
Abstract
In a sample of 242 women in treatment for severe mental illness (SMI), we used regression analysis to test the hypothesis that lifetime physical and sexual abuse would correlate with self-harm behaviors (thoughts of self-harm and suicide, self-harming behaviors, and suicide attempts) when controlling for psychiatric symptoms, substance abuse, and negative appraisals of trauma. Lifetime physical abuse and alcohol use were the only significant factors in the model. Women with SMI should be screened regularly for physical abuse, alcohol use, as well as thoughts and behaviors related to self-harming behaviors. Limitations of the study include its cross-sectional design.
Introduction
Traumatic events such as physical and sexual abuse, having witnessed violence, or having experienced a life-threatening illness or injury are relatively common in people with schizophrenia spectrum and major mood disorders (i.e., severe mental illness [SMI]) with rates of having experienced one or more traumatic events approaching 90% or more (Lu et al., 2013; Mueser et al., 1998; O’Hare, Shen, & Sherrer, 2013c; O’Hare & Sherrer, 2009; Resnick, Bond, & Mueser, 2003). Rates of posttraumatic stress disorder (PTSD) range from 29-43% in SMI samples (Mueser et al., 1998; O’Hare, Sherrer, & Shen, 2006; Resnick et al., 2003) compared with the roughly 8% estimated in the general public (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Traumatized people with SMI have more severe psychiatric symptoms, incur increased risk for additional trauma, engage in more high risk behaviors (e.g., suicide attempts, self-mutilation, unprotected sex), more substance use, and have poorer treatment outcomes in general (Gearon, Kaltman, Brown, & Bellack, 2003; Lu, Mueser, Rosenberg, & Jankowski, 2008; O’Hare, Shen, & Sherrer, 2010; O’Hare et al., 2006; Rosenberg, Lu, Mueser, Jankowski, & Cournos, 2007).
Physical and sexual abuse are among the most frequently reported traumas in people with SMI, and a large proportion of victims have experienced multiple episodes (Mueser et al., 1998; O’Hare et al., 2013c; O’Hare & Sherrer, 2009). Mueser et al. (1998) reported that 44.7% of clients with SMI reported childhood sexual assault (females, 52.0%; males, 35.5%) and 18.3% reported childhood physical abuse (females, 16.3%; males, 20.8%). Rates of sexual assault during adulthood were reported by 46.7% (females, 63.6%; males, 25.9%), and 37.8% for physical assault (females, 36.3%; males, 39.7%). O’Hare and Sherrer (2009) found that 65.2% of women with SMI had been physically abused at least once in their lifetime and 48.4% had been victimized multiple times. Over half (53.6%) had been sexually abused at least 1 time with 31% reporting multiple episodes. For both lifetime physical and sexual abuse, these rates were about twice as high in women compared with men, although Mueser et al. (1998) found rates of physical abuse to be comparable by gender. However, in another sample, O’Hare et al. (2013c) found similar differences by gender for rates of both physical and sexual abuse as in their previous sample, and regression analysis revealed that lifetime physical abuse (but not sexual abuse) significantly correlated with posttraumatic symptoms when other psychiatric symptoms (e.g., depression, psychosis) were controlled. Collectively, several studies have shown that abused clients with SMI reported more severe symptoms of SMI and PTSD, more comorbid diagnoses, more substance abuse, and more frequent high risk behaviors (e.g., suicide attempts, self-harm) than nonabused clients (Gearon et al., 2003; Lu et al., 2008; O’Hare et al., 2013c; O’Hare et al., 2006; Rosenberg et al., 2007).
Abuse and Self-Harming Behaviors in People With SMI
Self-harm includes thoughts of self-harm and suicide, self-harming behaviors (e.g., cutting, burning oneself), and suicide attempts. People diagnosed with an SMI, including schizophrenia and major mood disorders, are at the highest risk for suicide among people with any mental illness (Arsenault-Lapierrer, Kim, & Turecki, 2004; Bolton & Robinson, 2010; Harris & Barraclough, 1997; Hawton, Sutton, Haw, Sinclair, & Deeks, 2005; Hor & Taylor, 2010; Kessler, Borges, & Walters, 1999; Palmer, Pankratz, & Bostwick, 2005; Saha, Chant, & McGrath, 2007). Risk factors for suicide include being younger, male, White, unemployed, relatively well educated, unmarried, having had good premorbid functioning, a family history of suicide, having suffered from severe depression and hopelessness, experienced family stressors, a history of substance abuse, and having made previous suicide attempts. Although men complete more suicides, women engage in more self-harming behaviors (e.g., cutting, self-poisoning, overdosing on medications) including suicide attempts (Harris & Barraclough, 1997; Haw, Hawton, Sutton, Sinclair, & Deeks, 2005; Hawton, Sutton, Haw, Sinclair, & Harriss, 2005; Hawton, Zahl, & Weatherall, 2003; Zahl & Hawton, 2004).
Despite the fact that trauma and suicide share some common risk factors (e.g., self-harm, depression, substance abuse), little research has explored trauma, including abuse, as a potential risk factor for suicide in people with SMI (Heila et al., 1999). A few studies of people diagnosed with schizophrenia and other mental illnesses (see Hor & Taylor, 2010, for review) have demonstrated that sexual and or physical abuse and other forms of interpersonal violence correlate with both suicidal thinking (Rosenberg et al., 2007) and completed suicides (Cohen, Abdallah, & Diwan, 2010). Similar links between suicide and trauma have been found in clients with major mood disorders (Gladstone et al., 2004). In a sample of SMI patients (including both schizophrenia and mood disorders), O’Hare, Shen, and Sherrer (2014) found that when controlling for psychiatric symptoms, lifetime self-injury, lifetime physical abuse (but not sexual abuse), and recent (6 months) alcohol use were significantly correlated with lifetime suicide attempts. Other trauma, including sexual abuse, traumatic losses, having witnessed violence, and life-threatening illness or injury, was not related to suicide attempts.
Cognitive Appraisal of Trauma
A growing body of theory and research has begun to focus on the role of cognitive mediators of trauma and its consequences. Evidence suggests that the victim’s negative cognitive appraisal of traumatic events with respect to their view of the self, the world, and potential for self-blame appear to play an essential role in the onset and persistence of posttraumatic stress symptoms (Brewin & Holmes, 2003; Dalgleish, 2004; Ehlers & Clark, 2000; Foa, Huppert, & Cahill, 2006). Negative appraisals can be obsessively intrusive and persistent due to the reinforcing effects of the victim’s conscious suppression of trauma-related thoughts and emotions. Negative appraisal of trauma appears to have a similar effect in people with SMI (see Sherrer, 2011, for review), and is correlated with and mediates the severity of PTSD symptoms (Kilcommons & Morrison, 2005; Mueser et al., 2008). Research with similar cognitive constructs also supports the potentially critical role of negative thinking associated with trauma and its effects. In their review, Olff, Langeland, Draijer, and Gersons (2007) found that women generally report greater perceived threat from trauma than men, thus putting them at greater risk to experience more psychiatric symptoms such as anxiety and depression. In a sample of men and women with SMI, O’Hare et al. (2006) showed that subjective distress from physical and sexual abuse had a significant direct effect on posttraumatic stress symptoms and a significant indirect effect via subjective distress associated with high risk behaviors (e.g., self-harming behaviors, suicide attempts). Women in that sample reported significantly more subjective distress from physical and sexual abuse than did men. In a separate sample, O’Hare, Shen, and Sherrer (2013b) found that lifetime self-injury and subjective distress from physical abuse (but not sexual abuse) were significantly correlated with lifetime suicide attempts when controlling for a range of psychiatric symptoms including substance abuse. In that sample, women reported significantly more suicide attempts; significantly greater symptoms of depression, mood dysregulation, and posttraumatic stress; and greater subjective distress related to both physical and sexual abuse.
The Current Study
In the current study, we focused exclusively on a sample of women with SMI to assess the relationship between a lifetime history of abuse and self-harming thoughts and behaviors. We hypothesized that lifetime frequency of physical and sexual abuse would be significantly associated with self-harming behaviors. Departing from previous related studies, we computed self-harm as the sum of thoughts of self-harm and suicide, self-harming behaviors, and nonfatal suicide attempts which we conceptualize on a continuum of proneness toward self-harm. To isolate the unique association between physical and sexual abuse and self-harm, we controlled for psychiatric symptoms (i.e., depression, psychosis, interpersonal problems, posttraumatic stress symptoms), substance abuse, and negative appraisals of the self, the world, and self-blame. We also controlled for symptoms of SMI rather than diagnosis as people with schizophrenia spectrum and major mood disorders share a range of common symptoms to one degree or another (Abrams, Rojas, & Arciniegas, 2008; Baynes et al., 2000), and because some studies with SMI samples have shown that people with major mood disorders report more trauma (including physical and sexual abuse) and engage in more suicide attempts and self-harm than do those with schizophrenia spectrum disorders (O’Hare, Shen, & Sherrer, 2013a; O’Hare & Sherrer, 2009). We also controlled for substance abuse (i.e., alcohol, other drugs, problems) given the high rates of comorbidity in people with SMI (Drake & Mueser, 2002), because it is a known risk factor for self-harm and suicide, and because it is a significant risk factor for mood disorders in women (Greenfield, Back, Lawson, & Brady, 2010). Finally, we also controlled for negative cognitive appraisals given their association with psychiatric symptoms (including posttraumatic stress; Kilcommons & Morrison, 2005; Mueser et al., 2008; Sherrer, 2011) in an effort to further isolate the unique variance explained in self-harm by lifetime physical and sexual abuse in this sample of women with SMI.
Method
Sample and Procedure
The original target sample for this study was 500 clients who were interviewed consecutively as part of their routine 6-month reassessments in four participating community mental health centers that provide community support services for people with SMIs in Rhode Island. Eligibility requirements for receiving community support services included having had an Axis I diagnosis of SMI and functional impairments severe enough to require support services to live independently in the community. The largest center from which 200 consecutive cases were sampled is an urban agency with a higher proportion of clients from African American and Hispanic backgrounds. The other three agencies (each of which recruited one hundred consecutive cases) are from more suburban and predominantly white communities. Admission criteria were the same in all centers as determined by the Rhode Island State mental health authority. Four-hundred sixty-six clients (93.2%) provided sufficiently useful data for the study after dropping cases where key data were substantially missing.
Preliminary analysis for this study began with a subsample of 227 women at least 19 years of age or older (age: M = 47.16; SD = 12.10) who were diagnosed by staff psychiatrists with an Axis I disorder of either schizophrenia (81, 35.7%) or major mood disorder (146, 64.3%) and reported one or more incidents of either physical or sexual abuse in their lifetime. One hundred nine (48.0%) had never married, 19 (8.4%) were married, and the rest were separated, divorced, or widowed (91, 40.1%) with two cases (.9%) not reporting. The sample was about three quarters White (168, 74.0%), followed by African American (24, 10.6%), Hispanic (21, 9.3%), and “mixed race” (6, 2.6%), with the remaining clients reporting the following at a rate of less than 1% each: Asian, Pacific Islander, Native American, “not applicable,” and no response. The majority of clients were supported by federal disability insurance (175, 77.1%) with the remainder self-supporting (26, 11.5%) or “other” (7, 3.1%), and eight (3.5%) not reporting. Median annual household income was US$9,000, and two thirds had achieved a high school diploma. Most clients (212, 93.4%) had been hospitalized at least once in their lifetime for a mental health or substance use problem, and almost all (220, 96.9%) were taking psychiatric medications at the time of the study. Clients had been involved with the agency for a median of 8 years, and average Global Assessment of Functioning (GAF) score was 48.30 (SD = 7.46).
This cross-sectional study was conducted as a naturalistic survey whereby data were collected as part of routine care. Four licensed and nationally accredited community mental health centers in Rhode Island participated in this study. The general purpose of the project was to incorporate brief, valid, and reliable measures into routine assessment and 6-month reassessments to enhance monitoring and evaluation of client care. Data were collected between the fall of 2008 and spring of 2009 by members of clinical teams (i.e., social workers, psychiatric nurses, case managers) during the course of their normally scheduled service contacts with clients. Data sources included a combination of face-to-face interviews for key clinical measures (e.g., trauma measures, appraisal measures, psychiatric symptoms, substance use) and medical records to transcribe psychiatrists’ diagnoses, demographic, and treatment event data. Procedures for this secondary data analysis were approved by each individual community mental health center’s quality assurance department and the Institutional Review Board of Boston College.
Measures
We used previously validated scales to measure the following: lifetime sexual and physical abuse, negative cognitive appraisals (of the self, the world, and self-blame), psychiatric symptoms (depression, mood dysregulation, psychosis, interpersonal functioning, posttraumatic stress symptoms), substance use and associated problems, thoughts of harming the self, and lifetime self-injury and suicide attempts. To measure negative appraisals, we used a brief version of the Posttraumatic Cognitions Inventory (PTCI; Foa, Ehlers, Clark, Tolin, & Orsillo, 1999) which assesses cognitions about the self (e.g., “I have been permanently changed for the worse”), the world (e.g., “You can never know who will harm you”), and self-blame (e.g., “The event happened because of the way I acted”) using a 7-point Likert-type scale with response options ranging from 1 (totally disagree) to 7 (totally agree). Higher scores indicate greater endorsement of negative beliefs associated with a traumatic event(s). The reliability and validity of the PTCI has been well established with samples of people with SMI (e.g., Kilcommons & Morrison, 2005; Mueser et al., 2008). We used the extensively validated 24-item Behavior and Symptom Identification Scale (BASIS-24; Eisen, Dill, & Grob, 1994; Eisen, Norman, Belanger, Spiro, & Esch, 2004) to measure six symptom and problem domains: depression, mood dysregulation, psychosis, interpersonal functioning, substance abuse problems, and thoughts of self-harm and suicide over the previous “7 days” using a combination of frequency and severity scales. To measure posttraumatic stress symptoms, we used a brief three-item version of the PTSD Symptom Scale–Interview (PSS-I; O’Hare, Shen, & Sherrer, 2012) version derived from the well-validated PSS-I developed by Foa, Riggs, Dancu, and Rothbaum (1993) and validated with another sample of people with SMI (N = 275; O’Hare, Shen, & Sherrer, 2007). Clients rated their symptoms on each item “over the past 7 days” with regard to the “most stressful or traumatic event” that has ever occurred to them as follows: (0) “not at all,” (1) “once per week/a little,” (2) “2 or 4 times per week/somewhat,” and (3) “5 or more times per week/very much.” Quantity-frequency (QF) of alcohol use was computed by multiplying the first two items of the Alcohol Use Disorders Identification Test (O’Hare & Shen, 2012; O’Hare, Sherrer, LaButti, & Emrick, 2004; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). Within the time frame of the “past 6 months,” respondents estimated “how often” they drank and “how many drinks” (i.e., 12 oz. beer, 5 oz. wine, 1.5 oz. of liquor) they consumed according to the following response set: frequency—(0) “never,” (1) “monthly or less,” (2) “2-4 times a month,” (3) “2-3 times a week,” (4) “4 or more times a week”; quantity—(0) “none,” (1) “one or two,” (2) “three or four,” (3) “five or six,” (4) “seven to nine,” (5) “10 or more.” Frequency of drug use (O’Hare & Shen, 2012) was measured similarly. In response to the query “how often over the past year have you used the following substances?” respondents selected one of the following responses: “never” (0), “less than monthly” (1), “monthly” (2), “weekly” (3), and “daily/almost daily” (4) for each of the following drug categories: marijuana, cocaine, amphetamines, heroin, and other narcotics (e.g., oxycodone); and tranquilizers (without a prescription), hallucinogens (e.g., lysergic acid diethylamide [LSD]), and inhalants. “Total drugs” (drugs only) were calculated through summation of all drug frequency items.
Lifetime sexual and physical abuse, self-harming behaviors, and suicide attempts were measured with the Risky Behaviors and Stressful Events Scale (RBSES; O’Hare et al., 2013c; O’Hare et al., 2006). The scale allows for three approaches to measurement for each item: ever occurred, lifetime frequency, and self-reported subjective distress at the time of interview. In the current study, we examined lifetime frequency (none, 1 time, 2-5 times, 6-10 times, and more than 10 times) which, for analysis purposes, was coded 0, 1, 3.5, 8, and 11). The dependent variable for this study, “self-harm” measures a general proneness toward self-harm by summing the scores from the “thoughts of self-harm/suicide” subscale of the BASIS-24 with lifetime self-reported self-harming behaviors and lifetime suicide attempts from the RBSES.
Data Analysis Plan
We provided data on measures of central tendency for all study variables, a correlation matrix, and then used hierarchical linear regression to test the main hypothesis of the study: Physical and sexual abuse would be significantly associated with self-harm when controlling for psychiatric symptoms, substance use and related problems, and negative appraisals of trauma.
Results
Univariate Data for Key Variables
About two thirds of the respondents (146, 64.4%) reported having been physically abused at least once, and more than half (134, 59.1%) reported multiple episodes of abuse. More than half (118, 53.2%) reported at least one episode of lifetime sexual abuse, and 96 (43.3%) reported more than one episode of abuse. Respondents thought of hurting themselves or committing suicide an average of 3 times in the 7 days prior to their study interview. Sixty-eight women (29.9%) reported self-harming behaviors (e.g., cutting, burning oneself) at least once in their lifetimes, and about one quarter (52, 22.9%) reported multiple incidents. Almost two thirds (142, 62.5%) attempted suicide at least once in their lifetimes, and almost half (104, 45.8%) reported multiple attempts. Eighty-one women (35.6%) reported having consumed some alcohol within the 6 months prior to the study, and 54 women (23.7%) reported having used some drug other than alcohol. Most of the drug use involved marijuana (37, 18.0%), cocaine (19, 9.0%), and sedatives (13, 6.2%). Other drugs, including heroin/opiates, hallucinogens, amphetamines, and inhalants, were reportedly used by 10 or fewer women in the sample. Because the frequency distributions for alcohol and other drugs were highly skewed, we transformed them for further analysis by calculating the cubed and square root, respectively. All scores reported in Table 1 are normally distributed or have moderate positive skews of <±2.
Means, Standard Deviations, and Range for All Key Study Scores and Subscales.
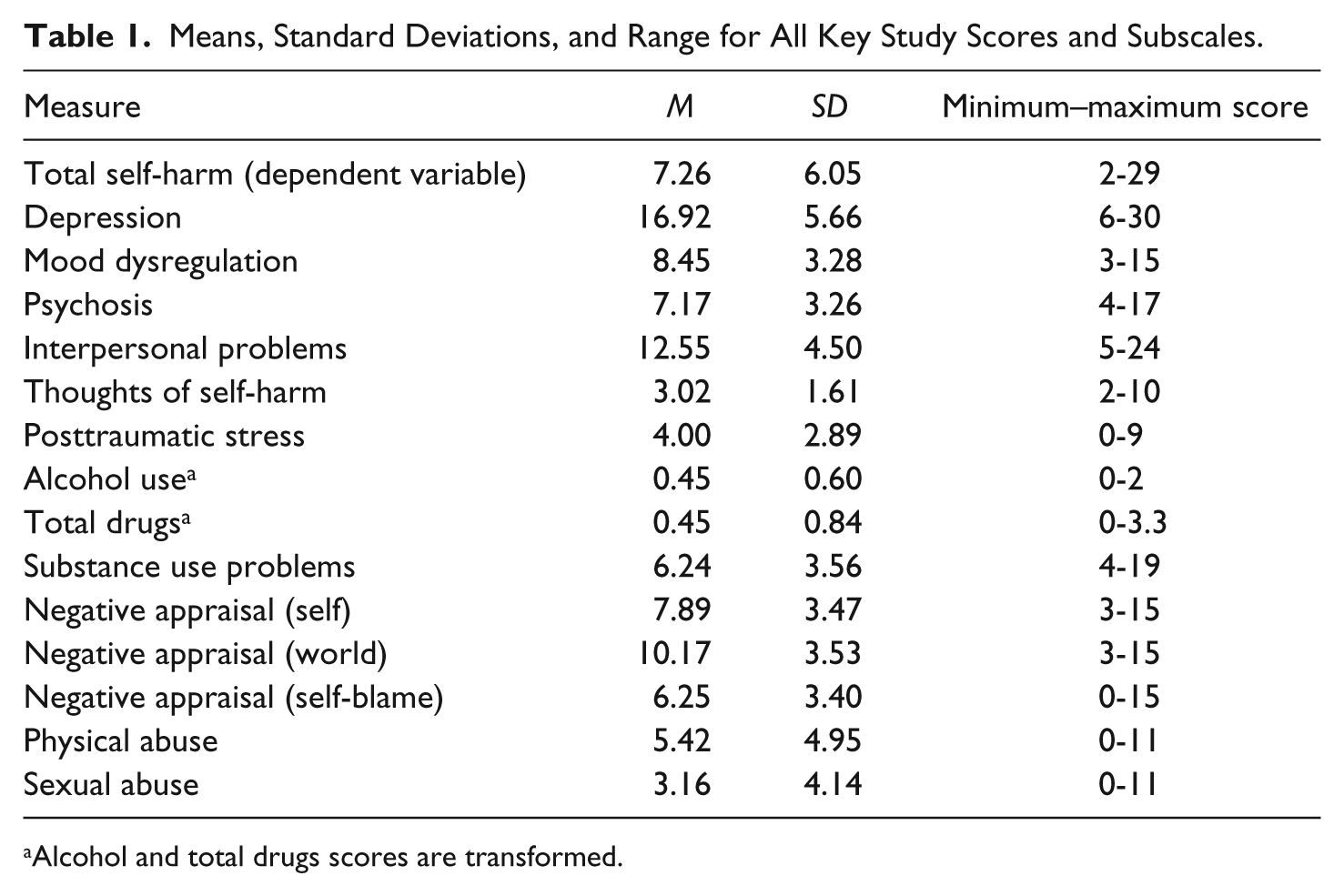
Alcohol and total drugs scores are transformed.
Correlation Matrix
Correlations (see Table 2) were all positive and generally in the low-to-moderate range with some exceptions. Physical abuse and sexual abuse were positively and moderately correlated, and both correlated in the low-to-moderate range with negative appraisals and mood-related psychiatric symptoms (depression, mood dysregulation, and posttraumatic stress symptoms). Physical and sexual abuse were not significantly correlated with alcohol use, showed low and significant positive correlations with total drug use and substance use problems, and both correlated significantly in the low-to-moderate range with self-harming behaviors. Total self-harming behaviors, the dependent variable in this study, correlated with all independent variables positively and in the low-to-moderate range.
Pearson Correlation Matrix for Key Study Variables (n = 227).
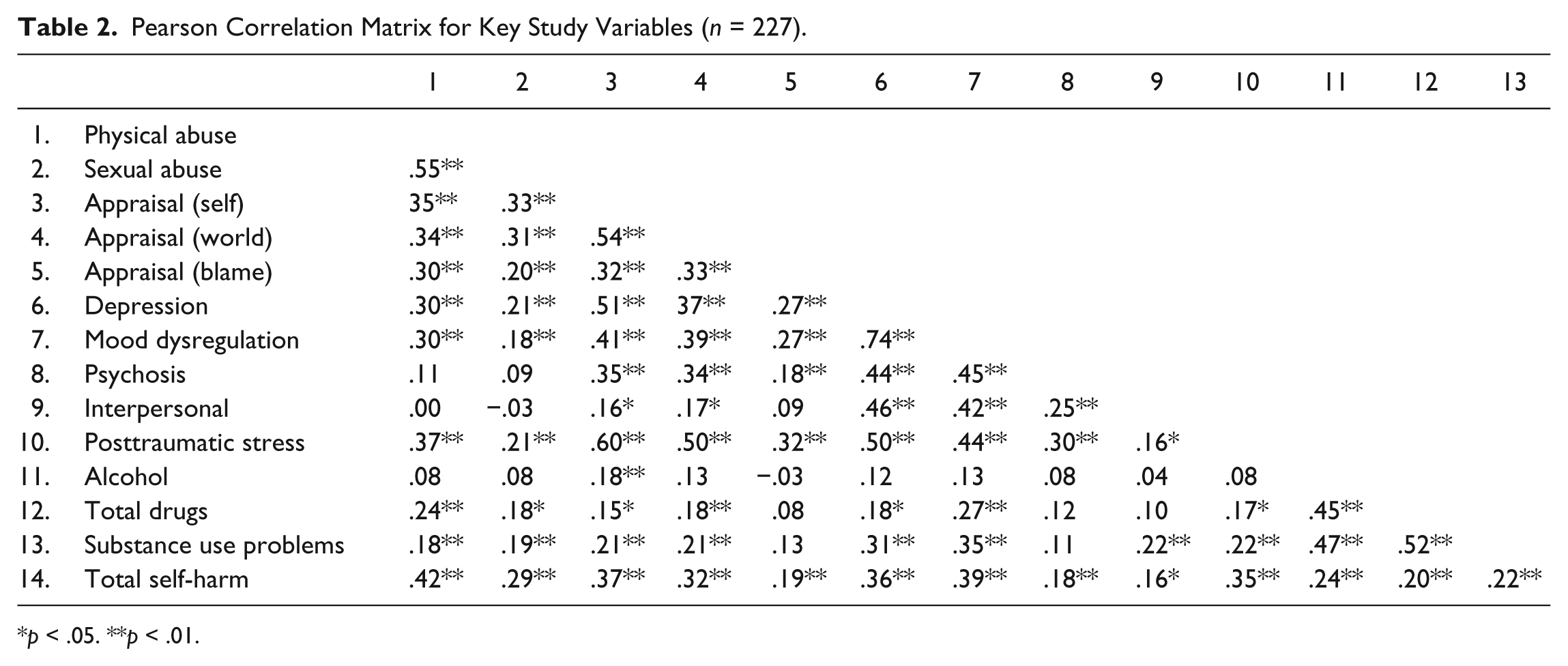
p < .05. **p < .01.
Regression: Testing the Association Between Abuse and Self-Harm When Controlling for Symptoms, Substance Use and Abuse, and Negative Appraisals of Trauma
Before calculating the regression equation, we dropped the variable “mood dysregulation” from the analysis because of the high correlation with depression (r = .74) to reduce risk of multicollinearity. The model was analyzed in the following steps: First, key psychiatric symptoms were entered into the equation (depression, interpersonal problems, psychosis, posttraumatic stress symptoms), followed, second, by three substance use/abuse measures (alcohol, total drugs, substance abuse problems). In the third step, the three negative appraisal subscales were entered (i.e., negative appraisal of the self, the world, and self-blame), followed, finally, by lifetime physical abuse and sexual abuse. The final model was significant, F(12, 175) = 5.81, p < .01; Adjusted R2 = .24, and only alcohol consumption and lifetime physical abuse were significantly associated with total self-harm. Lifetime physical abuse and alcohol consumption each accounted for about 4% of the variance in self-harm. No other factors, including sexual abuse, were significant in the model. Error terms were normally distributed (Durbin–Watson statistic = 1.96), and there was no evidence of multicollinearity in these data. Regression results can be examined in Table 3.
Hierarchical Linear Regression Models Testing the Association Between Total Self-Harming Behaviors and Physical and Sexual Abuse in Women With SMI (n = 227) While Controlling for Key Psychiatric Symptoms, Substance Use and Abuse, and Negative Appraisals (of Self, World, and Self-Blame).
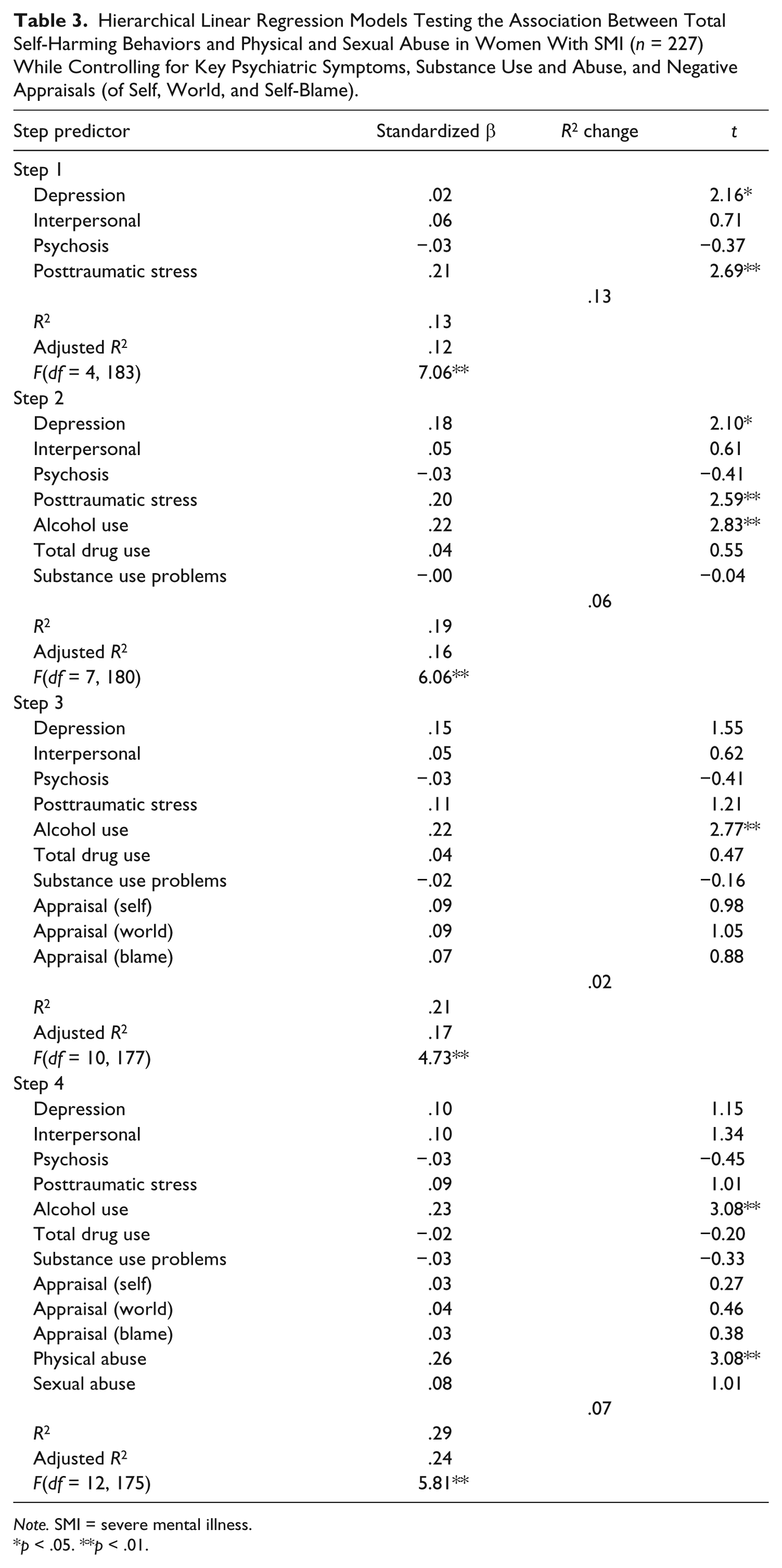
Note. SMI = severe mental illness.
p < .05. **p < .01.
Discussion
Our hypothesis was partially confirmed by this study: Physical abuse (but not sexual abuse) was significantly correlated with self-harming thoughts and behaviors when a range of psychiatric symptoms, negative appraisals, substance use, and related problems were controlled. In addition, alcohol use, a variable we used as a control, was also associated with self-harming behaviors. Both lifetime physical abuse and recent alcohol consumption appear to be associated with self-harm to a comparable degree.
The finding that psychiatric symptoms and negative appraisals dropped out of the regression equation is of considerable significance in these findings. Psychiatric symptoms, especially depression, but also symptoms of psychosis and posttraumatic symptoms, are well recognized as significant correlates or potential causal factors for suicide attempts and completed suicides. In addition, one might expect that negative cognitive appraisal would also be associated with self-harming behaviors given its association with trauma and depression. The correlation matrix bears out those expectations: Negative appraisals, particularly of the self and the world, are significantly correlated with physical and sexual abuse, depression and psychosis, and even more strongly with posttraumatic stress symptoms. However, physical abuse and alcohol use appear to account for the most variance in self-harming behaviors suggesting that lifetime abuse perhaps coupled with alcohol consumption as a possible form of negative coping have a significant role in the complex interplay of psychiatric, cognitive, and behavioral risk factors associated with self-harm. Studies of general population samples have shown correlations between child abuse and suicide risk (e.g., Joiner et al., 2007; Maniglio, 2011); however, such studies with SMI samples in which other key factors are controlled are few.
The finding that sexual abuse was not significantly associated with self-harm when other factors were controlled in this sample was an unexpected finding despite the significant correlation with self-harm (r = .29, p < .01). However, physical and sexual abuse have been shown elsewhere to correlate moderately in people with SMI (e.g., O’Hare et al., 2010; Rosenberg et al., 2007; as they do in the current data; r = .55, p < .01). Perhaps the failure to consider the age at which the abuse occurred, temporal proximity of the abuse to the study interviews, as well as the nature and severity of the abuse might have obscured some of the possible association between sexual abuse and self-harming behaviors. More detailed examination and measurement of various aspects of abuse could help lead to further understanding regarding the relationship between abuse and self-harm in people with SMI.
Women also appear to be at higher risk of self-harm due to alcohol abuse, possibly reflecting the elevated association between mood disturbances and alcohol use in women (Greenfield et al., 2010). In a previous study with a related sample of SMI clients who consumed at least one drink in the prior 6 months before the study, O’Hare and Shen (2012) showed that despite no gender differences in substance use associated with negative coping motives, women reported greater symptoms of depression. Depression also dropped out of the equation in the current study underscoring perhaps the particular importance of alcohol use as a factor in assessing risk of self-harm in women who are already compromised with severe psychiatric symptoms.
The links among psychiatric symptoms, cognitive factors, trauma, and self-harming behaviors are complex, and causal pathways among these factors remain unclear. In addition to the possibility that common neurological processes link various mental illnesses and substance abuse (Brady & Sinha, 2005), SMI also appears to be detrimentally influenced by stressful and traumatic life events as a result of repeated trauma such as physical and sexual abuse. Mueser, Rosenberg, Goodman, and Trumbetta (2002) have theorized that PTSD might mediate the relationships among trauma and symptoms of SMI directly and indirectly via effects on other correlated problems including substance abuse and additional trauma. In the absence of longitudinal data, the mediating role of PTSD is hard to confirm, especially given the significant correlations found between symptoms of PTSD and other psychiatric disorders (e.g., Kilcommons & Morrison, 2005; Marshall, Schell, & Miles, 2010) as is the case in the data from the current study.
It has been well documented (e.g., Mueser et al., 1998; Newman, Turnbull, Berman, Rodrigues, & Serper, 2010) that trauma and PTSD are not consistently assessed and diagnosed in many mental health treatment settings. In addition to regular trauma screenings, practitioners should pay particular attention to screening for violence and abuse directed at their female clients with SMI given its prevalence and association with a range of psychiatric symptoms and related problems. Practitioners should also review PTSD criteria closely given that posttraumatic stress symptoms appear similar to, overlap with, or exacerbate symptoms of SMI. In addition, substance abuse screening should be included in regular assessments and ongoing reevaluations of treatment progress in women with SMI given its association with depression and increased risk of self-harm and suicide.
The current study has several limitations. Although we used a composite measure of self-harm, we used one-item indexes to measure suicide attempts and self-harming behaviors. A more thorough assessment of self-harming behaviors and suicide attempts is warranted to further this important area of research. In addition, although it is well documented in the introduction that self-harm has relatively strong predictive value for suicide attempts, the relationship between self-harm and suicide remains somewhat ambiguous with respect to gauging whether self-harm is intentionally suicidal or not (Gratz, 2003). We also recognize the limitations of cross-sectional data and can make no definitive statements regarding causal pathways among these factors. Finally, we relied on the chart diagnoses of staff psychiatrists rather than having them recorded via structured diagnostic interview.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.