Internet (Han et al., 2010; Hartoonian, Ormseth, Hanson, Bantum, & Owen, 2014), prescription drug information seeking (DeLorme, Huh, & Reid, 2011), and information seeking through informal and formal communication in an organizational setting (Johnson, Donohue, Atkin, & Johnson, 1995).
This study relies on theoretical arguments and empirical evidence related to the antecedents and information carrier factors that are relevant to CMIS. For antecedents, it uses health consciousness and health literacy. For information carrier factors, it uses media trust and utility of TV health programs. For information seeking actions, it uses intention to view health TV programs. By explicating the underlying processes through which people intend to seek health information on TV, we can draw practical implications by identifying factors that determine whether people will actively use television for seeking out information on healthy lifestyles and disease prevention.
Health TV Programs in South Korea
In the South Korean media system, TV has played a critical role in informing audiences about health and disease (Kang, 1998). According to industry statistics, TV has been a popular platform for health information, followed by the Internet for people in their 20s and 30s, and newspapers for those in their 40s through 60s (C. J. Choi et al., 2003). A 2013 survey study on health information use reaffirms these findings (Seoul National University Hospital [SNUH], 2014). About 27% of respondents reported that the health information providers they rely on most are doctors and mass media such as TV and newspapers, while only 9% reported that they rely on the Internet.
These findings might be explained by the degree to which people trust the sources and channels for health information. A study on media trust indicated that Koreans consider the most trustworthy source of health information to be TV, followed by their acquaintances and the Internet (Yu, Cho, & Ahn, 2011). Although young people tend to use TV less than other age groups, and although new digital multimedia channels have become increasingly popular, broadcast and cable TV continue to be the most preferred channels for health information across all ages (J. Kim, Cho, Jang, & Youn, 2015).
In recent years, various health-related programs have appeared and flourished in South Korea. These programs cover a variety of health issues, including disease prevention and treatment, fitness, exercise, beauty, and leisure. Most of them have an “infotainment” format that packages health information in genres such as celebrity interviews or talk shows, reality shows, and dramatizations.
The popularity of health-related programs has given rise to cable channels that focus solely on health. These channels feature not only health prevention and disease treatment but also a variety of healthy lifestyle topics. As of 2014, there were seven health-related channels (e.g., Vitamin TV, Health TV, Healthmedi TV, Oriental Medicine TV, Lifestyle Health TV), 19 leisure/travel channels (e.g., Horseriding TV, Mountain TV, Fishing TV), and 12 lifestyle channels (e.g., GTV, OnStyle, WISE TV, Diet TV, Kuki TV; Paek et al., 2014). Several health-related programs are very popular, for example Vitamin on KBS2, How to Eat and Live Well on SBS, The Secret of the Four Phases of Life on KBS1, Golden Egg on MBN, and Doctors’ Match on JTBC. While not all health-related channels have drawn satisfactory viewer ratings, major media companies have also looked into the business potential of starting health-focused cable channels (Paek et al., 2014).
Few published studies have examined the significance and impact of TV health programming (for an exception, see M. Choi et al., 2014). But it deserves more attention for at least two reasons. First, TV continues to be a viable and preferred channel of health information across generations. Second, the information health TV programs provide can help promote health prevention behaviors and thereby save money that might otherwise need to be spent on costly medical treatments. By identifying factors associated with people’s intention to view TV for health information, the current study aims to provide suggestions and develop strategies for getting more people to use TV for health information, and to do so in more informed ways.
The Comprehensive Model of Information Seeking
The CMIS is built upon existing theoretical accounts of people’s media use and of the processes and beliefs that predict their health-related behaviors. Its three core accounts are the uses and gratifications approach (Rubin, 2010), the HBM (Janz & Becker, 1984; Rosenstock, 1974), and the media exposure and appraisal model (Johnson & Meischke, 1993). The uses and gratifications approach assumes that people are active and motivated media users, and it identifies and typifies their media-related needs and motivations, one of which is information seeking (Rubin, 2010). The HBM explains that people’s health-related behaviors are conditioned by demographic and sociopsychological barriers to information seeking, as well as their beliefs about how susceptible they are to a disease or illness (perceived susceptibility) and how severe a disease’s consequences would be (perceived severity). Informed by uses and gratifications and the HBM, CMIS proposes that people’s needs, motives, and beliefs are psychological antecedents to their information seeking behavior. In addition, CMIS considers people’s media channel selection to be an important precursor to the actions they take to seek health information. For this reason, it also incorporates the media exposure and appraisal model to explain the important role of specific factors related to the media people use for information (Johnson & Oliveira, 1988). Based on the original model of Johnson and Meischke (1993), Figure 1 shows the relationships within the CMIS among antecedents, information carrier factors, and information seeking actions. Using the CMIS’s original conceptions and theoretical rationales, several studies have applied it to a variety of topics but modified it to fit different study contexts with different operating variables. Operating variables for these previous studies are summarized in Table 1.
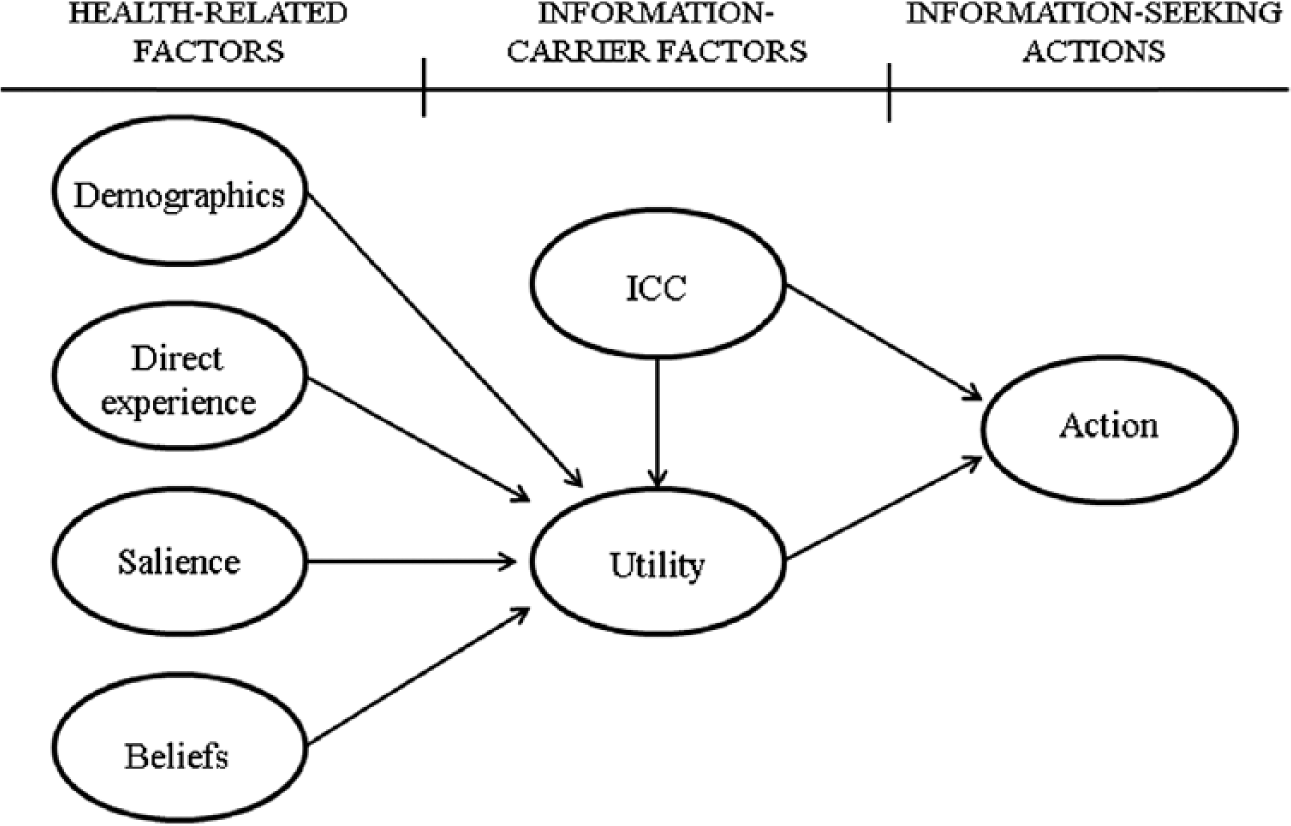
Comprehensive model of information seeking
Operating Variables for the Corresponding Constructs in CMIS Studies.
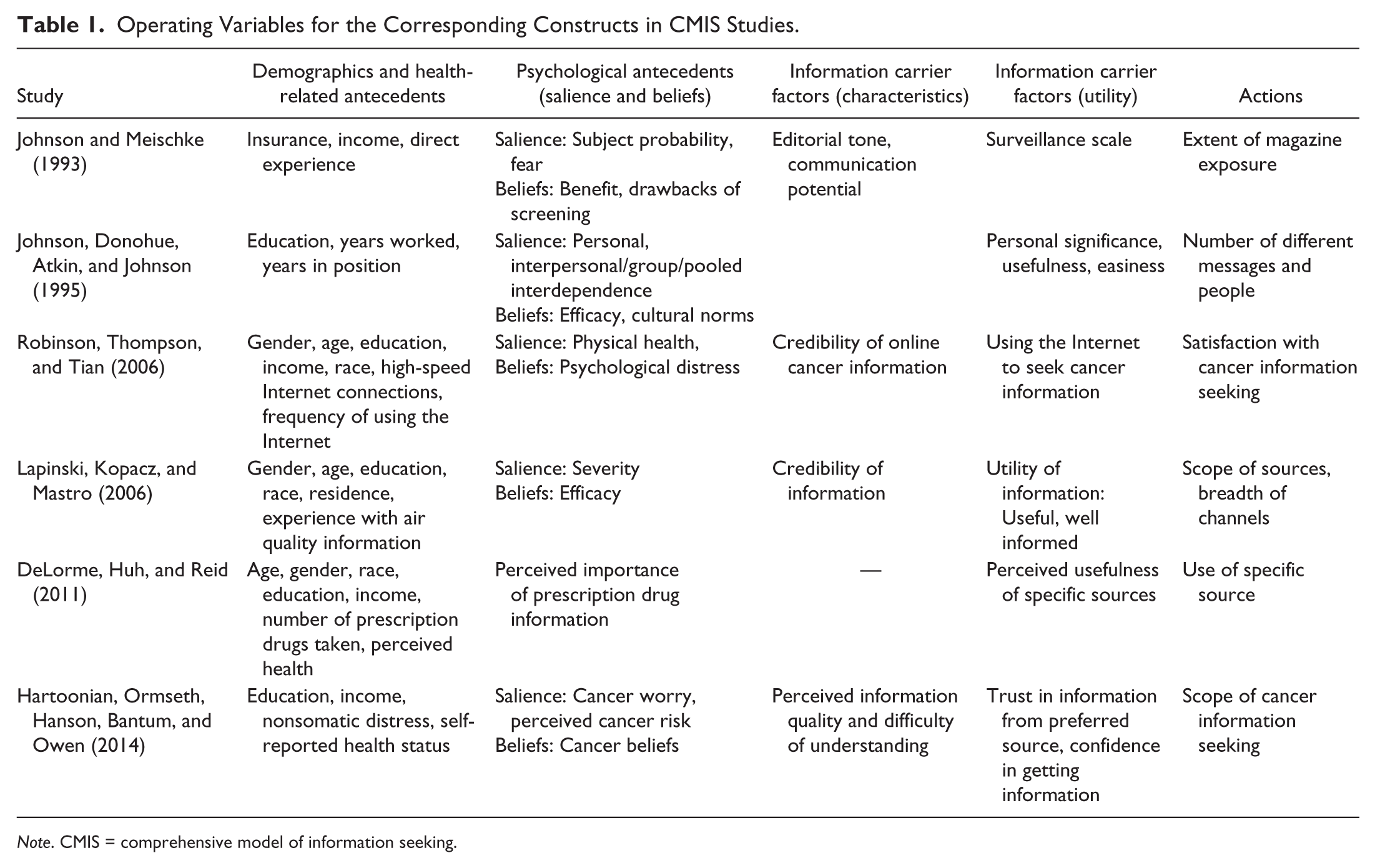
Note. CMIS = comprehensive model of information seeking.
Antecedents
CMIS identifies several types of antecedents to information seeking. First, it might be determined by demographic characteristics such as gender and age. Second, since CMIS was developed in the health context of cancer (Johnson, 1997; Johnson & Meischke, 1993), it also includes health-related antecedents such as personal experience with a disease and a disease’s perceived threat to health. Third, the key psychological antecedents it highlights are salience and beliefs. Salience refers to “the personal significance of health information to the individual” (Johnson, 1997; Johnson & Meischke, 1993, p. 347), and it serves as the underlying motivation for seeking information. Beliefs as antecedents are people’s expectations about the outcomes of information seeking.
Information Carrier Factors
CMIS goes further than the HBM because it incorporates communication variables that play a critical role in the information seeking process. Based on the media exposure and appraisal model, two information carrier factors have been identified: information carrier characteristics (ICC) and utility. ICC includes editorial tone (people’s perception of credibility), and communication potential, which is related to issues of style and comprehensiveness (Johnson & Oliveira, 1987). Drawn from the uses and gratifications perspective, utility refers to audience judgments about the relevance, importance, and/or usefulness of the information provided (Johnson, Andrews, & Allard, 2001; Johnson et al., 1995).
Actions
This variable in the original CMIS research by Johnson and Meischke (1993) is information seeking. It is defined as “the purposive acquisition of information from selected information carriers” (Johnson et al., 1995, p. 275; Johnson & Meischke, 1993, p. 350), and it should be distinguished from merely incidental, passive exposure to health information (Yang & LeValley, 2015). Information seeking has been broken down into different dimensions such as method (channels selected), scope (the number of different people from whom information is sought), and depth (the number of different messages involved; Johnson et al., 1995). However, existing studies either deal with only one of these dimensions or have adopted different types of information seeking actions that are better suited to fit their study contexts (see Table 1).
Proposed Model With Modified CMIS
Previous studies using CMIS followed different methods in identifying and operationalizing antecedents, information carrier factors, and information seeking actions. One reason why is that, while CMIS provides a basic causal structure, different contexts will generate different kinds of relationships within that structure (Johnson et al., 1995). To fit CMIS to the current study’s context, the demographic antecedents to health information seeking we used were gender, age, education, and income. These variables were chosen for two reasons: they are most closely related to TV use for health information (C. J. Choi et al., 2003; M. Kim & Yoo, 1996; Nam, Yoon, & Gye, 1998), and they are the main demographic factors identified in previous CMIS literature (DeLorme et al., 2011; Hartoonian et al., 2014; Johnson et al., 1995). Although existing CMIS studies have not specified either a clear rationale or directions in their hypotheses for these demographic factors, one study has documented that older adults, females, and people with lower education and income were more likely to think that health information on TV is useful (C. J. Choi et al., 2003). To explore this finding more thoroughly, we propose the following multipart hypothesis.
The original CMIS shown in Figure 1 posits a relationship between direct experience and utility. Applying this prediction to our study, we expect that people’s frequent use of TV for health information will be positively related to their perception that TV is useful for health information.
Two other important antecedents to health information seeking are the motivational and psychological factors of health consciousness and health literacy.
Health consciousness refers to people’s attentiveness, responsibilities, and motives with respect to health (Hong, 2011), and it serves as a motivational force that makes people pay more attention to health (Iversen & Kraft, 2006). It incorporates people’s sense of health-related alertness, involvement, and monitoring (Ture & Ganesh, 2012), and it aids efforts to assess their readiness to take health-related actions (Jindabot, 2015). Empirical studies have demonstrated significant relationships between health consciousness and people’s positive responses to health messages and healthy attitudes (e.g., Hong, 2011; Royne, Fox, Deitz, & Gibson, 2014). For example, Hong (2011) found that health consciousness was positively related to people’s intention to carry out an action recommended by health news stories. Similarly, a panel survey among 45-year-old Norwegian women indicated that the respondents with a high sense of health consciousness showed adaptive responses to cancer-related messages (Iversen & Kraft, 2006). Another line of research has shown that health-oriented and health-conscious people tend to seek health information more actively (Dutta-Bergman, 2004, 2005). Particularly related to the current study’s focus on TV, Dutta (2007) found that health orientation—measured by health consciousness along with health information orientation, health beliefs, and healthy activities—is positively related to learning health information from a variety of TV programs such as documentaries, news, talk shows, sitcoms, and health shows.
Conceptual definitions and empirical evidence suggest that health consciousness is an important motivational precursor to health-related actions such as information seeking. But the original CMIS model predicts that the motivational precursor leads to people’s perception that TV is useful for health information (utility), which in turn influences actions. Accordingly, we propose a direct relationship between health consciousness and utility, and we explore the direct relationship between the two variables in an alternative model.
Another frequently used variable and predictor of health information seeking is health literacy (see Gutierrez, Kindratt, Pagels, Foster, & Gimpel, 2014; Lam & Lam, 2012; Lubetkin et al., 2015; Manganello & Clayman, 2011). Health literacy refers to the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions (U.S. Department of Health and Human Services [USDHHS], 2000). Health literacy has been defined in various ways. In clinical settings, it includes functional skills specific to relevant health topics (e.g., the Test of Functional Health Literacy in Adults [TOFHLA]; the Rapid Estimate of Adult Literacy in Medicine [REALM]). In everyday life situations in which people seek health information, health literacy generally focuses more on self-reported competency related to understanding and evaluating health information (Norman & Skinner, 2006; Paek & Hove, 2012). Research has examined health literacy as both predictor and outcome. Studies using it as a predictor have examined the relationship between health literacy and trust in different types of health information sources (Lubetkin et al., 2015), and the relationship between health literacy and preference for types of health information sources (Gutierrez et al., 2014). In addition, a study that applied the technology adoption model (TAM) in the context of viewing intention for health TV found that health literacy was a significant antecedent to viewing intention—not directly but indirectly through perceived easiness, enjoyment, and usefulness of health information on TV (M. Choi et al., 2014). In our proposed model, utility is operationally defined in a way similar to perceived usefulness in TAM. Based on the reasoning and empirical findings of previous research, we propose the following hypothesis.
Finally, our information seeking actions variable is slightly different from the ones used in previous studies (see Table 1) in that ours is intention to view health TV programs (cf. Johnson et al., 1995). The key characteristic of this variable is activeness. When viewing TV, people can often end up acquiring information passively. But now that people have to seek out and select a specific channel and program among the many that have proliferated, viewing has become more of an active and deliberate behavior. Within the uses and gratification perspective, Rubin and Perse (1987) categorized the more active type of TV viewing as “instrumental.” Instrumental viewers are active because they watch TV with the deliberate goal of seeking information (Levy & Windahl, 1984). Actively instrumental viewers have more expectations and plans for specific media and program uses, make more cognitive efforts to view TV, and reach out to others to talk about programs they have viewed. We use this conception of intention to view health TV programs as the actions variable of CMIS. This conception is appropriate for two reasons: first, because CMIS is built upon the uses and gratification perspective regarding audiences’ active media uses; second, because the intention to view health TV programs variable reflects how information seeking is a purposive act that is initiated by a perceived need for information.
According to the original conception of CMIS, the demographic and psychological antecedents serve as initial motivating forces, while information carrier factors mainly drive information seeking actions (Johnson & Oliveira, 1988). Among information carrier factors, ICC such as the quality of the content and perceived trust in the content could lead people to seek health information not only directly but also indirectly by way of perceiving that the health information is useful. By contrast, people’s perceived utility could lead directly to their information seeking actions. Using data from the Health Information National Trends Survey (HINTS), Hartoonian et al. (2014) also predicted that perceived quality as ICC was related to cancer information seeking among cancer survivors directly and indirectly through their perceived trust in the cancer-related information. At the same time, they hypothesized that the cancer survivors’ perceived trust in information as utility served as a direct determinant of action. Leaving out ICC, DeLorme et al. (2011) predicted and found a direct relationship between perceived usefulness of specific sources (their utility variable) and use of specific sources (their action variable). Following the lead of these previous studies, we predict the following:
Our proposed model is presented in Figure 2. In addition, we explored several alternative models—for example, direct effects of demographic and psychological antecedents on viewing intention—and compare them with the proposed model.
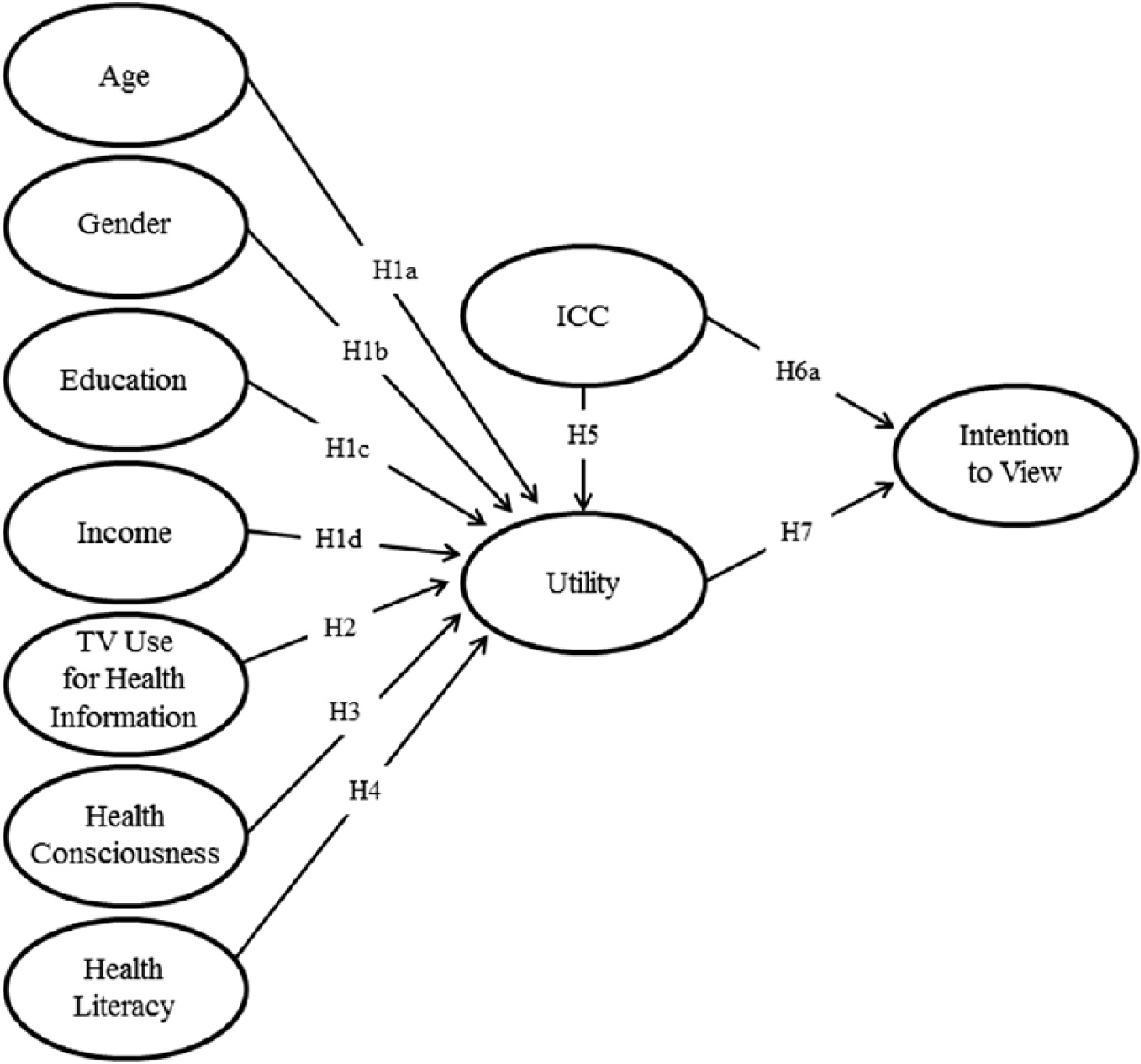
Proposed model.
Method
Data
A leading research firm was hired to collect survey data representative of the entire nation of South Korea. The survey was conducted via face-to-face interviews among 1,020 Korean adults during February 2014. The samples selected reflected regions and age groups proportionally based on an address register that was available at the end of December 2013. More specifically, a lower level of administrative unit (Gu/Goon) was proportionally allocated to each of the selected cities/provinces nationwide based on the population composition of each region. Within each unit, households with people aged 19 or older were randomly chosen to participate in the survey.
Survey Procedure and Sample Characteristics
Each interviewer conducted 15 to 20 face-to-face interviews through door-to-door visits. The interviewers were already experienced, and they were trained extensively and informed about the purpose of the current study and the content of the questionnaire so that they would all have similar understandings of the survey. Thorough training sessions were also provided to avoid any interviewer bias and to standardize the interview procedure. Before conducting the interviews, interviewers informed the respondents about their rights and assured them about privacy and confidentiality as protected by the Korean Statistics Act. Once the respondents agreed to participate, those younger than 60 years answered each survey question by themselves, based on the interviewers’ explanations. For interviewees older than 60 years, interviewers asked them each question and recorded their answers. The entire interview took about 30 to 40 min.
Among the total 1,020 respondents, 56.4% were females. Mean age was 46.84 (SD = 14.54), with each age bracket well distributed. Monthly income on average was 3.79 (SD = 1.81), ranging from 2 to 4 million Korean won (about US$2,400-US$4,800). Mean education level was between high school graduate and 2-year technical college graduate (SD = 1.08). This study’s demographic characteristics closely resemble Korean census data (Korean Educational Statistics Service [KESS], 2016; Korean Statistical Information Service [KSIS], 2016a, 2016b), albeit with slightly different numbers for females (census data: females = 50.0%), age (39.8 years), and education level (51.9% high school degree). For more detailed demographic data, see Table 2.
Descriptive Statistics.
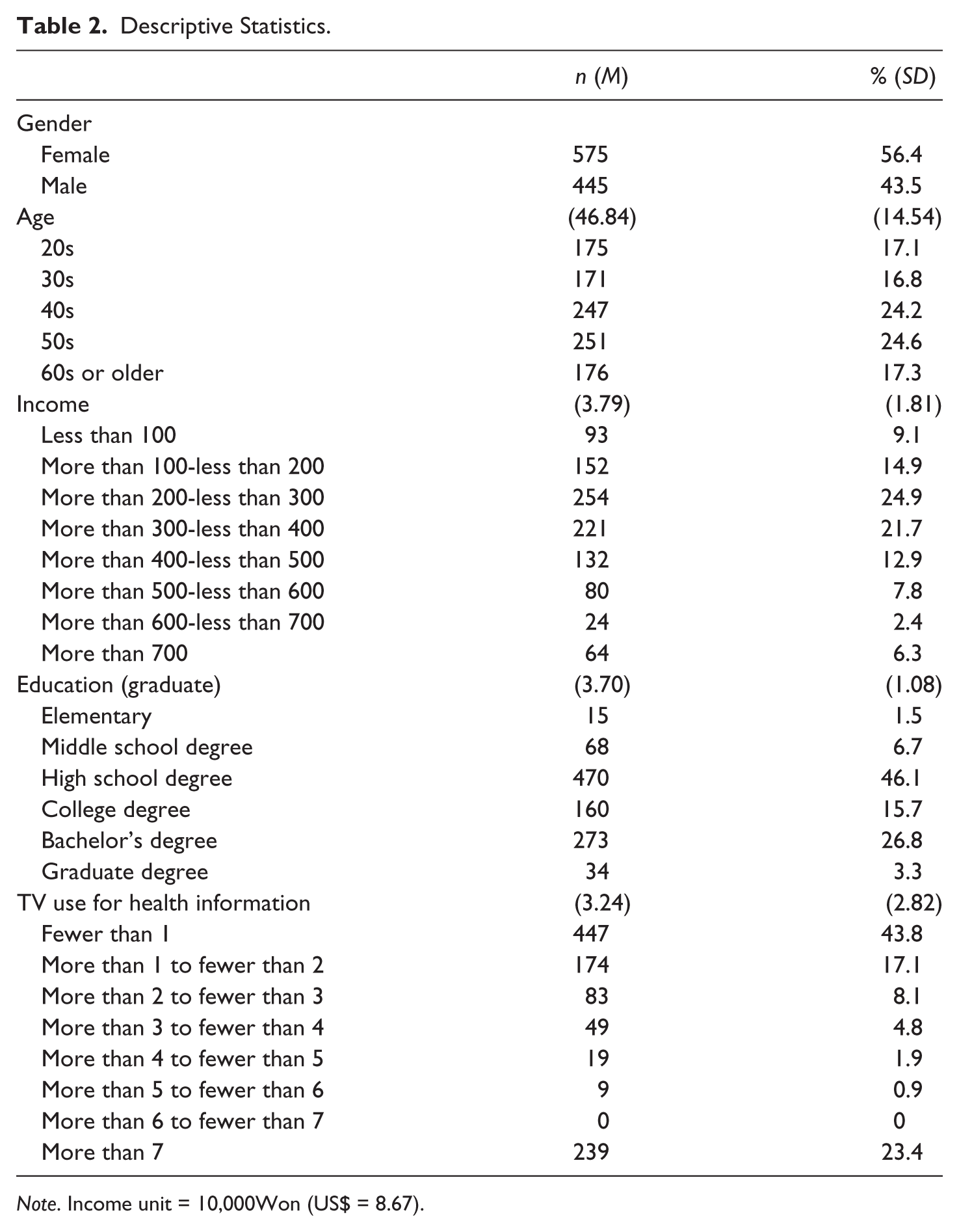
Note. Income unit = 10,000Won (US$ = 8.67).
Measures
The action variable for this study was intention to view (health TV programs). The information carrier factors were media trust as ICC and utility. The antecedent variables included sex, age, income, education, and frequency of TV use for health information. Variables measured with multiple items were examined with the following: exploratory factor analysis (EFA) for preliminary factor structure; Cronbach’s alpha reliability for internal consistency; and confirmatory factor analysis (CFA) for checking discriminant/convergent validity and measurement model fit.
Intention to view was constructed with three question items that were drawn from existing literature and modified to fit the current study context (Levy & Windahl, 1984; Park & Hwang, 2001): (a) “If a new health program is on TV, I will be among the first to watch it”; (b) “If a new health program is on TV, I will inform other people about it”; (c) “I will actively recommend viewing health programs to other people.” Responses were rated on a 5-point Likert-type scale with 1 = not at all and 5 = very much. EFA indicated clearly one factor (89.85% of total variance explained). Reliability analysis also showed strong internal consistency (α = .94).
For information carrier factors, ICC was measured with two media trust items that were drawn from an early study of CMIS (Johnson & Oliveira, 1988): “How much do you trust health information on (a) network TV and (b) cable TV?” Responses were rated on a 5-point Likert-type scale with 1 = not at all and 5 = very much. EFA indicated clearly one factor (87.67 % of total variance explained). Interitem correlation was .75. The utility variable was measured with three items on the same 5-point scale: (a) “Health programs improve my life”; (b) “Health programs give me useful information”; and (c) “Health programs help me with my own health issues” (Johnson & Meischke, 1993; Payne, Severn, & Dozier, 1988). EFA indicated clearly one factor (78.58% of total variance explained). Reliability analysis also showed strong internal consistency (α = .86).
For the salience- and beliefs-related antecedents, health consciousness and health literacy were measured. Health consciousness was measured on the same 5-point scale with two items: (a) “I am very involved with my health” and (b) “I often talk about health with my friends, family, or relatives” (Hong, 2009). EFA indicated clearly one factor (79.27 % of total variance explained). Interitem correlation was .59 (p < .001).
Health literacy was measured with four items drawn from existing literature on e-health literacy (Norman & Skinner, 2006; Paek & Hove, 2012) and modified to fit the current study’s context: (a) “I know where (through which channel) to find useful health information”; (b) “I can understand the health information that health programs provide”; (c) “I know how to judge whether the health information in media is reliable or unreliable”; and (d) “I know how to use the health information I find on media to help myself” (5-point Likert-type scale with 1 = not at all and 5 = very much). EFA indicated clearly one factor (75.42 % of total variance explained). Reliability analysis also showed strong internal consistency (α = .89).
In addition to demographic characteristics such as age, gender, income, and education level, frequency of TV use (for health information) was included as an antecedent to intention to view health TV programs. The frequency variable was measured with the question, “How many times do you use TV for health information?” To acquire accurate and detailed responses, the response category ranged from times per day to times per year. This large range also enabled identification of a range of respondent types from heavy to light health information users. The variable was computed as follows: times/year {times × (day × 365) or (week × 52) or (month × 12) or (year × 1)}. Descriptive statistical results show that people’s TV use for health information ranged from 0 (never, 22.9%) to 70.19 times (0.1%) per year. Because diagnostic statistics showed nonnormality (skewness = 4.297, kurtosis = 33.912), the frequency variable was recoded on an ordinal-scale weekly basis to meet the normality assumptions for SEM testing as follows: (a) fewer than 1 time, (b) more than 1 time to fewer than 2 times, (c) 2 times to fewer than 3 times, (d) 3 times to fewer than 4 times, (e) 4 times to fewer than 5 times, (f) 5 times to fewer than 6 times, (g) 6 times to fewer than 7 times, and (h) 7 times or more (M = 3.24, SD = 2.82).
Model Specification
Prior to model specification, we checked structural equation modeling (SEM) assumptions such as multicollinearity and normality and found no evidence for violating any assumptions. Before fitting the proposed model using SEM, we first fit our measurement model by performing CFA using the AMOS 18 program with the maximum likelihood estimates method. A listwise deletion method was used to handle missing data. Because the chi-square test is sensitive even to small misfit when the sample size is large (i.e., more than 200; Kline, 1998), several goodness of fit indexes were also examined: root mean square error of approximation (RMSEA); Tucker–Lewis index (TLI); standardized root mean square residual (SRMR); and comparative fit index (CFI; Hu & Bentler, 1999). For model evaluation, these indexes were designed to avoid some of the problems of sample size and distributional misspecification associated with the conventional overall test of fit (the χ2 statistic; Hu & Bentler, 1999; Kline, 1998). For the maximum likelihood method, it is generally considered that a value close to 1.00 on both the nonnormed fit index (NNFI; or TLI in AMOS) and the CFI represents a good fit; a model counts as acceptable if SRMR is less than .08 (Hu & Bentler, 1999). RMSEA values between .05 and .08 are considered to be an “adequate” fit, and values between .08 and .10 a “mediocre” fit (Browne & Cudeck, 1993). A CFA model, with five latent variables constructed by 14 observed indicators, was reasonably well fitted: chi-square (67) = 221.08, p < .001, RMSEA = .05 (90% confidence interval [CI] = [.041, .055]), TLI = .98, SRMR = .03, CFI = .98. (For factor loadings see Figure 3. For correlations of the variables see the appendix.)
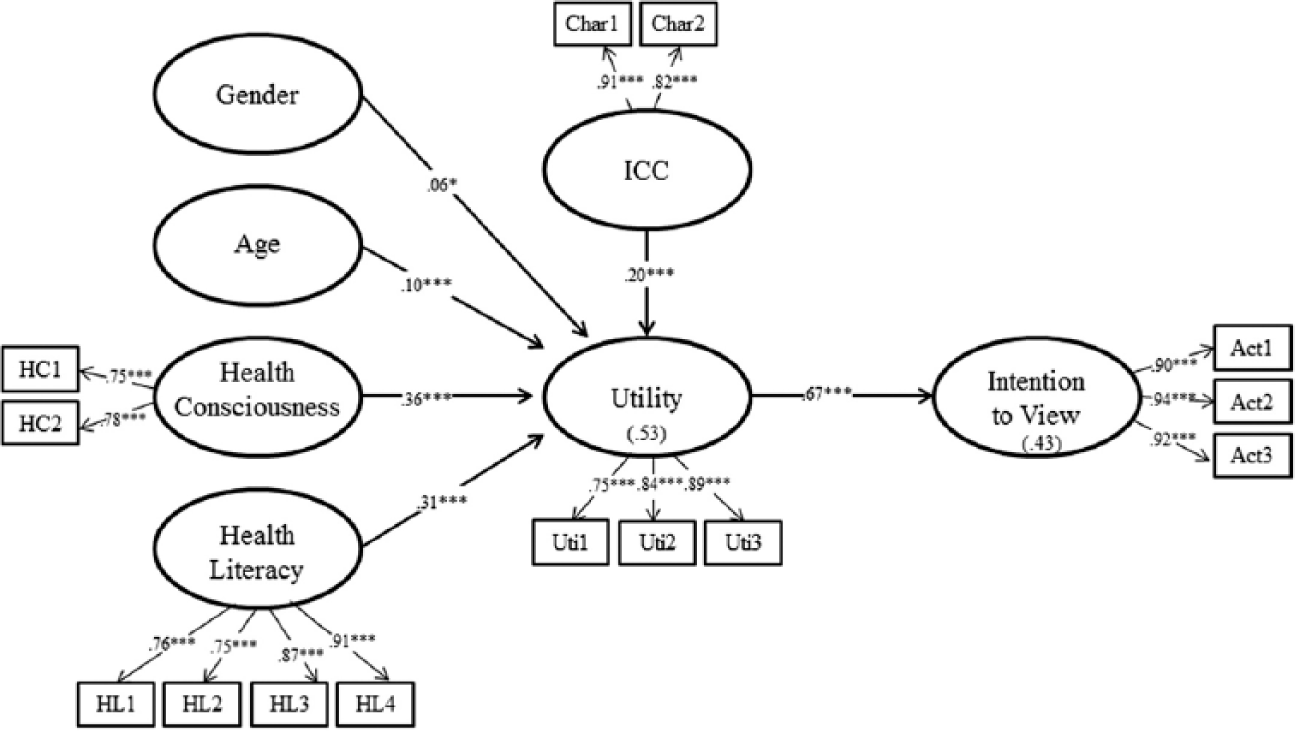
Final fitted model.
After the measurement model fit was verified, discriminant and convergent validity of the latent variables were examined. Results showed that all items significantly (p < .001) loaded to the intended factors, indicating good convergent validity (Anderson & Gerbing, 1988). In addition, our investigation of correlations demonstrated discriminant validity because it showed that all measures had higher correlation with the items of the corresponding latent variable than with items of the other latent variables (Kline, 1998). After fitting and trimming the measurement model, SEM was fitted with the 10 latent constructs and 19 observed indicators by adding five demographic and behavioral variables (age, gender, income, education level, and frequency of TV use for health information), each of which was measured with a single item and therefore not included in the CFA model. Following the original CMIS, the error terms of the seven antecedents (exogenous variables) were all correlated with each other (by AMOS default), but they were excluded from Figure 3 to simplify presentation. The proposed model was reasonably well fitted: chi-square (119) = 348.76, p < .001, RMSEA = .04 (90% CI = [.038, .049]), TLI = .97, SRMR = .03, and CFI = .98. Figure 3 shows standardized coefficients and statistical significance for the final model. Although the model shown in Figure 3 fits the proposed model, it presents only the significant paths for the sake of simplicity. All the gamma and beta coefficients are presented in Table 3.
Parameter Estimates (N = 1,020).
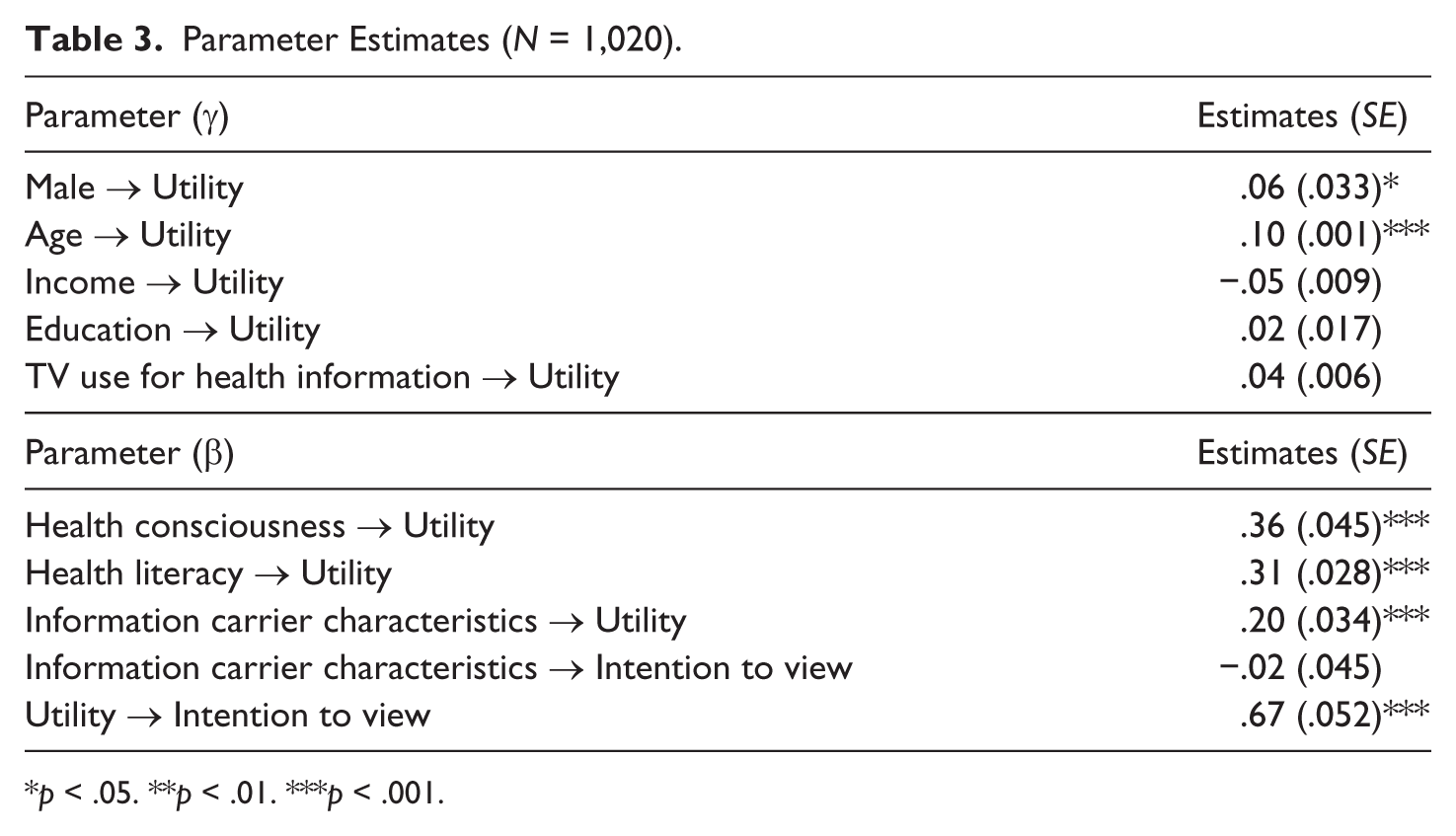
p < .05. **p < .01. ***p < .001.
Results
The fitted model generally confirms CMIS, showing significant relationships among the antecedents, information carrier factors, and intention to view. First, as predicted, among the demographic antecedents age and gender were significantly and positively related to utility. That is, older adults and females are more likely to think that health TV programs are useful for improving their life and health (completely standardized coefficient = .06 and .10, p < .05 and .001, respectively). These findings support
Both psychological antecedents—health consciousness and health literacy—were positively related to utility, supporting
For information carrier factors, ICC were significantly related to utility, supporting
Finally, utility was significantly related to intention to view, supporting
Altogether, the proposed model explained 43% of total variance in intention to view.
Testing Alternative Models
While the original CMIS did not directly relate demographic and psychological antecedents to actions, previous studies suggest the potential for direct relationships between them (Hartoonian et al., 2014; Johnson et al., 1995). We therefore considered this possibility and fitted four alternative models that link the paths toward intention to view from each of the following four significant antecedents: gender and age (demographic), and health consciousness and health literacy (psychological). Results are presented in Table 4. Age (completely standardized coefficient = .055, p < .05), but not gender (completely standardized coefficient = .034, p = ns), was significantly and directly related to intention to view. The model with the path linking age and intention to view also improved model fit (chi-square difference test = 4.14, df = 1, p < .05). Among the psychological antecedents, health consciousness was significantly related to intention to view (completely standardized coefficient = .187, p < .001), while health literacy was not (completely standardized coefficient = .026, p = ns). The model that links health consciousness to intention to view improved model fit significantly (chi-square difference test = 19.34, df = 1, p < .001), while the other model that links health literacy to intention to view did not (chi-square difference test = .57, df = 1, p = ns).
Goodness of Fit Indexes and Chi-Square Differences for Model Modifications (N = 1,020).
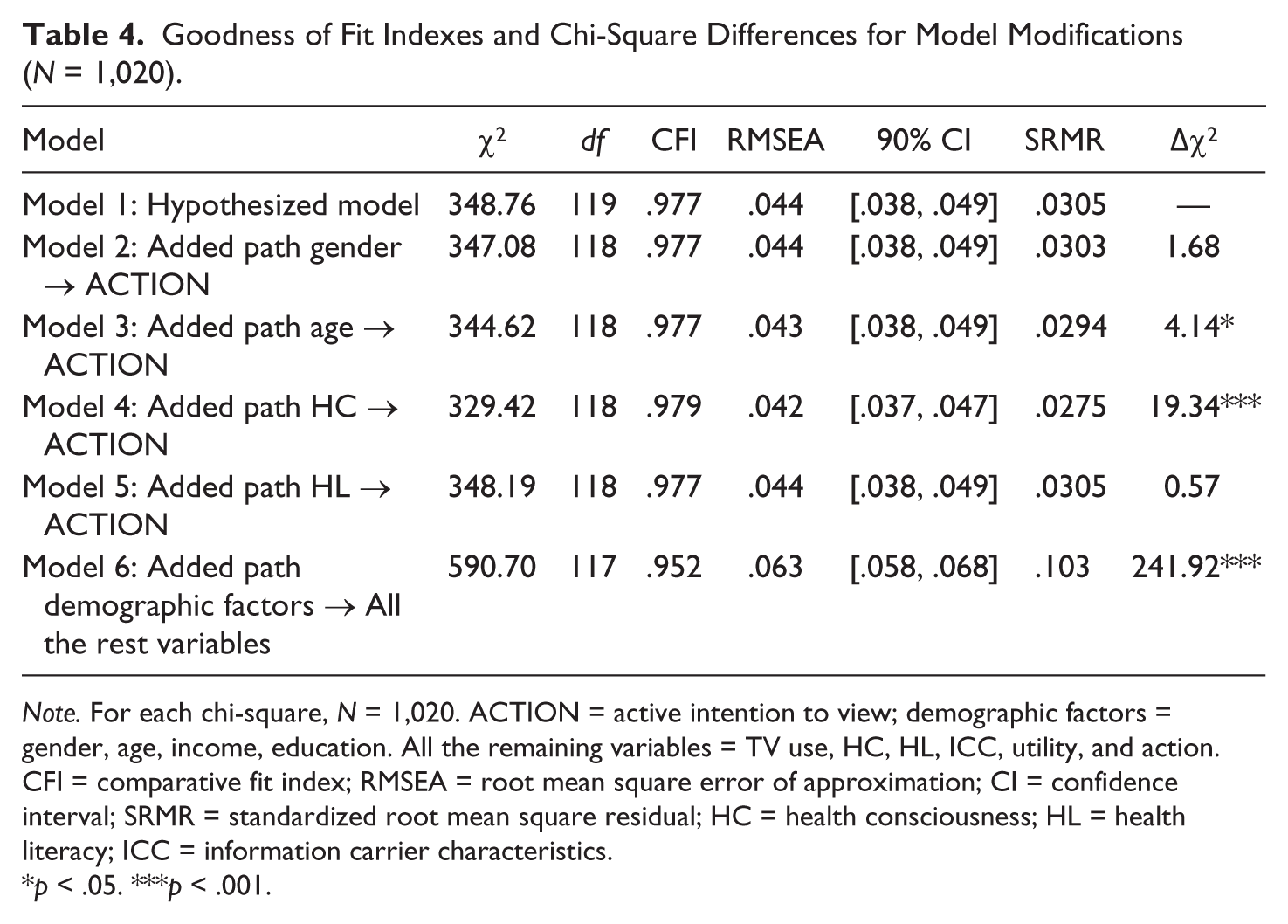
Note. For each chi-square, N = 1,020. ACTION = active intention to view; demographic factors = gender, age, income, education. All the remaining variables = TV use, HC, HL, ICC, utility, and action. CFI = comparative fit index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean square residual; HC = health consciousness; HL = health literacy; ICC = information carrier characteristics.
p < .05. ***p < .001.
Finally, we explored Model 6 in Table 4, which treated the demographic variables as exogenous variables. However, according to a chi-square difference test, Δχ2(dfD = 2) = 241.92, p < .001, the model fit was significantly poorer than that of our proposed model.
Discussion
In apparent response to increasing public interest in health, health programs have proliferated on South Korean television. The current study attempted to identify the factors associated with and processes through which Korean adults intend to view such programs. To achieve this goal, it employed the CMIS in a version modified to fit the context of health TV programming. Results show that CMIS was generally well fitted.
Major Findings
First, among the demographic antecedents, gender (female) and age were positively and significantly related to utility as an information carrier factor. This finding makes sense because females and older adults tend to prefer TV as a media channel, particularly for health information (M. Kim & Yoo, 1996). A recent national survey on media dependency in South Korea also indicates that older adults tend to depend more on TV (Korea Press Foundation, 2015). A contrasting finding was that education level and income were not significant antecedents to subsequent evaluation and information seeking actions. This finding may indicate that TV is a media channel that can overcome health information inequalities across socioeconomic status. According to Coverdell and Utley (2005), health information gaps are likely to remain even in societies where the Internet grows rapidly, and especially where there is poverty, illiteracy, or indifference. By comparison, TV is a more available medium, and it has become more popular in recent years as people continue to view cable and network TV not only on traditional home sets but also online (Drier, 2015). In addition, our alternative model testing the direct relationship between age and action may imply that older adults, who are usually less active in seeking information online (Cline & Haynes, 2001), are likely to be more active in viewing health programs on TV.
The finding that some of the demographic antecedents (i.e., education, income) were not significant may imply that psychological antecedents play a more critical role in people’s evaluation of health information carriers. Health consciousness and health literacy (replacements for salience and beliefs in the original CMIS) were found to be significant antecedents to people’s perception of TV health programs’ usefulness. The important role of such motivational factors in health information seeking has been consistently documented in previous studies (Dutta-Bergman, 2004, 2005). Our post hoc results on the direct relationship between health consciousness and intention to view further support Dutta’s (2007) claim that motivation is a strong antecedent to both evaluating health information and taking further health information seeking actions. This finding suggests that motivating people to care about health and to seek out useful health information could help them take better advantage of the health information provided by TV. Motivational factors therefore need to be considered for better understanding of how people not only seek but also process health information.
Furthermore, health literacy has been found to be a significant predictor between trust in types of health information source and health information seeking (Lubetkin et al., 2015), and between preference for types of health information source and health information seeking (Gutierrez et al., 2014). It therefore makes sense to find that people who perceive themselves to know and evaluate health information properly will find health programs to be useful. The issue of how people assess utility with respect to the quality of health TV programs is beyond the current study’s scope. However, it is possible that improving people’s health literacy can lead them to make more critical assessments of the utility, usefulness, and quality of health information on various health TV programs and to use that information to maintain and improve their health.
Finally, turning to information carrier factors, utility was positively related to intention to view, but the ICC variable was not. Instead, ICC was indirectly related to intention to view through utility. This result suggests that the degree to which people trust in health programs on network and cable TV may not itself be sufficient to motivate them to seek for health programs on TV. In other words, even if people across all age groups prefer TV as a medium, they will not seek out health programs unless they have already evaluated them to be useful.
The insignificant relationship between ICC and information seeking actions is inconsistent with the original CMIS studies by Johnson and his associates (1993; Johnson et al., 1995), as well as a later CMIS study by Hartoonian et al. (2014). This inconsistency may be explained by the different operational definitions of ICC and information seeking actions (also see Table 1 for operating variables). For ICC, Johnson and Meischke (1993) used a multi-item, multidimensional scale: editorial tone (five items) and communication potential. By contrast, the current study captures only the dimension of their scales that is related to editorial tone (i.e., trust in health programs on TV). Their information seeking actions were operationalized with magazine exposure to cancer information and its extent, while our action variable was intention to view. However, their study also showed a stronger relationship between utility and actions than between characteristics and actions, which is consistent with our study and suggests that utility plays a stronger role in predicting actions.
Another explanation for the inconsistent finding may be the unstable nature of CMIS. In organizational communication contexts, Johnson and his associates (1995) ended up with much messier results: failure to fit the original CMIS, insignificant relation between characteristics and actions, and insignificant relation between utility and actions. In their later study in the context of cancer, Hartoonian et al. (2014) also failed to fit the original CMIS, and to improve the model fit at an acceptable level they had to add post hoc paths between salience and actions. These studies seem to indicate that CMIS may not be sufficiently robust, and that its conceptual and operational definitions need to be further refined.
Limitations
Two main limitations should be noted. First, as mentioned earlier, several of our variables’ operational definitions may be limited. One is that of ICC, whose measures in the current study incorporate only media trust. To explain intention to view more clearly and to delineate more diverse pathways through which people intend to actively use health TV programs, future studies may need to include more psychological antecedents in addition to salience and beliefs.
Second, our action variable was not actual behavior such as information seeking and exposure to cancer information but rather behavioral intention related to active TV viewing. But according to the uses and gratifications approach (Levy & Windahl, 1984; Rubin & Perse, 1987), our measures of viewing intention (i.e., “be one of the first to view a health TV program” “recommend health TV programs to others”) are well suited to the conception of information seeking as a purposive act initiated by a perceived need for information, as opposed to a passive viewing behavior like mere exposure. Nevertheless, future research should explore people’s actual viewing behavior of various health TV programs.
Third, while CMIS is by nature a causal model (Johnson et al., 1995) and therefore requires SEM, our cross-sectional survey data are limited in making strong causal claims. Thus, all the significant causal paths found in our study should be interpreted as correlational rather than causal until we replicate our findings using experimental data.
Conclusion
Despite these limitations, the current study yields several theoretical and practical implications. For its theoretical contributions, it applies CMIS to the previously unstudied context of health TV programs in South Korea, and it finds the model to be well fitted. Since existing research on CMIS has been done mainly in the United States and in the contexts of organizational communication (Johnson et al., 1995), cancer information (Hartoonian et al., 2014), and prescription drugs (DeLorme et al., 2011), this study’s findings extend that research both geographically and topically. These findings can also give future CMIS studies directions for improving and refining the conceptual and operational definitions of the model’s key factors, and for clarifying the relationships among them. The unstable nature of the original CMIS and the inconsistent findings in previous research may have been partly the result of differing conceptual and operational definitions. The current study further tested alternative models to achieve more rigorous model comparisons, and it used important health-related psychological antecedents (health consciousness and health literacy) to improve explanatory power. One of the CMIS’s theoretical contributions is to have included information carrier factors (characteristics and utility) that mediate the relationships between antecedents and actions. However, these factors should be more rigorously defined both conceptually and operationally. In addition, considering other mediators could improve CMIS’s explanatory power.
As for practical implications, this study highlights how TV can serve as an important and widely used medium for health information. Despite the rapid development of digital technology and personally tailored media, recently network and cable health TV programs have proliferated not only in South Korea but also around the globe (Drier, 2015). Health TV programs package useful information in a variety of entertainment and narrative formats, and as a result they have become a viable source of health information for many people—particularly older adults, the poor, and the less educated. Compared with the Internet, TV continues to be more widely available and less susceptible to accessibility issues. If, as industry statistics and trends show, people are becoming more health conscious, they will evaluate health TV programs to be more useful and therefore actively seek them out. Improving health literacy also helps people to evaluate and detect differences in the quality of health information. Learning such information from health TV programs could help people improve their knowledge of health, make better informed decisions, and adopt healthier behaviors.
Footnotes
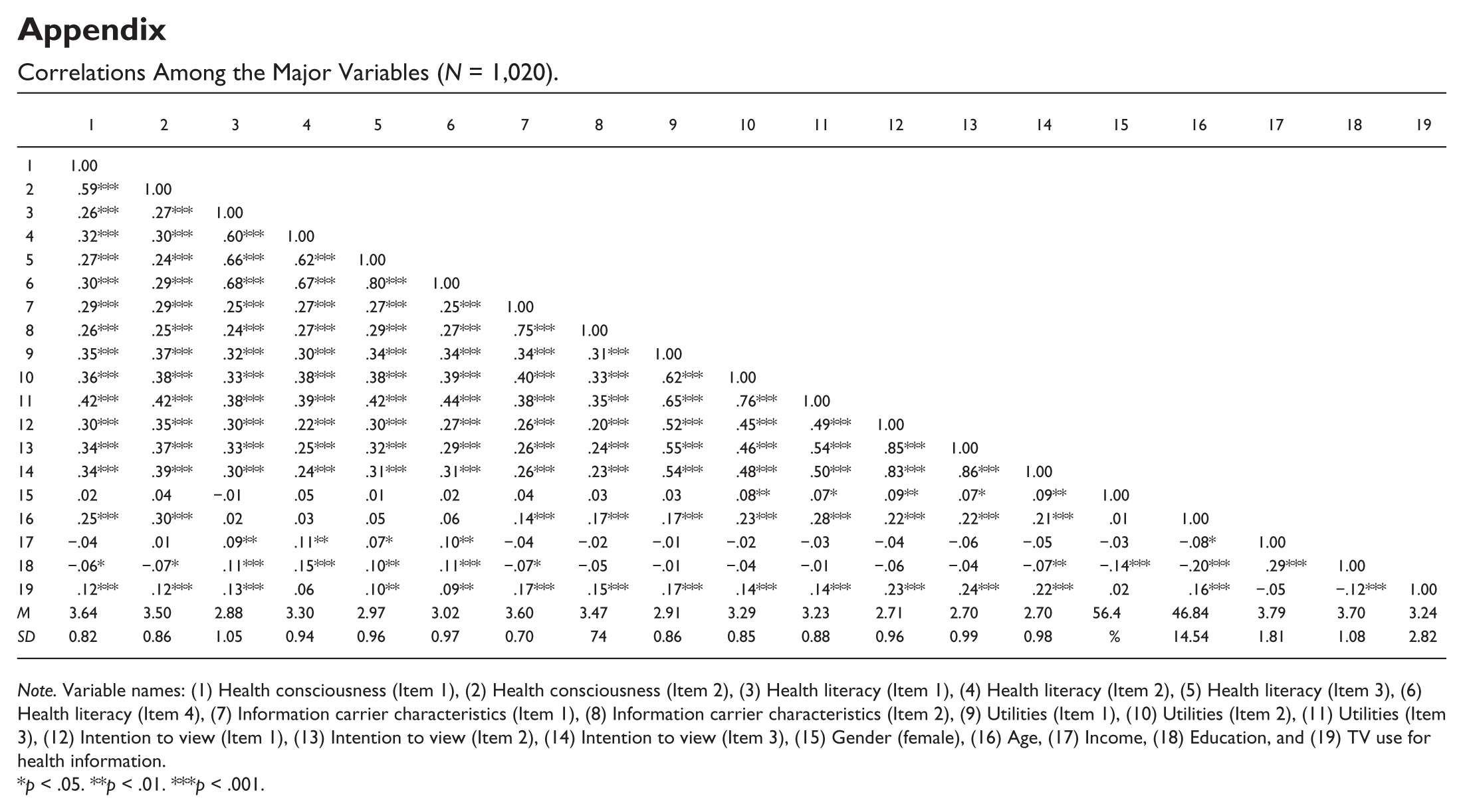
Appendix
Correlations Among the Major Variables (N = 1,020).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1.00 | ||||||||||||||||||
| 2 | .59*** | 1.00 | |||||||||||||||||
| 3 | .26*** | .27*** | 1.00 | ||||||||||||||||
| 4 | .32*** | .30*** | .60*** | 1.00 | |||||||||||||||
| 5 | .27*** | .24*** | .66*** | .62*** | 1.00 | ||||||||||||||
| 6 | .30*** | .29*** | .68*** | .67*** | .80*** | 1.00 | |||||||||||||
| 7 | .29*** | .29*** | .25*** | .27*** | .27*** | .25*** | 1.00 | ||||||||||||
| 8 | .26*** | .25*** | .24*** | .27*** | .29*** | .27*** | .75*** | 1.00 | |||||||||||
| 9 | .35*** | .37*** | .32*** | .30*** | .34*** | .34*** | .34*** | .31*** | 1.00 | ||||||||||
| 10 | .36*** | .38*** | .33*** | .38*** | .38*** | .39*** | .40*** | .33*** | .62*** | 1.00 | |||||||||
| 11 | .42*** | .42*** | .38*** | .39*** | .42*** | .44*** | .38*** | .35*** | .65*** | .76*** | 1.00 | ||||||||
| 12 | .30*** | .35*** | .30*** | .22*** | .30*** | .27*** | .26*** | .20*** | .52*** | .45*** | .49*** | 1.00 | |||||||
| 13 | .34*** | .37*** | .33*** | .25*** | .32*** | .29*** | .26*** | .24*** | .55*** | .46*** | .54*** | .85*** | 1.00 | ||||||
| 14 | .34*** | .39*** | .30*** | .24*** | .31*** | .31*** | .26*** | .23*** | .54*** | .48*** | .50*** | .83*** | .86*** | 1.00 | |||||
| 15 | .02 | .04 | −.01 | .05 | .01 | .02 | .04 | .03 | .03 | .08** | .07* | .09** | .07* | .09** | 1.00 | ||||
| 16 | .25*** | .30*** | .02 | .03 | .05 | .06 | .14*** | .17*** | .17*** | .23*** | .28*** | .22*** | .22*** | .21*** | .01 | 1.00 | |||
| 17 | −.04 | .01 | .09** | .11** | .07* | .10** | −.04 | −.02 | −.01 | −.02 | −.03 | −.04 | −.06 | −.05 | −.03 | −.08* | 1.00 | ||
| 18 | −.06* | −.07* | .11*** | .15*** | .10** | .11*** | −.07* | −.05 | −.01 | −.04 | −.01 | −.06 | −.04 | −.07** | −.14*** | −.20*** | .29*** | 1.00 | |
| 19 | .12*** | .12*** | .13*** | .06 | .10** | .09** | .17*** | .15*** | .17*** | .14*** | .14*** | .23*** | .24*** | .22*** | .02 | .16*** | −.05 | −.12*** | 1.00 |
| M | 3.64 | 3.50 | 2.88 | 3.30 | 2.97 | 3.02 | 3.60 | 3.47 | 2.91 | 3.29 | 3.23 | 2.71 | 2.70 | 2.70 | 56.4 | 46.84 | 3.79 | 3.70 | 3.24 |
| SD | 0.82 | 0.86 | 1.05 | 0.94 | 0.96 | 0.97 | 0.70 | 74 | 0.86 | 0.85 | 0.88 | 0.96 | 0.99 | 0.98 | % | 14.54 | 1.81 | 1.08 | 2.82 |
Note. Variable names: (1) Health consciousness (Item 1), (2) Health consciousness (Item 2), (3) Health literacy (Item 1), (4) Health literacy (Item 2), (5) Health literacy (Item 3), (6) Health literacy (Item 4), (7) Information carrier characteristics (Item 1), (8) Information carrier characteristics (Item 2), (9) Utilities (Item 1), (10) Utilities (Item 2), (11) Utilities (Item 3), (12) Intention to view (Item 1), (13) Intention to view (Item 2), (14) Intention to view (Item 3), (15) Gender (female), (16) Age, (17) Income, (18) Education, and (19) TV use for health information.
p < .05. **p < .01. ***p < .001.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.