
Abstract
This mixed-method study investigated perceptions women domestic violence survivors/victims have about why women do not seek help from formal support structures and actions domestic helping agencies can take to facilitate survivor access to services. Congruent with previous research, quantitative analysis identified 17 reasons women do not seek help from formal support structures. Expanding current knowledge, concept mapping revealed six ways family violence programs can better reach women in abusive relationships, including (1) remove barriers to services, (2) improve comfort with services, (3) “talk about it,” (4) improve community awareness, (5) victim-targeted marketing, and (6) “I honestly don’t know.”
Intimate partner violence (IPV) against women is a prevalent worldwide social and public health concern (e.g., Garcia-Moreno, Watts, Jansen, Ellsberg, & Heise, 2003; Mechanic, Weaver, & Resick, 2008; Saltzman, Green, Marks, & Thacker, 2000). Defined as experienced or threatened physical and/or sexual violence by a current or former intimate partner (Saltzman, Fanslow, McMahon, & Shelley, 1999), worldwide estimates indicate between 15% and 71% of women experience physical and/or sexual abuse in their lifetimes (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). In the United States, the National Violence Against Women Survey found that 25% of all women have been physically assaulted and/or raped by an intimate partner at some point in their lives (Tjaden & Thoennes, 2000a, 2000b). All too often IPV is not limited to acts of physical and sexual violence but also includes a continuum of specific behaviors that includes threats, isolation, coercive control, intimidation, and minimization (Pence & Paymar, 1993). Although professionals working to end family violence use a number of different terms to describe abusive relationships (e.g., domestic violence, battering, partner abuse, IPV), there is little consensus on how these terms are defined and measured (e.g., Cook & Swan, 2006; Graham-Kevan, 2007; Johnson, 2004, 2006; Stark, 2006). For the purpose of the following discussion such issues are less important than finding ways helping programs can better facilitate survivor/victim access to services; thus, the term IPV is used broadly to describe the women’s experiences.
One of the identified problems with reaching IPV victims/survivors is that most abuse goes unreported since “it often occurs in private, and victims are often reluctant to report incidents to anyone because of shame or fear of reprisal” (Catalano, 2007, p. 1). Although the earlier women in abusive relationships seek help the better the outcomes for them and for their children, getting IPV victims/survivors to access family violence intervention services is often difficult. Most women in abusive/controlling relationships simply do not utilize formal helping structures (e.g., shelters, domestic violence support groups, hot lines). Although a number of researchers have addressed the factors influencing help-seeking behavior of this important population (e.g., Bacchus, Mezey, & Bewley, 2003; Liang, Goodman, Tummala-Narra, & Weintraub, 2005; Peckover, 2003), some suggest that understanding how to best reach women IPV victims/survivors is impossible because their voices concerning the utility and/or effectiveness of services designed to help them are generally overlooked (e.g., Fugate, Landis, Riordan, Naureckas, & Engel, 2005; Grauwiler, 2008). To address these cited needs, the current mixed-method study reports the voices of 121 women IPV survivors concerning reasons they believe women do not seek help and ways they feel family violence intervention agencies can better reach other women in abusive relationships.
A Serious Problem
Finding ways to reach women in violent relationships is important because of the serious impact that IPV has on society as a whole and on the lives of women victims/survivors. The economic consequences of IPV in the United States are estimated to exceed US$5.8 billion annually, which include financial costs related to medical and mental health services (Centers for Disease Control [CDC], 2003) and lost productivity at home and in the workplace (CDC, 2003; Tjaden & Thoennes, 2000a). More important than the economic costs are the serious problems IPV causes for the women who are in violent relationships. These consequences are well documented and include acute and chronic health problems (e.g., Campbell, 2002; Coker, Smith, Bethea, King, & McKeown, 2000; Heise, 1993; Tjaden & Thoennes, 2000a, 2000b), ongoing mental health concerns (e.g., Golding, 1999; Jaffe, Wolfe, Wilson, & Zak, 1986), and reduced ability to care for self and family. National and state-specific studies indicate 40% to 60% of women IPV victims/survivors experienced substantial physical injury from their assaults (CDC, 1998, 2000; Tjaden & Thoennes, 2000a, 2000b), whereas 30% of all homicides involving women victims in 2006 were IPV related (Catalano, 2007). Few would argue with the statement that IPV is a serious problem with serious consequences.
Help Seeking Defined
With IPV prevalence large and consequences extreme, a need exists for helping agencies to reach out to women who are in abusive relationships. However, successful outreach is often dependent on the ability and willingness of women victims/survivors to seek help from others. It is important to note that blame for the abuse should always fall on the offender/abuser and should never be placed on the victim/survivor. Likewise, each victim/survivor has the right to self-determine whether or not to seek help and from whom (if anyone) to seek help. Such help-seeking behavior is defined as disclosure of IPV victimization in an effort to obtain assistance (e.g., Mays, Caldwell, & Jackson, 1996; Morrison, Luchok, Richter, & Parra-Medina, 2006; Taylor, Hardison, & Chatters, 1996). Although disclosure of IPV victimization and help seeking share similarities, the two concepts are different (e.g., Montalvo-Liendo, 2009; Naved, Azim, Bhuiya, & Persson, 2006; Rodriguez, Quiroga, & Bauer, 1996). Disclosing abuse to a health care worker or family friend does not necessarily mean the woman is ready to obtain services or leave the abusive relationship but may instead be indicative of an attempt to cope with the situation (e.g., Montalvo-Liendo, 2009; Naved et al., 2006). For example, an injured woman who unwillingly discloses abuse to her primary care doctor is not considered help seeking. Similarly, a woman who is not interested in obtaining services but verbally shares her story with a friend who can listen and validate her experiences is not considered help seeking. Such disclosure may be a first step in preparation for help seeking, but unless the goal to obtain assistance is present, it is not considered help seeking for the purpose of the current discussion and study.
To better understand the help-seeking process, Liang et al. incorporated cognitive theory into a conceptual framework suggesting three relevant processes or stages of help seeking: defining the problem, deciding to seek help, and selecting a source of support. These internal processes are influenced by both interpersonal factors (i.e., individual and relational history) and sociocultural factors (i.e., economic, political, and cultural context). Interrelated and variant, these three processes form a dialectical interaction with each informing the other. For example, the way an abused woman defines and appraises her experiences shapes her decision about whether and from whom she will seek help. Individual expressions of oppression, including feelings of guilt and shame brought on by both her abuser and the forms of institutional oppression she encounters, affect current and future decision making. Indeed, the person or organization from whom she chooses to seek help will influence the way she defines her experiences and whether she will choose to seek help again. To understand this process it is essential that a historical and dynamic view of the individual take into account the “inner” influences of action (individual expectations, goals, and beliefs), while also taking into account broader contextual influences of her life experiences (e.g., Brandstadter, 1998; Liang et al., 2005). Thus, the help-seeking process is seldom linear, often protracted, and is influenced by a variety of individual, interpersonal, and sociocultural experiences (Liang et al., 2005).
Formal and Informal Structures
When IPV victims/survivors choose to seek help, they do so from a variety of informal and formal venues (Gondolf & Fisher, 1988; Tjaden & Thoennes, 2000a, 2000b). Research indicates that most women prefer to seek assistance from people in their informal social networks (i.e., family and friends; for example, Horton & Johnson, 1993; Pakieser, Lenaghan, & Muelleman, 1998; Taylor et al., 1996). Support from informal networks is vital to women IPV victims/survivors as it provides: (a) emotional sustenance in the form of advice, affirmation, and encouragement; (b) material support such as financial help, babysitting, transportation, and/or a place to stay (Goodkind, Gillum, Bybee, & Sullivan, 2003); and (c) protective functions in relation to psychological health and well-being (Arias, Lyons, & Street, 1997; Carlson, McNutt, Choi, & Rose, 2002; Tan, Basta, Sullivan, & Davidson, 1995). Although most studies indicate IPV victims/survivors report these informal networks are helpful and supportive (e.g., Horton & Johnson, 1993; Pakieser et al., 1998; Taylor et al., 1993), they are likely unprepared (and sometimes unable) to protect women from their abuser or to help them rebuild their lives. Inversely, formal support structures such as shelters, advocates, crisis hotlines, mental health centers, domestic violence support groups, and other family violence programs are specifically designed to do just that. One of the many problems addressed by professionals working to end family violence is that most women in abusive relationships do not access these formal support structures.
A large body of literature attempts to understand reasons women in abusive relationships do not seek assistance from formal support structures. When summarizing the dearth of empirical evidence related to disclosure and help-seeking behavior, Montalvo-Liendo (2009) focused on cross-cultural factors in her review of 42 studies identifying fear, shame, embarrassment, time constraints by health care providers, health care providers not asking about IPV, religious beliefs, children, language barriers, and cultural prohibitions among the reasons women did not seek help from formal systems. However, different researchers report varied findings. For example, Fugate et al. conducted qualitative interviews with 491 abused women who were seen in different public health care settings with the purpose of better understanding women’s stated reasons for not accessing formal helping services. Data analysis revealed the following seven major themes: (1) not needed or not useful, (2) barriers, (3) protect partner and preserve relationship, (4) privacy and confidentiality, (5) consequences, (6) fear, and (7) other. Fugate et al. then incorporated these seven themes into three broad reasons women in abusive relationships did not seek help: individual thresholds for the seriousness of the violence, a perceived requirement to end the relationship, and certain specific barriers. In their discussion they called for both increased awareness and victim-centered analysis to help broaden conceptual understanding of women IPV survivors’ needs and experiences (Fugate et al., 2005). Although it is clear from the evidence that women in violent relationships have very real reasons for not using formal support services, little is known about how to break through these reasons to better reach the women family violence support agencies are designed to help.
Current Study
From the above discussion, the need to link evidence regarding reasons abused women give for not utilizing formal support structures to practical ways helping agencies can reach them is identified. To understand this we must first understand survivors/victims’ opinions about why women in abusive relationships do not seek services. Therefore, the current mixed-method study elicited the opinions of 121 women IPV survivors to investigate the following research questions:
Research Question 1: What are women survivors’ beliefs concerning why people who are abused do not seek help from formal structures?
Research Question 2: How do women IPV survivors believe domestic violence intervention service providers can better reach those women who are in need of services?
Method
Because a great deal is known about reasons women give for not seeking help from formal services, quantitative methods are appropriate to address the first research question. However, the descriptive-exploratory nature of the second research question lends itself to qualitative methods. Therefore, the current study uses a mixed-method design to analyze help-seeking behaviors and opinions about how to best reach women who are in violent relationships.
Participants
Participants for this study include 121 women IPV survivors recruited from two helping agencies in a metropolitan area located in the mid-South region of the United States. Although all of the women included in this study were actively engaged in services from formal support structures at the time of this study, each also had a period of time when they were in an abusive relationship and had not sought such services. Therefore, they were selected as viable informants to address the research questions. Their ages ranged from 20 to 52 years with a mean age of 32 years (SD = 7.13). Ethnic representation was predominantly African American, 71.9% (N = 87), with 17.4% (N = 21) self-identifying as Caucasian, 7.4% (N = 9) as Hispanic, and 3.3% (N = 4) as “Other.” Most of the participants (61.2%) reported employment outside the home (N = 74). The relationship participants had with the offender varied with 43.8% (N = 53) reporting being separated, 43.8% (N = 53) reporting other/unsure, 9.9% (N = 12) reporting being divorced, and 2.5% (N = 3) reporting still living with/dating their abuser. The length of their relationships ranged from 1 to 23 years with a mean length of 6.76 years (SD = 4.90).
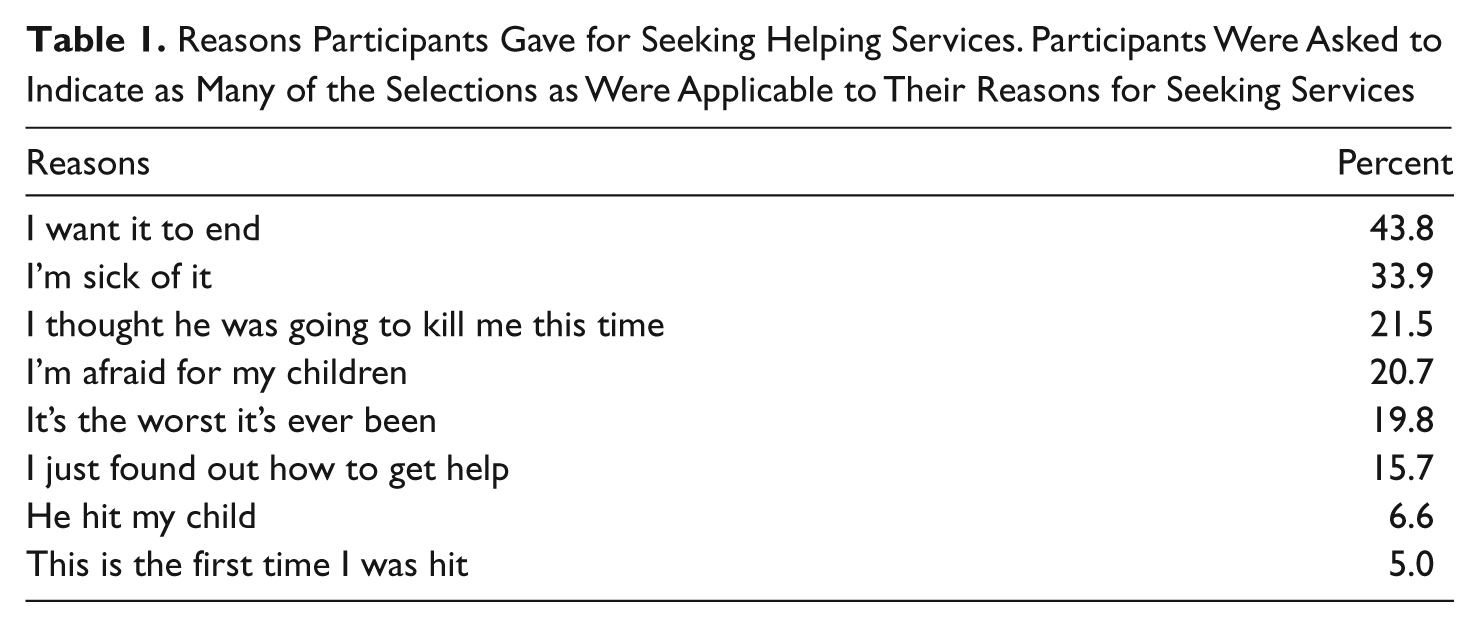
History of help-seeking behavior is important to this study. Therefore, participants were asked how long they waited to seek help after the most recent violent incident and to select the reasons they chose to seek help from a list of choices. Most of the participants, 57.8% (N = 70), waited more than a week after the most recent violent incident to seek help from formal IPV services; 21.4% (N = 23) sought help that day or the next day, and 20.7% (N = 25) sought help between 1 and 7 days after it happened. Table 1 shows the reasons participants gave for seeking help. The most frequently indicated reasons were, “I want it to end” (43.8%, N = 53) and “I’m sick of it” (33.9%, N = 41). Relatively few indicated it was because their child was hit (6.6%, N = 8), or because it was the first time they had been hit (5%, N = 6). Participants were also given the opportunity to write “other” reasons, including two who lost custody of their children, three who had nowhere to live, and two who wrote, “my church.”
Reasons Participants Gave for Seeking Helping Services. Participants Were Asked to Indicate as Many of the Selections as Were Applicable to Their Reasons for Seeking Services
Measurement
Variables were measured using a short survey instrument designed to better understand participants’ help-seeking experiences and their opinions about why women who are abused do not seek help. Based on literature indicating a need to include IPV survivors in service provision decisions (e.g., Fugate et al., 2005; Liang et al., 2005; Montalvo-Liendo, 2009), the instrument utilizes mixed response, Likert-type scale, and open-ended opinion questions. Two primary question clusters were analyzed for this study. The first was a series of 5-point Likert-type scale questions asking participants to indicate degree of agreement or disagreement to 17 statements about why women who are abused do not seek help. The second was an open-ended question that asked participants to provide their opinion about what formal helping agencies can do to better reach women who are abused. The 17 statements (included in Table 2) and the open-ended question were based on findings from previous conceptual and empirical work (e.g., Fugate et al., 2005; Liang et al., 2005; Montalvo-Liendo, 2009) with the assistance from staff and former clients of the cooperating agency.
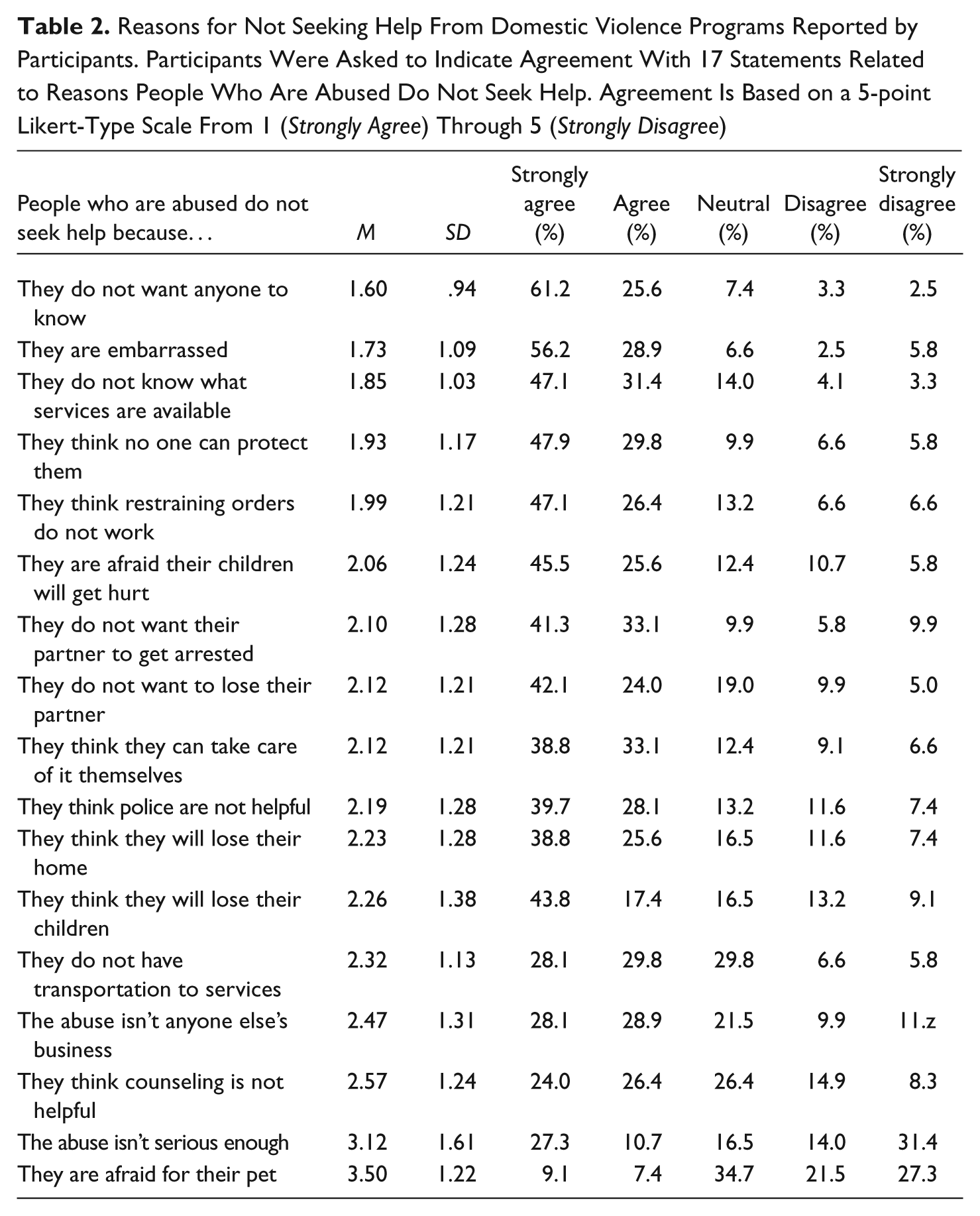
Reasons for Not Seeking Help From Domestic Violence Programs Reported by Participants. Participants Were Asked to Indicate Agreement With 17 Statements Related to Reasons People Who Are Abused Do Not Seek Help. Agreement Is Based on a 5-point Likert-Type Scale From 1 (Strongly Agree) Through 5 (Strongly Disagree)
Qualitative Data Analysis
A concept mapping approach to data analysis was selected for the qualitative portion of this project because it synthesizes qualitative data into a quantitatively structured diagram. Based on the work of Trochim (1989a, 1989b) and Jackson and Trochim (2002), concept mapping has been used for research in the areas of public health (Burke et al., 2005; Trochim, Cabrera, Milstein, Gallagher, & Leischow, 2006), mental health (Johnsen, Biegel, & Shafran, 2000), study abroad programs (Poole & Davis, 2006), and program evaluation (Kane & Trochim, 2007).
The process of concept mapping consists of 5 distinctive stages where qualitative data are reduced and sorted into meaningful categories. In the first stage, participants’ responses to the survey question were divided into units of analysis with each unit consisting “of a sentence or phrase containing only one concept” (Jackson & Trochin, 2002, p. 313). In the second stage, eight people (coders) representing a variety of backgrounds independently sorted these units of analysis into meaningful groups. From the sorting process, a matrix was created for each coder using a binary code grid with cell values representing “whether (1) or not (0) a pair of statements was sorted by that coder into the same pile” (p. 315). The individual grids were then combined into a larger matrix with cell values representing the number of coders who combined the respective concepts (i.e., units of analysis). In the third stage, multidimensional scaling analysis was conducted on the larger matrix using the computer program SPSS. The multidimensional scaling function graphically showed how different objects of comparison do or do not cluster based on a series of similarity or distance judgments made by the sorters in Step 2 of the concept mapping process. During multidimensional scaling, a type of perceptual mapping takes the form of a scatter plot (or perceptual map) using a Euclidean Distance model. The stability of these scatter plots was reported using (a) the stress value, which ranges from 0.0 to 1.0 with 0.0 indicating a perfect goodness of fit, and (b) the RSQ (i.e., correlation between factors), which ranges from 0.0 to 1.0 with 1.0 indicating a perfect solution. In the fourth stage, individual points on the scatter plots (the units of analysis) were grouped together into final cluster solutions. Clusters were based on (a) the location of answers on the scatter plot, (b) the appropriateness of merging and splitting the statement groups, and (c) the number of times sorters grouped the ideas together with all of the connections being made by at least 75% (N = 6) of the sorters. In the fifth stage, clusters were named based on the central idea of the group cluster, recommendations of the sorters, and the best judgment of the primary researcher.
Results
Research Question 1
To address the first research question, “What are women survivors’ beliefs concerning why people who are abused do not seek help?,” participants were asked to indicate agreement with 17 statements related to reasons people who are abused do not seek help. Table 2 shows the findings in order of support according to a 5-point Likert-type scale ranging from 1 (strongly agree) to 5 (strongly disagree). Most participants reported a belief that women in violent relationships did not seek services because of shame (86.8% agree or strongly agree with “did not want anyone to know” and 85.1% agree or strongly agree with “embarrassed”). Following these were indications that participants believed there was a lack of information available to women in abusive relationships (78.5% agree or strongly agree with “did not know what services were available to them”) and a belief that helping services cannot provide safety (77.8% agree or strongly agree with the item “no one can protect them” and 73.5% agree or strongly agree with the item “restraining orders do not work”). After personal safety, reasons for not seeking help included concerns for their children’s safety (71.1% agree or strongly agree with the item “afraid their children will get hurt”), desire for partner not to be arrested (74.2% agree or strongly agree with “do not want their partner to get arrested”), and fear of losing the relationship (66.1% agree or strongly agree with “do not want to lose their partner”). Participant responses to this question are further shown in Table 2.
Research Question 2
To address the second research question, “How do women IPV survivors believe domestic violence service providers can better reach those women who are in need of services?,” participates were asked the open-ended question, “What do you think we can do to bring people to our program who are abused and not getting help?” Responses were analyzed using the concept mapping approach previously described (e.g., Jackson & Trochin, 2002; Trochim, 1989a, 1989b). The Euclidean Distance model revealed 6 answer clusters with a stress value of .106 and an RSQ value of .957 after 4 iterations indicating a stable solution using the Kruskal’s stress formula. Illustrated in Figure 1, answer clusters include (a) remove barriers to services, (b) improve comfort with services, (c) “talk about it,” (d) improve community awareness, (e) victim-targeted marketing, and (f) “I honestly don’t know.”
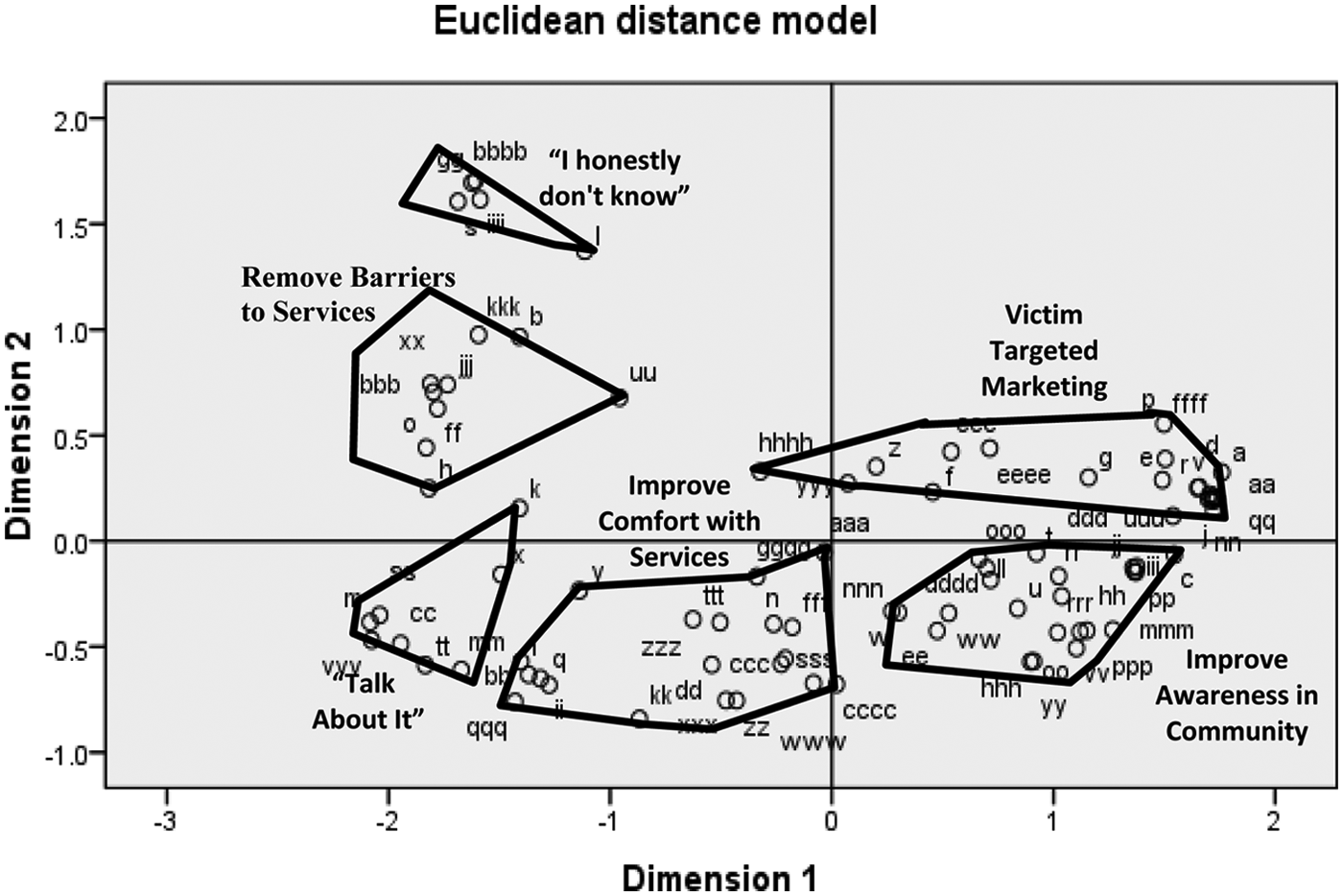
The concept map represents participants’ answers to the question, “What do you think we can do to bring people to our program who are abused and not getting help?”
Cluster 1, improve community awareness, represents 28.7% of the responses and includes answers indicating that advertising should target victims. Rather straightforward, this cluster included ideas such as “advertise,” “TV commercials,” “. . . if possible go to them,” “community outreach,” and “put out more information on TV or radio, drop flyers” would be helpful. One participant stated, “Some women don’t know how much help is out there,” while another stated, “Advertise more on TV and in places women most likely go (grocery store, laundromats).”
Cluster 2, improve comfort with services, represents 26.4% of the responses and includes answers indicating that survivors can be better served by incorporating practices designed to make the victim/survivor feel more comfortable with the services provided. Although responses did not cluster as such in analysis, three primary means emerge from this larger cluster. The first is directly related to reassurance that the victim/survivor feels she is cared about such as “continue to show you care and make victim feel you are attentive to family,” “make victims feel comfortable to talk,” and “let them know that they will be safe and not judged.” The second encourages victims/survivors to reach out to those women in violent relationships such as “have survivor victims speak to other victims,” “bring in people who have had similar experiences to meet with them,” and “testimonies from survivors.” The third is related to confidentiality and privacy such as “encourage them that what they say is confidential” and “private counseling with individual.”
Cluster 3, victim targeted marketing, represents 19.5% of the responses and includes answers indicating word of mouth or “buzz” will help. Responses in this cluster include increasing awareness for women in violent relationships such as “spread the word about services,” “better words of mouth,” and “basically just getting the word out there, so many of us are just afraid.” A second idea incorporated into this includes better description of services available such as “explain programs that are available,” “give them information,” “make information more available instead of waiting for police help,” and “make sure the info is out there, ask questions at ER, clinic, and DHS visits. Let the person know that it is completely confidential & set up codes. Women are dying for help out here.”
Cluster 4, remove barriers to services, represents 10.9% of the responses and includes answers indicating that difficulties many women have accessing services, such as language and transportation, should be addressed. Responses in this category include “many times it is the language (Spanish) or the lack of information or simply clients cannot drive (no transportation),” “. . . provide a taxi voucher to get to and from counseling . . .,” and “. . . some places have turned some away because of requirements.” Interestingly, two participants noted that criminal justice responses to the abuser form a barrier that needs to be removed: “keep the abuser away . . . once the abuser is locked up he should not be able to make bail and get out to hurt the woman” and “making sure the abuser is put away the first time he strikes the abused.”
Cluster 5, talk about it, represents 9.1% of the responses and includes answers indicating the need to talk about family violence to people in the community. Responses include “getting together and talking about it,” “our race (African American) needs to have more communication,” “talk to them as much as you can,” “keep talking to people to let them know there is help,” and “encourage people to talk about domestic violence.” Some of the participants felt talking about it will increase awareness such as “help them build strength and know that there are options,” “stress the importance of breaking the cycle,” “put on workshops for women,” and “education on services available, info on the typical things victims do that cause them to stay in an abusive relationship.”
Cluster 6, “I honestly don’t know,” represents 5.7% of the responses and includes answers indicating they were unsure what would work. Responses include “I honestly don’t know,” “I am not sure,” and “unsure.”
Discussion
For those working in the field some of the findings of this study are not surprising. It is generally known that reaching women in abusive relationships is predicated on breaking through concerns about embarrassment, fear, distrust, and safety (Fugate et al., 2005; Montalvo-Liendo, 2009). It is also known that there is a need to both remove barriers to services and improve existing services. However, it is interesting that the IPV victim/survivor participants provided support for the need to (a) improve services and marketing by asking women who have elicited help to “talk about it” with others, (b) improve overall community awareness about what domestic violence is and what helping services are available in the community, and (c) target marketing specifically at women in violent relationships. It is also interesting that a number of women indicated they honestly don’t know how to improve outreach services. From these findings emerge practical ways that formal systems (i.e., shelters, advocates, crisis hotlines) can better help women in abusive relationships define the problem, decide to seek help, and select a source of support.
Research Question 1: Supporting the Known
Results from items designed to investigate Research Question 1 add to the current body of knowledge by providing additional support for known explanations abused women have for not seeking help from formal support structures. As discussed in the literature review, women in violent relationships have very real reasons for not seeking help from formal helping services, including fear, shame, embarrassment, religious beliefs, children, language barriers, and cultural prohibitions (Fugate et al., 2005; Montalvo-Liendo, 2009). The current study was designed with this previous research in mind. Thus, similar results are not unexpected with the majority of participants (>50%) agreeing or strongly agreeing with 15 of the 17 listed reasons women do not seek help from formal helping systems. As is the case with previous research, women participants of the current study endorsed shame and embarrassment, concern for their children, concerns for partner, and fear as reasons women in abusive relationships do not seek help from formal support structures.
An important piece that is not consistently found in previous literature is strong support for the idea that abused women don’t utilize formal support systems because they both lack information about services that are available and believe that helping services cannot provide safety. What is interesting about these findings is that most family violence agencies do a great deal of outreach targeted at their identified population. In addition, family violence intervention agencies work diligently to help manage/minimize the risks victims/survivors are exposed to by their abusive partner, by life factors, and by involvement in the system(s). However, these findings indicate that those working in the antidomestic violence field may need to work harder promoting the message that services are available and, indeed, they can provide options, resources, and information that are likely to improve safety. Combined with the qualitative findings, these two ideas indicate that outreach methods may need to (a) be tailored to specific populations, (b) include direct marketing of services that are available to abused women, and (c) focus on improving understanding about safety protocols formal support services follow.
Research Question 2: Broadening Knowledge
Expanding the empirical knowledge about how to better reach women who are being abused, the current study provides ways family violence intervention programs can improve their outreach efforts. Representing more than half of the responses (57.3%), three of the clusters specifically address the need for better marketing. The first cluster indicated participants thought there was a need to improve community awareness about what domestic violence is and what helping services are available. Although many family violence intervention agencies make significant attempts to do this, participants of the current study believe greater effort is needed. A second similar cluster of respondents identified a need to target marketing specifically to women in abusive relationships, and a third cluster acknowledged the need to “talk about” family violence. It is clear that IPV is not a “safe” topic for many women to discuss. However, the more we can improve community awareness, communication, and understanding, the more likely it is that we can encourage attentiveness to what family violence is and what services are available to help.
The current study also provides support for the need to improve services to women who are being abused. Representing more than one third of the responses (37.3%), two clusters identified the need to improve these services (Cluster 2 and Cluster 4). The first of these clusters (Cluster 2, improve comfort with services) identified three ways this can be done: (1) ensure the victim/survivor feels cared about, (2) ensure confidentiality and privacy, and (3) encourage victims/survivors to reach out to other women in violent relationships. Interestingly, the first two ideas coincide with research and conceptual work addressing ways helping professionals can better engage and encourage ongoing involvement with communities, parents, and trauma survivors (Franco, Chambers, Miranda, & McKay, 2006; McKay, Pinto, Bannon, & Guilamo-Ramos, 2006; Sperber & McKay, 2008). The third, encouraging victims/survivors to reach out to others, has likely been tried by multiple agencies with various degrees of success. Issues of safety, privacy, and simply keeping track of survivors make it difficult for agencies to lead this activity, though it certainly has merit and is a good area for future research and practice endeavors. Despite the limitations, it is clear from these responses that survivors believe they will be better served by practices designed to make them feel more comfortable, connected, and safe.
In addition to improving victim/survivor comfort with services, participants indicated that barriers to services exist and need to be removed. Barriers identified include language, transportation, and criminal justice responses. The conceptual framework described by Liang et al. provides further support for these ideas. A woman who chooses to seek support from an agency she believes to be supportive and responsive to her needs influences the way she defines her experience, her decision to continue with services, and her decision about seeking help in the future (Liang et al., 2005). Thus, providing supportive services, listening to women’s needs, ensuring confidentiality, removing barriers to services, and increasing options and resources for improving safety are likely to aid both immediate and future help seeking.
The final cluster underscores the fact that women in abusive relationships are a difficult population to reach. Although the smallest cluster, 5.7% of respondents reported they do not know how to better reach other abused women. Regardless of what those in the family violence intervention professions do, self-determination is an important aspect of intervention. Women have to (a) feel the services are relevant to them, (b) believe the services increase their options and resources, and (c) trust the services will keep them safe. It is the responsibility of domestic violence intervention professionals to continue working to ensure these criteria are met and to find ways to better reach women in abusive relationships. However, this is a difficult task that requires creativity to accomplish.
Limitations
There are three primary limitations of the current study. First, it should be stated that the participants of this study were self-identified IPV victims/survivors who were in the process of eliciting services from family violence intervention programs. Therefore, findings are indicative of women who have utilized formal support structures. The time that elapsed between their not seeking services and the present may have altered their perceptions of the helpfulness of formal support structures and the things necessary to help others who are not utilizing such services. Second, it is possible that participants do not represent the entire population of women in abusive relationships; the sample was relatively small (N = 121), not randomly selected, and recruited from an urban area. A third limitation is related to the nature of measurement. The quantitative list of statements used to address the first research question, though based on findings of prior conceptual and empirical work (Fugate et al., 2005; Liang et al., 2005; Montalvo-Liendo, 2009), consisted of a finite list of responses with a limited scope. Likewise, the qualitative questions used to address the second research question were broad and subjective in nature. Thus, more research is needed to determine whether the findings are generalizable to the greater population. Nevertheless, findings of the current work are helpful to understand the opinions of the current study’s participants because they may have insight into the help-seeking behavior/beliefs of those not yet ready to seek services due to an array of reasons (e.g., risks from the abusive partner and/or systemic barriers that may prevent access to services).
Conclusion
In closing, findings of the current study provide additional support to previous findings indicating that help seeking is dependent on breaking through concerns about embarrassment, fear, distrust, religious beliefs, children, language barriers, and cultural prohibitions (Fugate et al., 2005; Montalvo-Liendo, 2009). In addition, findings expand the current knowledge by eliciting the opinions of women IPV survivors about how domestic violence intervention service providers can better reach those women being abused by an intimate partner. The resulting six response clusters provide ways formal support structures can better reach women with abusive partners. Indeed, it is important for family violence programs to remove barriers to services, improve survivor comfort with services, help people “talk about it,” improve community awareness, and target marketing directly to women in violent relationships.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.