
Abstract
We examined body-esteem and self-esteem based on rape experience, rape labeling status (yes; no) and recency of rape (recently, within past year; earlier, between age 14 and the past year). Undergraduate women (n = 1,005) completed the Body-Esteem Scale, Rosenberg Self-Esteem Scale, and Sexual Experiences Survey. Women raped within the past year (recently) reported lower levels of both body-esteem and self-esteem than those raped over a year ago (earlier) and nonvictims, but women raped earlier did not differ from nonvictims. Rape labeling status was not significant. Findings identify lower body-esteem, in addition to lower self-esteem, as correlates of recent rape.
Rape experience is common among college women. For example, in a large study sampling from 27 campuses in the United States, 10.8% of undergraduate women reported being raped since starting their college career (Cantor et al., 2015), and we found rates ranging up to 30% in other female college student samples (Botta & Pingree, 1997; Cleere & Lynn, 2013; Littleton, Axsom, Breitkopf, & Berenson, 2006; Osman, 2016). Rape has been linked to negative self-evaluations, including lowered self-esteem (Ackard & Neumark-Sztainer, 2002; Cecil & Matson, 2005; Kucharska, 2017; Murphy et al., 1988; Neville, Heppner, Oh, Spanierman, & Clark, 2004; Perilloux, Duntley, & Buss, 2012; Sachs-Ericsson et al., 2014; Zweig, Crockett, Sayer, & Vicary, 1999) and heightened body-related concerns (e.g., body shame, body surveillance, disordered eating; Ackard & Neumark-Sztainer, 2002; Davidson & Gervais, 2015; Kremer, Orbach, & Rosenbloom, 2013; Merwin & Osman, 2017; Perilloux et al., 2012; Zweig et al., 1999). However, although self-esteem and some body-related constructs have been examined, the relationship between rape and body-esteem is in need of further investigation (Kulkoski & Kilian, 1997). Thus, one purpose of the current study was to contribute to the literature by further examining the associations between rape and self-esteem and body-esteem, as both may have important implications for emotional and sexual health (Kilimnik & Meston, 2016; Seal, Bradford, & Meston, 2009; Silberstein, Striegel-Moore, Timko, & Rodin, 1988; Stokes & Frederick-Recascino, 2003; Zweig et al., 1999).
Rape was operationally defined in the current study as vaginal, oral, or anal penetration without consent due to using force, threatening physical harm, or incapacitation. This definition is based on the widely used Sexual Experiences Survey (SES) measuring victimization experiences and is consistent with legal definitions and operational definitions of rape in the scientific literature (Koss et al., 2007; Muehlenhard, Peterson, Humphreys, & Jozkowski, 2017). Self-esteem represents an individual’s global self-evaluation of worth (Rosenberg, 1965), whereas body-esteem is described as a dimension of overall self-esteem: an individual’s attitude toward aspects of one’s own body that are associated with physical appearance or capability (Franzoi & Shields, 1984).
Researchers have asserted that women with rape experience may associate themselves and their bodies with negative feelings produced by rape, putting them at risk for less favorable self-evaluations (Janoff-Bulman & Frieze, 1983; Merwin & Osman, 2017; Schechter, Schwartz, & Greenfeld, 1987). The negative association between self-esteem and rape, as well as other forms of sexual assault, has been well established in the literature in student (Kulkoski & Kilian, 1997; Neville et al., 2004; Perilloux et al., 2012), community (Kucharska, 2017; Zweig et al., 1999), clinical (Cecil & Matson, 2005; Murphy et al., 1988), and national female samples (Sachs-Ericsson et al., 2014). On the contrary, although lower body-esteem has been linked to sexual victimization in childhood (Eubanks, Kenkel, & Gardner, 2006; Kilimnik & Meston, 2016; Wenninger & Heiman, 1998), the only published article we found investigating body-esteem and adult sexual assault was not conclusive regarding a relationship between the two (Kulkoski & Kilian, 1997).
Kulkoski and Kilian (1997) included only victims who had been assaulted at least 1 year or more ago, found no significant body-esteem differences between women with sexual assault experience and women with no sexual assault experience, and suggested that the women with sexual assault experience may have worked through potential body-esteem disturbances by the time of the data collection. This possibility is consistent with past studies utilizing various designs (i.e., between-groups, retrospective, longitudinal), suggesting that recency of rape can affect rape outcomes including body shame (Merwin & Osman, 2017), trauma (Testa, VanZile-Tamsen, Livingston, & Koss, 2004), sexual satisfaction (Orlando & Koss, 1983), depression and self-esteem (Kucharska, 2017; Murphy et al., 1988). For instance, Murphy et al. (1988) recruited individuals with rape experience from a treatment facility and a community comparison group of nonvictims. Self-esteem was measured at seven points over time following rape (6-21 days, 1 month, 3 months, 6 months, 1 year, 18 months, 2 years). The women with rape experience had lower self-esteem than the nonvictims, but this difference diminished by 1 year, diminished further by 18 months, and disappeared by 2 years. Also, Kucharska (2017) found that women who experienced rape or attempted rape within the past 2 years reported lower self-esteem than those who experienced this earlier. Thus, recency of rape has been found to affect self-esteem, but its impact on body-esteem remains unknown. Although we found no other studies examining both esteem and recency of rape, Sachs-Ericsson et al. (2014) found an association between rape and lower self-esteem in a sample of older women, and the victims had experienced rape an average of 36 years prior to the study. This suggests that a victim’s lowered esteem could exist many years following rape and, thus, other factors may interact with recency of rape to affect esteem (Burt & Katz, 1987).
One factor that may interact with recency to affect rape-related outcomes is whether or not a woman labels her rape experience as “rape” (Merwin & Osman, 2017). Women reporting experience consistent with behavior-based operational definitions of legal rape but not labeling this experience as “rape” have been referred to in the literature as unacknowledged rape victims (i.e., nonlabelers). Acknowledged rape victims are those who have labeled their rape experience as “rape” (i.e., labelers) (Koss, 1985; Layman, Gidycz, & Lynn, 1996; Peterson & Muehlenhard, 2011). Unacknowledged rape is prevalent among college women, as it is estimated that more than 50% with rape experience do not label their experience as “rape” (Wilson & Miller, 2016). If acknowledgment occurs, a woman may label “rape” immediately or shortly following rape but labeling often takes place at a later point in time (Botta & Pingree, 1997; Cleere & Lynn, 2013; Peterson & Muehlenhard, 2011). Therefore, the potential impact of recency of rape and labeling may occur simultaneously. Furthermore, some researchers have suggested that labeling may prompt a victim to deal with the rape and move toward better outcomes, or perhaps recovery (Kelley & Gidycz, 2015; Littleton et al., 2006).
With regard to rape outcomes, we did not find any studies specifically examining self-esteem or body-esteem based on rape labeling, but the impact of labeling on other rape outcomes has been studied, and the results are mixed. Labeling has been associated with positive outcomes (e.g., better coping, more social support; Botta & Pingree, 1997; Littleton et al., 2006), negative outcomes (e.g., more posttraumatic stress disorder [PTSD] symptoms, greater feelings of stigma; Layman et al., 1996; Littleton, Breitkopf, & Berenson, 2008), neutral results (e.g., psychological well-being; sexual satisfaction; McMullin & White, 2006; Orlando & Koss, 1983), and inconsistent findings (e.g., self-blame, alcohol consumption; Bondurant, 2001; Botta & Pingree, 1997; Layman et al., 1996; McMullin & White, 2006). However, McMullin and White (2006) found evidence that rape labeling may be associated with a decrease in alcohol consumption over time. Also, Merwin and Osman (2017) found that women raped within the past year reported greater levels of body shame than those raped longer ago, but only for acknowledged victims. (Note that body-esteem and body shame have been correlated, but they are distinct constructs; McKinley & Hyde, 1996; Varnes et al., 2015). Therefore, it is important to examine both recency and labeling, and how they may interact to affect various rape-related outcomes, as some researchers have suggested that labeling can be part of a recovery process that occurs over time (Kelley & Gidycz, 2015; Littleton, et al., 2006).
Labelers who were raped within a recent time period may more likely be in the midst of coping with their rape experience, which could heighten negative outcomes relative to other women with rape experience. Labelers who were raped longer ago may have more likely progressed further through the recovery process and, thus, have better outcomes than other women with rape experience. Nonlabelers may be unable to fully move through the recovery process, so that their negative outcomes would not differ based on recency of rape (Kelley & Gidycz, 2015; Merwin & Osman, 2017). The primary purpose of the present study was to test this rationale by examining self-reports of both body-esteem and self-esteem based on rape labeling (yes; no) and recency of rape (within past year; between age 14 and the past year). We also included nonvictims to build on past research examining the impact of rape on esteem, particularly body-esteem, given the lack of studies in this area.
Among the women who have experienced rape, we predicted an interaction between labeling and recency of rape, such that labelers who were raped within the past year would report the lowest esteem of all groups of women with rape experience, and labelers who were raped prior to the past year would report the highest esteem of all groups of women with rape experience. For nonlabelers, esteem was not expected to differ based on recency of rape. We also predicted that nonvictims would report higher esteem than each group of women with rape experience.
Method
Participants
Participants were drawn from an original sample of 1,005 undergraduate women who volunteered as an option for extra credit in either an introductory or upper-level psychology course at a public university on the east coast of the United States. Only those women who met our criteria were included in the data analyses; those who reported an experience that met our operational definition of rape, those who reported no experience with any type of sexual victimization, and those who were not missing pertinent data. This resulted in a final sample of 673 women. They ranged in age from 18 to 24 years (M age = 19.1, SD = 1.3). Seventy-four percent identified as European American, 15% African American, 3% Hispanic, 4% Asian, and 4% Biracial or Multiracial. Fifty-five percent of participants identified as first-year students, 20% sophomores, 9% juniors, and 16% seniors (see Table 1 for demographic information based on group).
Means and Percentages for Sample Demographics by Group.
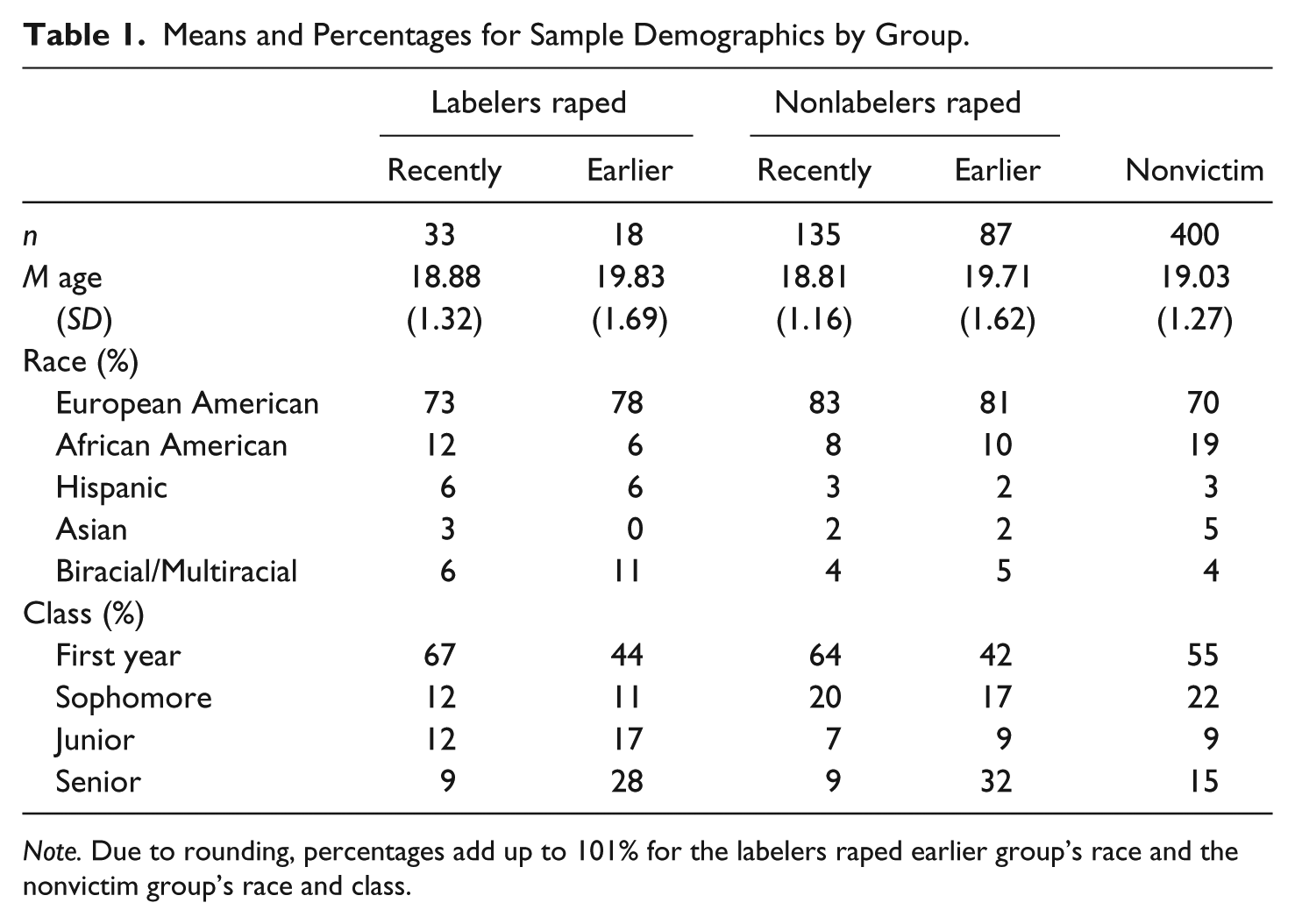
Note. Due to rounding, percentages add up to 101% for the labelers raped earlier group’s race and the nonvictim group’s race and class.
Measures
The Body-Esteem Scale (BES; Franzoi & Shields, 1984) measures attitudes toward one’s own body. Participants rated their feelings toward 35 body parts or functions on a 5-point scale ranging from 1 (have strong negative feelings) to 5 (have strong positive feelings). For women, 32 items on the BES (e.g., “lips,” “thighs,” “physical coordination”) can be scored to create three subscales (i.e., Sexual Attractiveness, Weight Concern, Physical Condition), or all items can be summed for a total BES score. Given the high Cronbach’s alpha (.91) in the present sample, we used the overall score, which is consistent with previous research (Goldenberg, McCoy, Pyszczynski, Greenberg, & Solomon, 2000; McKinley & Hyde, 1996; Seal et al., 2009; Silberstein et al., 1988; Wilski, Tasiemski, & Dabrowski, 2016). BES scores have been associated as expected with variables including body shame, self-surveillance (McKinley & Hyde, 1996), disordered eating (Silberstein et al., 1988), depression, sexual inhibitions (Kilimnik & Meston, 2016), sexual desire (Seal et al., 2009), and liking body-related aspects of sexual activity (Goldenberg et al., 2000).
Participants also completed the widely used Rosenberg Self-Esteem Scale (RSE; Rosenberg, 1965), which measures global self-esteem. Participants evaluated themselves by rating the 10 RSE items on a scale from 1 (strongly disagree) to 5 (strongly agree). Sample items include, “On the whole, I am satisfied with myself,” “At times I think I am no good at all,” and “I wish I could have more respect for myself.” The RSE has been associated in the expected directions with variables including depression, sexual esteem, body image, emotional well-being, relationship quality, and self-efficacy (McKay, Boduszek, & Harvey, 2014; Zweig et al., 1999). The Cronbach’s alpha in the current sample was .88.
The Sexual Experiences Survey-Short Form Victimization (SES-SFV; Koss et al., 2007) was completed to identify women with rape experience and nonvictims. This survey includes nine questions measuring rape (without using the term “rape”), and 26 additional questions measuring other forms of sexual victimization. Rape includes vaginal, oral, or anal penetration without consent due to using force, threatening physical harm, or intoxication. A sample item is, “A man put his penis into my vagina, or someone inserted fingers or objects without my consent by threatening to physically harm me or someone close to me.” To determine recency of rape (within the past year; between age 14 and the past year), the SES-SFV also includes standard questions that assess whether rape occurred “in the past 12 months” and “since age 14.” If multiple rapes were reported, categorization was based on the most recent rape. Rape labeling was then measured by asking “yes” or “no,” “Have you ever been raped?” If a participant indicated experience with one of the nine items measuring rape and then responded “yes” to the labeling question, she was classified as a labeler. However, if a participant indicated experience with one of the nine items measuring rape and then responded “no” to the labeling question, she was classified as a nonlabeler. SES-SFV responses have been linked as expected to variables including intimate partner violence, body surveillance, body shame, and distress (Cleere & Lynn, 2013; Davidson & Gervais, 2015).
Procedure
Participants provided informed consent and were then administered surveys to complete in a large classroom setting. Participants were instructed to sit at least every other seat apart to ensure privacy and were informed that all responses were anonymous. Surveys included demographic questions, the BES, RSE, and SES-SFV. After completing the survey, participants placed it into an anonymous drop bag and were then handed contact information for counseling service options as they left the room. This study was approved by an Institutional Review Board.
Data Analyses
Participants from the final sample were categorized into five groups to test the hypotheses (nonvictims, labelers raped recently, labelers raped earlier, nonlabelers raped recently, and nonlabelers raped earlier). Women who reported no experiences on the SES-SFV were categorized as nonvictims (n = 400; 59%). Women who reported rape within the past year were categorized as “raped recently” (n = 168; 25%), and they either labeled their experience as “rape” (“labelers,” n = 33; 20%) or did not (“nonlabelers,” n = 135; 80%). Women who reported rape prior to the past year (since age 14) were categorized as “raped earlier” (n = 105; 16%), and they were either “labelers” (n = 18; 17%) or “nonlabelers” (n = 87; 83%). Participants from the original sample were dropped from analyses because they did not meet our criteria; they either had experience with sexual victimization (but not rape) (n = 249; 25%) or had missing data on the SES-SFV (n = 83; 8%). Additional participants’ missing data on the BES (n = 3 women with rape experience; n = 5 nonvictims) or the RSE (n = 3 women with rape experience; n = 1 nonvictim) were dropped from those respective analyses.
Given the unequal sample sizes, Levene’s test was conducted for all analyses and demonstrated that the assumption of homogeneity of variance was not violated (ps > .10-.707). Regarding group differences on our demographic variables, women raped earlier were older and further along in school than women raped recently and nonvictims (ps < .0001). Thus, we entered age and college class as covariates in all analyses to control for their effects, and they were not significant (ps > .05-.851; see Table 1 for demographic means and percentages based on group). To test the interaction hypothesis among the four groups of women with rape experience, 2 × 2 (Labeling Status × Recency of Rape) analyses of covariance (ANCOVAs) were performed on the body-esteem and self-esteem scores. To test the hypothesis involving nonvictims, one-way ANCOVAs were performed for all five groups on the body-esteem and self-esteem scores, followed by pairwise comparisons.
Results
Results of the ANCOVAs testing the hypothesis among women with rape experience revealed no significant interaction or labeling status main effect for either body-esteem or self-esteem. However, there was a significant main effect for recency of rape on body-esteem, F(1, 268) = 5.34, p = .022,
Results of the ANCOVAs testing the hypothesis involving nonvictims revealed significant effects for body-esteem, F(4, 660) = 4.23, p = .002,
Means, Standard Deviations, Cell Sizes, and Confidence Intervals for Esteem Scores.
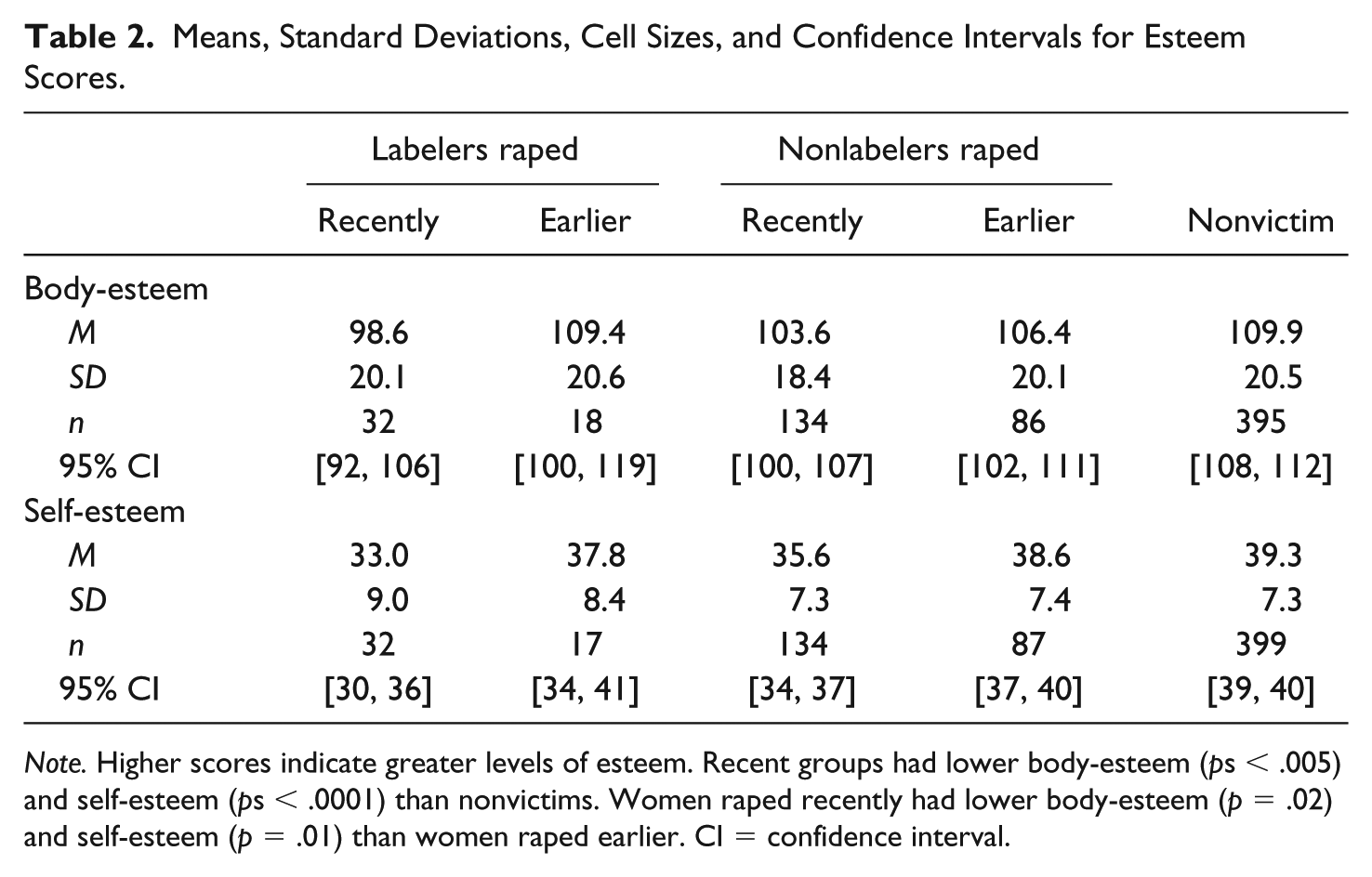
Note. Higher scores indicate greater levels of esteem. Recent groups had lower body-esteem (ps < .005) and self-esteem (ps < .0001) than nonvictims. Women raped recently had lower body-esteem (p = .02) and self-esteem (p = .01) than women raped earlier. CI = confidence interval.
Discussion
The current study is among the first to investigate a relationship between body-esteem and rape, and to examine the influence of rape labeling status and recency of rape on both body-esteem and self-esteem. Regardless of labeling status, women raped within the past year reported lower levels of both body-esteem and self-esteem than those raped less recently, and than nonvictims. Although the current study was not longitudinal, results are consistent with prior research (Kucharska, 2017; Murphy et al., 1988) and suggest that a longer time period since rape may be associated with better body-esteem and self-esteem, and possibly with recovery of esteem, given that women raped earlier and nonvictims did not differ. However, it should be noted that the current results are not consistent with Sachs-Ericsson et al.’s (2014) finding of an association between rape and lower self-esteem measured an average of 36 years after rape occurred, but Sachs-Ericsson et al. used a 1-item measure of self-esteem in a sample of older women (M age = 69). These and other factors may also contribute to esteem levels.
In fact, the current data are correlational. Therefore, caution should be taken in assuming that recency acts alone to influence esteem. Although the current study does not support rape labeling status as a predictor of esteem, other unknown factors (e.g., coping strategies, therapy, relationships, rape frequency) may have played a role during the time frames studied and could be avenues for future research investigating the relationship between rape, recency, and esteem.
It is also important to continue considering the impact of rape labeling status and how it may interact with various factors (including recency of rape) to affect esteem and other rape-related outcomes (e.g., distress, PTSD, shame). Labeling status did not predict body-esteem or self-esteem in the current study, but it has been found to interact with recency of rape to predict body shame (Merwin & Osman, 2017). Although body shame is a different construct (McKinley & Hyde, 1996; Varnes et al., 2015), these findings mirror the mixed results found in the rape acknowledgment literature and suggest further research is needed to disentangle and understand factors interacting and associated with rape acknowledgment, which appears to be a complicated process (Johnstone, 2016; Wilson, Miller, Leheney, Ballman, & Scarpa, 2017). For example, outcomes may be influenced by a woman’s motivations for labeling “rape” (Peterson & Muehlenhard, 2011). Furthermore, researchers may consider the impact of acknowledging forms of sexual victimization other than rape (e.g., attempted rape, sexual coercion) by using labels other than “rape” (e.g., “sexual assault,” “sexual abuse”) (Harned, 2005; Kelley & Gidycz, 2015). This future research should include esteem, given that this may be only the first study to examine it based on labeling.
Other limitations include that the current effect sizes were not large, as was expected due to the many factors that can influence esteem. However, findings may indicate subtle impacts on esteem in individual cases. Also, generalizability is limited given that the participants were college women and largely European American. In addition, the time frames used in the current study to examine recency of rape were limited by those standardized on the SES-SFV. For instance, it is possible that an individual raped 13 months ago may be more similar to an individual raped within the past year than to an individual raped 3 years ago, yet 13 months and 3 years ago would both be considered earlier in the current study. It should also be noted that how recently labeling occurred was not measured. Thus, future research including men, noncollege samples, and more racial diversity, as well as examining other time frames for recency of rape, recency of labeling, longitudinal designs, and other rape-related factors may be fruitful.
Conclusion
The current study contributes to the literature as perhaps the first to identify lower body-esteem as a correlate of rape and replicates prior findings of a negative association between global self-esteem and rape, but only for women raped within the past year. This is consistent with the assertion that women with rape experience are at risk for unfavorable self-evaluations possibly due to associating themselves and their bodies with negative feelings produced by the rape (Janoff-Bulman & Frieze, 1983; Merwin & Osman, 2017; Schechter et al., 1987). Although other factors may help explain these findings for esteem based on recency of rape, the current findings suggest that rape labeling status does not influence self-esteem or body-esteem. However, given that this study also contributes as perhaps the first to examine esteem based on rape labeling, for which the literature is mixed, caution is warranted in drawing conclusions about the relationship between labeling and esteem prior to further investigation, which should include questions designed to further understand the seemingly complicated process of acknowledgment over time. In the meantime, individuals who may be interacting directly with women they suspect or know have rape experience should be cautious about their use of labels, as the positive and negative outcomes of labeling “rape” are not yet clearly understood (Johnstone, 2016; Peterson & Muehlenhard, 2011; Wilson et al., 2017).
The high prevalence rates of nonlabelers in this (n = 222; 81%) and other samples of college women (Bondurant, 2001; Layman et al., 1996; Littleton et al., 2006; Peterson & Muehlenhard, 2011; Wilson & Miller, 2016) suggest that the reality of unacknowledged rape must be considered in efforts to accurately assess rape prevalence on individual campuses and that rape education targeting college women may be enhanced by highlighting definitions of rape, as well as identifying body-esteem, along with self-esteem, as correlates of recent rape. Findings may also be important for therapists working with women who have been raped or clients who have disturbances in body-esteem or self-esteem, which have been linked to numerous other emotional and sexual health–related factors (e.g., depression, happiness, sexual desire and response, disordered eating; Kilimnik & Meston, 2016; Seal et al., 2009; Silberstein et al., 1988; Stokes, Frederick-Recascino, 2003; Zweig et al., 1999). For example, awareness that a woman with rape experience may suffer lowered body-esteem might help therapists to better design well-rounded treatment plans. Furthermore, findings may provide hopefulness to women with recent rape experience who may be suffering negative outcomes that resilience is possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.