
Abstract
Sexual assault is a widespread problem on college campuses, and survivors rarely use campus supports. However, there is no established measure of service barriers for this population. This study develops and provides preliminary evidence for a measure of psychological service barriers. Data were collected from 100 college sexual assault survivors. Results provide evidence for three factors: social-emotional barriers, negative treatment barriers, and minimization barriers. Additional tests offer evidence for consistency and reliability in these factors over time and across campus supports. This work offers preliminary evidence for the psychometric properties of this measure and lays the groundwork for future validation research.
Sexual assault is a widespread and persistent problem within institutions of higher education (Coulter et al., 2017; Eisenberg et al., 2021; Fedina et al., 2016). In the context of this study, sexual assault includes a full range of nonconsensual sexual acts, including completed and attempted penetration of the vagina and/or anus, oral sex, sexual coercion, and sexual contact. Experiencing sexual assault can lead to numerous mental health problems (e.g., depression, posttraumatic stress, suicidality; Campbell et al., 2009; Dworkin et al., 2017; Jordan et al., 2010). Formal resources, under ideal circumstances, can assist survivors’ recovery after an assault (Grych et al., 2015; Ullman, 2010). For instance, trauma-informed care includes (a) realizing the prevalence and impact of trauma on people’s lives, (b) recognizing the signs of trauma, (c) integrating this knowledge of trauma into every part of institutional or organizational practice, and (d) resisting re-traumatization (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). These practices can be integrated into all formal supports, including the criminal justice system (International Association of Chiefs of Police, 2015), medical care (Raja et al., 2015), and mental health services (SAMHSA, 2014). Survivors who do not seek help report more psychological distress and symptoms of depression and posttraumatic stress (Ahrens et al., 2010); however, use of mental health services is associated with greater posttraumatic growth—a positive mental health outcome—for sexual assault survivors (Hassija & TurchiK, 2016).
In recent years, institutions have experienced increased pressure to address the problem of campus sexual assault and to support survivors. For example, under the Obama administration, the Department of Education’s Office for Civil Rights (OCR) enhanced its focus on sexual assault, releasing “significant guidance documents” that emphasized how colleges and universities must respond to sexual assault to be in compliance with Title IX (e.g., 2011 Dear Colleague Letter). Grassroots activism by students and sexual assault survivors helped increase the public’s awareness of Title IX and the OCR’s role in holding universities accountable for failing to prevent and respond appropriately to sexual assault (Pérez-Peña, 2013). As a result, colleges and universities have implemented and expanded formal supports for students who experience sexual assault, including policies and reporting mechanisms, victim advocacy services, and mental health counseling options (Richards, 2016). Higher education is an ideal context to deliver affordable, high-quality, coordinated care to survivors. However, student sexual assault survivors rarely use available formal supports (Halstead et al., 2017; Richardson et al., 2015; Sabina & Ho, 2014). Accessing formal supports may not be the first or even best choice for all survivors (Ullman, 2010), but these supports can provide options and resources to aid recovery. Given the serious negative consequences of experiencing sexual assault, there is great need for research to understand the barriers that prevent students from accessing services. In particular, a uniform assessment of service barriers that is grounded in theory and empirical evidence would improve the measurement of service barriers across institutions, formal supports, and samples of survivors. To address this gap, this study capitalizes on data collected as part of a larger pilot study to develop and provide preliminary evidence for a comprehensive measure of service barriers for college survivors.
Sexual Assault Survivors’ Use of Formal Supports
Prior research has examined college sexual assault survivors’ use of a variety of formal supports after an assault. One of the most frequently examined supports in the literature is reporting to law enforcement. Rates of reporting to law enforcement have ranged from 0.6–13%, with most studies finding that fewer than 10% report to the police (e.g., Fisher et al., 2003; Krebs et al., 2007; Lindquist et al., 2013; Walsh et al., 2010; Wolitzky-Taylor et al., 2011). Only a few studies have looked at rates of reporting to campus law enforcement specifically, and the rates are generally very low: approximately 5% of survivors report the assault to Campus Police (e.g., 5.3% in Fleming et al., 2018; 4% in Nasta et al., 2005). In addition to reporting to the police, college students have the option to report the assault through their institution’s disciplinary process. The U.S. Department of Education and the Supreme Court have long recognized sexual harassment (which includes sexual assault) of students as a prohibited form of sex discrimination under Title IX, a civil rights law established to eliminate sex discrimination in educational programs (U.S. Department of Education, Office for Civil Rights, 2015). Since 1997, the Department of Education’s OCR—the federal agency responsible for the enforcement of Title IX—has provided guidance to institutions of higher education about how to be in compliance with Title IX around sexual harassment and assault, including establishing formal procedures for reporting and adjudicating allegations (e.g., U.S. Department of Education, 1997, 2001, 2011). However, researchers have found that very few survivors report via these formal university procedures (e.g., to a “Title IX Office”), with rates ranging from 0–4.3% (e.g., Fleming et al., 2021; Khan et al., 2018; Lindquist et al., 2013).
Most college students in the United States have access to formal resources beyond reporting options (i.e., police, Title IX Office). Counseling centers exist in every type of institution of higher education, where students can access short-term and/or long-term mental health care at little to no cost (LeViness et al., 2017). Many institutions have also established campus sexual assault centers and/or victim advocacy services (Richards, 2016). These services focus explicitly on the needs and interests of sexual assault survivors (Martin, 2005). However, research finds that many sexual assault survivors are not using these services. That is, rates of students’ use of victim advocacy services range from 1–25%, with most studies finding usage rates less than 10% (e.g., Fisher et al., 2003; Fleming et al., 2021; Krebs et al., 2007; Lindquist et al., 2013; Walsh et al., 2010; Wolitzky-Taylor et al., 2011). Fewer studies have examined student survivors’ use of campus counseling services, but rates of use tend to be slightly higher than other services (e.g., 15.2% in Fleming et al., 2021; 8% in Nasta et al., 2005; 34% in Krebs et al., 2007; 4.4–13.2% in Lindquist et al., 2013). Overall, the literature suggests that when survivors seek assistance from formal campus resources after an assault, they are most likely to go to a counseling center or victim advocacy service and least likely to report to law enforcement or the university (Fisher et al., 2016). Although college survivors have access to more resources than survivors in the community (i.e., non-college populations), they are less likely to report and seek help from formal resources (Spohn et al., 2017).
Despite the low rates of formal resource use, research suggests that survivors do want information about resources and believe that resources can be beneficial. Many survivors find it helpful when informal support providers (e.g., friends, family) discuss tangible aid, but informal supports rarely provide this type of support (Ahrens et al., 2009; Filipas & Ullman, 2001). A recent study of survivors’ motivation for disclosing their sexual assault found that they wished to receive help to improve their psychological well-being, receive information, and facilitate other tangible outcomes (e.g., advocacy, academic or housing accommodations, justice; Demers et al., 2017). When done well (e.g., trauma-informed), services provided by formal resources can facilitate survivors’ psychological well-being (Grych et al., 2015; Hassija & TurchiK, 2016; Ullman, 2010). To enable survivors’ ability to use formal resources, it is essential to assess and address barriers to service use.
Review of Research on Service Barriers
There is ample existing literature that has identified and/or examined survivors’ reasons for not using formal supports, including a wide range of psychological barriers (e.g., shame, self-blame, confidentiality concerns, fear of being mistreated, belief that the incident was not serious enough to report; Ameral et al., 2020; Fisher et al., 2003; Krebs et al., 2007; Nasta et al., 2005; Walsh et al., 2010; Zinzow & Thompson, 2011). Yet, there is currently no consistent way of measuring, categorizing, or analyzing these barriers. Some studies have presented survivors a list of possible reasons for not reporting and/or using resources from the National Violence Against Women Survey (e.g., Thompson et al., 2007; Zinzow & Thompson, 2011), the National College Women Sexual Victimization Survey (e.g., Fisher et al., 2003; Walsh et al., 2010), or the National Crime Victimization Survey (e.g., Sloan et al., 1997). Multi-institution campus climate studies have developed their own lists of reasons why survivors did not use formal supports, including the College Sexual Assault Study (Krebs et al., 2007), the HBCU College Sexual Assault Study (Lindquist et al., 2013, 2016), and the Association of American Universities Climate Study (Fisher et al., 2016). Other studies at a single institution have developed their own lists as well (e.g., Amar, 2008; Ameral et al., 2020; Nasta et al., 2005; Richardson et al., 2015; Walsh & Bruce, 2014). Across these studies, survivors are presented with a list of about 14 reasons on average for why they did not use formal services.
Qualitative research on college sexual assault survivors’ experiences of service barriers have found similar types of barriers to those that have been included in quantitative research. For instance, several qualitative studies found strong psychological barriers preventing survivors from accessing formal services, including minimizing the event, experiencing self-blame, shame and embarrassment, fearing consequences for themselves and/or the perpetrator, and anticipating negative treatment or inadequate action by formal support providers (e.g., Khan et al., 2018; Miller et al., 2011; Ollen et al., 2017). A recent qualitative study theorizing the process of help-seeking decisions after an assault identified the importance of such psychological factors in survivors’ disclosure decisions (DeLoveh & Cattaneo, 2017).
All of these studies to date have provided essential information about survivors’ use of formal resources after an assault, but there are limitations to this entire body of work that, if addressed, would advance understanding of service barriers and how to mitigate them. First, research in this area has lacked theoretical grounding. A comprehensive review of research on service use among college sexual assault survivors (Sabina & Ho, 2014) noted the lack of systematic, theoretical conceptualization of service barriers. Other researchers in this area have also noted the need for more theoretically focused analyses of sexual assault survivors’ help-seeking decisions (e.g., Ameral et al., 2020). Second, much of the prior research on service barriers for college sexual assault survivors has either (a) assessed barriers for only one specific support, typically law enforcement (e.g., Fisher et al., 2003; Huemmer et al., 2018; Krebs et al., 2007; Miller et al., 2011; Sloan et al., 1997; Thompson et al., 2007; Walsh & Bruce, 2014; Zinzow & Thompson, 2011) or (b) collapsed across several formal resources, including confidential supports and reporting options (e.g., Ameral et al., 2020; Fisher et al., 2016; Guerette & Caron, 2007; Nasta et al., 2005; Richardson et al., 2015; Walsh et al., 2010).
These limitations make it difficult to consistently evaluate the prevalence and impact of different service barriers and how they may vary across institutions, formal supports, and groups of survivors. Although there is overlap in survivors’ reasons for not using reporting options (i.e., to law enforcement and/or the university) and confidential supports (e.g., Counseling Center, Victim Advocacy), there is also evidence to suggest that there is variability in the experience of different service barriers across supports (e.g., Amar, 2008; Holland & Cortina, 2017). For example, Holland and Cortina (2017) found that experiencing negative emotions and anticipating consequences were more frequently identified as service barriers for the Title IX Office compared with the campus Sexual Assault Center. Some service barriers may also be more (or less) relevant among survivors with marginalized identities. A recent study found some differences in the psychological service barriers experienced by heterosexual and lesbian, gay, bisexual, queer (LGBQ) college sexual assault survivors (Richardson et al., 2015). Other research studies have found evidence to suggest that some service barriers may be more strongly related to negative mental health outcomes than others (e.g., Carson et al., 2019; Miller et al., 2011). Therefore, the goal of this study was to develop and provide preliminary empirical evidence for a comprehensive measure of psychological service barriers that is grounded in theory and empirical evidence, which would allow for replication, comparison, and the examination of variability in service barriers across institutions, formal resources, and survivor groups.
This Study
This study capitalizes on service barrier data collected as part of a larger pilot study, which examines a wide range of reasons that college sexual assault survivors do not use campus reporting and resource options—including the Campus Police, Title IX Office, Victim Advocacy, and Counseling Center. The barriers examined in the study were developed from the large body of empirical evidence on this topic and a theoretical typology of service barriers. “Access” to formal resources has been theorized as the fit between a client/patient and a particular resource and comprised overarching dimensions such as availability (e.g., lack of services), affordability (e.g., cost of services), accessibility (e.g., ease of access), and acceptability (e.g., patient beliefs, expectation of services; Penchansky & Thomas, 1981). Logan and colleagues have used this theoretical framework to conceptualize service barriers among survivors of intimate partner violence in the community (Logan et al., 2005; Logan et al., 2004). Drawing from this theoretical model, Holland and Cortina (2017) also identified and classified barriers to using campus supports among college sexual assault survivors. Given availability of reporting mechanisms and free or affordable resources on college campuses, the majority of reasons that college survivors did not use campus supports fit with the theoretical category of acceptability barriers, for instance, experiencing negative emotions, anticipating consequences, and/or minimizing the assault. Some college survivors also identified accessibility barriers (e.g., lacking time). Other reasons, such as alternative coping strategies (e.g., seeking help from informal supports instead), fell outside the theoretical framework. College survivors’ experiences of service barriers are distinct from decisions to cope in ways that do not involve formal resources, such as telling a friend (DeLoveh & Cattaneo, 2017). Taken together, the theoretical categorization of service barriers includes psychological barriers (i.e., acceptability barriers) as well as reasons related to the context (e.g., accessibility barriers) and/or survivor actions (e.g., alternative coping strategies).
Although existing research studies have presented survivors different lists of “yes/no” items that ask about possible reasons for not reporting and/or using resources, something may be missed if the measurement and analysis of service barriers is not grounded in theory and empirical evidence (e.g., collapsing across barriers that are conceptually distinctive, using single items to assess particular service barriers). A measure of service barriers for college sexual assault survivors, which is currently absent from the literature, would allow a more consistent analysis of barriers and how they may differ across resources and campuses. For example, evidence suggests that college students’ use of campus resources is more strongly predicted by psychological factors than demographic factors or assault characteristics (Fleming et al., 2021). Given the centrality of psychological factors within the literature on this issue, this study focused on developing a measure of psychological service barriers (e.g., negative emotions, anticipating consequences, minimizing the assault, beliefs about the usefulness of a resource) rather than reasons related to the context and/or survivor actions (e.g., logistical issues, alternative coping strategies). Thus, this study provides preliminary evidence for a comprehensive measure of psychological service barriers to using formal campus supports among college sexual assault survivors.
Method
Procedures and Participants
The items examined in this study were embedded in a larger pilot consisting of two waves of survey data collected in spring 2018 and fall 2018 (approximately 6 months apart). The research team recruited undergraduate students from a large, Midwestern university using several recruitment approaches. Flyers were posted in buildings across campus (e.g., academic buildings, library, residence halls, health center). The team also posted flyers in off-campus locations that students frequently patronized (e.g., coffee shops). Information about the study was announced by members of the research team in undergraduate classes (e.g., courses in psychology, sociology, and women’s studies) and distributed electronically via listservs (e.g., student organizations) and social media pages (e.g., university class Facebook pages). Across all recruitment methods, messaging invited students who had an unwanted sexual experience while attending the university to participate in a research study about the types of support they do and do not look for. Interested students were instructed to email, call, or text the research team. In total, 160 students sent a message (email, text, and/or voicemail) to express interest in the study. A member of the research team responded with a request for a brief screening phone call to verify eligibility. Inclusion criteria were that a student (a) be of age 17 years or older, (b) be a current undergraduate at the university, (c) plan to enroll the following semester, and (d) have had an unwanted sexual experience while attending the university. Procedures were approved by the university Institutional Review Board.
Of the 160 students who expressed interest, 124 were screened for eligibility (33 did not respond to the screening request, and three withdrew from participation). There were 17 students who did not meet eligibility criteria. At the end of the screening call, research staff scheduled the 107 eligible participants to come into the research lab and complete the survey (programmed in Qualtrics) on a computer in a private room to ensure participant safety and security. Seven students did not show up for their scheduled time slot, leaving a total of 100 participants. The 100 participants were given a thorough explanation of study procedures by a trained research assistant and provided informed consent. Research assistants assigned each participant a unique ID number and set up the survey on a laptop in a private room next to the research lab. When they were finished, participants were provided US$20 compensation.
The team contacted students who participated in the first wave (spring 2018 semester) again during the fall 2018 semester to complete the second wave. Invitation emails informed students that the follow-up survey would take about 30–45 min, be taken in a private research room, and participants would be compensated US$30. In total, 90 of the 100 participants responded (no reply n = 10). Of those 90, one withdrew from the study, three informed the team they were no longer students at the university, four never scheduled, and 82 were scheduled for the follow-up. Of these, five students did not show for their appointment; thus, 77 completed both surveys.
Following recommendations for maintaining quality of web-survey data (Meade & Craig, 2012), the research team examined these data and removed participants with excessive missing data on study variables and/or failing attention checks (i.e., items that ask for a specific response). Data from seven participants were removed from Wave 1 (W1: n = 93), and data from four participants were removed from Wave 2 (W2: n = 73; all four were also among the seven whose data were removed from W1). This gave a 78% retention rate across the two surveys.
At W1, approximately one third (n = 30, 32.3%) of the sample identified as LGBQ (six lesbian or gay; 17 bisexual; four asexual; one unsure/questioning; two another sexual identity, for example, asexual or pansexual) and 64.5% (n = 60) identified as heterosexual (three did not provide their sexual identity). The sample was primarily cisgender women (n = 73, 78.5%), 8.0% (n = 7) were transgender or gender nonconforming, and 8.0% (n = 7) were cisgender men (six did not provide their gender identity). All of the transgender or gender nonconforming participants also identified as LGBQ. For racial/ethnic identity, participants primarily described themselves as White/Caucasian (n = 59, 63.4%). The remainder of individuals identified themselves as African American/Black (n = 7, 7.5%), Latinx/Hispanic (n = 6, 6.5%), Asian/Asian American/Pacific Islander (n = 5, 5.4%), biracial/multiracial (n = 15, 16.1%), and one (1.1%) participant identified as another race/ethnicity. Participants’ average age was 19.8 years (SD = 1.32 years, min = 18 years, max = 25 years). The sample was mainly in their first through third year at the university, with 32 freshmen (first years), 26 sophomores (second years), 26 juniors (third years), eight seniors (fourth years), and one fifth year. There were no differences in demographic characteristics between W1 and W2.
Measures
Service knowledge
In the surveys, participants were presented a list of campus resources and asked, “Have you ever heard of any of the following resources at the University?” (0 = no, 1 = yes). In this study, the resources examined were Campus Police, Counseling Center, Victim Advocacy, and the Title IX Office. The official names for these resources were included in the survey, but general terms are used here to protect anonymity for the campus.
Service use
Respondents who indicated knowledge of a resource were then asked whether they had sought help from that resource after the assault (e.g., “Did you seek help from the Campus Police department? In other words, did you report the incident to Campus Police?”), and they responded with 0 = no or 1 = yes.
Service barriers
If participants did not use a support, they were presented with a comprehensive list of reasons that sexual assault survivors do not use resources that was created for the study. The measure was written by the authors with the context of understanding sexual assault survivors’ use of campus resources in the pilot study in mind, but also with the goal of establishing a more comprehensive measure of psychological service barriers that could be used in future research. First, authors generated an extensive list of items from prior research that examined college students’ use of formal sources of support (e.g., police, university officials, health care centers, women’s centers, counseling centers). Authors culled a comprehensive list of items from national or multi-university studies, including the National College Women Sexual Victimization Survey (Fisher et al., 2003; Walsh et al., 2010), the College Sexual Assault Study (Krebs et al., 2007), the HBCU College Sexual Assault Study (Lindquist et al., 2013, 2016), and the Association of American University’s Campus Climate Survey (Fisher et al., 2016), in addition to individual studies that developed and used their own list (Amar, 2008; Ameral et al., 2020; Nasta et al., 2005; Zinzow & Thompson, 2011). Authors checked these items against the findings in several recent qualitative studies of college student help seeking after sexual assault, and added additional items based on the qualitative findings (DeLoveh & Cattaneo, 2017; Holland & Cortina, 2017; Miller et al., 2011; Ollen et al., 2017). Authors mapped the items onto a theoretical categorization of reasons for non-resource use (e.g., accessibility, acceptability) and then reduced the items by identifying the most frequent and salient reasons for non-resource use across all of the prior studies. Example items included, “I didn’t think the incident was serious enough” and “I thought they would blame me.” The full list of items is presented in the appendix.
The prompt for the items read, There are many reasons why students may not use the [support] after incidents like this. We would like to better understand the reasons why you did not use this resource after the incident. Are any of the following a reason you did not use the [support]?
Response options included 0 = no, 1 = yes, slightly, 2 = yes, moderately, 3 = yes, definitely. Given the aim of this study—to establish and provide evidence for a measure of psychological service barriers for college sexual assault survivors—not all items were included in the analysis. The categories of items that fell outside the parameters of “psychological service barriers” were as follows: (a) logistical barriers (e.g., “It would cost too much money”), (b) assault characteristics (e.g., “Because of where the incident happened”), and (c) alternative coping strategies (e.g., “I handled the incident myself”). Possibilities for including these reasons in future research are presented in the discussion section following the results.
Analytic Approach
To assess the psychometric properties of the Psychological Service Barriers for Sexual Assault Survivors in Higher Education (PSBSS-HE), the factor structure, reliability, and validity of the measure were examined. The primary analysis included service barriers for Campus Police, as more students had (a) heard of this resource, (b) not used this resource, and (c) answered the service barrier items for this resource compared to the other supports. In other words, Campus Police had the largest, most complete service barrier data. The psychometric properties of the survey items from Waves 1 (W1) and 2 (W2) of data collection are presented.
First, an exploratory factor analysis using principal component analysis (PCA) as the method of estimation with oblimin rotation was conducted. SPSS was used to estimate the PCA for the items representing psychological service barriers to using the Campus Police at W1 to determine the degree to which the individual items formed separate factors and confirmed theory. Prior to examining the factor structure, the Kaiser–Meyer–Olkin (KMO) Measure of Sampling Adequacy (KMO > .60) and Bartlett’s Test of Sphericity (null hypothesis that all off diagonal elements are 0; want to reject) were examined. To determine the number of factors, the eigenvalues, the scree plot, communalities, and the interpretability/utility of the factors were examined. Factor loadings were expected to be higher than 0.40 and communalities to be higher than 0.30. Second, the PCA was estimated restricting the factors to three based on theory and preliminary findings to see how well the factors replicated what was found in the first step. Third, the PCA was estimated with data from W2 to examine how well the factor structure replicated what was found at W1 as an indicator of test–retest validity (e.g., measurement is stable over time). Fourth, internal consistency was examined using Cronbach’s alpha for Campus Police supports at Waves 1 and 2. Fifth, correlations between scores at W1 and W2 were examined as an additional indicator of test–retest validity. Paired samples t tests were examined to determine if there were mean differences across waves. Finally, as a follow-up, preliminary evidence for the reliability of the factors was examined for three additional supports—the Counseling Center, Victim Advocacy, and Title IX Office.
Results
Descriptive Findings
Descriptive findings for Campus Police at W1 demonstrate that 79% of students within the sample had heard of this resource, yet, 89% of students did not seek help from Campus Police. At W2, more students had heard of Campus Police (93%), but the majority still did not make use of this resource (91% did not). For the Counseling Center, at both waves, a majority of students had heard of this resource (W1: 83%, W2: 96%), but most did not use this resource (W1: 52%, W2: 51%). For the campus Victim Advocate, more than half had heard of this resource at the first survey (W1: 58%) and three quarters had heard of it at the second survey (W2: 78%); but, most students did not seek help from this resource (W1: 72%, W2: 75%). Finally, for the Title IX Office on campus, a majority of survivors had heard of this resource (W1: 61%, W2: 78%), but most did not use it (W1: 84%, W2: 86%). The number of survivors completing the service barrier items for each resource was dependent upon (a) having heard of the resource and (b) having not used this resource. The largest service barrier sample was for the Campus Police (W1: n = 60, W2: n = 65); thus, this resource was used for the statistical analysis.
Factor Validity and Reliability (Campus Police)
Results of the initial and constrained PCA analysis (Steps 1 and 2) for W1 suggest that all items loaded onto one of three theorized scales based on the eigenvalues (>1; see Table 1), W1: KMO = 0.72, Bartlett’s Test: χ2(210) = 801.76, p = .000. There were no items that cross-loaded (factor loadings > 0.40 on multiple factors), suggesting a clean factor solution (i.e., items do not “fit” with more than one subscale). The three factors corresponded to the hypothesized service barrier scales: social-emotional (12 items), minimization (four items), and negative treatment (five items), and factor loadings ranged from 0.47–0.92. The three factors explained 59.81% of the variance (social-emotional barriers: 35.16%, minimization barriers: 14.35%, negative treatment barriers: 10.30%). The factor structure was stable and replicated from W1 and W2, W2: KMO = 0.79, Bartlett’s Test: χ2(210) = 1,090.69, p = .000. For W2, factor loadings ranged from 0.44–0.93. There was one item that cross-loaded on the minimization factor and the negative treatment factor (i.e., “I thought incidents like this are common”; factor loadings = 0.437 and 0.415, respectively). The factor structure explained 70.26% of the variance (social-emotional barriers: 50.17%, minimization barriers: 11.99%, negative treatment barriers: 8.11%). Taken together, these findings suggest that the items in the measure can be grouped into three subscales.
Principle Components Analysis Results.
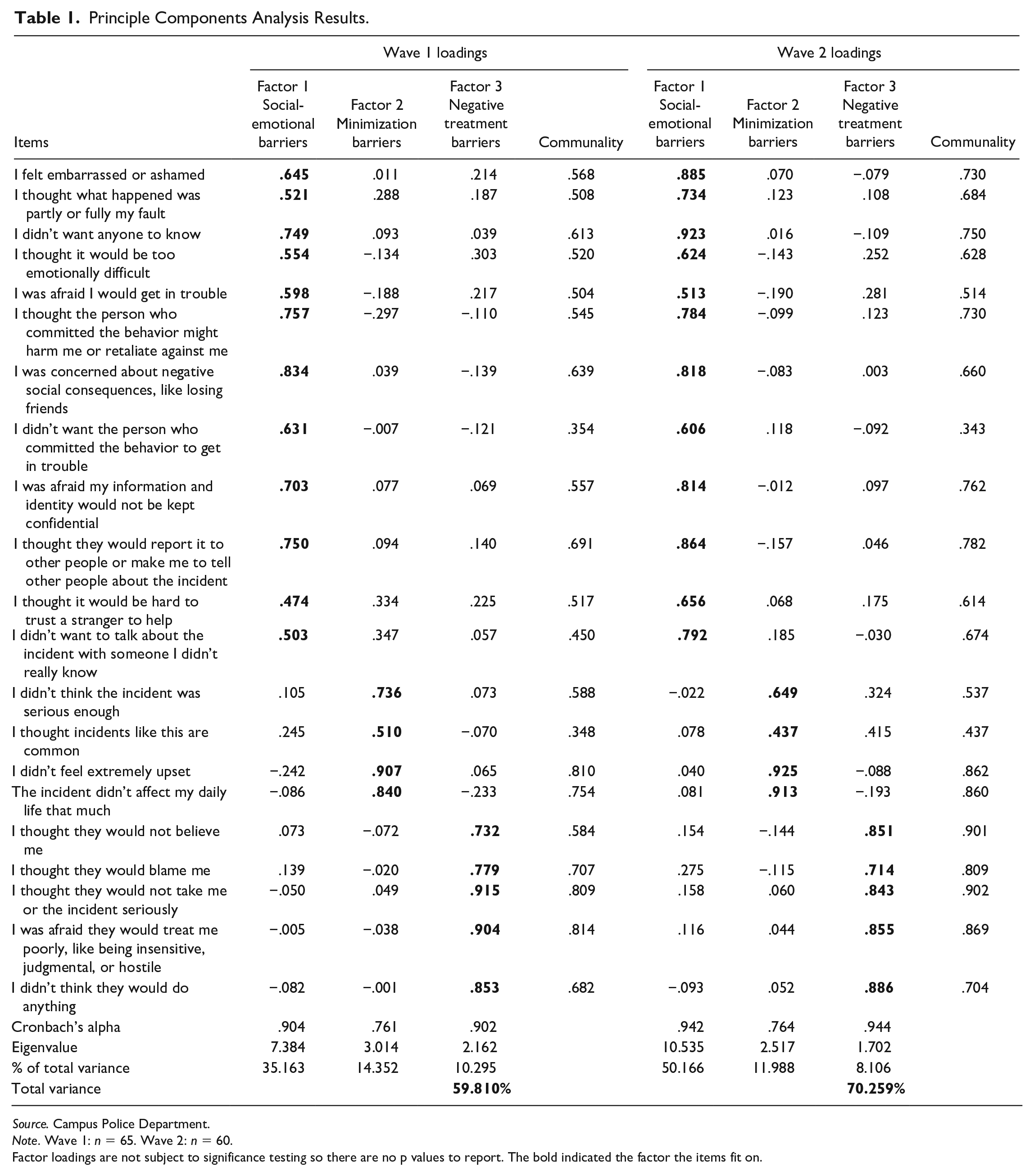
Source. Campus Police Department.
Note. Wave 1: n = 65. Wave 2: n = 60.
Factor loadings are not subject to significance testing so there are no p values to report. The bold indicated the factor the items fit on.
Based on this analysis and theoretical considerations, subscales were created by summing the items to measure social-emotional barriers (12 items, score range 0–36, W1: α = .90, W2: α = .94), minimization barriers (four items, score range 0–12, W1: α = .76, W2: α = .76), and negative treatment barriers (five items, score range 0–15, W1: α = .90, W2: α = .94). As another indicator of test–retest validity, correlations between measures at W1 and W2 were large and in the hypothesized direction (social-emotional barriers r = .74, minimization barriers r = .54, negative treatment barriers r = .79; see Table 2). This suggests that there was considerable stability in these service barriers over time. In addition, the means across waves were not statistically different for social-emotional barriers, t(47) = 0.55, p = .584, minimization barriers, t(46) = −0.74, p = .464, and negative treatment barriers, t(46) = −1.48, p = .145 (see Table 2).
Descriptive Statistics for Service Barriers Factors—Campus Police Resource.
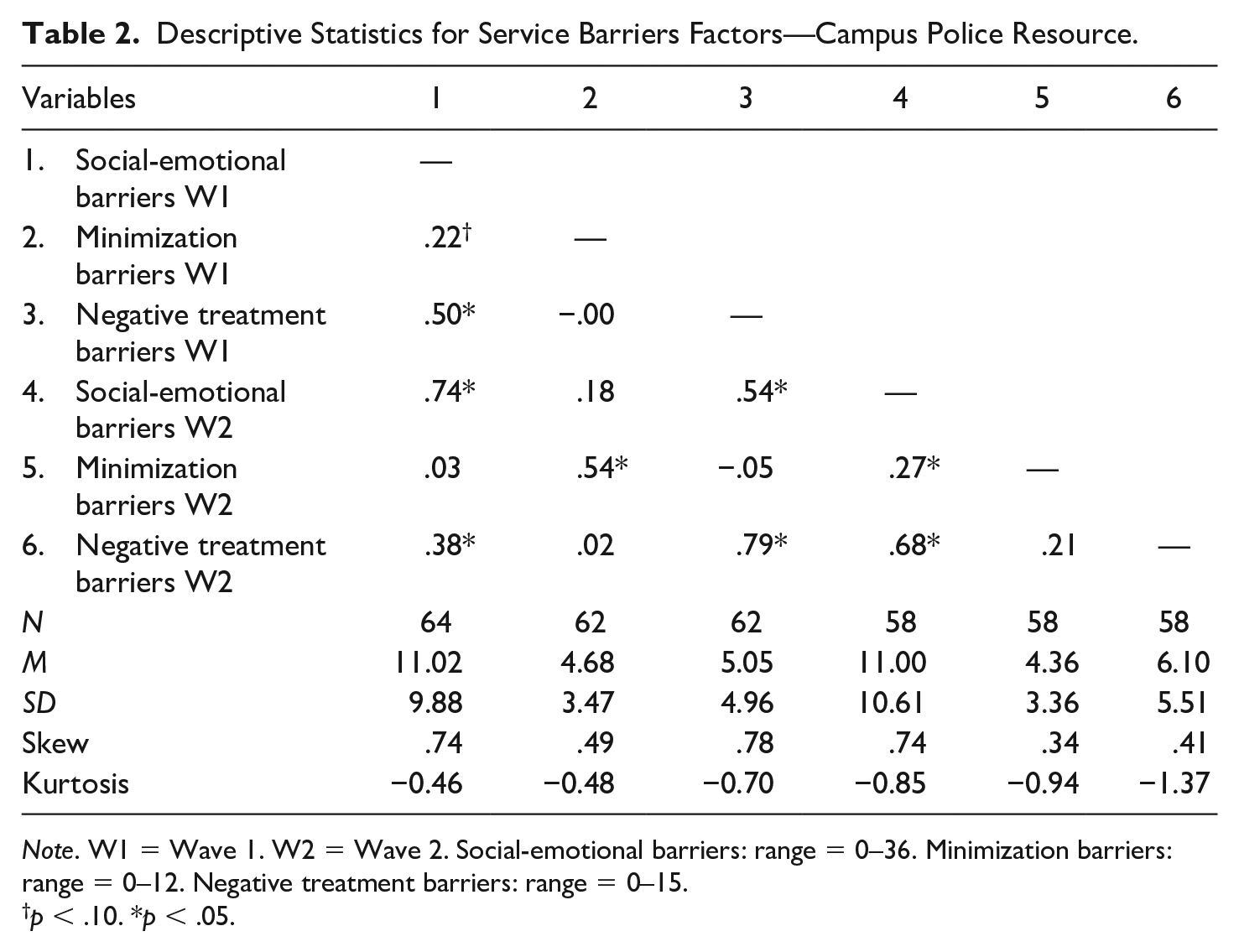
Note. W1 = Wave 1. W2 = Wave 2. Social-emotional barriers: range = 0–36. Minimization barriers: range = 0–12. Negative treatment barriers: range = 0–15.
p < .10. *p < .05.
Factor Reliability (Other Resources)
Although smaller samples of students completing service barrier items for the three other resources precluded testing factor structures across supports, the internal reliability and test–retest reliability of the three subscales was examined for the Counseling Center, Victim Advocacy, and Title IX Office. Table 3 presents the means, standard deviations, alphas for the subscales at W1 and W2, and the correlations between W1 and W2. These results suggest that the three subscales had adequate internal reliability across time for the Counseling Center, Victim Advocacy, and Title IX Office (i.e., the items in each subscale “fit together” for all of these supports). The significant correlations between the subscales at W1 and W2 also suggested adequate test–retest reliability of the measure across different formal supports (i.e., subscales are stable over time).
Descriptive Statistics and Reliability for Other Campus Resources.
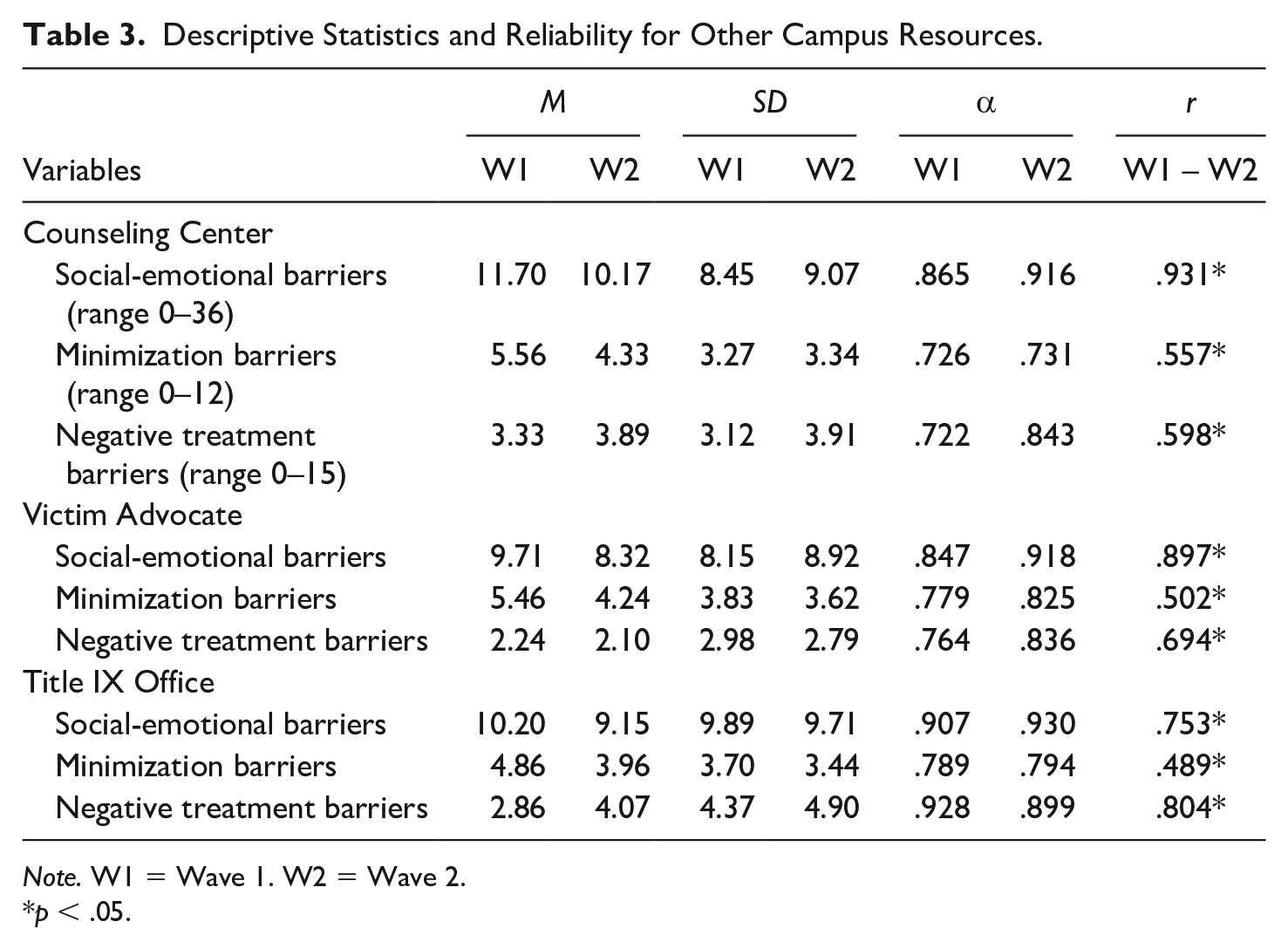
Note. W1 = Wave 1. W2 = Wave 2.
p < .05.
Finally, paired samples t tests were estimated for each of the supports. For the Counseling Center, there were no significant differences between means at W1 and W2 for negative treatment, t(24) = 0.33, p = .742, and minimization, t(24) = −0.07, p = .948, but there was a significant decrease in social-emotional barriers, t(24) = 2.85, p = .009. There were no mean differences between W1 and W2 for the Victim Advocate, social-emotional barriers: t(24) = 1.47, p = .153, minimization barriers: t(24) = 0.54, p = .593, negative treatment barriers: t(24) = −0.17, p = .864. For the Title IX Office, there was a significant increase in negative treatment barriers between W1 and W2, t(30) = −2.15, p = .040, but there were no differences for social-emotional barriers, t(30) = 1.07, p = .293, and minimization barriers, t(30) = 0.46, p = .651. These findings suggest that most service barriers did not increase or decrease between W1 and W2.
Discussion
The purpose of this study was to develop and provide preliminary evidence for a measure of psychological service barriers grounded in theory and research. Such a measure would allow for replication, comparison, and the examination of variability in service barriers experienced by college sexual assault survivors. The current findings provide the opportunity for a more uniform approach to the assessment of acceptability-related service barriers in the field. For the Campus Police, the results lend support for a three-factor structure for the Psychological Service Barriers for Sexual Assault Survivors in Higher Education (PSBSS-HE) measure: social-emotional barriers, minimization barriers, and negative treatment barriers.
The first subscale, social-emotional barriers, includes a variety of emotional reactions and beliefs that hinder survivors’ use of formal supports. This includes experiencing negative emotions (e.g., shame, self-blame), expecting negative social interactions to result from using a resource (e.g., discomfort from the lack of familiarity with the support provider, loss of confidentiality), and anticipating consequences for their life and/or well-being (e.g., fearing retaliation by the perpetrator, fearing ostracism in their social group). This subscale corroborates and synthesizes barriers that many previous studies have included in lists of reasons survivors did not use formal supports (e.g., Ameral et al., 2020; Fisher et al., 2003, 2016; Krebs et al., 2007; Nasta et al., 2005; Walsh et al., 2010; Zinzow & Thompson, 2011). The second subscale, negative treatment barriers, includes survivors’ assessments about a resource—specifically, their anticipation of receiving negative treatment at the hands of that service provider (e.g., they will not do anything, they will blame or doubt the victim, they will be judgmental and hostile). Although negative treatment is less frequently imagined to be a key barrier for survivors compared with social-emotional barriers (Allen et al., 2015; Sable et al., 2006), the items captured in this subscale have been identified and endorsed by survivors in prior research (e.g., Fisher et al., 2003; Holland & Cortina, 2017; Ollen et al., 2017; Richardson et al., 2015; Zinzow & Thompson, 2011). The final subscale, minimizing the assault, includes beliefs that minimize the seriousness of the assault and/or the psychological impact of the assault (e.g., not thinking it is bad enough to warrant using a resource). This subscale captures a service barrier that is very common among college sexual assault survivors (e.g., Carson et al., 2019; Holland & Cortina, 2017; Lindquist et al., 2016; Miller et al., 2011; Walsh et al., 2010).
The three factors had strong internal consistency and demonstrated test–retest reliability. These findings suggest that the items that comprise each subscale are important to measure together and that the subscales can be used to examine service barriers across time. Moreover, there was preliminary evidence for the three subscales for other campus resources—the Counseling Center, Victim Advocate, and Title IX Office. The subscales had adequate internal reliability across time for all three of these resources. The significant correlations between the subscales at W1 and W2 also suggest adequate test–retest reliability across different formal supports. These results imply that this new measure can be useful for assessing service barriers across a variety of campus supports and testing how service barriers differ across formal supports. This may be particularly useful in the wake of shifting Title IX guidance from the OCR; Candice Jackson (the prior acting assistant secretary for civil rights) rescinded prior Title IX guidance explicitly addressing college sexual assault and proposed new guidance that enhances protections for students accused of sexual assault (Jackson, 2017). Thus, researchers can establish how social policies that minimize and excuse sexual assault affect service barriers. This would be particularly helpful for determining which resources rouse concerns about negative treatment and designing interventions to improve service delivery by those resources.
Research Implications and Recommendations
A comprehensive measure of psychological service barriers will allow researchers to evaluate service barriers more consistently (e.g., across samples and institutions) and determine how service barriers are associated with other key variables. For example, the measure can be useful for examining potential differences in service barriers across survivor groups (e.g., gender, sexuality, race/ethnicity). Students who hold stigmatized and marginalized identities may face different and/or more service barriers after an assault (Brubaker et al., 2017). College women report more negative changes after experiencing sexual assault compared with men (e.g., in their academic plans, health, sexual intimacy; Banyard et al., 2007), but women are also more likely to seek help from formal supports than men (Ameral et al., 2020; Banyard et al., 2007). Other research has found some differences in sexual assault survivors’ resource use based on sexual identity; for instance, a study by Eisenberg and colleagues (2021) found that 12.1% of sexual minority men versus 2.7% of heterosexual men used health care services after an assault. However, other studies have found similar (low) rates of resource use among heterosexual and sexual minority sexual assault survivors (Richardson et al., 2015; Spencer et al., 2017). These studies provide some insight into group differences in service use but using an established measure of service barriers would allow researchers to test differences in survivors’ service barrier experiences more consistently.
In addition, this new measure can be used to test how service barriers relate to survivors’ mental health outcomes. A few research studies have found evidence to suggest that certain service barriers may be more strongly related to negative mental health outcomes for campus assault survivors (e.g., Carson et al., 2019; Miller et al., 2011). Research with military sexual assault survivors also suggests that experiencing greater psychological service barriers may exacerbate symptoms of posttraumatic stress and depression (Holland et al., 2016). These cross-sectional studies used different measures of service barriers—often combining elements of social-emotional and negative treatment barriers—so an established measure of service barriers would allow for more consistent assessment of service barriers and analysis of how these barriers relate to mental health outcomes over time. This knowledge will allow researchers to identify novel ways to mitigate service barriers.
This study also informs recommendations for researchers interested in using this measure of psychological service barriers. One recommendation is that researchers should ask participants about their awareness of resources first, and then ask about service barriers separately for each resource. Awareness of a service is necessary to accurately assess service barriers for that resource. Nasta and colleagues (2005) found that sexual assault survivors had greatest awareness of the campus Counseling Center, followed by health services, Campus Police, and the women’s center. Similarly, in this study, participants had the greatest awareness of the Counseling Center and Campus Police. Asking about service barriers for each resource separately will also allow the opportunity to examine whether psychological service barriers differ across resources (as suggested in previous research, for example, Holland & Cortina, 2017) and whether service barriers for a particular type of support (e.g., a campus Counseling Center) differ across institutions.
Second, researchers interested in assessing other factors associated with survivors’ use of formal resources could assess them with additional, context-specific measures. For example, prior research has asked detailed questions after a measure of sexual assault (e.g., the Sexual Experiences Survey, Koss et al., 2007; the National College Women Sexual Victimization Survey, Fisher et al., 2003; the College Sexual Assault Study, Krebs et al., 2007) to gather information on assault characteristics, such as alcohol use, physical injury, assault location, and perpetrator–victim relationship. Researchers have used these detailed assault characteristics to predict whether or not a report was made (e.g., Fisher et al., 2003; Lindquist et al., 2013; Spencer et al., 2017; Wolitzky-Taylor et al., 2011) and the reasons for not reporting the assault to the police (e.g., Thompson et al., 2007). Including separate questions about assault characteristics of interest will yield more nuanced and interpretable data than more general questions about barriers related to assault characteristics (e.g., because of where the incident happened). Similarly, prior research suggests that survivors’ decision to cope on their own is a decision distinct from the processes of deciding to use formal resources and experiencing barriers to using resources (DeLoveh & Cattaneo, 2017). Therefore, it may be useful for researchers to include a validated measure of coping that assesses a wide range of coping strategies in addition to psychological service barriers. Finally, accessibility barriers will differ across institutions, for example, the cost and location of services. If researchers are interested in understanding such logistical barriers, they may consider including context-relevant items (see the appendix for example accessibility barrier items included in the pilot). More detailed measures of the other reasons that survivors do not use formal resources allow researchers to examine how these factors are associated with service use and psychological service barriers.
Limitations
Limitations to this research must be acknowledged and then addressed in future research. First, the non-probability sample collected at a single, 4-year public university limits the generalizability of the findings. In addition, the sample size limited the ability to validate findings using Confirmatory Factor Analysis in multiple samples. This study was a first critical step in validating a measure of psychological barriers, but future research—including a larger sample of sexual assault survivors across institutions of higher education—is needed to explicitly test how the factor structure of this measure replicates across samples.
Although the sample was diverse in terms of sexual identity (a result of one aim of the pilot study in which the measure was embedded), the size and composition of the sample did not allow us to test how the factor structure held across identity groups (e.g., race/ethnicity, gender, sexuality). It will be essential for future research to test how this measure functions within and across survivor groups, and especially among survivors with marginalized social identities.
Finally, there are limitations to assessing the psychometric properties of a new measure that is embedded in an ongoing pilot study. Some potentially valuable psychometric properties, including reliability across subgroups and concurrent and discriminant validity were not assessed in this study. More research will be needed to assess these psychometric properties. Embedding the measure in an ongoing pilot aimed at understanding sexual assault survivors’ use of a variety of campus resources allowed us to test preliminary evidence for the measure across several campus resources; however, future research will need to collect more data to test the factor structure and other indicators of reliability and validity across supports.
Conclusion
Addressing several gaps in the literature, this study offers a new measure of service barriers that is grounded in theory and empirical evidence. The current findings suggest that college sexual assault survivors face three overarching psychological service barriers: social-emotional, negative treatment, and minimization. This study offers preliminary evidence for the psychometric properties of this measure and lays the groundwork for future research to further validate this measure. This work is essential, as a comprehensive measure of psychological service barriers will provide needed insight into the function of service barriers in sexual assault survivors’ lives and how to mitigate them.
Footnotes
Appendix
Acknowledgements
The authors thank the service providers and administrators who assisted in advertising this study, the research assistants who helped facilitate the study, and the students who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by Nebraska Tobacco Settlement Biomedical Research Development Funds and a University of Nebraska Foundation Layman Seed Research Grant.